
Abstract
Aim
To assess the mechanical properties of different types of intraradicular retainers using a tensile test and the failure types.
Materials and Methods
Sixty single-rooted mandibular premolars underwent endodontic treatment and were divided into three groups: The cast metal core (CMC) group, in which the CMC was cemented with zinc phosphate sealer; the CAD/CAM group, in which the fiberglass post was fabricated with the CAD/CAM system; and the prefabricated fiberglass post (PFP) group, in which a prefabricated fiberglass post was used. The latter two groups were cemented with Relyx® U200 resin sealer. Tensile strength tests were conducted on the specimens, followed by analysis under an microscope to determine failure types. The normality of tensile strength values was confirmed using the Shapiro–Wilk test. Group comparisons were made via one-way ANOVA with Tukey’s HSD post hoc test.
Results
The CMC group exhibited the highest mean tensile strength, followed by the CAD/CAM and PFP groups (p < .001). Predominantly post-localized failures occurred mainly in the PFP group, while cohesive root failures were observed only in the CMC group (p < .05). Adhesive failures at the sealer–dentin were more frequent in the CAD/CAM post group, whereas mixed failures (dentin/post) were noted in the CMC group (p < .05).
Conclusion
While cast metal core demonstrated superior strength, its use may lead to root cohesive failures. Understanding these mechanical behaviors and failure patterns can inform treatment strategies and minimize complications.
Highlight Key Points
The mechanical performance and failure modes of different types of retainers can enhance treatment outcomes and mitigate associated risks.
The cast metal core (CMC) group outperformed the milled fiberglass post groups in the CAD/CAM system and prefabricated fiberglass post (PFP) when subjected to the tensile test.
Cohesive failures were observed in the CMC group, highlighting the disadvantage of employing this type of intraradicular retainer.
Introduction
To achieve a successful and enduring endodontic treatment, proper coronal restoration is crucial alongside adherence to current cleaning and shaping standards.1, 2 In this context, without adequate restoration, the root canal system risks recontamination and treatment failure. Therefore, immediate coronal restoration post-endodontic treatment completion is imperative. 3 The choice of restoration depends on the amount of remaining tooth structure after carious tissue removal and creating the endodontic access. 4 For teeth with minimal remaining structure, a cast metal core (CMC) is recommended, while fiberglass posts are suitable for teeth with sufficient dentin depth. 3 CMCs offer precise adaptation but may contribute to root fractures due to their high modulus of elasticity and compromised esthetics.
Conversely, prefabricated fiberglass posts (PFPs) have a modulus of elasticity similar to dentin, which reduces fracture risk and provides better esthetics and adhesion. 5 However, PFPs lack precise adaptation to the root canal shape. 4 To solve the adaptation problem of PFP, fiberglass blocks milled in the CAD/CAM system based on a scan of the intraradicular space have been introduced. This new material aims to combine the esthetic and adhesive advantages of PFP with the excellent adaptation of CMC.4, 6
This study aimed to investigate the tensile strength and failure mode of three intraradicular retainers: CMCs, CAD/CAM-fabricated fiberglass posts, and PFPs. The null hypothesis tested whether there would be no significant difference in tensile strength between CMCs and CAD/CAM-fabricated fiberglass posts, as both are fabricated from precise impressions. Regarding failure mode, the null hypothesis was that there would be a significant difference between the two types of fiberglass posts due to differences in modulus of elasticity, impacting fracture susceptibility.
Materials and Methods
This study was approved by the São Leopoldo Ethics and Research Committee (approval number: CAAE 03482818.5.0000.5374). Sixty human single-rooted mandibular premolars were directly obtained from extraction for several reasons. Sample size determination was based on the effect size observed in a previous study by Karzoun et al. 7 An effect size of 1.53 (Cohen’s f) was observed. Assuming a type I error of 5% (study confidence level of 95%) and a type II error of 20% (study power of 80%), the effect size observed in that study indicates that a minimum of nine samples required in each study group. For three experimental groups, the calculated minimum total sample size was 27 teeth. The calculations were performed using the statistical software G*Power (version 3.1.9.4, Heinrich Heine University, Düesseldorf, Germany). A power of 88.57% is expected for this sample.
Inclusion criteria were straight roots of at least 13 mm length, absence of caries, cracks, fractures, and prior endodontic intervention, with foraminal diameter standardized using a 15/.02 C pilot file. (VDW GmbH, Munich, Germany).
The specimens were stored in a 0.1% thymol solution and cleaned through prophylaxis. After cleaning, the crowns were sectioned using a double-sided diamond disk (KG Sorensen, São Paulo, Brazil) attached to a handpiece and micromotor (Kavo do Brazil Ind. and Com. Ltda., Joinville, Brazil), with an air/water spray for cooling. This process left a 2 mm coronal remnant (ferrule) on each specimen.
The specimens were measured with a caliper (Bio-Art, São Paulo, Brazil) to ensure a minimum total length of 15 mm, including both the root and ferrule. The working canal length was established using a 15/.02 C pilot file (VDW), with the length set as 1 mm short of the apex.
To encase the roots, a 3-mm-thick layer of Filtek Z250 composite resin (3M Dental Products Ltd., São Paulo, Brazil) was applied to the apical third of the roots. This provided stability during the tensile test by securing the roots within the acrylic resin block.
The roots were vertically inserted 2 mm into a pre-prepared acrylic plate, with the apical portions facing upward, and fixed in place using utility wax (Wilson Polidental, São Paulo, Brazil). A PVC ring (21 mm in diameter and 20 mm in height) was centered around the fixed roots, with its edges sealed using heated wax (Wilson Polidental) to prevent material spillage. The PVC ring was then filled with self-polymerizing acrylic resin JET (Clássico Dental Articles, São Paulo, Brazil).
After the initial polymerization stage, the specimens were immersed in water for 12 h. Following this period, the abutments were removed from the acrylic plate by immersing them in water heated to 50 °C, and the endodontic treatment was initiated for the samples. Endodontic treatment was performed with Reciproc R40 files (VDW) coupled with the X-Smart IQ motor (Dentsply Sirona, Ballaigues, Switzerland). During instrumentation, each canal was irrigated with 20 mL of 2.5% sodium hypochlorite (NaOCl) (Asfer Chemical Industry Ltd., São Caetano do Sul, Brazil).
For the final irrigation protocol, 5 mL of 17% EDTA (Biodinâmica Chemical and Pharm. Ltda., Ibiporã, Brazil) and 5 mL of 2.5% NaOCl (Asfer) were used. This final solution was agitated using the Irrisonic E1 insert (Helse Ultrasonic, Santa Rosa do Viterbo, Brazil) at a frequency of 30,000 Hz. Following irrigation, the canals were aspirated with a capillary tip (Ultradent, Induiutaba, Brazil) and dried using absorbent paper tips (Tanari Industrial Ltda., Manacapuru, Brazil). The drying was followed by obturation using the Tagger hybrid technique, which involved R40 gutta-percha cones (VDW) and AH Plus Jet sealer (Dentsply Sirona). After the endodontic treatment, the samples were wrapped in gauze (Cremer, Itapeva, Brazil) and stored in distilled water (Asfer) at 37 °C for 24 h.
The teeth were randomized divided into three experimental groups: Cast metal core (CMC) Milled fiberglass post groups in the CAD/CAM system (CAD/CAM) Prefabricated fiberglass post (PFP)
For the CMC and CAD/CAM groups, the preparation for the intraradicular retainer was performed with a size 4 Largo bur (Dentsply) to a depth of 10 mm, followed by post space cleaning with a canal brush (MK Life, Porto Alegre, Brazil) and saline solution. The drying was performed with a capillary tip aspirator (Ultradent) and absorbent paper tips (Tanari). The root dentin was treated with KY gel (Jonson and Jonson Ltda, São Paulo, Brazil) applied with a microbrush (Angelus, Londrina, Brazil), and the post molding was performed with the self-polymerizing red acrylic resin Pattern Bright (Kota Dental Products, Cotia, Brazil) and Pinjet posts (Angelus). Finishing was performed with a Minicut tungsten cutter (American Burss, Palhoça, Brazil) attached to a straight handpiece and micromotor (Kavo do Brasil Ind. and Com. Ltda., Joinville, Brazil). The molds were sent to the laboratory for casting CMC in a nickel-chromium alloy, while the samples of the CAD/CAM group were milled in Fiber Cad glass fiber blocks (Angelus).
For the PFP group, the preparation for the intraradicular retainer was performed with the drill provided by the manufacturer in the Exacto System Fiberglass Post Kit #1 (Angelus) at a depth of 10 mm. The samples were cleaned and dried in the same way as the CMC and CAD/CAM groups.
In the CMC group, the samples were cemented with zinc phosphate sealer (SS White Dental Products Ltd., Rio de Janeiro, Brazil), which was applied into the canal using a Lentulo Spiral #25 (MK Life, Porto Alegre, Brazil). In the CAD/CAM and PFP groups, the fiberglass posts were silanized (Angelus) and cemented with Relyx U200 self-adhesive resin sealer (3M) using precision syringe injection needles (Maquira Dental Group, Maringá, Brazil). Each sample underwent light-curing for 40 s with the Valo curing device (Ultradent). Before cementing the intraradicular retainers, the roots in all three groups were etched with 37% phosphoric acid (FGM Dental Group, Joinville, Brazil) for 15 s. Following cementation, specimens from all three groups were wrapped in gauze (Cremer) and stored in distilled water (Asfer) at 37 °C for 24 h to allow the sealer to set.
Tensile Test of the Intraradicular Retainers
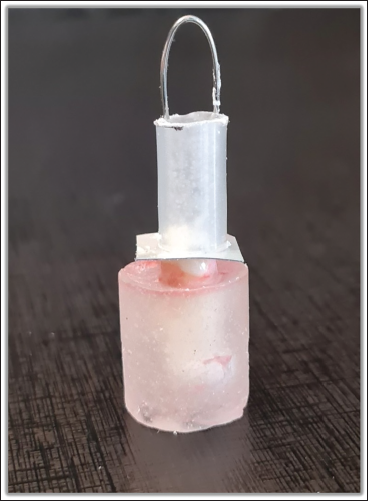
For the tensile test, a cylinder of acrylic resin with a metal eyelet on the coronal part of the post was fabricated (Figure 1). To create these cylinders, plastic anesthetic tubes (SS White) measuring 1.5 cm in length were affixed with wax #7 (Wilson Polidental) onto radiographic films (Carestream Dental Brazil, São José dos Campos, Brazil). These films had a central perforation allowing penetration into the coronal part of the cemented post. The self-polymerizing acrylic resin JET (Clássico Dental) was poured into each cylinder. A 0.8 mm orthodontic wire loop (Morelli Dental Products, Sorocaba, Brazil) was then positioned at the top of the cylinder.
Representative Specimen of the Different Types of Intraradicular Retainers Tested in the Present Study.
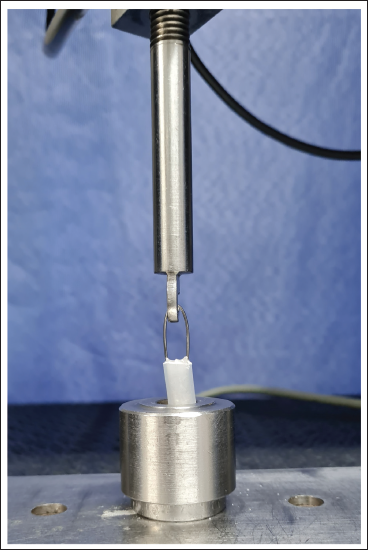
After resin polymerization, the specimen was positioned in the EMIC universal testing machine, model DL 2000 (Instron Brazil Ltda, São José dos Pinhais, Brazil) (Figure 2), where an axial tensile load was applied at a speed of 0.5 mm/min. For this purpose, the acrylic resin cylinder containing the root was affixed to the machine base, and the metal loop with its clips was attached to a 200 kilogram-force (kgf) load cell. Upon detachment of the post, the machine operation ceased automatically, and the force values in kgf were recorded and tabulated for statistical analysis.
EMIC Universal Testing Machine, Model DL 2000, Utilized for Tensile Testing of Intraradicular Retainers.
When the tensile test was finished, the sixty samples underwent analysis under microscope at 5× magnification (Alliance, São Carlos, Brazil) to determine the predominant failure mode in each group. These failures were classified as cohesive failure, occurring when either the post or the root broke during the tensile test, and adhesive failure, occurring when the post detached from the root without specimen breakage.
For specimens showing adhesive failure, microscopic analysis was conducted to identify whether the failure transpired at the sealer–dentin or sealer–post interface, or if it was a mixed failure involving both dentin and post. The resulting data were recorded and tabulated for subsequent statistical analysis.
Results
The tensile strength data were analyzed using IBM SPSS software (version 26.0, IBM Corporation, Armonk, New York, USA). The analysis began with the Shapiro–Wilk test, which confirmed that the tensile strength values were normally distributed across all test groups. Subsequently, groups were compared using one-way ANOVA with Tukey’s HSD multiple comparisons post-test. Magnitudes of the differences between groups (Cohen’s f and d) were calculated using G*Power software (version 3.1.9.4, Heinrich Heine University, Düesseldorf, Germany), and distribution plots of obtained values were generated using GraphPad Prism software (version 9.0.0, GraphPad Software, San Diego, CA, USA). Pearson’s chi-square test with Yates’ continuity correction was employed to compare the frequency distributions of observed failure types across experimental groups. A significance level of 5% was assumed for all analyses.
The highest mean tensile strength was observed in the CMC group, followed by the CAD/CAM group, and the final group, PF, exhibited the lowest mean tensile strength (Table 1). Statistically significant differences were found when comparing the test groups (p < .001), with a considerable difference between the compared groups. Specifically, significant differences were noted between the CMC and CAD/CAM groups (p = .011; Cohen’s d = 0.86), considered a large effect size, and between the CMC and PF groups (p < .001; Cohen’s d = 1.25), also considered a large effect size. However, no statistically significant difference was observed between the CAD/CAM and PF groups (p = .383; Cohen’s d = 0.54), considered a moderate effect size.
Comparison of the Tensile Strength Values (kgf) Determined for the Different Test Groups.
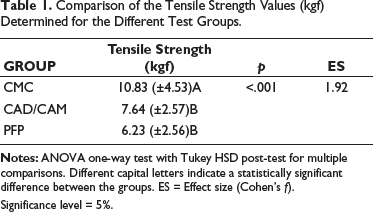
Significance level = 5%.
Based on the results and the effect size of the group comparisons, the study’s evidence strength was estimated at 97.85%. Table 2 illustrates that the distribution of cohesive failure types varied among the test groups (p < .05). Cohesive failures in the post area predominantly occurred in the PFP group, while cohesive failures in the root area were exclusively observed in the CMC group. The absence of cohesive failure was similarly distributed across post types. Adhesive failures also exhibited different distributions among the study groups (p < .05). Adhesive failures at the sealer–dentin interface were more prevalent in the CAD/CAM group, whereas mixed failures (dentin–post) were more common in the CMC group. The absence of adhesive failure was more frequently observed in the PFP group.
Comparison Between the Test Groups Regarding the Distribution of the Observed Failure Types.
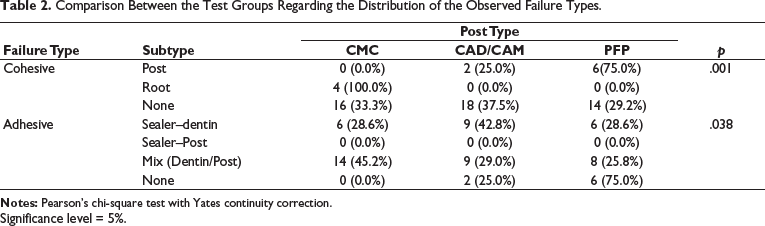
Significance level = 5%.
Discussion
To achieve successful and long-lasting endodontic treatment, proper coronal restoration plays a pivotal role, along with adherence to modern standards of cleaning and shaping.1, 2 Without an adequate restoration, the root canal system is at risk of recontamination, which can ultimately lead to treatment failure. Thus, immediate coronal restoration after the completion of endodontic therapy is not merely recommended but essential. 3
The choice of restoration is inherently dictated by the amount of remaining tooth structure following the removal of carious tissue and the endodontic access. 4 When minimal tooth structure remains, CMCs are often the preferred option, whereas fiberglass posts are considered more appropriate for teeth with sufficient dentin walls. 3 While CMCs offer precise adaptation to the tooth structure, their high modulus of elasticity, combined with limited esthetic value, may predispose the tooth to root fractures. This presents a significant clinical challenge, highlighting the need for careful case selection and restoration technique to balance durability, aesthetics, and functional outcomes.
The results of the tensile tests revealed that the CMC group showed significantly higher tensile strength compared to the PFP and CAD/CAM groups, thereby leading to the rejection of the first null hypothesis. Conversely, no statistically significant difference was observed between the CAD/CAM and PFP groups. These findings align with those reported in previous studies.8, 9
Cohesive root failures were exclusively identified in the CMC group, corroborating the results of prior research.9, 10 Furthermore, cohesive failures within the post region were more prevalent in the PFP group, indicating a greater susceptibility to fractures when compared to the CMC and CAD/CAM groups. This observed discrepancy among the groups can be attributed to differences in the modulus of elasticity of the materials used.
Additionally, variations in adhesive failure patterns were observed, demonstrating a stronger bond interface between the post and the sealer relative to the bond between the sealer and the dentin. These findings are consistent with previously documented evidence.8, 11, 12 Based on these observations, the second null hypothesis was accepted.
The tensile test was chosen for this study as it allows for the evaluation of the mechanical resistance of three distinct types of intraradicular retainers without altering the design of the post, and also simplifies the complex forces encountered in clinical mastication. This is in contrast to the push-out test, which requires sectioning of the sample.8, 13, 14 Consequently, the authors suggest that a clinical study investigating the adhesive strength of fiberglass posts to root dentin would be invaluable for both the scientific community and dental practitioners.
Although the CAD/CAM and PFP groups in this study were cemented using adhesive sealers, while the CMC group employed zinc phosphate sealer, existing literature highlights the advantages of adhesive cementation for CMCs. Adhesive cementation has been shown to enhance retention in the root canal and reduce the likelihood of root fractures when compared to conventional cementation techniques. 15 These observations emphasize the critical role of selecting an appropriate cementation system to ensure the quality and durability of intraradicular restorations.
Despite the limitations associated with CMCs, including their higher tensile strength but increased susceptibility to root fractures, CAD/CAM fiberglass posts have emerged as a compelling alternative for the restoration of endodontically treated teeth, particularly in situations involving extensive loss of coronal structure.9, 12, 15, 16 These posts offer aesthetic advantages and possess a modulus of elasticity similar to dentin. However, their adaptation to the remaining tooth structure is significantly influenced by the process used to obtain an impression of the root canal, showing the importance of precision in this step of the restorative workflow.
The study clearly demonstrates that CMCs exhibit the highest mean tensile strength, but critically, only the CMC group experienced cohesive root failures.8, 13, 14 This presents a significant clinical implication, as understanding these mechanical behaviors and failure patterns can inform treatment strategies to minimize complications, urging caution despite CMC’s strength. Conversely, CAD/CAM fiberglass posts are highlighted as a compelling alternative, offering aesthetic advantages and a modulus of elasticity similar to dentin, especially in cases of extensive coronal destruction.9, 12, 15 These findings largely align with previous studies that also reported higher tensile strength for CMCs8, 9 and corroborated the occurrence of cohesive root failures exclusively in the CMC group.9, 10
However, the primary limitation of this study is its in vitro nature, which does not fully replicate the complex oral environment. Furthermore, the use of different cementation agents, zinc phosphate for CMCs versus adhesive resin for fiberglass posts, represents a methodological limitation that could influence the results.8, 13, 14
To mitigate potential adaptation errors of posts produced with the semi-digital approach, proper preparation of the core’s cervical margins is essential, ensuring perpendicular angles and well-defined edges for accurate scanning of the acrylic resin mold and subsequent precise milling.17, 18 The analyses indicated that CAD/CAM fiberglass posts were more effective in terms of bond strength and post adaptation compared to PFP and achieved similar outcomes to CMC.12, 16, 19 Nonetheless, there remains debate regarding the biomechanical behavior of various intraradicular retainers. A clinical study investigating the adhesive strength of fiberglass posts to root dentin would be invaluable to both the scientific community and dental practitioners.
Conclusion
Within the limitations of this in vitro study, it was concluded that the CMC group outperformed the milled fiberglass post groups in the CAD/CAM system and PFP when subjected to the tensile test. However, cohesive failures resulting in root fractures were solely observed in the CMC group, highlighting the disadvantage of employing this type of intraradicular retainer.
Footnotes
Authors’ Contribution
Conception and design were performed by V, L; R, DG.
Material preparation, data collection, and analysis were performed by V, L; M, AS; L, AG; N, WM; F, CE; P, RA; B, CE.
The first draft of the manuscript was written by L, AG; R, G; MA, M; M, AS.
All authors commented on previous versions of the manuscript.
All authors read and approved the final manuscript.
Data Availability Statement
All data supporting the findings of this study are available in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Human teeth were used after approval from the Ethics Committee (approval number: 03482818.5.0000.5374).
Funding and Acknowledgment
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) (E-26/200.184/2023) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (446114/2024-3), Brazilian Governmental Institutions.
Informed Consent
Informed consent was obtained from all individual participants included in the study.