
Abstract
Background
Fixed orthodontic appliances are essential for correcting malocclusions but often induce discomfort and pose challenges to maintaining oral hygiene. Pain and gingival issues are among the most common complaints, yet few studies have assessed both parameters comprehensively.
Aim
This study aimed to evaluate the levels of pain and gingival health among patients undergoing fixed orthodontic treatment using a structured, questionnaire-based approach.
Methods
A cross-sectional study was carried out among 110 orthodontic patients, aged 18–35 years, who had received treatment using the 0.22-slot MBT bracket system. Two questionnaires were administered: one assessing pain 24 hours after appliance placement using the Modified McGill Pain Questionnaire and visual analog scale (VAS) and another evaluating gingival health 2 months post-treatment initiation. Descriptive statistics were employed for data analysis.
Results
Over 70% of participants reported nonpainful sensations such as pressure, aching, and soreness according to the McGill Pain Questionnaire descriptors. Descriptive terms like miserable, strange, and annoying were frequently associated with higher subjective pain perception. Numeric pain intensity measured by the VAS showed that average scores remained within the mild-to-moderate range, with no participants reporting consistently severe pain. Regarding gingival health, 30% reported bad breath, 29.1% had difficulty brushing, and 24.5% experienced spontaneous gum bleeding. Only 18.2% perceived an improvement in gingival health during treatment.
Conclusion
The study highlights that while many patients experience discomfort during fixed orthodontic treatment, subjective pain perception varies and is best understood through qualitative descriptors alongside numeric VAS scores. Gingival health issues remain prevalent, underscoring the importance of targeted oral hygiene reinforcement. A comprehensive assessment of both pain quality and intensity is essential for improving patient management and compliance during orthodontic care.
Keywords
Introduction
Crowded or misaligned teeth are common malocclusions that make oral hygiene more difficult. According to Ainamo (1972), misalignment hampers effective cleaning, and fixed orthodontic appliances can further irritate soft tissues due to components like bands and bonded attachments. 1 These factors contribute to changes in the oral microbial environment and plaque composition. 2 Zachrisson and Zachrisson (1972) observed that even with good hygiene and regular encouragement, orthodontic patients often develop mild-to-moderate gingivitis within 1–2 months of starting treatment. 3 Inflammation may cause bleeding, swelling, and discomfort, potentially affecting treatment outcomes if it progresses to periodontitis. However, the need for strict hygiene during treatment can foster lasting positive habits.2, 4
Pain is also a common concern. Patients report sensations such as tightness, pressure, soreness, and general discomfort during orthodontic treatment.5–8 This can impact eating, brushing, and self-esteem, particularly during appliance placement, activation, or removal.9, 10 Although typically short-lived, pain can deter individuals from seeking or continuing treatment and reduce compliance. 11
Despite 90% of orthodontic patients experiencing pain, most studies focus only on intensity—often measured using visual analog scales (VAS)—with little attention to pain quality or type.12–15 Other tools like verbal rating scales and pressure algometry are underutilized.16, 17 Understanding pain’s nature is critical, especially for those genetically predisposed to heightened sensitivity, as unmanaged pain may lead to central sensitization.18, 19
There is a lack of questionnaire-based studies evaluating both pain and gingival issues in early treatment stages. This study aims to fill that gap by assessing patient-reported pain and gum problems at 24 hours and 2 months using a structured questionnaire, ultimately aiming to improve orthodontic care and hygiene practices.
Aims and Objectives
Aim
The aim of this study was To assess the pain levels and gingival health of patients receiving fixed orthodontic treatment using a questionnaire.
Objectives
Assess the level of pain experienced by patients 24 hours after receiving fixed orthodontic treatment using a questionnaire.
Assess the gingival health of patients 2 months after the initiation of fixed orthodontic treatment using a questionnaire.
Materials and Methods
Sample Size
Considering 45% prevalence of pain after 24 hours of orthodontic treatment, minimum 110 patients was undertaken to achieve 95% confidence with 20% relative precision.
Statistical Plan
Descriptive statistics like frequency, percentage, mean, and standard deviation (SD).
Kruskal–Wallis test to compare differences across pain descriptors. Post-hoc pairwise comparisons were conducted where applicable. A p value less than .05 was considered statistically significant.
Categorical data from the questionnaire were analyzed using chi-squared tests to evaluate differences in responses. A p value of less than .05 was considered statistically significant.
Inclusion and Exclusion Criteria
Methodology
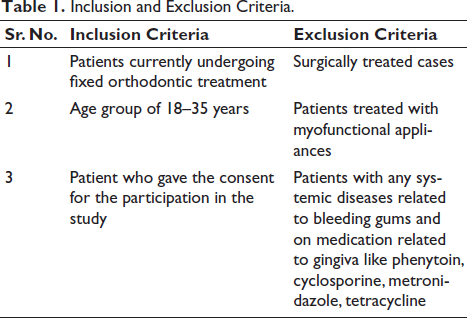
The study included 110 orthodontic patients treated with the 0.22-slot MBT bracket system, and each consenting participant was asked to complete a two-part questionnaire. Table 1 outlines the criteria for inclusion and exclusion of patients participating in the study.
Inclusion and Exclusion Criteria.
Part One: Assessment of pain 24 hours after the initiation of fixed orthodontic treatment.
Part Two: Evaluation of gingival health 2 months after the commencement of fixed orthodontic treatment.
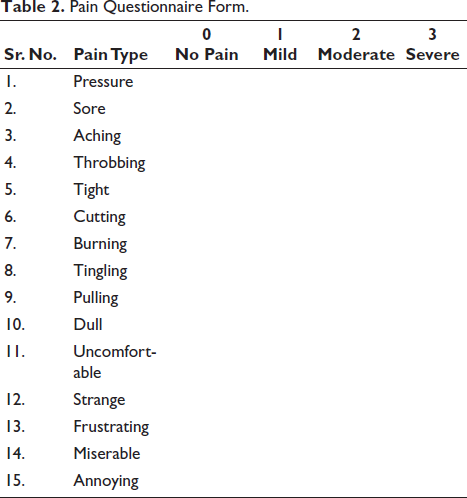
Pain was assessed using the Modified McGill Pain Questionnaire, 20 which included the VAS. This form addresses various dimensions of pain experienced by patients during orthodontic treatment. The tool has demonstrated reliability and effectiveness in assessing pain among orthodontic patients and has shown strong correlation with VAS in previous studies.
Gingival health was evaluated using a structured questionnaire designed to assess gingiva-related issues experienced by patients 2 months after the initiation of fixed orthodontic treatment. 21
Pain Questionnaire Form
The words below are sometimes used to explain how your mouth feels while you have braces. Place an
Pain Questionnaire Form.
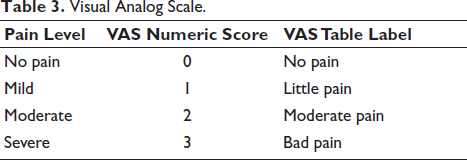
Visual Analog Scale.
Gingival Health Questionnaire Form
The questions was a mix of multiple-choice questions. After getting informed consent, gender, and age, the following questions will be asked: 1. How many times a day do you brush? ONCE/TWICE A DAY 2. Do you experience spontaneous bleeding from your gums after brushing? YES/NO 3. Do you observe enlargement in your gums? YES/NO 4. Do you experience itching of gums? YES/NO 5. Do you experience food lodgment in your gums? YES/NO 6. Do you experience pain in your gums? YES/NO 7. Do you face difficulty in brushing your teeth? YES/NO 8. Have you experienced a bad breath from your mouth during fixed orthodontic treatment? YES/NO 9. Do you think this orthodontic treatment have improved your gum health? YES/NO 10. How would you rate your ongoing orthodontic treatment experience from 1 to 5? Very good Very bad Good Average Bad
Result
Table 4 presents the distribution of pain descriptors reported by participants, categorized by severity (“No Pain,” “Mild,” “Moderate,” “Severe”) and converted to VAS scores (0 = No pain, 1 = Little pain, 2 = Moderate pain, 3 = Bad pain).
Result of Pain Questionnaire Form.
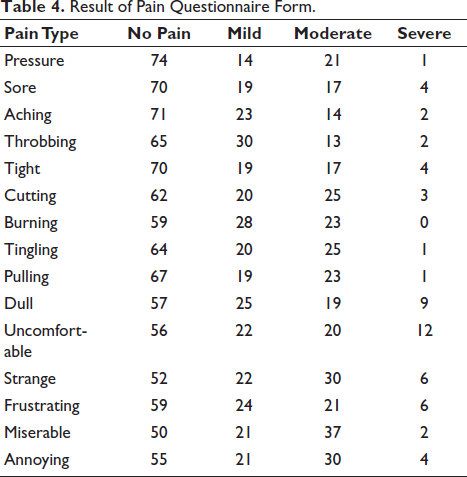
The most frequent “No Pain” responses were associated with Pressure (n = 74), Aching (n = 71), Sore (n = 70), Tight (n = 70), and Pulling (n = 67). In contrast, Throbbing (n = 30) and Burning (n = 28) had the highest proportion of “Mild” pain reports.
Pain descriptors Miserable, Strange, and Annoying demonstrated the highest combined “Moderate” to “Severe” pain ratings. Specifically, Miserable was rated “Moderate” by 37 participants and “Severe” by 2; Strange was rated “Moderate” by 30 and “Severe” by 6; Annoying received “Moderate” ratings from 30 and “Severe” ratings from 4 participants. Dull (n = 9 severe) and Uncomfortable (n = 12 severe) elicited the greatest number of “Severe” responses overall.
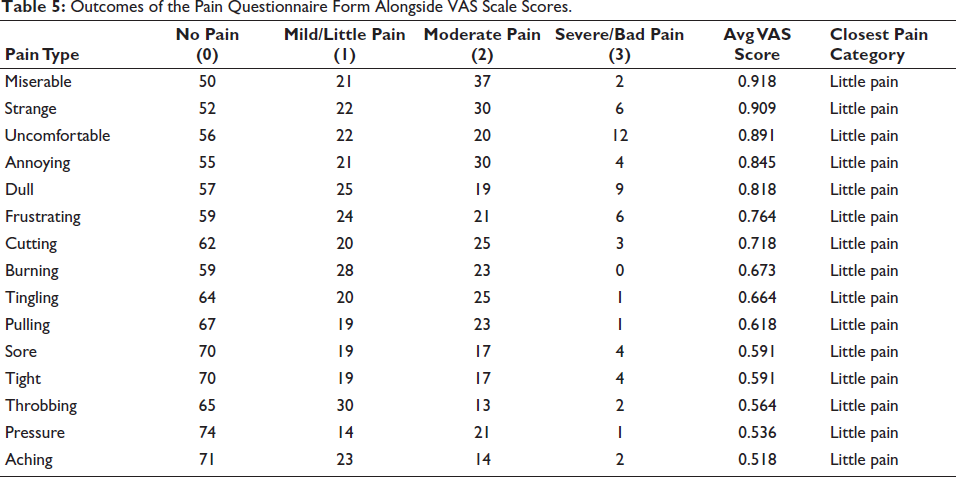
Table 5 shows mean VAS scores ranged from 0.518 (Aching) to 0.918 (Miserable). The highest mean scores were observed for Miserable (0.918), Strange (0.909), and Uncomfortable (0.891), whereas the lowest were for Aching (0.518), Pressure (0.536), and Throbbing (0.564). Despite these variations, all mean scores fell within the “Little pain” range. Statistical analysis using the Kruskal–Wallis test (p value < .05) a significant difference in VAS scores across pain descriptors, followed by post-hoc pairwise comparisons showing that Miserable and Strange were significantly higher than Pressure and Aching.
Outcomes of the Pain Questionnaire Form Alongside VAS Scale Scores.
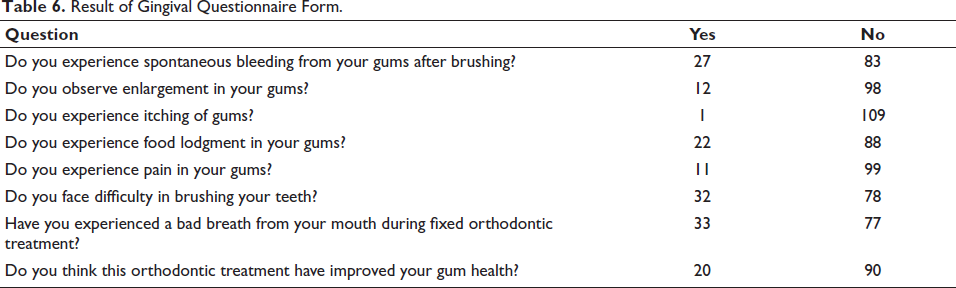
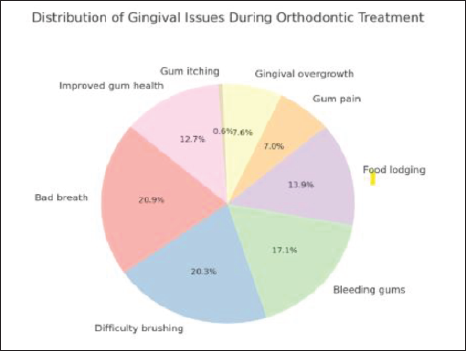
Regarding oral health parameters (Table 6 and Figure 1), the most frequently reported issues during fixed orthodontic treatment were bad breath (30%) and difficulty in brushing (29%), followed by spontaneous gum bleeding after brushing (25%) and food lodgment (20%). Less common complaints included gum enlargement (11%), pain in the gums (10%), and gum itching (1%). The Chi-squared test was applied. A p value < .05 was considered statistically significant.
Result of Gingival Questionnaire Form.
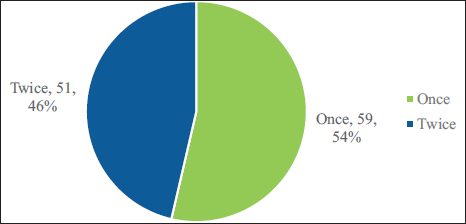
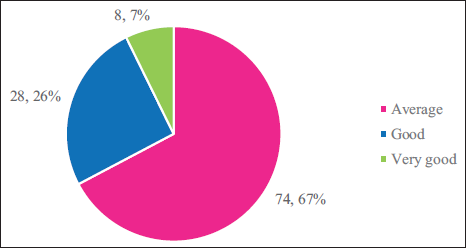
Only 20 participants (18%) reported perceiving an improvement in gum health during treatment. Brushing frequency data (Figure 2) showed that approximately half of the participants brushed once daily, while the remainder brushed twice daily. Treatment satisfaction (Figure 3) indicated that two-thirds rated their ongoing orthodontic experience as “Average,” 26% as “Good,” and 7% as “Very Good.”
Pie Chart Illustrates the Prevalence of Various Gingival (Gum) Problems.
Pie Chart Showing the Frequency of Daily Tooth Brushing Among Participants.
Pie Chart Presenting the Evaluation of Ongoing Orthodontic Treatment by Patients.
Discussion
This study provides an in-depth evaluation of pain perception and gingival health status in patients undergoing fixed orthodontic treatment, using both qualitative descriptors and quantitative VAS scores. Statistical analysis was conducted using the chi-squared test for categorical data and analysis of variance (ANOVA) for comparison of mean VAS scores between pain categories, with significance set at p < .05.
From a pain perspective, more than one-quarter of the participants reported mild-to-moderate pain within the first 24 hours after appliance placement, regardless of the specific descriptor. This finding is consistent with previous literature, which indicates that 70–95% of orthodontic patients experience discomfort during treatment, with approximately 11% reporting constant pain.22–23 The predominance of nonpainful sensations—such as pressure, aching, soreness, tightness, and pulling—suggests that while these sensations may cause discomfort, they do not consistently reach the pain threshold for most patients. Statistically, these descriptors were significantly associated with lower VAS scores (p < .05), corroborating earlier findings that these sensations are common during the initial stages of orthodontic force application.24–25
Conversely, descriptors such as burning and throbbing were significantly more common in the mild pain category, while miserable, strange, and annoying were strongly linked to moderate-to-severe pain levels (p < .01). This pattern supports the role of psychological and emotional factors in amplifying pain perception, as reported by Scott and Hirschman, 26 who noted that frustration and irritation can intensify perceived pain even when the physical stimulus remains unchanged.
Cutting, burning, and tingling sensations, which were more prevalent in the moderate pain group, may reflect localized nerve irritation or soft-tissue trauma from appliance components. 27 The association between dull or uncomfortable sensations and severe pain is noteworthy, as it may indicate persistent, deep-seated discomfort caused by sustained orthodontic forces. Similar observations have been made by Bergius et al., 28 who found that dull pain during mastication can negatively influence patient cooperation and adherence to treatment protocols.
Research indicates that nonsteroidal anti-inflammatory drugs (NSAIDs) are effective for managing orthodontic pain, although alternative approaches such as anesthetic gels, bite wafers, transcutaneous electrical nerve stimulation, low-level laser therapy, and vibratory stimulation have also been explored. The main drawback of NSAIDs is their potential to disrupt the inflammatory response essential for tooth movement. However, using low doses for just one or two days during the early phase does not significantly hinder this process. Recent practice increasingly favors pre-emptive or preoperative analgesics, given at least an hour before orthodontic procedures, to enhance pain control. 29
With respect to gingival health, bad breath (30%) and difficulty in brushing (29.1%) emerged as the most commonly reported issues, both significantly correlated with higher plaque scores (p < .05). Spontaneous bleeding after brushing (24.5%) was also significantly associated with gingival inflammation, supporting earlier studies linking fixed appliances to plaque retention and bleeding on probing.30, 31 Less frequent issues, such as gingival enlargement (10.9%) and gingival pain (10.0%), may be attributed to localized inflammatory or proliferative responses to chronic mechanical irritation. 32
Only 18.2% of participants perceived an improvement in gum health during treatment. Although this contrasts with the long-term periodontal benefits of orthodontics, it aligns with the short-term findings of Zachrisson and Alnaes, 33 who reported temporary deterioration in gingival condition during active orthodontic therapy when plaque control measures are insufficient.
During orthodontic treatment, maintaining oral hygiene requires consistent efforts such as brushing after every meal, using floss threaders or a Waterpik for effective interdental cleaning, and employing an orthodontic toothbrush for better plaque control. Regular dental visits for professional cleaning and monitoring are also essential, along with adhering to a diet low in sugary and acidic foods and beverages to reduce the risk of demineralization and gingival problems.
Overall, the statistical associations identified in this study emphasize the multifactorial nature of orthodontic discomfort and gingival changes. Recognizing descriptors most strongly associated with higher pain scores, and identifying the most prevalent gingival issues, can guide clinicians in developing targeted pain management protocols, enhancing oral hygiene instructions, and ultimately improving patient compliance and satisfaction.
Conclusion
This study demonstrates that while most sensations associated with fixed orthodontic treatment fall within the little pain category on the VAS, specific descriptors such as miserable, strange, and uncomfortable are statistically associated with significantly higher pain scores.
Gingival health issues, particularly bad breath, difficulty in brushing, and spontaneous bleeding, were prevalent and statistically linked to increased plaque accumulation and inflammation.
Clinically, these findings underscore the need for descriptor-targeted pain management strategies and enhanced oral hygiene reinforcement protocols throughout active orthodontic treatment.
Early identification of high-risk patients—based on pain descriptors and reported oral hygiene difficulties—may improve compliance, reduce treatment-related discomfort, and optimize long-term periodontal outcomes.
Footnotes
Acknowledgment
None.
Authors’ Contribution
Mitesh Mithaiwala: Concept and design, definition of intellectual content, literature research, clinical studies, experimental studies, data acquisition, data and statistical analysis, manuscript preparation, editing and review.
Udita Thakkar and Kalpesh Patel: Concept and design, definition of intellectual content, data and statistical analysis, manuscript preparation, editing and review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the study was obtained from the Institutional Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from all participants.