
Abstract
Aim
To assess the knowledge, attitude, and practice regarding the management of gum diseases among traditional medicine professionals in Tamil Nadu.
Materials and Methods
A descriptive cross-sectional study was conducted among 382 undergraduate students (house surgeons—CRI/CRRI), faculty members, and practitioners at traditional medicine colleges in Tamil Nadu. A pre-validated and pre-tested structured questionnaire was used for collecting the data. Data was analyzed using SPSS software version 27.0. Results were expressed as frequency and percentage.
Results
Out of 382 participants, 46.1% were Ayurvedic, 26.3% were Siddha, and 27.6% were Homeopathic professionals. A total of 58.1% reported the inclusion of gum diseases in their curriculum. A total of 78.9% were aware of the multi-factorial causes of tooth pain. A substantial proportion of study participants correctly identified contributing key factors for bleeding gums (86.6%), gingival recession (85.5%), mobile tooth, bad breath (73.7%), and risks of tobacco usage on gums (53%). In terms of attitude, 73.7% acknowledged alternative medicine as a viable option for gum diseases, 52.6% were aware of the availability of other treatment options for mobile teeth, and 60.5% reported the presence of an inter-relationship between systemic and gum diseases. Owing to practice, 38.2% agreed that they treat emergency dental problems mainly with medicines (64.5%), powders (15.8%), and paste (6.6%). Moreover, 64.5% prescribe medicinal mouthwash for bad breath. However, only 47.4% perform oral examination before treating gum diseases.
Conclusion
Results imply that a substantial proportion of traditional medicine professionals possess adequate knowledge, demonstrate a positive attitude, and exhibit medicinal practices toward gum disease management. However, there is a need for regular interdisciplinary awareness programs to enhance collaboration and further improve comprehensive patient care across disciplines.
Introduction
Periodontal disease stands to be the most common oral health concern next to dental caries. 1 The term “periodontal disease” encompasses a wide range of inflammatory conditions that affect the supporting tissues of the teeth, including the gingiva, periodontal ligament, cementum, and alveolar bone.2, 3 Periodontal diseases often lead to tooth loss and contribute to systemic inflammation, resulting in poor quality of life. 3
Nearly half of the Indian adults suffer from some form of periodontal disease, with overall prevalence accounting for about 51%. 4 Despite its high prevalence, the percentage of patients seeking treatment and preventive measures remains low. This could be attributed to a lack of awareness about the cause and consequences of periodontal diseases among the general population, which remains the major barrier.
In developing nations such as India, many patients actively seek advice from non-dental health professionals, such as general physicians and Ayurveda, Naturopathy and Yoga, Unani, Siddha, and Homeopathy (AYUSH) personnel for their oral health problems. 5 Well-informed healthcare professionals can play a crucial role in guiding and referring patients with oral health care needs to dental professionals, as this can be a stepping stone in reducing the overall oral health burden.
The traditional medicine system has its origin in India, which is deeply rooted in Indian culture. Recently, many people have started seeking an indigenous system of medicine as a holistic approach to treating their diseases.
Ayurveda (“science of life”) is an ancient and traditional system of medicine that dates back approximately 5,000 years. In Ayurveda, dentistry has been covered under the section Shalya-Chikitsa (surgical treatments), where dental health is referred to as “danta swasthya.” To address oral health problems, Ayurveda strongly advocates daily therapeutic practices such as dant dhavani (brushing), jivha lekhana (tongue scraping), and gandoosha (gargling or oil pulling) to maintain oral health.6, 7
Siddha, a traditional Indian medical system that emerged 2,000 years ago in Tamil Nadu, utilizes 108 herbs known as “karpa mooligaigal” for treating various diseases, including oral conditions. Siddha system of medicine utilizes medicinal herbal plants for managing dental ailments, as most of them possess anti-plaque, anti-cariogenic, antibacterial, anti-inflammatory, analgesic, antitumor, anti-stress, anti-fungal, and rapid healing properties.6, 8
Homeopathy originated from the Greek words “homoios,” meaning “similar,” and “pathos,” meaning suffering or sickness. The basic principles were introduced by Paracelsus and Hippocrates, which were later codified into a medical science in 1789 by Dr. Samuel Hahnemann, a German physician. From the literature, it is evident that homeopathic medicines were used for managing various dental conditions such as mouth ulcers, toothache, TMJ disorders, neuralgia, hemorrhage, gingivitis, periodontitis, and others. 9
From the literature, it could be understood that traditional medicine practitioners play a significant role in enhancing public understanding of dental health. But there remains a literature gap in understanding the knowledge, attitude, and practices (KAP) among traditional medicine professionals regarding the management of gum diseases.
Thereby, the present cross-sectional study was conducted to explore the KAP of traditional medicine professionals in Tamil Nadu regarding gum disease management. By assessing their awareness, attitudes toward conventional treatments, and actual practices in managing gum diseases, this research seeks to provide insights into the role of traditional medicine professionals in oral health care. Understanding their perspectives and practices can inform strategies for integrating traditional and modern approaches to improve oral health outcomes in the region.
Materials and Methods
A descriptive, cross-sectional study was conducted among undergraduate students (house surgeons—CRI/CRRI), faculty members, and practitioners at traditional medicine colleges in Tamil Nadu.
Study Population
The study population comprised house surgeons (CRI/CRRI), faculty members, and practitioners at various traditional medicine colleges in Tamil Nadu.
Sample Size
Sample size was calculated using the formula N = z2pq/d2
At 5% significance level, 60% expected proportion, and 5% margin of error, the required sample size was calculated to be 369. Anticipating 5% non-response rate, the final sample size was adjusted to 388.
Study Area
The research was carried out in Tamil Nadu, a state with a significant population of practitioners of traditional medicine.
Sampling Method
A convenience sample technique was used to select the study participants.
Eligibility Criteria
Inclusion Criteria
Undergraduate CRI/CRRI students (house surgeons), faculty members, and practitioners at various traditional medicine colleges in Tamil Nadu were included in the study.
Exclusion Criteria
Students who did not complete their degree were excluded.
Participants who satisfied the eligibility criteria were included in the study. The purpose of the study was clearly explained to the participants, and written informed consent was obtained from them. KAP of traditional medicine practitioners regarding gum disease management was collected using a pre-validated and pre-tested structured questionnaire.
The questionnaire was structured into four sections. Section I included four questions designed to collect data on demographic details, educational qualifications, the inclusion of gum/periodontal disease topics in their curriculum, and sources and updates of knowledge regarding gum/periodontal disease. Section II consisted of eight questions aimed at evaluating the knowledge of students, faculty, and practitioners on the management of gum/periodontal diseases. Section III included five questions that focused on assessing attitudes toward the management of gum/periodontal diseases. Section IV comprised six questions that gathered information on the practices of the study participants toward the management of gum/periodontal diseases.
Data was collected by a single investigator. The questionnaire was distributed to study participants and collected on the same day. On average, it took participants 5–10 minutes to complete the questionnaire. Only those forms with complete responses were included for data analysis, while incomplete forms were rejected.
Statistical Analysis
Data was entered in Microsoft Excel, and statistical analysis was carried out in SPSS software version 27.0. Significance level of p < .05 is considered statistically significant. The result was expressed in frequency and percentage.
Results
The study participants comprised 46.1% Ayurvedic professionals, 26.3% Siddha professionals, and 27.6% Homeopathic professionals. Among them, 58.1% confirmed that gum diseases were included in their curriculum. A significant portion, 69.7%, attained their knowledge on gum diseases through their academic curriculum, while 26.3% gained knowledge from journals. Additionally, 57.9% of participants regularly update their knowledge on gum diseases.
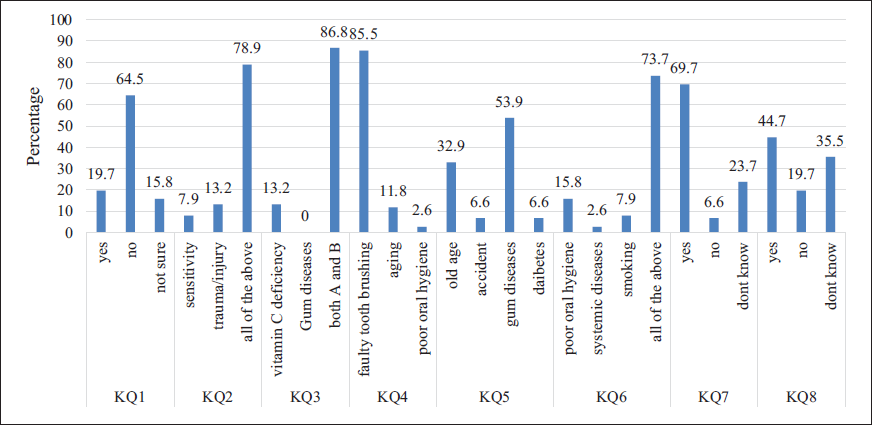
Results from Figure 1 indicated that the majority of respondents (64.5%) disagreed with the statement that tooth pain occurs only due to tooth decay, while 78.9% identified sensitivity, trauma/injury, and other factors as common causes of tooth pain. For bleeding gums, 86.8% of respondents recognized both vitamin C deficiency and gum disease as contributing factors. A significant proportion (85.5%) attributed receding gums primarily to faulty tooth brushing, and 53.9% identified gum diseases as the main cause of tooth loosening, with old age being a secondary factor (32.9%). In terms of bad breath, 73.7% agreed that poor oral hygiene, systemic diseases, and smoking were all contributing factors. Furthermore, 69.7% of respondents acknowledged that tobacco use increases the risk of developing gum disease. Forty-four point seven percent of participants reported being aware of a separate specialty in dentistry dedicated to treating gum diseases.
With respect to attitude questions, results from Figure 2 showed that the majority of respondents (53.9%) disagreed that only allopathic medicine can treat gum diseases, with 73.7% acknowledging alternative medicine as a viable option. When considering the treatment of mobile teeth, 52.6% did not believe that tooth removal was the only method, indicating the availability of other treatments. Additionally, 60.5% of respondents reported the existence of an inter-relationship between gum diseases and systemic diseases, highlighting the importance of holistic health awareness. Opinions were more divided on whether treating gum diseases alone would significantly improve oral health quality; 39.5% disagreed, while 36.8% agreed, and 23.7% were unsure.

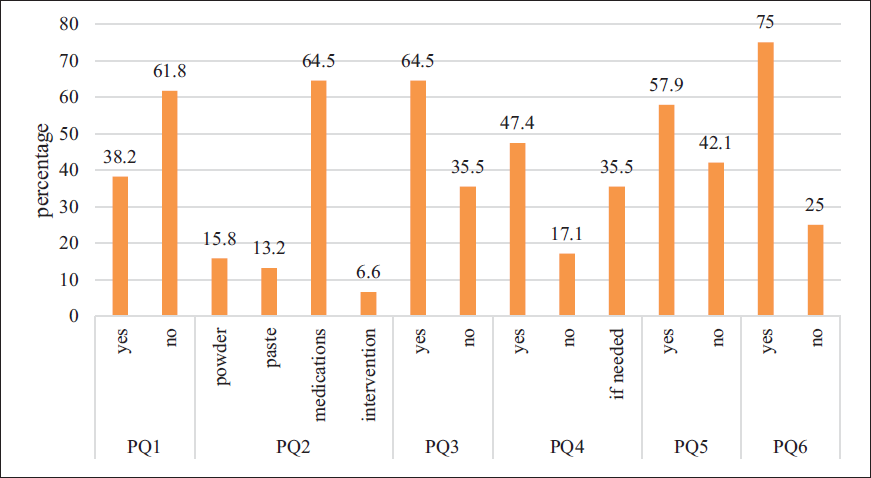
The study results (Figure 3) indicate that 38.2% of participants treat emergency dental problems to alleviate pain, with 64.5% using medications, 15.8% using powders, 13.2% using pastes, and 6.6% employing interventions. Additionally, 64.5% recommend medicinal mouthwash for bad breath, while 35.5% do not. Regarding oral examinations before gum treatment, 47.4% always perform them, 17.1% do not, and 35.5% do so only if needed. Furthermore, 57.9% advise using medicinal powder with toothpaste, and 75% refer patients with gum disease to a general dentist.
Discussion
Oral health is an integral part of general health, which directly affects the quality of life of an individual. Many members of the Indian population seek oral health advice from non-dental health personnel such as Ayurvedic, Siddha, and Homeopathic professionals as part of a holistic approach. Timely referral and positive attitude toward management of periodontal disease may aid in saving teeth from tooth loss, infection, and inflammatory conditions. Therefore, non-dental healthcare providers need to be aware of periodontal disease, including its cause, severity, and consequences. This can greatly aid in increasing awareness among the general public regarding their gum/periodontal health conditions and make timely referral to a dentist by non-dental health professionals. Thereby, the present study was carried out to assess the knowledge, attitude, and practice of traditional medicine health professionals in the management of gum diseases.
In the present study, 58.1% of dental students stated that gum diseases were included in their curriculum. In support of this, Ayurveda has included inflammatory conditions of the gums in the Paridara (gangrenous gums) and Upakusha (swollen, burning gums)section.10, 11 According to Khagen Basumatary, the Siddha system has included gum diseases under the terms dhantha piraloonam (boils in gums, swollen gums), dhantha sarkkaram (dental plaque), and dhantha moolarogam (palladi noigal affecting gums and tooth roots).8, 12 Similarly, in homeopathy, numerous herbal formulations were present and prescribed for gingivitis, periodontitis, and alveolitis. 13 This indicates that all the above three indigenous systems of medicine have included gum/periodontal disease in their curriculum.
Around 62.7% and 26.3% of participants acknowledged academic books and journals as their primary source of knowledge about oral health and gum diseases. Similar results were found in the study done by Rajmohan et al. where 50% gained their oral health knowledge through academic books, while 23.5% from journals. 14
Findings of the present study indicate that a substantial proportion (64.5%) of study participants do not agree with the statement that tooth pain is caused only by dental caries. This indicates that they were aware (78.9%) of other contributing factors for tooth loss, such as trauma/injury, sensitivity.
Results showed that 86.8% of participants reported that both vitamin C and gum diseases as the common causes for bleeding gums. This indicates that participants have better knowledge of the impact of vitamin C deficiency on gum diseases. This is consistent with a study done by Carr and Frei. 15
A significant proportion (85.5%) of participants attributed receding gums primarily to faulty tooth brushing, demonstrating better understanding and awareness of the impact of improper brushing techniques on gum health. These results were inconsistent with the study done by Raghavendra et al. 5 where only 25.1% of Ayurvedic and 22.7% of Homeopathy students correctly identified faulty brushing as the primary cause of receding gums. This discrepancy might be due to the single-centric design of the latter study, which limits its generalizability.
Moreover, 53.9% identified gum diseases as the major cause of tooth loosening, followed by old age (32.6%), accident, and diabetes (6%). This indicates their better understanding of the multifactorial cause of periodontal diseases leading to mobile teeth.
With respect to bad breath, 73.7% agreed that poor oral hygiene, systemic diseases, and smoking were all contributing factors. These results were consistent with the study done by Raghavendra et al. 5 Furthermore, 53% of respondents acknowledged the increased risk of gum diseases associated with tobacco use. This is supported by substantial evidence linking tobacco use to periodontal disease progression. 16
About 73.7% of participants acknowledged alternative medicine as the choice of treatment for gum diseases, indicating their common practice of prescribing Ayurvedic, Siddha, or Homeopathic medicines for managing gum diseases. Substantial evidence supporting their prescription of herbal medicines for gum/periodontal diseases was found in the literature.6–9, 11, 12
For mobile tooth management, a significant proportion (47.4%) of participants believed extraction was the only available option for managing mobile teeth, indicating their lack of awareness toward other management options. Similar findings were reported in the study done by Aniyan et al. 17 where 75.56% displayed a lack of awareness toward mobile tooth management options.
Around 60.5% of respondents acknowledged the presence of an inter-relationship between gum diseases and systemic diseases, indicating their awareness of the systemic effects of gum diseases. Similar findings were reported in the studies done by Aniyan et al. 17 and Raghavendra et al. 5
From the results, it is evident that 38.2% of Ayurvedic, Siddha, or Homeopathic professionals treat emergency dental problems primarily with medications (64.5%), powders (15.8%), pastes (13.2%), and various interventions (6.6%). This indicates their common and preferred way of medicinal treatment (herbs) over procedural interventions for alleviating emergency dental problems. Medicinal interventions for oral health problems were well documented in the literature.6–9, 11, 12
It was found from the present study that a significant proportion (52.6%) of Ayurvedic, Siddha, or Homeopathic professionals do not examine (17.1%) the oral cavity before gum treatment, and 35.5% do so only if needed. This could negatively impact the prompt diagnosis of gum/periodontal diseases, which inherently affects the proper treatment plan. Similar results were found in the study done by Aniyan et al. 17 where 46.66% did not perform oral examinations in systemic conditions.
Further, 75% of participants refer patients with gum disease to a general dentist. This indicates their informed referral, recognizing the need for specialized care for gum diseases from dental professionals. Consistent findings were found in the study done by Aniyan et al. 17 where 100% participants referred patients with complex oral health problems to a dentist. This forms a collaborative inter-disciplinary approach for effectively managing patients with complex oral health problems.
The multi-centric nature of the present study is the major strength. Further studies with other non-dental health professionals, such as general physicians, practitioners of Unani, naturopathy, and yoga, are recommended. This approach would provide a broader perspective on oral health management and contribute to comprehensive healthcare strategies across different disciplines.
Conclusion
Results from the present study imply that a substantial proportion of Ayurvedic, Siddha, and Homeopathic professionals possess adequate knowledge, demonstrate a positive attitude, and exhibit medicinal practices toward gum disease management. However, there is a need for regular interdisciplinary awareness programs to enhance collaboration and further improve comprehensive patient care across disciplines.
Footnotes
Authors’ Contribution
Pooja T, Abirami Thanigaimalai, Bhuvaneswari B : Concept, data collection, data analysis, manuscript preparation and validation.
Juala Catherine, Parthasarathy T, Vineet V: Supervision, manuscript review, validation and data analysis.
Sri Sanjhanaa C, Ramya V: Data collection, data analysis and manuscript review.
Data Availability
Data will be available upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical committee approval was obtained from the Institutional Review Board (IRB) before starting the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent is obtained from all the participants priorly.