
Abstract
Background
Cardiovascular disease (CVD) is a leading cause of disability and death worldwide, particularly in lower-middle income countries like India. This study investigates Fordyce granules (FGs) as a potential marker for hyperlipidemia, alongside diagonal earlobe creases (DELC) and corneal arcus as indicators of coronary artery disease, aiming to enhance cardiovascular risk assessment in the Indian population.
Objective
To evaluate the association between cardiovascular conditions and maxillofacial markers, including corneal arcus, DELC, and FGs.
Materials and Methods
This cross-sectional study involved 60 participants: 30 CVD patients (Group I) and 30 non-CVD patients (Group II). The presence of DELC, FGs, and corneal arcus was recorded for each group.
Results
In Group I (CVD patients), prevalences were 40% for DELC, 66% for corneal arcus, and 6% for FGs. In Group II (non-CVD patients), prevalences were 3% for DELC, 10% for corneal arcus, and 30% for FGs, with significant differences between the groups. A significant association was found between DELC and corneal arcus (p < .01) and FGs (p = .02), emphasizing their link to cutaneous oral signs in CVD patients.
Conclusion
DELC, FGs, and corneal arcus may serve as valuable markers for early CVD detection in dental patients.
Keywords
Introduction
Coronary heart disease (CHD) is the leading cause of mortality worldwide, with prevention remaining a significant public health priority. 1 Over 75% of these deaths occur in emerging nations, while mortality rates in advanced countries are decreasing rapidly. Chronic heart disease, including CHD, accounts for 30% of global deaths. In India, the prevalence of chronic heart disease ranges from 7% to 13% in urban areas, with a much higher rate of up to 27% in rural regions.2, 3 Numerous case-control studies have identified key risk factors for chronic heart disease in India, including smoking, diabetes, hypertension, obesity, stress, and insufficient physical activity. 4
The earlobe crease, first formally observed by Frank in 1973, is a wrinkle or furrow in the skin that extends at a 45-degree angle from the tragus to the posterior edge of the earlobe. This crease is also referred to as the deep diagonal earlobe crease (DELC). 5 An autopsy-based study has suggested that the progression of atherosclerosis may be linked to changes in collagen metabolism occurring in the skin. 6 The DELC has been proposed as a visible marker for coronary heart disease, being easily observable. However, several studies have reported conflicting findings, suggesting that it may merely be an indicator of aging rather than a definitive sign of CHD.7, 8
Corneal arcus, a lipid-rich extracellular deposit located at the corneoscleral limbus, is the most common form of peripheral corneal opacity. This condition results from lipid accumulation rather than tissue degradation. First proposed as a cardiac risk factor by Virchow in 1852, 9 corneal arcus has since been associated with hypercholesterolemia, xanthelasmas, alcohol consumption, high blood pressure, smoking, diabetes, and coronary heart disease. 10 The presence of corneal arcus has been proposed as a visible marker for cardiovascular risk, as it can be easily observed. However, its significance as a definitive indicator of coronary heart disease is still debated, with some studies suggesting it may be more indicative of aging rather than a clear sign of heart disease.
Sebaceous glands, typically found as adnexal structures in the skin, can also be present in the mouth, where they are referred to as Fordyce granules (FGs) or ectopic sebaceous glands. 11 First described by Fordyce in 1896, 12 the chemical composition of FGs is similar to that of sebaceous glands in the skin, with approximately 50% of the sebum consisting of triglycerides.13, 14 The prevalence of FGs increases with age, with 60%–80% of cases observed in older individuals.15, 16 While FGs are generally benign and asymptomatic, their presence is often associated with the natural aging process and may not necessarily indicate any underlying pathology.
This study aims to examine the association between DELC, corneal arcus, FGs, and cardiovascular disease (CVD).
Methodology
An institute-based cross-sectional study is conducted to explore the relationship between cardiovascular conditions and various maxillofacial markers, including DELC, corneal arcus, and FGs.
Ethical Approval
The study received ethical approval from the institution (Ref. No. PMNMDCH/955/2024-25) and was carried out between August 2024 and September 2024 in the Oral Medicine and Radiology Outpatient Department. The study included two groups: Group I consisted of 30 patients diagnosed with CVD, and Group II consisted of 30 patients without CVD.
Subject Details and Recruitment
Before participation, the study’s purpose and procedures were fully explained to each participant, and informed consent was obtained. A complete case history was recorded for all participants, along with photographic documentation. The presence or absence of DELC, corneal arcus, and FGs was assessed for both groups. Participants were then evaluated to ensure they met the study’s inclusion criteria. Individuals who were unwilling to participate were excluded. The research proposal and synopsis were discussed and approved by the ethical committee. All study participants were between 30 and 85 years of age.
Sample Size Estimation
Sample size estimation was performed using OpenEpi software version 2.3.1, with a 95% confidence level (α = 0.05, two-tailed) and 80% power (β = 0.20). Based on this, it was determined that 30 participants should be included in each group, resulting in a total of 60 participants. The sample size was calculated using the following formula: n = (Zα/2 + Zβ)² × (p1(1 − p1) + p2(1 − p2))/(p1 − p2)², where Zα = 1.960 is the standard normal deviate for α (two-tailed) at a 95% confidence level, and Zβ = 0.84 is the standard normal deviate for β at 80% power.
Inclusion Criteria
Adults must be aged 30 years and above (both men and women).
Participants must meet the following criteria for the presence of specific clinical signs:
Exclusion Criteria
Participants with incomplete demographic data.
Patients with an ambiguous or incomplete deep diagonal earlobe crease (DELC).
Individuals with distorted ear anatomy, ear piercings, or incomplete earlobe creases.
Patients diagnosed with diabetes mellitus, thyroid disorders, or those who are taking hypoglycemic medications.
Note: These conditions were excluded due to their potential confounding effects on lipid metabolism, which is a key focus of this study. Since diabetes, thyroid disorders, and hypoglycemic medications are known to significantly impact lipid metabolism, their inclusion could interfere with analyzing the association between lipid metabolism, DELC, and FGs in relation to CVD.
Participants lacking cardiovascular system assessment.
Statistical Analysis
Data were entered and sorted using the Statistical Package for the Social Sciences (SPSS) version 21 for Windows (SPSS Inc., Chicago). The chi-square test was used to assess the association between the presence of clinical features (DELC, corneal arcus, and FGs) and CVD status in both groups. Prevalence of these clinical features was calculated for each group. A p value of less than .05 was considered statistically significant.
Result
Table 1 presents the distribution of oral and cutaneous signs in both groups. In the CVD group, 12 patients had a positive Frank sign and 18 had a negative Frank sign. For corneal arcus, 20 patients had a positive sign and 10 had a negative sign. Regarding FGs, 2 patients had a positive sign and 28 had a negative sign. In the non-CVD group, 1 patient had a positive Frank sign and 29 had a negative Frank sign. For corneal arcus, 3 patients had a positive sign and 29 had a negative sign. Finally, 21 patients had a positive FG sign and 9 had a negative sign.
Chi-square Test for Association of Oral Cutaneous Sign in Two Groups.
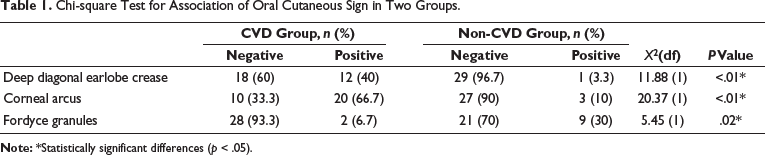
The percentage distribution of these signs in both groups is as follows: In the CVD group, 40% of patients had a positive Frank sign, while 60% had a negative Frank sign. For corneal arcus, 66.7% of patients exhibited a positive sign and 33.3% exhibited a negative sign. Regarding FGs, 6.7% of patients had a positive sign and 93.3% had a negative sign. In the non-CVD group, 3.3% of patients had a positive Frank sign and 96.7% had a negative Frank sign. For corneal arcus, 10% of patients had a positive sign and 90% had a negative sign. Lastly, 30% of patients showed a positive sign for FGs, while 70% had a negative sign.
The chi-square test was used to assess the association between oral and cutaneous signs in the two groups. A significant relationship was found, with the p values for the Frank sign (p < .01), corneal arcus (p < .01), and FGs (p = .02) indicating a higher association of Frank sign and corneal arcus in the CVD group compared to the non-CVD group.
Discussion
This study aimed to evaluate the association between CVD and maxillofacial markers, including DELC, corneal arcus, and FGs. The main findings indicate a significant association between DELC and corneal arcus with CVD, while FGs showed a weaker, although still significant, association. The null hypothesis, which proposed no association between these maxillofacial markers and CVD, was rejected. These results suggest that DELC and corneal arcus could serve as potential indicators for CVD.
DELC has been recognized as a potential marker for CVD since 1973. 5 In this study, DELC was found in 40% of CVD patients compared to just 3.3% in individuals without CVD. This prevalence is lower than that reported in studies by Raman et al., who observed a 60% prevalence in an urban South Indian population, 17 and Ramdurg et al., who reported 63.21% in CHD patients compared to 26.79% in controls. 4 The lower prevalence in our study could be attributed to the smaller sample size. Additionally, Kuon et al. suggested that while DELC is associated with age and increased BMI, it does not directly predict CVD, 18 supporting the notion that DELC may serve more as a marker of cardiovascular disease rather than a definitive predictor (Supplementary Figure 1).
Corneal arcus, a lipid-rich deposit at the corneoscleral limbus, was first linked to atherosclerosis in 1852. 19 In our study, the prevalence of corneal arcus was significantly higher in CVD patients (66.7%) compared to non-CVD individuals (10%). This finding aligns with previous studies, such as those by Zech et al. and Rosenman et al., who also reported a strong association between corneal arcus and CVD.20, 21 However, Fernandez et al. found no significant association between corneal arcus and CVD after four and eight years of follow-up, 22 suggesting that the association may vary over time or in different populations (Supplementary Figure 2).
FGs, first described by Fordyce in 1896,12, 23–25 showed a weaker association with CVD in this study. FGs were found in 6.7% of CVD patients, whereas 30% of non-CVD individuals had them. This finding contrasts with that of Gaballah and Rahimi et al., who reported a significant association between FGs and hyperlipidemia, 26 but is consistent with that of Diajil et al., who found no significant correlation with triglyceride levels. 27 The discrepancy may be due to differences in sample characteristics or the relatively low prevalence of FGs in our cohort (Supplementary Figure 3).
An important factor to consider is the significant age difference between the CVD group (mean age = 65 years) and the non-CVD group (mean age = 41 years). Since DELC and corneal arcus are age-related changes, this age disparity could have confounded the observed associations. Future studies should account for this by using age-matched cohorts or adjusting for age in analyses, reducing potential confounding factors and providing more accurate insights.
While this study offers valuable evidence linking DELC and corneal arcus with CVD, there are limitations to acknowledge. The sample size was relatively small, and larger studies with more diverse populations are needed to strengthen these findings. Additionally, because this is a cross-sectional study, it cannot establish causal relationships between these markers and CVD. Longitudinal studies are necessary to confirm these associations over time and explore any potential causal links.
The clinical implications of these findings are noteworthy. DELC, corneal arcus, and FGs are easily detectable during routine clinical examinations and could serve as non-invasive indicators for assessing cardiovascular risk, particularly in dental practice. Identifying these markers during dental check-ups could help identify patients at higher risk for cardiovascular conditions, leading to earlier interventions and better preventative care. Incorporating these markers into routine screenings could enhance cardiovascular risk management in healthcare settings.
Additionally, it is important to note the role of sebum in aging, which is complex. After age 50, women experience a reduction in sebaceous gland activity 10–20 years earlier than men, which may contribute to gender differences in skin dryness, sensitivity, and infection susceptibility. However, there is no clear evidence supporting a significant sex-based difference in skin function. 28
The findings of this study suggest that DELC and corneal arcus may be useful non-invasive markers for cardiovascular risk, especially in clinical and dental settings. Future research should focus on larger, age-matched cohorts and longitudinal studies to further investigate the long-term predictive value of these markers. Additionally, exploring the relationship between FGs and other cardiovascular risk factors such as lipid levels, hypertension, and metabolic disorders could provide more clarity on their role in clinical practice. These findings may ultimately lead to improved early detection of cardiovascular risk, enabling timely interventions and better patient outcomes.
We acknowledge that the results of this study may not be widely applicable because of the small sample size, the homogeneous ethnic group, and the single-center design. As such, we recommend conducting further longitudinal studies with larger and more diverse cohorts across various institutions. Additionally, the study does not include details on the extent or severity of coronary disease.
Conclusion
This study provides preliminary evidence of a significant association between maxillofacial indicators, such as DELC, corneal arcus, and FGs, with CVD and its major coronary risk factors. The high prevalence of these indicators in CVD patients highlights their potential role in cardiovascular health assessments.
Footnotes
Acknowledgment
None.
Authors’ Contribution
The manuscript was written by the corresponding author. All authors reviewed and approved the final version.
Data Availability Statement
A dataset was generated and analyzed during the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval Institutional Statement
The study received ethical approval from the institution (Ref. No. PMNMDCH/955/2024-25)
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained from all patients for being included in the study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.