
Abstract
Objective
Resting heart rate (RHR) independently predicts cardiovascular death. Increased RHR is related to chronic diseases, but community-based studies are rare. We investigated this population and factors related to RHR.
Methods
In total, 374 participants underwent medical examinations from March 2019 to December 2019. Participants were divided into groups with low RHR (LRHR; <65 beats/minute) and high RHR (HRHR; ≥65 beats/minute). RHR was judged using resting electrocardiogram at physical examination. We conducted laboratory examinations, including glycosylated hemoglobin (HbA1c), fasting plasma glucose (FPG), and blood lipids, among participants with chronic diseases. We used Cox proportional risk regression and multivariate analyses for the following covariates: previous chronic diseases, body mass index (BMI), smoking, blood lipids, and FPG.
Results
The incidence of type 2 diabetes mellitus (T2DM) and HbA1c values were both significantly higher in the HRHR group than in the LRHR group. Spearman correlation analysis showed RHR had a positive correlation with low-density lipoprotein, BMI, FPG, and HbA1c (r = 0.104574, 0.117266, 0.116041, and 0.311761, respectively). Multiple linear regression analysis showed age, hypertension, T2DM, and HbA1c were factors influencing RHR.
Conclusion
RHR showed strong correlation with T2DM and HbA1c in our community population, suggesting that RHR may be a risk factor for cardiovascular disease.
Keywords
Introduction
Heart rate has evolved from a common clinical indicator to become a recognized marker of cardiovascular risk that is associated with poor prognosis. 1 Resting heart rate (RHR) is an easily assessable clinical variable that is potentially modifiable with lifestyle changes and pharmacotherapy. 2 There is a great deal of evidence in epidemiological and clinical studies among different subgroups, including the general population and patients with cardiovascular disease, which describes the adverse consequences associated with RHR.3,4 Epidemiological studies have also found that elevated RHR is an independent predictor of all-cause, non-cardiovascular, and cardiovascular deaths. 5 The effects of an increased RHR are equivalent to those of smoking, hypertension, and dyslipidemia and it is a risk factor for coronary heart disease (CHD). 6
The mechanisms underlying the harmful effects of an elevated RHR are unclear, but several plausible biological mechanisms have been proposed. Regarding pathways involved in the link between elevated RHR and mortality, it has been suggested that an increase in RHR indicates a potential autonomic imbalance and an increase in the RHR may reflect sympathetic hyperactivity. 7 Additionally, an elevated RHR is associated with increased metabolic activity and systemic inflammation and is part of the ultimate pathways of many systemic diseases involving inflammatory, metabolic, and neurological processes. 8 It has been found that elevated RHR is associated with cardiovascular risk factors, such as impaired glucose metabolism, type 2 diabetes mellitus (T2DM), obesity, hypertension, dyslipidemia, smoking, and physical activity levels.9–11
We conducted a community-based observational study using data from routine physical examinations among community residents of Guangzhou in Guangdong, China, and we analyzed those factors related to heart rate.
Methods
Participants
This study was observational; therefore, we did not set inclusion or exclusion criteria for the included participants. However, because the data were from a community-based population who underwent physical examination, no severely ill patients or those needing hospitalization were included. According to physical examination data, participants were divided into two groups by RHR: a group with low RHR (LRHR; <65 beats/minute) and a group with high RHR (HRHR; ≥65 beats/minute). Heart rate was determined using a resting electrocardiogram (ECG). The examination data included ECG, blood pressure measurement, glycosylated hemoglobin (Hb1Ac), fasting plasma glucose (FPG), blood lipids, and other characteristics.
The Research Ethics Committee Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences approved this study (no. GDREC2020174H), and all private participant information was kept confidential. All participants signed an informed consent form. The reporting of this study conforms to the STROBE guidelines. 12
Statistical methods
Statistical analyses were performed using R version 3.5.1 (The R Project for Statistical Computing, Vienna, Austria). Quantitative variables with a normal distribution are expressed as mean and standard deviation and were compared using the Student t-test for independent samples. Categorical variables were analyzed using the chi-square or Fisher’s exact test. The Mann–Whitney U test was used for variables with a non-normal distribution. P < 0.05 was considered statistically significant. We used the Pearson correlation analysis function in R to analyze the correlations between different factors and represented these using heat maps. We used Cox proportional risk regression analysis to estimate the relationship between RHR and various risk factors. Multivariate analysis was performed using the following covariates: previous chronic diseases, body mass index (BMI), smoking, blood lipids, and FPG.
Results
This study included 374 participants, 225 men and 149 women, aged 25 to 65 years, between March 2019 and December 2019.
Comparison of chronic diseases and laboratory examinations according to heart rate
The results of data analysis showed that participants’ RHR ranged from 52 to 90 beats/minute, with a 95% confidence interval of 57 to 80 beats/minute. There were 150 participants in the HRHR group, with a mean heart rate of 72.8 beats/minute, and 224 participants in the LRHR group, with a mean heart rate of 62.2 beats/minute. We observed a significantly higher incidence of T2DM and a significantly higher HbA1c value in the HRHR group than in the LRHR group (both P < 0.05). However, there were no significant differences between the groups with respect to age, smoking, hypertension, CHD, total cholesterol (CHOL), triglycerides (TG), low-density lipoprotein (LDL), high-density lipoprotein (HDL), BMI, and FPG. Detailed results are shown in Table 1. To obtain a clearer result for individual patients, we visualized the data using a heat map. This also showed that patients in the HRHR group had a significantly higher incidence of T2DM and HbA1c values than those in the LRHR group. The results are shown in Figure 1.
Baseline characteristics by quintiles of resting heart rate.

HRHR, high resting heart rate; LRHR, low resting heart rate; CHD, coronary heart disease; CHOL, total cholesterol; TG, triglycerides; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BMI, body mass index; FPG, fasting plasma glucose; HbA1c, glycosylated hemoglobin.

Heat map of laboratory examinations and chronic diseases among participants. All original data were standardized before creating the heat map.
Correlation analysis of heart rate-related factors
Spearman correlation analysis showed a positive correlation of LDL, BMI, FPG, HbA1c with RHR (r = 0.104574, 0.117266, 0.116041, and 0.311761, respectively; P < 0.05).There was no significant difference in the correlations between TG, HDL, and RHR. The results are shown in Figure 2.

Spearman correlation analysis of heart rate and related factors **P < 0.01; *P < 0.05.
Multiple linear regression analysis of RHR
Multiple linear regression analysis of RHR showed that age, hypertension, T2DM, and HbA1c were influencing factors for RHR (P < 0.05). The factors related to RHR are shown in Table 2.
Multiple linear regression analysis of factors related to resting heart rate.
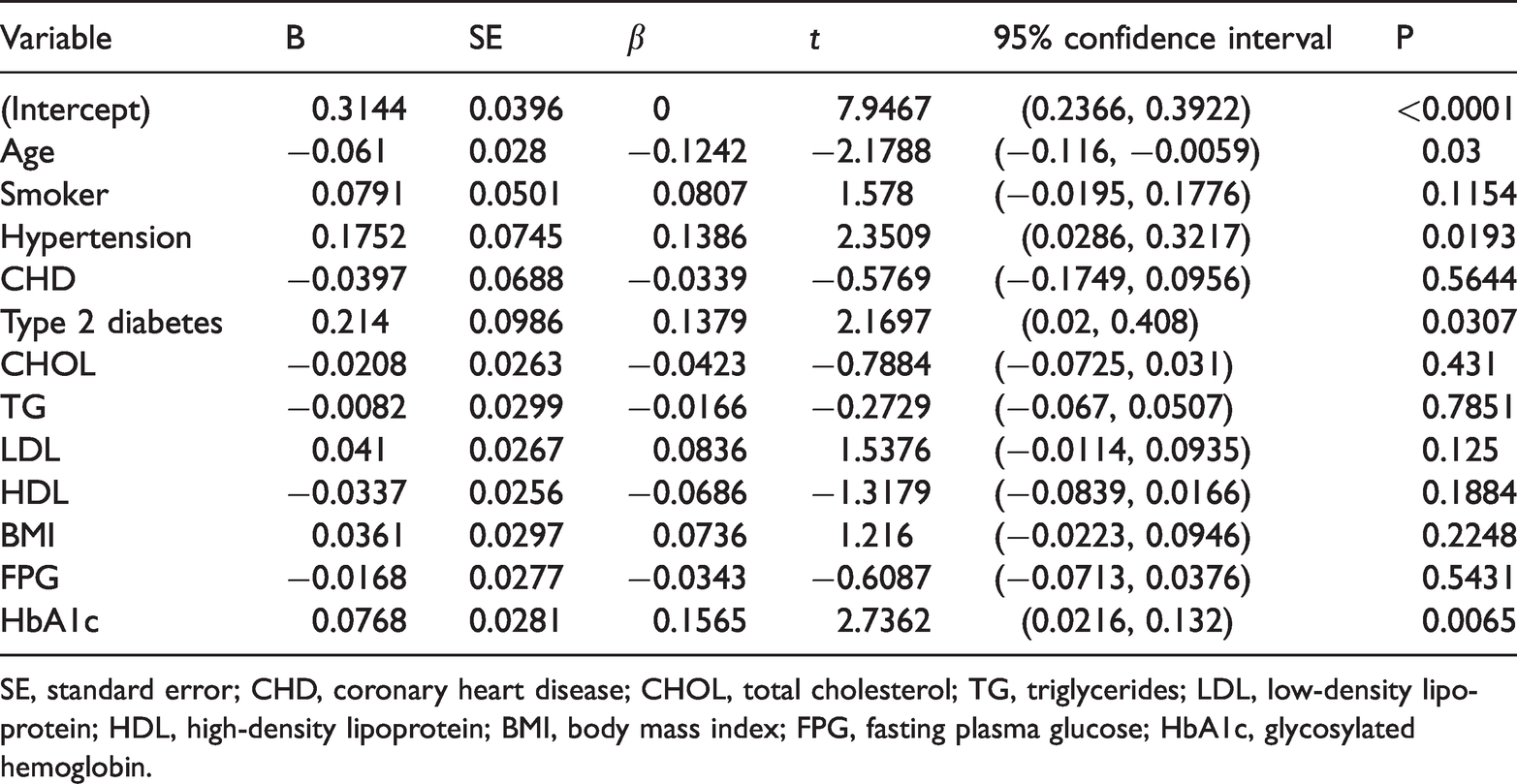
SE, standard error; CHD, coronary heart disease; CHOL, total cholesterol; TG, triglycerides; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BMI, body mass index; FPG, fasting plasma glucose; HbA1c, glycosylated hemoglobin.
Discussion
Imbalance in the cardiovascular autonomic regulatory system results in arrhythmias. In clinical practice, RHR is considered an indicator of the functional status of the autonomic nervous system. Some studies have suggested that obesity and reduced insulin sensitivity are associated with increased RHR; however, most relevant studies have focused on people with chronic diseases, 12 and data among community populations have rarely been reported. Studies have found that impaired cardiovascular autonomic function is a serious complication in patients with T2DM, characterized by nerve cell degeneration and segmental demyelination of nerve fibers, which can be easily overlooked by clinicians. 13 Impairment of autonomic fibers in the heart and vascular system can lead to elevated RHR, reduced heart rate variability, and hemodynamic disturbances. 14 A survey of patients with clinical T2DM found that the incidence of CHD and levels of FPG, 2-hour plasma glucose, and HbA1c were higher in patients with HRHR than in those with LRHR. Moreover, the incidence of CHD was increased with duration of T2DM, suggesting that glycemic control did not meet the target values. Patients with T2DM combined with CHD have a higher RHR.15,16 Increased RHR leads to increased secretion of several inflammatory cytokines, such as high-sensitivity C-reactive protein, fibrinogen, and interleukin-6, implying that the general population with high RHR is in a subclinical inflammatory state.17–20
Our observational study was conducted among a community-based population and included individuals with no obvious symptoms of discomfort; additionally, all data were from routine physical examinations. Most RHR values in our study population were in the range 57 to 80 beats/minute. The mean heart rate was 72.8 beats/minute in the HRHR group and 62.2 beats/minute in the LRHR group. We also found a positive association of RHR with T2DM and HbA1c, similar to previous studies. BMI and LDL were higher in the HRHR group, but the differences were not statistically significant. Our results suggest that abnormal glucose metabolism can increase RHR in a community-based population or among individuals with sub-optimal health, suggesting that this may be a mechanism by which hyperglycemia causes cardiovascular disease complications and that this mechanism may be independent of atherosclerosis.
In this study, multiple regression analysis also showed an association between hypertension and heart rate, although there was no statistical difference in the prevalence of hypertension between the two groups. Age was also found to be a factor affecting heart rate, but this could not be further elucidated in our study owing to the sample size.
Limitations
This was an observational study with a small sample size; larger interventional or prospective studies may be necessary to confirm our findings. Using the heart rate on resting ECG as the RHR, some heart rate changes could be affected by patient stress when performing ECG, resulting in an RHR is not the actual rate. Last, we did not consider sex differences in the data analysis.
Conclusions
In this study, we focused on a community-based population and found that abnormal glucose metabolism was associated with RHR. In community populations, RHR is only used as a therapeutic target in patients with CHD, hypertension, and diabetes. These findings imply that metabolic abnormalities combined with cardiovascular disease are present in community populations, especially among individuals with sub-optimal health. We suggest that elevated RHR is an important consideration in community populations.
Footnotes
Acknowledgements
We thank the staff of the Guangdong Provincial People's Hospital Medical Examination Centre for their work in data collection, and all participants who shared their experiences in data analysis.
Author contributions
WW designed the study. ZP and JY performed data collection. ZW and LF wrote and edited the article. ZH offered project management, supervision, and editing. All authors read and approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.