
Abstract
Introduction
Dental trauma is an irreversible injury that may occur in both children and adults. Disability has been identified as a risk factor for dental injuries; however, the distribution of disabilities and dental trauma among people in Pakistan who live in shelters/institutes is unknown. Thus, the current study sought to investigate the frequency of disability and its association with dental trauma among individuals residing in Pakistan’s special institutions.
Methods
An observational study was conducted. A total of 200 institutionalized subjects were recruited for the current study. The groups comprised a case group (n = 100) with dental trauma and a control group (n = 100) without dental trauma. Data were gathered from people who live full-time in various shelters/institutions in Karachi. The odd ratios (OR) were derived to assess the association of dental trauma with gender, age, and disability.
Results
Participants with disabilities had higher odds of experiencing dental trauma, with an OR of 14.426 (P = < 0.001*), compared to non-disabled participants. Among the study population, the most commonly reported type of disability was mental retardation (MR), accounting for 38%. Individuals under 20 years of age had higher odds (2.953) of having dental trauma compared to those over 20 years old (P = 0.002*).
Conclusion
MR among institutionalized people is the most prevalent type of disability. Disabled people are more vulnerable to dental trauma, living full time in shelters/institutions. There is a need to implement oral health protection strategies for all individuals residing in special shelters in Karachi.
Introduction
Dental trauma is an irreversible injury that has been prevalent worldwide. 1 Frequently reported dental injuries are among athletes, warriors, and disabled children that interfere with their professional or routine activities.2–4 Dental trauma is a common problem in Pakistan, affecting a significant number of people due to several factors, including falls, assault, and domestic abuse. 5 Children and adolescents with special care needs are illustrated as a high-risk group for dental injuries due to neurological, physical, and behavioral abnormalities.4–7 In Pakistan, around 6.2% of the population is reported to have some form of disability and faces significant disparity in access to oral health services as compared to the general population. 8 Besides that, there is limited data on dental trauma among disabled individuals, as most studies on this topic have focused on the general population rather than on disabled individuals within the country.
Many people in Pakistan are forced to live in special shelters such as orphanages due to poverty, health problems, and other domestic issues.9, 10 These shelters are run by governmental and non-governmental organizations (NGOs), housing disabled and non-disabled people. 11 Among these institutionalized individuals, mental and physical trauma is common, which has been linked to the availability of limited resources in the institutes. 12 Similarly, dental trauma is pervasive among institutionalized individuals in various Asian regions.13–15 Dental trauma has been linked to a variety of behavioral issues, including risk-taking behaviors, attention deficit syndrome, and hyperactivity disorders, 16 and non-behavioral problems, which include a history of falls. 17 However, among disabled people, even in the absence of contact sports or vigorous physical activities, dental injuries are common. 18 This could be due to complications prevalent in disabled people, like poor motor coordination, uncontrolled head movements, seizures, or a delayed response to surrounding obstacles. 19 In the same way, the risk of dental trauma in children is considered higher due to a lack of motor coordination and dexterity in daily activities,14, 15 which may rise in children with disabilities.20, 21 In the dental arch, anterior teeth are more vulnerable to dental trauma, predominantly maxillary anterior teeth, as their vulnerability escalates with increased overjet.20, 22
The authors believe that there is scarce data available to estimate oral and general health among Pakistan’s institutionalized people. Previous studies on institutionalized individuals primarily examined dental caries, with no instances of dental trauma reported. Furthermore, many previous studies in Pakistan on this topic were cross-sectional studies, which limits the assessment of multiple risk exposures for dental trauma. To explore the impact of disabilities on dental trauma, an observational study is essential. Thus, this study aims to examine an association of age, gender, and disability to dental trauma among individuals residing in special institutions. Moreover, to the authors’ knowledge, this study is the first in Pakistan to measure dental trauma and distribution of types of disabilities among institutionalized people in Pakistan, including visual impairment, speech and hearing disabilities (SHD), physical disabilities, mental retardation (MR), and multiple disabilities (MD).
Methods
An observational study was conducted in special shelter homes in Karachi to evaluate dental trauma and disability association. Our study recruited two groups based on the presence or absence of dental trauma, named cases and controls, respectively. Both groups were observed for age, gender, and disabilities. Ethical approval was obtained from the ERC (ethical review committee) of JMDC; ERC protocol number is (00078/20). Institutions and participants/interpreters were informed about the objectives, risks and benefits of the study. Signed and informed consent was obtained from them on agreement to participate in the present study.
Sample
Inclusion Criteria
Dental trauma of upper and lower anterior teeth, according to the criteria described by Andreasen et al. (2013). 23
Children and adults residing in special institutions/shelters, irrespective of gender.
Disabled and non-disabled individuals voluntarily agreed to participate in clinical examination.
Exclusion Criteria
Subjects who deny voluntary participation.
Dental wear due to any pathological condition.
Non-cooperative individuals.
Individuals with extreme medical conditions like history of a major stroke, active cancer within five years, atrial fibrillation, heart failure, kidney failure, recent major surgery, severe psychiatric disease that may limit the subjects’ aptitude to participate.
Disability was assessed according to the Guidelines for the evaluation of various disabilities and procedure for certification (2008)
24
which are distributed into the following categories:
Visual impairment Speech and hearing disability Physical disability Mental retardation Multiple disabilities. Defined as a combination of two or more the above-mentioned disabilities.
Sample Size
The sample size for unmatched case-control was used, in which the case was assigned to institutionalized individuals with dental trauma and the control group to institutionalized individuals without dental trauma. A minimum sample size of 180 was required (90 in each group), based on the hypothetical proportion of cases with exposure 25 from a previous study, 95% confidence interval, and 80% power of test. OpenEpi version 3 was used for sample size calculation. Finally, a total of 200 individuals were recruited. Due to the availability of limited resources to access special institutions and reaching out disabled population, subjects in each study group were selected via non-probability consecutive sampling as a case group with dental trauma (n = 100) and a control group without dental trauma (n = 100).
Data Collection
The study was conducted from January 2019 to December 2019, reaching out various shelters and institutions in Karachi. A group of dentists, including the authors of the study, visited three institutions: the Edhi Foundation, Darul Sukoon, and the Kashafan-e-Nonehal Atfal Orphanage. All assessors were trained before participating in the data collection. Variables recorded on the data sheet by examiners include age, gender, type of disability, any traumatic injury, and lastly, clinical dental trauma.
Dental trauma of upper and lower anterior teeth was recorded clinically among all participants. Dental trauma recorded includes enamel and dentine fractures, following the criteria established by Andreasen et al. (2013). 23 For the clinical examination, subjects were seated to ensure clear visibility using natural light. Sterilized mouth mirrors, disposable tongue depressors, and gauze were used in compliance with biosafety standards 26 for oral examination and to diagnose dental trauma. This study was approved by the ERC of a local medical institute in Karachi.
Statistical Analysis
Data analysis was completed using IBM SPSS statistics (version 20 Armonk, NY). Frequencies were derived for age groups, gender, and types of disabilities among institutionalized individuals. Odd ratios (OR) were calculated to assess the association of dental trauma with gender, age, and disability. A P < .05 was considered significant.
Results
A total of 200 individuals were recruited for this study. The groups were separated into the case group with dental trauma (n = 100) and the control group without dental trauma (CG; n = 100). Frequency of disabilities among 200 sample size was n = 94 distributed as VI (n = 6), SHD (n = 7), PD (n = 14), MD (n = 31), and MR (n = 36). The most prevalent type of disability that appeared in the studied population was MR (38%), followed by MD (33%) and PD (15%), as shown in Figure 1.
Distribution of Type of Disability in Disabled Population (n = 94).
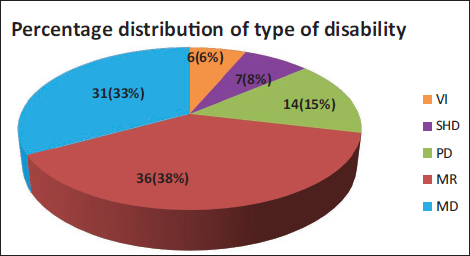
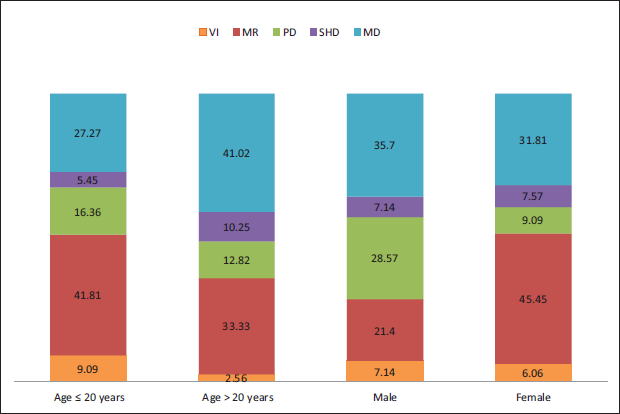
Figure 2 shows the distribution of types of disabilities according to age and gender. MD (35.7%) and MR (45.45%) appeared more frequently in males and females, respectively. The most frequent type of disabilities that appeared in children (≤20 years) and in adults (>20 years) were MR (41.81%) and MD (41.02%), respectively, as shown in Figure 2. In the total of 94 disabled individuals, 76 appeared with dental trauma. Figure 3 shows the frequency of dental trauma according to the type of disability, with the highest in MR (n = 34) followed by MD (n = 27) and the lowest in VI (n = 3) and SHD (n = 2).
Percentage Distribution of Type of Disability According to Demographic Variables Among Disabled Population (n = 94).
Dental Trauma According to the Type of Disability Among Disabled Population (n = 76).
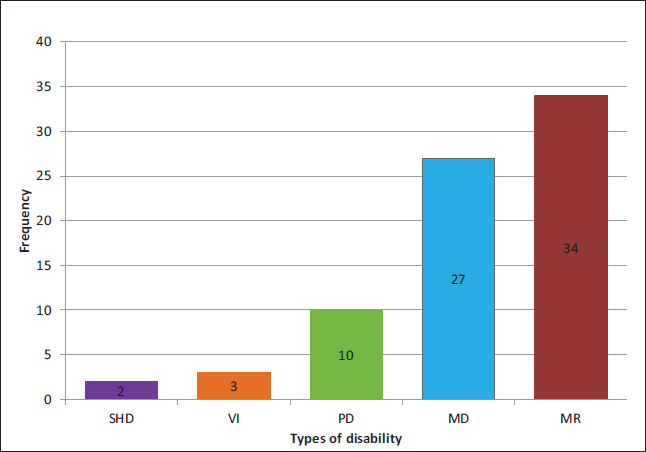
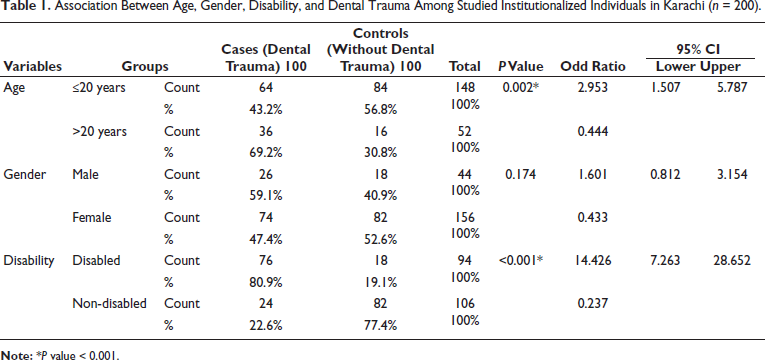
Table 1 shows the proportions of dental trauma between age groups, gender, and the presence or absence of disability in the study population. Participants with disability have shown a greater proportion of dental trauma (80.9%) than non-disabled participants (22.6%). Adult (>20 years) participants have higher proportions of dental trauma (69.2%) than age group ≤20 years (43.2%). Males have a higher proportion (59.1%) than females (47.4%) for dental trauma. According to the chi-square test, age group <20 years shown higher odds (2.953) of having dental trauma as compare to >20 years group (0.002*). Males had 1.601 times the odds of females for dental trauma, however, the results were not statistically significant (P = .174). Participants with disability shown higher odds (14.426) of dental trauma than non-disabled participants (P = < 0.001*).
Association Between Age, Gender, Disability, and Dental Trauma Among Studied Institutionalized Individuals in Karachi (n = 200).
Discussion
In Pakistan, dental caries and periodontal disease are recognized as significant oral health issues. To the authors’ knowledge, aside from dental decay, 27 there has been no documentation of other dental diseases, such as dental trauma, particularly among institutionalized individuals in the country. Therefore, this study may be the first to address dental trauma and types of disabilities among institutionalized people in Pakistan. According to the current study, the most common type of disability among Pakistan’s institutionalized people was MR 36%. However, according to age, among adults (41.02%), MD appeared more. The current study found that disabled adults experienced more dental trauma (69.2%) compared to children (43.2%). Nevertheless, children and adolescents showed higher odds of dental trauma, and this odd was statistically significant (P < 0.001). Most previous studies discovered on dental trauma have focused on school-aged children, which may make it challenging to distinguish trends in dental trauma by age. Therefore, cohort studies are needed to examine patterns of dental trauma under similar conditions for both adults and children.
In our study assessing the distribution of disabilities in children, it was found that children and teenagers with MR experienced a higher frequency of dental trauma, which was recorded at 41.81%. This finding contrasts with research conducted by Nayak (2015), who reported that children with developmental disabilities (MD) had the highest frequency of dental trauma at 40.90%. 28 Additionally, Nayak’s study indicated that children with SHD experienced the least amount of dental trauma, which aligns with our current findings showing that individuals with SHD also sustained the lowest incidence of dental trauma. In the present study, it was observed that dental trauma was more common among male residents (59.1%) than female residents (47.4%). This aligns with findings from several previous studies, which indicate that males tend to experience higher rates of dental traumatic events compared to females, regardless of the presence of disabilities. 29 In assessing types of disabilities associated with dental trauma, former studies have shown a higher risk of dental trauma among MR and VI individuals. 30 In our study, although dental trauma was more frequent with MR disability, particularly among females, it was less frequent with VI residents. However, males with VI have shown more frequency of dental trauma than females with VI. Previously, Children with both VI and MR conditions showed similar patterns for gender as boys experienced higher rates of dental traumatic events compared to girls.31, 32 This trend is usually attributed to increased participation in contact sports and rough play among males, which increases their risk of experiencing dental trauma. 32 Additionally, a study by Malak (2021) reported that the odds of dental trauma were higher in males (5.36) compared to females. 33 Likewise, the current study shows a similar trend, indicating that males have higher odds (1.6) of experiencing dental trauma than females.
The prevalence of dental trauma in disabled individuals reported in previous studies varies. Old studies conducted by Ogunboded in 1998 and by Holan et al. in 2005, reported that dental injuries were present among half of the participating disabled population.34, 35 According to Murthy et al. (2013), the prevalence of dental trauma in disabled appeared more as compared to non-disabled individuals. 36 Similarly, in our study, the prevalence of dental trauma in disabled people appeared widely more (80.9%) as compared to non-disabled individuals (22.6%). Our results contradict multiple previous studies, like one by Santos et al. (2009), where the prevalence of traumatic dental injuries in mentally challenged individuals was similar to that in healthy individuals. 37 Moreover, studies by Acharya et al. (2010) and Rajab (2019) found that non-disabled children had experienced more traumatic dental injuries compared to children with disabilities.38, 39 Rajab (2019) explained the reason that individuals with mental disabilities may struggle to develop adequate interpersonal skills, which can lead to social withdrawal and reduced participation in various activities. In the current study, dental trauma was found to be significantly associated with disabilities, resulting in an OR of 14.42. This finding is supported by Sakeenabi’s (2021) research, which revealed that children with cerebral palsy are 3.18 times more likely to experience dental trauma compared to their healthy peers. 40
During the study, the examiners observed untreated dental trauma and poor oral hygiene among all institutionalized individuals. One of the limitations of our study was a deficiency of information available about the time, place, and cause of dental injury from institutions to evaluate dental trauma association with relevant exposures as co-founding factors. Since participants were not selected randomly, the sample may not accurately represent the diverse characteristics of institutionalized individuals. Therefore, it is essential to include more institutions in Pakistan in future studies to obtain generalized information about the target population.
It is recommended that nationwide awareness programs be developed to prevent dental trauma and promote oral hygiene among people with disabilities, particularly those living in specialized shelters in Pakistan. These programs should focus on raising awareness among doctors, dentists, and teachers who work in special needs institutions, as well as parents and guardians. Additionally, institutions need to educate caregivers on how to manage and report dental trauma, and policymakers should establish guidelines for managing dental trauma in individuals with special needs.
Conclusions
MR among institutionalized people is the most prevalent type of disability. Although disabled people appear to be more at risk of dental trauma, it is a subdued threat to all people who are living full-time in Pakistan’s special institutions. There is a need to endorse oral health protection strategies for people living in special shelters in Pakistan. Furthermore, immediate educational programs are required to prevent dental trauma and promote oral hygiene among all institutionalized individuals.
Footnotes
Abbreviations
MD: Multiple disabilities; MR: Mental retardation; PD: Physical disability; SHD: Speech and hearing disability; VI: Visual impairment
Authors’ Contributions
MKS designed the study. MKS and HHJ conducted the literature search. HHJ, HP and MKS collected and organized the data. SN and MKS performed data analysis. HP and MKS have prepared tables and figures. HP and MKS were involved in manuscript writing. MKS edited and revised the final draft of the article. All authors have approved the final draft of the manuscript.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
All procedures were carried out in compliance with the Helsinki Declaration. Ethical approval was obtained from the ERC of a local medical institute in Karachi. Institutions and Participants/Interpreters were informed about the objectives, risks and benefits of the study. Signed and informed consent was obtained from them on agreement to participate in the present study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.