
Abstract
This paper details the characteristics of traumatic dental injuries (TDIs) during the Coronavirus 2019 (COVID-19) pandemic in 2020 at an Urgent Dental Care hub at King’s College Hospital Dental Institute, London, UK. For comparisons to be made, the characteristics of TDIs from a similar period in 2019 was also collected. Data was collected retrospectively from clinical records of patients suffering from dental trauma during both periods. An analysis was completed and conclusions drawn. The results suggest that the COVID-19 pandemic influenced the frequency, aetiology and type of TDIs. In order to suitably manage the provision of dental services, consideration must be given to the influence of pandemics on the characteristics of dental emergencies.
Learning Objectives
To analyse and understand the characteristics of traumatic dental injuries occurring during the COVID-19 pandemic
To compare the characteristics of traumatic dental injuries during the COVID-19 pandemic to a similar period in 2019
To consider and understand the reasons for these differences
Introduction
In December 2019, an outbreak of anovel pneumonia-like illness emerged in Wuhan, China. The causative pathogen, severe acute respiratory syndrome coronavirus 2 (SARS-Cov-2), was identified and has since spread to become a global catastrophe resulting in hundreds of thousands of deaths from the Coronavirus Disease 2019 (COVID-19). 1
In the United Kingdom, a nationwide lockdown was announced on 23rd March 2020 in response to the spreading virus. Two days later, on the 25th March 2020, the 2020 Coronavirus Act was passed granting unprecedented powers to the government and other authorities to enforce this lockdown. 2 On the same day, the Chief Dental Officer (England) announced that all routine, non-urgent dental care would be stopped and deferred; primary care practices were to establish a remote triage service and if the patient’s condition could not be managed by these means, they would be referred to, and seen by, a local Urgent Dental Care (UDC) service. 3
Although several reports from China4,5 and France 6 have described several characteristics of dental emergencies during a pandemic, little is known about the influence COVID-19 had on traumatic dental injuries (TDIs) and the factors associated with presentation to an Urgent Dental Care (UDC) service.
Aims and objectives
To quantify and analyse the characteristics of dental trauma presenting to an urgent dental care hub during the COVID-19 pandemic in 2020 and to compare this to patients presenting with dental trauma over the same period in 2019.
Methodology
Data was collected from all patients presenting with a TDI during the COVID-19 pandemic at a regional UDC hub located within King’s College Hospital London. The sample included all patients who attended from 13 April to the 8 June 2020. After this period, dental practices were advised to open their surgeries for face-to-face care for urgent patients by the Chief Dental Officer. 7
A retrospective analysis was conducted to scrutinise the clinical information and extract data. In order to draw comparisons, data was collected for a similar period in 2019 (15 April to 10 June 2019). Both sets of data were subsequently input into Microsoft Excel for descriptive comparisons to be made.
The data collected included:
Total number of patients
Gender
Age
Date of injury
Date of presentation
Aetiology of injury
Diagnosis of the traumatic dental injury sustained
Results
Trauma incidence
In total 28 patients presented with TDIs during the COVID-19 pandemic from 13 April to 8 June 2020. In the previous year, there were 52 patients with TDIs 15 April 2019 to 10 June 2019.
Patient characteristics
The age range of the patients presenting during the COVID-19 pandemic was 18-68 years with a mean of 34 years and two months. In 2019, the age range was 19-78 years with a mean age of 25 years and 10 months (Figure 1).
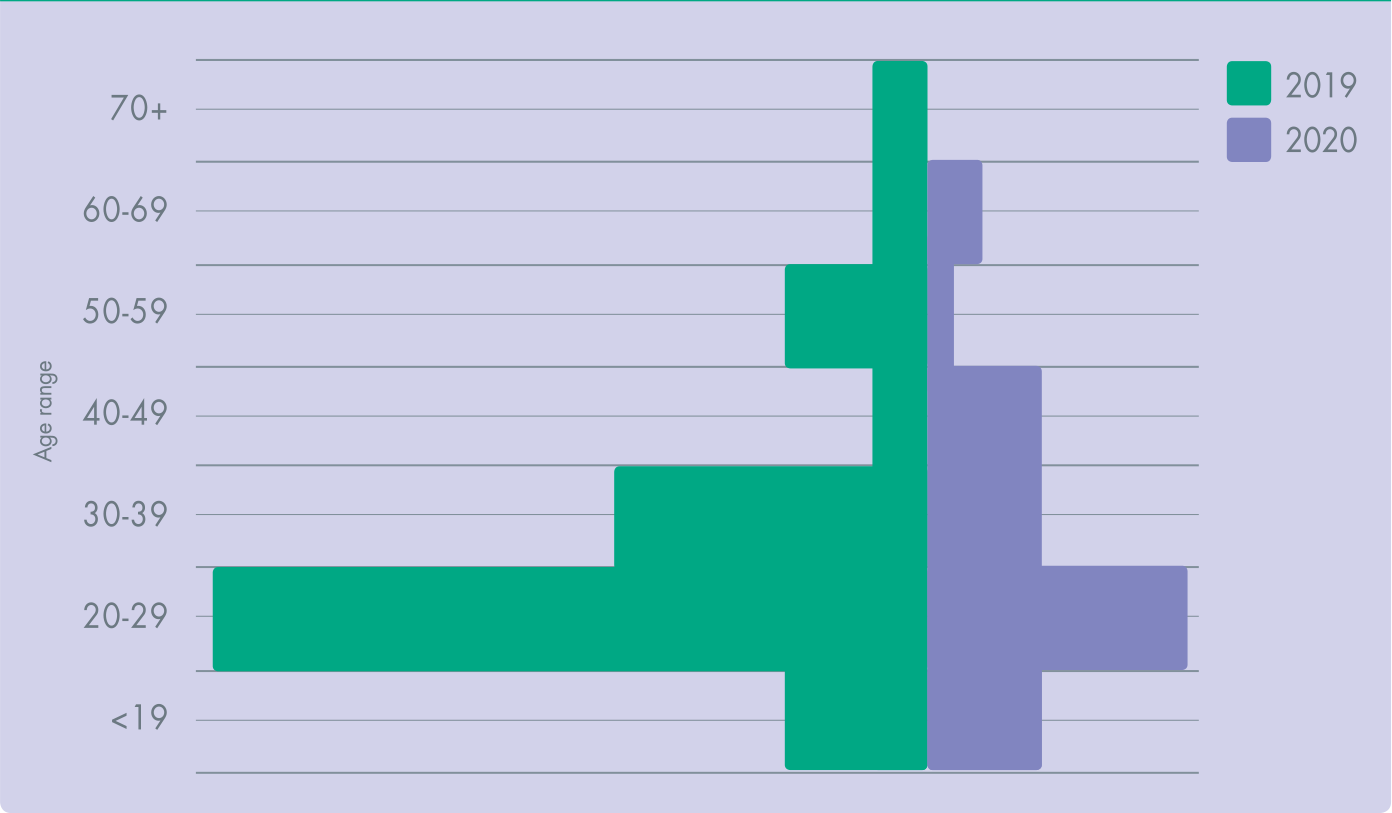
Population Pyramid for Ages of Patients Presenting in 2019 and the COVID-19 Pandemic in 2020
Of the 28 patients presenting in 2020 during the COVID-19 pandemic, 16 were female (57.1%) and 12 were male (42.9%). Of the 52 patients seen in 2019, 24 were female (47.1%) and 27 were male (52.9%) as depicted in Figure 2.
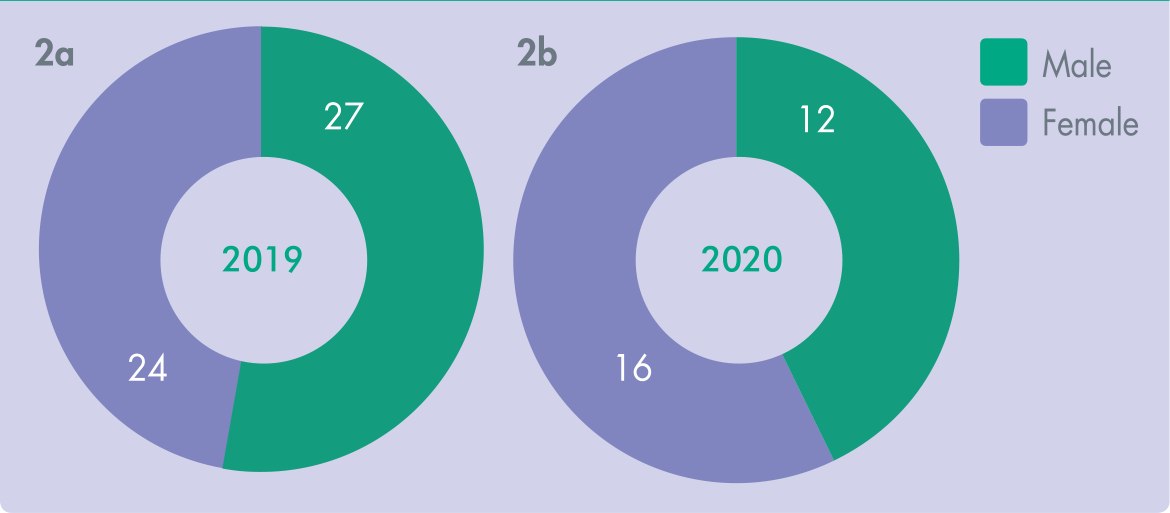
Genders of Patients Presenting in 2019 and the COVID-19 Pandemic in 2020
Aetiology of trauma
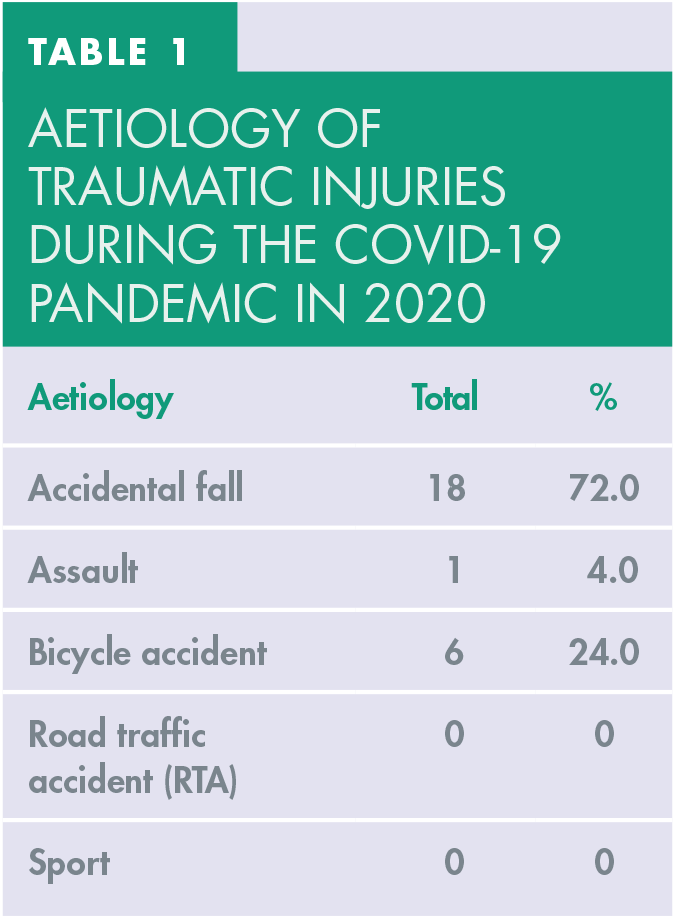
The aetiology of the TDIs for the 28 patients seen during the COVID-19 pandemic can be seen in Table 1. There were 18 accidental falls (72.0%), six bicycle accidents (24.0%) and one assault (4.0%). There were no TDIs as a result of road traffic accidents (RTA) or sport-related incidents during this period.
Aetiology of traumatic injuries during the COVID-19 pandemic in 2020
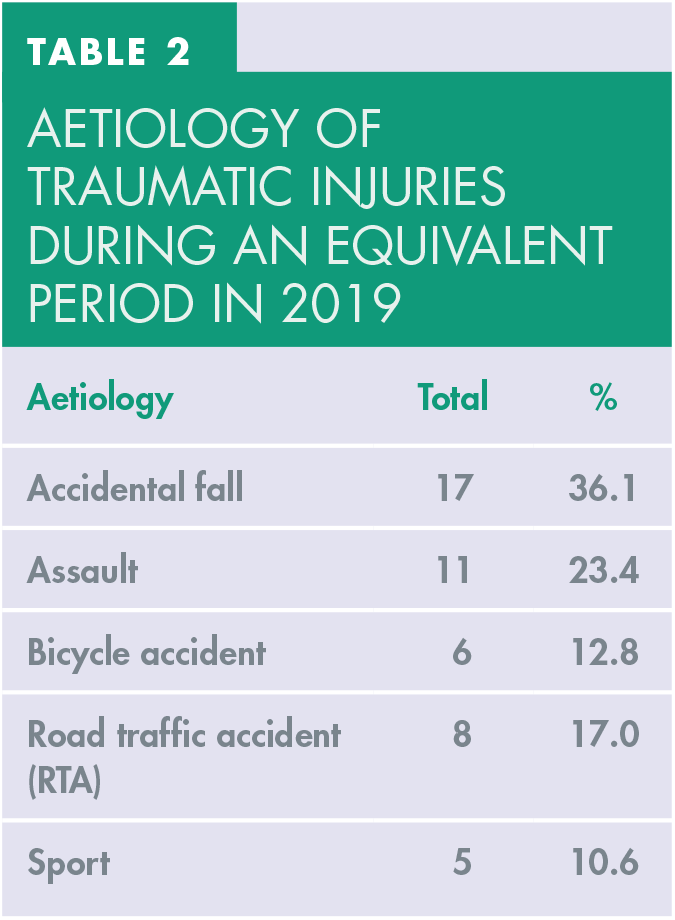
In 2019 (Table 2), of the 52 TDIs that presented to the UDC, 17 were caused by accidental falls (36.1%). This was followed 11 TDIs caused by an assault (23.4%), eight from RTAs (17.0%), six from bicycle accidents (12.8%) and five from sports injuries (10.6%).
Aetiology of traumatic injuries during an equivalent period in 2019
A comparison of the aetiology of dental trauma can be seen in Figure 3. Accidental falls are the most common of the TDIs in both 2019 and during the COVID-19 pandemic in 2020.
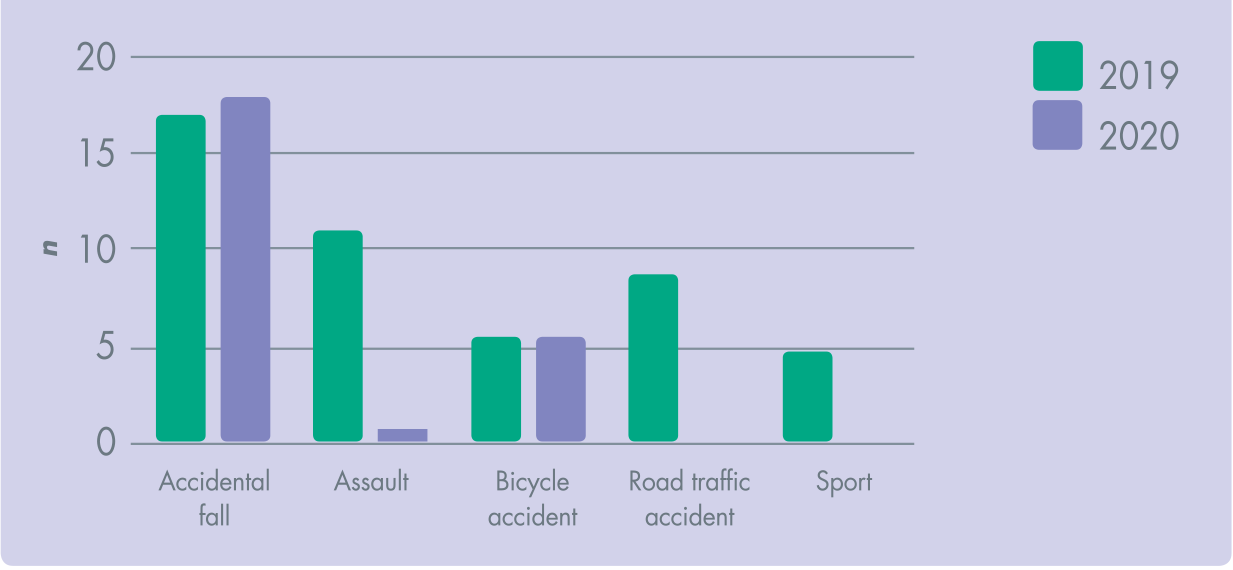
Aetiology of Dental Trauma During 2019 and COVID-19 Pandemic in 2020
Delay in presentation
The delay in presentation was measured in days from the date of the injury to the date of presentation at the UDC. Any delay in presentation for both cohorts of patients was calculated and the mean value was obtained. During the COVID-19 pandemic in 2020, the mean delay in presentation following the injury was 5.3 days and in 2019, the mean delay in presentation was 2.4 days.
Diagnosis of TDI
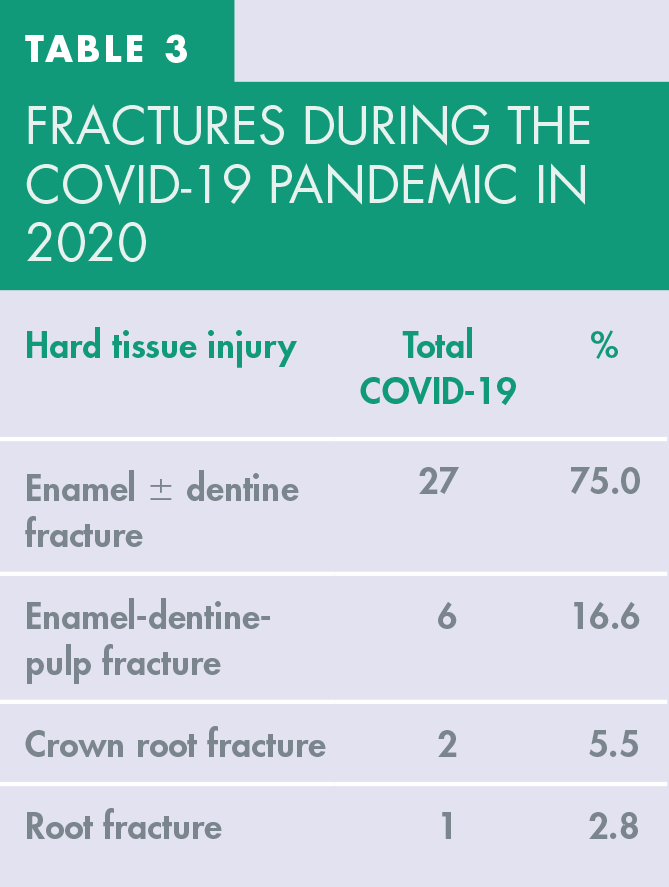
The most frequent TDI during the COVID-19 pandemic in 2020 was an enamel ± dentine fracture occurring 27 times. These accounted for 75.0% of all hard tissue injuries (Table 3). There were six enamel-dentine-pulp fractures (16.0%), two crown-root fractures (5.5%) and one root fracture (2.8%).
Fractures during the COVID-19 pandemic in 2020
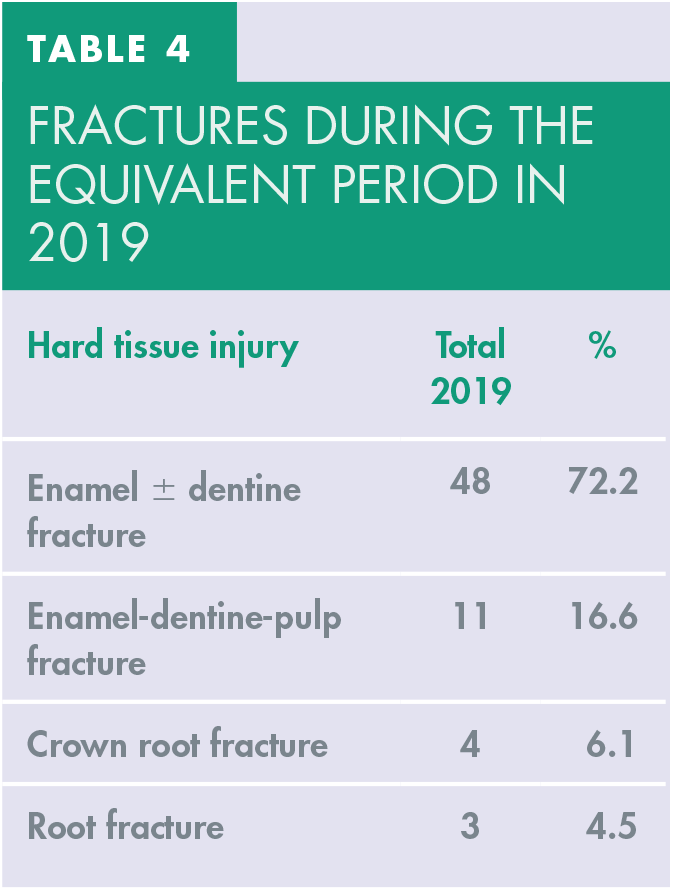
In 2019, there were 48 enamel ± dentine fractures, a total of 72.2% of all hard tissue fractures. In addition, there were 11 enamel-dentine-pulp fractures (16.6%), four crown-root fractures (6.1%) and three root fracture (4.5%) (Table 4).
Fractures during the equivalent period in 2019
A comparison of the fracture injuries during the COVID-19 pandemic in 2020 and in 2019 can be seen in Figure 4. In both periods, the most common TDI was an enamel ± dentine fracture, followed by enamel-dentine-pulp fractures, crown-root fractures and lastly, root fractures.
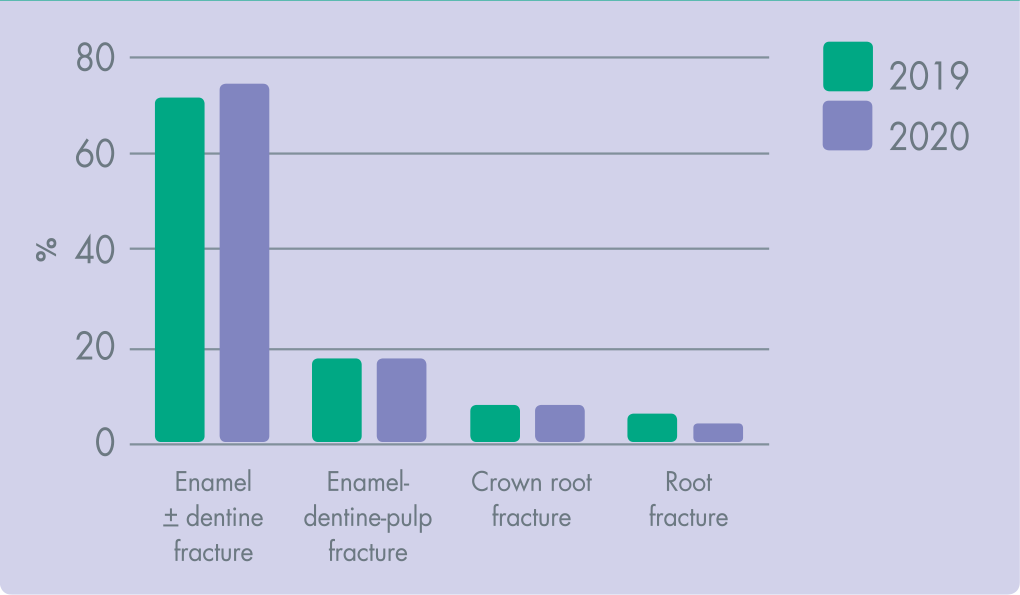
Comparison of Fractures Between 2019 and COVID-19 Pandemic in 2020
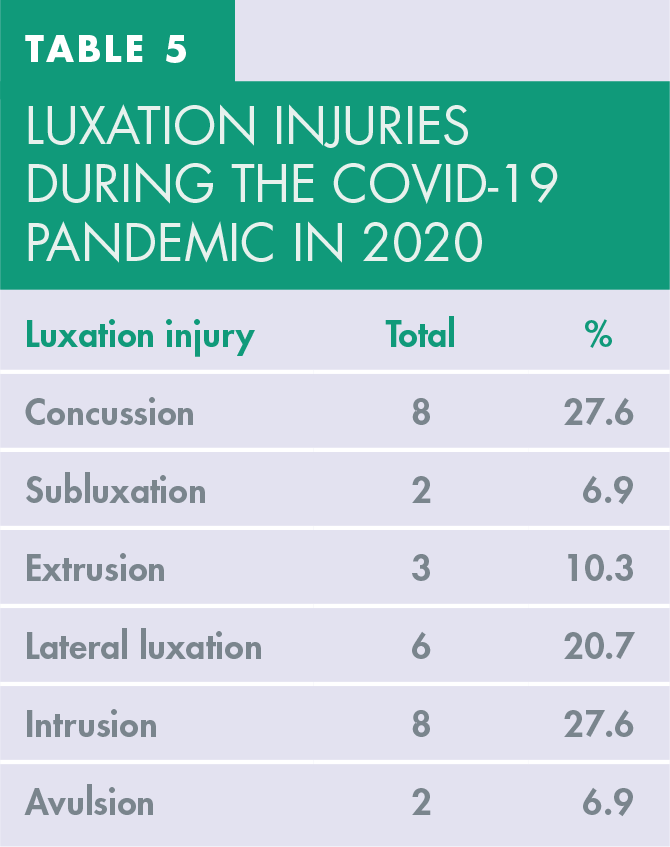
With respect to luxation injuries, during the COVID-19 pandemic in 2020 there were 8 teeth with concussion (27.6%); 6 teeth with lateral luxation (20.7%); 3 teeth with extrusion (10.3%) and 8 teeth with intrusion (27.6%) as seen in table 5.
Luxation injuries during the COVID-19 pandemic in 2020
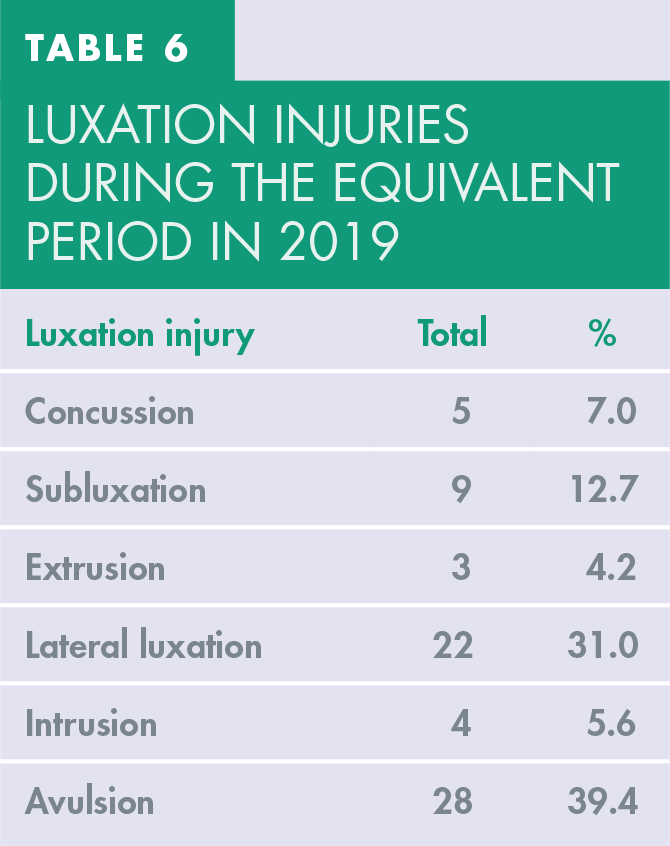
In the equivalent period in 2019, there were 5 teeth with concussion (7.0%); 9 teeth with subluxation (12.7%); 3 teeth with extrusion (4.2%); 22 teeth with lateral luxation (31.0%), 4 teeth with intrusion (5.6%) and 28 teeth with avulsion (39.4%) as seen in table 6.
Luxation injuries during the equivalent period in 2019
A comparison of the percentage of luxation injuries occurring between the COVID-19 pandemic in 2020 and in the equivalent period in 2019 can be seen in Figure 5. The graph demonstrates a different distribution of luxation injuries between the two periods, particularly for concussion, intrusion and avulsion.
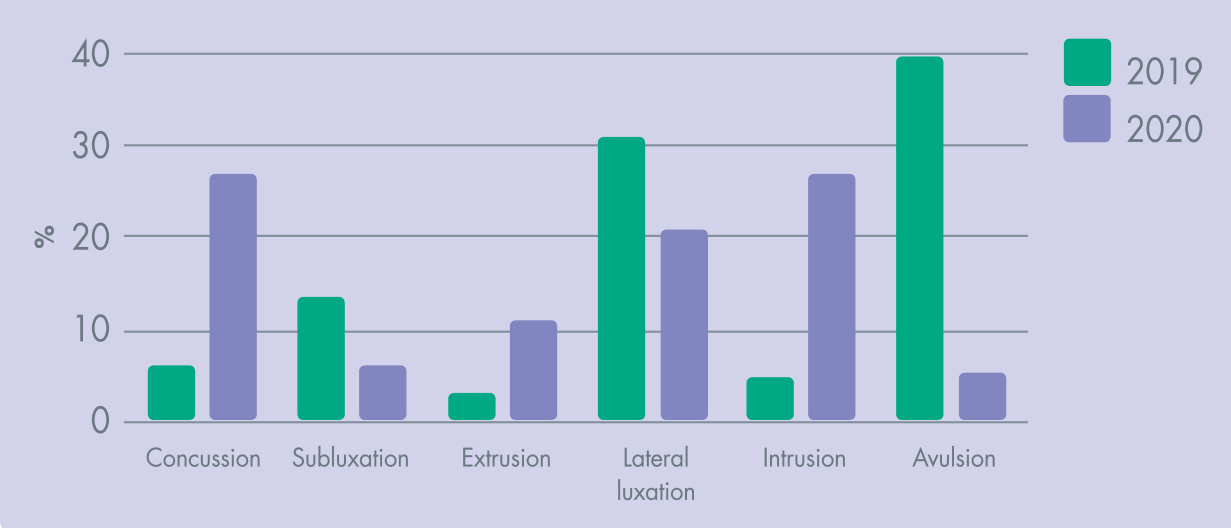
Comparison of Luxation Injuries Between 2019 and COVID-19 Pandemic in 2020
Discussion
Prior to conducting this analysis, it was unclear whether there would be a significant change in the incidence and characteristics of TDIs throughout the COVID-19 pandemic. This analysis has produced meaningful results from which conclusions can be drawn.
As dental practices were forcibly closed during the COVID-19 period, 3 it was uncertain whether Urgent Dental Care (UDC) services would be inundated with patients suffering from TDIs. However, this analysis has demonstrated that this was not the case with a significant reduction in the overall number of TDIs compared to an equivalent period in 2019.
Prior research has revealed that patients are more hesitant to visit a hospital out of the potential risk of contracting acute viral infections. 4 Due to the very nature of operative dentistry, with aerosol-generating procedures (AGPs) and potential heightening of the risk of transmission, 8 it could be suggested that this would lead to a reduction in the patients utilising this UDC service. In addition to, and as a result of,a reduction in the frequency of precipitating activities leading to TDI’s, this analysis has demonstrated a reduction of 50% of TDI’s presenting during the COVID-19 period compared to 2019. In addition, the increased delay in presentation could be due to this anxiety or more worryingly, could be due to problems in accessing care.
Throughout this stage of the pandemic, this UDC was under unprecedented strain due to the inundation of non-TDI emergency patients, PPE issues and evolving standard operating procedures. The delay could therefore be a consequence of patients having difficulties in obtaining an appointment from the UDC service for their injury.
Despite the lockdown measures enforced by the government, the age distribution of patients suffering with TDIs did not differ hugely for the population below the age of 50 during the COVID-19 period, albeit a higher total number of patients presented in 2019 (Figure 1). Above this age range, there was a significant reduction in patients, with no TDIs seen in patients above the age of 70 during the COVID-19 lockdown and fewer above the age of 50.
The reduction in patients from the over 70 age range may be explained by the perceived fear of contracting a viral infection. Patients in this age range are considered more vulnerable to SARS-Cov-2 and therefore may be less willing to go to a UDC hub, especially if this hub is situated within a large hospital. 4
During the COVID-19 pandemic, there was a marginal variation in the ratio of males to females seeking treatment for a TDI. Previous studies have shown that gender disparities within TDIs are declining, although males have a greater tendency to suffer trauma as a result of violence or contact sports.9,10 The slight variation in the gender of patients presenting during the COVID-19 lockdown could be explained by the difference in causative activities during the nationwide lockdown. Due to the features of a lockdown, with no contact sports and a decrease in violence, this analysis suggests that this lead to a reduced propensity for males to suffer trauma and therefore the gender disparities normally present in TDI’s were concealed.
As expected, the aetiology of TDIs were different during the COVID-19 lockdown compared to 2019. The majority of the populations had restrictions on movement and sport, social distancing measures were in place and traffic in London reduced by roughly 53%. 11 This was clearly evident in the data analysis, with TDIs sustained from car accidents, sports and violence/assault contributing a minor 4% of the total TDIs compared to 51% in the pre-COVID-19 period in 2019.
Enamel ± dentine fractures are the most common hard tissue dental injury in the permanent dentition.9,12,13 This study demonstrated that during this stage of the COVID-19 pandemic, this was still the case. Interestingly, the relative frequencies of intrusions during the COVID-19 period was far higher than the corresponding period in 2019. This observation could be explained by a difference in the aetiology of injury between the two periods. The extent of trauma to both the hard tissues and the supporting structures is governed by the energy and direction of the impact. The main causes for dental trauma during the COVID-19 period were falls and cycling, whereas in the 2019, more traumas occurred playing sport, violence/assault, and road traffic accidents. It could be suggested that because of an increase in falls during the COVID-19 period and owing to the nature of falling, patients had a tendency to suffer an impact with an axial direction, forcing a tooth into the alveolar bone (intrusion). Through falling, patients are less likely to suffer non-axial impacts, which would more likely result in an avulsion, extrusion or lateral luxation. Comparatively, during sports or through violence and assaults, the direction of the impact may result in non-axial forces tending towards non-intrusive injuries.
This retrospective analysis of dental trauma during the COVID-19 pandemic has shown substantial and meaningful findings. We have observed a steep reduction in the number of traumatic dental injuries during the COVID-19 pandemic. The results suggest that the period affected the aetiology and diagnosis of traumatic dental injuries as well as patients’ behaviours in seeking dental care.
While trends were evident in the collected data, these must be carefully interpreted. Due to nature of the study, the sample size was limited. Ultimately there is a chance that the sample size may have resulted in type II errors in the results. Further studies will require comprehensive prospective planning with a large prospective cohort of subjects and a suitable standardised team of clinicians to ensure that there is adequate power to test the significance of the hypothesis.
Conclusion
Within the constraints of this analysis, the results suggest that the COVID-19 pandemic had an influence on the characteristics of traumatic dental injuries and the patients utilising an Urgent Dental Care (UDC) service. The nationwide lockdown may have reduced activities that lead to TDIs as well as the capacity for patients to access care.
It is important to recognise the effect that pandemics can have on dental emergencies in order to facilitate support mechanisms for patients, management strategies for dental professionals and appropriately allocate resources to where they are most needed.