
Abstract
The aim of this study was to determine whether adherence, satisfaction, and overall satisfaction in a remote case management-based intervention influence changes in functional physical performance in older adults with a history of recurrent falls. A clinical trial was conducted with 28 older adults randomized to the intervention group (IG), who received an online case management program focused on fall prevention and reducing modifiable risk factors for 16 weeks. The control group (CG) consisted of 26 participants who received general health guidance. Performance was assessed using the Short Physical Performance Battery (SPPB), Timed Up and Go (TUG), and Timed Up and Go Dual Task (TUGDT) tests at three time points (baseline, after 16 weeks, and after 1 year). After 16 weeks, adherence was evaluated based on participation frequency in the intervention, and satisfaction with remote interventions was assessed using a questionnaire based on the Short Assessment of Patient Satisfaction (SAPS). Adherence significantly influenced changes in postural balance (p = 0.044, R² = 0.09) and in muscle strength gain in lower limbs (sit-to-stand, seconds) (p = 0.034, R² = 0.11). Overall satisfaction positively influenced changes in verbal fluency (p = 0.048, R² = 0.11). Good adherence and satisfaction contributed to improvements in muscle strength, mobility and postural balance in older adults.
Introduction
Falls represent the second leading cause of death from unintentional injuries worldwide, accounting for approximately 684,000 deaths each year (WHO, 2021). They can also result in a loss of physical ability and a strain on the healthcare system (Tiedemann et al., 2024). Falls result from a complex interaction of factors, classified as extrinsic, such as environmental factors, and intrinsic, related to age, gait impairments, reduced mobility, fear of falling, and others (Colón-Emeric et al., 2024; Shelton et al., 2024; WHO, 2007). A higher risk of falls implies more potential falls, which, in turn, is directly related to their outcomes: older adults who fall recurrently, meaning those who experience two or more falls per year, have worse outcomes compared to those who fall only once annually (Jehu et al., 2021; Kelsey et al., 2012).
As a result of the COVID-19 pandemic (SARS-CoV-2) and social isolation measures to reduce the spread of infections, older adults became more prone to falling. This is because social isolation has contributed to decreased social mobility, reduced vitamin D intake through sun exposure, and consequently, a decline in physical performance and an increased risk of falls (Boucher, 2012; Pelicioni & Lord, 2020; Perracini et al., 2021).
Thus, the COVID-19 pandemic contributed to the need for a reassessment of the treatments provided. In this context, telemedicine became essential in the care of older adults, a group already affected by the intrinsic and extrinsic ageing factors, such as limited mobility, the risk and fear of falling, transportation barriers, and lack of a companion. These factors, especially when combined with pandemic situations and social restrictions, negatively affect adherence to in-person treatments or interventions, thus encouraging the use of remote formats in these cases (Dos Santos et al., 2021; Melo et al., 2025; Ozsoy et al., 2022; Souza et al., 2020).
Thus, there is a need for remote-format interventions tailored for older adults with a history of previous falls in the community. It is reiterated that falls are multifactorial events that require combined measures for the development of treatments, preventive actions, smart home systems, medication reviews, and educational initiatives to minimize their occurrence (Chan et al., 2021; Silva et al., 2019; Van Scherpenseel et al., 2023). Among multifactorial interventions, the case management identifies individual risk factors based on a multidimensional assessment. It develops intervention plans that effectively address the needs indicated by the individual, minimizing health complications in older people (Gonzales et al., 2003; Huntley et al., 2013).
In this context, case management can be applied to older adults with a history of falls, especially those with a history of recurrent falls. Older adults’ adherence and their satisfaction with the proposed interventions are needed to achieve the effectiveness (Burnier & Egan, 2019; WHO, 2003). Low adherence contributes to health complications and a decrease in quality of life, as well as an increase in healthcare costs (Santos et al., 2022). Therefore, for the sustainment of positive effects of falls prevention programs, older adults need to adhere to the recommendations as long as possible and be satisfied with the services provided (Mittaz Hager et al., 2019).
Although several studies have addressed factors that influence adherence and satisfaction (Janducci et al, 2023; Kavalnienė et al., 2018; Stineman et al., 2011), there is a need to understand how adherence and satisfaction with a falls prevention program influence changes in motor risk factors for falls. Two systematic reviews conducted in 2012 and 2023 did not find studies that addressed the relationship between improvement in functional physical performance and adherence or satisfaction with interventions. Furthermore, there is a scarcity of research evaluating adherence and satisfaction in studies conducted remotely through telemedicine (Candanedo et al., 2023; Simek et al., 2012). Assessing adherence and satisfaction in remote interventions is crucial (Bernocchi et al., 2019; Chan et al., 2021, Lach et al., 2023) and their benefits to the patient/client/consumer need to be further explored.
Thus, the aim of this study was to determine whether adherence, satisfaction and overall satisfaction with a remote intervention based on case management influenced changes in functional physical performance in older adults with a history of recurrent falls. It was hypothesized that high adherence and satisfaction with a remote intervention would promote positive changes in physical performance, mobility and dual task performance.
Methods
Study Design
This controlled, single-center, parallel-group (1:1 allocation rate), blinded (evaluator) clinical trial included an intervention group (IG) and a control group (CG). This study is part of the Multidimensional and Management Assistance Program for Faller Older People (MAGIC) (São Carlos, Brazil). The program aims to evaluate the effects of remote case management on reducing risk factors for falls in older adults with a history of falls (Alberto et al., 2022). The study was approved by the Human Research Ethics Committee of the Federal University of São Carlos/SP (CAAE: 34696620.0.0000.5504) and included in the Brazilian Clinical Trials Registry (REBEC) (RBR-3t85fd). It also followed the recommendations of the Consolidated Standards of Reporting Trials (CONSORT) (2010) (Schulz et al., 2010). The aims and procedures of the research were explained to the participants and family members. The participants signed a free and informed consent form.
Participants
Eligibility criteria were: noninstitutionalized individuals with a history of falls in the previous year who reside in Brazil and are 60 years old or older and can communicate via the telephone were included in this study. Participants were recruited using posters and pamphlets, media such as TV and radio, social media and public and private social and health services through December 2021. The inclusion criteria were availability and interest in participating in the study; ability to walk alone for at least 6 meters, with or without a walking aid; a history of two or more falls in the previous year; and access to virtual media, with cameras and audio in good working condition and stable internet access due to the remote format of this study.
The exclusion criteria were: individuals with uncorrected hearing or visual impairment that made communication during assessments and interventions impossible; any active inflammatory or neurological disease that could interfere with balance performance (such as advanced (stage 5) Parkinson disease according to the modified Hoehn and Yahr scale without the use of antiparkinsonian medications, multiple sclerosis, Huntington disease, dementia, uncontrolled vestibulopathy, epilepsy, traumatic brain injury or severe motor sequelae of stroke), Older individuals or family members/caregivers who were not able to read the support materials and participants without stable internet access for participation in the evaluations and interventions .
Sample Size
The sample size was calculated, taking into account the purpose of verifying whether adherence and satisfaction with an intervention based on case management would influence changes in physical functional performance. The rule of at least 10 cases of the outcome (success or failure) was used, depending on which is rarer, for each independent variable used in the logistic regression model (Peduzzi et al., 1996). Therefore, considering an improvement/maintenance of physical functional performance (SPPB) of 59.7% based on a pilot study and the use of univariate linear regression analyses, a minimum of 25 people should constitute the total sample. With a chance of loss of 20%, a sample of at least 30 people in total was estimated.
Randomization and Blinding
After the initial assessment, an independent researcher conducted the randomization using random allocation software to generate a sequence list of participants. Randomization was performed in blocks of 10 at a 1:1 allocation ratio, and participants were allocated to the IG or the CG. Each participant received an opaque and sealed envelope, numbered in order, containing the card that indicated which group the individual was placed in. The card was opened by another independent researcher, who informed the volunteers of the allocation. The evaluators were blinded to randomization, but the researchers responsible for the interventions and the volunteers were not blinded to randomization due to the nature of this clinical trial.
Assessment
The evaluation was conducted remotely using Google Meet. The remote assessment was conducted by undergraduate gerontology students and by a nurse (MS). All assessors were previously trained. The tests conducted in this assessment demonstrated good reliability (Melo et al., 2025). Initially, clinical and sociodemographic data were collected, including age, gender, body mass index, medication use, morbidities and history of falls. At baseline, after 16 weeks and after 12 months, the Timed Up and Go test (TUG) and TUG dual task (TUGDT) (Podsiadlo & Richardson, 1991) were used to assess functional mobility. The TUG test requires the participant to stand up from a chair, walk three meters at the usual speed, turn around, return to the chair and sit down. The TUGDT requires the participant to perform the TUG with verbal fluency (naming animals) while completing the test (Shumway-Cook et al., 2000).
The Short Physical Performance Battery (SPPB) was used to assess physical functional performance (Guralnik et al., 1994; Nakano, 2007). The SPPB consists of three tests: a postural balance test in three positions (standing with one’s feet together for 10 seconds, with one foot partially in front for 10 seconds, and with one foot in front for 10 seconds); a 3-metre gait speed test; and a 5x sit-to-stand test. Each test is scored from zero to 4 points, with 4 points indicating a better performance (Nakano, 2007). In addition, after 16 weeks of intervention, adherence to the fall prevention program was assessed by the response rate to telephone calls made to both groups—16 calls to the intervention group (one per week) and four to the control group (one per month). Participants were classified as having satisfactory adherence if they responded to at least 70% of the calls.
A questionnaire was administered to assess satisfaction with the interventions in both groups on the basis of the Short Assessment of Patient Satisfaction (SAPS) (Hawthorne et al., 2014). The SAPS is a valid and reliable measure of patient satisfaction in clinical settings, with seven questions. Each question has 5 possible answers including very satisfied, dissatisfied, neither satisfied nor dissatisfied, satisfied and very dissatisfied, with scores ranging from 0 to 4. A score of 28 indicates very satisfied, whereas a score of 0 indicates very dissatisfied (Hawthorne et al., 2014). Furthermore, an additional question was included regarding overall satisfaction with patient care (“How would you rate the care you received in the past four months?”). The score for this question ranged from 0 (“the worst possible”) to 10 (“the best possible”).
Intervention
The volunteers in the CG were encouraged to maintain their routine, and their overall health was monitored through monthly phone calls. The IG received case management for 16 weeks via weekly phone or video calls. During the first week, instructions for the assessments and interventions and a tutorial regarding the multidimensional assessment and use of phone/video calls were provided. The multidimensional assessment was used, including screening of potential modifiable risk factors for falls, such as a history of previous falls, footwear used, foot shape, cognitive parameters, anxiety and depression, fear of falling, vitamin D deficiency, acute and/or chronic diseases (osteoporosis/osteopenia, urinary incontinence, cardiovascular disease, dizziness or cerebellar dysfunctions), low visual acuity, heart rate and rhythm alterations, living alone, use of medications, hypotension and postural instability, home safety, use of walking aids, functional activities, muscle strength, mobility and balance and pain (Alberto et al., 2022).
During the second week, case managers (two gerontologists and a nurse with prior training) explained the identified risk factors for falls to the volunteers and/or their family members identified multidimensional assessment. An individualized plan for fall prevention and controlling the identified risk factors for falls was developed in collaboration with the volunteers, taking into account their personal preferences and priorities. From the third to the sixteenth week, the intervention plan was implemented, with guidelines and recommendations for achieving the goals and motivational support. During monitoring, the case managers discussed any doubts and difficulties in carrying out the activities and achieving the goals with the volunteers. Assistance, referrals and modifications of the plan were provided to facilitate the process (Alberto et al., 2022).
All interventions were supervised by two professors with experience in falls prevention. The case managers were undergraduate and graduate students in Gerontology, with meetings to discuss cases every week. All interventions were trained previously. Additionally, all of the volunteers in the IG were encouraged to participate in a physical exercise program. Medical consent was required to participate in the physical exercise. The physical exercise program was performed at home twice a week using recorded videos available via WhatsApp.
The participants were instructed to contact 2 trained and qualified professionals (physical therapist and physical educator) via WhatsApp with any questions or concerns. The physical exercise program lasted 16 weeks, and the 60-min session consisted of warm-up, balance exercises, walking, muscular strength exercises for the trunk and lower limbs with a functional focus and cool-down (breathing and global flexibility exercises, including ankle flexibility) (Buto et al., 2019; Chodzko-Zajko et al., 2009). More information regarding this protocol has been reported previously (Alberto et al., 2022).
Statistical Analysis
A significance level of α = 0.05 was used, and the statistical tests were performed via the Statistical Package for the Social Sciences software (SPSS) (version 22.0, Chicago, Ill., USA). The Kolmogorov‒Smirnov normality test was used to verify the data distribution of the continuous variables. The chi-square test and the Mann‒Whitney U test were used to assess differences between the groups at baseline. To evaluate whether adherence to the interventions (frequency) and satisfaction with remote interventions (SAPS score) influenced changes in risk factors for falls (the dependent variable categorized as improvement/maintenance or worsening for each motor risk factor), a simple logistic regression test was used (probability for stepwise: entry 0.05 and removal 0.10), with a 95% confidence interval for exp (B).
Results
The sample consisted of 62 participants at baseline. After 16 weeks, 7 volunteers had been lost, resulting in a final sample of 28 participants in the IG and 27 volunteers in the CG. Five more volunteers were lost after 12 months (Figure 1). There were no significant differences in clinical or sociodemographic characteristics between the groups (Table 1). The sample was mostly female (88.9%) with a median age of 70–73 years. The intervention frequency was 100% (interquartile range of 25–75%: 100–100) for both groups (p > 0.05). The IG was more satisfied (median SAPS score (interquartile range 25–75%) = 25 (22.00–27.00) points) than the CG (22 (20.00–25.50) points) (p<0.05). Overall satisfaction had a median (interquartile range 25–75%) score of 10 (8.25–10.00) points in the IG and 10 (9.00–10.00) points in the CG (p > 0.05).

Flowchart of the volunteers included in the study (CONSORT 2010).
Clinical and Sociodemographic Characteristics.
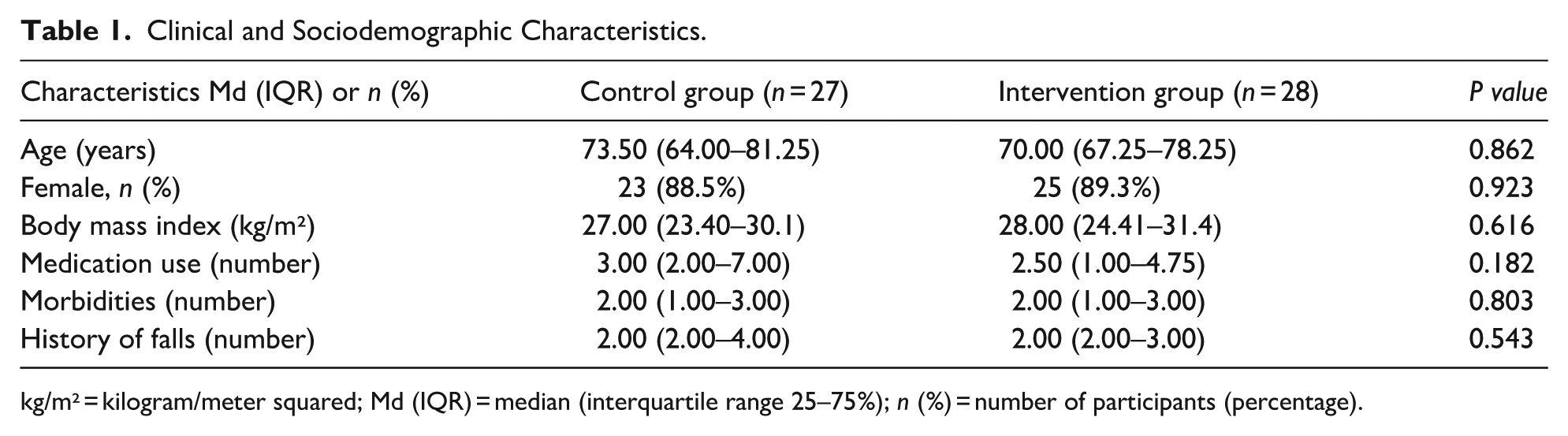
kg/m² = kilogram/meter squared; Md (IQR) = median (interquartile range 25–75%); n (%) = number of participants (percentage).
No significant differences were found between the groups in terms of physical functional performance, and both groups presented improvements in sit-to-stand performance and maintenance of other functional physical performances. After 12 months, the physical functional performance was maintained, with no significant differences between the groups (Table 2). Adherence significantly improved the postural balance and muscle strength of the lower limbs (delta split-to-stand test) after 16 weeks. Volunteer satisfaction, measured using the SAPS score, did not influence physical functional changes. Overall satisfaction significantly influenced improvement in verbal fluency during the TUGDT. Other physical functional changes did not influence adherence, satisfaction or overall satisfaction 16 weeks (Table 3). After 12 months of intervention, adherence influenced postural balance (B (95% IC) = −0.01 (−0.02 - −0.06); p ≤ 0.001). Other factors did not influence adherence or satisfaction with the interventions (Table 4).
Changes in Physical Function Between the Groups After 16 Weeks and 12 Months.
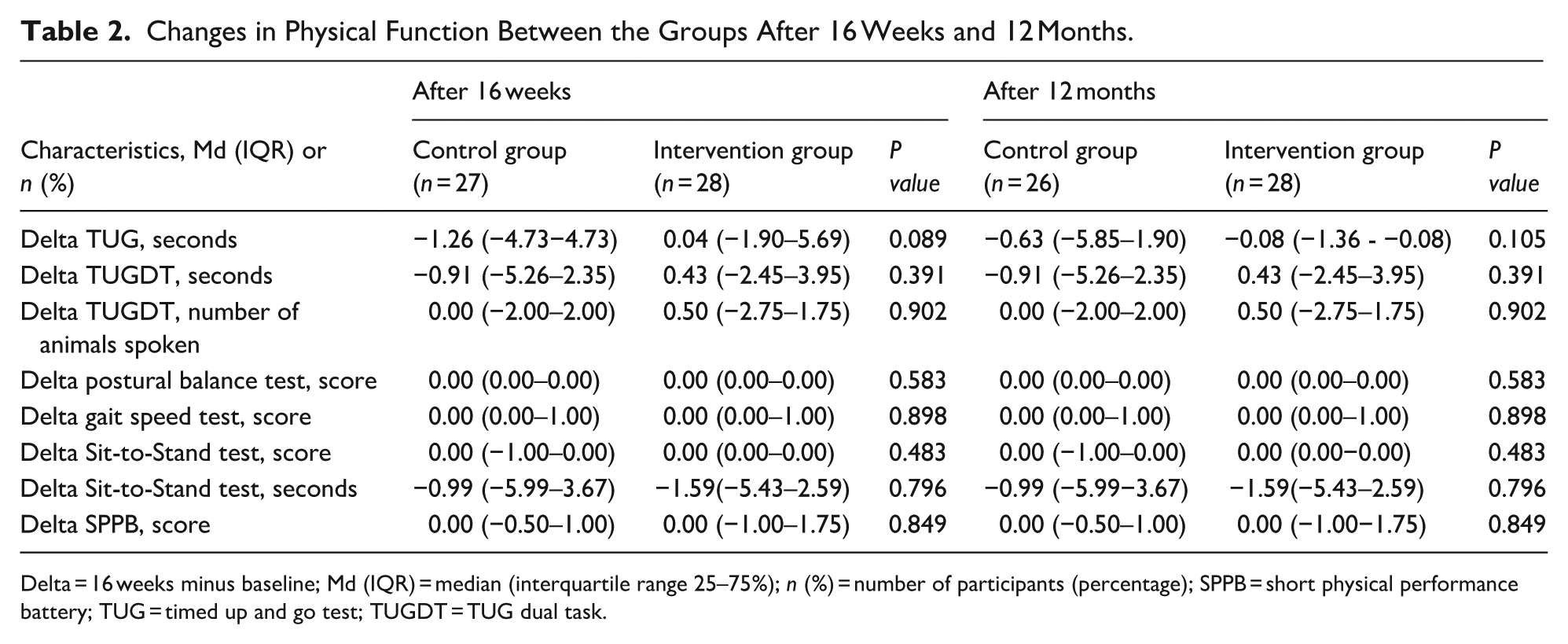
Delta = 16 weeks minus baseline; Md (IQR) = median (interquartile range 25–75%); n (%) = number of participants (percentage); SPPB = short physical performance battery; TUG = timed up and go test; TUGDT = TUG dual task.
Influence of Adherence and Satisfaction with Interventions on Physical Functional Changes During 16 Weeks of Intervention (n = 55).

Delta = 16 weeks minus baseline; CI = confidence interval; n = number of participants; P value≤0.05; SPPB = short physical performance battery; TUG = timed up and go test; TUGDT = TUG dual task; StS = sit-to-stand. Bold value means p < 0.05.
Influence of Adherence and Satisfaction with Interventions on Physical Functional Changes Over 12 Months (n = 54).
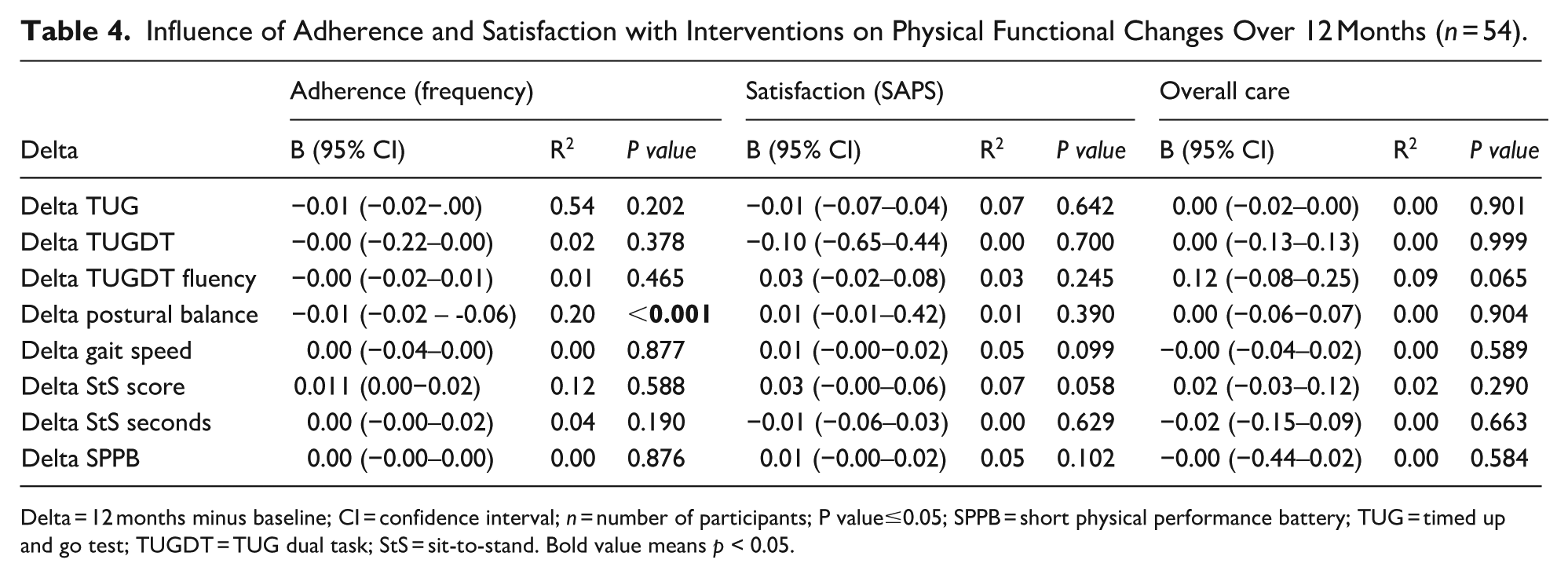
Delta = 12 months minus baseline; CI = confidence interval; n = number of participants; P value≤0.05; SPPB = short physical performance battery; TUG = timed up and go test; TUGDT = TUG dual task; StS = sit-to-stand. Bold value means p < 0.05.
Discussion
This study aimed to investigate the influence of adherence and satisfaction with remote interventions on changes in physical functional performance after 16 weeks and 12 months in older adults with a history of recurrent falls. After 16 weeks, volunteers in the IG had greater satisfaction with the remote intervention than volunteers in the CG. Adherence to and satisfaction with overall care were positively rated in both groups. After 16 weeks, adherence significantly influenced postural balance and muscle strength of the lower limbs. Additionally, overall satisfaction positively influenced changes in verbal fluency during the dual-task situation. After 12 months, the physical functional performance of both groups was maintained, and adherence continued to influence changes in postural balance.
The participants were between 64 and 81 years old, and most were female (88.9%). Both groups had a history of recurrent falls and a median of 2 chronic diseases. The median age was also similar; however, the IG was younger, with a median age of 70 years compared to the CG, which had a median age of 73.50 years. These findings are consistent with studies (Mazo et al., 2007) which show that the majority of participants are women, which can be explained by the higher life expectancy compared to men. Although both groups showed good adherence, overall satisfaction, and satisfaction with the interventions, participants in the case management intervention were more satisfied. It was expected that the IG would feel more satisfied with the intervention compared to the CG, as they received case management and participated in the exercise program. According to the 2020 WHO guidelines on physical activity and sedentary behavior, “doing some physical activity is better than none” (Bull et al., 2020).
Therefore, it can be assumed that participation in an exercise program brings improvements to health and may reflect in satisfaction with the intervention. Furthermore, this result can be explained by the weekly communication with case managers who contacted participants to provide guidance, address any questions, and actively modify the intervention plan when necessary, thus ensuring greater safety and social interaction for the participant. This result highlights the relevance of case management in fall prevention, as it coordinates patient-centered actions, such as personalized interventions according to identified risk factors, health education, and monitoring the person’s progress, thus optimizing their care (Candanedo et al., 2023). When the person feels supported, encouraged, and has their preferences considered by the healthcare team, patient satisfaction increases (Çakmak & Uğurluoğlu, 2024).
After 16 weeks, the sit-to-stand performance was improved in the IG; however, there were no significant differences between the groups. Both groups maintained their physical functional performance, even after 12 months. After 16 weeks of intervention, adherence influenced changes in postural balance and muscle strength of the lower limbs, whereas satisfaction positively influenced verbal fluency during the dual task. After 12 months, adherence continued to impact changes in postural balance. This association between satisfaction and adherence with positive changes in functional physical performance suggests that intrinsic (age) and extrinsic (environment, health status) factors influence the response to training (Hughes et al., 2019). Therefore, falls prevention programs should develop strategies that increase satisfaction and adherence.
Unlike the STRIDE and PreFIT clinical trials (Bhasin et al., 2020; Bruce et al., 2021), this clinical trial had good adherence; however, it was expected that the greater the adherence to the intervention, the greater the positive changes in functional physical performance. This is because adherence influences the dose of multicomponent exercises, and this, in turn, improves the functional physical performance of older adults with a history of falls, as evidenced by Sherrington et al. (2019), Izquierdo et al. (2025).
In the present study, participants in the intervention group received an individualized multicomponent exercise protocol via recorded videos, developed from the initial functional assessment. After an orientation session, the program was performed independently at home, without synchronous professional supervision, which may have contributed to a suboptimal result in the functional physical performance tests. The format of delivery of the exercise program in person versus remote the sociodemographic characteristics of the participants and the environment where the intervention is performed may have interfered with the clinical results.
In line with these findings, it was expected that greater adherence would result in positive changes in functional physical performance. According to a meta-analysis, the hypothesis that increased adherence could enhance intervention outcomes in fall prevention programs remains inconclusive due to potential controversies and biases in the evidence arising from imprecise or indirect measurements of adherence to the interventions (Hughes et al., 2019). Adherence and satisfaction are important indicators of quality, though measuring and comparing these indicators across studies is complex due to the lack of consensus. Some studies assess adherence on the basis of frequency, whereas others use duration in weeks and questionnaires (Hughes et al., 2018; Mansson et al., 2020; Mikolaizak et al., 2022).
Another study (Mikolaizak et al., 2022) evaluated the impact of adherence to a physical exercise program integrated into lifestyle for older adults with a mean age of 66 years. It was found that adherence to the program was associated with improvements in physical capacity, such as balance and mobility. In this case, adherence was measured using the Exercise Adherence Rating Scale (EARS) in post-test and follow-up, which consists of a questionnaire with 16 questions, each with 5 response options scored from zero to four. Six questions aimed to identify the level of adherence, while the other 10 questions sought to identify facilitators and barriers. Another method used was the Monthly Adherence Report, which consisted of one question with seven response options regarding whether participants completed the planned activities, such as “they forgot, they didn’t feel well, they didn’t like the activities. . .” Adherence was considered in terms of full adherence, partial adherence, or non-adherence.
Overall, a better understanding is needed to comprehend how adherence and satisfaction influence physical performance. Furthermore, it is important to understand the barriers that prevent participants from adhering to the intervention before starting it (Mikolaizak et al., 2022; Seppala et al, 2025) the challenge is to develop strategies to ensure continuous and lasting adherence to evidence-based interventions, rather than determining which exercises are most effective for fall prevention (Izquierdo et al., 2021).
Regarding the strengths of the study discussed in this research, we highlight the use of the TUG, a test previously validated for remote use and which proved safe for evaluating functional mobility in older people with a history of falls at home (Melo et al., 2025; Pelicioni et al., 2022). Also, the use of case management to monitor participants provided social contact and encouragement to participate in the physical exercise program. All interventions considered the needs of each participant when performing the trainings, respected individuality and preferences, and promoted the necessary adaptations and progressions.
It is important to include adapted and validated physical tests to assess older people with falls risk and to measure patient satisfaction when performing falls prevention programs. Satisfaction is a good indicator of quality of health services, not only in person but also through telehealth. Through satisfaction analysis, it is possible to improve the quality of the service provided, implement strategic actions to engage the patient in the treatment and thus reduce health costs. Also, satisfaction with interventions can impact in changes in the health of older people. There is a need to implement more falls prevention programs for older people with falls risk, where users feel satisfied with the care and intervention received (Janducci et al., 2023).
This study has several limitations, including a small sample size, the predominance of participants residing in the Southeast region of Brazil and the high educational level of our sample. Therefore, these findings cannot be generalized to the entire Brazilian population due to the representativeness of different areas and the limitations in access to technology. Additionally, no validated tools are available for assessing satisfaction with nonpharmacological interventions in Brazil. Future studies should include a larger sample size, a longer intervention period and validated remote assessment methods.
Conclusion
After 16 weeks of intervention, participants in both the intervention and control groups showed good participation, demonstrating the feasibility of interventions in this format. Adherence significantly influenced changes in postural balance and lower limb muscle strength. Satisfaction with overall care significantly influenced positive changes in verbal fluency during the dual task. After 12 months of intervention, functional physical performance in both groups was interrupted, and continued adherence influenced postural balance in older adults with a history of falls. The influence of these variables in the tests reinforces the importance of considering motivational and behavioral factors as modulators of the response to the intervention.
Footnotes
Ethical Approval
The study was approved by the Human Research Ethics Committee of the Federal University of São Carlos/SP (CAAE: 34696620.0.0000.5504) and included in the Brazilian Clinical Trials Registry (REBEC) (RBR-3t85fd).
This study is part of the Multidimensional and Management Assistance Program for Faller Older People (MAGIC) (São Carlos, Brazil). The program aims to evaluate the effects of remote case management on reducing risk factors for falls in older adults with a history of falls (Alberto et al., 2022). The evaluation was conducted remotely using Google Meet. The tests conducted in this assessment demonstrated good reliability (De Melo et al., 2025).
Consent to Participate
All participants signed the informed consent form.
Consent for Publication
Informed consent for publication was obtained from the participant(s) through the informed consent form
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by FAPESP (2024/10699-6), CNPq (408323/2024-8) and in part by the CAPES (001).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.