
Abstract
Perceptions that women are in greater need of fall prevention might impact their participation in programs. This study aimed to understand gender differences in motivating factors and experiences in a fall prevention program. Thirty-four adults (18 men and 16 women) aged 60 years or older participated in focus groups after 12 weeks of fall prevention exercises and education. Six main themes emerged. It might be a macho thing represented an overarching theme of why men might not participate in fall prevention as readily as women. Personal experience as a motivator, Get my balance back, and Challenges/Successes were common themes for men and women. Both genders realized the benefits of the program; however, men emphasized the importance of personal outcomes (Being part of something bigger), whereas women highlighted group outcomes (Socialization). These findings can guide the future messaging and marketing of fall prevention programs for older adults.
Both older men and women perceive women as more in need of fall prevention programs
Different motivating factors for men and women can influence participation in fall prevention
Marketing strategies for fall prevention programs should consider gender differences
The perception that men do not need fall prevention could negatively impact older adults who are at risk of falls and in need of interventions
Health care providers need to be aware of potential gender differences and identify strategies to promote participation
Introduction
Falls are the second leading cause of unintentional injury deaths worldwide (WHO, 2021) and the leading cause of injury hospitalizations for older adults in Canada (PHAC, 2014). Approximately one in four older adults in North America experiences a fall each year (CDC, 2020; PHAC, 2014), costing approximately 10 billion dollars—Canadian dollars—average annual healthcare in Canada (Parachute, 2021) and 50 billion dollars—U.S. dollars—in the United States (CDC, 2020). Women are almost twice as likely to be injured after a fall; however, men have higher fatality rates (Nordstrom et al., 2011; Stevens et al., 2006). Interestingly, men are less likely to seek medical attention after a fall and are more likely to reduce activity levels after falling frequently (Sandlund et al., 2017; Stahl S & Albert, 2015), which might put them at a higher risk of future falls and deterioration of functional status. Both men and women view women as more receptive to and in need of fall prevention messaging than men (Sandlund et al., 2017), suggesting that men are less likely to participate in fall prevention programs.
Exercise programs focused on balance, strength, and functional mobility are known to decrease the fall risk in community-dwelling older adults (McLaughlin et al., 2020; Sherrington et al., 2020). The factors that motivate older adults to participate in fall prevention programming are less clear. Previous studies found that women are more likely than men to participate in lectures on fall prevention and fall prevention group exercise programs (Malik et al., 2020; McMahon et al., 2011). A recent study found that both men and women had similar knowledge about the risks and serious outcomes related to falling. However, men were more likely to analyze their risks and use knowledge from healthcare providers, whereas women felt they learned about fall risk through their experiences in taking care of others (Patton et al., 2021). Multiple factors facilitate and challenge older adults’ participation in exercise, such as socioeconomic status, cognitive impairment, frailty, motivation, perception of exercise intensity as too low or too high, presence of health conditions or pain, involvement in decision-making, and perception that the programs are both relevant and will improve quality of life (Malik et al., 2020; McMahon et al., 2011; Noonan et al., 2011; Yardley et al., 2006, 2008). The majority of older adults attending fall prevention programs are women; therefore, the understanding of how gender influences challenges and facilitators in fall prevention participation is limited (Sandlund et al., 2017).
This study describes the motivators, experiences, and challenges to participation in a fall prevention program and explores older adults’ perceptions of gender differences in participation experiences, motivators, and challenges.
Methods
Design
This qualitative study utilized thematic content analysis and followed the guidelines for Consolidated Criteria for Reporting Qualitative Research (Tong et al., 2007). Ethical approval for this study was obtained from the University of Saskatchewan Biomedical Ethical Review Board (Bio 16-238). The trial protocol was registered at ClinicalTrials.gov ID NCT04988334. Participants aged 60 years and older who were community-dwelling and able to ambulate independently were recruited to participate in a prospective cohort study involving 12 weeks of a control period followed by 12 weeks of a fall prevention intervention program. This study was part of a larger intervention study that evaluated the functional and fall injury risk outcomes in older men and women.
The recruitment methods included newspaper advertisements, community organization email distributions, and flyers posted within the community. Recruitment efforts focused on achieving an equal balance between men and women. After the initial recruitment resulted in an approximately 4:1 female to male ratio, the recruitment strategy was modified to attempt to increase participation interest in men. Revised advertising focused on the recruitment of older adults for a balance and strengthening exercise program instead of a fall prevention program. This modified marketing strategy helped generate a gender ratio sample size closer to 1:1. Community-dwelling adults aged 60 years or older were included in this study. Participants were excluded if they had recent injuries or fractures or medical conditions that might jeopardize their safety when participating, signs of significant cognitive impairment, or an inability to safely and independently ambulate (with or without a walking aid) in the community. A medical and demographic screening questionnaire, as well as the Mini-Cog (Borson et al., 2000), were used to determine eligibility.
All participants completing the program (n = 65) were invited to participate in the focus groups and were self-selected into either men or women. Separated men’s and women’s focus groups were used to directly discuss gender differences and avoid any hesitancy to voice these differences if another gender was present. The total was five focus groups, three for women and two for men, ranging in group size from four to ten members. The focus groups were held in a private meeting room at the same community site where the exercise program was conducted. The individual facilitating the focus groups was an experienced, trained Qualitative Research Manager/Specialist with a Bachelor of Arts degree and was external to the research team. This approach was used to avoid any influence and discourage conversation with one of the researchers present and who was involved in aspects of testing and intervention management. The focus group facilitator was identified as a woman. At the start of each focus group, she provided a brief introduction of her background, experience, and role, indicating no bias or assumptions. She had no previous relationships with the participants. Field notes were taken during the focus group discussions and were used to cross-reference responses during transcription. The notes were shared with the research team at the end of the group discussion.
A semi-structured discussion guide (Appendix 1) was developed by the principal investigator of the study (CA). Minor modifications were made following consultation with other research team members, including three older adults living in the community who were engaged in the research project as patient-family partners (CIHR, 2019). The duration of each focus group discussion was approximately one hour. All focus group discussions were recorded using an audio recorder (Olympus WS-803, Toronto, Ontario, Canada) located centrally in the room after participants provided consent. The data were transcribed by someone not directly involved in the study, who was under the supervision of the focus group facilitator. This transcription service utilized an experienced and trained transcriber who worked for the same qualitative research methodology organization to facilitate the focus groups. After the transcription was completed, a research assistant (DB) sent de-identified transcripts via email to all group participants to verify the accuracy. Participants had two weeks to send recommendations for correction, and the final transcripts were adjusted accordingly.
Intervention
The intervention was designed and administered by two physical therapists with extensive experience in fall prevention for older adults. Additional staff assisted with leading and supervising the 12-week program. Two 12-week program cohorts were included in the recruitment of the focus groups. The intervention was conducted in a community at a recreational facility with a room for walking and mobility. The participants then transported themselves to the site. The focus of the intervention was to improve the modifiable factors to reduce fall risk and the risk of related injuries, including strength, functional mobility, and gait and balance practice. Details of the intervention are described elsewhere (Arnold et al., 2017). In addition to the 45-minute, twice-a-week exercise session, the participants attended a half-hour fall prevention education session once a week. The topics with invited guest speakers included an overview of fall risk factors, balance strategies, medications, vision, bone health, environmental aids, safety planning, vestibular dysfunction, blood pressure hypotension and dizziness, emotional impact of falls, and mobility aids. The participants received a hardcopy handout of exercises that they could practice at home, with accompanying information related to the educational sessions.
The overall goals of the program were to decrease fall risk and increase fall-arrest capacity or neuromuscular ability to prevent or minimize injury during a fall. The program included a combination of general strength, balance, and functional activities and a focus on upper body strengthening, speed of arm motion, and learning a strategy to land and control a forward fall. The participants recorded their attendance by checking off an attendance sheet in each class, and attendance was tabulated as a percentage throughout the 12 weeks.
Analysis
Content analysis was used to determine common themes emerging from the focus group discussions. Several strategies were used to ensure trustworthiness and credibility (Nowell et al., 2017): transcripts were sent to the participants to verify accuracy were coded multiple times, team consensus discussions were held, and participants’ quotes were verbatim. To ensure interpretive validity, both open-ended and probing questions (refer to Appendix 1) were used during the focus group discussions to clarify the participants’ responses and obtain greater depth and accuracy regarding their experiences. All the group participants were given the opportunity to contribute during the group discussions, and the facilitator kept notes on any concerns or irregularities.
The transcripts were analyzed by two teams: a primary and a secondary analysis team. The primary analysis team consisted of a research assistant (DB), researcher (CA), three older adults living in the community, and members of the research team as patient-family partners. The role of the patient-family partner was to contribute to the development of the semi-structured discussion guide, participate in the focus groups as an observer, and provide input for transcript thematic coding. The secondary analysis team consisted of five student researchers. All members of the analysis teams familiarized themselves with the transcript data by reading, reflecting, and discussing them during a six- to nine-month period. The researcher, research assistant, and five student researchers received training in thematic coding and the use of NVivo software (three-hour training session with ongoing consultation from a qualitative research methodology support organization).
The five group transcripts were first thematically analyzed by the primary analysis team. The hardcopy transcripts were first read independently by each primary analysis team member, who identified common themes categorized into each of the main questions asked in the discussion guide (Appendix 1). The primary analysis team then met on two occasions at a central community meeting site to reach a consensus on the themes. Common themes emerging from the independent reviews across all five transcripts were discussed, as were emerging themes specific to the targeted question regarding perceived gender differences in fall prevention participation and motivation. To optimize researcher triangulation, a secondary analysis team of five student researchers word counted, coded, and themed the transcripts using NVIvo 11 software (NVIvo 11, QSR International, Doncaster, Victoria) following the same discussion coding guide previously described without knowledge of the primary team’s hardcopy coding. The secondary team inductively coded together during several team meetings to determine the consensus of the emerging themes, in consultation with the researcher (CA). The researcher reviewed both analyses and identified consistency in theming and a final merging of the thematic analysis with consensus from the primary analysis team. Inductive thematic saturation (Saunders et al., 2018) was considered to have been met because no new codes or themes emerged after the secondary team reviewed and analyzed the transcripts.
Results
Thirty-four individuals (16 women and 18 men) participated in one of the five focus groups (three women and two men). A comparison of the demographic information, fall history, and attendance between men and women is shown in Table 1. An independent sample t-test showed no significant differences between men and women in age, number of prescription medications, or program attendance rates (86% and 90%, respectively; p > .05).
Comparison of descriptive variables for men (n = 18) and women (n = 16) participants.
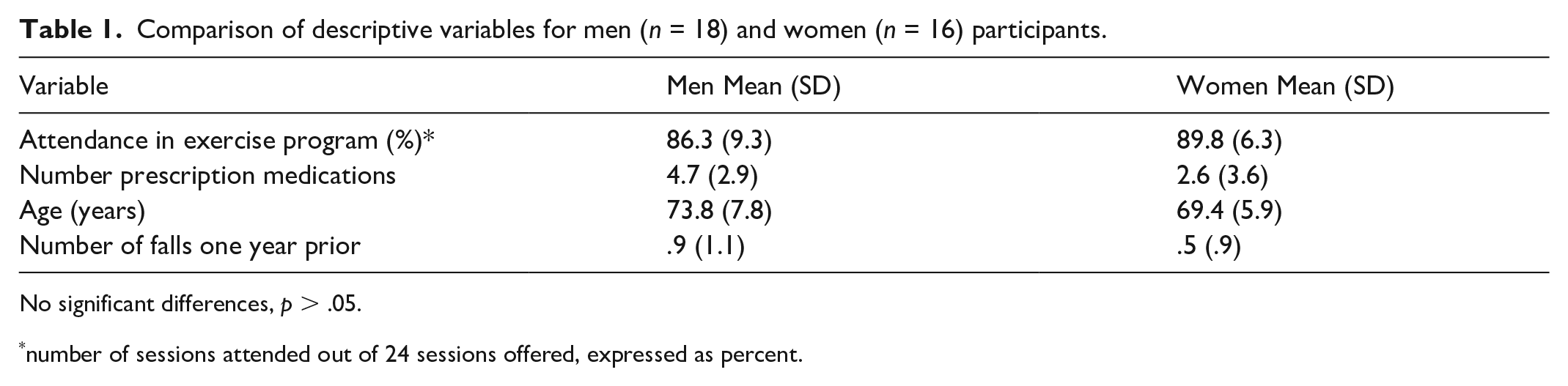
No significant differences, p > .05.
number of sessions attended out of 24 sessions offered, expressed as percent.
Six main themes emerged: Personal experience as a motivator, Get my balance back, Socialization, Being part of something bigger, Successes/Challenges (Continuing on after the program), and It might be a macho thing. It might be a macho thing represented a cross-cutting descriptor across themes regarding why men might not participate in fall prevention programs to the same extent that women do. It might be a macho thing interconnected with Socialization and Being part of something bigger were related to men participating and seeing benefits from self-motivational factors and personal gain in a research setting, whereas women tended to have the view of a collective group outcome and socialization. Both men and women noted personal experiences and balance as reasons for their participation. Structure and Leadership and Incorporating exercise into daily living emerged as sub-themes for Successes/Challenges. Figure 1 shows a visual representation of the six themes and two sub-themes.
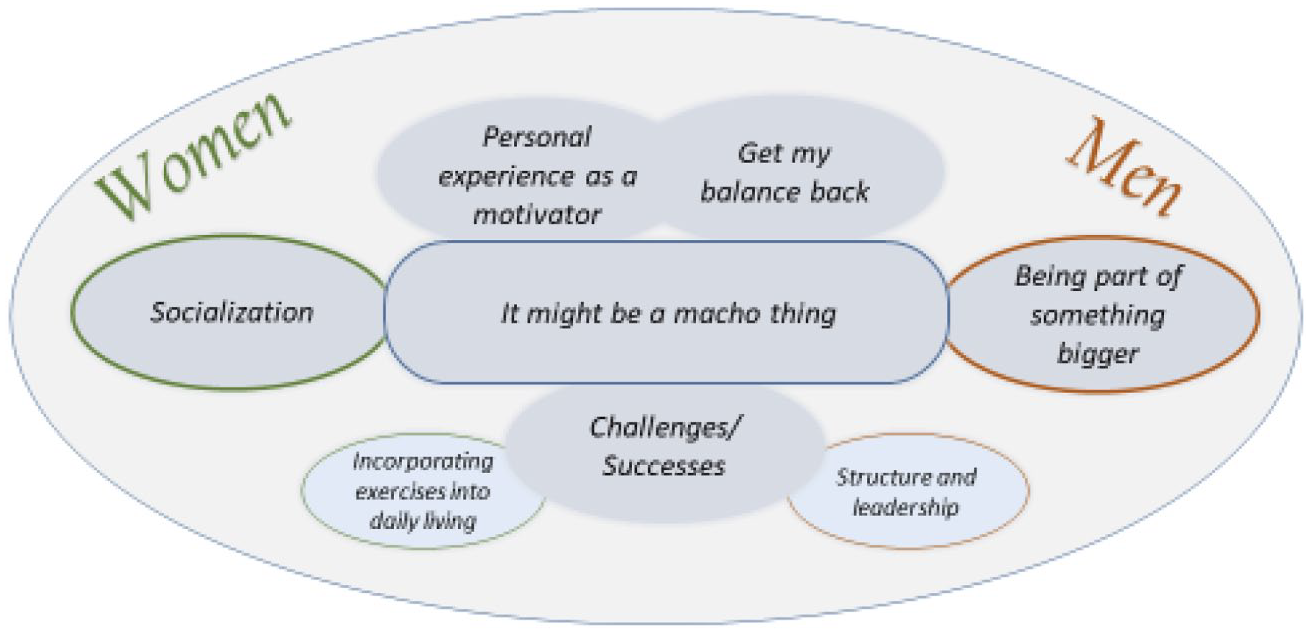
Visual Representation of Six Main Themes and Two Sub-themes.
Theme 1: Personal experience as a motivator
This theme emerged in both gender focus groups and was related to personal experiences that impacted their decisions to seek fall prevention programming. The subsequent quotes illustrate the participants’ unique underlying motivations for wanting to enroll in a fall prevention program. Experiences of a previous fall or loss of balance were common and were reported to trigger motivation and interest in participation.
“What got me interested when I saw it in the paper was the number of people living in our units that fall and don’t come back. So, they either go to long-term care or they don’t survive. I thought, this is something important to get looked after. That’s why I am here.” (P9.1 woman) “I came because I was tipping over just putting my underwear on in the morning and I thought, “Wow! I got to fix this.” (P4.1 woman) “Suddenly I didn’t have the balance. I found I couldn’t skate anymore. I had to pack it up and that’s why I thought this might be a good place to try and get some of that back again and be able to carry on with it.” (P3.2 man) “All of a sudden, I find myself on the ground [. . .] Cracked some ribs and so on. I was suffering in pain and dizziness as I rested there. [. . .] That’s why I came into the classes.” (P3.2 man)
Theme 2: Get my balance back
This second theme was consistent across both gender focus groups and included both reasons for participating and experiences from being in the program. This theme has some crossover related to personal experiences as a motivator (previous experiences of falls and balance loss), but the coding revealed that balance was addressed frequently and consistently as a reason and an outcome experienced across all focus groups by both men and women. Thus, balance was identified as an independent theme.
“I think I have more confidence to walk in the wintertime.” (P 2.2 woman)
“I think that I have really improved my balance.” (P 5.1 woman)
“I have a problem with my balance. Apparently, I have very bad memory I guess. I don’t remember falling but my daughter says, “Dad you fall lots of times.” (P 2.1 man)
“I’m starting to trip over that age where my balance is definitely being lost.” (P 4.1 man)
Theme 3: Socialization
This theme was gender-specific to women. Women tended to report the “fun” aspect of the program, meet people, and connect outside the program. Both men and women spoke of socialization as a reason that women participate in fall prevention but not as a reason for men to seek group fall prevention opportunities. This finding also reflects the gender cross-cutting theme, “It may be a macho thing,” indicating that men are less likely to acknowledge the need for or seek out socialization group exercise experiences. For women, socialization was both a reason for participating and a positive outcome of being involved in the program.
“[. . .] our group stays and has coffee together afterwards. We’ve discovered that that’s really important.” (P 6.3 woman)
“I like to be social. So, I thought it would be a good way to meet more people and have some fun, and do some exercises. I found less stress because I knew I was coming here, and if things weren’t going right or something, or if I was having a bad day [. . .]. Then I thought, “Oh, but I am going to the exercise program today. I do not even have to think about it.” (P 10.1 woman)
“Do you think it’s a psychological thing; perhaps women are more likely to join groups?” (P4.1 man)
“Perhaps women are more open to doing things with other people and with other women, too, with other people. [. . .] an exercise class, that seems more of a woman thing to do. I do not know. I have never done a group exercise before, so maybe.” (P 10.1 man)
Theme 4: Being part of something bigger
This theme was specific to men as a motivator for participation and a positive outcome, with comments supporting this theme observed in both gender focus groups. The theme has interconnecting components to Theme 6 and might speak to some of the reasons men are attracted to a specific type of research-based programming versus general community fall prevention programming. Men might tend to seek out programming with a goal to “see results.” This theme also addressed a common theme for men who indicated a personal reason for participating because of life changes, such as retirement, no longer working, not being active in sports or other recreational activities, and the importance of personal accomplishment. Being part of something bigger reflected both a motivation to contribute to research based on group findings and personal motivation to see quantitative changes after the program.
“He’s not lazy, but if it’s not related to getting something accomplished, he’s not that interested.” (P 4.1 woman)
“I’m very research focused and interested in supporting research. When I turned 60 a couple of years ago I stopped doing a lot of sports that I did most of my life. I just thought that if I can continue on with an exercise program that’s somewhat structured, learn a little bit more about a factor that’s going to possibly be affecting me as I get older.” (P 9.2 man)
“The idea of the combination of the study and something to benefit personally was appealing.” (P5.2 man)
“I’m looking forward to the test because I would like to know what the difference in improvement has been.” (P 5.1 man)
Theme 5: Successes/Challenges (Continuing on after the program)
The analysis revealed two emerging sub-themes for this main theme: 1) Incorporating exercises into daily living and 2) Structure and leadership. Incorporating exercise into daily living was encouraged and stressed throughout the program. Both men and women noted both challenges and facilitators as being able to transition from what was taught during the program to the home environment. Women tended to comment more often on the challenges and facilitators to incorporating exercise into a home routine but also noted ways that they attempted to do so. Women seemed to appreciate the connection of the program to daily living that was stressed as part of the programming. In contrast, men more often noted the importance of structure and leadership as motivators to continue exercising.
“There’s so much other stuff – housework – to do. I think, ‘I have to do this first.’ Then I never get to it.” (P 7.1 woman)
“I would justify not specifically doing them by using them in everyday things. I’m in front of my sink always – cleaning veggies or whatever. The whole time, I did it on one leg and with really good posture.” (P 4.1 woman)
“The thing is, then, if I rest a day, you get in the habit of missing an exercise then all of the sudden you’re missing more and more. I am afraid of this sloping off.” (P 6.1 man)
“I recognize I’m one, somebody that needs- doing this Tuesday and Thursday. I need that kind of structure.” (P 6.2 man)
“They could be stern with us when they had to, but incredibly supportive and knew what they were talking about, and made us all feel like we were a team.” (P 8.1 man)
Theme 6: It might be a macho thing
This central theme represented the perceived gender differences in the challenges to participation in fall prevention programming, as well as attending to health needs, including falls and related injuries. This overarching theme was consistent across both gender focus groups and was woven into the other themes, representing a perception that men are reluctant to participate and have other reasons for seeking fall prevention support than women do. Both men and women noted gender differences in self-awareness and seeking support to address health concerns, including fall risk. The perception was that men were less likely to identify, discuss, or seek interventions for fall risk because of a social stigma of “macho” behaviors or attitudes. This theme helps with understanding gender differences in participation in group exercises and education programs.
“I really do think it’s the macho thing more than anything else that keeps men out of these sorts of classes.” (P 4.2 man)
“Maybe it is just a macho thing, I do not know. It is a lot when you hear somebody, “Yeah, I have been having these pains for a couple of days now.” Why did you not go to the hospital and see a doctor?” (P 6.1 man)
“The men will stuff it and suppress it, and would rather talk about last night’s game and that sort of thing. There are dramatic differences.” (P 5.1 man)
“Some probably seem to have it in their heads. They will not go and do yoga, they won’t go and do swimming, or they won’t do. . . Somehow, that is a feminine thing to do.” (P 10.1 woman)
Discussion
The purpose of this study was to identify participation motivators, experiences, and challenges in a fall prevention program and explore older adults’ perceptions of gender differences. We found that similarities and differences exist between women and men in their reasons for participating, experiences in the program, and challenges and facilitators of participation and continuing exercise.
Both men and women agreed that the primary reason to seek out fall prevention intervention and enroll in the study was their personal experience. The primary personal reasons motivating involvement included the realization of balance loss or the experience of a fall. This has been highlighted in a review of 19 qualitative and quantitative studies (McMahon et al., 2011) of older adults’ perspectives (majority women) on fall risk and prevention programs, for which personal relevance was a strong attractor to participation in fall prevention interventions. However, personal relevance could also act as a deterrent if the intervention was deemed irrelevant or practical for addressing personal needs (McMahon et al., 2011). In a recent review of older adults’ preferences for fall prevention exercise programming, perceived benefits was also noted as a commonly occurring theme (Sandlund et al., 2017), and more frequent near falls was associated with participation in balance classes (Currie et al., 2020). In contrast, denial of fall risk, not wanting to be defined as a “faller,” or the perception that fall prevention is not necessary can also act as barriers to participation (McMahon et al., 2011).
Understanding the motivational factors that differ between men and women is important to encourage men to participate in fall prevention programs. A previous study that sampled 12 fall prevention programs found that approximately 80% of the participants were women (Malik et al., 2020). The initial recruitment experience for this study had a similar gender disparity, with the majority of participants being women. We had to modify our advertising at the midpoint to target marketing for men. We found that changing the wording to seek participants interested in a “Balance and Strengthening” program instead of a “Fall Prevention” program generated more male participation. This finding is important in advancing fall prevention programming to ensure that programs appeal to both older men and women in the community and to carefully consider how the words used in advertising can positively or negatively influence participation.
The participants (both men and women) overwhelmingly agreed that men have a persona of “macho” thinking that might influence their reluctance to engage in fall prevention programming. However, the underlying reasons for this reluctance remain unclear. Women might be perceived as being more at risk. Alternatively, perhaps the generally higher attendance of women in fall prevention education and exercises further enhances the image that fall prevention programs are for “women, not men.” Men might require more targeted and different marketing strategies to draw them into fall prevention programming. In this study, once engaged in the program, the men attended just as regularly and realized similar positive outcomes. Perhaps focusing on the marketing and design of fall prevention to clearly address the outcomes of balance and strength, with exercises designed to be practical and address personal needs, would help attract both men and women.
Men and women voiced similar positive experiences after completing the program and saw improvements in balance and confidence in movement. They also recognized similar challenges in continuing with exercise after the program was completed and in attempting to fit exercise into their daily lives. Men more frequently noted the need for structure and leadership as a positive influence on their motivation to exercise. This finding is supported in previous research in which gender difference themes for perceptions about preventing falls are included: Men are Analyzing Risks and Modifying Behaviors and Women are Caregivers (Patton et al., 2021). Men tend to seek more information from healthcare providers and utilize it in their risk analysis, whereas women voiced more self-efficacy and learning from experiences (Patton et al., 2021). In this study, men emphasized the relevance and importance of the healthcare provider leader and observing positive personal outcomes. In contrast, women more frequently noted the positive component of socialization as a result of involvement in a group program.
The participants in this study were community-dwelling older adults, independent of daily living, with a mean age of approximately 70 years. Other studies found that older adults with lower socioeconomic status, older age, and history of a recent fall prefer home-based exercise programs over group exercise programs (Yardley, 2008). We found that the socialization component and the structure and leadership offered in the group-based exercise program appealed to this participant pool who faced challenges in continuing the exercises at home. Careful consideration of the demographic and personal differences that attract individuals to group or home programming is important in designing and implementing different options.
The strength of this study is the contribution from both men and women to the perceptions of gender differences in fall prevention programming. One limitation of this study was that all of the focus group participants were involved in fall prevention programming, and thus, might represent a bias of perspectives. Another potential limitation was that the focus groups were gender-specific. Gender-specific groups were purposefully chosen to provide an environment to express perceptions without the influence of the other gender, particularly because several participants had spouses involved in the program. However, the limitation of this approach was that discussions with men and women might have provided further context and sharing, resulting in a deeper understanding of the similarities and differences. Additionally, group setting discussions can sometimes detract from understanding individual perspectives. However, focus groups present a more natural social atmosphere that can enrich data and stimulate further dialog on and understanding of a topic (Baillie, 2019). The participant pool was also a relatively homogenous group. All of them completed the program, were functionally able to transport themselves to the site, and were motivated to be involved in an intervention study. Future studies should extend the reach to explore gender differences in more marginalized populations, with higher fall risk, and older age groups.
Conclusion
Little information exists regarding gender differences in the motivational factors that encourage older adults to participate in fall prevention programming. It might be a macho thing summarizes a theme that might explain why men are less likely to see the need to attend fall prevention programming and the belief of both genders that women are more in need of fall prevention programming. The findings from this study can help address challenges in participation and motivation for older adult participation and guide decisions for designing group fall prevention programs in communities. Understanding the facilitators and barriers to participation will help improve efforts to reduce falls and improve the quality of life of older adults.
Supplemental Material
sj-docx-1-jag-10.1177_07334648221095623 – Supplemental material for Is it a Macho Thing? Older Adults’ Perceptions of Gender Differences inFall Prevention Class Participation
Supplemental material, sj-docx-1-jag-10.1177_07334648221095623 for Is it a Macho Thing? Older Adults’ Perceptions of Gender Differences inFall Prevention Class Participation by Catherine Arnold, Joel Lanovaz and Danelle Banman in Journal of Applied Gerontology
Footnotes
Acknowledgements
The authors would like to acknowledge the following students who assisted with transcript coding: Kennedy Graff, Melissa Doerksen, Natasha Patterson, Stephen Hutton, and Chad Magee. The authors would also like to acknowledge the contributions of Janet Barnes, Margareth Peterson and Howard Giles for their support and guidance in the planning of the focus group discussions and their contributions to determining the final themes. Finally, we would like to acknowledge the Canadian Hub for Applied and Social Research at the University of Saskatchewan, particularly Rachel Tang, for methodology support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Saskatchewan Health Research Foundation (SHRF) and the Saskatchewan Centre for Patient-Oriented Research (SCPOR).
Ethical Approval
The study was approved by the University of Saskatchewan Biomedical Ethics Review Board (Bi0 16-238).
Intervention Clinical Trial Registration
BLINDED
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.