
Abstract
This study aimed to develop a measurement instrument of frailty experiences, the Frailty Experiences Scale, in community-dwelling older adults and test its psychometric properties. The process involved three steps: expert sessions (n = 10) to assess face and content validity; think-aloud interviews (n = 5) with older adults > 60 years to check feasibility and comprehensibility; and testing the scale (N = 187) among older adults (71.9 ± 7.8; 65% female; 70.4% highly educated) to assess internal consistency and structure. The layout and instructions facilitated easy administration. Factor analysis confirmed the four-dimension structure (physical, psychological, social, and cognitive) and showed good reliability (Cronbach’s alpha = .872). Items six, nine, and 16 were removed due to poor contribution, low or negative factor loadings. The cognitive subscale contributed the least. The Frailty Experiences Scale is a feasible and reliable instrument for measuring experienced frailty in older adults, with promising implications for research and practice.
• The Frailty Experiences Scale differs from existing frailty (screening) instruments by incorporating and emphasizing personal experiences and can complement current instruments
• This study provides evidence for a reliable and valid instrument to assess experienced frailty in community-dwelling older adults
• The findings raise opportunities to implement the Frailty Experiences Scale in daily practice in care for older adults
• Implementing the Frailty Experiences Scale opens opportunities for meaningful dialogs between older adults and their formal and informal caregivers about their frailty experiences and priorities
Introduction
Aging populations poses challenges for governments and healthcare systems to adapt to the increasing number of people with a wide range of functional abilities. Developing and maintaining these functional abilities depends on individuals’ intrinsic capacity (IC), someone’s physical and social environment and the interaction between the two (United Nations Department of Economic and Social Affairs, 2023). Intrinsic capacity is known as the composite of all the physical and mental capacities of an individual (Beard et al., 2016). Intrinsic capacity reveal similarities with the concept of frailty, however, is seen as a distinct construct (Belloni & Cesari, 2019). Frailty is widely and increasingly used to describe individuals at increased risk of adverse health outcomes (Clegg et al., 2013). Frail older adults experience losses in one or multiple domains of human functioning such as physical, psychological, or social (Gobbens, Luijkx et al., 2010). Both concepts, intrinsic capacity and frailty, are stemming from the need to overcome traditional medical paradigms (Belloni & Cesari, 2019). Intrinsic capacity helps reduce the stigma surrounding frailty by shifting attention from decline and dependency to remaining functional abilities. The two concepts differ in their focus and are assessed using distinct methods. Intrinsic capacity is determined by longitudinal assessment to inform public health strategies and frailty by cross-sectional assessment to detect and address the individual clinical needs of older adults (Belloni & Cesari, 2019). However, how older adults experience frailty and what their personal needs are instead of their clinical needs remain unknown.
Many instruments have been developed to identify frailty and to assess frailty levels in older individuals, such as performance tests, physical examinations, or questionnaires, that focus on one or multiple domains of frailty (Faller et al., 2019; Ruikes et al., 2016; Van Der Vorst et al., 2017). Frailty Assessment instruments can be distinguished into two distinct categories: (1) clinical observant and (2) proxy- or patient reported. In the first category the clinician establish a frailty level by observation and information of the patient files (e.g., the Clinical Frailty Scale (Rockwood et al., 2005) or Edmonton Frail Scale (EFS; Rolfson et al., 2006)). In the second category the patient or proxy is asked to answer questions regarding several elements of frailty such as the Comprehensive Frailty Assessment Instrument (CFAI; De Witte et al., 2013), the Groninger Frailty Indicator (GFI; Steverink et al., 2001); the Tilburg Frailty Indicator (TFI; Gobbens, van Assen et al., 2010), or the Evaluative Frailty Index for Physical Activity (EFIP; De Vries et al., 2013). Neither approach acknowledges the feelings of the patient regarding frailty. In addition, there appears to be an inconsistency between these frailty classifications and the general understanding and experiences of older adults regarding frailty (De Witte et al., 2013; Grenier, 2006; Smetcoren et al., 2018). A distinction referred to as ‘being frail’, indicated by measures on frailty, and ‘feeling frail’, emphasizing the emotional component of everyday experiences of living with frailty (Grenier, 2006). The same distinction was identified in more recent studies indicating a discrepancy between being classified as frail and experiencing frailty (Cluley et al., 2021; R. D. J. Golbach et al., 2025). Moreover, frailty experiences were characterized by temporality, experienced during certain moments in life (e.g., while in the hospital or when ill), in contrast to a more permanent or progressive course of frailty (Ambagtsheer et al., 2019; Cluley et al., 2021; R. D. J. Golbach et al., 2025; Peek et al., 2012; Su et al., 2023). Another distinction between frailty and frailty experiences was found in the origin. Frailty experiences might be triggered by internal (e.g., personal characteristics) or external (e.g., how you are treated by others or by external events such as experiences of loss) factors. Instead the frailty syndrome was characterized by an imbalance in homeostatis after a stressor, caused by a range of variables which might result in diseases or decline in physiological reserves and therefore frailty (Clegg et al., 2013; Gobbens, Luijkx et al., 2010). Although attention is paid to individuals’judgment of their functioning in frailty assessment, for example, by using the proxy- or patient-reported questionnaires, older adults’ experiences of living with frailty and their personal needs remain underreported and therefore also in care and treatment of frail older adults.
Several studies have shown that personal beliefs and previous experiences affect the predisposition to frailty and might drive someone’s actions (Chew-Graham & Ray, 2016; Cremers et al., 2013; de Albuquerque Sousa et al., 2012; Pegorari & Tavares, 2014; Petrie et al., 2007). In addition, subjective health might be a good global indicator of health status (Wu et al., 2013). Despite the complexity of this relationship, experiences, beliefs, and perceptions seem to affect health behavior and evidence has shown that low subjective health is related to negative health outcomes and even mortality (Archibald et al., 2020; Bloem & Stalpers, 2012; Perrig-Chiello et al., 1999). Furthermore, a positive attitude toward aging might reduce the risk of becoming frail (Gale et al., 2017). However, little is known about the relationship between perceptions and feelings toward frailty and health behaviors or outcomes. Besides, frailty in older adults is challenged by stigma and negative associations which might affect their well-being and interactions with professionals negatively (Markle-Reid & Browne, 2003; Pan et al., 2019). Moreover, older adults do not identify as frail and do not use the term to describe themselves (R. D. J. Golbach et al., 2022; Minkler, 1990; Nicholson et al., 2013; Pan et al., 2019; Van Campen, 2011). Therefore, it is especially important to acknowledge older individuals’ feelings and experiences of living with frailty.
Furthermore, societal trends in health care, including a shift toward person-centered or integrated care, by means of shared decision-making (SDM), require the recognition of the personal experiences of individuals facing frailty (Ekman et al., 2011; Pel-Littel et al., 2021). In the Netherlands, older adults are expected to live longer independently and to take control over their health and healthcare (Ministry of Health Welfare and Sport, 2018). With an increase in age, they are more likely to live with multiple chronic conditions, including frailty. To enhance their self-management and self-esteem, aspects considered to be important by the individual should be taken into account. This is consistent with the concept of positive health, which emphasizes an individual’s values (Huber et al., 2016). Focusing on older adults’ perceptions and experiences toward frailty aligns with these societal trends and might improve relationships between care professionals and older adults.
To understand the differences in the conceptualization of frailty (i.e., theoretical or clinical frailty definitions and frailty experiences by older adults), it is essential to consider older adults’ perceptions and experiences. Insights into frailty experiences might help caregivers, such as social- or care professionals (e.g., nurses) or informal caregivers, understand where older adults’ attitudes or behaviors originate. In addition, they can adopt effective communication strategies to support older adults experiencing frailty. Furthermore, understanding frailty experiences can help older adults acknowledge their vulnerabilities and explore what matters most. To obtain and evaluate relevant information on frailty experiences in older adults we aimed to develop the Frailty Experiences Scale (FES) in community-dwelling older adults and test its psychometric properties.
Method
Design
The FES was developed to assess experienced frailty in community-dwelling older adults. The FES was evaluated for face and content validity, feasibility, comprehensibility, reliability, and construct validity by following the steps of measurement development. These steps were: definition of the construct, development of items and response options, and testing (De Vet et al., 2011).
The initial draft of the FES was developed based on theoretical and empirical methods. Items and response scales for the draft FES were determined based on; the findings of a Delphi procedure regarding which terminology to use (R. D. J. Golbach et al., 2022), literature on the multidimensionality of frailty (Gobbens, Luijkx et al., 2010), qualitative analysis (R. D. j. Golbach et al., 2024; R. D. J. Golbach et al., 2025) which resulted in the addition of the cognitive domain and provided content for the items, and existing instruments such as the Research and Development-36 Health Survey (RAND-36; Van der Zee & Sanderman, 2012) and the Experience of Aging Scale (In Dutch: ‘Beleving van het Ouder Worden Schaal’ BOWS; Steverink et al., 1999), which provided insight into response options and item formulation.
The study was approved by the Ethical Advisory Committee of the Hanze University of Applied Sciences (heac.T2024.005). Written or online informed consent was obtained from all participants.
Operationalization
The construct of experienced frailty was operationalized in this study as; a person’s judgment about their feelings of frailty, in physical, psychological, social, and cognitive domains. These experiences may arise from internal (within the person e.g., personality characteristics) or external triggers (e.g., related to contexts or events) and implicate a dynamic state, characterized by temporality. It indicates a relationship between one’s experiences and associated feelings/emotions (R. D. J. Golbach et al., 2025).
Sample
The draft version of the FES was tested among community-dwelling older adults, aged ≥ 60 years. Respondents were recruited via several channels such as network partners of FAITH research (e.g., Denktank 60+, the Alzheimer’s Foundation, or (home)care organizations such as ZuidOostzorg; http://www.faithresearch.nl), senior citizen associations and participation groups, and through the personal networks of the researchers (e.g., via relatives working in senior (home)care), snowball sampling was used to increase the range.
Procedure
The first step involved determining the draft FES’s face and content validity. Experts were consulted throughout multiple sessions. The first two sessions were with the research team (RG, HH, HJ, and EF), and with two end-users (i.e., community-dwelling older adults) respectively. Subsequently, separate sessions were held with experts (n = 4) in frailty research (i.e., Dutch researchers engaged in frailty research). Decisions on adjustments to the draft questionnaire were made by the first two authors and approved by the research team.
The second step was to evaluate the feasibility and comprehensibility of the draft FES, using a think-aloud protocol. First, two pilot interviews were conducted to establish the method. Then, in March 2024, five interviews were held with community-dwelling older adults, using concurrent and retrospective interviewing (Alshammari et al., 2015). Participants were instructed to provide their immediate thoughts while completing the draft questionnaire. In addition, they were asked several questions (based on an interview guide) on the feasibility and comprehensibility of the draft questionnaire (e.g., How do you get to an answer? How do you interpret this item? What events are you thinking of while answering this item? Are any relevant items missing? Why is that question unclear to you?). Additionally, they could revisit questions or add to their previous thoughts upon completing the draft questionnaire. Based on the analysis of the interviews and in agreement with the research team, adjustments were made to the draft questionnaire before testing.
The third step, of testing the FES took place in a larger sample, aimed at 200 older adults (Kyriazos, 2018). Data were collected in April and May 2024. The questionnaire could be completed online (using the survey tool Enalyzer) by following a link or on a paper form. In addition, participants completed the Tilburg Frailty Indicator (TFI), a frailty screening tool (Gobbens, van Assen et al., 2010).
Measurement
The initial draft of the questionnaire consisted of 39 items. Respondents could score each item on a 5-point Likert scale (never – rarely – sometimes – often - always). Next to the items on experienced frailty, the following demographics were collected: age, gender, educational level, and native language. After the expert sessions adjustments were made and the draft version, before the think-aloud interviews and testing, consisted of 24 items in four domains: physical, psychological, social, and cognitive. A higher score on the FES indicates less experienced frailty.
In addition, the TFI was administered to determine respondents’ frailty status and expand the demographics with marital status, birth country, monthly income, health status (healthy – not healthy, not unhealthy – unhealthy), and the presence of two diseases or chronic conditions (Gobbens, van Assen et al., 2010).
Data-analysis
Data from the various steps (i.e., expert sessions, think-aloud interviews, and testing) were analyzed as follows: first, the output of the expert sessions was summarized on paper, and adjustments to the draft version of the FES were made in collaboration with the research team. Second, the think-aloud interviews were audio-recorded and transcribed verbatim. The interview data were analyzed in Atlas.ti 24. A codebook was developed based on the interview guide. Implications from the data analysis resulted in adjustments to the draft FES, which were made in collaboration between the first two authors.
Third, data from the testing were analyzed in IBM SPSS statistics version 28.0.0.1 and R 4.4.0 (R Core Team, 2021) running RStudio. Data were inspected for missing values and, if necessary, replaced with the nearest integer to the mean. Before the analysis, seven items, 3, 5, 6, 9, 11, 16, and 22, were recoded from negative to positive. Subsequently, to determine the construct validity of the FES a confirmatory factor analysis was performed. A confirmatory factor analysis (CFA) was conducted using robust maximum likelihood estimation (MLM) with Satorra–Bentler scaled X2 and robust standard errors to account for non-normality (Rosseel, 2012), testing whether the data fit the hypothesized four-factor structure of frailty: physical, psychological, social, and cognitive. Robust estimation was used because non-normality was observed. To evaluate whether this theoretical model fits the data, several types of fit indices were computed. Cut-off values were determined to enhance the interpretation of each index: CFI (Comparative Fit Index) > 0.95 is considered good (Hu & Bentler, 1999), RMSEA (Root Mean Square Error of Approximation) is considered a good fit with values < 0.05 and an adequate fit with values < 0.08 (MacCallum et al., 1996), and SRMR is considered a good fit if ≤0.08 (Hu & Bentler, 1999). Internal consistency of the overall FES scale and the subscales were analyzed using Cronbach’s alpha of which values of >.7 are considered good (Cohen, 1988; Nunnally & Bernstein, 1978). In this study, only the statistically significant factor loadings were interpreted when these were substantial in the sense of being larger than 0.32 (Tabachnick & Fidell, 2007). The level of significance was set at .05.
In addition, the relation between, the overall and the subdomains of, the TFI and the FES was investigated by correlation coefficients (Pearson correlation) to assess its construct validity. These subdomain constructs were expected to correlate > 0.50, which is considered large (Cohen, 1988) because they assessed different yet similar (i.e., frailty vs. experienced frailty) constructs.
Respondents’ characteristics were described by the frequencies of the demographic data for example, age, sex, and marital status. In addition, the overall scores on the TFI were calculated, a total score ≥ 5 indicated the presence of frailty (Gobbens, van Assen et al., 2010).
Results
Face and Content Validity
The expert session with the research group led to a reduction of 14 items from the original 39. Overlapping items were deleted, several items were rearranged, and small adjustments were made in the phrasing of the items. This resulted in 25 items. The second session, with end-users, resulted in two additional items in the social dimension and a change in the formulation of several items. The sessions, with experts engaged in frailty research (N = 4), resulted in the deletion of nine items, the addition of four items, and the rephrasing of seven items. Some adjustments were small (e.g., deletions of one word) others were major (‘I feel good with the social contacts I have’ into ‘I can make and/or keep contact with others’). Finally, 24 items remained, in four dimensions, seven in physical, seven in psychological, seven in social, and three in the cognitive dimension. Consultations with multiple experts confirmed the face and content validity of the draft FES as a result of these different sessions.
Feasibility and Comprehensibility
The five participants of the think-aloud interviews were aged between 63 and 83 years, two were female, four were highly educated, and two participants’ native language was other than Dutch. Three participants were considered frail according to the TFI (score ≥ 5). The findings indicated that draft FES had a clear layout and was easy to read and understand. Moreover, the instructions were easy to follow. In addition, one item was deleted because of its ambiguity (i.e., about hearing and vision loss), and one item, moving outside the home, was added based on participants’ suggestions. It took participants less than 10 minutes to complete the draft questionnaire.
Confirmatory Factor Analysis
The draft FES, of 24 items, was completed by 187 community-dwelling older adults during testing. Two hundred fifteen respondents started the questionnaire, five did not provide consent to use their data, 12 opened the questionnaire but left it blank, four ended the questionnaire after the demographics, and seven did not meet the inclusion criteria of age over 60 years. The demographics of the respondents are presented in Table 1. The sample consisted of 65% females, aged between 60 and 93 years, they were mostly highly educated (N = 131), and 24% were considered frail based on their TFI scores (score ≥ 5).
Characteristics of the Respondents (n = 186).

Total n = 181 due to missing data.
Total n = 180 due to missing data.
≥5 score on the Tilburg Frailty Indicator (TFI).
Of the 187 completed questionnaires, two showed missing data. One respondent missed 17 of 24 items and its data was deleted from further analysis. Another respondent included three missing items, and the data were supplemented by mean substitution (rounded to the nearest integer). Data from 186 respondents were submitted to the CFA.
Two out of the three goodness of fit indexes for the four-factor model met their standards. The RMSEA (=0.062, cut-off < 0.08) showed an adequate fit and the SRMS showed a good fit (=0.076, cut-off ≤ 0.08). The CFI (=0.828, cut-off > 0.95) did not met its standard of good fit.
Table 2 shows item-level descriptive properties, including response distributions, floor and ceiling effects, skewness, and kurtosis for the newly developed measure.
Descriptive Item Properties of the Frailty Experiences Scale (FES).

Note. NA = not available.
Indicates a significant deviation from normality (p < .05).
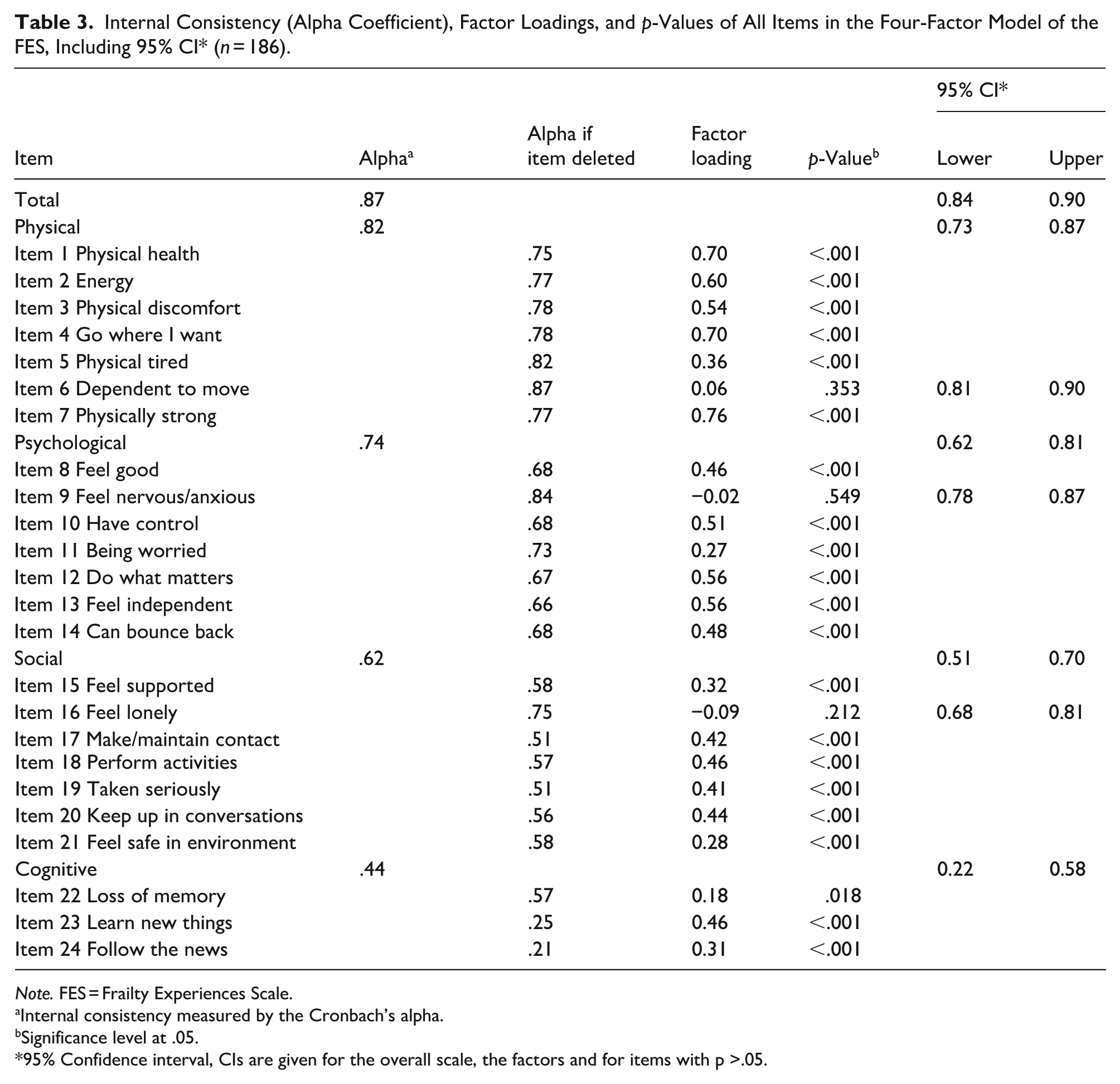
Table 3 shows the factor loadings and p-values of the four-factor model of the FES and the internal consistencies. In addition, Figure 1 shows the confirmatory four-factor model of the FES with factor loadings, correlations between factors, and robust standard errors. The factor loadings vary between −0.092 to 0.757 and range from excellent (>0.70) and good (0.63) to fair (0.45) and poor (<0.32; Tabachnick & Fidell, 2007). Items with poor factor loadings (<0.32), that is, items 6, 9, 11, 15, 16, 21, 22, and 24 were reconsidered. Items 6, 9, and 16 seemed problematic, with low or negative factor loadings. Items 11, 15, 21, 22, and 24 explained little of the variance but contributed positively to the factor. All p-values were <0.05, except for items 6, 9, and 16 (Table 3).
Internal Consistency (Alpha Coefficient), Factor Loadings, and p-Values of All Items in the Four-Factor Model of the FES, Including 95% CI* (n = 186).
Note. FES = Frailty Experiences Scale.
Internal consistency measured by the Cronbach’s alpha.
Significance level at .05.
95% Confidence interval, CIs are given for the overall scale, the factors and for items with p >.05.

Four-factor model of the Frailty Experiences Scale with factor loadings, correlations between the factors, and robust standard errors (N = 186).
Large correlations (>0.5; Cohen, 1988) were found between the factors: physical − psychological = 0.82, physical − social = 0.53, psychological − social = 0.75, psychological − cognitive = 0.67, and social − cognitive = 0.71, except for the correlation between physical and cognitive, this was = .46. However, 0.46 indicates a moderate correlation between the two factors (Cohen, 1988; Tabachnick & Fidell, 2007). The overall internal consistency by Cronbach’s Alpha of the FES was .872, which indicated a good internal consistency of the overall scale (Cohen, 1988).
Physical
The factor loadings of the physical factor were all significant except for item six (I am independent of help from others and/or aids to move outside my home). In addition, item six showed a low factor loading of 0.061. After the deletion of item six, the scale’s internal consistency by Cronbach’s alpha increased from .817 to .866 (Table 3).
Psychological
The factor loadings of the psychological factor were all significant except for item nine (I feel nervous anxious). In addition, item nine showed a negative and low factor loading of −0.049.
After the deletion of item nine, the scale’s internal consistency by Cronbach’s alpha increased from .740 to .836 (Table 3).
Social
The factor loadings of the social factor were all significant except for item 16 (I feel lonely). In addition, item 16 showed a negative and low factor loading of −0.092. After the deletion of item 16, the scale’s internal consistency by Cronbach’s alpha increased from .623 to .751 (Table 3).
Considering the size and significance of the factor loadings, Cronbach’s alpha’s, and their content (e.g., overlapping with other items in the scale) it was decided to delete items six, nine, and 16 from the draft questionnaire. After the deletion of items 6, 9, and 16 the internal consistency of the subscales physical, psychological, and social was considered good (>0.70; Cohen, 1988).
Cognitive
The cognitive factor consisted of three items and the internal consistency by Cronbach’s alpha of the factor seemed moderate (=.435). Item 22 showed a low factor loading of 0.175 but was significant (p = .018, <.05). In addition, item 22 contributed positively to the factor. Considering the content of item 22 (I experience memory loss) and the rationale to incorporate the item into the cognitive domain it was decided to retain item 22.
The correlations of the subscales were presented (Table 3) including their 95% confidence intervals and the internal consistency of the adjusted scales after the deletion of items 6, 9, and 16.
Relation Between the TFI and the FES
Table 4 presents the correlation coefficients (Pearson correlation) between the FES and the TFI as well as between their domains. The correlation coefficient of the total scales was −.725, which indicated a strong correlation between the two scales (Cohen, 1988). The correlation of subscales varied between −.335 and −.730 indicating weak to strong correlations (Cohen, 1988). All correlations were significant (p < .05).
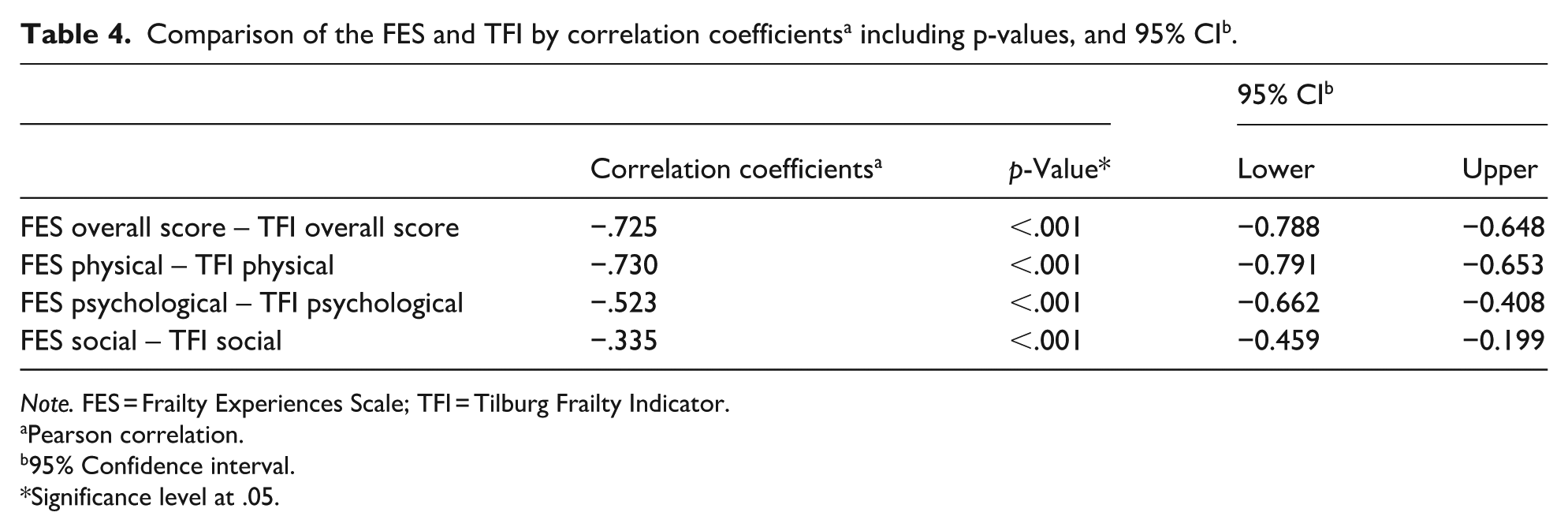
Note. FES = Frailty Experiences Scale; TFI = Tilburg Frailty Indicator.
Pearson correlation.
95% Confidence interval.
Significance level at .05.
Discussion
This study aimed to develop the Frailty Experiences Scale (FES) and test its psychometric properties. The FES is a unique self-reported questionnaire designed to assess experienced frailty in older adults across four domains: physical, psychological, social, and cognition. The FES seemed a comprehensible and user-friendly instrument to assess experienced frailty in community-dwelling older adults. The proposed four-factor model was confirmed. The construct validity and reliability were evaluated and considered good for three domains of experienced frailty: physical, psychological, and social. The cognitive domain contributed the least and should be adjusted. The FES showed sufficient to good internal consistency within the subscales and overall. The newly developed FES offers promising opportunities for implementation in research and practice.
This study provides evidence for a valid and reliable measure of experienced frailty in at least three domains; physical, psychological, and social. It is suggested to remove three items, items 6, 9, and 16, to increase the internal consistency of the subscales. The physical domain seemed the strongest, with the highest factor loadings (0.356–0.757) and internal consistency values, above the cutoff of 0.7 (Cohen, 1988). In addition, the psychological and social domains were sufficient in measuring experienced frailty, with adequate factor loadings (0.280–0.559) and internal consistency scores within the scales (>0.5) and overall (>0.7; Cohen, 1988). All the factors contributed to experienced frailty, which showed the multidimensionality of experienced frailty (Gobbens, Luijkx et al., 2010).
The cognitive domain contributed the least to the overall scale and can be re-evaluated. It consisted of three items with relatively low factor loadings (0.175–0.460) and an overall internal consistency (Cronbach’s alpha of .435) slightly below the cutoff of 0.5 which was considered adequate (Cohen, 1988). The relevance of preserving the cognitive domain for experienced frailty was studied and demonstrated in qualitative research on older adults’ perceptions of frailty (R. D. Golbach et al., 2024). Older adults experienced fear of losing their cognitive abilities, and they mentioned features of dementia, memory loss, or not being able to keep up, which could be accompanied by feelings of extreme anxiety or frightfulness (R. D. Golbach et al., 2024). They described cognitive aspects as important to frailty, which can be confirmed by the recent literature in which cognition was more often perceived as a separate dimension of frailty compared to earlier frailty research (De Roeck et al., 2018; National Institute for Public Health and the Environment, 2016). Therefore, we propose small adjustments to this scale to improve its validity and reliability. The cognitive domain of the FES could be extended by adding items that should closely cover the cognitive aspects of frailty and experienced frailty, for example, items reflecting handling finances or banking, remembering or managing appointments, (in)flexibility to change, or difficulties getting thoughts in line (De Roeck et al., 2018; R. D. J. Golbach et al., 2024; National Institute for Public Health and the Environment, 2016). Further research is required to validate a revised version of the cognitive domain of the FES, to enhance its applicability in research and practice.
The correlation between the FES and the TFI was assessed and confirmed the construct validity. The overall scales were highly correlated (−0.725), indicating the constructs have similarities, however, the TFI only partly explained the variance of the FES. The FES measures a construct quite similar yet distinct from those assessed by frailty (screening) instruments, providing additional value. This becomes more evident when comparing the subscales, which show correlations from weak to strong (−.335 to −.730). The FES includes more extensive scales in the psychological and social domains, with six items each, compared to the TFI, which has four and three items respectively. Additionally, the FES addresses these domains differently in terms of content. Therefore, adding frailty experiences to existing frailty instruments could provide additional information to care professionals, older adults, and informal caregivers.
To the best of our knowledge, the FES is the first instrument to indicate experienced frailty in older adults, emphasizing the importance of incorporating personal experiences into the understanding of frailty. Personal experiences of older adults are not reflected in current definitions or operationalizations of frailty (Gobbens, Luijkx et al., 2010; Markle-Reid & Browne, 2003). Moreover, research showed that older adults’ experiences might differ from frailty classifications or clinical judgments (De Witte et al., 2013; R. D. J. Golbach et al., 2025; Grenier, 2006; Smetcoren et al., 2018). Attention to the personal experiences of older adults enriches the understanding of frailty by going beyond clinical classifications, offering a more holistic view of the individual. This can provide opportunities for professionals and researchers to be sensitive to the large individual differences among older adults (Khalil & Gobbens, 2023). Using the FES might raise opportunities for older adults and their caregivers to start or improve their dialogs into what matters to older adults based on their experiences.
Furthermore, indicating experienced frailty by the FES offers opportunities to comprehend frailty experiences in research and practice. The FES can help to explore what older adults value or consider important, potentially affecting an individual’s coping and adherence to management plans. Moreover, it aligns with care methods, such as person-centered care and positive health (Ekman et al., 2011; Huber et al., 2016), emphasizing attention to an individual’s wishes and desires. Therefore, understanding frailty experiences and what matters to older adults is essential not only for the individuals themselves but also for their caregivers, including both informal caregivers and care professionals, to provide appropriate support.
In addition, the development of the FES raises opportunities to explore the relationship between frailty classifications (‘being frail’) and experienced frailty (‘feeling frail’). A potentially similar distinction was made between actual health status and subjective health (Song & Kong, 2015; Wu et al., 2013). It was shown that self-perceptions were important predictors of survival, mortality, and actual health status (Song & Kong, 2015; Wu et al., 2013). The relationship between experienced frailty and frailty status has not been studied yet, nor has the predictive value of experienced frailty. Developing the FES indicating experienced frailty in older adults presents considerable opportunities for further research on the predictivity of experienced frailty and its relationship with frailty status (based on classifications).
Strengths and Limitations
The current study has various strengths. First, the FES was developed based on theoretical and empirical evidence. Experts and end-users, that is, community-dwelling older adults, were involved during the development enhancing its usability and contributing to the substantiation of the questionnaire. Second, the questionnaire is a short (final version of 21 items, Supplemental File S1), feasible instrument that can and should be completed by older adults themselves. It is an easy-to-administer tool for use in the community. Third, the questionnaire consists of mainly positively formulated questions, in four domains, focusing on individual experiences. Therefore, the FES invites older adults and their caregivers (e.g., professionals and informal caregivers) to look beyond the clinical or stigmatized view of frailty.
In addition, the study has some limitations. First, during data collection, some participants felt tested and were afraid of failing, potentially leading them to respond more positively than they felt. In developing the questionnaire, we aimed to align with older adults’ perceptions and used positive language to avoid pressure. While we may have partially succeeded, it is crucial to recognize this possibility, especially when using the questionnaire in practice. This underscores that a questionnaire should complement, and not replace, live conversations, serving as an additional resource for older individuals and care professionals. Second, the homogeneity of the sample might have affected the results. The respondents were predominantly of Dutch origin, highly educated, and belonged to the highest income category. It is expected that the results from a more diverse sample may slightly differ, as factors, such as financial issues or language barriers, possibly affect experienced frailty.
Implications for Research and Practice
The FES seems a promising instrument to asses experienced frailty and could be added as a subpart of existing frailty instruments (e.g., screening instruments), to ensure the inclusion of older adults’ experiences regarding frailty in frailty assessment. It is recommended to reevaluate the validity and reliability of the FES after expanding the cognitive scale. Suggestions for improvement of the cognitive scale include adding two to four items that specifically reflect the content of experienced frailty on cognitive aspects. Reevaluation could be conducted in larger, more diverse samples, and settings (e.g., hospitals or institutions) to strengthen the evidence for its applicability in practice. In addition, the answers of older adults on the FES might be a starting point for a dialog between older adults and their caregivers (e.g., care professionals or informal caregivers). The information obtained might retrieve input to conversations about what matters to older adults. Professionals or caregivers may use specific communication strategies to discuss the reasons behind certain feelings, or how experiences are handled or dealt with (e.g., coping). The development of the FES presents opportunities to evaluate the connection between frailty classifications and experiences. It would be particularly interesting to investigate the predictive value of the FES for identifying the risk of frailty or adverse outcomes. This could open up possibilities for early prevention or management of frailty.
Conclusion
The Frailty Experiences Scale is a short, feasible, and comprehensible instrument. It shows sufficient to good psychometric properties on reliability and construct validity. The Factor analysis confirmed that the subscales effectively measure the constructs: physical, psychological, and social. The cognitive domain requires adjustment. These findings are promising for implementing the FES in research and practice to improve support for older adults.
Supplemental Material
sj-pdf-1-ggm-10.1177_30495334261420369 – Supplemental material for Development and Testing a Measure of Experienced Frailty for Community-Dwelling Older Adults: The Frailty Experiences Scale (FES)
Supplemental material, sj-pdf-1-ggm-10.1177_30495334261420369 for Development and Testing a Measure of Experienced Frailty for Community-Dwelling Older Adults: The Frailty Experiences Scale (FES) by Rianne D. J. Golbach, Hans J. S. M. Hobbelen, Wim P. Krijnen, Harriët Jager-Wittenaar and Evelyn Finnema in Sage Open Aging
Supplemental Material
sj-pdf-2-ggm-10.1177_30495334261420369 – Supplemental material for Development and Testing a Measure of Experienced Frailty for Community-Dwelling Older Adults: The Frailty Experiences Scale (FES)
Supplemental material, sj-pdf-2-ggm-10.1177_30495334261420369 for Development and Testing a Measure of Experienced Frailty for Community-Dwelling Older Adults: The Frailty Experiences Scale (FES) by Rianne D. J. Golbach, Hans J. S. M. Hobbelen, Wim P. Krijnen, Harriët Jager-Wittenaar and Evelyn Finnema in Sage Open Aging
Footnotes
Acknowledgements
We thank students Mayke Gardebroek and Anne-Karlijn Mos, who were in their final year of Applied Psychology at the Hanze University of Applied Sciences, for their contributions during the data collection and analysis. In addition, we thank the experts, older adults, and researchers, for sharing their expertise and collaboration in determining the face and content validity of the questionnaire. Finally, we would like to thank all respondents who took the time to complete the questionnaire or share their thoughts during the interviews.
Ethical Considerations
The study was approved by the Ethical Advisory Committee of the Hanze University of Applied Sciences (heac.T2024.005).
Consent to Participate
Written or online informed consent was obtained from all participants.
Author Contributions
RG, HH, HJ, and EF contributed to the design and implementation of the research. RG, HH, and WK to the analysis of the results and all the authors to the writing of the manuscript.
Funding
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.