
Abstract
Contact with blue spaces appears to benefit older adults’ health and well-being, but evidence on its relationship with frailty is scarce. This cross-sectional study investigated associations between exposure to blue spaces and multidimensional frailty in 189 community-dwelling people aged ≥65 years (Portugal). Measurements included the Tilburg Frailty Indicator, questionnaire regarding exposure, and Geographic Information System data for proximity. Purposeful visits once or twice a month were associated with lower physical frailty, as were visits with pets, engaging in physical activity, and spending 1–2 hours or >2 hours in these environments. Visiting with others was associated with lower social frailty. Incidental exposure—passing by visible blue spaces during daily commutes—was linked to lower total and physical frailty. Walking travel times <20 minutes were associated with lower total, physical, and social frailty, with different distances within this range showing domain-specific associations. Results suggest blue spaces may promote healthy aging.
Demonstrates that both intentional and incidental exposure to blue spaces are linked to lower multidimensional frailty in older adults. Identifies domain-specific associations between blue space exposure and physical and social frailty. Shows that subjective (self-reported) and objective (GIS-based) exposure measures capture distinct exposure–frailty relationships.
Suggests that increasing access and walkability to blue spaces may help reduce frailty in community-dwelling older adults. Highlights the value of social and physical engagement in blue spaces as part of “blue care” strategies for healthy aging. Findings provide a basis for policies and interventions integrating blue spaces into age-friendly planning.What This Paper Adds
Applications of Study Findings
Introduction
The substantial growth of the aged population has brought increasing attention to frailty as a critical public health issue (Clegg et al., 2013; Hoogendijk et al., 2019). Frailty is a geriatric syndrome characterized by an amplified vulnerability to stressors, resulting from significantly diminished physiological reserve across multiple systems and its interplay with life course factors and diseases, which in turn increases the risk of disability, hospitalization, institutionalization, and mortality (Abellan van Kan et al., 2008; Clegg et al., 2013; Fried et al., 2001; Gobbens, Luijkx, et al., 2010; Hoogendijk et al., 2019; Morley et al., 2013; Rockwood & Mitnitski, 2007). It is a dynamic and multidimensional condition, highly prevalent in older populations, but not an inevitable consequence of aging, as there is evidence that modifiable factors can be targeted to prevent its onset or reduce its severity (Apóstolo et al., 2018; Clegg et al., 2013; Hoogendijk et al., 2019; O'Caoimh et al., 2021; Ofori-Asenso et al., 2019; Woolford et al., 2020). Depending on how frailty is operationalized, prevalence estimates range from approximately 12% to 42% among community-dwelling older adults (O'Caoimh et al., 2021; Qiu et al., 2024), and this burden is expected to increase with population aging (Hoogendijk et al., 2019). With this in mind, there is an urgent need to better understand and identify protective elements that can support healthy aging and effectively reduce the health burden associated with frailty, as many of these factors remain poorly defined or underexplored.
An increasing body of evidence confirms that exposure to natural outdoor environments might improve health and well-being in older adults (World Health Organization, 2023). Several studies have focused on the positive effects of green spaces (e.g., forests and parks), particularly in urban settings (Gascon et al., 2015; Ribeiro et al., 2024; Rojas-Rueda et al., 2019; Smith et al., 2021). However, an increasing number of studies, especially over the past decade, have started to investigate the health-related benefits of blue spaces (Britton et al., 2020; Gascon et al., 2017; Georgiou et al., 2021; Grellier et al., 2017; Ribeiro et al., 2024). Blue spaces can be defined as outdoor environments, either natural or artificial, that prominently feature water and are accessible to people either proximally (by being in, on, or near the water) or distally/virtually (through seeing, hearing, or sensing water) (Britton et al., 2020; Grellier et al., 2017). These include bodies of water such as oceans, rivers, and lakes.
Blue spaces provide a wide range of sensory stimuli (visual, auditory, tactile, and thermal) that create immersive experiences, fostering a connection with nature and eliciting profound psychological responses and personal significance (Bell et al., 2015; Wang & Sani, 2024; White et al., 2020, 2021). The distinct characteristics of water, such as the sight of rippling waves, the sound of flowing streams, and the cooling sensation, contribute to a unique sensory experience that promotes relaxation and well-being (Britton et al., 2020; Nutsford et al., 2016; Vaeztavakoli et al., 2018; White et al., 2020). These features evoke a “soft fascination,” an effortless state of attention that facilitates mental restoration, alleviating cognitive fatigue and improving focus (Basu et al., 2018; Jarosz, 2023; Smith et al., 2021; Wang & Sani, 2024). Exposure to water elements can also induce positive emotional responses, reducing physiological stress markers like cortisol and heart rate, further enhancing feelings of tranquility and comfort (Triguero-Mas et al., 2017; Vaeztavakoli et al., 2018; White et al., 2020; Yin et al., 2023). The multisensory appeal and aesthetic qualities of blue spaces amplify these effects, contributing to improved mood and psychological well-being (Dempsey et al., 2018; Georgiou et al., 2021; Ibarra et al., 2017; White et al., 2020). Beyond psychological benefits, blue spaces offer environmental advantages, helping to mitigate urban heat, improve air quality, and reduce exposure to pollutants (Burkart et al., 2016; Georgiou et al., 2021; White et al., 2020). Additionally, there is some evidence that marine aerosols may enhance respiratory health, and that blue spaces are associated with higher levels of solar irradiance, which can promote vitamin D synthesis (White et al., 2020).
Blue spaces also act as natural meeting points, encouraging social activities and engagement, fostering a sense of community and reducing social isolation, which is vital for maintaining psychological resilience and well-being, particularly in older adults (Britton et al., 2020; Georgiou et al., 2021; Nutsford et al., 2016; Wang & Sani, 2024; White et al., 2020). Furthermore, these environments promote physical activities such as walking or swimming which enhances physical health by improving cardiovascular fitness, muscle strength, and mobility (Britton et al., 2020; Gascon et al., 2017; Georgiou et al., 2021; Nutsford et al., 2016; Wang & Sani, 2024). The combined effects of factors such as increased physical activity, strengthened social bonds, reduced stress, and greater psychological restoration make blue spaces valuable resources for promoting health and well-being across various populations, with potential implications for urban planning and public health strategies aimed at improving access to these salutogenic environments (Britton et al., 2020; Gascon et al., 2017; Georgiou et al., 2021; Nutsford et al., 2016; Wang & Sani, 2024).
Despite the increasing recognition of these benefits, most research has focused on general well-being and mental health outcomes, with limited direct examination of blue spaces’ impact on specific health markers such as frailty. Addressing this gap, the aim of this study was to examine the association between exposure to blue spaces and multidimensional frailty among community-dwelling older adults. Specifically, we investigated whether different indicators of exposure to blue spaces (proximity, types of exposure, and characteristics of intentional visits) were associated with total frailty and with its physical, psychological, and social domains.
Methodology
Study Design and Participants
A cross-sectional study was conducted with a non-probabilistic convenience sample of 189 community-dwelling older adults in Northern Portugal. Participants were recruited through seven institutions serving older adults, including retirees’ associations and senior universities, which shared the study proposal with their members. Eligible participants were individuals aged ≥65 years and residing in the community. The sole exclusion criterion was the presence of severe communication deficits that would prevent completion of the questionnaire. Before data collection, which took place via telephone from May to July 2021, participants provided informed consent after receiving detailed information about the study’s objectives, confidentiality assurances, and their right to withdraw at any time without consequences. The study was approved by the E2S, Polytechnic of Porto Ethics Committee (registry number CE0044B).
Measurements
Participants were assessed regarding sociodemographic variables (age, sex, and education) and frailty (total, physical, psychological, and social) using the Portuguese version of the Tilburg Frailty Indicator (TFI) (Coelho et al., 2015; Gobbens, van Assen et al., 2010). The TFI is a valid and reliable measure of frailty (Gobbens & Uchmanowicz, 2021; Metzelthin et al., 2010; Mulasso et al., 2015; Pialoux et al., 2012), divided in two parts: Part A addresses the determinants of frailty such as sociodemographic, life-event, and lifestyle-related information and part B which includes 15 components of frailty distributed across 3 domains: physical (8 items; score range: 0–8), psychological (4 items; score range: 0–4), and social (3 items; score range: 0–3). In the Portuguese validation study (Coelho et al., 2015), the TFI showed good internal consistency for the total score (KR-20 = 0.78) and excellent test–retest reliability (r = 0.91). Higher scores indicate greater frailty and, in the Portuguese version, a total score ≥6 indicates frailty.
Exposure to blue spaces was assessed using both subjective and objective indicators. Subjective exposure was assessed through a questionnaire focusing on participants’ perceived proximity, frequency and duration of visits, social context, and type of interaction with blue spaces. Objective exposure was assessed using Geographic Information System (GIS)-based measurements to quantify residential proximity and surrounding environmental characteristics. Subjective and objective indicators were analyzed as complementary measures of exposure, reducing reliance on self-reported data alone.
The questionnaire, developed based on prior research (Garrett et al., 2019; Payne et al., 2005; Völker et al., 2018), underwent pre-testing with a pilot sample of 10 older adults to ensure clarity, resulting in refinements for improved accuracy and participant comprehension. The final version included an introductory explanation in which examples of natural and artificial blue spaces (e.g., rivers, lakes, sea, ponds, and reservoirs) were provided, and participants were asked to respond based on their usual experience in a typical year. Proximity was assessed by asking participants to estimate their walking time to the nearest blue space. Response options included “up to 5 minutes,” “6–10 minutes,” “11–15 minutes,” “16–20 minutes,” and “more than 20 minutes.” Frequency of intentional visits was categorized as “daily,” “more than three times a week,” “one to three times a week,” “one to two times a month,” “less than once a month,” or “never.” Average duration of these visits was measured using the following categories: “less than 15 minutes,” “15–30 minutes,” “30 minutes to 1 hour,” “1–2 hours,” and “more than 2 hours.” The social context of intentional visits was evaluated by examining whether participants were accompanied by family, friends, or pets. Engagement in physical activity during visits was assessed using a dichotomous item distinguishing participation in moderate-to-vigorous physical activity lasting more than 20 minutes from sedentary or light-intensity activity. Participants also provided information about passing by visible blue spaces during daily commutes (incidental exposure) and whether they observed these spaces from their homes (indirect exposure). This questionnaire (available in supplemental material) also included similar questions about green space exposure to allow for direct comparisons and control of potential confounding effects.
Objective measures of exposure to blue spaces were derived using Geographic Information System (GIS) analysis, ensuring precise and standardized data collection. Residential addresses were provided by participants and georeferenced using Google Maps and the ArcGIS Online Geocoding Service (Ribeiro et al., 2014). Two network-based proximity metrics were calculated using ArcGIS Pro 3.4.0: (A) the distance from participants’ residences to the nearest blue space, measured in meters, and (B) the presence of blue spaces within a 2000-meter radius of their homes, considering prior evidence (Browning & Lee, 2017). As in previous research (Almeida et al., 2022; Paciência et al., 2021), the mapping of blue spaces was based on data provided by the “Water Atlas” of the Portuguese National Water Resources Information Service (SNIRH), ensuring accuracy and consistency in identifying these outdoor natural water bodies. To account for the potential confounding effects of green spaces, exposure to these spaces was evaluated using the Normalized Difference Vegetation Index (NDVI), a generic measure of the amount of vegetation in each location often used in epidemiological research (Cavaleiro Rufo et al., 2021; Paciência et al., 2022). NDVI values were derived from the MODIS 250-m NDVI satellite mission (MOD13Q1, https://earthdata.nasa.gov/), covering the Northern region of Portugal during the spring and summer of 2021, periods associated with peak vegetation. The NDVI is calculated based on the reflectance of visible and near-infrared light, with values ranging from −1 to 1, where higher values indicate greater vegetation density. The average NDVI value was calculated for a 2000-meter radius around each participant’s residence, after excluding negative values.
Statistical Analysis
Data were analyzed using SPSS version 27.0. Descriptive statistics were presented as means and standard deviations for continuous variables and as counts and percentages for categorical variables. Linear regression models were used to assess associations between blue space exposure variables and frailty outcomes (total, physical, psychological, and social domains). Models were adjusted for confounders, including sociodemographic variables (age, sex, and education) and green space exposure variables. Assumptions underlying the regression analyses were assessed, including multicollinearity and indicators of overall model fit, and statistical significance was set at p < 0.05.
Results
Participant characteristics regarding sociodemographic variables and frailty (n = 189)
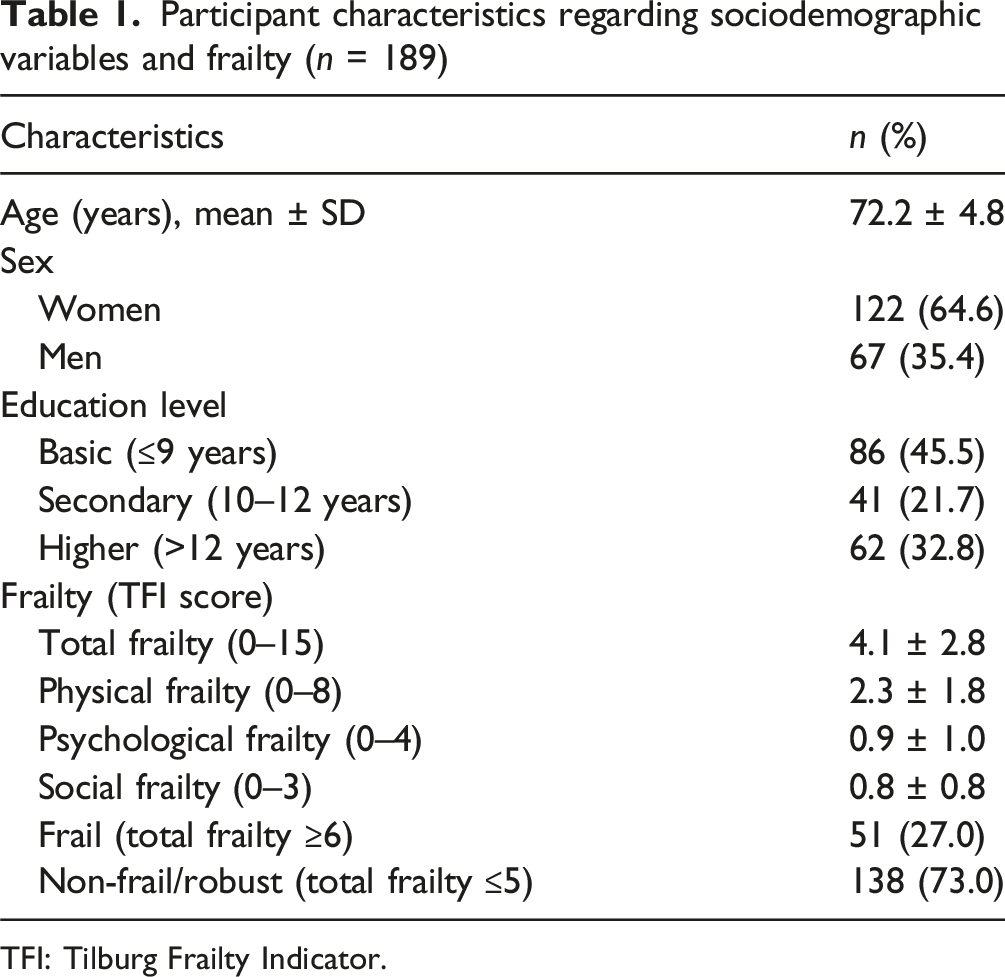
TFI: Tilburg Frailty Indicator.
Among the 189 participants, the average self-reported walking time to the nearest blue space was predominantly more than 20 minutes, reported by 37.6% of participants, while 20.6% reported walking times of up to 5 minutes. Objective measures derived through GIS revealed an average distance to the nearest blue space of 3842.1 m (SD ± 3095), with 37% of participants having a blue space within 2000 m of their home. Regarding the frequency of visits to blue spaces, 19.6% reported daily visits, 29.1% visited 1–3 times per week, and 21.7% reported never visiting these spaces. For visit duration, 46.6% of participants spent more than 2 hours in blue spaces, and 27.7% reported spending 1–2 hours per visit.
Most participants that visited blue spaces engaged in physical activity during their visits (83.8%), and 84.5% were accompanied by family or friends, while 10.1% visited blue spaces with pets. Indirect exposure was reported by 24.3% of participants who had views of blue spaces from their residences. Incidental exposure, such as passing by visible blue spaces during daily commutes, was more common, reported by 58.2% of participants.
Regarding green spaces, the average NDVI value within a 2000-meter radius of participants’ residences was 0.5 (SD ± 0.1), reflecting moderate vegetation density. Self-reported walking times to the nearest green space were generally shorter, with 55.6% of participants reporting up to 5 minutes. Visits to green spaces were more frequent compared to blue spaces, with 38.1% reporting daily visits and 20.6% visiting more than three times per week. Duration of visits was also shorter, with 35.8% spending 1–2 hours and 22.1% spending more than 2 hours per visit. Most participants that visited green spaces reported engaging in physical activity (71.1%), and 15.1% visited with pets.
Participant exposure to blue and green spaces (n = 189)
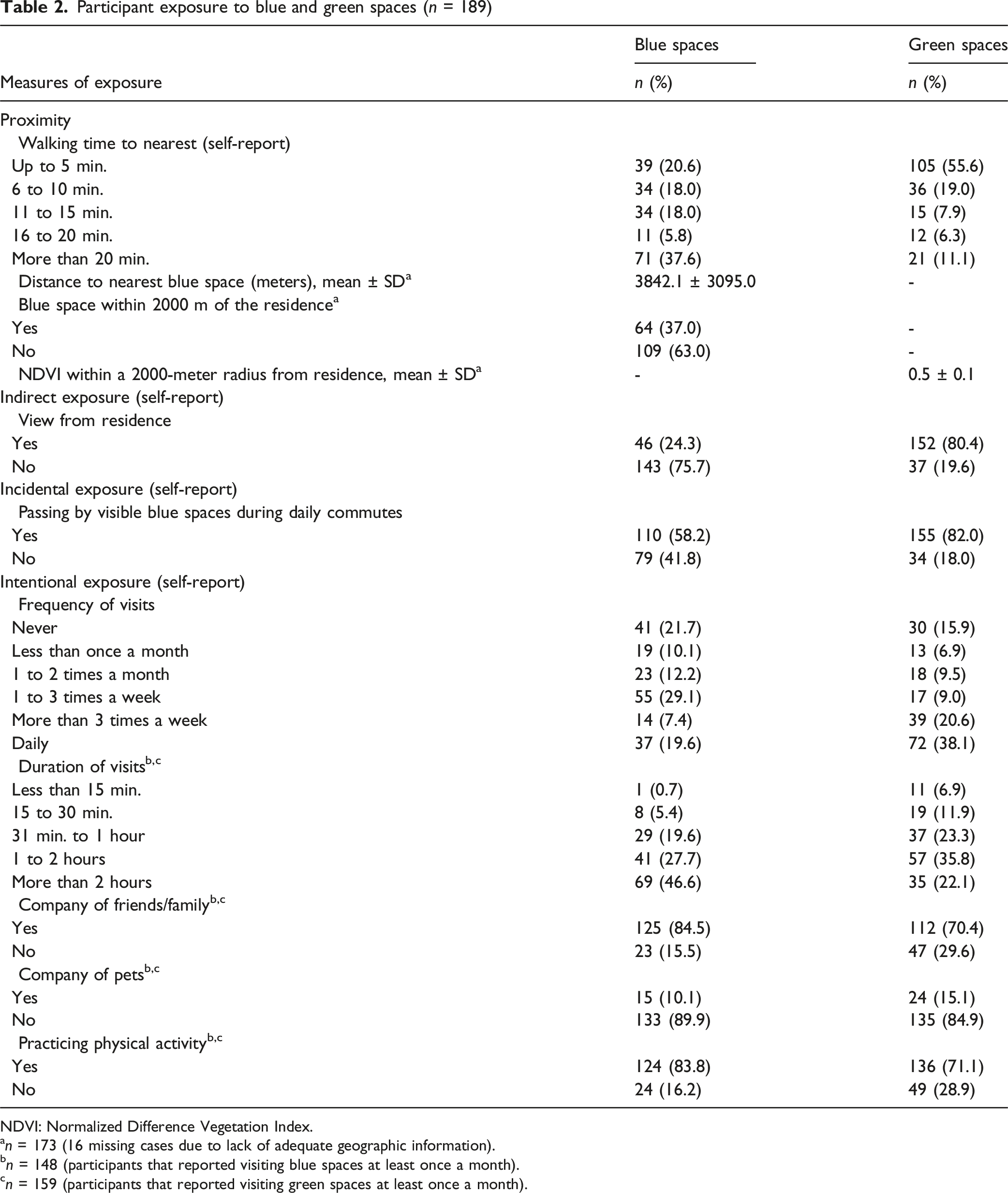
NDVI: Normalized Difference Vegetation Index.
an = 173 (16 missing cases due to lack of adequate geographic information).
bn = 148 (participants that reported visiting blue spaces at least once a month).
cn = 159 (participants that reported visiting green spaces at least once a month).
After adjusting for the effects of age, sex, education level, and measures of exposure to green spaces, several significant associations were found between frailty and exposure to blue spaces. Living within a 5-minute walk from the nearest blue space was associated with lower levels of social frailty (b = −0.36; 95% CI [−0.68, −0.04]), living 11 to 15 minutes away was associated with lower physical frailty (b = −0.86; 95% CI [−1.51, −0.21]), and living 16 to 20 minutes away was associated with lower total frailty (b = −2.55; 95% CI [−4.16, −0.94]) and lower physical frailty (b = −1.43; 95% CI [−2.44, −0.41]), when compared with individuals living more than 20 minutes away on foot. Incidental exposure, measured as passing by visible blue spaces during daily commutes, was associated with lower total (b = −0.85; 95% CI [−1.59, −0.12]) and physical frailty (b = −0.53; 95% CI [−1.00, −0.06]). Visiting blue spaces 1 to 2 times a month was associated with lower physical frailty (b = −0.87; 95% CI [−1.72, −0.03]), when compared with never visiting. Visiting blue spaces for the duration of 1 to 2 hours (b = −3.23; 95% CI [−6.30, −0.16]) and for more than 2 hours (b = −3.23; 95% CI [−6.27, −0.18]) was associated with lower levels of physical frailty, when compared with never visiting. Having the company of friends or family during visits to blue spaces was associated with lower social frailty (b = −0.45; 95% CI [−0.83, −0.06]), and being accompanied by pets was associated with lower physical frailty (b = −1.16; 95% CI [−2.11, −0.20]). Finally, engaging in physical activity in these spaces was associated with lower physical frailty (b = −0.83; 95% CI [−1.58, −0.07]).
Association between frailty (total, physical, psychological, and social) with measures of exposure to blue spaces (n = 189)
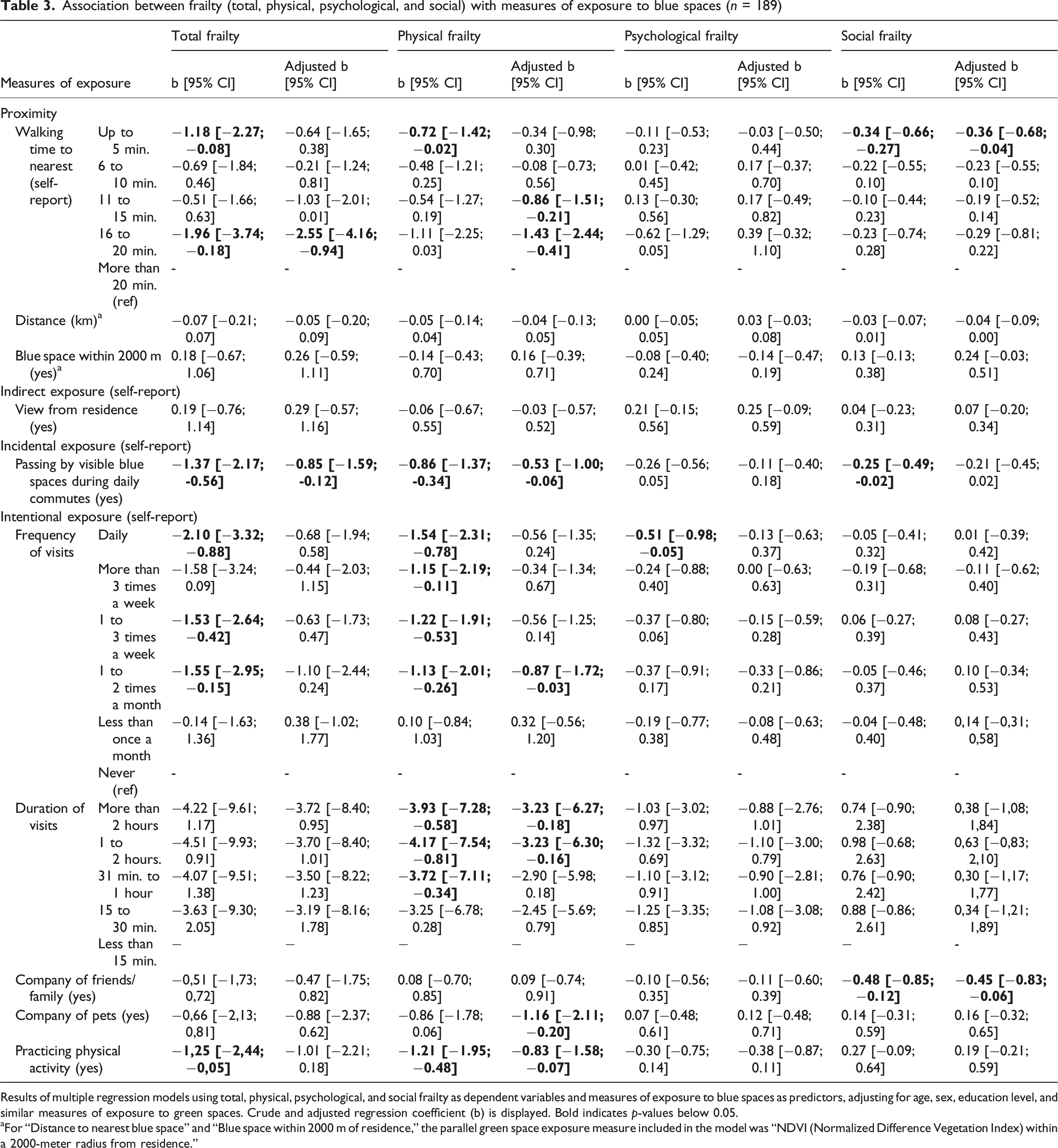
Results of multiple regression models using total, physical, psychological, and social frailty as dependent variables and measures of exposure to blue spaces as predictors, adjusting for age, sex, education level, and similar measures of exposure to green spaces. Crude and adjusted regression coefficient (b) is displayed. Bold indicates p-values below 0.05.
aFor “Distance to nearest blue space” and “Blue space within 2000 m of residence,” the parallel green space exposure measure included in the model was “NDVI (Normalized Difference Vegetation Index) within a 2000-meter radius from residence.”
Discussion
This study demonstrated significant associations between various measures of exposure to blue spaces and different domains of frailty, even after accounting for potential confounding factors such as age, sex, education level, and similar indicators of exposure to green spaces. Specifically, making purposeful visits to blue spaces once or twice a month and spending at least 1 hour in these spaces was associated with lower physical frailty, as was visiting with pets and engaging in physical activity during such visits. Also, visiting blue spaces with family members or friends was associated with lower levels of social frailty. Incidental exposure, such as passing by visible blue spaces during daily commutes, was linked to lower total and physical frailty. Conversely, walking travel times to blue spaces under 20 minutes were associated with lower levels of total, physical, and social frailty, with different distances within this range showing associations with different frailty domains, highlighting the nuanced relationship between environmental exposure and multidimensional frailty in older adults.
The observed association between deliberately visiting and spending time in blue spaces with reduced physical frailty aligns with existing evidence suggesting that natural environments promote physical activity (Britton et al., 2020; Gascon et al., 2017; Georgiou et al., 2021; Nutsford et al., 2016; Wang & Sani, 2024), a critical factor in preventing frailty by helping mitigate sarcopenia, preserving muscle strength, and improving endurance and mobility (Apóstolo et al., 2018; Clegg et al., 2013; Landi et al., 2010; McPhee et al., 2016; Navarrete-Villanueva et al., 2021; Oikawa et al., 2019; Rogers et al., 2017; Woolford et al., 2020). In this study, most individuals who visited blue spaces engaged in physical activity during their visits, highlighting these environments as facilitators of active lifestyles. As expected, involvement in such activities was significantly associated with lower levels of physical frailty, reinforcing the role of blue spaces in fostering behaviors that protect against physical decline (Britton et al., 2020; Gascon et al., 2017; Georgiou et al., 2021; Nutsford et al., 2016; Wang & Sani, 2024). However, physical activity was assessed in a general manner, without differentiation between specific types of activity, which may have limited a more nuanced understanding of this association.
In addition, there was an association between visiting blue spaces in the company of pets and lower physical frailty. This finding aligns with evidence that walking pets promotes interaction with outdoor environments and physical activity, enhancing physical function and reducing daily activity limitations in older adults (Christian et al., 2013; Curl et al., 2017; Friedmann et al., 2023; Shibata et al., 2012). Additionally, blue spaces, with their unique sensory stimuli and aesthetic qualities, may have a calming effect that promotes mental restoration and stress reduction, which could indirectly contribute to better physical fitness (Britton et al., 2020; Gascon et al., 2015; Smith et al., 2021; Wang & Sani, 2024; White et al., 2021). Finally, contacting blue spaces is often accompanied by sunshine exposure, which promotes vitamin D production, with low levels of this vitamin being linked to increased physical frailty (Clegg et al., 2013; Marcos-Pérez et al., 2020). These results emphasize the importance of not only the existence but also the quality and accessibility of blue spaces, as they may encourage longer visits and greater engagement (Haeffner et al., 2017; Knight et al., 2022; Pool et al., 2023; Poulsen et al., 2022; Vert et al., 2019).
Similarly, visiting blue spaces with family members or friends was associated with lower social frailty, which is in line with research showing that shared outdoor experiences may strengthen social bonds and reduce the feeling of loneliness among older adults (Astell-Burt et al., 2022; Britton et al., 2020; Cole et al., 2024; Georgiou et al., 2021; Leavell et al., 2019; Wang & Sani, 2024; White et al., 2020).
The finding that incidental exposure to blue spaces was associated with reduced total and physical frailty is also relevant. This suggests that even passive interaction with blue spaces, such as passing near visible blue spaces on daily routines, may confer health benefits. Such exposure could reduce stress, enhance mood, promote attention restoration, and provide brief but meaningful connections with nature, supporting both physical and mental health (Britton et al., 2020; Gascon et al., 2015; Smith et al., 2021; Wang & Sani, 2024; White et al., 2020, 2021; Zijlema et al., 2018). Importantly, this highlights the potential for urban planning to integrate blue spaces into daily life, ensuring their visibility and accessibility to the broader community. Interventions aimed at creating walkable communities enriched with blue spaces could be particularly beneficial for older adults, who are more likely to face mobility limitations and would greatly benefit from accessible, health-promoting environments (Britton et al., 2020; Pool et al., 2023; Wang & Sani, 2024). However, the absence of a significant association between frailty and having a view of blue spaces from home in this study contrasts with previous research that suggests visual access to blue spaces may enhance well-being (Dempsey et al., 2018; Nutsford et al., 2016; Wang & Sani, 2024; White et al., 2020). This finding underscores the critical role of physical proximity and direct interaction with blue spaces, highlighting that mobility and the ability to engage actively with these environments may be key factors in realizing their full health benefits.
On the other hand, the association between shorter walking travel times to blue spaces and lower total, physical, and social frailty suggests that proximity may play an important role in enabling access and opportunities for engagement. Older adults living farther from blue spaces may experience fewer opportunities for regular physical activity and for participation in community or recreational activities, which are critical for maintaining physical function, preserving social networks and supporting psychological resilience (Britton et al., 2020; Gascon et al., 2017; Georgiou et al., 2021; Haeffner et al., 2017; Nutsford et al., 2016; Pool et al., 2023; Vaeztavakoli et al., 2018; Wang & Sani, 2024; White et al., 2020). This emphasizes the importance of equitable access to blue spaces, particularly in urban areas, where distance and infrastructural limitations may disproportionately affect vulnerable populations (Haeffner et al., 2017; Pool et al., 2023; Vert et al., 2019). Notably, while this study found associations with subjective measures of blue space exposure, such as self-reported travel times, no significant associations were observed with objective measures, including the distance to the nearest blue space or the presence of a blue space within 2000 m of home, a buffer chosen based on its predictive value for physical health in previous studies (Browning & Lee, 2017). This discrepancy, consistent with findings in the literature (Dean et al., 2022; Georgiou et al., 2021; Hur et al., 2010; Nyunt et al., 2015), highlights the distinct information provided by subjective and objective measures. Subjective measures may capture daily experiences, perceptions, and attitudes toward blue spaces, which could be more directly linked to health outcomes (Dean et al., 2022; Hur et al., 2010; Nyunt et al., 2015). These findings underscore the importance of integrating both subjective and objective measures in future research to provide a comprehensive understanding of the relationship between environmental exposure and frailty.
Interestingly, no significant associations were found between psychological frailty and any measures of blue space exposure. It is possible that the restorative effects of blue spaces on psychological well-being require more sustained or intense interactions than those captured in this study. Similarly, the absence of a significant association between the frequency of visits to blue spaces and frailty, contrasted with the observed relationship between frailty and the duration of visits, highlights the importance of the quality of these interactions. Longer, more meaningful visits may have a greater impact on health than frequent but brief encounters (Aliyas, 2021; Garrett et al., 2019; Georgiou et al., 2021), emphasizing the need for future research to explore how the intensity and quality of exposure to blue spaces influence different dimensions of frailty.
It is also important to consider the potential bidirectional relationship between frailty and blue space exposure. While this study focused on the influence of blue spaces on frailty, it is equally plausible that frailty itself limits individuals’ ability to access and engage with these environments. For example, older adults with physical frailty may face mobility challenges that reduce their exposure to blue spaces, creating a cycle that perpetuates health disparities. However, when considering the relationship between proximity to blue spaces and frailty, it is more plausible that proximity exerts a stronger influence by facilitating access to environments that promote physical activity, social interaction, and overall health, than that frailty leads individuals to live in locations further from blue spaces. Longitudinal studies are needed to disentangle these relationships and identify causal pathways.
Indeed, the cross-sectional design of the present study does not allow for causal inferences regarding the associations observed. Additional limitations include the use of a non-probabilistic convenience sample, which restricts the generalizability of the findings, and the possibility of selection bias, as healthier individuals may have been more likely to participate. Furthermore, like other studies on the impact of residential environments on health, this study may be affected by residential self-selection bias, where healthier individuals choose to live in areas that support their well-being, potentially influencing the observed associations (Boone-Heinonen et al., 2010).
Conclusion
This study highlights the complex associations between exposure to blue spaces and multidimensional frailty in older adults. Key findings reveal that deliberately visiting and spending more than 1 hour in blue spaces, engaging in physical activity during visits, and visiting with pets were linked to lower levels of physical frailty, while visiting with family members or friends was associated with lower social frailty. Passing by visible blue spaces during daily commutes was associated with lower levels of total and physical frailty. Moreover, different travel distances to blue spaces under 20 minutes were related to lower levels of total, physical, and social frailty. These results underline the diverse ways in which blue space exposure can influence different dimensions of frailty, emphasizing their potential in supporting healthier aging processes.
The results of this study contribute to the growing body of evidence on the health benefits of natural environments, particularly blue spaces, and their potential role in reducing frailty. The concept of “blue care,” which emphasizes the health-promoting aspects of interactions with blue spaces, is reinforced by these findings. Blue care strategies, such as promoting accessibility to water-based environments and integrating these spaces into urban planning and therapeutic interventions, could be valuable in mitigating frailty, particularly among older adults. These findings also highlight the need to ensure appropriate and equitable access to blue spaces to maximize their benefits across diverse populations.
Future research should build on these findings by exploring the causal pathways between blue space exposure and frailty through longitudinal studies. Investigations into the intensity and quality of exposure, as well as the mechanisms underlying the observed associations, are warranted. Further, understanding how individual and environmental factors interact with blue space exposure will provide a more comprehensive picture of its potential benefits. Continued research in this area is essential to inform evidence-based strategies and public health interventions to enhance the health and well-being of aging populations.
Supplemental Material
Supplemental Material - The Association Between Exposure to Blue Spaces and Multidimensional Frailty in Community-Dwelling Older Adults: A Cross-Sectional Study
Supplemental Material for The Association Between Exposure to Blue Spaces and Multidimensional Frailty in Community-Dwelling Older Adults: A Cross-Sectional Study by Tiago Coelho, Diana Leite, Daniela Maciel, Ana Isabel Ribeiro, Nuno Rocha in Journal of Applied Gerontology
Footnotes
Ethical Considerations
The study was approved by the E2S, Polytechnic of Porto Ethics Committee (registry number CE0044B).
Consent to Participate
Informed consent was obtained from all participants included in the study.
Author Contributions
Study conception and design: TC, AIR, and NR; data collection: DL and DM; analysis and interpretation of results: TC, DL, AIR, and NR; draft manuscript preparation: TC, DL, and AIR. All authors reviewed the results and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fundação para a Ciência e Tecnologia (FCT) through R&D Units funding UID/5210/2025 (https://doi.org/10.54499/UID/05210/2025), UID/4750/2025 (https://doi.org/10.54499/UID/04750/2025), and LA/P/0064/2020 (https://doi.org/10.54499/LA/P/0064/2020). This research also received support from the Centre of Studies in Geography and Spatial Planning (CEGOT), funded by national funds through the Foundation for Science and Technology (FCT) under the reference UIDB/04084/2025. Ana Isabel Ribeiro was supported by National Funds through FCT, under the “Stimulus of Scientific Employment – Individual Support” programme within the contract CEECIND/02386/2018, https://doi.org/10.54499/CEECIND/02386/2018/CP1538/CT0001.
Declaration of Conflicting Interests
The authors declare that they have no competing interests.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online