
Abstract
Background and Purpose:
The global population is aging rapidly, with the proportion of those aged 65 and above projected to reach 16% by 2050. Gait disorders are common in older adults and can predict negative health outcomes, including falls. While aging and gait disorders are risk factors for falls, the effects of falls on gait parameters remain unclear. This cross-sectional study aimed to describe spatiotemporal gait parameters and associated factors in older adults hospitalized after a fall.
Methods:
This cross-sectional study was conducted at the Department of Gerontology of our University Hospital from January to April 2024. The collected data included sociodemographic data (age and sex), clinical data (height, weight, BMI, Mini-Mental State Examination score, serum albumin levels, rhabdomyolysis, long lie on the floor, and fall history), and functional data (Timed Up and Go test, Short Physical Performance Battery, Floor Transfer Test). The Physiolog 6S gait sensors from GaitUp were used to record gait parameters, which were analyzed by stratifying the aforementioned data.
Results and Discussion:
Thirty patients were included (mean age 83.5 ± 5.1 years, 11 men and 19 women). Eight spatiotemporal gait parameters were analyzed: walking speed, cadence, stride length, right and left step length and height. Patients with rhabdomyolysis, lower serum albumin levels had significantly slower walking speeds (0.5 ± 0.1 vs. 0.8 ± 0.2 m/s and Spearman’s rho = 0.8, 95% CI: 0.62–0.9 p < .001). Patients with lower functional capacity had slower walking speeds (SPPB: 0.5 ± 0.2 vs. 0.8 ± 0.1 m/s; TUG: 0.4 ± 0.1 vs. 0.7 ± 0.1 m/s; FTT: 0.5 ± 0.2 vs. 0.8 ± 0.0 m/s, p < .001).
Conclusion:
This study emphasizes the connection between declining gait parameters, biological markers, and functional performance. More comprehensive prospective studies are necessary to investigate how biological markers, cognitive and functional abilities, fall history, and gait parameters are related in older adults for improved management.
Introduction
The global population is aging rapidly (Padeiro et al., 2023). As people age, physiological changes can weaken their walking and balance, increasing the risk of falls (Zhu et al., 2020).
One-third of people aged 65 and older experience at least one fall per year globally. The risk of being injured or dying from a fall increases with age and is highest among people aged 60 and older. Falls are also a leading cause of hospitalization in older adults (WHO, 2021).
Gait disorders are common in older adults, with one study reporting a prevalence of 35% in a community-based cohort (Verghese et al., 2006). Analysis of gait parameters has been shown to predict negative health-related outcomes in the clinical, cognitive and physical domains such as disability, falls, hospitalizations, and even mortality (Bortone et al., 2021). Among spatiotemporal gait parameters (STGP), gait speed is the most widely studied. It has been linked to various physical or cognitive characteristics that can affect the quality of life of patients when they are diminished, to the point that it is considered by some authors as the “sixth vital sign” (Fritz & Lusardi, 2009). Limited research has examined STGP in older adults hospitalized after falls. These studies have found that gait performance is impaired in hospitalized older adults compared to community-dwelling older adults (Leirós-Rodríguez et al., 2020; Peel et al., 2013).
While aging and gait disorders are known as risk factors of falls, the effects of falls on gait parameters remain unclear (Herssens et al., 2018; Zhu et al., 2020). Studies have shown that individuals who fall may have shorter strides and wider steps, but these modifications in gait may be influenced by various confounding variables, further complicating the relationship between aging, walking, and falls (Morfis & Gkaraveli, 2021; Niederer et al., 2021; Pophal da Silva et al., 2021). For instance, in previous studies authors have discussed that functional capacity could play a more significant role than fall history, or may be a more discriminating factor than age to explain modifications in gait parameter among different age groups in geriatric populations (Dapp et al., 2022; Pophal da Silva et al., 2021).
The objective of this cross-sectional study was to describe the STGP and the associated factors in older adults hospitalized after a fall, in order to explore the effect of falls on gait parameters more broadly. We hypothesized that the older adults included in the study would have impaired gait performance compared to reference values for healthy older adults, particularly for subgroups with lower functional capacity.
Methods
This study is a cross-sectional ancillary study of the HydroFall protocol conducted at the Department of Gerontology of our University Hospital. The period of inclusion and data collection spanned from January to April 2024. This research report was written in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines (von Elm et al., 2007). The study was authorized by the institution’s review board and the Committee for the Protection of Persons (CPP) of Ile de France under the number 22.02023.000104 – 2022-A01157-36.
Eligible patients were recruited by convenience during outpatient visits dedicated to gait disorders. The investigator carried out the inclusion process and provided the consent form for the patient, their trusted person, or legal representative to sign.
The inclusion criteria were that participants must be aged 70 years or older, have somatic complaints such as dizziness, lower limb weakness, gait disorders, or psychomotor slowing, have a history of falls, be informed and non-opposed to participation, and be affiliated with a social security regime. The non-inclusion criteria were that participants present with severe neurocognitive disorders (MMSE ≤ 17), require continuous assistance for mobility, or be under legal protection measures such as guardianship, conservatorship, protective supervision or future protection mandate. The exclusion criteria were that participants could not achieve the gait assessment analysis for physical or any health status reason.
All gait data were collected using a Physilog® 6 inertial measurement unit (IMU; MindMaze Assessments), a sixth-generation wearable nine-DoF motion sensor system with integrated barometer (Beauchet et al., 2005). The sensor was attached to the back of the foot, on the usual footwear of the patient, either by passing through the laces or using an elastic strap with Velcro patches. The data were recorded locally and transferred to a computer via USB cable for analysis with the GaitLab software. No calibration was needed. The required patient information included height (in cm), weight (in kg), and foot length (in cm). The data were securely stored in a collaborative space managed by our University Hospital, accessible only via username and password. The validity of IMU, as represented by Lin’s concordance correlation coefficient (LCC), was excellent (LCC > .9) for stride length, cadence, and walking speed, good (LCC > .65) for step length, fair (LCC > .40) for double support and heel maximum height. Additionally, all these gait parameters had high Pearson’s correlation coefficients (>.75), indicating a strong linear relationship between the IMU and the reference standard measurements (Homan et al., 2022). Among STGP, the only known clinical minimal difference was for walking speed, which was 9.6 cm/s (Hars et al., 2013).
Patients were instructed to perform a round trip, covering approximately 20 m, including a half-turn. Before the test, patients were required to stand still for 5 s to allow for sensor calibration. They were then asked to walk as naturally as possible. Patients had the option of holding onto a handrail on their left on the way out and on their right on the return, or using a technical aid if needed. An investigator accompanied the patient to ensure the smooth running of the test and their safety, preventing them from falling during the test.
The data were recorded locally and transferred to a computer via USB cable for analysis using the GaitLab software. The required patient information included height (in centimeters), weight (in kilograms), and foot length (in centimeters). After the GaitLab software analysis, collected STGP were submitted to statistical analysis along with other variables to determine which factor influence the STGP.
Sociodemographic variables included age and gender, anthropometric data included height and weight. A multidisciplinary team, consisting of an occupational therapist, a physiotherapist, and the overseeing physician, collected clinical variables. These included mobility and functional capacity, assessed through the Timed Up and Go (TUG) test, Short Physical Performance Battery (SPPB), and Floor Transfer Test (FTT), and cognitive state, assessed through the Mini-Mental State Examination (MMSE). Blood samples were collected to measure serum albumin and creatine kinase levels. The time spent on the floor after a fall, and the report of previous falls were also recorded.
The statistical analysis was conducted using JASP software version 0.18.3. All tests were two-sided and the risk α was set at 0.05. Data collection was thorough, resulting in a dataset with no missing values. Continuous variables were presented as means and standard deviations (SD), while categorical variables were reported as absolute numbers and percentages. To assess the assumptions of the statistical tests, Shapiro-Wilk and Levene’s tests were performed. Since not all variables followed a normal distribution and the sample was not homoscedastic, non-parametric tests were used for the analyses. Mann-Whitney U tests were chosen to analyze STGP (the outcome variable) stratified by gender, capacity to perform FTT, prolonged time spent on the floor, presence of biological rhabdomyolysis, MMSE and SPPB scores. Spearman correlations were used to compare STGP with height, weight, BMI, serum albumin, and TUG scores. Due to the large number of statistical tests performed (112), a post-hoc Holm-Bonferroni correction was applied to the p-values to control inflation of the alpha risk.
Effect sizes were reported as biserial rank correlation (r) or Spearman’s rho (ρ) depending on whether the test was a Mann-Whitney U test or a Spearman correlation, respectively. Biserial rank correlation values .1 < r < .3 were considered as small, .3 < r < .5 as medium and r < .5 as a large effect. Spearman’s rho values 0.00 < ρ < 0.19 were considered as very weak, 0.20 < ρ < 0.39 as weak, 0.40 < ρ < 0.59 as moderate 0.60 < ρ < 0.79 as strong and ρ < 0.8 as very strong.
Results
Of the 37 patients admitted for fall-related reasons, 30 were included in the gait assessment and data analysis. The remaining seven patients were excluded because they required assistance to stand or walk. The selection criteria for patients included in this study are described in Figure 1.

Flow diagram.
The demographic and clinical characteristics of the participants are presented in Table 1. The mean age of the participants was 83.5 years (±5.1 years). The youngest included patient was 73 years old and the oldest was 95 years old. Among the participants, 11 were men (36.7%) and 19 were women (63.3%).
Participant Characteristics (n = 30).
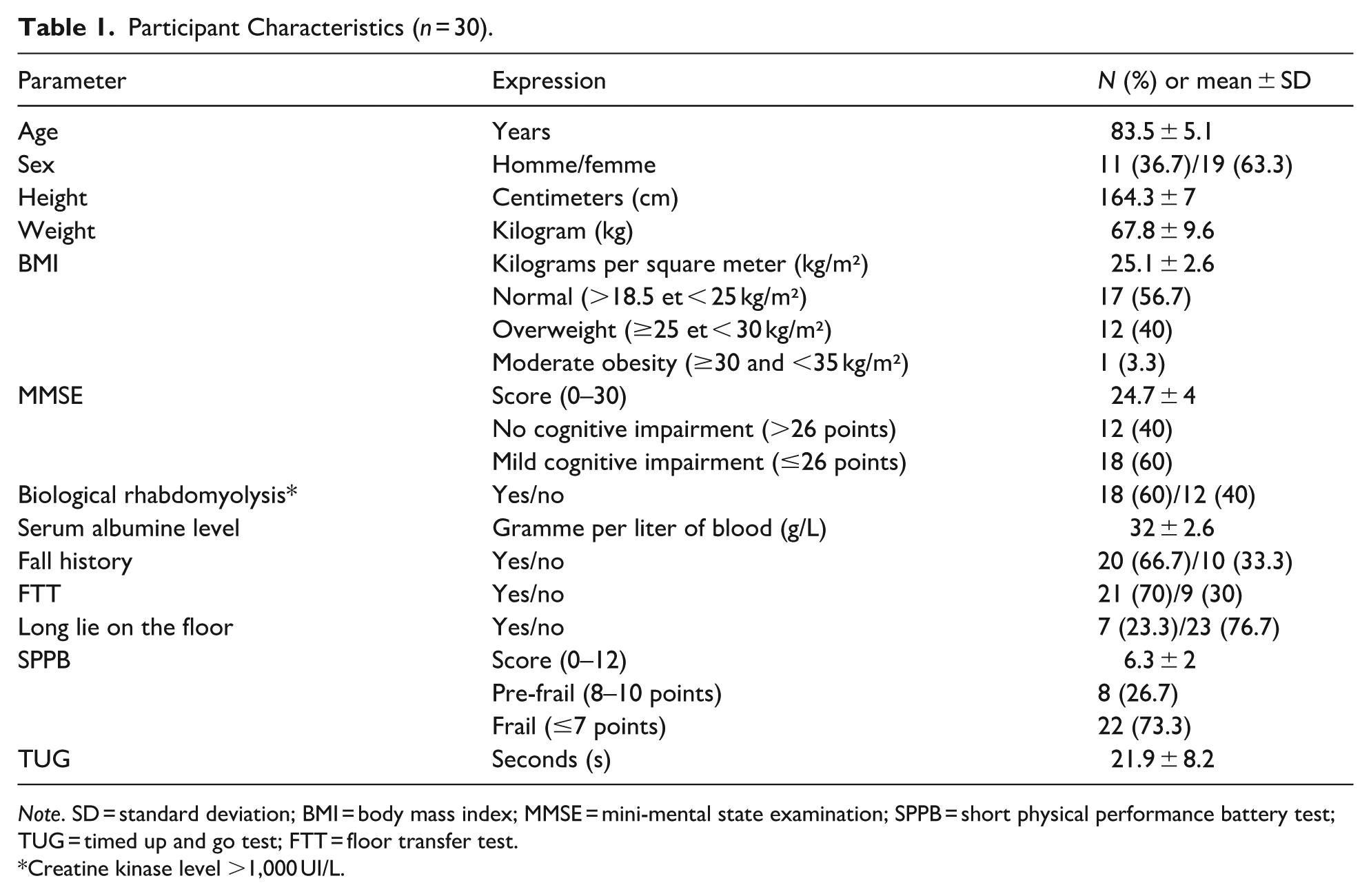
Note. SD = standard deviation; BMI = body mass index; MMSE = mini-mental state examination; SPPB = short physical performance battery test; TUG = timed up and go test; FTT = floor transfer test.
Creatine kinase level >1,000 UI/L.
Overall, a large proportion of participant performed poorly on clinical assessments. Specifically,
The description of the STGP of the participants is presented in Table 2. The studied variables included walking speed, cadence, stride length, right and left step lengths, percentage of double support, as well as the maximum heights of the right and left heels. The mean walking speed was low, at 0.6 ± 0.2 m/s. Stride length (0.6 ± 0.2 m) and step length (0.3 ± 0.1 m) were also reduced. However, cadence was relatively high, with participants walking at 99.4 ± 9.7 steps per minute.
Spatiotemporal Gait Parameters of the Participants.

Results of univariate analysis are presented in Tables 3 and 4. After the Holm-Bonferroni correction, Mann-Whitney tests and Spearman’s correlation analysis revealed no differences or correlations between anthropometric data, socio-demographic data, cognitive function and STGP. Differences were observed based on the presence or absence of rhabdomyolysis for all STGP. Patients with rhabdomyolysis had significantly slower walking speeds (0.5 ± 0.1 vs. 0.8 ± 0.2 m/s, p < .001) compared to those without rhabdomyolysis. Similarly, patients with prolonged time spent on the ground (>1 hr) also had slower walking speeds (0.5 ± 0.2 vs. 0.8 ± 0.1 m/s, p < .001) in comparison to those with shorter ground station times. All STGP were also correlated with serum albumin levels (all p < .001). Correlation for walking speed was strong with a Spearman’s rho of .8 (95% C.I.: .62–.9).
Univariate Analysis of Spatiotemporal Gait Parameters Stratified According to Clinical Examination Results.
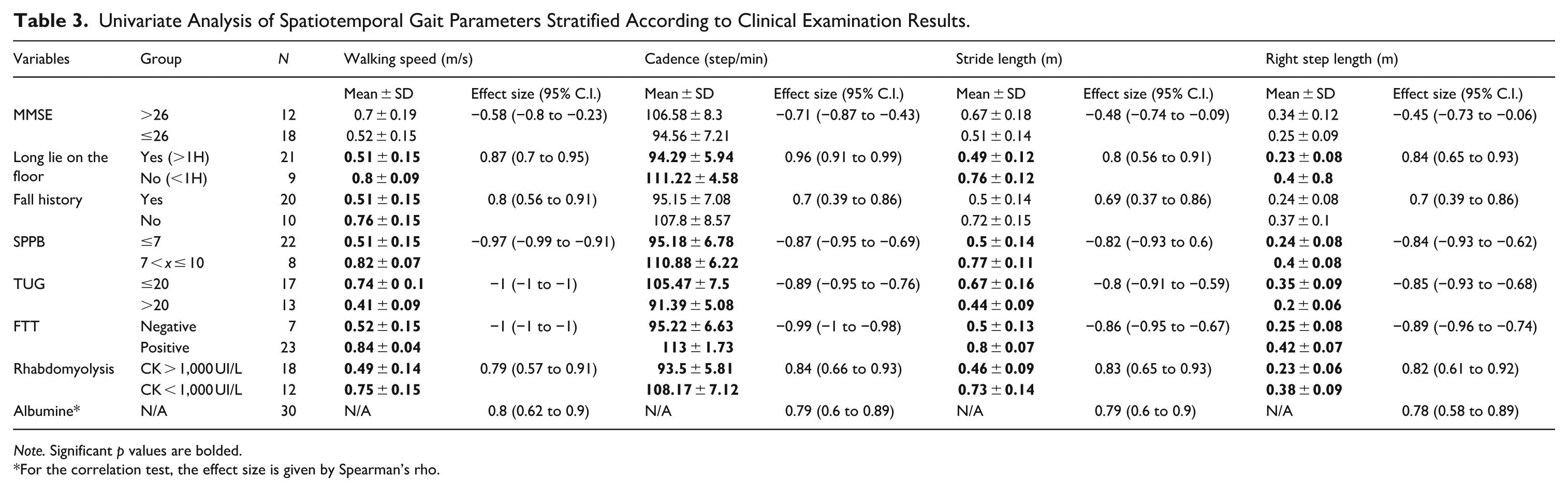
Note. Significant p values are bolded.
For the correlation test, the effect size is given by Spearman’s rho.
Univariate Analysis of Spatiotemporal Gait Parameters Stratified According to Clinical Examination Results.

Note. For the Mann-Whitney test, the effect size is given by the Biserial rank correlation. MMSE = mini-mental state examination; SPPB = short physical performance battery test; TUG = timed up and go test; FTT = floor transfer test; CK = creatine kinase; CI = confidence interval; N/A = not applicable.
For the correlation test, the effect size is given by Spearman’s rho. Significant p values are bolded.
Differences were observed based on functional status as well for all STGP except for heel height. Patients with lower SPPB scores (≤7), higher TUG scores (>20 s) and who were unable to perform an FTT had slower walking speeds (0.5 ± 0.2 vs. 0.8 ± 0.1 m/s, 0.4 ± 0.1 vs. 0.7 ± 0.1 m/s, 0.5 ± 0.2 vs. 0.8 ± 0.0 m/s, p < .001 respectively).
Finally, patients who had experienced repeated falls only showed slower walking speeds (0.5 ± 0.2 vs. 0.8 ± 0.2 m/s, p < .001) and increased double support time percentage (36.5 ± 5.4% vs. 26.4 ± 4.1%, p < .001) compared to those without a history of falls.
Discussion
The aim of this study was to examine the factors that influenced the STGP of older adults hospitalized after a fall. The STGP studied included walking speed, cadence, percentage of double support, stride length, and the length and height of the right and left steps. This is the first study to examine blood test results in relation to gait parameters and demonstrated associations between changes in gait parameters and both rhabdomyolysis (creatine kinase > 1,000) and serum albumin levels. All functional tests and prolonged time spent on the floor were also found to be associated with changes in STGP, and fall history to a lesser degree.
Therefore, a key strength of this study is the addition of innovative data to the reference dataset for patients hospitalized due to falls. Additionally, the study followed the minimal set of recommendations by Beauchet et al. for evaluating gait parameters, which contributes to reduce data heterogeneity in the literature (Beauchet et al., 2017).
The STGP recorded in this sample indicated impaired gait performance. Compared to the normative data from Hollman et al., our sample showed slower walking speed (0.6 m/s), reduced mean step length (0.28 m), and reduced stride length (0.57 m), about half the reference values (Hollman et al., 2011). Similar results were recently reported by Bourgarel et al. for an older adult population (mean age 85.9) hospitalized and compared to the same reference data. The only notable difference was a significantly higher double support time (>40% of the cycle) in their study, compared to 29.5% in the Hollman data and 33.8% in our study. Bourgarel et al. attributed these modifications to the pathological nature of their study population. In our sample, we did not identify comorbidities beyond rhabdomyolysis or fall histories. However, the high rate of rhabdomyolysis (60.0%), low functional capacity (mean SPPB score of 6), and high proportion of recurrent fallers (66.7%) suggest poor general health status, supporting their hypothesis. Dapp et al. also compared STGP in community-dwelling older adults (mean age 78.5; Dapp et al., 2022). The group considered frail (SPPB < 8) still showed better gait performance than our hospitalized sample, despite equivalent functional levels. This difference may be explained by the more compromised health status of the hospitalized patients. Similarly, González-Castro et al. reported that combining accelerometric with non-accelerometric factors (e.g., clinical and demographic data) significantly improved fall risk prediction using machine learning. This supports our findings by highlighting the added value of integrating biological and functional measures with gait parameters in hospitalized older adults (González-Castro et al., 2025).
After Holm-Bonferroni correction, no significant correlation or difference was found between the anthropometric data (height, weight, BMI), the sociodemographic data (age and sex) and the STGP measures, in contrast to previous findings (Hollman et al., 2011; Niederer et al., 2021; Thaler-Kall et al., 2015). One potential explanation is that the anthropometric data in the sample had limited variability, with mean height of 164.3 ± 7 cm, mean weight of 67.8 ± 9.6 kg, and mean BMI of 25.1 ± 2.6 kg/m². Alternatively, the lack of association between anthropometric data or age and STGP could be due to uncontrolled confounding factors, such as functional capacity level. This could also account for the absence of sex differences in STGP (Niederer et al., 2021).
An association between cognitive performance and STGP could not be demonstrated in this study. The MMSE, although widely used, may not be sufficiently valid or responsive to detect changes in cognitive status (Salis et al., 2023). Previous studies have found that STGP and gait in general are linked to cognitive abilities (Bortone et al., 2021; Fuentes-Abolafio et al., 2021). Lindemann et al. have proposed a classification system for STGP based on the pathologies that influence them, where walking speed and variability of different parameters are already associated with cognitive functions (Lindemann, 2020). Further research in this area seems warranted.
Regarding functional capacity and mobility, participants had an average TUG time of 21.9 s and an SPPB mean score of 6 (±2). Additionally, 70% of the participants were unable to get up from the floor. These characteristics indicate low functional capacity and mobility, which are consistent with the high proportion of recurrent fallers included in the study. Previous research has shown a link between a TUG time greater than 13.5 s and the inability to get up from the floor alone, a condition referred to as “non-recovered fall” (Karpusenko et al., 2023). Our analysis revealed that almost all the STGP were associated with assessment tests of functional capacity and mobility. These results align with findings from similar studies (Dapp et al., 2022; Pophal da Silva et al., 2021).
The only STGP measures associated with fall history in this sample were walking speed and the percentage of double support. In 2014, a systematic review by Mortaza et al. highlighted differences in walking speed and stride length between fallers and non-fallers, but did not evaluate functional capacity as a moderator (Mortaza et al., 2014). Since then, only two studies have evaluated the functional capacity of patients with or without fall histories, and found that fall history does not influence walking performance when functional capacity is the same between the groups (Pophal da Silva et al., 2021; Svoboda et al., 2017) . Bourgarel et al. hypothesized that it may not be relevant to differentiate between fallers and non-fallers in a population of hospitalized geriatric patients with impaired walking performance, as they would all be at high risk of falling (Bourgarel et al., 2023). This hypothesis warrants further investigation. Specifically, it would be valuable to determine whether falls causally influence STGP. Our study design did not include a multivariate analysis to account for confounding factors such as functional capacity, so we cannot conclusively determine the association between fall history and the observed differences in walking speed or percentage of double support in our sample. More methodologically rigorous research is required to explore this relationship. Additionally, it may be valuable to investigate whether the timing of a fall (i.e., the chronological proximity to the assessment) plays a moderating role in the association between fall history and walking performance, as this factor has not been reported in the existing literature on these topics.
Patients in this study likely developed rhabdomyolysis, a condition characterized by the breakdown of muscle tissue, due to prolonged time spent on the floor or from a fall-related injury (Kodadek et al., 2022). The breakdown of muscle and the systemic nature of this condition could disrupt gait and motor function, accounting for the differences observed in all STGP analyses between patients with and without a diagnosis of rhabdomyolysis. Patients with rhabdomyolysis may benefit from closer monitoring of their gait. Future research could investigate whether gait parameters can help predict the risk or severity of rhabdomyolysis.
Hypoalbuminemia, or low serum albumin levels, was associated with impairment in all STGP analyses. Schalk et al.′s previous research found that hypoalbuminemia (low serum albumin levels) was associated with functional decline in a population with a mean age of 74 years, using a threshold of 43 g/L (Schalk et al., 2005). In our study of older adults with a mean age of 85 years, the mean serum albumin level was 32.0 g/L, and only two participants had levels above the 36 g/L threshold proposed for geriatric populations in previous research (Kubota et al., 2012). Our findings support the existing evidence linking hypoalbuminemia to poorer health status (Arques, 2018; Schalk et al., 2005; Seidu et al., 2020). Serum albumin should not be considered a direct cause of walking dysfunction, but rather an indicator of other contributing factors, such as malnutrition, cardiovascular disease, and metabolic disorders. Therefore, since albumin measurement is standardized, simple, and inexpensive, it may be a relevant factor to consider when assessing, both in clinical practice and research (Arques, 2018; Seidu et al., 2020).
The main limitation of this study is its cross-sectional design, which prevents establishing directional or causal relationships. A prospective cohort study would have been more appropriate. Additionally, the single-center nature of the study restricts the generalizability of the findings to other acute geriatric populations. The small sample size also limits the statistical reliability, especially for subgroup analyses.
Furthermore, the study did not report several key elements recommended in the guidelines by Beauchet et al., including participants’ ethnicity, medication use, presence of anxiety/depression, comorbidities, motor function history, sensory deficits, use of walking aids, and subjective gait difficulties. Of the four recommended gait parameters, only walking speed was analyzed (Beauchet et al., 2017). The absence of these key geriatric confounders may limits comparability with previous studies. Finally, the results should be interpreted cautiously as no adjustments were made for potential confounding variables.
Conclusion
This cross-sectional study has identified several factors that could influence gait parameters in older adult individuals hospitalized after a fall. Specifically, we observed statistically significant associations between worsened gait parameters and the presence of rhabdomyolysis or lower serum albumin levels.
The results revealed a deterioration in gait performance in this sample, with values diverging from those observed in healthy older adults populations. These findings align with data from similar studies available in the literature focusing on the analysis of functional levels and varied clinical contexts in older adult fallers.
However, it is important to note that this study has certain limitations, including its cross-sectional design, limited sample size, and lack of control over confounding variables.
It would be valuable to conduct prospective studies with larger samples and more in-depth statistical analyses to confirm these results and further explore the associations between biological markers, cognitive and functional abilities, and fall history with gait parameters.
In conclusion, this study contributes to understanding the factors influencing gait parameters in older adult individuals hospitalized after a fall. It highlights the importance of considering the multiple dimensions associated with gait in the assessment and management of these patients. From a clinical perspective, integrating gait analysis with biological and functional assessments may enhance geriatric evaluations and guide individualized rehabilitation strategies aimed at reducing fall risk and promoting recovery.
Footnotes
Ethical Considerations
The study was approved by the local ethics committee and was conducted following the principles of the Declaration of Helsinki. The study as the record number (ID-RCB) 2022-A01157-36 from the French National Agency for Medicines and Health Products Safety.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.