
Abstract
This study aimed to identify predictive risk patterns for older individuals who are likely or unlikely to reverse from frailty 3 years later using the Kihon Checklist (KCL) and a machine learning model. Data were collected from community-dwelling individuals aged 65 and over with frailty but without long-term care at baseline. A decision tree analysis revealed that the cognitive function domain of the KCL was the primary determinant of frailty reversal. Among those with low cognitive function, low physical activity predicted remaining frailty status 3 years later. The derived model achieved a specificity of 81.0% and a precision of 82.6% in predicting individuals with remaining persistent frailty. These findings suggest that the pattern combining cognitive and physical risk factors plays a key role in predicting frailty outcomes, and that the proposed model may be useful for screening individuals who require targeted interventions.
What This Paper Adds
This study is the first to utilize a decision tree model to examine complex, non-linear interactions among the Kihon Checklist domains in predicting frailty reversal in community-dwelling older individuals.
This study highlights a pattern combining cognitive and physical risk factors for predicting individuals likely to remain frailty, moving beyond traditional linear models like logistic regression.
Applications of the Study Findings
The proposed decision tree model provides an effective community-based screening tool that enables municipalities and health professionals to predict older individuals who are likely or unlikely to reverse frailty, facilitating early, and targeted interventions.
Policymakers can use these insights to design integrated frailty reversal strategies targeting both cognitive and physical domains, potentially enhancing the efficient resource allocation in community health planning.
Introduction
In nations with aging populations, enhanced health assessment methodologies for older individuals are necessary for the coordinated and integrated development of treatment plans and long-term care (Rudnicka et al., 2020). There has been an increased focus on frailty (Hoogendijk et al., 2019), which is an age-associated, nonspecific vulnerability characterized by declining function across multiple physiological systems (Fried et al., 2001; Hoogendijk et al., 2019; Rockwood & Mitnitski, 2007). Frailty exerts a detrimental influence on both a national level, where it leads to increased healthcare insurance costs (Makizako et al., 2021), and on an individual level, where it leads to a decline in individual quality of life (Kojima et al., 2016). To prevent those influences, some interventions have been suggested for reversing from frailty, such as low- to moderate-intensity exercise (Zang et al., 2025), individualized home-based interventions (Hsieh et al., 2019), or physical, nutritional and cognitive interventional approaches (Ng et al., 2015). Healthcare resources, however, are limited, the efficient and effective allocation of healthcare resources are necessary. Thus, there is a need for an effective community-based screening tool that can predict older individuals who are likely or unlikely to reverse from frailty, enabling specific interventions to be provided efficiently to targeted older individuals earlier.
Japan is aging faster than most other countries (Statistics Bureau, Ministry of Internal Affairs and Communications, 2023), making it a useful model for nations facing similar challenges. Japan’s strategy for healthy aging may offer lessons for other nations (Ikegami, 2019). The Japanese government developed the Kihon Checklist (KCL; The Japanese Ministry of Health Labor and Welfare, 2006), which is one of the candidate tools used to early predict older individuals who are likely or not likely to reverse from frailty (for detail, see “Methods” section). The KCL is a self-assessment questionnaire consisting of 25 yes or no items, with higher scores indicating a worse condition. The KCL encompasses seven domains, namely instrumental activities of daily living (IADL; five items), physical activity (five items), nutritional status (two items), oral function (three items), house-boundedness (two items), cognitive function (three items), and depressive mood (five items; Arai & Satake, 2015). The KCL score can also assess the phenotype of frailty status, with frailty and prefrailty defined with score cut-offs of 7/8 and 3/4, respectively (Fried et al., 2001; Satake et al., 2016). Previous studies have demonstrated that the KCL items and domains could predict the development of frailty from baseline until 5 or 6 years of follow-up (Imai et al., 2023; Ohashi et al., 2021). Notably, the KCL has been used by the municipal government to screen older individuals who are at risk of requiring care and at risk of long-term care insurance (LTCI) certification in Japan (Ito et al., 2021; Yamada & Arai, 2020). In addition, the KCL was translated into English (Arai & Satake, 2015), Chinese (Tao et al., 2020), and Spanish (Sentandreu-Mañó et al., 2021), thus ensuring its widespread use in frailty screening.
These previous uses of the KCL suggest its potential as an effective community-based screening tool for predicting older individuals who are likely or not likely to reverse from frailty. However, to the best of our knowledge, only one study has examined the predictors of reversal from frailty using the KCL (Imai et al., 2023). Imai et al. used logistic regression analysis to identify the predictors of the KCL, but this study had methodological issues with regards to the independence and linearity of independent variables (Sato (Osaki) et al., 2020). Furthermore, logistic regression analysis cannot simultaneously investigate multiple and heterogeneous relationships, wherein one predictor may have two or more types of relationships with a dependent variable (Sato (Osaki) et al., 2020). Thus, the existing model has limitations in capturing multiple and heterogeneous relationships. Decision tree analysis with Exhaustive Chi-squared Automatic Interaction Detector (E_CHAID) can address these limitations of independence, linearity and homogeneity (Sato (Osaki) et al., 2020). E_CHAID is a method of data mining that does not assume the aforementioned statistical assumptions of independence, linearity and homogeneity (Sato (Osaki) et al., 2020; Song & Lu, 2015). It can flexibly model the distribution and relationships of data, and its effectiveness in research related to older individuals care has been established (Sato (Osaki) et al., 2020). Decision tree techniques have also been widely used to construct classification models (Katayama et al., 2022), since these models are very similar to human reasoning and are easy to understand (Kotsiantis, 2013). Therefore, a decision model can serve as a useful tool in community-based screening. However, E_CHAID has not previously been used to create a decision model for predicting older individuals who are likely or not likely to reverse from frailty.
This study aims to identify predictive patterns among older individuals who are likely or not likely to reverse from frailty, as indicated by complex relationships among independent and dependent variables. A model evaluation was conducted to ascertain the precision of the derived model and determine its degree of usefulness. We believe that the derived model can be used by the municipal government or related clinical staff for screening older individuals in the community setting.
Methods
Study Population and Participants
This study was designed as a retrospective, longitudinal, and observational study, using the anonymized data provided by Iiyama City, Japan. This city has conducted an annual municipal government survey of older individuals who were not certified for LTCI in Iiyama City to examine the impacts of various factors, including KCL domains, on the risk of LTCI certification. Iiyama City is the most aged rural city in Nagano Prefecture with significant older individuals, making it a suitable data source for this study, since it provided a sufficient sample size. This study was approved by the Institutional Review Board of Nagano University of Health and Medicine (No. 2020-4). This study followed the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis-artificial intelligence (TRIPOD-AI) statement (Collins et al., 2024).
The process of participant selection is illustrated in Figure 1. The municipal government disseminated a survey to 6,123 older individuals aged ≥65 years on December 1, 2016, among which 5,368 provided responses. Responses with missing information were excluded, resulting in a total of 3,785 responses. The KCL classification (Satake et al., 2016) was used to categorize participants into three categories based on score: robustness (n = 2,350, KCL total score ≤ 3), prefrailty (n = 884, KCL total score 4–7) and frailty (n = 551, KCL total score ≥ 8). Among the 551 participants with frailty, 178 were deemed ineligible due to LTCI certification, death, or relocation to other cities during the period from December 1, 2016, to October 31, 2019. In 2019, 373 participants with frailty were surveyed again using the KCL, and 317 responded. After excluding 115 responses with missing information, the total sample size for analysis was 202 participants.

Flow diagram of participant selection.
Variables for Analysis
The independent variables were age, gender and the 6 KCL domains in 2016 (i.e., physical activity, nutritional status, oral function, house-boundedness, cognitive function, and depressive mood). The IADL domain was excluded because it had no published cut-off value (Satake et al., 2019). The dependent variable was frailty status defined using the KCL in 2019 (i.e., robustness, prefrailty, and frailty).
The KCL is a 25-item self-administered questionnaire to identify frail older individuals who are at risk of being newly certified for LTCI in the near future. Each question was rated on a yes/no basis, with positive responses assigned a value of 0 and negative responses assigned a value of 1. The total item score and the domain scores of seven were calculated. The total item score ranged from 0 to 25, with higher scores indicating poor function. During the initial evaluation in 2016, each domain was evaluated based on whether it was low or not (see the Supplemental material for calculation methods; Fukutomi et al., 2013; Satake et al., 2019). During the 2019 evaluation, frailty status was defined based on the KCL classification (Satake et al., 2016), wherein individuals with KCL total scores of ≤3, 4 to 7 and ≥8 were considered to have robustness, prefrailty, and frailty, respectively. Following a previous study (Imai et al., 2023), the improvement of KCL total scores from frailty to robustness or prefrailty was defined as a reversal from frailty.
Statistical Analysis: Classification and Evaluation
The total sample for analysis (n = 202) was divided into training and testing datasets with a 7:3 ratio. The training dataset was utilized to develop the predictive model, while the testing dataset was employed to evaluate its performance. As the quantity of the training set increased, the efficacy of the model’s learning process was enhanced. This, in turn, facilitated the transfer of the model’s learned principles to novel data (Sivakumar et al., 2024). Separating the testing dataset from the training set helped to reduce evaluation bias, which allowed the model’s performance to better reflect its ability to generalize to unseen data, rather than simply fitting the training data (Sivakumar et al., 2024). Regarding the dependent variables in the training dataset, 11, 36, and 94 participants, respectively, were considered to have robustness, prefrailty and frailty in 2019. This imbalance between classifications may be problematic because of the negative impact of machine learning algorithms on classification performance (Jeni et al., 2013). To address imbalanced datasets, Synthetic Minority Over-sampling Technique for Nominal Continuous (SMOTE-NC) was used to oversample the minority class (Chawla et al., 2002; Ganganwar, 2012). After implementing SMOTE-NC on the training dataset, the sample size was adjusted to 282, with 94 cases assigned to each of the dependent variables (i.e., robustness, prefrailty, and frailty; see Figure 1). The E_CHAID algorithm (a modification of the basic CHAID algorithm; Biggs et al., 1991; Kass, 1980) was utilized for the oversampled training dataset in order to construct the decision tree model. Notably, E_CHAID does not assume the statistical assumptions of independence, linearity and homogeneity (Sato (Osaki) et al., 2020; Song & Lu, 2015). The following settings were used: maximum tree depth = 3, minimum number of parent nodes = 100 and minimum number of child nodes = 50. The significance level for splitting nodes was set at p < .05 with Bonferroni correction, based on the chi-squared test, indicating that the differences between groups defined by the predictor were statistically significant (Biggs et al., 1991; Kass, 1980). The testing dataset was used to evaluate the model. Then, the derived model was evaluated via a multiclass confusion matrix using the one-against-all approach to calculate accuracy, sensitivity, specificity and precision (see the Supplemental material for details; Elsayad et al., 2018; Sathyanarayanan & Tantri, 2024). IBM SPSS Statistics 27 was used for decision tree analysis, and Python (ver. 3.11.7) was used for SMOTE-NC and model evaluation.
Results
Demographic Characteristics
The study cohort of 202 participants included 89 males and 113 females with a mean age of 75.9 (SD: 7.4) years. From 2016 to 2019, 16 participants reversed from frailty to robustness, 52 participants reversed from frailty to prefrailty, and 134 participants did not reverse from frailty (Table 1).
The Number of Status Transition from Frailty in 2016 to Each Status in 2019.

Decision Model
Figure 2 presents the decision tree model, which consists of three patterns: Node 2 (n = 138), Node 3 (n = 72), and Node 4 (n = 72). Among eight predictors (i.e., age, gender, physical activity, nutritional status, oral function, house-boundedness, cognitive function, and depressive mood), cognitive function was the most influential factor for reversing from frailty. Meanwhile, the presence of low physical activity concomitant with low cognitive function emerged as an influential factor associated with remaining frailty status.

Decision tree model for predicting reversal from frailty.
Node 2 showed that 65.2% of participants who did not have low cognitive function demonstrated a reversal from frailty. Node 3 showed that 70.8% of participants who had low cognitive function and low physical activity remained their frailty. Node 4 showed that 73.6% of participants who had low cognitive function but not low physical activity transitioned from frailty to prefrailty.
The results of model evaluation are shown in Table 2. For identifying robustness, the model had a classification accuracy of 57.4%, sensitivity of 20%, specificity of 60.7% and precision of 4.3%. For identifying prefrailty, the model had a classification accuracy of 65.6%, sensitivity of 31.3%, specificity of 77.8% and precision of 33.3%. For identifying frailty, the model had a classification accuracy of 59.0%, sensitivity of 47.5%, specificity of 81.0% and precision of 82.6%.
Performance Metrics of the Derived Decision Tree Model.
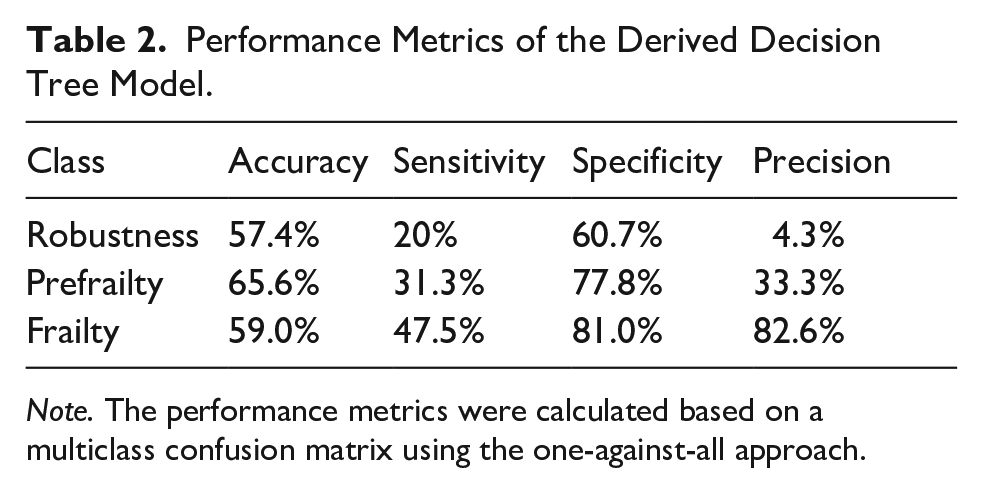
Note. The performance metrics were calculated based on a multiclass confusion matrix using the one-against-all approach.
Discussion
To the best of our knowledge, this is the first study to develop a decision tree model that can predict older individuals who are likely or unlikely to reverse from frailty. As illustrated in Table 1, approximately 33.7% of individuals categorized as frailty in 2016 reversed from frailty in 2019. The decision tree model analysis revealed that the cognitive function domain of the KCL was the strongest predictor for reversal from frailty. Meanwhile, the presence of low physical activity concomitant with low cognitive function emerged as an influential factor associated with remaining frailty. The derived model is effective in predicting older individuals with a high risk of difficulty in reversing from frailty 3 years later, with a precision of 82.6%. Furthermore, the model can also identify older individuals who are likely to reverse from frailty 3 years later, with a specificity of 81.0% for predicting frailty, although particular factors and patterns are unclear due to low precision for predicting robustness and prefrailty.
The cognitive function domain of the KCL was the most influential factor in determining reversal from frailty. Meanwhile, having low physical activity was a risk factor for remaining frailty status among those with low cognitive function. A previous study revealed that adding cognitive impairment to frailty enhanced its predictive validity for adverse health outcomes (Avila-Funes et al., 2009). Additionally, a recent meta-analysis indicated that frailty had a negative impact on cognitive function (Robinson et al., 2022). Furthermore, the previous studies examining association between frailty and cognitive impairment based on separate constructs indicated that the concomitant presence of frailty and cognitive impairment may lead to an exacerbation of disability, a decline in quality of life and increased morbidity and mortality (Avila-Funes et al., 2009; Fabrício et al., 2020; Xue et al., 2021). Therefore, coexisting low scores in both the cognitive and physical function domains among individuals with KCL total score ≥ 8 (i.e., frailty) may be indicative of advanced-stage frailty (Brigola et al., 2015). Consequently, among older individuals with frailty, having low scores in both the cognitive and physical function domains are likely to predict a lower likelihood of reversing from frailty. These results suggest the necessity of intensive interventions to promote frailty reversal—particularly those that simultaneously enhance both cognitive and physical functions, such as dance-based programs (H. Zhang et al., 2025; Zheng et al., 2022).
It is possible that the other KCL domains—including nutritional status, oral function, house-boundedness, and depressive mood—are less influential in predicting reversal from frailty, particularly among community-dwelling older adults. In this population, primary prevention of the onset or progression of frailty typically involves modifying unhealthy lifestyle behaviors (Hoogendijk et al., 2019). Lifestyle factors, including dietary patterns, are associated with nutritional status (Ledikwe et al., 2004), oral function and depressive symptoms (Kunugi, 2023). The ability to change one’s lifestyle may be supported by both physical and cognitive capacities (Berkman, 2018). A previous study also reported that lower cognitive function was associated with reduced engagement in IADL and less favorable lifestyle choices (Derakhshanrad & Zeynalzadeh Ghoochani, 2024). Therefore, aside from the cognitive and physical domains, the remaining KCL domains may have limited predictive value for frailty reversal.
The derived model had a specificity of 81.0% and a precision of 82.6% for predicting the remaining frailty status 3 years later based on the KCL. High specificity suggests that the derived model can capture effectively negative instances (Sathyanarayanan & Tantri, 2024), meaning that individuals without frailty (i.e., prefrailty or robustness) were correctly predicted to not have frailty at a rate of 81.0%. Meanwhile, high precision suggests that the derived model can make accurate positive predictions (Sathyanarayanan & Tantri, 2024), meaning that among those predicted to have frailty, 81.0% actually had frailty. Therefore, the derived model can effectively predict individuals who are likely or unlikely to reverse from frailty 3 years later. Although robustness and prefrailty could be individually identified by the derived model (i.e., Node 2 and Node 4), the sensitivity and precision were inadequate, making particular factors and patterns unclear. Nonetheless, the risk pattern combining the cognitive and physical function domains can be effective in predicting older individuals who are likely or unlikely to reverse from frailty, enabling specific interventions to be provided efficiently to targeted older individuals earlier. Compared to the previous model (Imai et al., 2023), we believe that our model can be useful in community-based screening because decision tree models are very similar to human reasoning and are easily understandable (Kotsiantis, 2013), facilitating the efficient and effective allocation of healthcare resources. In addition, the KCL—originally used in Japan to screen older adults at risk of LTCI certification—has been translated into multiple languages, which may facilitate its global applicability in predicting frailty reversal.
Limitations
The limitations of this study must be acknowledged. First, we did not consider other factors in making the model, such as comorbidities, educational level, presence of a spouse, and having a harmonious family relationship. Future studies must consider these factors, as they are known to influence frailty status (Y. Zhang et al., 2020). Moreover, when undertaking predictions, it is believed to be essential to undertake a personalized evaluation of the aforementioned factors, which has not been incorporated into this study, in order to identify the direction of intervention for each individual case. Second, the derived model was based on data from a single city in Japan, thereby limiting the generalizability of the findings. Thirdly, given that the KCL is a self-reported outcome, the definition of frailty status was dependent on the self-reported data. This was subject to bias and inaccuracy, particularly among aged individuals with cognitive impairment. Future studies should consider incorporating objective expert evaluations and include other older individuals to enhance the reliability and validity of the research findings. Lastly, although the derived model could capture robustness and prefrailty, it had inadequate sensitivity and precision. Consequently, the factors that influence a reversal from frailty to robustness or prefrailty remain ambiguous. Future studies should aim to enhance the predictive model, which can be achieved by increasing the sample size and incorporating additional factors.
Conclusions
This study investigated the risk patterns for predicting older individuals who are likely or unlikely to reverse from frailty 3 years later using decision tree analysis. The cognitive function domain of the KCL was the primary determinant of the reversal from frailty to robustness. Moreover, among older individuals with low cognitive function, low physical activity was a strong predictor for remaining frailty status 3 years later. The derived model exhibited a specificity of 81.0% and a precision of 82.6% for predicting the remaining frailty status 3 years later based on the KCL. These results emphasize that among older individuals with frailty, the risk pattern combining the cognitive and physical function domains can be effective in predicting older individuals who are likely or unlikely to reverse from frailty, enabling specific interventions to be provided efficiently to targeted older individuals earlier.
Supplemental Material
sj-docx-1-ggm-10.1177_30495334251365595 – Supplemental material for A Pattern Combining the Cognitive and Physical Risks Predicts Frailty Reversal in Community-Dwelling Older Individuals 3 years Later: A Decision Tree Analysis
Supplemental material, sj-docx-1-ggm-10.1177_30495334251365595 for A Pattern Combining the Cognitive and Physical Risks Predicts Frailty Reversal in Community-Dwelling Older Individuals 3 years Later: A Decision Tree Analysis by Noriki Yamaya, Tomomi Furukawa, Kazuki Kitazawa, Kazuki Hirao, Takaaki Fujita, Fusae Tozato, Yayoi Kitamura, Naoyuki Oi, Tsutomu Iwaya and Kenji Tsuchiya in Sage Open Aging
Footnotes
Acknowledgements
We would like to express our gratitude to Iiyama City for their cooperation in the completion of this study. Additionally, we would like to thank Megumi Shinji at Statcom for assistance in the organization of the data.
Ethics Considerations
This study was approved by the Institutional Review Board of Nagano University of Health and Medicine (No. 2020-4).
Consent to Participate
Informed consent was not required, as the study utilized anonymized data provided by Iiyama City, which had conducted an annual municipal survey of older adults in Iiyama City, Nagano Prefecture, Japan.
Author Contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Health Labour and Welfare (23GC2001) and JSPS KAKENHI Grant (21K17421).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The study protocol, data, and code remain unavailable due to its non-approval by the Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.