
Abstract
Any effective intervention for elder abuse should start from the perspectives and needs of all stakeholders, including the older persons themselves. Based on face-to-face interviews, this descriptive qualitative study explored the different stakeholders’ perspectives and the challenging obstacles in preventing, detecting and addressing elder abuse. The purposive sample included patients and experienced professionals such as nurses, GPs, social workers, notaries, lawyers and judges. The main themes identified were the empowerment of older persons, the need for sensitisation of all key actors, deontological issues and the need for and barriers to interprofessional collaboration. The findings highlight the complexity of elder abuse, the vulnerability of victims, their reluctance to request help and the potential for abuse of powers of attorney. Healthcare professionals identified a tension between maintaining a trust-based relationship and the obligations of secrecy inherent in their professional and interprofessional roles. They advocate for developing and implementing an interprofessional collaboration model that can overcome the obstacles for collaboration and integrate the patient’s perspective.
Introduction
Abuse affects one in six older persons worldwide, about 141 million people with a prevalence rate of 15.7% (Yon et al., 2017). A systematic review by Yon et al. found that 64.2% of nursing home staff admitted to elder abuse within the past year (Yon et al., 2019). A 2010 Belgian study reported a 32% prevalence among women over 60 years old (De Donder & Verté, 2010).
In Flanders, 967 incidents of elder abuse and intimate partner violence were reported in 2021 by the Flemish Support Centre for Elder Abuse (VLOCO). These data, collected from the professional hotline on violence (‘1712’), the 11 Centres for General Welfare Work and VLOCO’s data on caregiver requests, are likely an underestimate (VLOCO, 2021). The growing older population is expected to increase the number of those at risk of abuse (United Nations, 2019). The COVID-19 pandemic has exacerbated the situation, with restrictive measures in nursing homes, assisted living facilities and at home, leading to increased social isolation, psychological distress, and higher vulnerability to abuse (Makaroun et al., 2020). Addressing elder abuse is urgent, given its severe consequences for the victims, such as physical health problems, including increased hospitalisation and mortality; psychological distress; and loss of property and security (Dong, 2015). However, elder abuse remains a relatively neglected problem in Belgium, where policies mainly address partner and child abuse.
Despite calls from the World Health Organization and the International Network for the Prevention of Elder Abuse (INPEA), elder abuse remains a low priority globally due to limited interest of policymakers, lack of organisational and individual leadership and disagreement on prevention and intervention strategies (Mikton et al., 2022). The United Nations Decade of Healthy Ageing 2021–2030 offers an unique opportunity to address elder abuse through a coordinated global collaboration involving governments, civil society, international agencies, professionals, academia, media and the private sector, aiming to improve the lives of older persons, their families, and their communities (World Health Organization, 2022).
Despite the significant impact of abuse on older persons and society, comprehensive research remains limited (Marshall et al., 2020). The first problem is that elder abuse often goes undetected (Sethi et al., 2011), as many victims are reluctant to report due to fear of retaliation (Burnes et al., 2019). Healthcare, social welfare and legal professionals are crucial in detecting and reporting elder abuse, but they are currently ill-equipped and face barriers such as a lack of appropriate skills and validated tools, and obligations to maintain professional secrecy (Gallione et al., 2017; Ries & Mansfield, 2018; Schmeidel et al., 2012; Van Royen et al., 2020). Another major concern is the profound lack of knowledge about the circumstances of elder abuse as well as the scarcity of effective interventions (Fearing et al., 2017; World Health Organization, 2022). In Belgium, research on elder abuse is largely absent, resulting in a fragmented approach and insufficient awareness. Moreover, there is little focus on the unique perspectives and needs of older persons in addressing abuse (Ludvigsson et al., 2022).
Addressing the complex issue of elder abuse requires close collaboration among various sectors and professionals (Marshall et al., 2020). However, despite strong advocacy for a multidisciplinary approach, there is limited evidence on how to implement this effectively. This study aims to gain a detailed understanding of the perspectives and roles of all actors involved (older persons, informal/volunteer caregivers, and healthcare, social welfare, and legal professionals), while also examining relevant legal and deontological issues and improving knowledge on interprofessional collaboration in this field.
Methodology
This descriptive qualitative study used semi-structured interviews to explore the perspectives and experiences of all involved professionals on elder abuse. The research was conducted by the Department of Family Medicine and Population Health and the Research Group on Personality Rights and Property Rights at the University of Antwerp. Additionally, data from a 2021–2022 interview study involving older persons and nurses in home care were re-analysed and incorporated in this paper.
An advisory board of experts from the fields of welfare, healthcare and justice, and representatives of older persons (n = 30) functioned as a peer review group to ensure the study’s rigour and relevance.
Belgian Context
Belgium is a complex country with several governments namely a federal and one for each of the regions, Flandres and Walloon. Some responsibilities are federal, and some are regional.
Welfare and preventive health care is the responsibility of Flandres, and justice and medical care are federal responsibilities. ‘De Orde van Artsen’ is a committee of physicians and a magistrate, taking care of the deontological aspects. If physicians don’t keep their professional secret, they can have a sanction even losing their permit to work. Citizens can also go to court when a physician don’t keep their professional secret.
There is an organization VLOKO, who has a reporting point for maltreatment of older people, but there are not so many cases reported. They only give some general advice.
The Flemish government has also a reporting point called 1,712 but it is for all cases of maltreatment (children, partners, older people). There is no specific programme for older people (Ricour et al., 2020).
Study Population
A purposeful sample of two relevant stakeholder groups was recruited: healthcare providers and legal professionals. Inclusion criteria for healthcare providers were being a general practitioner (GP) who cares for older persons or a geriatric specialist, with at least 5 years of experience and ideally familiarity with elder abuse. Legal professionals consisted of lawyers, prosecutors, justices of the peace and notaries, also with a minimum of 5 years of experience with issues related to elder abuse. GPs were recruited from local GP circles and by snowballing, while geriatric specialists were identified and contacted through the network of the Department of Family Medicine and Population Health. For healthcare providers working within an organisation, permission was obtained from management prior to participation. Legal experts were identified and contacted through the network of the Research Group on Personality Rights and Property Rights, and by snowballing.
Data Collection
Data were collected through individual semi-structured interviews, based on a topic guide tailored by the research and stakeholder group. The initial topic guide was developed based on earlier interviews with nurses and patients and further enriched with information derived from the literature (Table 1). Following a pilot interview, the research team performed a preliminary analysis and refined the topic guide accordingly.
Topic List.

All interviews with healthcare providers were conducted by a doctoral student in medicine (NA), while those with legal professionals were conducted by a researcher from the faculty of law (MC). Both interviewers were female and had no prior relationship with the participants. During and immediately after the interviews they took field notes to capture the most important issues and attitudes of respondents.
Data collection took place both face-to-face and online from September 2022 to May 2023. Interviews lasted between 45 and 60 min and were held at a location chosen by the respondent. All recordings were transcribed verbatim by two master’s students under a confidentiality clause. Data was collected until data sufficiency was reached to comprehensively answer the research question.
Data Analysis
The analysis used a descriptive adaptive framework combining inductive and deductive methods (Gale et al., 2013; Ward et al., 2013) . Before data collection, researchers identified key concepts based on a literature review and prior interviews with patients and nurses. Subsequently, a minimum of two interviews per stakeholder group were thematically analysed using an inductive approach. Transcripts were divided into meaningful segments and tagged with descriptive codes and later with interpretative codes, which were organised into a codebook. The research team then examined the relationships between the themes structured within the framework. The final framework was collaboratively constructed by the entire research team (NA, MC, LP, HB), adjusted until consensus was reached, and then used for further analysis. The framework was adaptive, allowing the incorporation of new codes as the analysis progressed. Further analysis was conducted using QSR NVivo software version 1.5.1.
To strengthen internal validity, the research team employed a cyclic process and practiced reflexivity. Finally, researchers conducted both within-case analysis to understand individual cases, and cross-case analysis to identify themes across cases and stakeholder groups. Results were regularly discussed with the advisory board, whose feedback was used to develop the next phases of the project.
Ethical approval was obtained from the Ethics Committee for the Social Sciences and Humanities (EASHW, number SHW_2022_86). Ethical approval for the earlier interview study involving older persons and nurses in home care was granted by the Commissions for Medical Ethics of both the Hospital Network Antwerp (ZNA) and the University Hospital Antwerp (UZA, number 5398)’.
Results
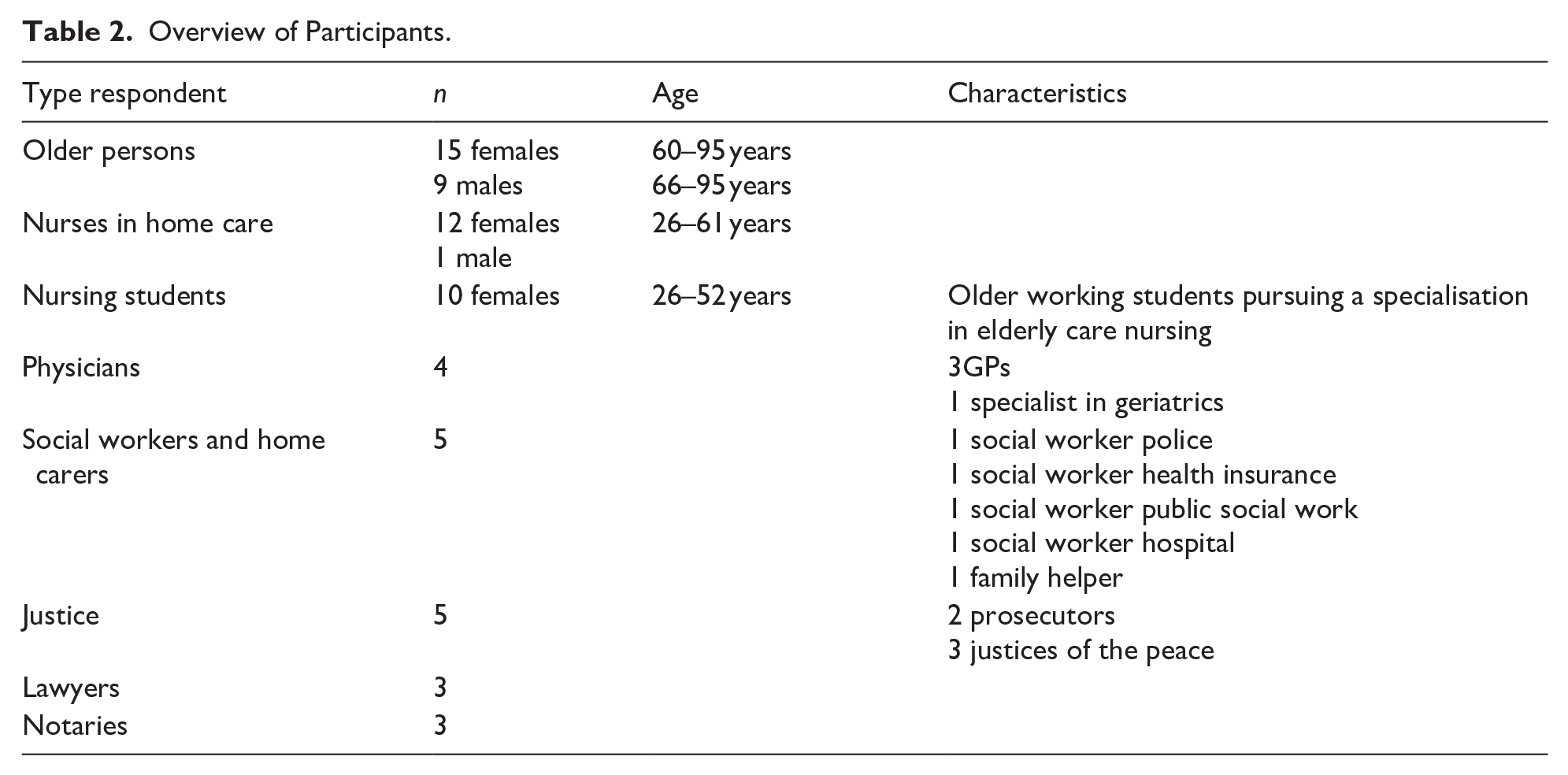
Table 2 provides a detailed overview of the respondents who participated in the study.
Overview of Participants.
Five themes emerged from the data: (1) the concept of elder abuse; (2) the empowerment of older persons; (3) the need to sensitise key actors about elder abuse; (4) challenges related to deontological obligations; and (5) the need for and barriers to interprofessional collaboration.
The Concept of Elder Abuse Through the Eyes of Older Persons
Most older persons are unaware of the concept of elder abuse. When they did mention abuse, it was mainly in the context of financial or physical abuse tied to long-standing domestic violence. Previous child abuse by parents often resulted in these children becoming perpetrators themselves. Many older persons shared stories of derailed care or neglect due to high work pressure in nursing homes and home care. Hidden forms of elder abuse included verbal aggression, healthcare workers who were unfit for the job, withholding of appropriate medical care, even by physicians, and financial abuse by healthcare workers. Nursing students working in nursing homes reported witnessing residents experiencing a loss of autonomy, disrespect and neglect. Additionally, they noted that healthcare workers often struggle to communicate appropriately with older persons due to a lack of language proficiency or the use of infantilising language.
Elder abuse is a very broad concept, I think, because you can do something physical, and you can pinch someone when you want to help her. But recently, I heard someone who wanted to go to the toilet, and then the nurse said: ‘you don’t need to go, just hold it, I’m not going to help you. (Student, 51 years) Yes, with words especially. Also, that, for example, when setting the table, they skip you and so on, do not serve you those things and food. I find all that incomprehensible. . . . I think sometimes mental abuse is more important than physical. (Older person, 65 years)
Interviewed older persons cited shame and fear of worsening the situation as the main reasons for not reporting abuse.
I think that’s hard to admit that. Or having to tell someone. . . Shame huh. . . I would be ashamed of myself. (Older women, 84 years)
Empowering Older Persons
Autonomy and dignity are crucial for the quality of life in older persons. Fear of losing autonomy is an important barrier to seeking help, although good care sometimes requires making decisions for older persons who live in very bad conditions. Knowledge of advance care plans was very limited, and older persons found their GP the most trustworthy person to talk to.
I believe that older persons should be able to retain their independence and dignity for as long as possible. And that is mainly by being able to live at home and make your own decisions. But sometimes . . . no matter how difficult it is, I think you have to dare to make a decision and say: this is no longer possible. (Social worker police) If I really can’t do it anymore and I can’t take care of myself anymore, I ask for euthanasia. I don’t want to go through that. Oh no, I’m very afraid of that. (Woman, 60 years)
Cognitive decline, social isolation, complex family dynamics and lack of resources increase the risk of maltreatment for older persons, as suggested by the interviewed stakeholders.
I think it’s very sad that even healthcare providers take advantage of those people because they were suffering from dementia, and they had no idea what was happening to them. (GP) One of the first things that often comes to mind, is the material itself. For example, an older person with an incontinence problem, who only has a limited pension, the mattress is permeated with urine. Do we buy a new mattress for our mother? No, because it costs too much money. And the children manage the budget, so it is sometimes a bit of a struggle to get that done. (Professional caregiver)
Raising awareness about elder abuse is crucial for prevention. Older people need support to overcome shame associated with their situation and the fear of losing their relationship with their family. Healthcare providers, especially GPs, are well-positioned to inform them about protective legal instruments. However, empowering and protecting older persons can sometimes jeopardise their fragile family relationships.
If you’re like, “Yes, I’m the representative, I’m the advocate of the older person as a GP,” then of course you put yourself in a situation where it is possible that the family turns completely against you. And then they say, “That’s not a good GP, you should get another GP.” (GP)
The Need of Sensitisation of Key Actors About Elder Abuse
The complexity of elder abuse highlights the urgent need for sensitising and educating professionals. Older persons often ignore or avoid discussing maltreatment, which underscores the importance of the competencies of professionals in recognising these issues.
It’s not so straightforward. That depends very much on who those people end up with. Some people will be much more susceptible to noticing those signals and may be more likely to worry about them or start addressing them. (Solidaris, social worker health assurance)
Awareness increases when attention to elderly maltreatment is embedded in the organisation’s vision and mission, and when a specific protocol is in place. There is also a need to develop communication skills and competencies for detecting maltreatment. None of the healthcare providers reported using a tool for screening and detecting elder abuse.
While discussing concerns with healthcare providers is a first step, most older persons experience no further action being taken. Reporting is often perceived as ineffective due to a lack of appropriate support.
Yes, I then called that hotline for elder abuse. But yes . . . it didn’t really help me much. On one hand, because it made me feel very hard like: “You’re doing a good job.” But on the other hand, it made me feel very hard like: “You have a very hard dilemma here, see that you intervene in time, because that is your duty, but you must not break your professional secrecy, because then you will also be in trouble.” And then I was like, ‘Yes, but why am I calling you?’ (OCMW) – about the Flemish Support Centre for Elder Abuse (VLOCO)
Challenges Related to Deontological Obligations
Struggles With Ethical Boundaries
GPs often face the challenges of balancing respect for an older person’s autonomy with the need to address abusive situations. The focus remains on patient-centeredness, yet the perspectives of the older person and the healthcare provider can differ significantly. Maintaining trust while managing derailed care or even abuse is a delicate and complex ethical issue.
That is something that is very sensitive and that is a bit of a search of where is the line to make a statement about this. But that is also a very long process. And you lose the patient’s trust very quickly. At a certain point, I said something, and she dismissed me as her GP. (GP)
Lasting Powers of Attorney
Both older persons and healthcare providers are often unaware of existing legal protective measures, such as lasting powers of attorney. This tool allows older persons to appoint a representative, supporting their autonomy in advance care planning. This representative is supposed to have a relationship of trust with the older person.
However, legal professionals warned that this instrument can be misused to facilitate financial abuse instead of preventing it, especially when there is insufficient supervision. In Belgium, notaries responsible for drafting these documents are also tasked with providing internal control but may sometimes side more with the representative than with the older person. Lawyers and judges were very critical of this procedure, while notaries tended to be more supportive. Judges suggested implementing an ‘alarm bell procedure’ before the justice of the peace for better control and protection.
Yes, a notary should normally refuse to perform their duties if they believe someone is no longer of sound mind. That’s a civil servant. That goes of course. . . often family notaries handle these cases. . . I’m not going to say any more about that. . . that’s not always a guarantee. (Lawyer) Sometimes you indeed have situations where a mother and a son are together here for a will. If that happens and there are other children, I will always ask the son to leave. ‘Ask to leave’ is an exaggeration (. . .). That mother should be able to tell her story alone. (Notary)
Professional Secrecy
A lack of understanding about professional secrecy causes many healthcare providers to fear legal repercussions for breaches. They reported challenges in balancing the protection of their patients, maintaining trust and adhering to professional secrecy obligations. In contrast, attorneys indicated that such fears are often unfounded, as breaches of professional secrecy would very rarely lead to prosecution.
But when I give training to social services, I always say: “In all those years that I have been a magistrate, I have never seen anyone prosecuted for violation of professional secrecy, only for culpable negligence.” And then I hope that gets through, because I think that’s really the big issue. (Public prosecutor)
The Need for and Barriers to Interprofessional Collaboration
Currently, effective elder abuse intervention depends heavily on personal initiative and existing relationships among professionals, resulting in fragmented care. The lack of robust and detailed protocols means complex situations are often inadequately addressed.
Healthcare providers advocate for establishing interprofessional local advisory groups that include representatives from justice, healthcare and welfare sectors to discuss specific cases. Additionally, they emphasised the need for policymakers and deontological bodies to provide clearer guidelines on handling professional secrecy in cases of suspected elder abuse.
It’s useful to meet other professionals in person and learn what all those services and organizations can bring to the table in certain situations. This creates mutual trust and a social map of the network around a client (police service social assistant) There must be a health care team with professionals, who trust each other. That’s the ideal world, that there is a health care team with legal support looking for a few patients (GP)
Discussion
Healthcare providers and legal professionals must navigate a delicate balance between maintaining trust, protecting older persons and respecting their autonomy. Often, older persons may not recognise their abuse or neglect or may feel too ashamed to report it.
In our study, no participants used screening tools for early detection of elder abuse. There is ongoing debate whether it is ethical to perform screening without evidence from randomised clinical trials (Feltner et al., 2018). Only one study (n = 139) assessed the accuracy of screening for elder abuse among older persons presenting for routine dental care (Fulmer et al., 2012). Screening was conducted using the 15-item Hwalek-Sengstock Elder Abuse Screening Test (H-S/EAST), compared against the Conflicts Tactics Scale CTS (Neale et al., 1991; Straus et al., 1996). This group exhibited a relatively high prevalence of elder maltreatment based on CTS violence or verbal aggression scales (41%). Compared with the CTS (violence and verbal aggression scales combined), the H-S/EAST tool had a sensitivity of 46% (95% CI, 32%–59%) and a specificity of 73% (95% CI, 62%–82%) for detecting elder abuse.
Van Royen et al.’s scoping review of assessment tools highlighted that current tools lack validation and adaptation for at-risk groups, and none were suitable for use in primary care (Van Royen et al., 2020). Additionally, there is concern about the lack of attention to preventing the adverse effects of assessments and interventions (Perel-Levin & World Health Organization, 2008; Van Royen et al., 2020). This is in line with our findings that older persons fear losing autonomy and harming family relationships.
Abuse poses significant challenges for care teams, who must balance the rights and freedoms of older persons who have been abused with concerns for their safety. This dual commitment by staff and other caregivers may unintentionally infringe upon the patient’s right to autonomy (Saghafi et al., 2019).
Empowering older persons, raising caregiver awareness and improving communication skills are essential for prevention (Mydin & Othman, 2020). Mydin et al. recommend educational interventions tailored to the needs of healthcare professionals. These interventions should be problem-based and include face-to-face teaching, role-play and case simulations, addressing the issues of elder abuse and neglect. While e-learning platforms can increase knowledge, they do not necessarily enhance skills and attitudes (Mydin et al., 2021). During our interviews, healthcare providers, welfare workers, and even legal professionals emphasised the need for developing practical skills, noting that most educational tools on elder abuse consist of webinars and e-learnings focused on theoretical knowledge.
Another significant factor contributing to the low reporting rates of elder abuse is concern over professional secrecy. Healthcare providers often lack a clear understanding of the legislation governing professional secrecy and the ambiguities inherent in interprofessional collaboration. In many countries, the absence of clear legislation is a major obstacle to reporting elder abuse and protecting the rights of older persons. Confidentiality issues were a particularly controversial topic in our study. Donovan noted that care teams can disclose information in cases of serious harm without informing the victim, which aligns with the views of the legal professionals we interviewed and the deontological code in Belgium (Donovan & Regehr, 2010). However, vague definitions, concerns about respecting autonomy, and fears of deontological sanctions make reporting a challenge for healthcare professionals (Saghafi et al., 2019).
All professionals in our study agreed on the lack of effective interprofessional interventions for addressing elder abuse. One existing protocol was deemed too generic to be useful in daily practice (Ricour et al., 2020). Given the complexity of elder abuse, the consensus is that the gold standard for interventions involves a multidisciplinary team collaborating with both the legal and social sectors (Blowers et al., 2012; Pillemer et al., 2016; Twomey et al., 2010).
Strengths and Limitations
Triangulating data from interviews with older persons and various professionals strongly validates the identified themes. Researcher triangulation was achieved by combining analyses conducted by both legal and healthcare researchers.
A notable limitation of the study was the difficulty in including older persons who had directly experienced abuse.
Future research should focus on improving legal instruments, particularly addressing the risks associated with lasting powers of attorney. Interventions should be conceptualised from the bottom up, incorporating multidisciplinary perspectives while respecting the older person’s perspective and considering quaternary prevention (Van Royen et al., 2020).
Governments must invest in campaigns to raise awareness about elder abuse, especially among older persons, rather than focusing only on child abuse and domestic violence. The absence of comprehensive legal and ethical regulations creates many ambiguities in interpreting the applicable ethical and legal codes, leading to severe underreporting of abuse by care teams. Deontological bodies should establish clear guidelines and ethical principles specific to elder abuse. Additionally, more robust protections are needed for healthcare providers confronted with suspicions of elder abuse (Perel-Levin & World Health Organization, 2008).
Conclusion
The complexities of elder abuse challenge the development and implementation of an effective interprofessional collaboration model. This model should be able to overcome the obstacles to collaboration between healthcare, welfare and legal professionals, while considering the patient’s perspective. Older persons often fear losing autonomy and hesitate to report abuse because interventions frequently fail to meet their expectations. This highlights the urgent need for better-informed and more effective approaches to addressing elder abuse.
Footnotes
Ethical Considerations
Ethics Committee for the Social Sciences and Humanities, file SHW_2022_86_1
Approved on December 15th, 2022.
Consent to Participate
Because of the informed consent transcripts of the interviews are not available for a third party. The documents of the coding process are available.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University Antwerp Research Fund.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.