
Abstract
The home care workforce provides essential support for older people with dementia to live a life of fulfillment. “Enabling Choices,” an evidence-informed conversation tool, aims to negotiate risk around everyday activities between home care workers, people with dementia and their informal carers. This paper describes tool conversion into electronic format and preparation for implementation throughout a large Australian health and aged care service provider, utilizing the Implementation Framework for Aged Care (IFAC). Using codesign principles, the tool was converted from paper-based to electronic format involving frontline, operational and Information Management Services staff, and people with dementia/carers. Focus groups and interviews identified tool acceptability, feasibility, and appropriateness. For implementation preparation, the wider socio-cultural-political context was mapped, and key questions of the IFAC addressed. Environment, workflow, and training requirements were determined, and strategies for behavior change ascertained. Numerous opportunities and challenges exist for the widespread upscale of an evidence-informed tool into practice.
What this Paper Adds
Collaborative care partnerships based upon shared decision-making, as in the case of this tool, foster dignity and autonomy for the person with dementia.
To maximize the systematic uptake of a tool into practice, planning must be comprehensive, relevant, and adaptive.
Applications of Study Findings
Frontline workers, people with dementia and their carers value a shared decision-making approach for often difficult conversations.
Key questions of a fit-for-purpose framework guide implementation: (1) why we need to change; (2) what we know; (3) who will benefit; (4) who will make the change; and (5) what strategies will be used.
Mapping of the context identified factors associated with national aged care reforms and organizational requirements, with both limitations and opportunities affecting implementation.
Introduction
Within the Australian community care context, the home care workforce is essential to support people with dementia to continue living in their own homes as long as they are safely able. Globally, approximately 50 million people are living with dementia (Alzheimer’s Disease International, 2020), while in Australia, a relatively sparsely populated country, there are almost half a million people living with the disease, of which ~65% are living in the community (Dementia Australia, 2018). In Australia, lower levels of support for personal and instrumental activities of daily living are provided through the Commonwealth Home Support Program, while higher levels of support are provided through the Home Care Packages Program, with a supplement for those living with moderate to severe levels of cognitive impairment, including dementia (Australian Government, 2022). The vision of the WHO Global action plan on the public health response to dementia is for people with dementia to receive the care and support they require to live life with dignity, respect, autonomy, and equality (World Health Organization [WHO], 2017). This is predicated on collaborative care partnerships, between the home care workforce, people with dementia and their informal carers, with shared decision-making principles fostering dignity and autonomy for the person with dementia (Hirschman & Hodgson, 2018; O’Shea et al., 2017; Phillipson & Jones, 2011).
Dementia is an umbrella term for impairments in brain function that can affect memory, perception, language, and judgment (Australian Institute of Health and Welfare, 2022). Timely diagnosis of dementia is recommended (Pond et al., 2019), yet it is often associated with an overly cautious approach to risk that fails to balance the positive aspects and benefits against protection and risk avoidance (Manthorpe & Moriaty, 2010). Family members may be required to negotiate risk related to a decline in functional activities (Berry et al., 2015), with ethical dilemmas raised when aligning non-maleficence with promoting autonomy of the person with dementia (Smebye et al., 2016).
A paternalistic approach to risk intersects with rights of people with dementia and debates regarding substitute decision-making. The progressive nature of dementia over time lends itself to a spectrum of decision-making involvement (both formal and informal) from joint, through to supported and then substitute decision-making (Sinclair et al., 2019). In the context of community care, negotiating risk in activities of daily living can follow this approach depending on the level of cognitive impairment, needs, and preferences (Dickins et al., 2018). In line with this, a risk negotiation discussion tool was codesigned with people with dementia, informal carers, and community aged care staff, with 12 areas of activities of daily living with potential risks consolidated from 59 original items (Goeman et al., 2017). This “Enabling Choices” tool was developed and deemed acceptable for identifying and addressing concerns, supportive of the dignity and autonomy of the person with dementia (Goeman et al., 2017). To ensure uptake of such a tool into practice, implementation science principles are of value to embed it within the community aged care context.
Implementation of any tool into practice is complex, messy and predicated upon social relations and contextual factors (Braithwaite et al., 2018; Sturmberg et al., 2021). To maximize the systematic uptake of a tool into practice, planning must be comprehensive, relevant, and adaptive (Meyer et al., 2022). Numerous implementation frameworks exist but operationalizing the complex facets of implementation is challenging. The fit-for-purpose Implementation Framework for Aged Care (IFAC) is underpinned by Normalization Process Theory, focusing on how social processes are crucial to integrating implementation principles for change in practice (Meyer et al., 2022). This paper describes the conversion of the original paper-based tool into electronic format, utilizing codesign principles, and preparation for implementation with the IFAC throughout a large Australian health and aged care service provider.
Methods
Study Design
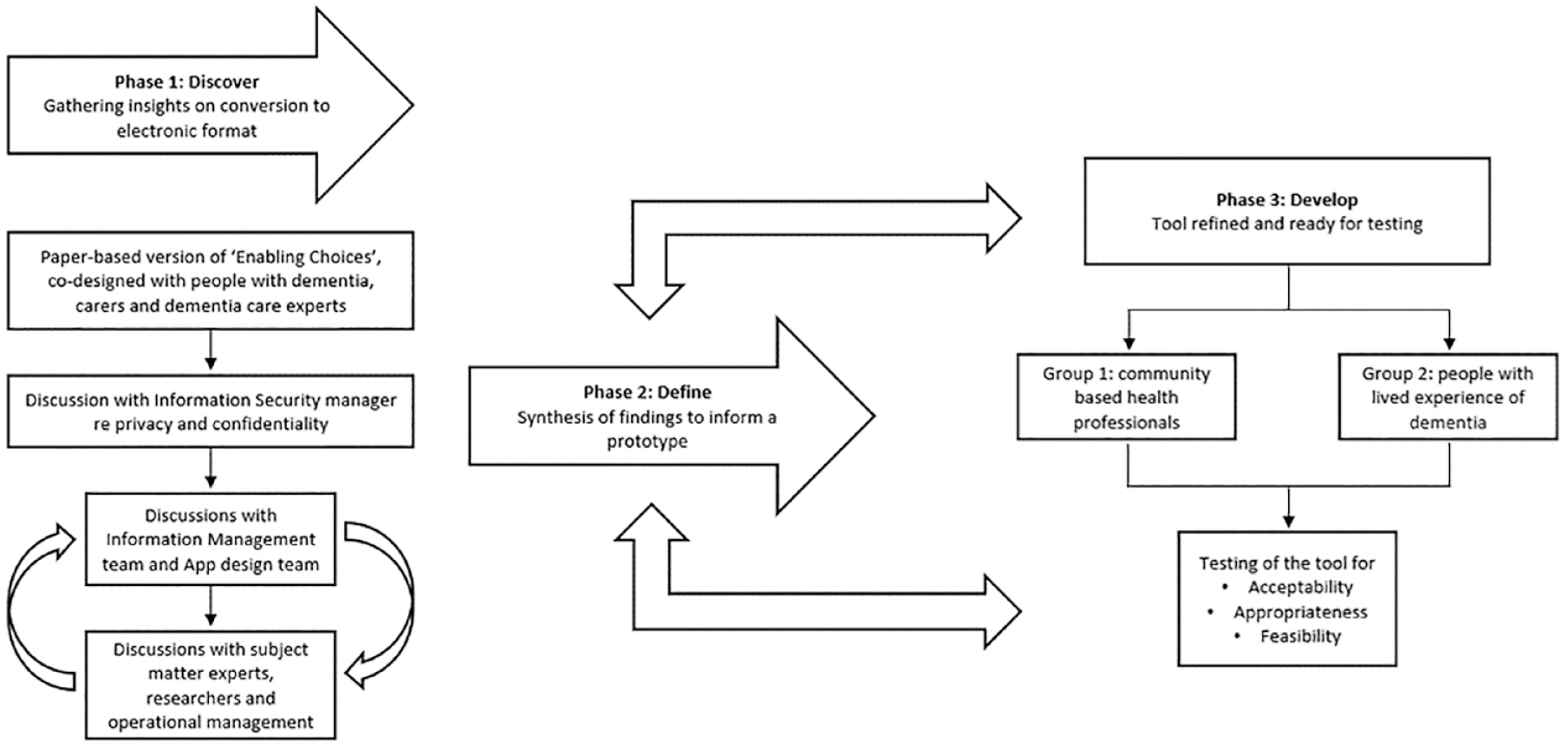
This study was underpinned by the IFAC, with five of the six questions addressed (Figure 1). The final question is being addressed through ongoing work. A co-design approach was utilized (Figure 2) drawing on a combination of the Design Council’s Double Diamond Framework (Design Council, 2015) and Boyd’s six-stage process of “engage, plan, explore, develop, decide, and change” (Boyd et al., 2012).

Implementation framework for aged care (IFAC).

Co-design approach as embedded within IFAC.
Participants
The co-design approach involved the organization’s Information Management Services team members, researchers, dementia care specialist staff, operational managers, people living with dementia and their carers. Participants were either employees or clientele of Bolton Clarke, a large, Australian aged care provider of community-based, retirement living, and residential care services. Research Institute team members (authors CM, MD) led the project, with MD being instrumental in the development of the original paper-based version of the tool (Goeman et al., 2017), and CM and JL having implementation expertise. Information Management Services team members were based in Melbourne and Brisbane, Australia. Within Bolton Clarke, this team have responsibility for ensuring information is managed and governed across the organization, including safeguarding critical private and confidential information. Dementia care specialist staff included author FO, the Senior Clinical Nurse Advisor (Dementia and Aged Care), who advise on clinical direction, reform, and policy frameworks, Dementia Clinical Nurse Consultants (including author KH), who contribute to expert knowledge translation, health education and research, and a social worker, who undertake holistic psycho-social assessment and care planning. Operational Managers support an extensive team of frontline workers (nurses, personal care workers, and allied health) to assist older people with dementia to remain living in their own homes and upholding their right to choice and dignity. Older people with dementia and their carers receiving community services from Bolton Clarke (n = 61) were involved in the development of the paper-based version of the tool (Goeman et al., 2017). They were to be a critical part of this project, but unfortunately the ongoing impact of the COVID-19 pandemic precluded their involvement beyond one dyad. Evaluation of the tool with this population is planned in the next stage of work.
Methodology
Phase 1: Discover—gathering insights on conversion to electronic format
This phase included the establishment of relationships between the Bolton Clarke Research Institute, Information Services—Management and Security team members, dementia care specialist nurses, operational managers, and a social worker. Shared insights and goals were identified through regular individual and Steering Group meetings. People with dementia and their carers were not involved in this phase due to the impact of the COVID-19 pandemic; however, findings from their involvement in the development of the paper-based version (Goeman et al., 2017) were used to inform the content of the tool (i.e., the electronic version of the tool did not deviate from the content proposed in the paper-based version).
Phase 2: Define—synthesis of findings to inform a prototype “Enabling Choices” tool
Data from Phase 1 were synthesized by members of the project team, reviewing and drawing together disparate views and opinions into a common understanding of the key components of the electronic version of “Enabling Choices.”
Phase 3: Develop—“Enabling Choices” tool refined and ready for testing
A prototype of “Enabling Choices” was developed, ready for preliminary testing. Two groups of participants were recruited for Phase 3: Group 1 were staff members who routinely provided care for people with dementia; and Group 2 were people with dementia and their carers.
Recruitment of Group 1 (staff members)
Participants were Bolton Clarke community health professionals providing in-home care to people with dementia or cognitive impairment across Melbourne and the south-east region of Queensland, Australia. Participants were providing care for older people under the Commonwealth Home Support Program (entry level support for older people requiring some help to remain living at home) and the Home Care Package Program (designed for older people with more complex care needs). Participants included registered nurses, clinical nurse consultants, and care managers. Members of the project team, in consultation with operational managers, identified staff members who might be interested in participating, approaching them via verbal and/or electronic communication to ascertain interest. Potential participants were informed that project participation was voluntary and was fully supported by Executive and Operational Management. A Participant Information and Consent Form (PICF) was circulated electronically 1 week prior to attendance at the training session to ensure sufficient time to read and ask questions, with a signed copy of the PICF received by the project team prior to testing of the tool. All participants were free to withdraw from the project at any time and were informed this would not affect their employment.
Recruitment of Group 2 (people with dementia and their carers)
The clinical nurse consultants (dementia) from Group 1 were asked to identify people with cognitive impairment (± diagnosis of dementia) and their carers, receiving services from Bolton Clarke. Eligibility criteria included: the person with cognitive impairment to have a RUDAS score of ≤22 (Storey et al., 2004) and aged 50 years or more; the carer aged over 18 years, and providing informal care at least 2 days per week; and both having proficiency in written and spoken English. The clinical nurse consultants provided written and verbal information to potential participants and gaining assent to forward their details to the researcher for further explanation. If interested, a home visit was arranged and a PICF sent by mail with sufficient time to read and ask questions. All participants were informed that they were free to withdraw from the project at any time and that this decision would not affect their care provision.
Prototype testing
Individual online testing sessions were arranged with Group 1 participants and face-to-face in-home sessions with Group 2 participants. Group 1 participants had a chance to familiarize themselves with the tool prior to the testing session. During the recorded online session, they were asked to run through the tool as though they were sitting with a person with dementia well-known to them. The researcher asked participants to navigate the tool using pre-determined questions designed to capture the ease of use of the tool, such as their ability to perform a task without error and in a timely manner (e.g., “locate client and start discussion” and “select suitable strategies and make comment”). Group 2 participants worked through the tool with a researcher (CM) and a Dementia Clinical Nurse Consultant (KH), providing feedback at the conclusion of the session as to their satisfaction with the tool. All sessions were audio-recorded, and notes generated.
Feedback was iteratively provided to the Information Management team and the Enabling Choices tool modified in accordance with this feedback.
Phase 4: Deliver—preparation for implementation of the “Enabling Choices” tool
The wider aged care landscape and context was mapped by the research team, specifically to identify organizational and broader system factors that may influence implementation of the tool into practice. In line with the IFAC, an implementation planning checklist was utilized (Meyer et al., 2022) to clarify:
Why we need to change?
What we know?
Who will benefit?
Who will make the change?
What strategies will be used?
In the same testing sessions as outlined above, specific questions were asked of the staff in line with three evaluation constructs of the IFAC—acceptability, appropriateness, and feasibility. Acceptability was defined as the perception of the above participants that the Enabling Choices tool was agreeable and palatable; appropriateness was defined as the perceived fit and relevance of the tool within the context of Bolton Clarke community care provision for people with dementia; and feasibility was defined as the extent to which the Enabling Choices tool can be successfully used within this context (Proctor et al., 2011). Questions included:
What is your overall impression of the tool?
Do you think other staff members will find it useful? In what way?
Which staff will benefit from it the most/use it the most? (e.g., is it more relevant for care managers or case managers, other staff?)
Do you think they will use it? If not, why not?
Can you foresee any issues for other staff?
Can you see any issues that face your clients or carers in using the tool?
Are you likely to recommend this tool?
Do you have any suggestions for engaging other staff in using the tool?
Do you have any suggestions for rolling out this tool?
Do you have any experience with rolling out other programs or products that could help us here?
What support will staff need to take this on?
How will it work best to train them?
Would you be willing to be a “champion” for the tool and be involved in the rollout?
Work on the final question of the IFAC—“what difference are we making”—is currently underway and will be reported separately.
Ethics Approval
This project received full approval from the Bolton Clarke Human Research Ethics Committee (Project No. 197).
Results
An iterative process for all three phases was undertaken, drawing on the expertise of the information management team (n = 5), people with lived experience of dementia (n = 2), subject matter experts (n = 11), researchers (n = 3), and operational management (n = 3) (Figure 3).
Iterative process between Phases 1 and 3.
Phase 1: Discover—gathering insights on conversion to electronic format
Summary of prior work (development of paper-based version)
A full description of the development of the paper-based tool has been published (Goeman et al., 2017). In summary, the user guide for the tool emphasizes:
A review of the person with dementia’s history, as per their intake assessment, prior to commencement
Reason/s for undertaking the tool jointly between the person with dementia and their carer, or separately
Use of the cards, all at once or a little at time. The cards cover several areas (see Table 1)
Acknowledging for whom the area is important and of concern (person with dementia, carer, health professional)
Strategies for each chosen topic of discussion, along with contacts for further information, and setting a priority level of concern
Risk Negotiation Topics.

Subject matter and information services expert input
Regular discussions were held with subject matter and information services experts (as per Figure 3 above) over a 6-month period. Shared insights and goals were collated:
In the first instance, a website was identified as the platform for the electronic version of the tool. This raised concerns of client privacy and confidentiality with the Information Security team, given that the discussion output was to be part of the client’s medical record. A workable solution wasn’t found.
Next, the Information Management team were tasked with developing an internal platform on which the tool could be hosted. An external digital design company was commissioned, and design brief negotiated.
Needs and preferences of the subject matter experts and operational managers were identified around layout, content, and readability of individual pages, along with flow and transition between pages.
Phase 2: Define—synthesis of findings to inform a prototype “Enabling Choices” tool
A prototype “Enabling Choices” tool was developed that incorporated and accounted for:
Using the tool on a laptop computer with no external mouse for navigation.
Viewing all cards on one screen, with a “pop-up” option for cards of interest and need for more detail.
Acknowledging previous discussions held, or actions taken, with client/carer prior to “Enabling Choices” with a free text box for “why are you concerned” and “what are you already doing for [this topic].”
Strategy pages divided consistently into “potential services or health professional referral,” “changes in behavior and/or environment,” and “further resources.” Numerous options were added under each sub-heading to broaden the frontline worker’s repertoire of strategies. The selected strategies needed to be readily visible for the next session.
A mechanism for saving the final document in the client electronic record, with a consistent file naming convention.
Phase 3: Develop—“Enabling Choices” tool refined and ready for testing
Frontline staff who routinely provided care for and with people with dementia participated in testing of the tool. This group included dementia clinical nurse consultants (n = 4), care managers (n = 4), and a registered nurse (n = 1). Each staff member spent a 1:1 session (up to 1 hour) with the lead researcher providing detailed feedback on using the tool with a known client (Box 1—case study). There were a wide variety of cards chosen, providing insights into highly complex situations. The feedback was divided into: (1) ease of navigation/functionality; and (2) content specific (see Supplemental Information for detail of feedback and the team response/changes). Responses were either structural or content changes to the tool by the Information Management team, or noted for training needs during implementation phase.
Case example of “Enabling Choices” in action.

The impact of the COVID-19 pandemic on clients of Bolton Clarke meant that no research activities were possible with people with dementia and their carers. Hence, there is no input from this group at present, but a separate project is underway to address this gap.
Phase 4: Deliver—preparation for implementation of the “Enabling Choices” tool
Acceptability, appropriateness, and feasibility of the tool were explored with Phase 3 participants. There was full support for the tool, with the following points noted:
A holistic learning tool for both staff and people with dementia and their families, promoting dignity and autonomy for the person with dementia.
Allows for a detailed, shared approach to care planning and decision-making, with capacity to monitor change from session to session, as well as options that have been declined.
Great potential for “how” to have conversations with people with dementia, identifying the various perspectives on a given topic.
The lead researcher also worked with operational and frontline staff to identify responses for implementation preparation in line with an implementation checklist (Meyer et al., 2022). Responses can be found in Table 2 for questions of: (1) why we need to change? (2) what do we know? (3) who will benefit? (4) who will make the change? and (5) what strategies will be used?
Implementation Preparation.

Discussion
People with dementia and their informal carers have the fundamental right to live life with dignity and autonomy (WHO, 2017), with this philosophy underpinning the Enabling Choices conversation tool. Determining level of risk for people with dementia is not a new concept (Manthorpe & Moriaty, 2010), but is challenging in the face of ever-changing perspectives of level of risk (Stevenson et al., 2017). The Enabling Choices tool allows for a structured approach in discussing activities of daily living that vary in risk perception, depending on the evolving dementia journey, external circumstances, and the multitude of health professionals potentially involved in the care of the person with dementia. It addresses the needs, preferences, and concerns of providing care for and with people with dementia at the macro, meso, and micro level.
Globally, there is recognition that our society and our care institutions should be equitable and inclusive (WHO, 2017), moving toward dementia friendly, dementia capable, and dementia positive approaches, where resources are integrated and attitudes, beliefs and behaviors of healthcare workers support a person’s strengths (Lin & Lewis, 2015). The Enabling Choices tool facilitates home care staff’s ability to provide care in line with the Australian Quality Standards, including consumer dignity and choice (Aged Care Quality and Safety Commission, 2018). Simultaneously, the provision of options within the tool comprehensively collates resources, so that healthcare professionals can work to a person’s strengths.
Health professionals often struggle to balance the narrative of vulnerability and protection of people with dementia (Bailey et al., 2013), with person-centered care principles designed to promote shared power and responsibility (Australian Commission on Safety and Quality in Healthcare, 2011). The Enabling Choices tool provides an opportunity for risk to be communicated (i.e., the potential benefits and harms of a situation or care option) between health professionals, people with dementia and their carers. A review by Stevenson et al. (2018) highlighted that risk is often conceptualized differently (e.g., wandering as a behavior of concern, or beneficial to health and wellbeing), can be constructed socially (including a stereotypical gendered construction of how people with dementia should behave) and can lack congruence between perception of risk and reality. Shared discussions are instrumental in facilitating a common understanding of risk for a particular activity, while simultaneously challenging potential bias and assumptions in the person with dementia’s abilities.
At a micro level, supported decision-making, as opposed to the legal entity of substitute decision-making, has evolved to strengthen self-determination of people with disabilities (Browning et al., 2014), including the cognitive disability of dementia. Sinclair et al. (2019) propose a spectrum model, with the level of support changing in response to a person’s situation and the nature and extent of cognitive impairment. This fits well with the Enabling Choices tool having several “cards” for discussion, dependent upon the pressing need or preference at the time. Concerns around safety are the prime driver for formal and informal carers struggling to promote independence and autonomy, with the constant need to negotiate and re-negotiate risky activities (Soilemezi et al., 2019). A spectrum model of supported decision-making through Enabling Choices could potentially ease such conflict.
This study has several limitations. The impact of the COVID-19 pandemic on Bolton Clarke’s service provision meant that meaningful involvement of people with dementia and carers was not possible. This is being rectified in a subsequent evaluation. Further, the study was conducted with staff in Melbourne and Southeast Queensland, but to enhance generalisability, the next phase will involve staff from other States as well as from regional areas.
The Enabling Choices tool was found to be acceptable and feasible in practice, with a strength of this study being the preparation for widescale implementation into practice using a fit-for-purpose implementation framework (Meyer et al., 2022). Non-adoption of technological innovations is common, most likely due to the complexity of the dynamic interactions between individual factors (Greenhalgh et al., 2017), with a need to consider the relationships between individuals and the organizational and system context in which they operate (Greenhalgh et al., 2016). These factors have been elucidated as part of the implementation planning process, critical to ensuring the “ducks are lined up” prior to the launch of the tool. Important next steps for research will be the evaluation of the implementation of the tool in practice. This will involve its effectiveness from the perspective of people with dementia and their carers (currently underway through a separate project), as well as implementation outcomes of reach and adoption, fidelity and sustainability. A further area for exploration will be the acceptability and feasibility of the tool with groups that are seldom heard, including culturally and linguistically diverse groups.
Conclusion
The “Enabling Choices” tool has been deemed acceptable, feasible, and appropriate through a co-design process with frontline workers, dementia specialists, people with dementia and their informal carers. It promotes dignity and choice for older people with dementia, allowing them to engage in a shared decision-making process around activities that are becoming risky. Implementing a tool into practice can be fraught with challenges but utilizing the IFAC ensured preparation and planning for its complexity.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214221149772 – Supplemental material for Risk Negotiation With People With Dementia: From Co-designed Paper Version to Implementation Preparation of an Electronic Conversation Tool
Supplemental material, sj-docx-1-ggm-10.1177_23337214221149772 for Risk Negotiation With People With Dementia: From Co-designed Paper Version to Implementation Preparation of an Electronic Conversation Tool by Claudia Meyer, PhD, Marissa Dickins, PhD, Fleur O’Keefe, MNurs, Kylie Hall, GDipGerontics and Judy Lowthian, PhD in Gerontology and Geriatric Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: State Trustees Australia Foundation.
Institutional Review Board
Bolton Clarke Human Research Ethics Committee (EC 00349), project approval no. 170015.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.