
Abstract
Compensation (e.g., alarm setting) has the potential to improve or maintain everyday functioning and delay conversion to dementia. Various psychological characteristics may impact compensation and therefore could inform intervention development and response to intervention. This study aimed to evaluate whether personality and affective characteristics are associated with compensation after accounting for cognition in older adults without dementia. Measures of compensation (both self-report and informant-report), cognition, personality (neuroticism, openness, extraversion, conscientiousness and agreeableness), grit, self-efficacy, positive affect, and two types of negative affect (sadness, anger) were administered to a sample of 126 older adults (mean age = 76.6; mean education = 15.5 years; 61% female; 45% non-White). In analyses using the entire sample, higher ratings of anger were associated with self-reported compensation. In follow-up analyses stratified by ethnoracial group, neuroticism was a predictor of self-reported compensation in non-Hispanic White participants and openness was a predictor of informant-reported compensation in non-White participants. Our findings suggest that anger may facilitate activation to compensate for real or perceived cognitive change. Additionally, personality characteristics associated with compensation may vary across diverse ethnoracial groups and reporting source.
Introduction
Roughly one in nine adults in the United States over age 65 suffer from Alzheimer’s disease and related dementias (ADRD), and that number is expected to increase as the population becomes older (Alzheimer’s Association, 2024). ADRD is characterized by cognitive impairment leading to a reduced ability to perform instrumental activities of daily living (IADLs; e.g., managing finances, cooking), increased care burden, and poor health outcomes (Alzheimer’s Association, 2024). ADRD has no known cure, so targeted interventions that help individuals maintain functional independence and delay further decline are especially important.
Older adults who use compensatory strategies (e.g., note-taking, alarm setting) perform better on everyday tasks (A. Weakley et al., 2019), have higher levels of independence, and a slower rate of functional decline independent of cognitive impairment (Tomaszewski Farias et al., 2018). Compensation refers to alternative strategies and methods individuals use to augment or replace impaired aspects of their cognition, such as memory (A. T. Weakley & Farias, 2023). Importantly, individuals with early-stage cognitive impairment can learn to use compensatory strategies with positive outcomes on everyday functioning and caregiving stress/strain (Kinsella et al., 2009). Further, compensation training is a practice standard in cognitive rehabilitation for traumatic brain injury (Cicerone et al., 2011) and should occur early in the course of cognitive decline to maximize benefit (A. T. Weakley & Farias, 2023).
To evaluate baseline compensatory strategy use and response to intervention, compensation can be evaluated by either observing if/how a person uses compensation on a given task (e.g., A. Weakley et al., 2019; Woods et al., 2020) or through questionnaires (e.g., de Frias & Dixon, 2005; Tomaszewski Farias et al., 2018). There are pros and cons to each assessment method. For example, while observation-based methods provide an objective estimate of compensation, they are time intensive, difficult to standardize, and may rely on performing tasks in an artificial environment limiting verisimilitude. Questionnaire-based assessment of compensation may either be completed by the older adult themselves (self-report) or a family/friend (informant-report). Benefits to self-report include time and effort efficiency and awareness of how they routinely use compensation in their daily lives (A. Weakley et al., 2019). However, as cognition declines, self-report may become less reliable and, in these cases, informant-report provides a more objective picture of compensation use patterns (Tomaszewski Farias et al., 2018).
Previous work suggests a variety of factors influence compensation including education level, health comorbidities (de Frias et al., 2003) and cognitive impairment (Hutchens et al., 2012; Tomaszewski Farias et al., 2018). Personality has also emerged as a potential predictor of compensation (Beech et al., 2021; de Frias et al., 2003; Dixon et al., 2001; Tomaszewski Farias et al., 2018), though the evidence is limited. Personality refers to characteristics individuals display in their habits, behaviors and attitudes. A set of personality traits with substantial empirical support (collectively referred to as “The Big Five”) include neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness (P. Costa & McCrae, 1999). High levels of agreeableness, neuroticism, and conscientiousness have been found to be strong positive correlates of self-reported compensation in community-dwelling older adults, whereas openness and extraversion were weak correlates (de Frias et al., 2003). Beech et al. (2021) also showed a relationship between neuroticism and self-reported compensation. Specifically, self-reported compensatory strategies used to assist with appointments, shopping, and cooking were predicted by neuroticism, whereas appointment related compensation was predicted by openness.
In addition to personality factors, affect has also emerged a possible contributor to compensation use. Specifically, negative affect and life stress have been found to be associated with compensation (de Frias et al., 2003; Garrett, et al., 2010).
Successful compensation training needs to be highly personalized based on the unique needs of the individual, the environment and other intrapersonal factors, including psychological factors, that influence engagement, and uptake (A. T. Weakley & Farias, 2023). As such, the present study’s purpose was to examine the impact of personality and affect on compensation use in an older adult sample. Based on previous, albeit limited, literature, we predict openness, agreeableness, neuroticism and conscientiousness are positively associated with compensation. Aspects of negative affect are also hypothesized to be contributors to compensation. A novel aspect of this study is also examining a wider range of intrapersonal factors including self-efficacy and grit. Since there are pros and cons of looking at self- and informant-reported compensation in isolation, we included both reporting sources for a comprehensive view of compensation behavior. From a clinical perspective, insights gained from this research may lead to development of new interventions and assist clinicians with predicting response to interventions.
Methods
Participants
All participants provided written informed consent, and all human participant involvement was approved by institutional review boards at University of California at Davis, the Department of Veterans Affairs Northern California Health Care System, and San Joaquin General Hospital in Stockton, California (approval: 215830) on 2/5/2011, renewed on 12/7/2024). through two routes: 1. memory clinic referrals (12%) and 2. community outreach (88%) using protocols designed to enhance both the racial and ethnic diversity of the sample. A community education specialist oversaw recruitment of the sample with the help of the UCD ADRC Outreach, Recruitment, and Education Core. Inclusion criteria for enrollment into the longitudinal cohort included age 60 or older at the baseline examination and an ability to speak English or Spanish. Exclusion criteria included unstable major medical illness or serious psychiatric disorder. All enrolled participants signed informed consent, and all human subject involvement was overseen by institutional review boards at UCD, the Veterans Administration Northern California Health Care System, and San Joaquin General Hospital in Stockton, California. Participants received clinical evaluations through the UCD ADRC on a roughly annual basis that followed the same protocol and included a detailed medical history, a physical, and a neurological and neuropsychological exam. They then received a consensus diagnosis, based on standard diagnostic criteria, of healthy older adult (HOA) versus mild cognitive impairment (MCI) versus dementia as well as etiologic diagnosis.
Measures
Participants completed the Revised NEO Personality Inventory (NEO-PI-R; P. T. Costa, 1992) to assess agreeableness, neuroticism, openness to new experience, conscientiousness, and extraversion. They also completed measures from National Institutes of Health (NIH) Toolbox (Salsman et al., 2013) on self-efficacy, positive affect and two types of negative affect (anger, sadness). A Computer Adaptive Test format was utilized which allowed for shorter and more targeted administration. The surveys were scored using IRT methods and converted to an uncorrected standard score (T-score).
Grit, defined as perseverance and passion for long-term goals at the trait level, was measured with the short (8 item) form of the Duckworth scale (Duckworth & Quinn, 2009). An average Grit score was used in analyses. Finally, self- and informant-report Everyday Compensation (Ecomp; Tomaszewski Farias et al., 2020) questionnaires were completed to assess compensation use across different activities (e.g., medication management, driving). An average compensation score was used in analyses.
Participants were allowed to complete the questionnaires and test battery in English or Spanish. They completed measures on a tablet independently without a researcher or psychometrist in the room. Participants also identified an informant who was provided with a paper copy of the EComp to complete. The informant or participant mailed the questionnaire back to the center in a prepaid envelope.
Cognition was measured using the Spanish and English Neuropsychological Assessment Scales (SENAS; Mungas et al., 2004) which includes measures of semantic language (object naming and picture association), episodic memory (word-list learning), executive function (category fluency, phonemic fluency, digit span backward, visual span backward and list sorting) and visual-spatial abilities (spatial configuration learning, pattern recognition and spatial localization). A SENAS composite score was calculated by averaging each the standardized score of each individual measure. The composite score is used as the measure of cognition.
Analyzes
All variables met normality standards except two values in anger and openness which were replaced with three deviations above the mean to normalize data. Analyses included Pearson correlations to examine the relationship between all variables. The significance level for correlations was set to p ≤ .01 to account for the number of correlations. Next, multiple linear regressions were performed to determine the relationship of personality and affect on compensation. If a predictor was significant, a hierarchical regression was performed with cognition in the first block (to control for cognitive abilities) and the personality/affect predictor in the second block. This was done on both self-reported and informant-reported scores to get a more comprehensive picture of compensation. Analyses were performed using R v4.3.2 stats package and a p ≤ .05 was considered significant.
Results
The sample comprised of 126 participants. One hundred participants met criteria for HOA (age M = 76.0; SD = 6.7) and 26 for MCI (age M = 79.4; SD = 6.4). Sixty-one percent were female; 55% were White; 20% were African American; 17% were Hispanic; 7% were Asian; and 1% were American Indian/Alaska Native. Please see Table 1 for additional demographic information as well as personality and affect measurement means, standard deviations, and ranges.
Participant Demographic, Health, and Neuropsychological Data.

Note. Compensation is the mean Everyday Compensation (EComp) score; Grit, Extraversion, Agreeableness, Conscientiousness, Neuroticism, and Openness are means; Anger, Positive Affect, Sadness, and Self Efficacy are standardized averages; Cognition is calculated from averaging standardized measures of semantic language, episodic memory, executive function and spatial memory from SENAS.
Pearson correlations were performed on all study variables as seen in Table 2. Age and education were not significantly related to self-reported compensation (r < −.01, p > .05 and r = −.20, p > .05, respectively) or informant-reported compensation (r = −.03, p > .05 and r = −.01 and p > .05, respectively) and thus were not controlled for in subsequent analyses to prevent reduction in power. Of note, apart from significant correlations among self- and informant-rated compensation, there were no significant correlations among the other study variables with compensation.
Table of Correlations for Main Variables.

Note. CS = compensation.
p < .01, **p < .001, two-tailed.
Regression analyses revealed that anger was a significant positive predictor of self-reported compensation over and above cognition with adjusted R2 = 0.04, p = .03; ΔR2 = 0.03; anger β = .18, p = .01 (see Table 3). While openness was a significant positive predictor of informant-reported compensatory strategy use with adjusted R2 = 0.03, p = .03; openness β = .20, p = .03, the model was no longer significant after including cognition R2 = 0.03, p = .10. No other personality/affect variables were significant predictors of self- or informant-reported compensation (adjusted R2s = −0.01–.02, ps ≥ .05).
Hierarchical Model of Personality Variables on Compensation.
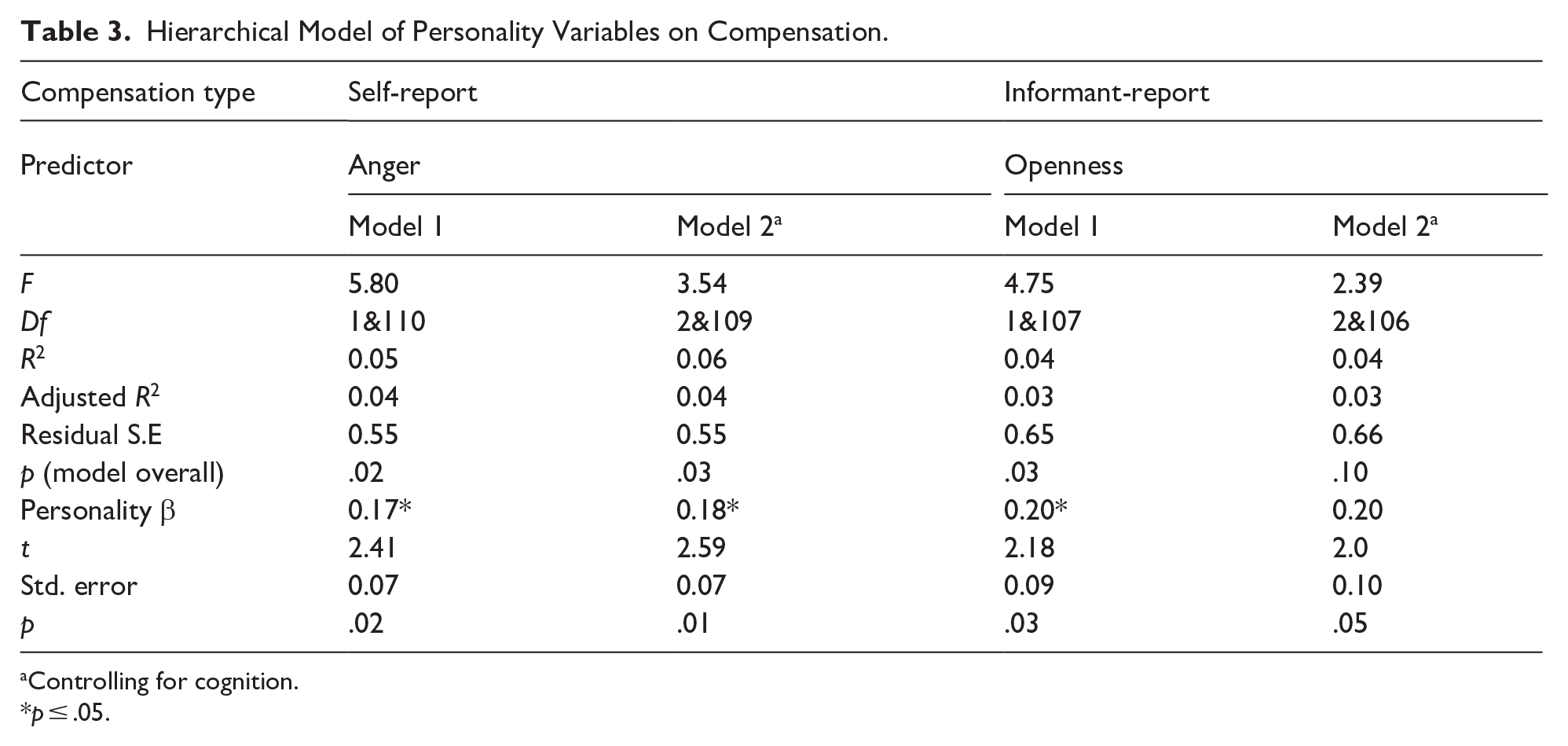
Controlling for cognition.
p ≤ .05.
Because our findings were only partially consistent with our hypotheses, we conducted secondary (follow-up) analyses to better understand our findings. Given the homogeneity of populations evaluated in prior related studies, we hypothesized that differences seen in our results may be due to the broader diversity in our sample. To test this secondary hypothesis, we divided our sample into non-Hispanic White (N = 69; referred to as White for simplicity) and Hispanic White/non-White (N = 57; referred to as non-White for simplicity).
First, we examined whether there were significant differences between the White (mean age = 76.8, SD = 6.6, mean education = 16.7, SD = 2.4, 54% female) and non-White (mean age = 76.5, SD = 7.1, mean education = 14.8, SD = 3.5, 70% female) groups on variables presented in Table 1. T-test comparisons performed on all variables revealed that education was significantly different between the two populations (t = −2.45, p = .02) and was thus controlled for in the following analyses.
When limiting analyses to White participants only neuroticism was a positive predictor of self-reported compensation over and above cognition with adjusted R2 = 0.12, p = .02; β = .17, p = .03 (see Table 4). This finding was not replicated in non-White participants. For informant-reported compensation, when limiting analysis to non-Whites, openness to experience was a positive predictor over and above cognition with adjusted R2 = 0.19, p < .01; β = .62, p < .001. This finding was not seen in the White group. Because we included education as a covariate in these secondary analyses, we repeated the full sample analyses while controlling for education and there were no changes in results.
Predictors of Self and Informant Reported Compensation by Group a .

Controlling for cognition and education.
p ≤ .05, **p ≤ .01.
To confirm our findings were not due to differences in predictor variables between groups (White, non-White), ANOVAs were performed on anger, neuroticism, openness, informant-compensation, and self-compensation. No differences were found (Fs 0.16–0.67; ps ≥ .05; see Table 5). An examination of outliers was also performed which was unrevealing.
ANOVA of Studied Variables by Group.
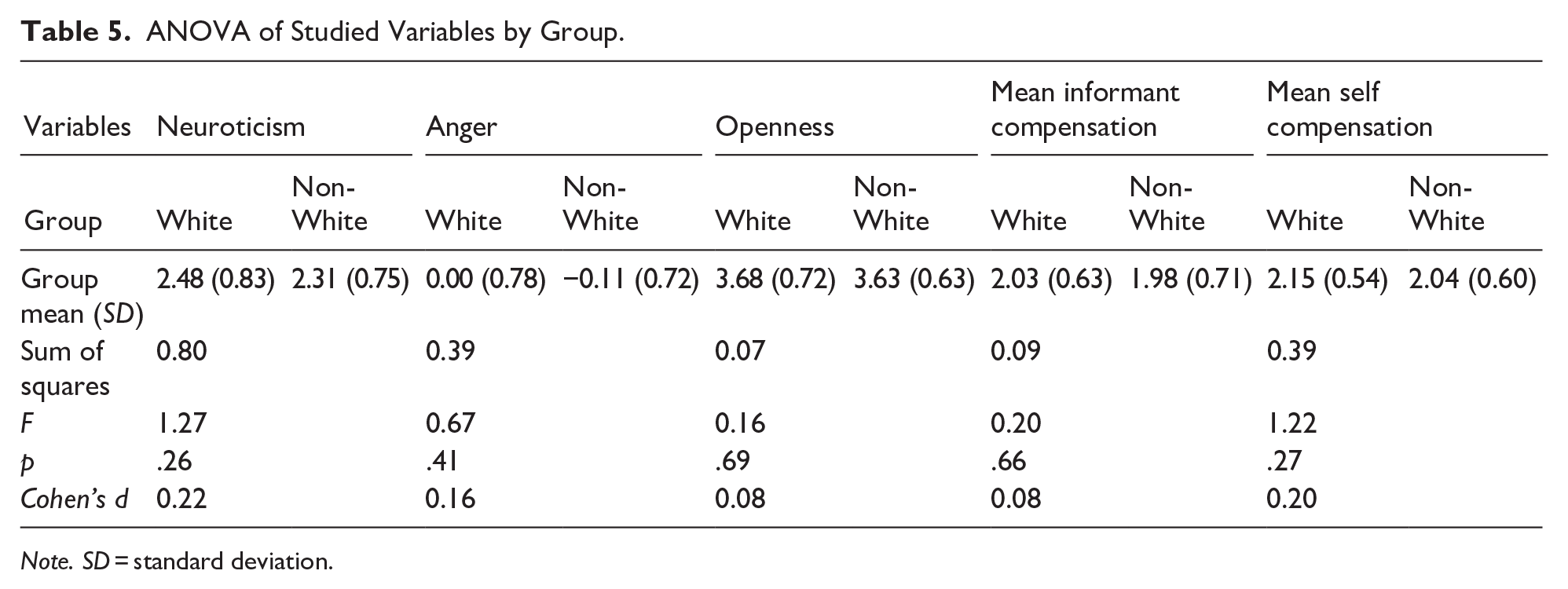
Note. SD = standard deviation.
Discussion
The goal of this study was to examine intrapersonal predictors of compensation, including personality and affect, in older adults. Based on prior literature, we hypothesized that personality traits such as openness, neuroticism, agreeableness and conscientiousness would positively predict compensation. We were, however, unable to support these findings in our full sample after controlling for cognition. Interestingly, we did find that anger was a positive predictor of self-reported compensation, even after accounting for cognition. While de Frias et al. (2003) found that negative affect was related to increased compensation, the measure they used (Affect Balance Scale; Bradburn, 1969) included items most consistent with items on our study’s sadness scale and was thus not replicated in the current study. There were no significant personality or affect predictors of informant-reported compensation after controlling for cognition.
While our finding that anger increases compensation was initially surprising, after a review of the literature, we speculate that anger could motivate individuals to engage in more compensation. Studies have shown anger as a driving force that spurs action and results in increased creative engagement (da Costa et al., 2020; Stanley et al., 2021). This fits with the cognitive neoassociation model of anger that highlights anger as an activating emotion that can prompt individuals to take strategies to eliminate the source of anger (Berkowitz, 2012). Using this perspective, individuals exhibiting higher anger could be more driven to take steps to reduce their memory complaints through compensation. This could also explain why individuals experiencing higher life stress had higher compensation scores as seen in previous literature (Garrett et al., 2010). Of note, we did not seem the same relationship with informant-report suggesting that anger increases compensation that is not noticed/observable by others.
Because our findings were not entirely consistent with prior results, we performed follow-up analyses to better understand our findings. We hypothesized that differences seen in our results may be due to the racial/ethnic diversity in our sample (45% non-White). While prior results did not provide racial/ethnic breakdown of their samples, they were completed in areas such as Alberta/British Columbia (de Frias et al., 2003) and Eastern Washington/Northern Idaho (Beech et al., 2021), which are more ethnically homogenous and primarily Caucasian. To explore potential differences, we re-ran the analyses in White and non-White subgroups. When we did this, we found that neuroticism predicted self-reported compensation in the White group, which is consistent with prior findings and our original hypothesis. Our findings suggest that the neuroticism fuels compensation in non-Hispanic Whites but not in other ethnic/racial groups.
Differences in cognitive aging perception may help explain our neuroticism finding. Specifically, non-western cultures often view cognitive decline as a normal and inevitable part of aging, instead of as an illness that can be prevented or reduced (Cox, 2007). Further, white participants often emphasize maintaining independence as a critical issue of their aging experience more than African American or Latino older adults (Roberts et al., 2015), which could explain why neuroticism only predicts compensation in White populations.
We also found that openness was a significant positive predictor of informant-reported compensation in the non-White participant group only. Research in diverse samples show that openness is associated with better cognitive outcomes (Tomaszewski Farias et al., 2024) and reduced memory errors (Sutin et al., 2024), which could explain its positive effect on compensation. It is unclear why openness-related compensation was not seen in White populations or with self-reported compensation. It is also possible that personality traits may not be accurately reflected in our sample of non-White individuals. Although the Big 5 personality traits are known to be robust and replicated across cultures (Carciofo et al., 2016; Courtois et al., 2018; McCrae & Allik, 2002; Schmitt et al., 2007), studies have shown that it does not capture all aspects of personality (Feher & Vernon, 2021) and constructs may not be equivalent in diverse groups; for example, individuals from collectivist cultures appear to use the Big 5 personality traits to a lesser degree to describe themselves and their behavior (Heine & Buchtel, 2009).
Limitations
Some limitations of our research include the relatively small sample size, limiting our ability to examine differences between cognitively normal individuals and those with mild cognitive impairment. Similarly, our sample size limited us from being able to do further sub-group analyses by race and ethnicity.
Conclusions
Our study explored the impact of personality traits and affect on compensation after controlling for cognition in an older adult sample. We contribute three novel findings. First, we found that anger played a role in predicting compensation. Clearly, it would not be a wise clinical approach to breed anger in individuals with the goal of increasing anger. Rather, future research may focus on growing activating emotions that promote compensation but do not trigger other negative emotions. Positive activating emotions such as enjoyment of learning, hope, and pride have been known to improve learning and performance and may be a good place to start (Pekrun, 2012). Motivational interviewing may be another method to activate self-directed use of compensation that can be explored.
Second, we found that differences in personality predictors of compensation between White and non-White participant groups. Thus, future studies should consider personality factors by race/ethnicity when examining compensation and developing interventions as different approaches may need to be taken to improve compensation in different ethnoracial groups. Finally, we also discovered differences between reporting source (i.e., self vs. informant) in different ethnoracial groups. Thus, care must be taken when selecting and evaluating questionnaire results in future research.
Footnotes
Acknowledgements
We would like to thank the research support staff at the UC Davis Alzheimer’s Disease Center for collecting this data and the participants for agreeing to be involved in this study.
Ethical Considerations
All participants provided written informed consent, and all human participant involvement was approved by institutional review boards at University of California at Davis, the Department of Veterans Affairs Northern California Health Care System, and San Joaquin General Hospital in Stockton, California (approval: 215830) on 2/5/2011, renewed on 12/7/2024.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Health/National Institute of Aging (NIH/NIA P30AG010129-24S1, NIH/NIA K23AG080152).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All datasets can be made available upon request.