AC1-AC26, RF1-RF19 and i1-i11 are
oral presentations
Presentation Number: AC1
Publishing Title: Comparison Of Long-term Outcomes Of The Ross Procedure Versus Aortic Valve Replacement With Mechanical Or Bioprosthetic Valves
Author Block: Marie-Ange Fleury, Sébastien Hecht, Nancy Côté, Vincent Chauvette, Mohamed Marzouk, Marie-Annick Clavel, Siamak Mohammadi, Philippe Pibarot, Jean Perron.
Institut universitaire de cardiologie et de pneumologie de Québec - Laval, Québec, QC, Canada.
Abstract Body:
BACKGROUND: The Ross procedure is an attractive therapeutic option for treating aortic valve disease, especially in younger patients. However, it remains a more complex operation than a standard aortic valve replacement (AVR) and thus, the ideal valve substitute in young adults remains a matter of debate.
METHODS: This is a retrospective analysis of prospectively collected data. A total of 1780 patients who underwent isolated AVR at the Institut universitaire de cardiologie et de pneumologie de Québec - ULaval from 1990 to 2023 were included (675 [38%] mechanical AVR, 711 [40%] biological AVR and 394 [22%] Ross procedure). Two separate propensity score matchings (PSM) were used to compare the Ross procedure with both mechanical and biological AVR. The primary study endpoint was all-cause mortality, and the key secondary endpoints were valve reintervention (on the aortic or pulmonary valve position) and the composite endpoint of mortality and valve reintervention.
RESULTS: At 30 years, there were no statistical differences regarding mortality, valve reintervention and the composite of valve reintervention and mortality between mechanical AVR and Ross procedure (log-rank p=0.84, log-rank p=0.72 and log-rank p=0.97, respectively). In contrast, biological AVR was associated with a significantly higher risk of valve reintervention and of the composite endpoint when compared to Ross (HR [95%CI]: 6.54 [3.57-11.99], p<0.001 and HR [95%CI]: 3.44 [2.44-4.87], p<0.001, respectively), but showed no difference regarding mortality (log-rank p=0.26). There were no significant differences between groups for post-operative complications including stroke and bleeding (all p>0.57).
CONCLUSION: At 30 years, the Ross procedure shows similar clinical outcomes to mechanical AVR in terms of mortality and reintervention but is superior to biological AVR with regards to valve reintervention.
Presentation Number: AC2Publishing Title: Sex Differences In Aortic Valve Inflammation And Remodeling In Chronic Severe Aortic Regurgitation
Author Block: Mattie Garaikoetxea, Carolina Tiraplegui, Alba Sadaba, Paula Castillo, Ernesto Martin-Nuñez, Miriam Goñi-Oloriz, Susana San Ildefonso, Eva Jover, Adela Navarro, Natalia Lopez-Andres.
Navarrabiomed, Pamplona, Spain.
Abstract Body:
OBJECTIVE: Aortic regurgitation (AR) is more prevalent in men, although cellular and molecular mechanisms underlying the sex differences in prevalence and pathophysiology are unknown. This study evaluates the impact of sex on the aortic valve (AV) inflammation and remodeling as well as the cellular differences in valvular interstitial cells (VICs) and valvular endothelial cells (VECs) in patients with AR.
METHODS: A total of 144 patients (27.5% women) with severe chronic AR were included. AVs were analyzed by imaging, histological and molecular biology techniques (ELISA, RT-PCR). VICs and VECs isolated from patients with AR were characterized and further treated with transforming growth factor (TGF)-β.
RESULTS: Clinically, men had smaller index aortic dimensions and greater AV thickness. Proteome profiler analyzes in AVs (n=40/sex) evidenced higher expression of inflammatory markers in men and that was further validated (interleukins, chemokines). Histological composition showed higher expression of inflammatory mediators and collagen thick fibers in AVs from men. Male VICs and VECs secreted higher levels of inflammatory markers than female cells. Interestingly, male VICs produced higher amounts of collagen type I and lower fibronectin and aggrecan, whereas male VECs secreted lower decorin. TGF-β exclusively enhanced inflammation in male VICs, and decorin and aggrecan in female VICs.
CONCLUSIONS: Compared to men, AVs from women were thinner, less inflamed and fibrotic. VIC seem to be the key cell type responsible for the sex-differences. Valvular inflammation associated with an active remodeling process could be a key pathophysiological process involved in AR.
Presentation Number: AC3Publishing Title: North American Trends In Utilization And Outcomes Of The Ross Procedure: A Word Of Caution
Author Block: Amine Mazine1, Steve Fan1, Joanna Chikwe2, Nimesh Desai3, Jennifer Chung1, Jad Malas2, Qiudong Chen2, Angel Chen1, Kyle Runeckles1, Michael Bowdish2, Joseph Bavaria4, Maral Ouzounian1.
1University of Toronto, Toronto, ON, Canada, 2Cedars-Sinai Medical Center, Los Angeles, CA, USA, 3Hospital of the University of Pennsylvania, Philadelphia, PA, USA, 4University of Pennsylvania, Philadelphia, PA, USA.
Abstract Body:
OBJECTIVE: There has been a renewed interest in the Ross procedure as an alternative to conventional aortic valve replacement (AVR) in young adults. This study aimed to assess contemporary trends in Ross procedure utilization in adults and examine the relationship between surgical volumes and in-hospital mortality.
METHODS: The Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Database was queried for patients who underwent the Ross procedure between 2008 and 2023. We used mixed-effects logistic regression, incorporating center- or surgeon-specific random intercepts, to investigate the relationship between Ross volumes and in-hospital mortality. Statistical significance was evaluated using likelihood ratio tests.
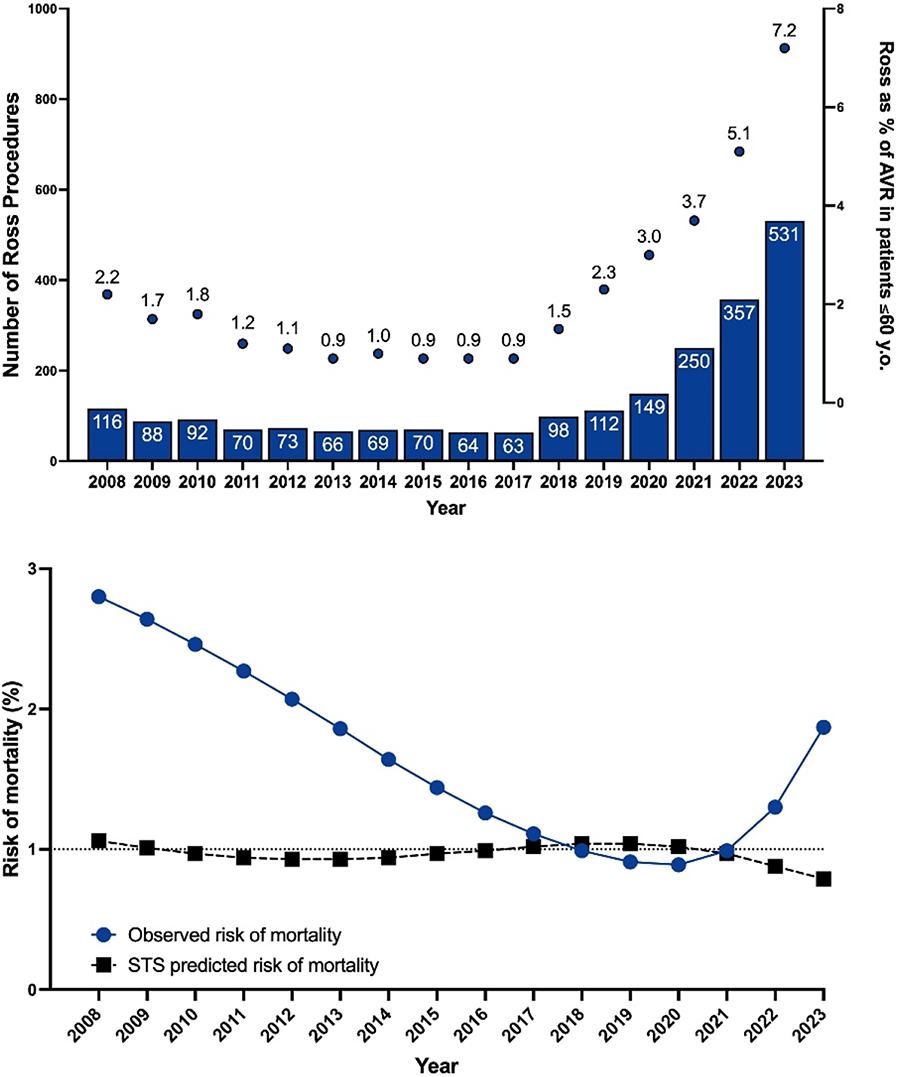
RESULTS: A total of 2,268 Ross procedures were reported across 217 centers from 2008 to 2023. Median age was 43 years (IQR: 32-52). Only 22 centers performed more than 15 Ross procedures during the study period. Ross procedure utilization reached a nadir in 2017 (n=63) before increasing annually, reaching 531 cases in 2023 (Figure 1). Ross procedures represented 0.9% of all AVRs in adults aged ≤60 years in 2017, increasing to 7.2% by 2023 (Figure 1). The risk of in-hospital mortality declined from 2.8% in 2008 to 0.9% in 2020 but rose to 1.9% in 2023 (Figure 1). In-hospital mortality was significantly higher at centers performing 1 or 2 Ross procedures annually compared to those performing more than 10 (OR 4.5 [95% CI: 1.5-13.2], p=0.006), and for surgeons performing 1 or 2 Ross procedures per year compared to more than 10 (OR 3.8 [1.2-12.2], p=0.007).
CONCLUSIONS: The Ross procedure is increasingly utilized in North America. Low-volume centers and surgeons are associated with higher mortality. The Ross procedure should only be performed in high-volume comprehensive valve centers of excellence.
Presentation Number: AC4Publishing Title: Life Time Management Of Aortic Insufficiency Starts With Aortic Valve Repair : Multicentric Comparative Outcomes Of Repair Versus Biological Replacement From The Heart Valve Society Aortic Valve Database
Author Block: Pichoy Danial, Emmanuel Lansac.
Pitié-Salpêtrière hospital, Paris, France.
Abstract Body:
BACKGROUND: Althought most patients suffering from aortic regurgitation (AR) and/or ascending aortic dilatation have reparable valve most of them are being replaced. The goal of this study was to compare long-term outcomes after aortic valve repair (AVr) versus biological AVR (bAVR).
METHODS: The Heart Valve Society Aortic Valve database which is a longitudinal observational study enrolling patients from 78 centers was used to identify adult patients suffering from AR and/or ascending aortic dilatation who had undergone AVr or bAVR. Propensity score framework analyzes were used to compare outcomes while controlling for confounders.
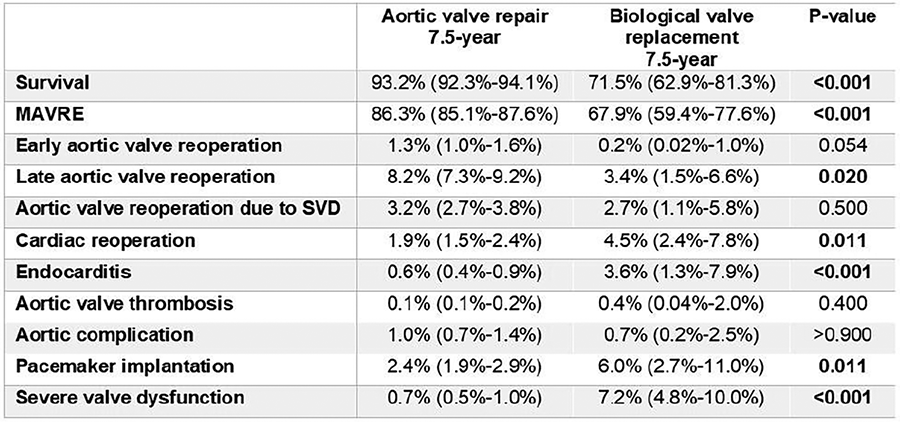
RESULTS: In total, 7,543 patients operated between 1985 and 2024 were included (AVr n=6,773, bAVR n=545). Propensity score matching yielded 1,006 patients who underwent AVr matched to 530 patients who underwent bAVR. Early mortality was comparable between the AVr-group (1.2%) and the bAVR-group (2.1%) (P=0.070). The overall post-operative survival in the bAVR-group was lower compared to the AVr-group (71.5% versus 93.2% pooled P<0.001). Patients in the bAVR group had higher occurrence of MAVRE (33.1% versus 13.7%, P=0.001), infective endocarditis (3.6% versus 0.6%, P=0.006) and severe structural valve deterioration (7.2% versus 0.7%, P<0.001) compared to patients in the AVr group (P=0.001, P=0.006, P<0.001 respectively). The cumulative incidences of late aortic valve reintervention (P=0.368), thrombo-embolism (P=0.858), bleeding (P=0.530), pacemaker implantation (P=0.671) were comparable.
CONCLUSION: Compared to bAVR, AVr improved patients outcomes with significantly better survival and fewer incidence of MAVRE, infective endocarditis or structural valve deterioration. This data reinforces medical evidence guideline should recommend aortic valve repair as the primary indication for aortic regurgitation.
Presentation Number: AC5Publishing Title: Outcomes Of Isolated Aortic Valve Repair Versus Valve-sparing Root Replacement In Patients With Primary Aortic Regurgitation
Author Block: Francesco Zito1, Kevin M. Veen1, Johanna J. M. Takkenberg1, Giovanni Melina2, Emmanuel Lansac3, Laurent de Kerchove4, Jan Vojáček5, Igor Rudez6, Peter Verbrugghe7, Vincent Chauvette8, Claudia Romagnoni9, Marek Jasinski10, Adrián Kolesár11, Ruggero de Paulis12, Jolanda Kluin1, Bardia Arabkhani1.
1Erasmus University Medical Center, Rotterdam, Netherlands, 2Sant'Andrea Hospital, Sapienza University of Rome, Rome, Italy, 3Pitié-Salpêtrière Hospital, Sorbonne University, Paris, France, 4Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Brussels, Belgium, 5Charles University Hospital, Hradec Králové, Czech Republic, 6University Hospital Dubrava, Zagreb, Croatia, 7University Hospitals Leuven, KU Leuven, Leuven, Belgium, 8Montreal Heart Institue, Montreal, QC, Canada, 9Fatebenefratelli Sacco Hospital, University of Milan, Milan, Italy, 10Central University Hospital Wroclaw, Wroclaw, Poland, 11East Slovakian Institute for Cardiac and Vascular Diseases, Košice, Slovakia, 12European Hospital Rome, Rome, Italy.
Abstract Body:
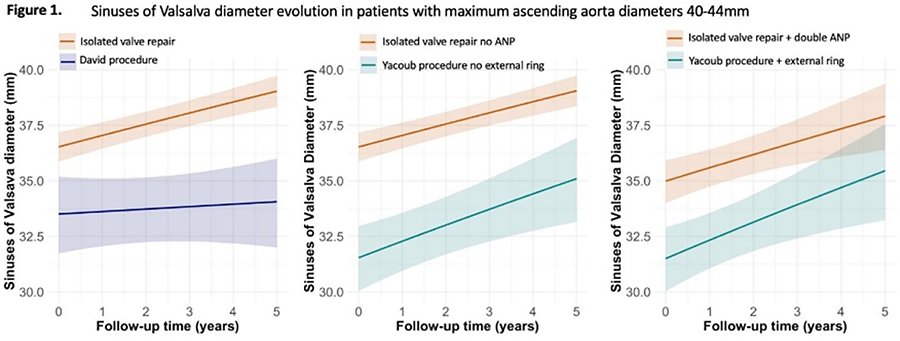
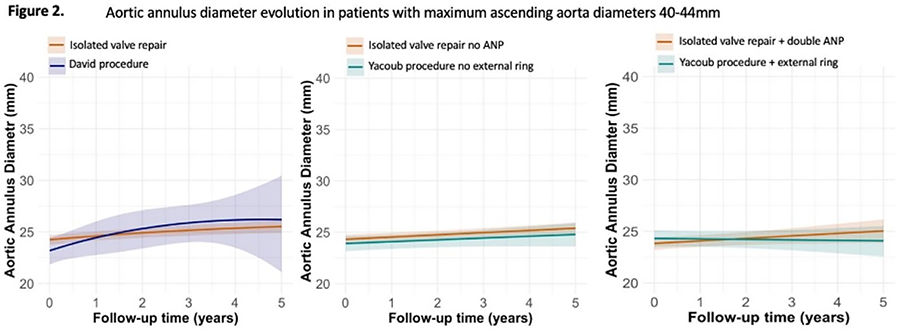
OBJECTIVE: Isolated aortic valve repair (IAVr) and valve sparing root replacement (VSRR) are surgical options for patients with severe isolated aortic regurgitation (AR) [ascending aortic diameters (AscAD)<40mm]. When the AscAD [sinus of Valsalva (SoV), sinotubular junction, tubular aorta] exceeds ≥45mm, replacement of the SoV/tubular ascending aorta should be considered. However, no guideline recommendations exist for patients with intermediate AscAD (40-44mm). Therefore, the study aimed to investigate post-operative outcomes and aortic valve dysfunction after IAVr or VSRR in patients with primary surgical-indication AR.
METHODS: Adult patients in the Heart-Valve-Society Aortic-Valve Database with moderate-severe/severe AR and maximum-AscAD<50mm were included. Endocarditis and aortic dissections were excluded. Patients were divided into groups based on maximum AscAD: GROUP-1:<40mm, GROUP-2:40-44mm, GROUP-3:45-49mm. In each group the patients were stratified for IAVr/VSRR. Time-to-event analysis were used to investigate clinical outcomes. AR and AscAD evolution were analyzed using repeated-measurement analyses.
RESULTS: In total, 535 patients were included (9.2%female, median age 45 years, IQR:35-57), with 70% having a bicuspid aortic valve. Total follow-up completeness for survival was 58%, with 84% completeness at one-year postoperatively. At 8-years, survival estimates were 92.6%(95%CI:86.75-98.90) for GROUP-1, 97.9%(95%CI:94.9-100) for GROUP-2, and 94.5%(95%CI:89.7-99.6) for GROUP-3 (p=0.08). The cumulative incidence of reintervention at 10-years was 20.2%(95%CI:4.3-44.3) for IAVr and 2.2%(95%CI:0.4-7.1) for VSRR in the 45-49mm group (p=0.009); no significant differences were observed in other groups. In the 40-44mm group, IAVr showed progressive root dilatation (p=0.08) and increased AR grade compared to the David-technique, while no significant difference in annular enlargement was observed among all techniques.
CONCLUSIONS: Primary AR with AscAD of less than 40mm may benefit from both IAVr and VSRR. Concerns may arise in patients with intermediate diameters (40-44mm) undergoing IAVr due to potential root enlargement; however, long-term follow-up is needed for a clearer understanding. VSRR should be preferred over isolated AVr when diameters exceed 45mm.
Presentation Number: AC6Publishing Title: Biomechanical Modeling Of Ascending Thoracic Aortic Aneurysms: Investigating The Relationship Between Aortic Regurgitation And Wall Stress
Author Block: Naomi Lynn Haddock, Siavash Zamirpour, Axel Casarez-Gomez, Liang Ge, Elaine E. Tseng.
University of California San Francisco, San Francisco, CA, USA.
Abstract Body:
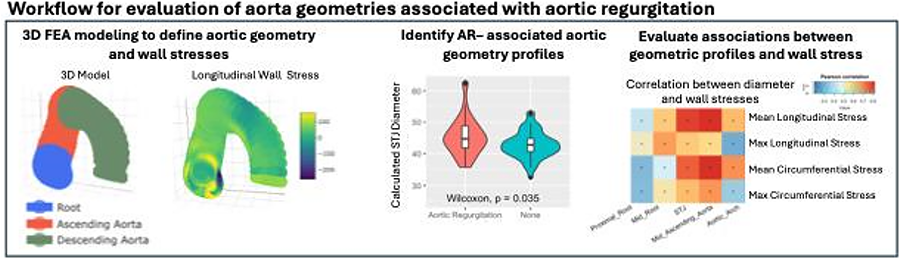
OBJECTIVE: Ascending thoracic aortic aneurysms (aTAAs) are localized dilations of the aorta that increase wall stress, potentially leading to rupture or dissection. Aortic regurgitation (AR) frequently coexists with aTAA, but the relationship between AR, differing aortic geometry, and resulting biomechanical stress patterns in aTAAs is not well understood. Fluid structure interaction (FSI) is often used to study AR but fails to capture geometry and wall stresses important in aTAA, while 3D finite element analysis (FEA) offers a promising alternative. Our objective is to develop a workflow leveraging FEA to explore the geography of aortic high stress patterns across the cardiac cycle and to use this approach to explore the impact of AR in aTAA.
METHODS: CT scans from 82 aTAA patients (38 with AR) were used to generate patient-specific FEA models at physiological pressures (120/80 mmHg). Spatial relationships of modeled aortic elements allow us to “unroll” the aorta while preserving dimensional variation for spatial analysis. Wall stress patterns were evaluated, identifying high-stress areas and comparing stress differences at different pressures.
RESULTS: Patients with AR had significantly higher calculated diameters at the proximal root and STJ. These patients had higher maximum longitudinal stress at both end-diastole (ED) and end-systole (ES) with larger area exceeding 100 kPa. Patients with AR experienced greater increases in longitudinal and circumferential stress from ED to ES as well as greater dimensional changes, compared to those without AR. (Figure: Workflow includes 3D FEA modeling of geometry and wall stress, identification of AR-associated geometries, and pearson correlation of geometric features with wall stresses.)
CONCLUSIONS: We have developed a workflow allowing spatial analysis of aortic wall stresses, found that AR is associated with distinct aorta geometry, and evaluated relationship between those geometric profiles and wall stress.
Presentation Number: AC7Publishing Title: Prosthesis-patient Mismatch Following Transcatheter Aortic Valve Replacement Is Not Associated With Adverse Three Year Outcomes
Author Block: Mohiuddin Cheema, Robert Hagberg, Sabet Hashim, Raymond Mckay, Khagendra Dahal.
Hartford Hospital, Hartford, CT, USA.
Abstract Body:
OBJECTIVE: The impact of prosthesis-patient mismatch (PPM) on adverse outcomes following TAVR remains controversial.
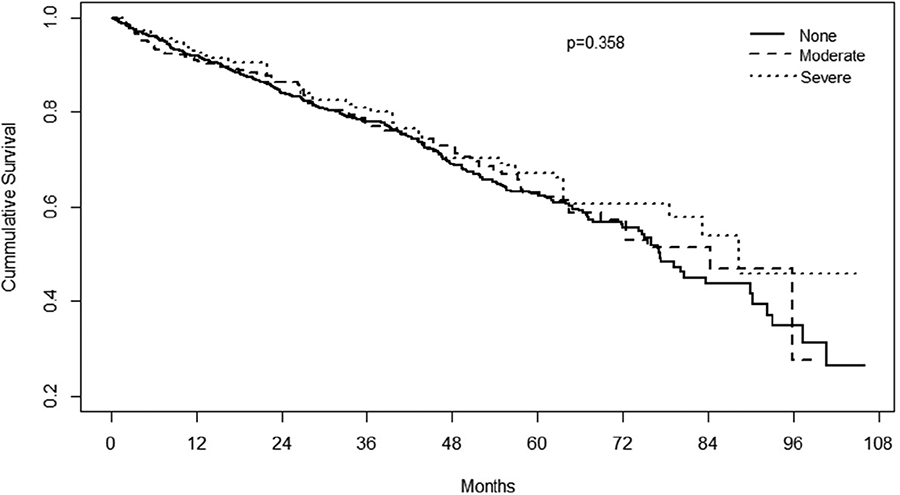
METHODS: We assessed in-hospital and late outcomes in 2,291 TAVR patients successfully treated from a transfemoral approach with current generation TAVR valves. Patients were classified as having No, Moderate and Severe PPM according to standard definitions adjusted for body mass index. Valve-in-valve cases were excluded.
RESULTS: Propensity matched patients included 72.7%, 20.3%, and 6.9% with No, Moderate and Severe PPM, respectfully. The 3 cohorts did not differ with respect to age, sex, race, comorbidities or STS Risk score. Balloon-expandable valves were more commonly used in Moderate and Severe PPM groups. Severe PPM patients had more strokes, annulus rupture, and atrial fibrillation, with a longer length of stay. No, Moderate and Severe PPM cohorts had similar 1-year mortality (8.2 vs 8.4 vs 8.8%, p=0.937) and hospital readmission (21.6 vs 22.6 vs 19.9%, p=0.136). At 32.5±23.8 month follow-up, the 3 groups had similar AV re-intervention (0.7 vs 0.6 vs 1.1%, p=0.164), AV endocarditis (0.0 vs 0.0 vs 0.0%, p=1.0), and total repeat hospitalization (28.9 vs 31.1 vs 29.7%, p=0.293). Kaplan-Meier survival analysis is depicted below.
CONCLUSIONS: Despite increased in-hospital complications in Severe PPM patients, there was no increase in all-cause mortality, AV re-intervention, AV endocarditis or hospital readmission in Moderate and Severe PPM cohorts at 32.5 months mean follow-up.
Presentation Number: AC8Publishing Title: Dysregulated Expression Of Toll-like Receptors In Valves From Rheumatic Heart Disease Patients
Author Block: Najma Latif1, Padmini Sarathchandra2, Ann McCormack3, Magdi H. Yacoub1.
1Imperial College, Magdi Yacoub Institute, Heart Science Centre, Harefield Hospital, United Kingdom, 2Magdi Yacoub Institute, Heart Science Centre, Harefield Hospital, United Kingdom, 3Magdi Yacoub institute, Heart Science Centre, Harefield Hospital, United Kingdom.
Abstract Body:
OBJECTIVE: Toll-Like Receptors (TLRs) critically link innate immunity with adaptive immunity. Cell surface TLRs mainly recognise membrane components of microorganisms to induce an inflammatory response. TLRs have been shown to be upregulated in calcified human leaflets and we sought to analyse their expression in aortic leaflets from patients with rheumatic heart disease (RHD) and compare this to calcified aortic leaflets. We also analysed normal and RHD mitral leaflets.
METHODS: 6 normal aortic leaflets, 6 aortic leaflets from RHD and 5 calcified human aortic leaflets were analysed by immunohistochemistry for the expression of TLR2 and TLR4. 6 normal mitral leaflets and 6 mitral RHD leaflets were also analysed.
RESULTS: We observed that not all VICs and VECs express TLR2 and TLR4. In normal aortic leaflets, TLR4 is expressed in a greater number of VICs (approx. 40%) than TLR2 (approx. 10%). RHD aortic leaflets showed a significantly reduced expression of TLR4 (p=0.0007) compared to normal, with some RHD aortic leaflets showing no expression. Calcified aortic leaflets showed a significantly higher expression of TLR4 compared to normals (p=0.004) and to aortic RHD (p=0.0095). RHD aortic leaflets showed a significantly reduced expression of TLR2 (p=0.0087) compared to normal, with some RHD aortic leaflets showing no expression. Calcified aortic leaflets showed a significantly higher expression of TLR2 compared to normals (p=0.004) and to aortic RHD (p=0.0043). Mitral RHD leaflets showed a similar pattern to aortic RHD leaflets in that they showed significantly reduced level of expression of TLR4 (p=0.029) and TLR2 (p=0.0087) compared to normals.
CONCLUSIONS: We have shown significantly reduced expression of TLR2 and TLR4 in aortic and mitral leaflets from RHD patients. This may be a compensatory mechanism in RHD patients to limit inflammation. Factors that reduce the expression of TLR2 and TLR4 in RHD are being investigated.
Presentation Number: AC9Publishing Title: High-intensity Statins Are Associated With Increased Aortic Valve Calcification In Patients With Severe Stenosis
Author Block: Veronika A. Myasoedova, Matteo Franchi, Donato De Giorgi, Valentina Rusconi, Alice Bonomi, Francesca Bertolini, Ilaria Massaiu, Vincenza Valerio, Paolo Poggio.
Cento Cardiologico Monzino, IRCCS, Milan, Italy.
Abstract Body:
OBJECTIVE: Aortic valve stenosis (AS) is the most common valvular disease, characterized by progressive fibro-calcific remodelling of the aortic valve leaflets, leading to increased mortality risk. Statins may influence the pathogenesis of AS by modulating the production of proprotein convertase subtilisin/kexin type 9 (PCSK9). While high concentration of PCSK9 leads to increase calcification. This study investigates the interaction between statins, PCSK9, and aortic valve calcification.
METHODS: In vitro, we evaluated valvular interstitial cell (VIC) calcification by a colorimetric assay and PCSK9 secretion by ELISA under atorvastatin (0.1-1µM) or pravastatin (0.1-100µM) treatments. We assessed indexed aortic valve calcification (AVC) volume and progression using computed tomography (CT) in 295 AS patients. We performed an epidemiological study to evaluate the 10-year incidence of non-rheumatic aortic valve replacement (AVR) in over 36,000 new users (matched for multiple confounding factors) of different intensity statin therapies.
RESULTS: In vitro, statins significantly increased, in a dose dependent manner, both VIC calcification (p-for-trend<0.001) and PCSK9 secretion (p-for-trend<0.01). Effects blunted by PCSK9 knock-down and neutralized by an anti-PCSK9 antibody. CT quantifications showed higher AVC content in patients on high-intensity statins compared to low-intensity ones (903.8±601 vs. 526.8±403mm³/cm²; p<0.0001), with no significant difference between low-intensity statin and non-users (p=0.226). At follow-up, high-intensity statin users exhibited a double annual calcium accumulation compared to low-intensity statins or non-users. Epidemiologically, high-intensity statin therapy was associated with a 30% increased incidence of AVR (follow-up 5 years; HR 1.30, 95% CI: 1.07-1.57) compared to low-intensity statin users.
CONCLUSIONS: Our in vitro model confirms increased VIC calcification and PCSK9 secretion upon treatment with high-dose statins only. Clinically, severe AS patients on high-intensity statins have higher AVC load and accumulation, with new high-intensity users showing increased AVR incidence. These findings underscore the necessity for further research to identify the optimal lipid-lowering strategy in AS patient management.
Presentation Number: AC10Publishing Title: Twenty-Year Outcomes Following Porcine Versus Bovine Pericardial Aortic Valve Replacement
Author Block: Amine Mazine1, Anna Chu2, Rodolfo Rocha1, Douglas S. Lee2, Vivek Rao1, Terrence M. Yau1, Tirone E. David1, Maral Ouzounian1.
1University of Toronto, Toronto, ON, Canada, 2Cardiovascular Program, ICES, Toronto, ON, Canada.
Abstract Body:
OBJECTIVE: Bioprosthetic valves are widely used for surgical aortic valve replacement (AVR), with porcine and bovine pericardial types being the most common. However, data comparing their long-term outcomes are limited. This study evaluates the twenty-year outcomes of patients who underwent isolated AVR with either porcine or bovine pericardial bioprostheses.
METHODS: We included patients who received first-time isolated AVR using a stented porcine (Hancock II) or bovine pericardial (Perimount/Magna-Ease) bioprosthesis from 1990-2014 in this single-center, observational study. Patient data were prospectively collected and linked to provincial administrative databases. The primary outcome was all-cause mortality, and the secondary outcome was aortic valve reintervention (surgical or transcatheter). Propensity score-based inverse probability treatment weighting was used to balance baseline characteristics.
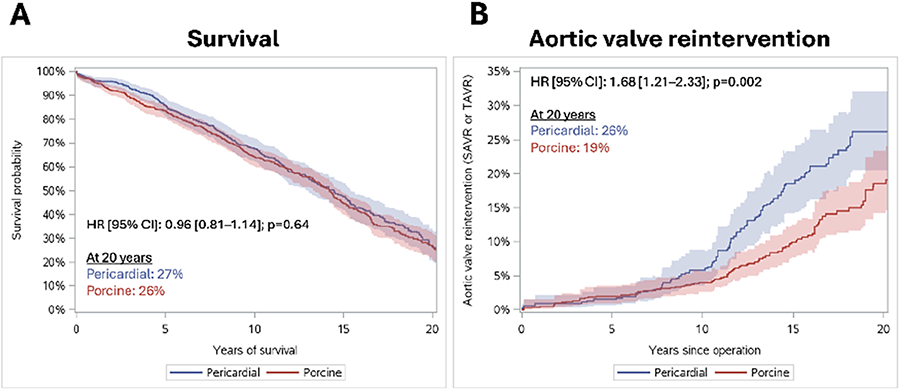
RESULTS: Among 1,306 patients (porcine: 751 [58%]; pericardial: 555 [42%]; mean age 68±12 years, 44% female), propensity score weighting resulted in comparable groups. At 20 years, survival was 26% in the porcine group versus 27% in the pericardial group (HR [95% CI]: 0.96 [0.81-1.14]; p=0.64) (Figure 1A). At 20 years, aortic valve reintervention occurred in 19% of the porcine group versus 26% of the pericardial group (HR [95% CI]: 1.68 [1.21-2.33]; p=0.002) (Figure 1B). Subgroup analyses showed higher reintervention rates in the pericardial group for both patients ≤65 years (HR: 1.66 [1.15-2.41]; p=0.007) and >65 years (HR: 2.21 [1.12-4.37]; p=0.022). Higher reintervention rates were also observed in the pericardial group when the implanted prosthesis' labelled size was ≥25 (HR: 2.44 [1.58-3.76]; p<0.0001) but not when the implanted prosthesis size was <25 (HR: 1.28 [0.69-2.36]; p=0.44).
CONCLUSIONS: Stented porcine and bovine pericardial bioprostheses show comparable long-term survival following AVR, though porcine valves have lower reintervention rates, particularly in larger sizes, suggesting a preference for porcine valves in cases where larger prostheses can be implanted.
Presentation Number: AC11Publishing Title: Iris Valve: A Novel Growth Accommodating TPVR System For Very Young Children
Author Block: Nnaoma Agwu1, Tanya Burney1, Ekaterina Perminov1, Christopher Alcantara2, Robert Edwards1, Michael Recto3, Arash Kheradvar1.
1University of California, Irvine, Irvine, CA, USA, 2Children's Hospital of Orange County, Orange, CA, USA, 3Children's Hospital of Orange COunty, Orange, CA, USA.
Abstract Body:
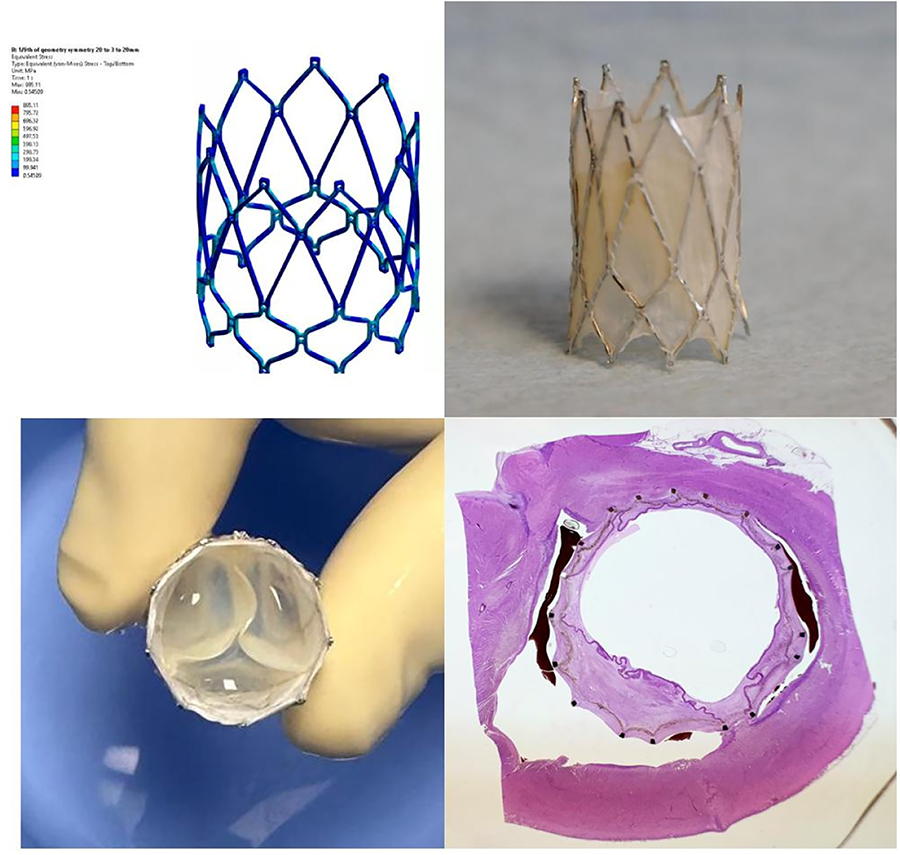
OBJECTIVE: Each year, ∼1.35 million infants are born with congenital heart defects. Most of those show some degree of right ventricular outflow tract (RVOT) abnormalities, which often necessitate pulmonary valve replacement to alleviate the harmful effects of pulmonary valve regurgitation on the right ventricle (RV). Current solutions, e.g., the Melody™ Valve by Medtronic, are not suitable for children smaller than 20 kg. Delaying replacement until a child reaches this weight increases the risk of RV dilation. To address this challenge, we have developed the IRIS transcatheter pulmonary heart valve, designed to accommodate growth in children as small as 8 kg.
METHODS: Maintaining leaflet coaptation throughout the valve's size range was achieved by implementing novel origami concepts. The unique stent design was validated through finite element analysis to ensure that cracking and fracture did not occur. Seven Yucatan mini-pigs, weighing between 9 and 17 kg, received the IRIS Valve via 12-Fr and 14-Fr delivery catheters. After a minimum of six weeks, the valve was balloon-expanded to accommodate growth, expanding to a size of up to 20 mm. Six months post-implantation, the pig’s heart was excised for histopathological analysis. The RVOT and pulmonary annulus containing the valve were embedded and stained for further examination.
RESULTS: Fluoroscopic and echocardiographic studies confirmed proper valve placement in the pulmonary annulus with no signs of regurgitation. Visual inspection during autopsy revealed clean, intact, and unobstructed leaflets, with the stent well-integrated into the pulmonary annulus. The H&E staining showed typical chronic inflammation characterized by lymphocytes, macrophages, and multinucleated giant cells reacting to the ePTFE skirt and suture material. Notably, neutrophils were absent, indicating no signs of infection.
CONCLUSIONS: These findings suggest that the IRIS Valve performs exceptionally well and remains intact throughout the six-month studies in swine models.
Presentation Number: AC12Publishing Title: Finite Element Analysis For Biomechanical Assessment Of Patient-specific Transcatheter Aortic Valve Implantation (tavi) Reveals Post-tavi Complications Correlates With Aortic Wall Stresses
Author Block: Huseyin C. Yalcin1, Abdulrahman Alnabti2, Onur Mutlu1, Noaman Mazhar1, Abdel Naser Ghareeb2.
1Qatar University, Doha, Qatar, 2Hamad Medical Center - Heart Hospital, Doha, Qatar.
Abstract Body:
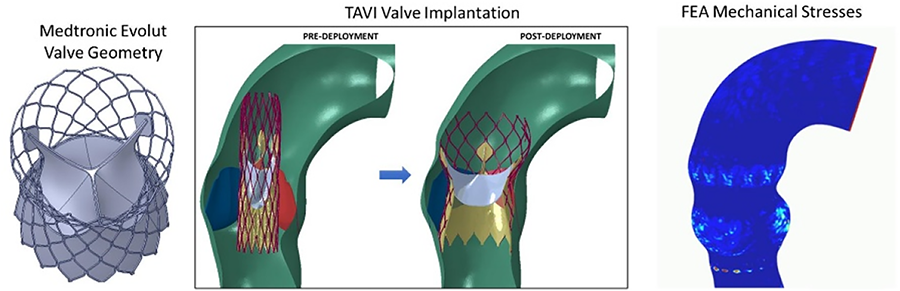
OBJECTIVE: For transcatheter aortic valve implantation (TAVI), valve size and implantation depth within the aortic root is crucial for preventing complications, such as conduction problems and paravalvular leak. Computational modeling offers comprehensive assessment of patient-specific TAVI scenarios at pre-operative stage enabling calculation of aortic wall mechanical stresses and deformations from the implanted valve. Our objective is to develop patient-specific finite element computational modeling approaches for comprehensive biomechanical assessment of TAVI to investigate correlations between post-TAVI aortic wall mechanics and post-TAVI complications.
METHODS: This investigation is in collaboration with Hamad Heart Hospital TAVI program in Qatar where Medtronic Core Valve is the most commonly used valve, hence we focused on this valve. A total of 54 retrospective cases were analyzed. Among the study cohort, 24 patients received 26mm valve, 23 patients received 29mm valve, and 7 patients received 34mm valve. ABAQUS finite element analysis (FEA) software was used for complete TAVI simulation operation, with valve crimping, valve insertion and valve deployment to calculate mechanical stresses and deformations on aortic root. For each TAVI case, FEA revealed biomechanical stress and deformation patterns on aortic root via calculation of stent contact area on aortic wall; average and maximum contact pressure; average and maximum von mises stresses; average and maximum radial displacements. Studied cases were grouped into cases that experienced complications post-TAVI and cases that did not experience complications post-TAVI.
RESULTS: Using ABAQUS, we successfully simulated complete TAVI implantation and carried out FEA for aortic root stress and deformation patterns for studied cases. Statistical analysis revealed, TAVI contact pressure was higher for cases suffering from conduction abnormalities, suggesting stent pressure is an important factor influencing conduction abnormalities experienced post-TAVI.
CONCLUSIONS: We have developed an FEA approach simulating TAVI implants for prediction of possible TAVI complications.
Presentation Number: AC13Publishing Title: Incidence, Progression And Predictors Of Mitral Valve Regurgitation In Patients Diagnosed With Ascending Aortic Dilatation
Author Block: Adine R. de Keijzer1, Maximiliaan L. Notenboom1, Guillaume S.C. Geuzebroek2, Robin H. Heijmen2, Roland R.J. van Kimmenade2, Jos A. Bekkers1, Johanna J.M. Takkenberg1, Jolien W. Roos-Hesselink1, Kevin M. Veen1, Annemien E. van den Bosch1, Jolanda Kluin1.
1Erasmus University Medical Center, Rotterdam, Netherlands, 2Radboud University Medical Center, Nijmegen, Netherlands.
Abstract Body:
OBJECTIVE: Mitral valve regurgitation (MR) can coexist in patients with ascending aortic aneurysms (AscAAs), especially in AscAAs with hereditary etiology. This retrospective study examines the prevalence, etiology, and progression of MR concomitant to AscAAs.
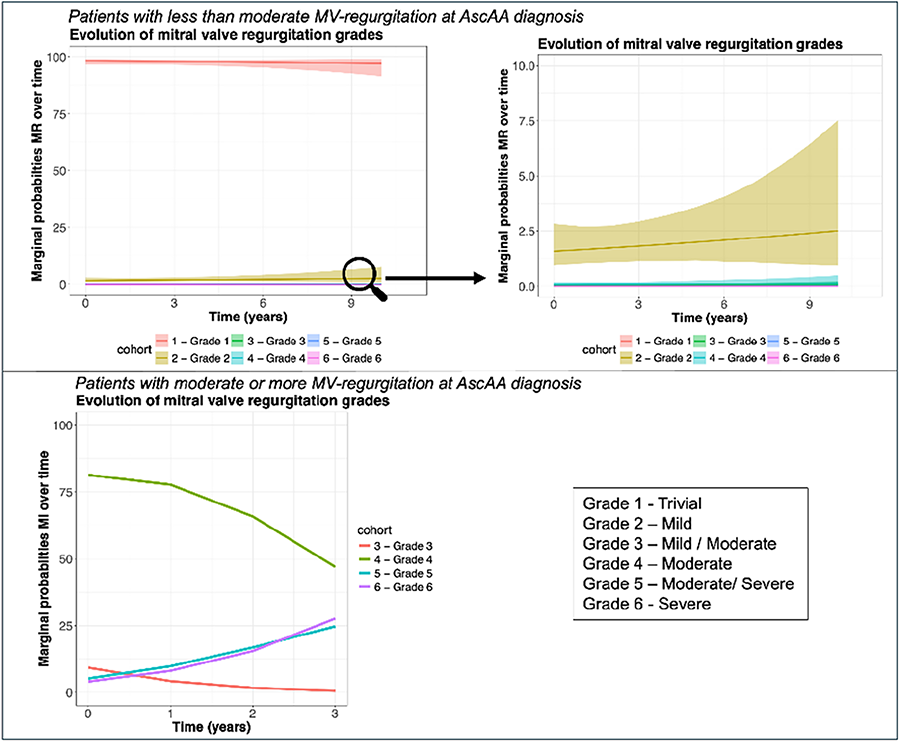
METHODS: Adult patients with AscAA (aortic root and/or ascending aorta ≥40mm) and mitral valve imaging between 2007-2022 at two academic centers were included, excluding prior mitral valve surgery. Follow-up ranged from AscAA-diagnosis until surgery for AscAA/death. Progression of MR was analyzed using continuation-ratio-mixed-effects-models. MR was graded 1-6 (Figure1). Baseline characteristics, treatment-strategies and survival were compared between patients with no/mild-MR and moderate/severe-MR at AscAA diagnosis. Primary (lesions of the apparatus) vs. secondary (geometry of the left ventricle/left atrium) MR-causes and MR outcomes after aneurysm repair in patients with moderate/severe-MR without concurrent mitral valve-surgery were explored.
RESULTS: Of 1,443 patients (30.5% female, 7.4% genetic diagnosis), 3.8% had moderate/severe-MR (35% primary, 66% secondary). Median follow-up was 6.6 years. 1.2%(N=16) had severe-MR at AscAA diagnosis. Patients with moderate/severe-MR were older (69.0vs.59.7 years, p<0.001) and had larger aortic diameters (51.0vs.46.0mm, p=0.007) than the no/mild-MR-group. Unadjusted survival at 10-years was lower in the moderate/severe-MR-group (54.6%(95%CI:38.1%-78.4%)) compared to no/mild-MR-group (81.0%(95%CI:78.4%-83.7%), p<0.001), but not after adjusting for covariates (p=0.877). The median time from AscAA diagnosis to aortic surgery was shorter for the moderate/severe-MR-group compared to no/mild-MR-group (1.1vs2.5-years, p<0.001). Twenty two percent of the moderate/severe-MR-group underwent concomitant mitral valve-surgery during aortic surgery. MR-grades worsened already in the first three years after AscAA diagnosis in moderate/severe-MR-group (Figure1). However, in most patients with secondary-MR, MR-grades improved after aortic surgery without concomitant mitral valve-surgery.
CONCLUSIONS: At AscAA diagnosis patients with moderate/severe-MR present in a more advanced disease stage in terms of aortic size, translating to earlier surgery and experience worsening MR over time. MR in AscAA-management should be considered, but for carefully selected patients with secondary-MR needing aortic surgery, a watchful-waiting-strategy regarding the mitral valve could be considered.
Presentation Number: AC14Publishing Title: Advanced Calcified Lesion Progression Engages Metabolic Shifts In Pentose Phosphate Pathway (ppp) And Lipid-mineral Complexes
Author Block: Alex Cruz1, Tania Sanchez-Bayuela2, Adithya Prabakaran1, Stephan Sutter1, Lara Estroff1, Carmen Garcia-Rodriguez2, Jonathan Butcher1, J. Alberto San Roman3, Olimpio Montero4, Mirian Peral-Rodrigo5, Mariano Sanchez Crespo4, Javier Lopez3.
1Cornell University, Ithaca, NY, USA, 2Universidad de Valladolid, Valladolid, Spain, 3Hospital Clínico Universitario de Valladolid, Valladolid, Spain, 4IBGM-CSIC, Valladolid, Spain, 5IBGM-Universidad de Valladolid, Valladolid, Spain.
Abstract Body:
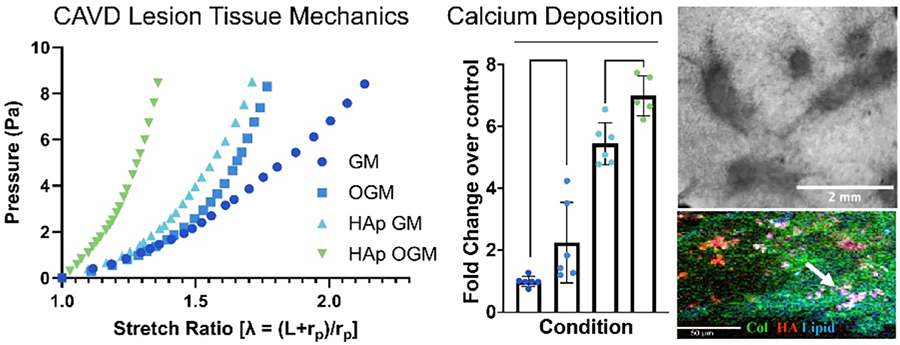
OBJECTIVE: Advanced Calcific Aortic Valve Disease (CAVD) is an understudied context critical for therapeutic intervention. CAVD engages both endothelial (VEC) and interstitial cells (VIC) within a mechanically regulated 3D matrix. We hypothesize that advanced CAVD exhibits distinct metabolic and cellular characteristics.
METHODS: Mineral, matrix, and lipid composition of Human CAVD tissues were characterized using RAMAN microscopy. Human and porcine VEC and VIC were cultured in 3D mechanically anchored collagen hydrogels and CAVD induced by osteogenic media (OGM) or inflammatory cytokines (INFy, LPS) for up to 10 days. Hydroxyapatite nanoparticles (HAnp) with CAVD-like crystallinity were synthesized and added to the 3D matrix as late stage. Matrix compaction, lesion mechanical properties, calcified lesion morphology, calcium deposition, cell differentiation, and metabolic programming were assessed.
RESULTS: Human CAVD exhibited unique signatures of mineral, collagen, and lipids, supporting metabolic shifts during lesion progression. Both OGM and inflammatory stimulation induced matrix compaction and calcium deposition, but only with VEC co-culture were 3D raised lesions formed. HAnp supplementation reduced matrix compaction but dramatically increased calcium deposition. VEC progressively aggregated to the surfaces of lesions, while VIC aggregated beneath them with prominent myofibroblastic differentiation. HAnp supplementation augmented myofibroblastic activation throughout the tissue. OGM and HAnp increased lesion stiffness synergistically. RAMAN spectroscopy of 3D co-cultures identified diffuse intracellular lipid formation within VICs under OGM, but much larger discrete extracellular lipid deposits associated with mineral when further stimulated by HAnp. Inflammatory stimulation increased 13C6-Glucose metabolite flux into Acetyl-COA, a prominent lipid substrate. Furthermore, increased glycolysis was associated with a novel reduction of oxidative pentose-phosphate pathway (oxPPP).
CONCLUSIONS: These findings demonstrate novel metabolic shifts in calcified lesions via lipid deposition, mineral complexing, glycolysis with reduction of oxPPP. Clinically relevant biological treatments may need to focus on unique advanced CAVD lesion programs.
Presentation Number: AC15Publishing Title: Technique Of Leaflets Thinning And Ship Technique In Aggressive Rheumatic Mitral Valve Disease.
Author Block: Shipra Shrivastava1, Sandeep Shrivastava1, Shitij Shrivastava2, Shashwat Shrivastava3.
1Medanta Superspeciality Hospital, Indore, MP, India, Indore, India, 2BronxCare Health System, New York, NY, USA, 3Montefiore Medical Center, New York, NY, USA.
Abstract Body:
OBJECTIVE: The objective of our Leaflets Peeling Technique is to improve the functionality of mitral leaflets affected by advanced rheumatic disease. Releasing of the anterior and posterior mitral leaflets from their dense fibrotic coverings effectively makes them thin and supple. The Ship Technique for commissural reconstruction further enhances the overall efficiency of the valve by optimizing the support mechanism.
METHODS: From January 2021 to September 2024, we performed 125 mitral valve repairs. Among these, 66.4% were rheumatic, contrasting with the west, where degenerative cases predominate. Aggressive rheumatic disease in our population leads to thickened and fibrotic leaflets, fused commissures and severe subvalvular pathology. In such cases, maintaining leaflet mobility and regaining commissural flexibility is essential for achieving durable repairs. We devised leaflet peeling techniques and commissural reconstruction, thus transforming the valve into a more functional, native-like structure. Notably, of the rheumatic repairs, 71% were females, and 96.4% of patients were under 60 years. The majority of patients presented with mitral stenosis (67.5%), a finding that is relatively rare elsewhere. More than half of our patients underwent commissural reconstruction using the Ship Technique, and Leaflets Thinning was performed in all our rheumatic patients, resulting in excellent postoperative outcomes. Additionally, we closed the left atrial appendage in all cases, irrespective of rhythm or left atrial size.
RESULTS: Our techniques yielded excellent results, with post-repair valves resembling normal native valves and functioning efficiently during both systole and diastole. Importantly, none of the patients have required repeat interventions, indicating the long-term success of our approach.
CONCLUSIONS: In cases of aggressive rheumatic mitral disease, our techniques of leaflet thinning and commissural reconstruction effectively restore leaflet movability and commissural flexibility. These interventions lead to improved hemodynamics and overall cardiac function, ultimately enhancing patient outcomes and quality of life.
Presentation Number: AC16Publishing Title: Multidimensional Proteomic Assessment Of Bioprosthetic Structural Valve Degeneration And Native Calcific Aortic Valve Disease
Author Block: Rachel Cahalane1, Cassandra Clift2, Mandy Turner2, Mark Blaser2, Taku Kasai2, Alesandra Campedelli2, Marie Billaud2, Jochen Muehlschlegel3, Amber Hendrickx4, Marie Van den Bosch4, Filip Rega4, Masanori Aikawa2, Laoise McNamara1, Bart Meuris4, Sasha Singh2, Elena Aikawa2.
1University of Galway, Galway, Ireland, 2Brigham and Women's Hospital, Boston, MA, USA, 3John Hopkins University School of Medicine, Baltimore, MD, USA, 4KU Leuven, Leuven, Belgium.
Abstract Body:
OBJECTIVE: Bioprosthetic (BP) valve degeneration and native calcific aortic valve (AV) disease share risk factors and end-stage characteristics. In AV disease, an accumulation of extracellular vesicles (EVs) and lipids, thrombosis, fibrosis, and calcification occur. However, the processes governing BP degeneration are underexplored. We conduct gross and histopathological assessments of BP valves and build proteomic comparison maps of aortic BP degeneration versus AV disease.
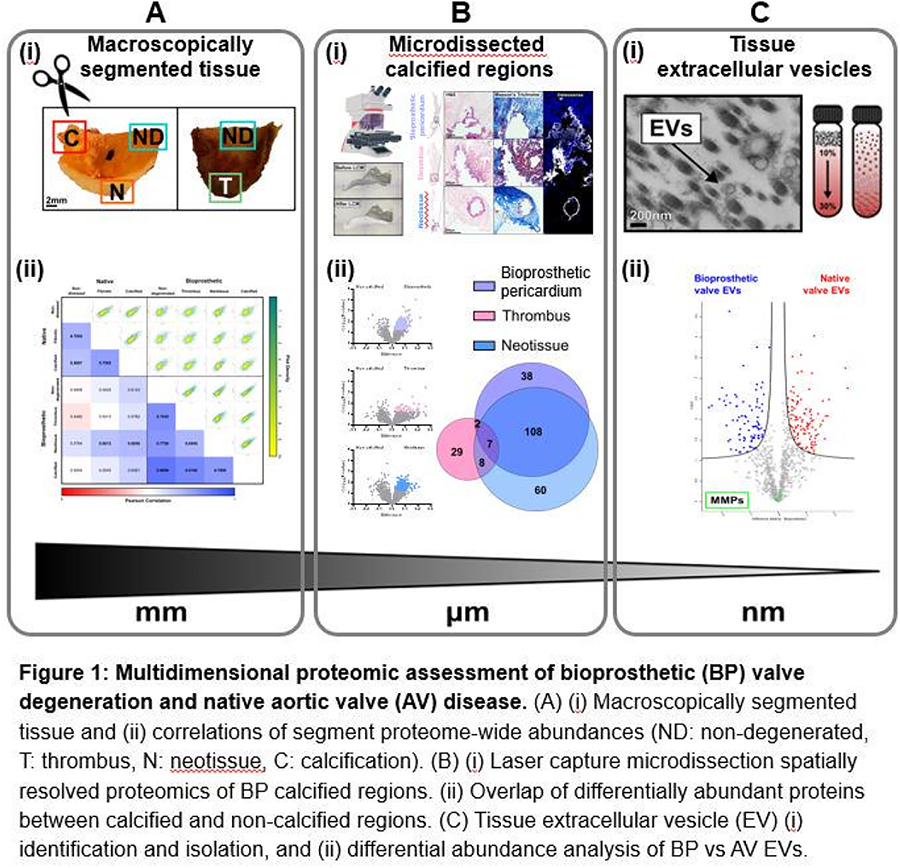
METHODS: Explanted bovine pericardial BP leaflets (n=48) and human AV valves (n=19) were macroscopically segmented according to their diseased states (BP: non-degenerated/thrombotic/neotissue/calcified, AV: non-diseased/fibrotic/calcified), validated by histopathology. Segment-specific proteomics was performed (Fig.1A(i)). Laser capture microdissection enabled spatially resolved proteomics of different BP calcification regions: non-degenerated pericardium, thrombotic, and neotissue (Fig.1B(i)). Valve EVs were isolated by enzymatic digestion, (ultra)centrifugation, density gradient separation, and underwent proteomics (Fig.1C(i)).
RESULTS: Principal component analysis of the BP and AV proteomes (2,005 and 2,012 proteins, respectively) clustered according to their diseased segments. Correlations of segment proteome-wide abundances revealed the highest intra- and inter-tissue similarity between non-degenerated and calcified BP (rp=0.87), and BP neotissue and calcified AV (rp=0.69) (Fig.1A(ii)). Histological analysis quantified the prevalence of calcification within different BP regions (bioprosthetic pericardium, thrombus, neotissue). Only 3% of differentially enriched proteins between calcified and non-calcified regions overlapped, suggesting distinct mechanisms of fibro-calcification (Fig.1B(ii)). For the first time, EVs were isolated from explanted BP valves. A comparison of AV and BP valve EV proteomes suggested that conserved proteins are associated with wound healing (GO:0042060) and include metalloproteinases (MMP9/12/14/23B, TIMP1/3) while coagulation (GO:0072378) and immune (GO:0002697) processes were uniquely enriched in BP EV proteins (Fig.1C(ii)).
CONCLUSIONS: This is the first comparative multidimensional proteomic study of degenerated BP valves and AV disease which may provide valuable insights towards future treatment of xenogenic matrix for commercial tissue valve production.
Presentation Number: AC17Publishing Title: Chemerin Is A Sex-specific Target Mediating The Aortic Valve Alterations In Aortic Stenosis Concomitant With Diabetes Mellitus
Author Block: Mattie Garaikoetxea, Miriam Goñi-Oloriz, Ernesto Martin-Nuñez, Susana San Ildefonso, Paula Castillo, Rafael Sadaba, Eva Jover, Natalia Lopez-Andres.
Navarrabiomed, Pamplona, Spain.
Abstract Body:
OBJECTIVE: Diabetes mellitus (DM) accelerates the progression of aortic stenosis (AS). The diabetic-related complications in AS presents sex-specific differences. Previous data have shown that aldosterone/mineralocorticoid receptor (Aldo/MR) pathway is involved in early stages of AS in a sex-dependent manner as well as in the development of diabetic complications in other cardiovascular diseases. We herein aim to identify new sex-specific targets in AS complicated with DM potentially related to the Aldo/MR axis.
METHODS: Discovery studies were conducted with Olink Proteomics® Proximity Extension™ Assay (PEA™) technology in 87 AS patient-derived aortic valves (AVs) (N=28 non-diabetic men, N=19 diabetic men, N=32 non-diabetic women and N=8 diabetic women). Further discovery approximation was performed in commercial human cytokine array kit (N=24 AV samples/sex/condition). In vitro experiments were performed in valve interstitial cells (VICs) treated with aldosterone (10-8M) with or without the MR antagonist spironolactone (10-6M).
RESULTS: Multivariate analyses revealed chemerin (RARRES2), a previously reported Aldo/MR-sensitive molecule, as a target differentially expressed in male diabetic AS patients. Cytokine array analysis and validation in AVs from 226 patients with severe AS (27% DM, 61.50% men) corroborated this finding. Correlation analysis showed that MR was directly associated with chemerin levels only in AVs from male diabetic patients (r=0.7119, p<0.0001). MR also correlated directly with markers of VIC activation, inflammation and calcification. Aldo significantly enhanced the production of chemerin only in VICs from diabetic male AS patients. In male cells, Aldo increased inflammatory (IL-6, ICAM-1, NGAL) and osteogenic (BMP-2, BMP-4, periostin, RUNX2) markers. Treatment with spironolactone blocked all the above effects. Interestingly, RARRES2-silenced male VICs did not respond to Aldo-induced inflammation and calcification.
CONCLUSIONS: Aldo/MR axis induction of inflammatory and calcific responses in diabetic male AS patients is mediated by chemerin, a new sex-specific target in concomitant AS and diabetes.
Presentation Number: AC18Publishing Title: Virtual Reality Planning For Complex Late Sequelae In Valve Surgery
Author Block: Alessandra Sala1, Francesco Grimaldi1, Jacopo Monti2, Marco Diena1, Carlo de Vincentiis1.
1IRCCS Policlinico San Donato, San Donato Milanese, Italy, 2Artiness srl, Milan, Italy.
Abstract Body:
OBJECTIVE: Virtual reality (VR) is becoming widely available in the medical field. Its application in surgery is not always clear and straightforward. However, in complex anatomical and uncommon situations, it may be decisive in visualising preoperatively the surgical scenario, analyse and cut through different anatomical planes and ultimately plan the most secure surgical technique.
METHODS: We took advantage of a VR platform for the preoperative assessment of a complex third redo surgery with the diagnosis of a massive chronic pseudo-aneurysm of the left ventricle. Due to the complex anatomy of the lesion and unclear point of origin on simple 2D CT scan, we employed an advanced 3D reconstruction software to plan surgical exclusion.
RESULTS: The 47-year-old patient, that had previously undergone two mitral valve replacement surgeries for rheumatic valve disease, was referred to our institution for a massive pseudo-aneurysm of the LV, arising from the mitral valve annulus. The patient underwent reintervention, through median sternotomy. The previously implanted mechanical Starr-Edwards prosthesis was removed, and without excessive time loss, the hole on the ventricular side of the annulus was clearly visible and perfectly reflected the preoperative reconstructions. The entry-point was completely excluded with a heterologous pericardial patch and a novel 27mm mechanical prosthesis was implanted. Pre-discharge CT scan showed complete exclusion of the pseudo-aneurysm, with effective and direct closure of the only orifice, identified with the help of 3D VR reconstruction.
CONCLUSIONS: VR in cardiac surgery becomes of incredible importance in preoperative planning of complex cases, as it allows visualisation of cardiac anatomy and permits sectioning/cutting through different structures to identify the best surgical option.
Presentation Number: AC19Publishing Title: Intraventricular Fluid Dynamics Study Using An In Vitro Model Of Mitral Valve Regurgitation And Edge-to-edge Therapy
Author Block: Cody Kubicki1, Michael Sacks2, Keefe B. Manning1.
1The Pennsylvania State University, University Park, PA, USA, 2University of Texas, Austin, Austin, TX, USA.
Abstract Body:
OBJECTIVE: Degenerative mitral valve disease associated with mitral regurgitation (MR) is pervasive. Of the many treatment options for MR, transcatheter edge-to-edge repair (TEER) is the most common. Despite its prevalence, there have been no publications experimentally quantifying the impacts of TEER on intraventricular hemodynamics. Characterizing flow changes can elucidate potential comorbidities associated with TEER, advance surgical therapy development, and improve MR patient outcomes.
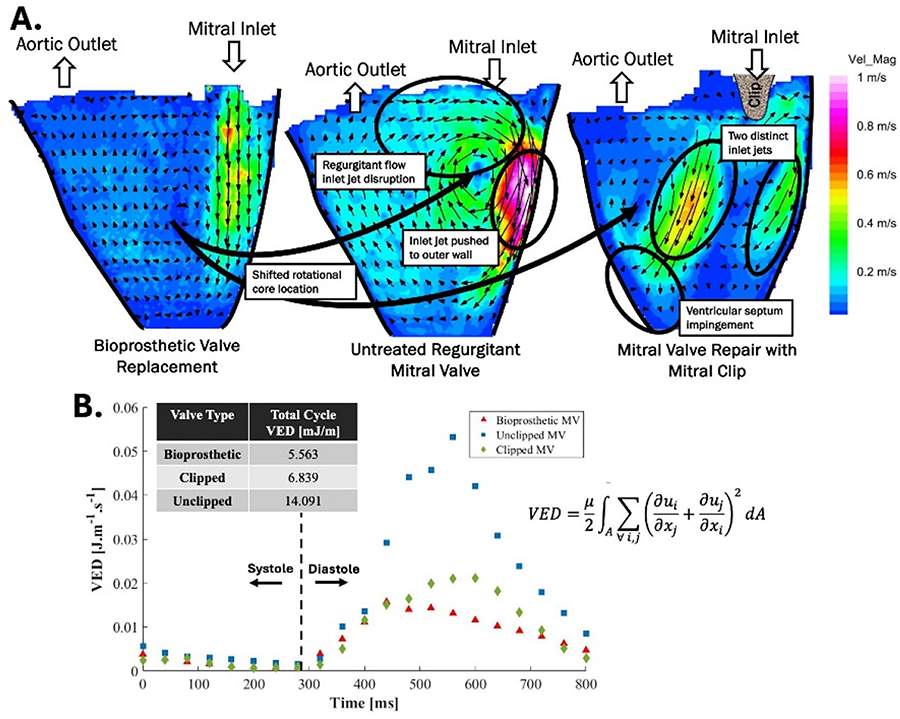
METHODS: We constructed a left ventricle (LV) duplicator with flow visualization capabilities and quantified flow within the LV experiencing MR, both pre- and post-TEER, using particle image velocimetry. The study compared intraventricular flow across three mitral valve cases: (1) an untreated regurgitant mitral valve, (2) a clipped mitral valve following TEER, and (3) a bioprosthetic valve representing complete surgical valve replacement.
RESULTS: The dual-orifice mitral valve post-TEER resulted in suboptimal flow for efficient ventricular filling and ejection. The dual inlet jet flow resulted in interacting vortices and produced a less coherent diastolic rotational flow structure characteristic of healthy ventricular flow (Figure 1A). These changes caused elevated viscous energy dissipation (Figure 1B), which indicates less efficient intraventricular flow and an elevated ventricle workload to maintain a healthy cardiac output.
CONCLUSIONS: A clipped mitral valve following TEER creates a two-orifice inlet to the LV, which drastically changes the fluid dynamics and ventricular efficiency. Reduced intraventricular flow efficiency may indicate the development of comorbidities such as ventricular hypertrophy or reduced ejection fraction resulting in heart failure in patients receiving TEER as a long-term treatment option for MR.
Presentation Number: AC20Publishing Title: The Impact Of Mitral Double-Orifice Asymmetry Post TEER On Hemodynamic Behavior
Author Block: Katell Delanoë1, Erwan Salaun1, Régis Rieu2, Philippe Pibarot1, Viktoria Stanová1.
1Institut Universitaire de Cardiologie et de Pneumologie - Université Laval, Québec, QC, Canada, 2Aix-Marseille Université/ Gustave Eiffel Université, LBA-UMRT24, Marseille, France.
Abstract Body:
OBJECTIVE: Transcatheter Edge-to-Edge Repair (TEER) is the most common percutaneous repair procedure for patients with severe mitral regurgitation who cannot undergo surgical intervention. However, due to the novelty of the procedure, long-term consequences of the intervention still need to be assessed. Aim of this study is to understand the influence of the MitraClip position on hemodynamic behavior.
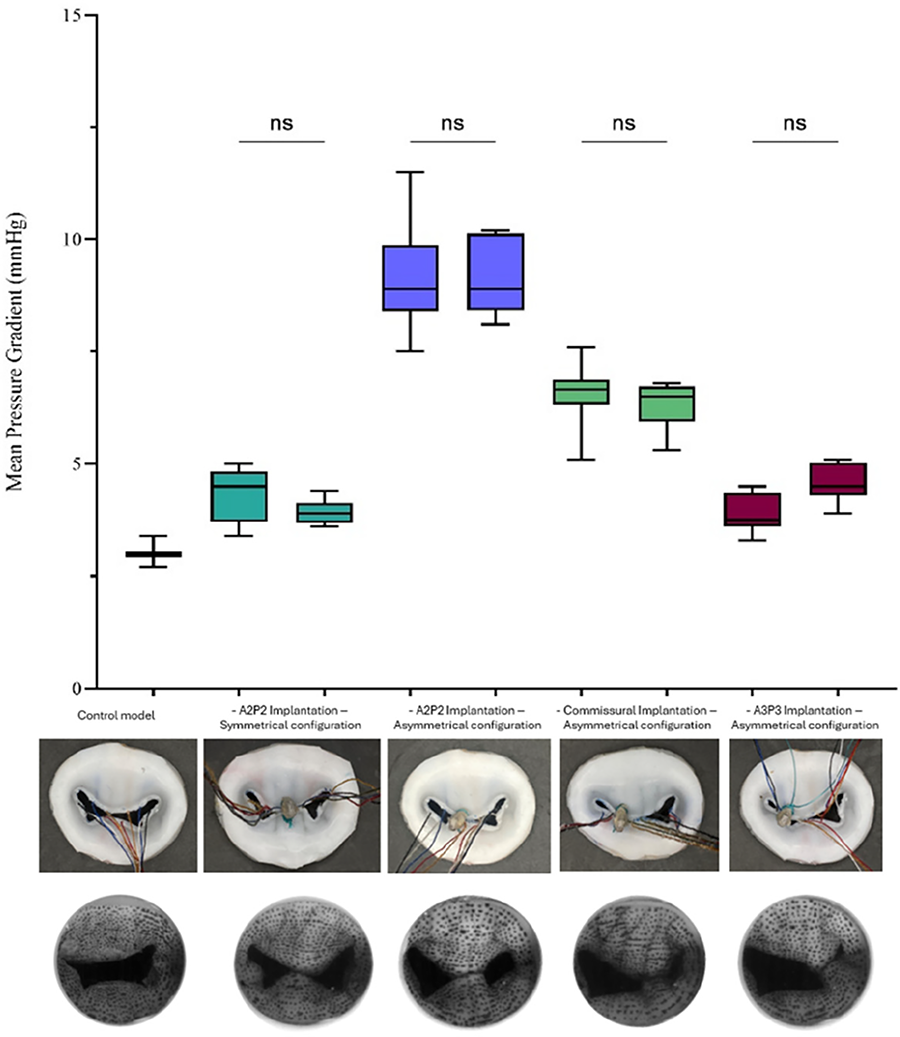
METHODS: Custom-made three-dimensional (3D) model of a physiological mitral valve (MV) using a specific silicon combination examined in previous studies was fabricated. Chordae was added between the silicon layers to ensure leaflet tension during cardiac cycle. A MitraClip was then placed at different positions to evaluate the influence of the double-orifice asymmetry on the hemodynamic response. Each configuration was tested on a dual-activation simulator under different physiological conditions (Heart Rate=70bpm, Stroke Volume=30, 50, 70mL, Mean Aortic Pressure=100mmHg). Doppler echocardiographic measurements were used to assess MV hemodynamic parameters.
RESULTS: In normal flow conditions (70bpm, 70mL, 100mmHg), the hemodynamic behavior (mean gradient, EOA) was affected by the device's lateral position. Symmetrical A2P2 configuration induced the lowest gradients and largest EOAs (4.36+/-0.44mmHg and 2.12+/-0.13cm2, p<0.001) and was followed by A3P3 implantation (4.80+/-0.42 and 1.93+/-13), commissural implantation (6.45+/-0.58 and 1.74+/-0.16) and finally asymmetric A2P2 implantation causing iatrogenic mitral stenosis (9.15+/-0.97 and 1.35+/-0.29). There was no or minimal mitral regurgitation after MitraClip implantation.
CONCLUSIONS: This study demonstrates that the position of the clip has a profound effect on mitral valve hemodynamics post-TEER. The position of the clip leading asymmetric configurations (i.e. 2 valve orifices of different sizes) was associated with worse mitral valve hemodynamics compared to symmetric configuration. Furthermore, all asymmetrical configurations were not equivalent and the worst hemodynamic performance was with A2-P2 asymmetrical implantation. The results demonstrate the usefulness of in vitro experiments to optimize the procedural strategy of TEER in terms of number and position of clips.
Presentation Number: AC21Publishing Title: Predictive Computational Modeling In Optimizing Surgical Outcome Of Valve-Sparing Aortic Root Replacements
Author Block: Sandra Loerakker1, Jur van Kimmenade1, Justina Ghebryal1, Morten Smerup2, Jesper Hjortnaes3.
1Eindhoven University of Technology, Eindhoven, Netherlands, 2Rigshospitalet - Copenhagen University Hospital, Copenhagen, Denmark, 3Leiden University Medical Center, Leiden, Netherlands.
Abstract Body:
OBJECTIVE: Aortic root dilatation disturbs valvular geometry, potentialy leading to aortic insufficiency. Valve-sparing aortic root replacement (VSRR) aims to restore valve function while preserving native valve leaflets [1]. Optimal valve function relies on surgical geometric adjustments to ensure sufficient coaptation, but predicting their effects on performance is challenging due to complex geometric relationships [2]. This computational study aims to examine the effect of geometric features on valve function. A better understanding of these factors will improve patient-specific surgical planning and, in turn, surgical outcomes.
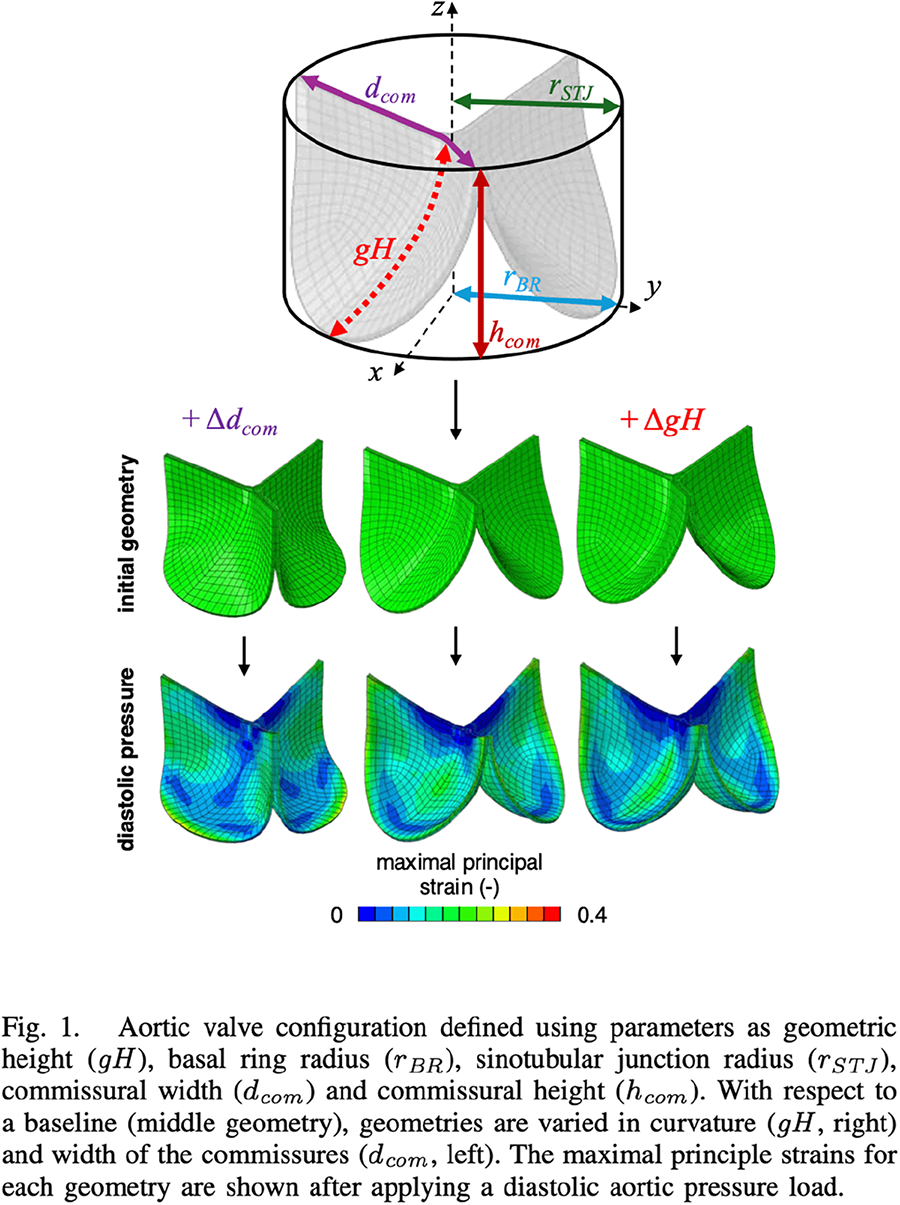
METHODS: To simulate valve deformation, a finite element model based on the Gulbulak valve geometry description was developed [3]. Geometrical manipulations were applied relative to a baseline geometry (Figure 1). A diastolic aortic pressure load of 75 mmHg was applied to evaluate coaptation surface area and strain distributions in diastole.
RESULTS: Initially, the baseline geometry exhibited the lowest coaptation area, while the elongated commissure geometry had the highest coaptation. Under diastolic pressure, the elongated geometric height geometry had the smallest increase in coaptation area, whereas the baseline showed the largest increase. Strain distributions within leaflet bellies were higher in the baseline and elongated geometric height geometries than in the elongated commissure geometry.
CONCLUSIONS: This study presents a computational framework for evaluating how geometric features of valve leaflets affect valve functionality. Here, it is shown that commissural width and geometric height influence coaptation and strain distribution differently. In the context of VSRR, achieving similar improvements in coaptation across different geometries may require tailored surgical approaches. Future work will investigate the effects of other geometric features.
[1] T.E. David and C.M. Feindel, J Thorac Cardiovasc Surg, 1992. [2] S. Matsushima et al., Indian J Thorac Cardiovasc Surg, 2020. [3] U. Gulbulak et al., J Mech Behav Biomed Mater, 2020.
Presentation Number: AC22Publishing Title: Propensity-matched 8-year Outcomes Following Surgical Aortic Valve Replacement With Novel Calcification-resistant Versus Contemporary Tissue Bioprostheses
Author Block: Tsuyoshi Kaneko, Douglas Johnston, Joseph E. Bavaria, Vinod Thourani
Edwards Lifesciences, Irvine, CA
Abstract Body:
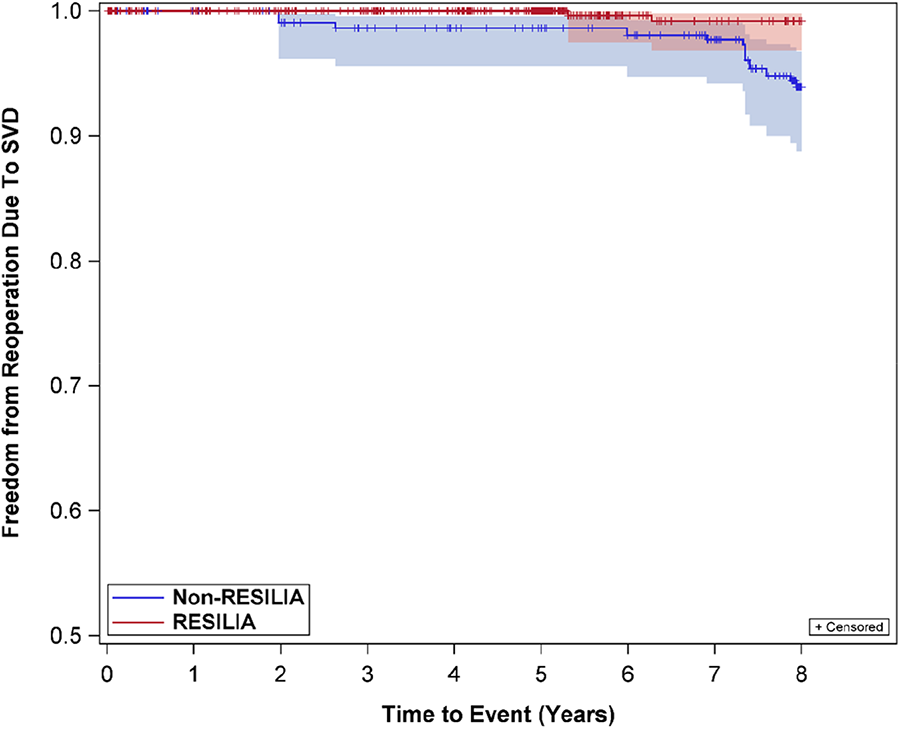
Purpose: Aortic bioprostheses with RESILIA tissue have demonstrated strong outcomes through 7 years of follow-up. However, studies comparing RESILIA tissue valve (RTV) outcomes to non-RTV (NRTV) outcomes are lacking. This study sought to determine if surgical aortic valve replacement (SAVR) outcomes in patients implanted with RTV were superior to those with NRTV at 8 yrs.
METHODS: The study cohort consisted of 689 RTV and 258 NRTV SAVR patients. To account for differences in baseline characteristics in the two cohorts, stabilized inverse probability of treatment weighting (sIPTW) with propensity score was used. Safety endpoints were compared between cohorts with sIPTW-adjusted Kaplan-Meier analyses and log-rank tests. The propensity score was calculated using a logistic regression model based on pre-specified baseline variables, including but not limited to age, sex, BMI, NYHA class, diabetes, and renal failure/insufficiency. Safety endpoints included reoperation due to SVD, SVD, all-cause reoperation, and all-cause mortality.
RESULTS: The mean age of the matched cohort was 67 yrs. old with a majority of patients female. After sIPTW adjustment, all pre-specified clinically relevant baseline variables were appropriately matched, resulting in no covariate differences between cohorts. Importantly, freedoms from reoperation due to SVD (99.2%, RTV vs. 93.9% NRTV; log-rank p-value= 0.0003), SVD (99.3%, RTV vs. 90.5% NRTV; log-rank p-value< 0.0001) and all-cause reoperation (97.0%, RTV vs. 90.5% NRTV; log-rank p-value= 0.0007) were statistically different between cohorts at 8 yrs. In addition, freedom from all-cause mortality was not statistically different between the two cohorts (83.3%, RTV vs. 81.3% NRTV; log-rank p-value= 0.3166). 81.3% NRTV; log-rank p-value= 0.3166).
CONCLUSIONS: In this propensity-matched patient population, SAVR with novel calcification-resistant tissue was associated with significantly lower rates of reoperation due to SVD, SVD, and all-cause reoperation at 8 yrs with similar rates of all-cause mortality also observed.
[3] U. Gulbulak et al., J Mech Behav Biomed Mater, 2020.
Presentation Number: AC23Publishing Title: In Vitro Study Of The Effect Of Geometric Differences On Bioprosthetic Aortic Valve Hemodynamics
Author Block: Nicolas Bueno1, Viktória Stanová1, Katell Delanoë1, Philippe Pibarot1, Julien Favier2.
1Institut universitaire de cardiologie et de pneumologie de Québec - Université Laval (IUCPQ-UL), Québec, QC, Canada, 2Laboratoire de Mécanique, Modélisation et Procédés Propres (M2P2) Aix Marseille Université, CNRS (UMR7340), Ecole Centrale de Marseille, Marseille, France.
Abstract Body:
OBJECTIVE: Bioprosthetic aortic valve (BAV) design influence hemodynamics and durability. This study aims to improve understanding of the geometry-hemodynamics relationship in BAV and to provide a foundation for evaluating the impact of specific geometries in native valves.
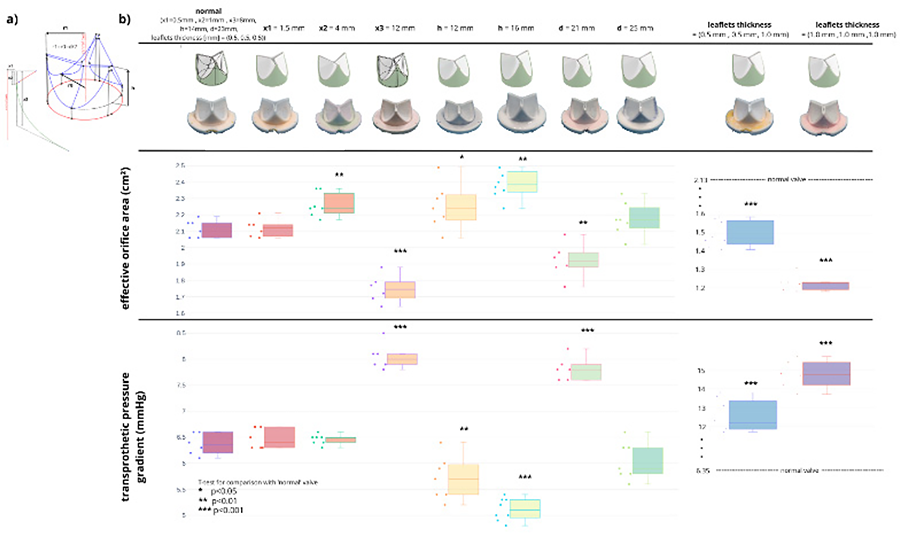
METHODS: A parametric valve design was used for this study (Figure 1a). A ‘normal’ geometry was based on a BAV Trifecta 25mm (inner diameter 23mm) from which nine variations were created by adjusting single parameter (diameter, leaflet height, curvatures and thickness). 10 molds, one for each model, were generated using custom-coded Python program, then 3D printed (Lulzbot Inc., ND, USA) and filled with silicone (DragonSkin30, Smooth-On, Inc., PA, USA). The stent for each valve was 3D printed. A cardiac simulator was used for in vitro testing of BAV and custom-made valves. The heart rate was set to 70 bpm, mean aortic pressure to 100 mmHg, stroke volume to 70 ml. Mean transprosthetic pressure gradient (TPG) and effective orifice area (EOA) were measured by continuous-wave Doppler (GE Vivid 7, GE Health Medical, Norway).
RESULTS: There was no significant difference (p>0.05) between the BHV vs silicone hemodynamic parameters (TPG: 6.08±0.36 vs 6.37±0.21 mmHg, EOA: 2.15±0.14 vs 2.12±0.05). As expected, increased leaflet thickness, smaller diameters (d) and greater leaflet belly curvature (x3) reduced significantly (p<0.01) the performance in terms of TPG and EOA. However, bigger diameter (d), bigger angle (x2) and taller leaflets (h) improved the hemodynamic performance.
CONCLUSIONS: This study demonstrates that silicone valves are suitable for evaluating the hemodynamic performance of various BHV geometries. Additional investigations will be carried out to examine the strain field, which is associated with the development of calcification. Patient-specific aortic valves will be developed and evaluated as the next step.
Presentation Number: AC24Publishing Title: Trends In Incidence And Outcomes Of Surgical Conversion For Transcatheter Aortic Valve Replacement In The United States
Author Block: Daniel McGrath1, Charley Sun2, Michael Zhu2, Aaron Sparks1, Lawrence Lee1, Yong Zhan1.
1Tufts Medical Center, Boston, MA, USA, 2Tufts University School of Medicine, Boston, MA, USA.
Abstract Body:
OBJECTIVE: As the use of transcatheter aortic valve replacement (TAVR) expands, some intraprocedural complications continue to necessitate conversion to emergent open cardiac surgery. The need for on-site surgical backup remains a topic of debate. This study investigates the current incidence and outcomes of surgical conversions during TAVR in the United States.
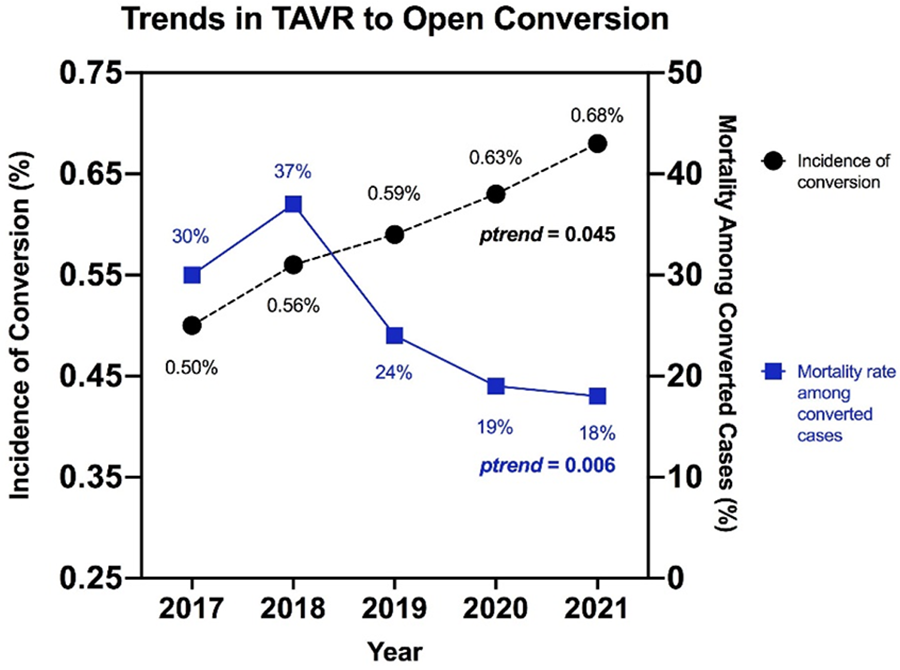
METHODS: We queried the National Inpatient Sample Database to identify patients aged 18 and older who underwent percutaneous TAVR as the primary procedure between 2017 and 2021. Conversion was defined as any open cardiac surgery performed within one day following TAVR. We compared the characteristics and outcomes of patients with and without conversions and analyzed trends in conversion incidence and in-hospital mortality.
RESULTS: Our analysis included 68,141 TAVR patients, of whom 410 (0.6%) required surgical conversion. The incidence of conversion increased from 0.50% to 0.68% over the study period (ptrend=0.045), while in-hospital mortality decreased from 30.0% to 17.9% (ptrend=0.006) (see Figure). Patients who underwent conversion were younger (73.9±12.4 vs. 78.5±8.5 years, p<0.001) and had a similar comorbidity burden (Charlson Comorbidity Index: 2.9±2.0 vs. 3.0±2.0, p=0.499). However, they experienced significantly higher in-hospital mortality (23.5% vs. 1.1%, p<0.001) and longer hospital stays (11.1±11.1 vs. 3.5±5.1 days, p<0.001). Independent risk factors for surgical conversion included liver disease (OR 1.63, 95% CI 1.14-2.35, p=0.008), malnutrition (OR 3.79, 95% CI 2.32-6.20, p<0.001), and rheumatic valve disease (OR 1.61, 95% CI 1.18-2.21, p=0.003). Prior coronary artery bypass graft surgery emerged as an independent negative predictor (OR 0.41, 95% CI 0.26-0.64, p<0.001).
CONCLUSIONS: This study reveals a concerning increase in the incidence of surgical conversions during TAVR, underscoring the necessity for cardiac surgical backup to facilitate timely intervention for life-threatening complications. Recognizing risk factors may enhance procedural planning and improve TAVR outcomes.
Presentation Number: AC25Publishing Title: Polymorphic Size Of Lipoprotein (a) And Structural Bioprosthetic Valve Degeneration
Author Block: Romain Capoulade1, Mikaël Croyal1, Thomas Senage1, Guillaume Guimbretiere1, Cedric Le May1, Arsenio Rodriguez Oliveira1, Maxime Carpentier1, Nicolas Piriou1, Imen Fellah-Hebia1, Cristina Costa2, Marta Vadori3, Manuel Galinanes4, Raphael Manez2, Jean-Michel Serfaty1, Jean-Paul Soulilou5, Emanuele Cozzi3, Vered Padler-Karavani6, Jean-Christian Roussel1, Bertrand Cariou1, Thierry Le Tourneau1.
1l'institut du thorax, Nantes, France, 2Bellvitge University Hospital-ICS, Barcelona, Spain, 3Padua University Hospital, Padua, Italy, 4University Hospital Vall d'Hebron, Barcelona, Spain, 5Center for Research in Transplantation and Translation Immunology, Nantes, France, 6Tel Aviv University, Tel Aviv, Israel.
Abstract Body:
OBJECTIVE: The use of biological heart valves (BHV) is constantly growing but their durability remains a main concern. Structural valve degeneration (SVD) occurs gradually and seems to reiterate, at least in part, the processes described in native valve stenosis. Lipoprotein (a) [Lp(a)] has been described as one of the main triggers of native valve calcification but its association with SVD remains unclear. We aim to determine whether Lp(a) plasma levels and/or the Lp(a) polymorphic sizes, determined by the apolipoprotein (a) [apo(a)] Kringle-IV copy number, were associated with SVD.
METHODS: 332 patients with BHV for at least 4 years from the Translink study were included. SVD was assessed on echocardiography and computed tomography. Lp(a) concentration was determined by immunoturbidimetry method and the apo(a) Kringle-IV copy number by liquid chromatography-tandem mass spectrometry. Univariable and multivariable models, adjusted for clinically relevant and statistically significant variables, were used to determine the independent association between Lp(a) concentrations and/or apo(a) Kringle-IV copy numbers with SVD.
RESULTS: Among the 332 patients included in this study, 76 (23%) presented clinically significant SVD on echocardiography. Bioprosthetic valve calcification was significantly higher in patients with versus without SVD (128 [24-259] vs 42 [0-150] mm3, p=0.005). Low apo(a) Kringle-IV copy number was associated with an increased risk of SVD (OR=2.71 [1.34-5.50], p=0.006), but not Lp(a) concentration (OR=0.99 [0.84-1.15], p=0.85). This association remained significant (OR=3.21 [1.31-7.84], p=0.01) after multivariable adjustments including Lp(a) concentration. The analysis of the transprosthetic mean gradient and bioprosthetic valve calcification provided consistent results (all p≤0.05).
CONCLUSIONS: This cross-sectional study from the Translink trial demonstrates the association between Lp(a) polymorphic size and SVD, highlighting a potential therapeutic option to limit the occurrence of SVD in selected patients who underwent AVR with surgical or transcatheter BHV.
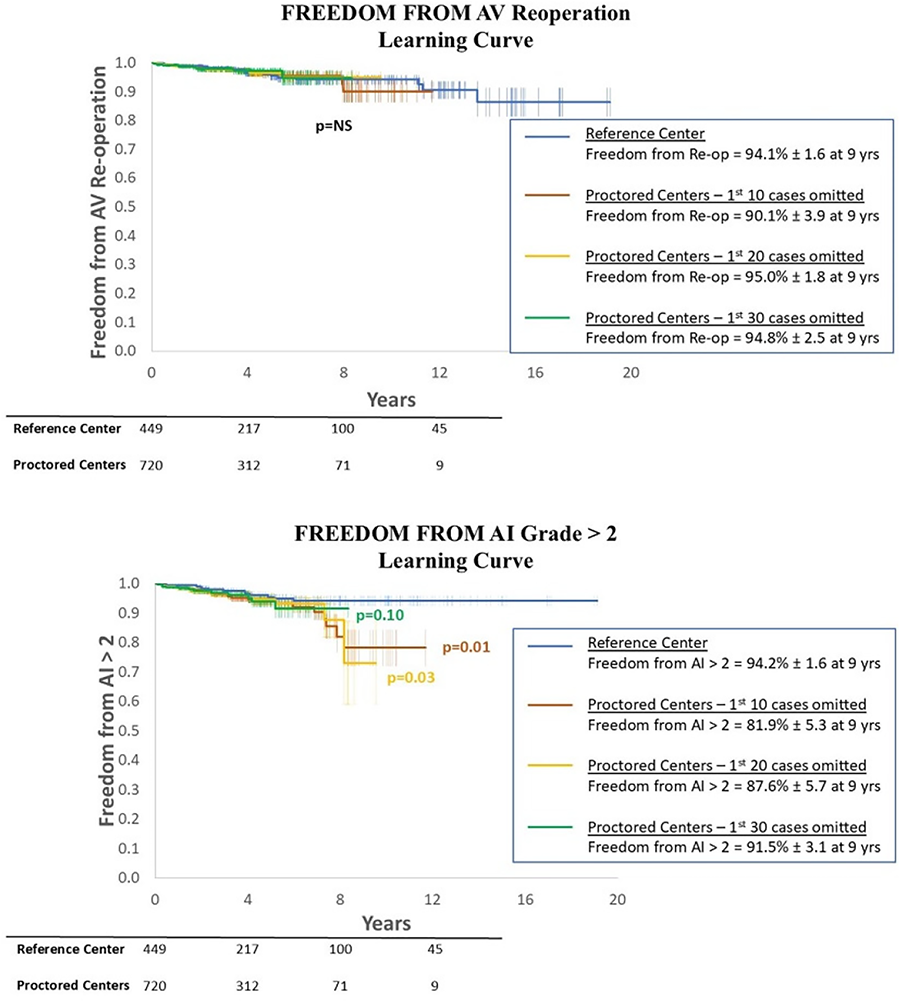
Presentation Number: AC26Publishing Title: Learning Curve For Standardized Valve-sparing Aortic Root Replacement Using The Remodelling Technique And External Ring Annuloplasty: Comparison Between Reference And Proctored Centers From 18 Countries
Author Block: Pouya Youssefi1, Pichoy Danial2, Ismail El-Hamamsy3, Vincent Chauvette3, Olivier Bouchot4, Igor Rudez5, Gianclaudio Mecozzi6, Jan Vojacek7, Pavel Zacek7, Peter Verbrugghe8, Adrian Kolesar9, Alejandro Crespo de Hubsch10, Christian Dinges11, Eric Bergoend2, Jaroslav Hlubocky12, Frederiek De Heer13, Maciej Matuszewski14, Marek Jasinski15, Francesco Patane16, Arnaldo javier Estigarribia17, Claudia Romagnoni18, Nathanael Shraer19, Mathieu Debauchez2, Emmanuel Lansac2.
1Royal Brompton & Harefield NHS Trust, London, United Kingdom, 2Pitie-Salpetriere Hospital, Sorbonne University, Paris, France, 3Mount Sinai Hospital, New York, NY, USA, 4Hospital Center University Dijon Bourgogne, Dijon, Dijon, France, 5University Hospital Dubrava, Zagreb, Croatia, 6University Medisch Centrum Groningen, Groningen, Netherlands, 7University Hospital in Hradec Kralove, Hradec Kralove, Czech Republic, 8Cardiac Surgery, KU Leuven, Belgium, Leuven, Belgium, 9Eastern Slovak Institute of Cardiovascular Disease, Kosice, Slovakia, 10Hospital de Cruces, Bizakaia, Spain, 11Paracelsus Medical University, Salzburg, Austria, 12General University Hospital, Prague, Czech Republic, 13Academic Medical Center, Amsterdam, Netherlands, 14New Cross Hospital, Wolverhampton, United Kingdom, 15Wroclaw Medical University, Wroclaw, Poland, 16Azienda Ospedaliera Papardo, Messina, Italy, 17Hospital Rambla, Santa Cruz de Tenerife, Spain, 18Policlinico, Milan, Italy, 19Necker Sick Children Hospital, pari, France.
Abstract Body:
OBJECTIVE: Compare outcomes of a standardized valve-sparing aortic root replacement using remodelling technique and external ring annuloplasty between a reference center (RC) and proctored centers (PC).
METHODS: Primary end-points were all-cause mortality, freedom from aortic valve (AV) re-intervention and freedom from AI grade>2.
RESULTS: A total of 1,169 patients were included (449 from RC, 720 from PC originating from 18 countries). Mean case number for PC was 40 (range 2-131). There was no difference in demographics between the 2 groups nor pre-operative AI grade. Survival at 9 years was similar (89.4% in RC vs 89.7% in PC, p=0.84), as was freedom from AV-related reintervention (94.1% for RC, 89.8% for PC, p=0.48). Freedom from AI Grade>2 was significantly better for RC at 9 years (94.2% vs 84.2% for PC, p=0.02). When assessing for the learning curve, this difference was still significant when excluding the first 10 or 20 cases of each center (p=0.01 and p=0.03 respectively). However, when excluding the first 30 cases, outcomes for PC improved and freedom from AI Grade>2 became similar (95.5% for RC, 91.5% for PC at 9 years, p=0.1). Freedom from AI Grade>2 was worse in lower volume centers (94.2% for ≥20 cases/yr, 95.6% for 10-19 cases/yr, 84.9% for 5-9 cases/yr, 87.5% for <5 cases/yr at 8 years, p<0.05), but this difference disappeared when excluding the first 30 cases (p=0.1).
CONCLUSIONS: A standardized valve-sparing aortic root replacement using the remodelling technique and external ring annuloplasty has reproducible long-term results with similar survival and freedom from AV-related reintervention in the hands of both a reference center as well as proctored centers. There are differences in freedom from recurrent AI which disappear following the first 30 cases, indicating this is the number required to surpass the learning curve.
Presentation Number: RF1Publishing Title: Menopausal Age And Risk Of Arrhythmic Mitral Valve Prolapse
Author Block: Lionel Tastet1, Luca Cristin1, Rohit Jhawar1, Amy Rich1, Dwight Bibby1, Qizhi Fang1, Anoop Muniyappa1, Viktória Stanová2, Marie-Annick Clavel2, Francesca N. Delling1.
1University of California San Francisco, San Francisco, CA, USA, 2Institut universitaire de cardiologie et de pneumologie de Québec-Université Laval, Québec, QC, Canada.
Abstract Body:
BACKGROUND: Studies suggest a higher arrhythmic risk, including sudden cardiac death (SCD), among women with mitral valve prolapse (MVP). However, the relationship between menopause and arrhythmic risk in MVP remains unclear. This study examined the association between menopausal age and arrhythmic MVP.
METHODS: We included 299 consecutive women with MVP (mean age 58±16 years) and comprehensive clinical, echocardiographic, and ECG data. Documented diagnosis of menopause (≥12 months without menstruation) was obtained through medical records. Patients were categorized as follows: 1) premature menopause (<40 years), 2) early menopause (40-45 years), 3) expected age of menopause (45-55 years), 4) pre/perimenopausal, and 5) undetermined age at menopause. Arrhythmic MVP was defined by a composite of SCD or arrest, ventricular fibrillation (VF)/tachycardia, or frequent ventricular ectopy.
RESULTS: Arrhythmic presentations occurred in 25% (n=76), 67% were postmenopausal, and 72% had no/mild mitral regurgitation (MR) at diagnosis. Menopause transition was premature in 2.3%, early in 4.4%, at expected age in 49.8%, and 30.8% were pre/perimenopausal; 12.7% had undetermined menopausal age. Postmenopausal hormone therapy use was 12% (n=36). Arrhythmic rate was significantly higher in those with premature or early menopause compared to other groups (55% vs 23%, 26% and 15% respectively; p=0.01), including one prior case of VF in the premature menopause group. After adjustment for age, atrial fibrillation, bileaflet involvement, MR severity, and left ventricular ejection fraction, premature/early menopause remained significantly associated with arrhythmic MVP risk (odds ratio [OR]: 4.39 [95% CI, 1.58-12.2]; p=0.004). Further adjustment for mitral annular disjunction or hormone therapy yielded consistent results (all, OR≥4.78; p<0.01).
CONCLUSIONS: Among women with MVP, those experiencing premature or early menopause had an increased risk of arrhythmic events, including ventricular fibrillation. Further studies are needed to unveil the mechanisms linking ventricular arrhythmia and menopause in MVP.
Presentation Number: RF2Publishing Title: Maternal And Neonatal Outcomes Among Pregnancies Complicated By Rheumatic Mitral Valve Disease In A Tertiary Hospital - A 3-year Retrospective Study
Author Block: Cassius Kay Gapol Ramos, Neil Wayne Salces.
Vicente Sotto Memorial Medical Center, Cebu, Philippines.
Abstract Body:
OBJECTIVE: Rheumatic heart disease (RHD) is common in the Philippines, yet there are limited studies to describe the outcome of pregnancies with RHD. This study then seeks to define the maternal and neonatal outcomes of pregnant women with rheumatic mitral valve disease.
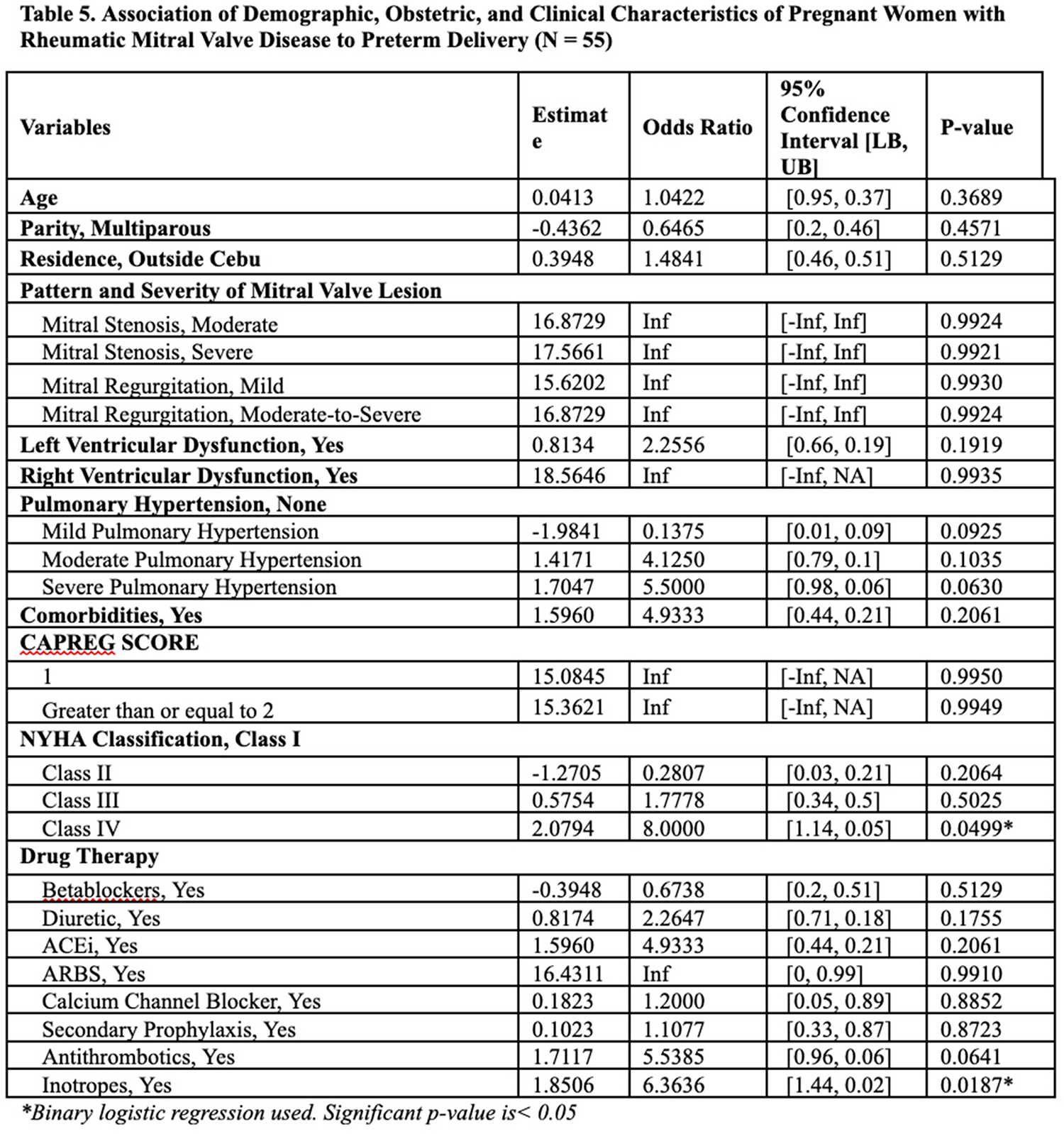
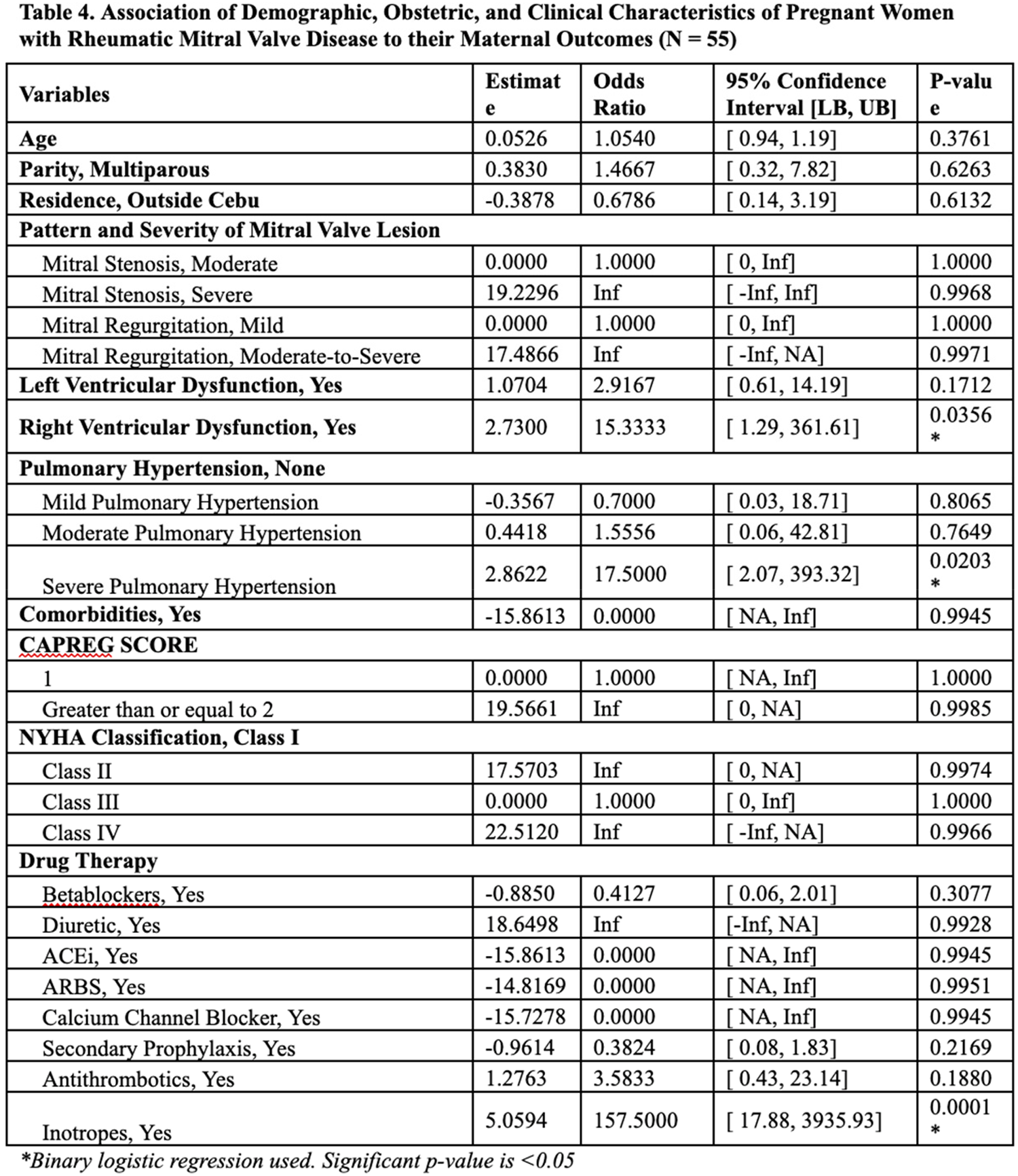
METHODS: A single-center, retrospective analysis of pregnant women admitted for delivery at the Vicente Sotto Memorial Medical Center from April 2020 to December 2023 was performed. Pregnant women with rheumatic mitral valve disease were identified. Data on clinical and sociodemographic factors, maternal mortality and complications, and neonatal adverse clinical events were collected. Logistic regression analysis was performed to determine the odds ratio for the risk factors for maternal mortality and preterm birth.
RESULTS: A total of 55 participants were included in the study. The mean age is 27 years old and 55% are multiparous. Sixty-four percent have mitral regurgitation and 36% have mitral stenosis with 49% and 22% belonging to severe lesions, respectively. The mortality rate showed 15% heart failure, pulmonary complications, and arrhythmia are common secondary outcomes, and 47% were subjected to Cesarean delivery. Right ventricular dysfunction (OR 15.33) and severe pulmonary hypertension (OR 17.50) emerge as significant predictors of mortality. Use of inotropes (OR 157.5) is also strongly associated with adverse maternal outcomes. Severe pulmonary hypertension (OR 8.0) and NYHA Class IV (5.5) are significant predictors of preterm birth.
CONCLUSIONS: Pregnant women with RHD are associated with significant mortality. Arrhythmia and Heart failure are the most common maternal cardiac complications. Critical care management in these patients with signs of severe pulmonary hypertension and right ventricular dysfunction is needed especially in a setting that requires inotropic support. Intensive care and early referral to neonatologists are of utmost importance.
Presentation Number: RF3Publishing Title: Comparative In Vitro Hemodynamic Assessment Of Mitral Annular Calcification And Rheumatic Mitral Stenosis Using Patient-specific 3d-printed Models
Author Block: Mohammad Saber Hashemi1, Atif Nehvi2, Gregg Pressman2, Arash Kheradvar1.
1University of California, Irvine, Irvine, CA, USA, 2Thomas Jefferson University, Philadelphia, PA, USA.
Abstract Body:
OBJECTIVES: Mitral annular calcification (MAC) is an increasingly recognized cause of valve stenosis, associated with symptoms such as dyspnea and effort intolerance. Structural valve changes due to MAC are distinct from rheumatic mitral stenosis, as are the associated hemodynamics. This study aims to compare in vitro hemodynamics of three patient-specific 3D-printed mitral valves: a normal valve, a rheumatic valve with severe stenosis, and a valve with severe MAC. By focusing on in vitro flow characteristics associated with severe MAC, we aim to define the contribution of this valvular pathology to altered hemodynamics, eliminating the confounding effects of multiple comorbidities prevalent in MAC patients.
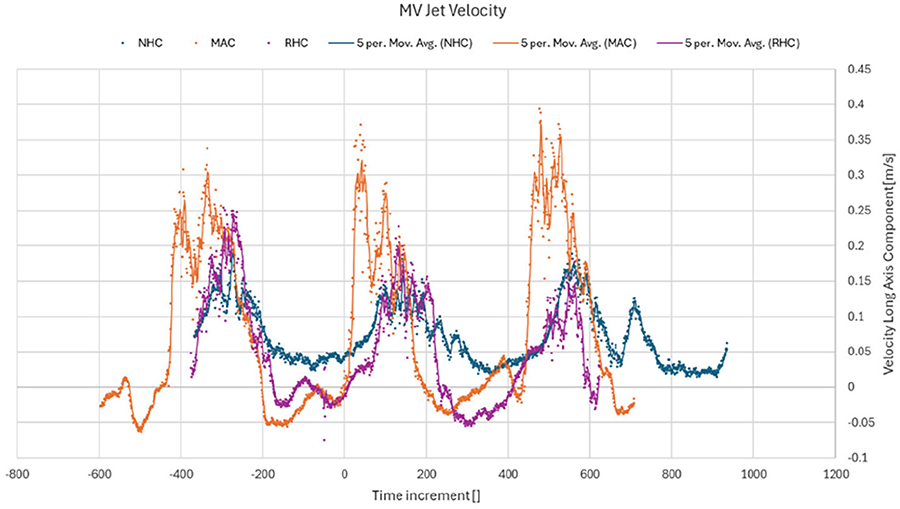
METHODS: We used KLAB heart flow simulator, where a scaled-up left ventricular (LV) model made of thin silicone was installed in a chamber pressurized by a pulsatile pump, simulating normal physiological volume changes. An SJM bioprosthetic valve used as the aortic valve, while three different 3D printed valves used at mitral position, representing: Normal Heart Condition (NHC), Rheumatic-stenosis Heart Condition (RHC), and Mitral Annulus Calcification (MAC). The mitral valves were 3D-printed based on 3D geometries extracted from 4D echocardiography of patients, made from silicone rubber with hard plastic overlays on the leaflets for calcification. Particle Image Velocimetry (PIV) was used to capture LV hemodynamics over several heart cycles.
RESULTS: The transmitral velocities indicated that mitral jet velocity peaks were significantly higher in MAC and marginally higher in RHC compared to NHC, while the average vorticity near the mitral valve was higher in NHC and MAC compared to RHC.
CONCLUSION: Our in vitro studies using patient-specific valve models highlights the unforeseen effects of MAC on LV hemodynamics compared to conditions due to RHC. These findings could inform improved diagnostic criteria, and potential interventions, enabling more targeted management of MAC.
Presentation Number: RF4Publishing Title: High-dimensional Multimodal Analysis Exploring Novel Biological Mechanisms Of Rheumatic Heart Valve Disease
Author Block: Adrien Lupieri1, Thanh-Dat Le1, Livia S. A. Passos1, Prabhash K. Jha1, Sasha A. Singh1, Taku Kasai1, Walderez O. Dutra2, Maria Carmo P. Nunes2, Victor Nizet3, Robert A. Levine4, Elena Aikawa1.
1Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA, 2Federal University of Minas Gerais, Belo Horizonte, Brazil, 3University of California San Diego, La Jolla, CA, USA, 4Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Abstract Body:
OBJECTIVE: Rheumatic heart valve disease (RHVD) is an autoimmune complication resulting from Streptococcus pyogenes infection, triggering mitral valve (MV) damage. It is a leading cause of acquired heart failure valve disease in children and young adults, affecting approximately 40 million people worldwide. Despite its considerable impact, pathophysiology remains poorly understood due to historical neglect by the scientific community.
METHODS: In an international collaborative initiative, we enrolled a cohort of RHVD patients (n=51) and control (n=21), including echocardiographic assessments and MV tissue samples. We employed unbiased proteomics on MV tissue to investigate proteomic changes associated with RHVD. This analysis was enhance through multimodal approaches, including correlation with echocardiographic phenotypes, integration with plasma proteomic data (n=215 RHVD, n=230 control), and integration with murine model of autoimmune valvular carditis (K/B.g7), which replicates outcomes observed in human RHVD
RESULTS: Our analysis revealed critical involvement of pathways related to extracellular matrix (ECM), inflammation, angiogenesis, and hemostasis, including TGFβ, PDGF, VEGF, and IGF/IGFBP pathways. Correlation with echocardiographic measurement using linear regression and weighted correlation network analysis demonstrated a strong association between disease progression and processes related to hemostasis/platelets and inflammation. Characterization of shared proteins and enrichment between MV and plasma proteomics emphasized robust associations with ECM, platelet, TGFβ and IGF/IGFBP pathways. Integration of single-cell RNA sequencing data from mouse MV with human MV proteomic findings identified key disease-driving cell populations, that are also present in human rheumatic MVs. These include myofibroblasts, mesothelial-like cells, T cells, and B cells, some of which are associated with TGFβ and IGF/IGFBP pathways.
CONCLUSIONS: Our high-dimensional multimodal analysis provides critical insights into the molecular and cellular mechanisms driving RHVD progression, characterizing key processes related to disease advancement and identifying novel therapeutic targets and potential biomarkers, which include platelets-associated factor and IGFBPs.
Presentation Number: RF5Publishing Title: Cellular And Connective Tissue Composition Of The Three Aortic Interleaflet Triangles - Functional Implications
Author Block: Najma Latif1, Padmini Sarathchandra2, Albaraa Al Holy2, Adrian Chester1, Magdi H. Yacoub1.
1Imperial College, Magdi Yacoub Institute, Heart Science Centre, Harefield Hospital, United Kingdom, 2Magdi Yacoub Institute, Heart Science Centre, Harefield Hospital, United Kingdom.
Abstract Body:
OBJECTIVE: The aortic valve apparatus performs extremely sophisticated functions. These functions depend on the composition and interaction of the different components. To date these studies have largely ignored the interleaflet triangles (ILTs). We, here, examine the tissue components of the ILTs and characterises the cells that are present within this region of the aortic root.
METHODS: Human aortic valves were collected (n=10), and each triangle was processed for immunohistochemical staining.
RESULTS: The three ILTs differed in size and macroscopic appearance, with the triangle between the non-coronary to left coronary leaflet (N-L) being the largest and most clearly defined. Each ILT was comprised of up to 5 distinct layers of tissue, each layer varying in thickness between the ILTs; an innermost endothelial layer, an inner elastin-rich layer, a thicker outer layer comprising of densely packed layers of collagen and glycosaminoglycans and an outer layer of intermingled myocardial and adipose tissue. The L-R (left-right) ILT had the thinnest layers of elastin and collagen (p<0.05). The N-L was the most fibrous ILT with supporting adipose tissue and the least myocardial support. An intermittent band of cells was expressed under the luminal surface expressing smooth muscle cell α-actin with a reduced and variable expression of smooth muscle myosin heavy chain. All ILTs showed the presence of nerve bundles with the L-R ILT having the lowest number of nerve bundles (p<0.05). These nerve bundles expressed the sympathetic marker, tyrosine hydroxylase with occasional parasympathetic expression of vasoactive intestinal polypeptide and acetylcholine transferase.
CONCLUSIONS: Historically the ILTs have been referred to as fibrous tissues however we show complex and regional patterning between the 3 ILTs and this may be important to the regulation of the structure-function relationship of the aortic root.
Presentation Number: RF6Publishing Title: Mastering The Ross Procedure: Global Practice Patterns And Insights From An International Survey
Author Block: Lucy Nam1, Dane Paneitz2, Michael Ibrahim3, Christopher Burke4, Maral Ouzounian5, Michael Chu6, Darryl Shore7, Ismail El-Hamamsy8, Jordan Bloom1.
1Massachusetts General Hospital, Boston, MA, USA, 2Johns Hopkins Hospital, Baltimore, MD, USA, 3University of Pennsylvania, Philadelphia, PA, USA, 4University of Washington, Seattle, WA, USA, 5University of Toronto, Toronto, ON, Canada, 6University of Western Ontario, London, ON, Canada, 7Royal Brampton Hospital, London, United Kingdom, 8Mount Sinai Hospital, New York, NY, USA.
Abstract Body:
OBJECTIVE: Recent data demonstrating superior outcomes and enhanced life expectancy with the Ross procedure (RP) have sparked renewed interest and increased utilization of the procedure. However, the RP remains technically challenging compared to conventional aortic valve replacement (AVR), necessitating specialized expertise and careful patient selection. This study aims to provide global insights into current RP practices, with a focus on patient selection, operative techniques, and postoperative care to establish best practices and inform future training programs.
METHODS: A web-based survey of over 60 questions was distributed globally to cardiac surgeons from May 1 to June 30, 2023, targeting those identified via social media and RP publications. The survey explored surgeon experience, RP volumes, patient selection criteria, preoperative imaging, intraoperative techniques, and postoperative care practices. Responses were analyzed to identify global trends and optimal approaches for RP care.
RESULTS: Of the 167 respondents, 123 (73.7%) performed the RP, with 75% performing 5-30 procedures annually. Approximately half involved a second attending surgeon. The majority treated younger patients (median age 60 years), and homografts were the preferred conduit for right ventricular outflow tract reconstruction. Variations existed in the techniques used to support ventriculoaortic and sinotubular junction (30% vs 45% always support), reflecting ongoing debate and clinical decision-making. Postoperative blood pressure control was common, with 90% prescribing beta-blockers and 54% using NSAIDs or steroids to reduce inflammation. Most surgeons (90%) re-image patients prior to discharge and 78% obtain annual transthoracic echocardiograms for follow-up.
CONCLUSIONS: This international survey provides valuable insights into current Ross procedure practices. The findings underscore the complexity of the RP and highlight the need for specialized training and collaboration. Establishing global best practices may help expand access to the RP, improve outcomes for patients requiring aortic valve replacement, and create more opportunities to standardize the procedure.
Presentation Number: RF7Publishing Title: Aortic Valve Repair And Replacement In Patients Affected By Infective Endocarditis: Short And Mid-term Results From The Heart Valve Society (HVS) Aortic Valve Database
Author Block: Jafar Hashims1, Wouter Oosterlinck1, Laurent de Kerchove2, Emmanuel Lansac3, Frederiek de Heer4, Bart Meuris1, Vincent Chauvette5, Carlotta Brega6, Claudia Romagnoni7, Jan Vojáček8, Igor Rudez9, Jesper Hjortnaes10, Francesco Patane11, Thierry Bourguignon12, Peter Verbrugghe1.
1University Hospital Leuven, Leuven, Belgium, 2Cliniques universitaires Saint-Luc, Brussels, Belgium, 3Institut Mutualiste Montsouris, Paris, France, 4Academic Medical Center Amstedam, Amsterdam, Netherlands, 5Montreal Heart Institue, Montreal, QC, Canada, 6Cotignola-Maria Cecilia Hospital GVM care & research, Cotignola, Italy, 7Azienda Socio Sanitaria Territoriale Fatebenefratelli Sacco, Università degli studi di Milano, Milan, Italy, 8Charles University Hospital, Prague, Czech Republic, 9University Hospital Dubrava, Zagreb, Croatia, 10Leiden University Medical Center, Leiden, Netherlands, 11Azienda Ospedaliera Papardo, Messina, Italy, 12CHRU de Tours - Hôpital Trousseau, Chambray-lès-Tours, France.
Abstract Body:
OBJECTIVE: To assess the short-and mid-term outcomes of Aortic Valve (AV) Repair vs. Replacement in patients with AV infective endocarditis (IE).
METHODS: This study utilized comprehensive international data from the Heart Valve Society (HVS) Aortic Valve Database. The analysis focused on evaluating the primary endpoint, defined as a composite of secondary outcomes, which included overall survival, freedom from reoperation, and freedom from severe aortic insufficiency (AI)
RESULTS: We conducted a retrospective analysis of 198 patients who underwent surgery for IE between 1998 and 2024. Patients were categorized into AVRepair (43.9%, n=87) and AVReplacement (56.1%, n=111) groups. Overall mean age was 55±14 years (AVRepair 52±15 years vs. AVReplacement 57±13 years; p=0.005). Valve morphology was not significantly associated with age(p=0.07). AVRepair group had a significantly lower mean euroscore (3.89±1.34 vs. AVReplacement 4.89±2.10; p=<0.0001). The cardiopulmonary bypass time (CPB) was significant between the groups (AVRepair 150.9±60.9 min vs. AVReplacement 116.1±54.7 min; p=0.001). The primary endpoint did not reach statistical significance (p=0.7). At the five-year follow-up, the overall survival rate was 91.9% (94.6% AVReplacement vs. 84.7% AV Repair; p=0.2), AVReplacement showed significant freedom from reoperation (98.2% vs. 83.9%; p=0.02), AVRepair was associated with an increased early postoperative bleeding (10%, n=9 vs. 2.7%, n=3; p=1.0) and a higher trend of severe AI (p=0.1). Patch reconstruction did not correlate with an increased risk of reoperation (p=0.6), no significant differences in outcomes between cases of healed and active IE was found (p=0.6)
CONCLUSIONS: In IE, while AVRepair preserves the native valve in select cases it is linked to higher early postoperative bleeding risks. AVReplacement tends to be favored in older, higher-risk patients, resulting in lower reoperation rates and less recurrent severe AI. Our findings support a tailored surgical strategy, optimizing patient selection and technique to improve outcomes. Further research is crucial to refine these approaches and enhance repair durability in IE
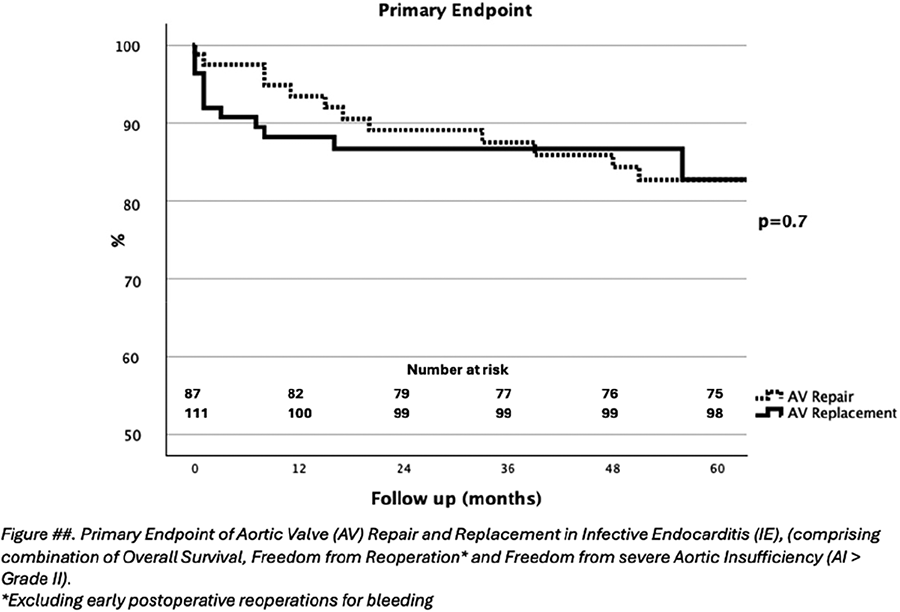
Presentation Number: RF8Publishing Title: The Role Of Right Ventricular- Pulmonary Arterial Coupling As A Predictor In Isolated And Combined Tricuspid Valve Surgery
Author Block: Jagdip Kang, MD, Svitlana Bielichenko, MD, Abdulaziz Dahou, MD, PhD, Jacob P. Dal-Bianco, MD, Nathaniel B. Langer, MD, David D'Alessandro, MD, Thoralf M. Sundt, MD, Evin Yucel, MD, Serguei Melnitchouk, MD, MPH.
Massachusetts General Hospital, Boston, MA, USA.
Abstract Body:
OBJECTIVE: This retrospective study evaluates the predictive value of right ventricular-pulmonary arterial (RV-PA) coupling in patients undergoing isolated or combined tricuspid and mitral valve surgery.
METHODS: All patients at our institution undergoing isolated tricuspid or combined tricuspid and mitral valve surgery between 01/2013 and 06/2024 with available preoperative transthoracic echocardiography images were included. RV-PA coupling ratio was calculated by dividing the tricuspid annular plane systolic excursion (TAPSE) by the PA systolic pressure. The optimal cut-off value for RV-PA coupling ratio was determined using the maximal log-rank test. A low RV-PA coupling ratio indicates poor RV contractile response to increased PA afterload. The primary outcome was all-cause mortality. Secondary outcomes were in-hospital mortality, duration of ICU-, hospital stay, and prolonged postoperative inotrope use.
RESULTS: 264 patients were included for a median follow-up of 23 months (IQR:7.0-48.0). The mean age was 67.4 ± 13.4 years and 54.5% were female. The median RV-PA coupling ratio was 0.390 mm/mmHg (IQR: 0.290-0.522) and the determined optimal cut-off value associated with mortality was 0.339. Patients with a RV-PA coupling ratio of ≤ 0.339mm/mmHg had significantly elevated all-cause mortality (25.5% vs 10.0%; p<0.002), mean length of ICU stay (8.4 days vs 4.3 days, p<0.001), mean length of hospital stay (16.5 days vs 10.9 days; p=0.002), prolonged need for inotropic support (45.7% vs 21.8%; p<0.001) and in-hospital mortality (10.6% vs 2.9%). In multivariable Cox regression analysis, a RV-PA coupling ratio >0.339 mm/mmHg was associated with a decreased risk of all-cause mortality (HR:0.28; 95% CI:0.12-0.64; p=0.003). TAPSE and RV free-wall strain had no association with mortality.
CONCLUSIONS: RV-PA coupling ratio is an independent predictor of all-cause mortality in patients undergoing cardiac surgery for combined or isolated tricuspid valve disease. Our data support using this ratio in preoperative surgical risk assessment and potentially in patient selection.
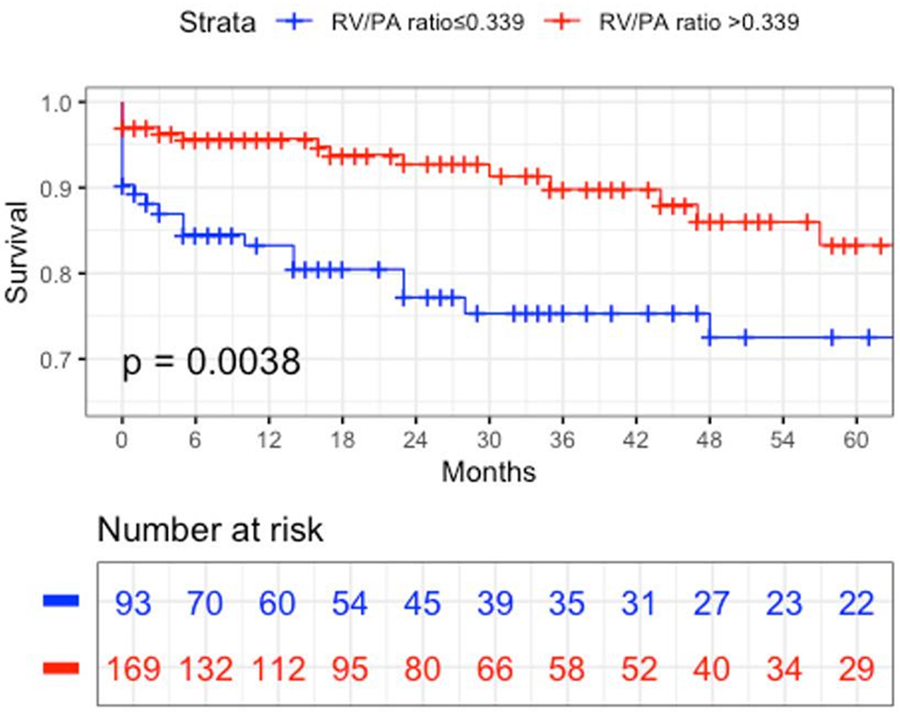
Presentation Number: RF9Publishing Title: Isolated Tricuspid Surgery: 25 Years’ Experience Of A Single Center
Author Block: Karim Tarek Ahmed1, Mohamed Mohamed El-Fiky2.
1Nasser instuite hospital, Cairo, Egypt, 2Ain shams university, Cairo, Egypt.
Abstract Body:
OBJECTIVE: In this study, we looked at our database from 1999 till the end of 2023 and reviewed all cases that performed isolated tricuspid valve surgery and explored their etiology, demographic criteria, in-hospital mortality risk predictors and incidence of complications and mortality.
METHODS: There were 305 cases that underwent isolated tricuspid valve surgery in our database, and this represented 1.9% of our total valve surgery load in this period. Their mean age was 40 ± 13.2 years, evenly split between males and females. The main pathologies were either functional (94 cases; 31%) or rheumatic (86 cases; 28%). Other pathologies include endocarditis, congenital, prosthetic valve failure, failed prior repair and ischemic etiology. There were 114 (37.4%) who had at least one open heart surgery beforehand. Right heart failure was present at the time of surgery in 38(12.5%) patients. All pre-operative criteria were analyzed then entered in a binomial logistic regression equation to identify the mortality predictors.
RESULTS: The in-hospital mortality in this group of patients was 13.1%. There were 5 criteria that predicted in-hospital mortality: older age, presence of diabetes mellitus, redo surgery, presence of right heart failure at time of surgery and history of previous balloon mitral valvuloplasty. Applying binomial logistic regression, the only predictors of in-hospital mortality are the older age of the patient and the presence of right sided heart failure. As for the etiology of the disease, patients with failed prior repair and patient with ischemic etiology did significantly worse than the rest of the population, whereas patients with endocarditis on the tricuspid valve did significantly better than the rest of the population.
CONCLUSIONS: This procedure carries a high risk of in-hospital mortality in our institution. The proper treatment of right heart failure or even the intervention before the issuance of overt right sided heart failure might improve the outcome.
Presentation Number: RF10Publishing Title: Genesis Of The Unseen: The Dawn Of An Unprecedented Surgical Tricuspid Valve
Author Block: Ki Han Kim, Irwan Shah Bin Mohd Moideen, Abdulrahman El Gohary, John C Stevens, Theo Kofidis, Faizus Sazzad.
National University of Singapore, Singapore, Singapore.
Abstract Body:
OBJECTIVE: At present, there is no commercially available surgical tricuspid valve prosthesis, leaving no choice for the surgeons but to employ mitral valve prostheses as an alternative. We developed and evaluated a dedicated surgical tricuspid valve prosthesis designed to closely replicate the natural anatomy and function of the native tricuspid valve.
METHODS: The novel tricuspid valve prosthesis features three flexible bovine pericardium leaflets, an adaptable asymmetric ring, and cords that mimic those of the natural valve. was validated through in-vitro testing in compliance with ISO 5840 standards. We performed in-vitro pulse duplicator tests to assess hydrodynamic performance and ex-vivo evaluations in porcine hearts to verify anatomical conformance. Following the design verification of the prototype, proof of concept validation was conducted via an acute porcine study (n=5), evaluating the implantation feasibility, safety, and efficacy. Additionally, a limited series of cadaver experiments were conducted to assess human implantation feasibility.
RESULTS: The new prosthesis demonstrated superior anatomical conformity and functional performance in preclinical tests. In-vitro pulse duplicator testing of early prototypes (n=2) showed respectable hydrodynamic performance, with an average effective orifice area (EOA) of 2.8 cm², an average mean pressure gradient of 1.9 mmHg, and an average regurgitation fraction of 11.0%. Ex-vivo beating heart testing on a porcine heart visually confirmed the results of chord implantation and leaflet function in the tricuspid position. An acute in-vivo porcine study (n=4) proved the concept's feasibility, confirming good anatomical conformance to native porcine hearts. Additionally, an acute in-vivo ovine study further validated proper valve functioning and acceptable tricuspid regurgitation, as confirmed by post-operative CT angiography and echocardiography.
CONCLUSIONS: This innovative surgical tricuspid valve prosthesis could greatly enhance patient outcomes. It addresses current technology limitations and requires first-in-human studies to confirm preclinical results and evaluate long-term benefits.
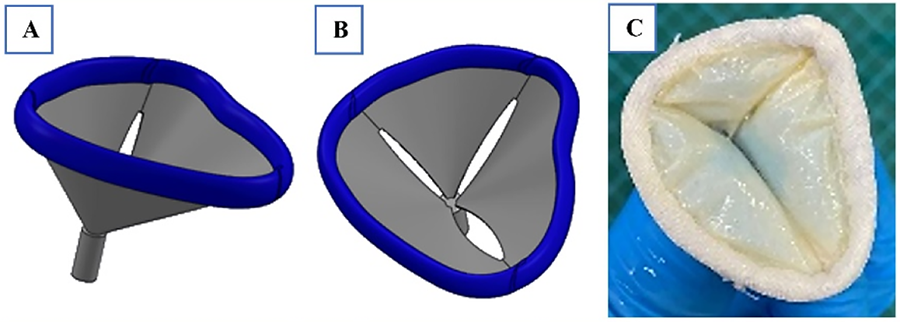
Presentation Number: RF12Publishing Title: Age- And Sex-specific Excess Mortality In Patients Undergoing Isolated Aortic Valve Repair And Valve Sparing Root Replacement
Author Block: Reda Rhellab1, Jolanda Kluin1, Laurent De Kerchove2, Gloria Färber3, Emmanuel Lansac4, Vincent Chauvette5, Peter Verbrugghe6, Claudia Romagnoni7, Jan Vojáček8, Jonathan R.G. Etnel1, Johanna J.M. Takkenberg1, Kevin M. Veen1.
1Erasmus MC, Rotterdam, Netherlands, 2Cliniques Universitaires Saint-Luc, Brussels, Belgium, 3Saarland University Medical Center, Homburg/Saar, Germany, 4Pitié-Salpêtrière APHP Hospital, Paris, France, 5Université de Montréal, Montréal, QC, Canada, 6University Hospitals Leuven (UZ Leuven), Leuven, Belgium, 7IRCCS Cà Granda Ospedale Maggiore Policlinico di Milano, Milan, Italy, 8University Hospital in Hradec Kralove, Hradec Kralove, Czech Republic.
Abstract Body:
OBJECTIVE: Excess mortality after valve surgery is the additional mortality not due to valve-related events, and an important parameter to quantify disease burden compared to the general population. This study aims to quantify age- and sex-specific excess mortality in patients undergoing isolated aortic valve repair (IAVr) and valve sparing root replacement (VSRR).
METHODS: IAVr and VSRR patients’ data were extracted from the HVS AV-database. Patients with Type-A dissection, rheumatic etiology and endocarditis were excluded. Royston-Parmar models were fitted to estimate age- and sex-specific 20-year survival. Age- and sex-specific early and late valve-related event risks and linearized occurrence rates were calculated which served as input parameters for a novel microsimulation model. Excess mortality up to 20 years after surgery was defined as the hazard ratio (HR) that calibrated the microsimulation survival-estimates to the Royston-Parmar survival-estimates, with random sampling of valve-event rates from their respective 95% confidence intervals in each run.
RESULTS: The IAVr-group group included 1770 (age:47.4y±16.1, 85% male) patients and VSSR-group included 3504 (age:51.5y±14.2, 85% male) patients. Within both subgroups younger patients had higher 20-year HRs of excess mortality compared to older patients (Figure-1A). The HRs of excess mortality were higher for males compared to females in both subgroups. For a typical patient in both groups, patient estimated survival is comparable to the matched-general-population until approximately 10 years postoperatively, after which they start to diverge (Figure-1B).
CONCLUSIONS: Especially younger male patients have high relative excess mortality not due to valve-related events compared to the general population, potentially explained by low general population mortality rates at younger ages. This translated to an absolute mortality difference that only becomes considerable from 10 years postoperatively. These findings can be used as input for future outcome-projection models to guide optimal lifetime treatment-strategies in AV disease.
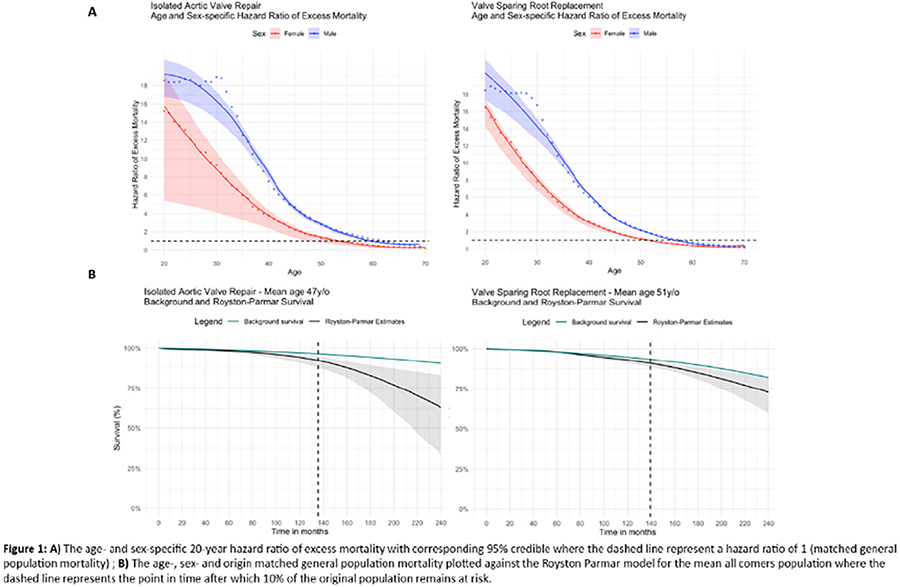
Presentation Number: RF13Publishing Title: Early Temporal Changes In Autograft Insufficiency With Progressive Autograft Deployment After The Ross Procedure
Author Block: Nader S. Aboelnazar, MSc, MD, Satoru Fujii, PhD, FRCPC, Brandon R. Loshusan, MFE, MD, Lin-Rui Guo, MD, FRCSC, Michael W. A. Chu, MEd, FRCSC.
London Health Science Centre, London, ON, Canada.
Abstract Body:
OBJECTIVE: Echocardiography provides invaluable assessment and guidance for pulmonary autograft function after the Ross procedure. Early after implantation, the pulmonary autograft takes a little time to fully expand, particularly when constrained within native aortic root tissue. We describe our experience with early changes in autograft geometry and temporal changes in early aortic insufficiency (AI), which often looks the worst immediately after aortic cross-clamp removal.
METHODS: We included 184 patients who underwent the Ross procedure between 2012 and 2024 and had complete imaging. The operations were performed by two cardiac surgeons. All patients had intraoperative transesophageal echocardiography (TEE), transthoracic echocardiography (TTE) at pre-discharge and at 3-6 months follow-up. The intraoperative TEE were interpreted by cardiac anesthesiologists. The degree of AI was graded from none/trace to severe. One-way ANOVA was utilized, and Bonferroni and Tukey’s post-hoc test conducted (p<0.05).
RESULTS: Overall, there were no 30-day or late mortalities. In-hospital complications were infrequent with stroke in n=2 (1%), respiratory failure in n=3 (1.6%) and renal failure in n=3 (1.6%) patients. N=26 (14%) had >mild AI post-CPB, while n=163 (88%) had ≤mild AI. In >mild AI, 100% of patients had improved AI severity on their follow-up TTE (p<0.001). In ≤mild AI, n=24 (15%) had improved AI, n=22 (13%) had worse AI, and n=112 (69%) had unchanged AI severities (p<0.001). Figure 1 depicts the changes in early AI in the entire cohort. N=4 (2%) patients underwent further adjunctive repair measures to address early residual aortic insufficiency.
CONCLUSIONS: Our findings suggest that early residual AI immediately after removal of the aortic cross-clamp after the Ross procedure is common and in most cases, resolves with time. We propose specific AI patterns that may be more benign and which may require additional surgical exploration and/or adjunctive repair procedures.
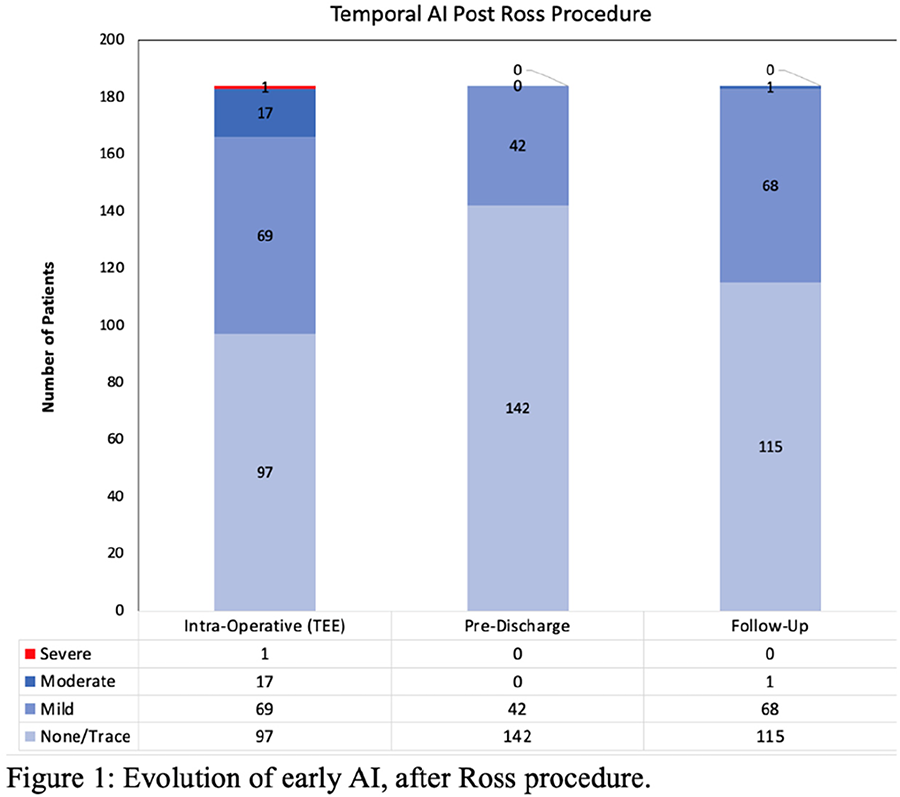
Presentation Number: RF14Publishing Title: An In-silico Study To Assess How Length, Number, And Anchoring Points Of Engineered Chordae Tendineae Affect Mitral Valve Function
Author Block: Elisa Lanzalaco1, Joan Dario Laubrie2, Federica Cosentino2, Giuseppe Raffa3, Michele Pilato3, Vincenzo La Carrubba4, Antonio Pantano4, Antonio D'Amore2.
1University of Palermo and Ri.MED Foundation, Palermo, Italy, 2Ri.MED Foundation, Palermo, Italy, 3ISMETT, Palermo, Italy, 4University of Palermo, Palermo, Italy.
Abstract Body:
OBJECTIVE: Mitral valve regurgitation (MVR) is the most common mitral valve (MV) disease. MVR is classified as primary or secondary and arises from structural damage of the MV leaflets (primary) or of the sub-valvular apparatus (SA). The SA establishes a mechanical continuum between MV and left ventricle (LV), supporting MV leaflets during ventricular contraction, preventing prolapse and harmonizing LV performance. This study develops a simplified methodology to engineer the chordal apparatus (CA), focusing on the number, optimal length, and anchoring points for chordae tendineae (CT) trying to, assist bioinspired design of MV prostheses.
METHODS: The numerical models was developed with Abaqus-explicit method. MV and CT were modeled with shell (S4) and truss (T3D2) elements, respectively. For the constitutive model, the Fan-Sacks structural anisotropic model and the Ogden model were utilized. The annulus is encastred and PM are pinned in time averaged position during cardiac cycle. Leaflets were loaded with normo-physiological atrial and ventricular pressure. Numerical models of MV and SA were considered by varying the three variables: - CT number:(2, 4, 6, 8), - CT length:(80%, 100%, 120% of physiological length), - CT anchoring (along the free edge or 4 mm above)
RESULTS: Numerical simulations indicate that Von Mises stress remains under 500-kPa across all the configurations.The 80% CT length showed higher tension due to increased pre-stretch, while keeping the clinical bulging limits (< 3mm) and maintaining a Geometric Orifice Area above 1 cm².
CONCLUSIONS: Numerical results identified the best functional configuration as the one with 8 CT, with a length of 80% of the physiological one and anchoring points distributed along the free marginal edge, 4 CT for each of the anterior and posterior leaflets were considered. Metrics utilized to comparatively compare the different configurations included: leaflet bulging, von Mises stress distribution, coaptation length and orifice area.
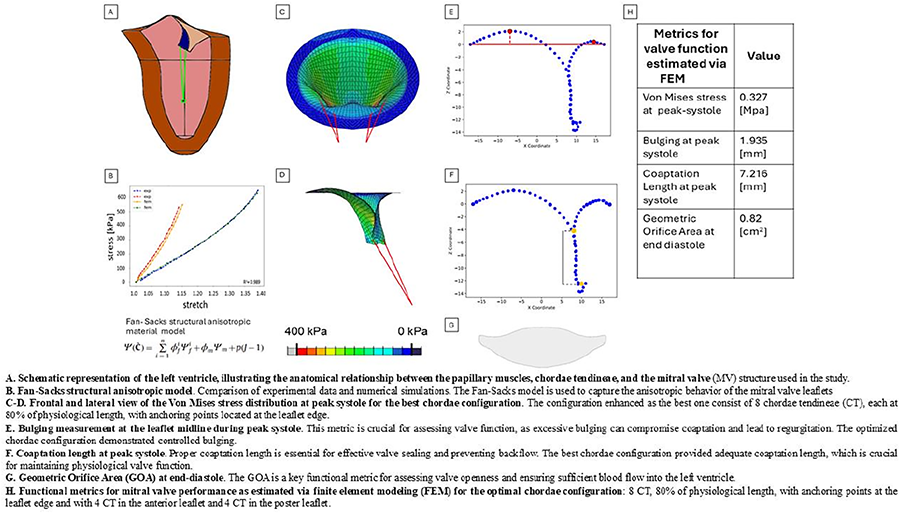
Presentation Number: RF15Publishing Title: Novel Parameter To Assess Right Ventricular Dysfunction And Outcomes In Asymptomatic Primary Mitral Regurgitation
Author Block: Mireille Bherer, M.Sc.1, Jérémy Bernard, M.Sc.1, Sophia Haloui1, Oumhani Toubal, MD1, Haïfa Mahjoub, MD, PhD1, Nancy Côté, PhD1, Mathieu Bernier, MD1, Jonathan Beaudoin, MD1, Kim O’Connor, MD1, Florent Leven, PhD2, Sébastien Hecht, M.Sc.1, Erwan Salaun, MD, PhD1, Philippe Pibarot, DMV, PhD1.
1Institut universitaire de cardiologie et de pneumologie de Québec, QUEBEC, QC, Canada, 2Department of Cardiology, Hôpital La Cavale Blanche–Centre Hospitalier Regional Universitaire, Brest, France.
Abstract Body:
OBJECTIVE: Recent studies demonstrated the incremental prognostic value of echocardiographic parameters of right ventricular (RV) function in the risk stratification of patients with primary mitral regurgitation (PMR). We hypothesized that the coupling of pulmonary arterial systolic pressure (PASP) to RV end-diastolic area (RVEDA) is a good surrogate of RV wall stress and is thus associated with clinical outcomes in PMR patients.
METHODS: The PASP/RVEDA ratio was measured in 209 patients (mean age: 60 ± 14 years; 52% men, 62% ≥ moderate PMR) enrolled between 2008 and 2022 in the multicentric and prospective PROGRAM study (NCT01835054). Receiver operating characteristics curve was used to determine the optimal prognostic threshold of PASP/RVEDA associated with all-cause mortality.
RESULTS: The feasibility of the PASP/RVEDA measurement was 96%, intra-observer reproducibility: ICC [95%CI]: 0.94 [0.71- 0.98], p ≤ 0.001, and inter-observer reproducibility: ICC [95%CI]: 0.85 [0.57 - 0.93], p ≤ 0.001. The optimal prognostic threshold of PASP/RVEDA was 1.5 mmHg/cm2. In univariate Cox regression analyses, continuous as well as dichotomic PASP/RVEDA were associated with higher risk of mortality (HR [95%CI]: 2.53 [1.31 - 4.91] per 1 mmHg/cm2 increment, p = 0.006 and HR [95%CI]: 8.49 [1.13 - 63.92], p = 0.04, respectively). In multivariate analysis adjusted for the Charlson score, there was a trend toward higher risk of mortality (HR [95%CI]: 5.51 [0.70 - 40.60], p = 0.11).
CONCLUSIONS: This study suggests that the PASP/RVEDA ratio provides a novel surrogate marker of RV wall stress and systolic dysfunction and may be useful to predict clinical outcomes and enhance risk stratification in patients with PMR.
Presentation Number: RF17Publishing Title: Mineralocorticoid Receptor Antagonism Prevents Calcification In Female Valve Interstitial Cells víA Mirna-19b/Nr2c3 And Tgfbeta Signaling
Author Block: Mattie Garaikoetxea1, Beatriz Delgado-Valero2, Ernesto Martin-Nuñez1, Miriam Goñi-Oloriz1, Susana San Ildefonso1, Paula Castillo1, Natalia Lopez-Andres1, Eva Jover1.
1Navarrabiomed, Pamplona, Spain, 2Universidad Complutense de Madrid, Madrid, Spain.
Abstract Body:
OBJECTIVE: Mineralocorticoid receptor (MR/NR2C3) is instrumental to sex-dependent AS. MicroRNAs are small, single-stranded non-coding RNAs that regulate multiple mRNA targets by complementary hybridation. Serum and myocardial miR-19b are downregulated in AS. We aimed to study the role of miR-19b within the stenotic aortic valve (AV).
METHODS: In silico tools predicted miR19-targets, lately confirmed by luciferase assays. Human valve interstitial cells (VICs, n=6/sex/experiment) were challenged with pro-calcific media (2.6mM Pi) relevant to model advanced calcific AS. AgomiR experiments were conducted in vitro and ex vivo in explanted AVs. In vitro drug repurposing of Spironolactone (MR/NR2C3 inhibitor) was tested. Validations were conducted in human AVs. QPCR, ELISA, western blotting, in situ hybridation and immunocyto/histochemistry were used.
RESULTS: In silico KEGG functional annotation revealed that miR-19b potentially regulates ‘TGF-beta signaling pathway’ (ACVR1, SMAD4, BMPR2, TGFBR2) and ‘Aldosterone-regulated sodium reabsorption’ (NR3C2). In vitro, baseline expression of miR-19b was higher, whilst miR19b-targets were lower, in female-VICs. Pi-challenge down-regulated miR19b only in female VICs, in parallel with NR3C2 up-regulation. TGF-beta targets were up-regulated in both sexes. Rescue experiments using agomiR-19b in calcifying female-VICs diminished calcification, miR19b targets and relevant inflammatory and osteogenic cues. AgomiR19b also prevented ex vivo calcification. Noteworthy, MR/NR2C3 antagonism (MRA) exerted likewise protective effects including miR19b up-regulation. Validation studies revealed a lower expression of miR-19b and higher NR3C2 in human stenotic AVs (n=198, 63.13% men) compared with controls (n=36, 69.44% men). Consistent with a prevalent calcific phenotype in AS men, valvular expression of miR-19b was lower than in women. Moreover, 68 AVs (61.9% men) were dissected into healthy, fibrotic, and calcific areas demonstrating a progressive miR-19b downregulation towards calcific areas only in women (p=0.0475).
CONCLUSIONS: Alternative to miRNA-based therapeutics, MRA prevents calcification in women-VICs via miRNA-19b/NR2C3 and TGFβ signaling. New mechanisms and MRAs repurposing potential are proposed for the ‘so-often-overlooked’ AS women.
Presentation Number: RF18Publishing Title: Shear Versus Contact Induced Platelet Activation In Mechanical Heart Valves: Which One Is Dominant?
Author Block: Syed Samar Abbas, Iman Borazjani.
Texas A&M University, College Station, TX, USA.
Abstract Body:
OBJECTIVE: The state-of-the-art research investigating the clotting potential of Mechanical Heart Valves (MHVs) and Transcatheter Heart Valves has been limited to the quantification of shear-induced Platelet Activation (PA), fully ignoring the contact-induced PA and thereby the intrinsic pathway of coagulation. Our objective is to develop a comprehensive numerical model to predict clot initiation in prosthetic heart valves by incorporating the shear-induced and contact-induced PA, thereby characterizing the dominant mechanism of PA in heart valves which is the prerequisite to improve their designs.
METHODS: We develop a parallel solver of several convection-diffusion-reaction equations, each modeling the transport of species involved in the coagulation cascade. These species include mobile and bound activated platelets, zymogens and enzymes that participate in the intrinsic pathway of coagulation. The contribution from both, the dynamic shear stresses and artificial surface contact (through activation of FXII) is accounted for in governing equations for the transport of platelets. The main product of the coagulation cascade is the thrombin (FIIa), which stabilizes to form a clot and activates further platelets.
RESULTS: The developed coagulation model is validated against benchmark experiments. To apply the model to MHVs, first we perform the numerical Fluid-Structure Interaction (FSI) simulations of two designs of MHVs, namely a Trileaflet MHV (TMHV) and Bileaflet MHV (BMHV). The flow field of the two MHVs is incorporated as an input to coagulation model to identify the dominant mechanisms (shear- or contact-induced) of coagulation in MHVs.
CONCLUSIONS: The developed coagulation model can identify and model both shear- and contact-induced coagulation mechanisms which have yet to be considered together in MHV studies.
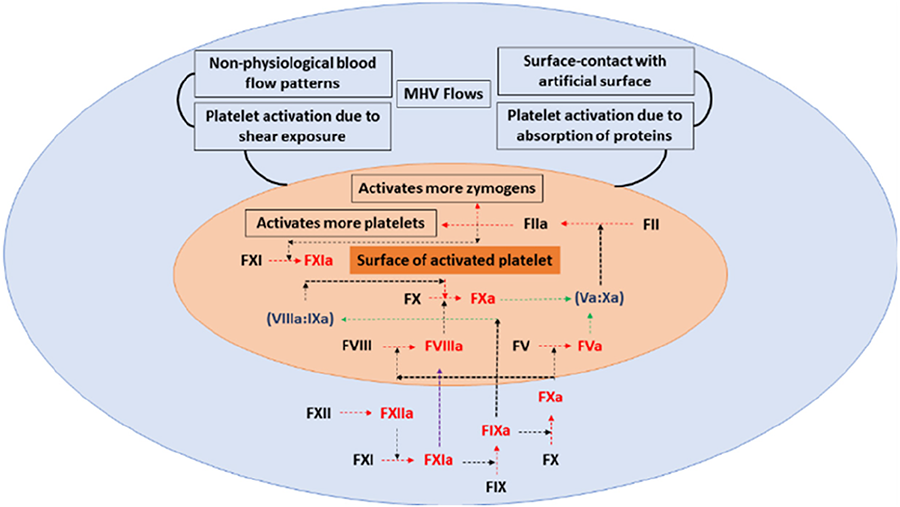
Presentation Number: RF19Publishing Title: Von Willebrand Factor Large Multimer Index In Patients With Aortic Stenosis: Dynamics And Correlation With Valvular Disease
Author Block: Shuji Tachioka1, Hideaki Kanda1, Sadayuki Higashi1, Munekazu Yamakuchi1, Misako Suzuki2, Drew N. Maywar3, Kenji Toyokawa1, Kosuke Mukaihara1, Kazuhisa Matsumoto1, Hisanori Horiuchi2, Teruto Hashiguchi1, Yoshiharu Soga1.
1Kagoshima university, Kagoshima city, Japan, 2Tohoku University, Sendai city, Japan, 3Rochester Institute of Technology, Rochester, NY, USA.
Abstract Body:
OBJECTIVE: The von Willebrand factor (VWF) large multimer index (LMI) from the preoperative period to early remote follow-up in patients with aortic stenosis (AS) remains unclear. Furthermore, the decrease in LMI might be better reflected if valvular diseases other than AS were considered in an integrated manner. However, this correlation remains to be investigated.
METHODS: We studied 23 patients with AS who underwent aortic valve replacement. A quantitative time-course assessment of the VWF, including LMI, was performed. Our proposed total valve score was used to study the correlation between LMI and valvular diseases, including diseases other than AS.
RESULTS: VWF LMI was significantly higher in the immediate postoperative period than in the preoperative period. This increase was maintained over a time course of nine measurements up to and including the one-year follow-up. The trend was stronger when considering only the group with a preoperative VWF LMI < 80%. The preoperative VWF LMI showed a weak negative correlation with the PFV (Spearman correlation coefficient rs = -0.2853, p = 0.187) and a weak negative correlation with the mean aortic pressure gradient (Spearman correlation coefficient rs = −0.3617, p = 0.091). The total valve score showed a moderate negative correlation with VWF LMI (rs = -0.5483, p = 0.0068). It showed a stronger negative correlation and lower p-value than the peak flow velocity and mean pressure gradient.
CONCLUSIONS: We are the first to show that improved VWF LMI is maintained 1 year after AS surgery, and correlates better with severity on echo when other valvular diseases are integrated rather than with AS severity alone. VWF LMI may be a useful indicator of acquired von Willebrand syndrome severity related to overall heart shear stress and treatment effectiveness up to the early remote stages.
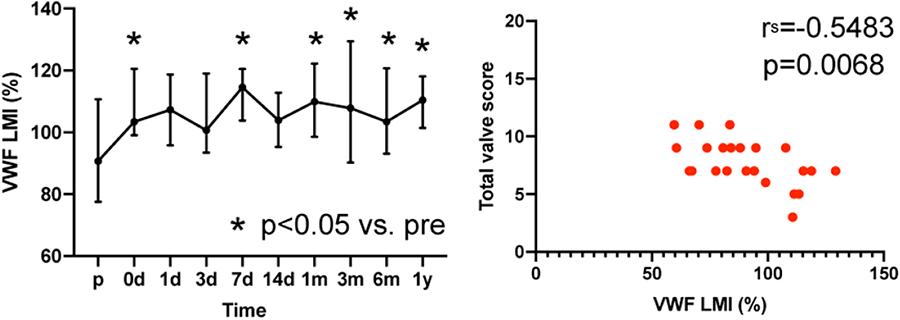
Presentation Number: i1Publishing Title: Structure-function Characterization Of Fresh Human Heart Valves
Author Block: Patrizia Caruso1, Marzio Di Giuseppe2, Laura Modica De Mohac2, Federica Cosentino2, Arianna Adamo3, Viktor Balashov2, Marianna Barbuto2, Drake Pedersen4, Bernardo Zuccarello5, Michele Pilato6, Giuseppe Raffa7, Garrett Coyan8, William R. Wagner9, Antonio D'Amore10.
1University of Palermo and Ri.MED Foundation, Palermo, Italy, 2Ri.MED Foundation, Palermo, Italy, 3Ri.MED Foundation and Columbia University Irving Medical Center, Department of Surgercial Science, New York, Palermo, Italy, 4McGowan Institute for Regenerative Medicine and Department of Bionengineering and Surgery - University of Pittsburgh, PITTSBURGH, PA, USA, 5University of Palermo, Palermo, Italy, 6Department for the Treatment and Study of Cardiothoracic Diseases and Cadiothoracic Transplantation, IRCCS-ISMETT, Palermo, Italy, 7Department for the Treatment and Study of Cardiothoracic Diseases and Cardiothoracic Transplantation, IRCCS-ISMETT, Palermo, Italy, 8Department of Cardiac Surgery - Vanderbilt University Medical Center, Nashville, TN, USA, 9Department of Bioengineering & Surgery - University of Pittsburgh, Pittsburgh, PA, USA, 10Ri.MED Foundation and McGowan Institute for Regenerative Medicine, University of Pittsburgh and Department of Bioengineering & Surgery - University of Pittsburgh, Palermo, Italy.
Abstract Body:
OBJECTIVE: The four human heart valves (HVs) exhibit differences in their physiology which are reflected in their structural and mechanical properties. HVs physiological properties still remain poorly characterized and are largely neglected in the design of commercially available prosthetic devices, with data being extracted only from animal or cadaveric tissues. This study aims to fully characterize human HVs structure and mechanics at the organ and tissue scale.
METHODS: Human valve samples from heart transplant patients were tested within 24 hours from the explant procedure. Thickness was measured across the whole leaflet area for the aortic, mitral, pulmonary, and tricuspid valves (AV, MV, PV, TV). Leaflet cellular and structural constituents were characterized using histological staining a decellularization protocol allowed for fiber network analysis via electron microscopy. Collagen fiber angle distribution and bundle diameter were quantified with digital image processing. Biaxial mechanics was measured on belly region samples utilizing a Lagrangian equi-stress control protocol with 400kPa peak stress.
RESULTS: Results showed that HVs collagen quantity and thickness correlates with transvalvular pressure, with increased thickness values measured at coaptation and free edge regions. The MV exhibited a higher average thickness. MV and TV showed greater stiffness than the semilunar valves (AV, PV), along the radial direction.
CONCLUSIONS: This study highlights structural and functional differences in fresh human HVs. Establishing a detailed HV structural-function database remains critical to assist valve engineering, and implement biomimicry in leaflet, supra and sub-valvular apparatus design.
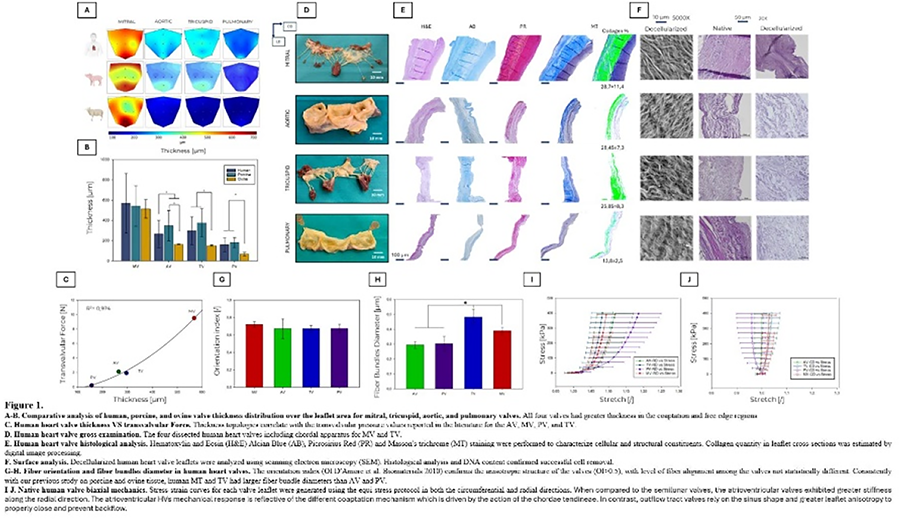
Presentation Number: i2Publishing Title: Cross-species Proteomics Applied To Explanted Cardiovascular Biomaterials Enables Distinction Of Donor Versus Host Extracellular Matrix Profiling In Bioprosthetic Implants
Author Block: Rachel Cahalane1, Bart Meuris2, Marie Billaud1, Joan Matamalas1, Taku Kasai1, Amber Hendrickx2, Jochen D. Muehlschlegel3, Filip Rega2, Masanori Aikawa1, Laoise McNamara4, Sasha A. Singh1, Elena Aikawa1, Cassandra L. Clift1.
1Harvard Medical School, Brigham and Women's Hospital, Boston, MA, USA, 2KU Leuven, Leuven, Belgium, 3Johns Hopkins University School of Medicine, Baltimore, MD, USA, 4University of Galway, Galway, Ireland.
Abstract Body:
OBJECTIVE: Xenogenic tissues are widely used in clinical practice, however immune-mediated rejection is an ongoing clinical challenge. Proteomics can assess molecular mechanisms contributing to xenogenic tissue implant failure. However, in traditional bottom-up approaches, shared peptide amino acid (AA) sequences across donor versus host species renders protein-level specificity a challenge.
METHODS: Three tissue cohorts were used: Xenogenic tissue explants (bovine pericardium-derived bioprosthetic valves [BPV], human host; n=47), bovine control (un-implanted BPV, n=7) and human control (native aortic valves; n=10). Tryptic peptides (PreOmics iST) were injected via Easy-nLC1200 HPLC on an Exploris 480 (Thermo Fischer Scientific) via data dependent acquisition. Data was searched against Homo sapiens and a Bos Taurus background FASTA (MaxQuant v.2.4.14.0). MSqRob, an analytical pipeline tool that combines intensity- and spectral count-based quantification, was used to species-delineate low-abundant bovine and human peptides (MSqRob, v0.7.7). Spectral libraries were generated using DIA-NN (v1.9.1).
RESULTS: Tryptic in silico digestion was performed on BPV proteins with high degree of shared AA sequence percent identity between species (400 proteins; IQR 75.82-94.96% identity). A total of 7175 of spectral library peptides overlapped across species (31% human [22901], and 26% bovine [27382]). Peptides <12 AAs in length accounted for 52.26% of the shared spectral library, correlating to searched peptide confidence scores, suggesting the need to adjust database parameters for cross-species datasets. The BPV dataset identified 1815 proteins: 24 orthologs (both species quantified confidently), and 88 ‘cannot differentiate’ across species. Species-delineated peptide-centric analysis implicated several extracellular matrix proteins with bovine-specific degradation and human-specific neo-tissue deposition profiles in failed BPV tissues. Network integration of unimplanted and explanted BPV data recategorized proteins from ‘cannot differentiate’ to human-specific, bovine-specific, or orthologous, increasing proteins worthy of downstream mechanistic analysis of BPV failure.
CONCLUSIONS: This is the first study to implement cross-species proteomics analysis in cardiovascular xenogenic tissue-based biomaterial implantation.
Presentation Number: i3Publishing Title: Regeneration And Calcification Of A Transcatheter Tissue Engineered Pulmonary Valve After 18-month Implant In Juvenile Sheep
Author Block: Abrielle Prunty1, Mariah McMahon1, Jacob Benkofske1, James Berry2, Rika Kawakami3, Richard Murphy1, Renu Virmani3, Gurumurthy Hiremath2, Jeffrey Lawson1, Zeeshan Syedain1.
1Vascudyne Inc., Saint Paul, MN, USA, 2University of Minnesota, Minneapolis, MN, USA, 3CVPath Institute Inc., Gaithersburg, MD, USA.
Abstract Body:
OBJECTIVE: Current bioprosthetic valves for congenital pulmonary valve disease degrade and calcify over time requiring young patients to undergo multiple replacements over their lifetimes. An engineered acellular allogenic tissue with minimal immunogenicity and regenerative potential could provide an alternative solution.
METHODS: The engineered tissue was manufactured by creating 3D scaffold of fibrin hydrogel and human fibroblasts then cultured in bioreactors to create robust tissue structures. The tissue was decellularized, and aseptically stitched to create nitinol framed valves. The transcatheter pulmonary valve was evaluated in a highly calcific juvenile sheep model (n=5). Explants were imaged using Faxitron, and sections were fixed for histology at 6 (n=2), 12 (n=1), and 18 months (n=2). Samples were imaged with MicroCT, then processed for wax embedding, sectioning, and staining.
RESULTS: Each valve was imaged using Faxitron (Fig a-f) showing no major calcification. Calcium was measured through mass spectrometry quantification. Preimplant tissue had a value of 0.181μg/mg dry weight. 18-month explants had average values of 0.141 and 0.158μg/mg dry weight indicating no significant increase in calcium content (Figure g). After 18 months, evidence of regeneration through endothelial coverage was observed in significant portions of the conduit with lack of endothelialization visualized only in localized inflammation or thrombus-attached areas (Fig h-j). Analysis showed interstitial cell migration from root into leaflets and full cellularization by interstitial cells in tissue within the frame (Fig k-n). There was evidence of elastin deposition near leaflet roots which potentially indicates healthy regeneration rather than fibrotic tissue formation, as seen with fixed pericardium leaflets.
CONCLUSIONS: Tissue engineered pulmonary valve derived from human cells has allowed for endothelization and reduced immunological response leading to deterioration and calcification. These results suggest the material has potential to regenerate and provide longer-term solutions for younger patients.
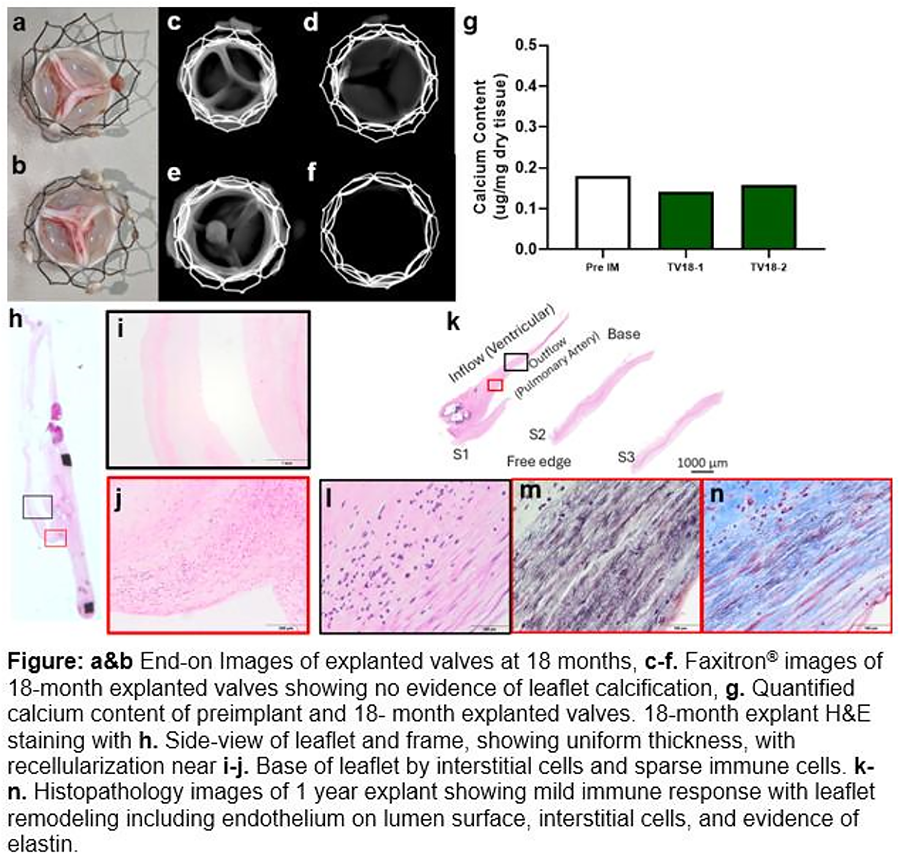
Presentation Number: i4Publishing Title: Potential Application Of A Novel Autologous Tissue-engineered Heart Valve For Various Valvular Diseases
Author Block: Yoshiaki Takewa, Yusuke Inoue, Takeshi Terazawa, Yasushi Sato.
Asahikawa Medical University, Asahikawa, Hokkaido, Japan.
Abstract Body:
OBJECTIVE: We have been developing a novel autologous biological heart valve (biovalve) using a unique technique, called in-body tissue engineering, in which tissue is formed by applying the encapsulation reaction of connective tissue. In this study, we evaluated the performance and tissue structure by implantation experiments using large animals (adult goats), and examined whether the biovalve could be an option for various valve diseases.
METHODS: The biovalve molds were made of acrylic and metal, implanted subcutaneously in the back of an adult goat, and the molds were removed around 8 weeks after implantation to obtain the biovalve. The biovalve was surgically implanted into the aorta and pulmonary arteries of adult goats and its performance was evaluated.
RESULTS: The biovalves could be implanted in the aortic or pulmonary valve positions by conventional open-heart surgery or transcatheter valve implantation, respectively. Postoperative angiographic and blood pressure waveform monitoring showed good mobility of the valve leaflets and no significant stenosis or regurgitation. The biovalves remained well beyond the maximum observation period of 3 years. At the end of the experiment, the biovalves showed good preservation of valve leaflet structure with little thrombus formation or calcification. Histologically, cellular invasion was observed in the connective tissue of the removed biovalves after 4 weeks, and neovascularization was also observed. A layer of vascular endothelium-like cells was also seen on the blood contact surface. In addition, these tissues were found to change into a structure resembling normal valvular tissue at the level of several weeks after implantation.
CONCLUSIONS: The biovalve is expected to be a promising alternative valve for various valve diseases because of its good histocompatibility in regenerative medicine, ease of application in artificial organs, and the advantage of being able to fabricate planned shapes.
Presentation Number: i5Publishing Title: 18 Months In Vivo Hemodynamic Performance Of A Transcatheter Tissue Engineered Pulmonary Valve Implant In Juvenile Sheep Model
Author Block: Zeeshan Syedain1, Mariah McMahon2, Abrielle Prunty2, Jacob Benkofske2, James Berry1, Rika Kawakami3, Renu Virmani3, Rick Murphy2, Gurumurthy Hiremath1, Jeffrey Lawson2.
1University of Minnesota, Minneapolis, MN, USA, 2Vascudyne Inc., St Paul, MN, USA, 3CV Path Institute, Gaithersburg, MD, USA.
Abstract Body:
OBJECTIVE: Congenital valve disease, predominantly in the pulmonary position, requires multiple replacements as current bioprosthetic valves degrade and calcify over time. An tissue engineered heart valve with minimum immune and calcification response would provide an ideal solution for young patients.
METHODS: A transcatheter pulmonary valve (TPV) with bioengineered tissue leaflets on a self-expanding nitinol stent was implanted for up to 18- months in five juvenile sheep using a 18Fr transapical delivery system. Serial echocardiogram monitoring was performed with explant tissue evaluated for mechanical properties, quantitative calcification and histopathology.
RESULTS: Serial echocardiogram showed an increase in cardiac output as the juvenile sheep grew without any decrease in effective orifice area (EOA) (>2cm2) or increase in pressure gradients (<10mmHg for both peak and mean). Linear regression analysis of systolic pressure drops and EOA showed no significant changes over implant duration (Fig 1a&b). Before explant at 18 months, valves were visually imaged using intravascular echocardiography which showed no flow restriction (Fig 1c), fully coapting leaflets (Fig 1d) and end-on view with leaflet coaptation and no central regurgitation. Paravalvular regurgitation was noted due to frame migration post-implant. Explants were performed at 6 months (n=2), 12 months (n=1) and 18 months (n=2). The comparison between implanted tissue and explanted valves after 6, 12, and 18 (Fig. 1 e&f) months showed a comparable tissue thickness with no deterioration. Quantitative measurements showed no change in calcium content (pre-implant= 0.181 μg/mg dry weight, vs explant 18months =0.150±0.012 μg/mg dry weight). MicroCT and histological assessment showed mild calcification and mild thrombosis.
CONCLUSIONS: The 18-month implants in the highly calcific juvenile sheep model showed no loss of function and no deterioration of the bioengineered tissue, suggesting a suitable alternative leaflet material for younger patients where functional longevity is critical.
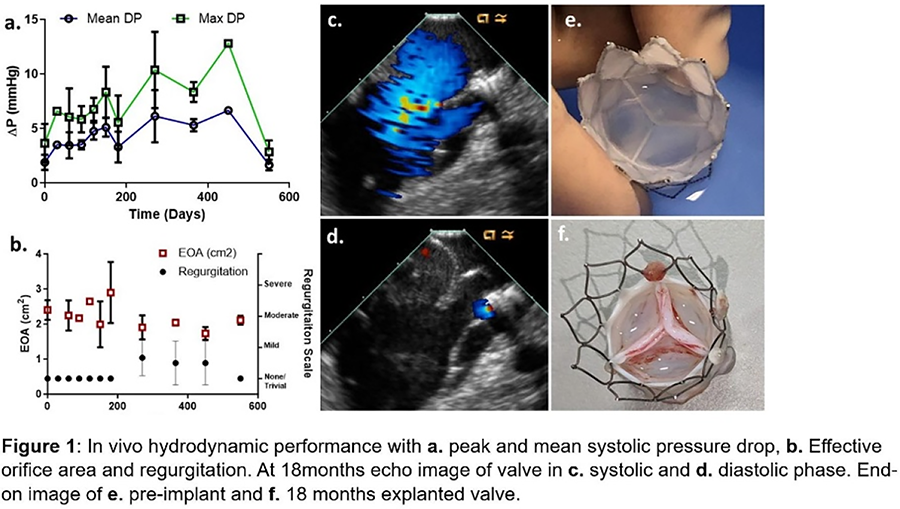
Presentation Number: i6Publishing Title: Optimal Decellularization And Xenoantigen Removal For Tissue
Valve
Author Block: Hong-Gook Lim1, So Young Kim1, Gi Beom Kim1, Yong Jin Kim2.
1Seoul National University Hospital, Seoul, Korea, Republic of, 2Sejong General Hospital, Bucheon, Korea, Republic of.
Abstract Body:
OBJECTIVE: Tissue valve has been used largely, but recipient immune response to antigenic components of the xenogeneic tissues results in deterioration, inflammation and calcification. The major xenoantigens are the Galα1-3Gal (α-Gal) epitope, which is responsibe for hyperacute graft rejection upon transplantation in humans, and the non-human sialic acid N-glycolylneuraminic acid (Neu5Gc), which cause acute graft rejection. The aim of this study was to evaluate safety and efficacy for optimal decellularization and enzymatic treatment for removal of xenoantigens.
METHODS: Porcine pericadia were treated with 0.25% sodium dodecyl sulfate (SDS) and 0.5% Triton X-100 through the multi-step methods with hypotonic, isotonic and hypertonic buffer solution. Decellularized porcine pericardium was treated with enzymatic xenoantigen removal with alpha-galactosidase for the removal of α-Gal xenoantigen and peptide N-glycosidase F (PNGase-F) for the removal of non-gal xenoantigens (Neu5Gc). We investigated the biomechanical properties, and efficacy through expression of carbohydrate-binding lectins in porcine pericardium for xenoantigen removal.
RESULTS: Mechanical test (tensile strain at break, tensile displacement at break, and tensile stress at break), and permeability test demonstrated that differently treated porcine pericadia resulted in no significant alterations in material characteristics. Decellularization was completed without histological changes, and showed lower fluorescence than native pericardium. Enzymatic xenoantigen removal reduced more effectively the expression of lectins (Jacalin, MAL-I, WGA, RCA-I, GSL, ECA, PNA, SBA, WFA, and DSL). We also confirmed the synergistic effects for decreased lectin expression of enzymatic xenoantigen removal with alpha-galactosidase and PNGase-F.
CONCLUSIONS: This study demonstrates the safety of our decellularization and xenoantigen removal. Our decellularization protocols and enzymatic xenoantigen removal effectively removed the carbohydrates-associated xenoimmunogenicity. These effects may require preclinical studies to confirm enhanced graft biocompatibility, and further modifications of the tissue engineering protocols in the future.
Presentation Number: i7Publishing Title: Material Topography Dictates Neutrophil Deposition On Synthetic And Natural Scaffolds For Tissue Engineered Heart Valve Scaffolds In A Blood Environment
Author Block: Valentine C. Vetter, Anthal i.P.M. Smits, Carlijn V.C. Bouten.
Eindhoven University of Technology, Eindhoven, Netherlands.
Abstract Body:
OBJECTIVE: Tissue engineered heart valves (TEHVs) offers a promising solution to the challenges associated with current valve replacements. However, clinical application of TEHVs is hindered by a limited understanding of the host response to them in the complex environment of the bloodstream, particularly the initial tissue formation. Neutrophils, play a critical yet poorly understood role in tissue regeneration. Neutrophils are the first cells to colonize TEHVs upon implantation and their interactions with biomaterials, including the formation of neutrophil extracellular traps (NETs), have attracted significant research attention. Nevertheless, how neutrophils respond to different scaffold materials and the implications for subsequent tissue regeneration remain critical unanswered questions. This study investigates neutrophil deposition on various tissue-engineered cardiovascular scaffolds —synthetic and biological— and its significance for tissue regeneration.
METHODS: Primary human neutrophils were seeded onto ten combinations of synthetic and biological scaffolds, including pericardium, electrospun, decellularized heart valves, and via a custom-made molding shaped as a heart valve (fig. 1B). Neutrophil characterization, activation, and NET quantification were assessed at 4 and 24 hours. To examine the influence of neutrophil-conditioning on materials, donor-matched monocytes were subsequently seeded onto the scaffolds and analyzed by multiplex ELISA, PCR and IF.
RESULTS: Neutrophil deposition occurred on all electrospun scaffolds, with NET formation showing a binary pattern and notable heterogeneity across samples. In contrast, this was not observed for most of the leaflet shaped scaffolds (fig. 1A,C). Thorough analysis of these materials revealed scaffold topography determined these interactions. Preliminary findings suggest that neutrophil deposition on electrospun biomaterials enhances either the pro- or anti-inflammatory responses of macrophages.
CONCLUSIONS: Our findings suggest that scaffold topography, rather than the material stiffness or its nature, drive the early host response to scaffolds materials. Furthermore, neutrophil preconditioning showed to impact the macrophage response to TEHVs.
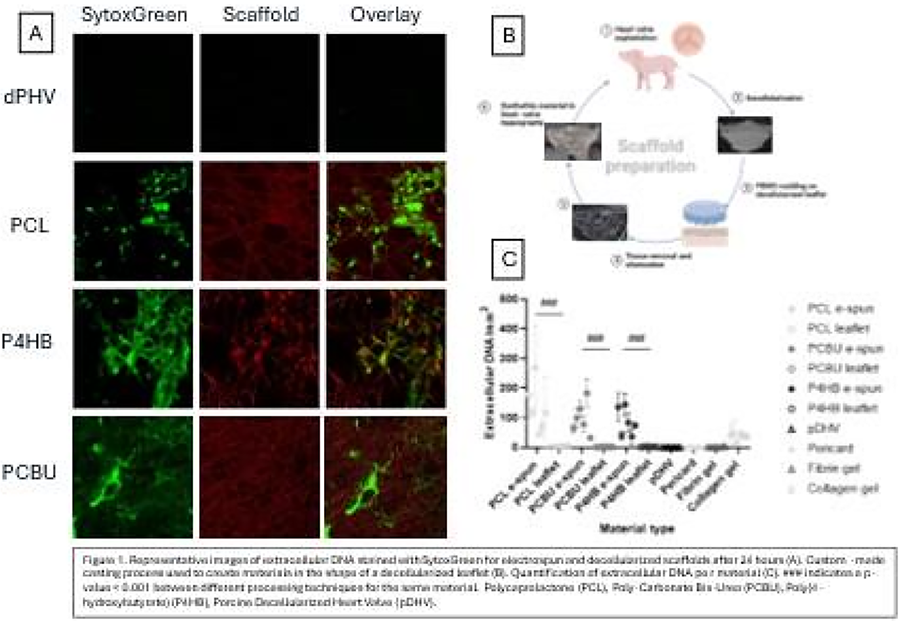
Presentation Number: i8Publishing Title: New Directions For Tissue-manipulating Protocol Optimization In Bioprosthetic Heart Substitutes: Quantification Of Xenoantigens And Enzymatic Treatment For Their Removal.
Author Block: Saima J. Imran, Bettina T. Talamini, Giorgia Cibin, Chiara Tessari, Gino Gerosa.
University of Padova, Padova, Italy.
Abstract Body:
OBJECTIVE: Although the large portfolio of heart valve substitutes, the major drawback of all currently available bioprosthetic heart valves (BHVs) is their limited durability. Α-Gal and Neu5Gc epitopes are recognized to be two potent xenoantigens inducing immunologic response in humans leading to pannus ingrowth, cusps’ stiffening and dysfunction, and calcification. It has been already demonstrated that BHVs with older tissue-manipulating protocols presented both xenoantigens on their surfaces. Tissue-manipulating protocols have the aim to improve BHVs structural durability, and one goal is to remove or inactivate xenogeneic/allogeneic determinants expressed in BHVs tissues. We investigate the residual presence of αGal and Neu5Gc xenoantigens in three BHVs models with the newest tissue-manipulating protocols currently available and the possibility to reduce them with an enzyme-based tissue-treatment protocol.
METHODS: Six devices from 3 different BHVs models with the newest tissue-manipulating protocols were tested. The number of epitopes was determined with reference to a standard αGal and Neu5Gc source by two dedicated ELISA tests. The presence of xenoantigens was subsequently confirmed by immunofluorescence analysis. Porcine tissue, knockout for both αGal and Neu5Gc epitopes, was used as negative control. Two concentrations of enzymatic treatment with α-Galactosidase enzyme (50 U/mL and 150 U/mL) were applied to remove αGal epitopes.
RESULTS: ELISA showed the significantly levels of αGal and Neu5Gc epitopes in the BHVs post treated with the washing buffer. The enzymatic treatments with the two different concentrations α-Galactosidase enzyme reduced the αGal to the maximum percentage between 97-99%. Lectin based immunofluorescence data shown to be comparable with the obtained results by ELISA.
CONCLUSIONS: The study showed the presence of αGal and Neu5Gc xenoantigens in all the evaluated BHVs models to a moderate levels. Alpha-galactosidase enzyme treatments found to be efficient in αGal epitope removal, representing a possible tool for optimizing tissue-manipulating protocols.
Presentation Number: i9Publishing Title: Spatial Proteomics Characterization Of In Situ Tissue Engineered Heart Valve Implants From Historical Ovine Animal Studies To Elucidate Material Remodeling
Author Block: Dewy C. van der Valk1, Esmee A. Meijerhof1, Cassandra Clift2, Rachel Cahalane2, Sylvia Dekker1, Taku Kasai2, Masanori Aikawa2, Marcelle Uiterwijk3, Jolanda Kluin3, Anthal I.P.M. Smits1, Sasha A. Singh2, Frank P.T. Baaijens1, Elena Aikawa2, Carlijn V.C. Bouten1.
1Eindhoven University of Technology, Eindhoven, Netherlands, 2Center for Interdisciplinary Cardiovascular Sciences, Boston, MA, USA, 3Amsterdam University Medical Center, Amsterdam, Netherlands.
Abstract Body:
OBJECTIVE: In situ tissue engineering (TE) of valvular grafts presents a promising alternative to current valve replacements. Although various performance studies have examined TE materials using in vitro techniques and large animal models, the underlying mechanisms behind successful or adverse remodeling of these materials remains unclear. This study utilized proteomics analysis to gain mechanistic insights into graft and tissue remodeling, leveraging historical data from two in situ TE sheep studies.
METHODS: Previously, valve scaffolds made from electrospun TE materials were implanted in sheep for durations ranging from 1 to 12 months in the pulmonary position. The explants were fixed in formalin and stored in paraffin. In this analysis, whole leaflet sections of donor-matched TE explants and their native counterparts were collected. Anatomical regions of the TE leaflets (including anastomosis, base, mid, and tip) were precisely dissected using Laser Capture Microdissection (LCM). All samples underwent a refined protocol for paraffin-protein extraction tailored for proteomic analysis.
RESULTS: Comparative analysis between TE explants and native leaflets revealed the presence of 109 proteins unique to native leaflets, 493 proteins unique to TE explants, and 692 proteins common to both. Network analysis indicated that the native explants primarily interacted with vascular regulation and cellular homeostasis processes, while TE explants were predominantly involved in immune system-related networks. The regional proteomic analysis identified 2,216 proteins, highlighting significant differences in protein patterns across regions over time. For example, the tip region exhibited more involvement in coagulation and immunity, whereas the anastomosis region highlighted metabolic and intracellular pathway processes.
CONCLUSIONS: This study represents a pioneering analysis of location-specific protein expression over time within in situ TE heart valves. It identifies immune processes as integral to TE remodeling, contributing valuable insights that can guide future research monitoring these critical processes.
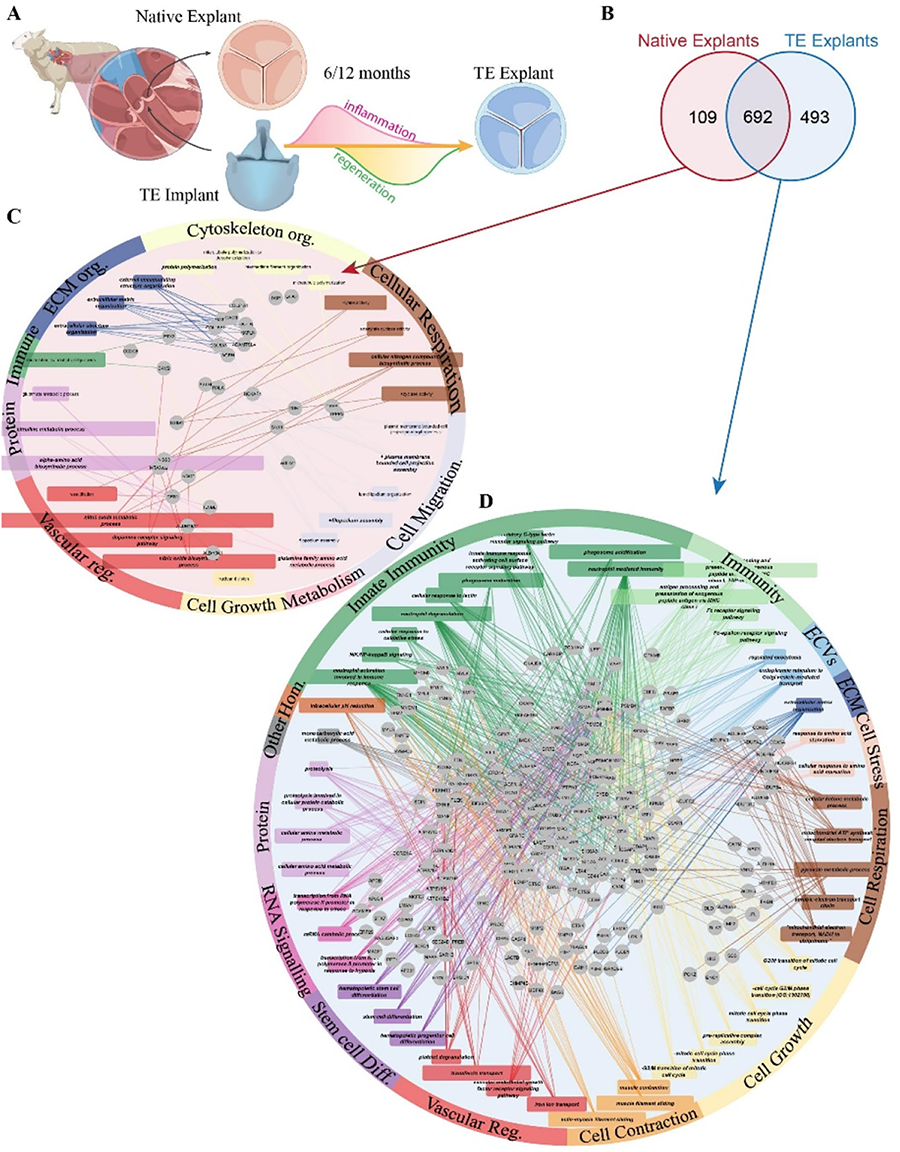
Presentation Number: i10Publishing Title: Can Losartan Controlled Release Improve The Bio-Hybrid Cardiac Patch In Preventing Left Ventricle Pathological Remodeling?
Author Block: Melika Malekhosseini1, Laura Modica De Mohac2, Giuseppe Pitarresi1, Wiliam Wagner3, Antonio D’Amore2.
1university of Palermo, Palermo, Italy, 2Ri.MED Foundation, Palermo, Italy, 3Departments of Surgery and Bioengineering, McGowan Institute for Regenerative Medicine, University of Pittsburgh, Pittsburgh, PA, USA.
Abstract Body:
OBJECTIVE: Cardiac patches (CP) are a promising alternative to prevent pathological remodeling following heart attacks. This study builds on previous research demonstrating the biohybrid approach's effectiveness in a rat chronic infarction model at 8 and 16-weeks post-injury, aiming to enhance this efficacy through the controlled release of Losartan.
METHODS: The bio-hybrid CP was created using double-stream-electrospinning, combining Poly(ester-carbonate-urethane) urea (PECUU) with cardiac extracellular matrix (ECM) gel derived from decellularized porcine hearts. Drug-loaded Poly (D,L-lactide-co-glycolide)(PLGA) microparticles were incorporated into the ECM-gel. The patch's microstructure was characterized using scanning-electron-microscopy and digital image analysis, focusing on fiber orientation, diameter, and intersection density. Cell viability and proliferation were assessed using Alamar-Blue over 14 days, along with histological staining at predetermined intervals. Patch topology, Young’s Modulus, and suture retention were measured via a dial indicator gauge-biquintic interpolation and uniaxial-tensile-testing (UTT), respectively. Biomaterial anisotropy was evaluated via biaxial-tensile-testing (BTT). hydrolytic degradation and Losartan release were evaluated over 14 days. C2C12 cell culture was adopted to assess cell infiltration.
RESULTS: The study utilized a custom algorithm to identify fiber orientation index of 0.65 for the ECM-side and 0.77 for the polymer-side, indicating a significant alignment in the polymer. The patch's anisotropy was relevant to physiological conditions, with mechanical testing showing the circumferential direction was stiffer (1.34 MPa) compared to the longitudinal (0.89 MPa). The patch's average thickness was 390±7.39 µm. Cell viability assays and histological evaluations confirmed the patch's biocompatibility, promoting cell growth and infiltration.
CONCLUSIONS: This research successfully integrates a biohybrid approach that combines mechanical control with bioactivity, achieving physiologically relevant anisotropy and enabling the controlled release of Losartan. Future studies will investigate the in-vivo performance of this cardiac patch in a rat coronary ligation model to determine the synergistic effects of Losartan on preventing pathological remodeling post-infarction.

Presentation Number: i11Publishing Title: Incremental Stretch Increases Strength And Toughness While Increasing Graft Size In 3d Printed Engineered Heart Valve Leaflets
Author Block: John Toftegaard, Benjamin Albert, Gaetano Scuderi, Jonathan Butcher.
Cornell University, Ithaca, NY, USA.
Abstract Body:
OBJECTIVE: Conditioning strategies for engineered heart valve tissues focus primarily on cyclic loading at constant peak stresses. Less is known about which incremental increases in mechanical loading optimize biomechanical remodeling. We hypothesized that incremental static stretching (ISS) of engineered valve tissues would augment biomechanical strengthening while achieving a larger stable graft size.
METHODS: 3D printed hydrogels were incrementally stretched across a custom expandable post array. We tested defined increments and timing of uniaxial stretch during a 14-day culture period of fibrin gels (2 mg/ml) with mesenchymal stem cells (1M/ml), up to 100% in tissue size. We then engineered valve leaflets and tested the effect of incremental biaxial stretch. Third, we engineered Type 1 collagen (5-15 mg/ml) fiber reinforced fibrin gels with varying fiber anisotropies. We quantified mechanical properties, developed cell phenotype, and matrix composition/alignment. Finally, we engineered valve conduits with homogeneous vs. fiber reinforcement and tested their functional performance in a novel hemodynamic bioreactor.
RESULTS: Incremental static stretch increased tissue ultimate stress >3 fold (170 +/- 21 kPa to 601 +/- 85 kPa, P<0.001), nonlinear stiffness >8 fold, and toughness >2.5 fold while increasing 100% in graft size. Earlier stretch increments (< Day 7) had greater effect than later (> Day 10). Tissue strengthening correlated with aSMA and vimentin expression, with more vimentin, cell alignment, and matrix alignment at greater stretch magnitudes. Incremental stretch of 3D printed fibrous leaflets demonstrated biomechanical anisotropy correlated with fiber pattern, with reduction in aSMA/Vimentin ratio and increased collagen production. Valved conduits fabricated with stretched leaflets demonstrated physiologically desirable low cracking pressure opening characteristics, large effective orifice area, and diastolic coaptation across pediatric pressure conditions.
CONCLUSIONS: ISS is a promising approach to accelerate biomechanical strengthening while achieving stable graft sizing in engineered valve leaflets.
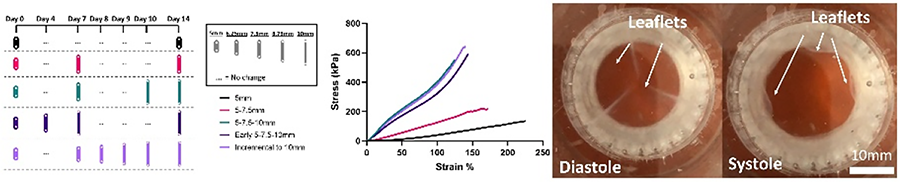
A1-A20, M1-M20, H1-H20 are poster competition presentations
Presentation Number: A1Publishing Title: Early And Midterm Outcomes Of Aortic Valve Leaflet Reconstruction With Three Same-sized Pericardial Leaflets
Author Block: Takeo Tedoriya, Ryuta Kiuchi, Kumiko Akiyama.
Tokyo D Tower Hospital, Tokyo, Japan.
Abstract Body:
OBJECTIVE: Aortic valve leaflet reconstruction with autologous pericardium or bovine pericardium is an option for aortic valve surgery. We have performed a unique technique of aortic valve leaflet reconstruction using three same-sized pericardial leaflets (ATLAS). We had introduced a three dimensional-virtual reality (3D-VR) workstation to clarify physio-anatomical details of the aortic root to enhance reproducibility of this technique. We evaluated early and midterm outcomes of ATLAS procedure with 3D-VR image analysis as well as echocardiogram.
METHODS: Basic technique; 1) autologous pericardium treated by 0.6 % or bovine pericardium are tailored to a template referred by the STJ diameter, 2) new commissures and nadirs were confirmed, 3) tailored leaflets are sutured to the annulus by continuous stitching, 4) commissure coaptation stitches between each leaflet were placed, 5) STJ is fixed by pericardial stripe. Enrolled patients underwent ECG-triggered cardiac CT to obtain 3D-VR image of the aortic root configuration. We evaluated trans-thoracic echocardiography results one month and six months, then in every year.
RESULTS: From 2016, ATLAS were performed in 52 patients (AS=20, AR=25, active IE=7). In 17 patients, 3D-VR analysis revealed unbalanced aortic annuls, which required additional procedures. Postoperative analysis showed appropriate correction of the aortic root. One patient died by sepsis of preoperative active IE. One redo AVR was required due to perforation of one leaflet. Echocardiographic evaluation revealed no aortic leaflet problem with minimum pressure gradient in maximum follow-up of 8.7 years
CONCLUSIONS: ATLAS can provide a simple and reproducible procedure that allows anatomical physiologic correction of the aortic valve. Early and midterm outcomes were acceptable for aortic valve surgery, although further strict follow up should be necessary.
Presentation Number: A2Publishing Title: National Trends In TAVR V. SAVR In Patients Younger Than 65
Author Block: Philip Allen1, Robert Semco2, Thais Faggion Vinholo1, Jake Awtry1, Paige Newell1, Sameer Hirji1, Ashraf A. Sabe1.
1Brigham and Women's Hospital, Boston, MA, USA, 2Harvard Medical School, Boston, MA, USA.
Abstract Body:
OBJECTIVE: Given increasing TAVR utilization for low-risk patients, we sought to analyze national TAVR trends for patients <=65 years.
METHODS: Using National Inpatient Sample (NIS), we identified (using administrative coding) patients <=65 yrs (stratified by age: <55, 56-60, and 61-65) undergoing isolated bioAVR, mechAVR or TAVR from 2012-2021 (2015 was excluded due to switch from ICD-9 to ICD-10). We compared pre and post-operative characteristics with univariate methods and conducted multivariable analysis to examine the association with center TAVR volume, teaching status and ownership to TAVR utilization.
RESULTS: A total of 138,705 patients were included - 22,865 (16.5%) underwent TAVR, 76,425 (55%) bioAVR, and 39,415 (28.4%) mechAVR. TAVR patients had significantly higher rates of heart failure 71.4% vs 32.4% bioAVR and 31.2% mechAVR, CKD 29.8% TAVR vs. 11.1% bioAVR and 9.8% mechAVR, COPD 32.0% TAVR vs. 20.5% bioAVR and 18.3% mechAVR and CAD 52.1% TAVR vs. 43.5% bioAVR and 30.4% mechAVR. In-hospital mortality was low among all 3 modalities and age groups (1-1.5%). The relative frequency of TAVR increased across all ages from <5% to a peak of 42% for patients 61-65 and 27% for patients 56-60 (Fig 1A). Low volume TAVR centers had a lower percentage of TAVRs compared to SAVRs (Fig 1B). On multivariable analysis, high volume centers were more likely to do TAVR in younger patients, but compared to private non-profits, government and private for-profits were associated with increasing TAVR use (0.33 and 0.08 regression estimates, p<0.05), as well as urban non-teaching hospitals (regression estimate 0.20, p<0.001).
CONCLUSIONS: The use of TAVR in patients <65 continues to increase, with TAVR ∼40% of isolated AVRs in patients 61-65 by 2021. Government and private, for-profit hospitals, as well as urban non-teaching hospitals, were associated with increased TAVR usage in younger patients.
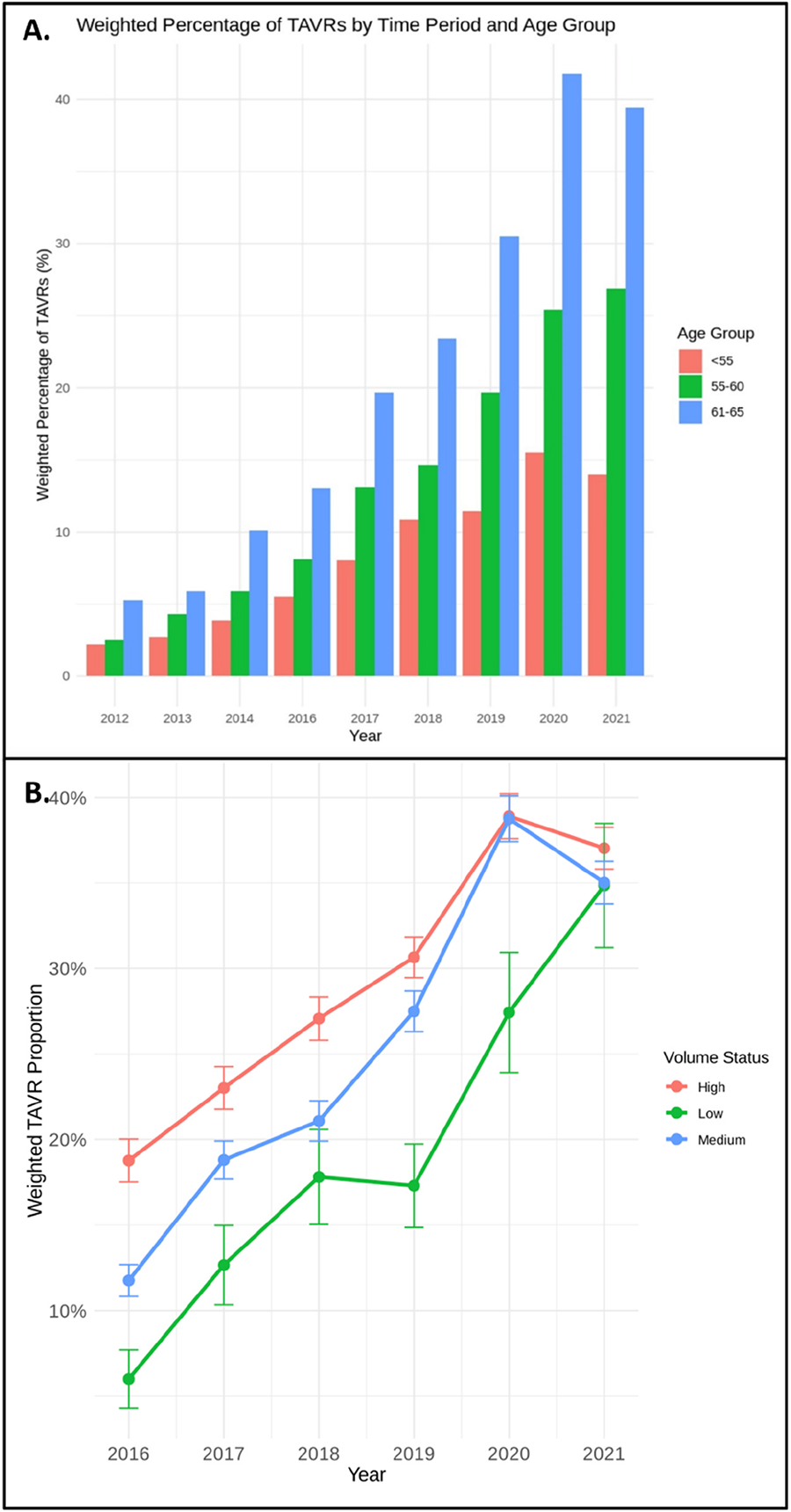
Presentation Number: A3Publishing Title: 8-year Follow-up Of Balloon-expandable Versus Self-expanding Bioprostheses In Patients Treated With Valve-in-valve Transcatheter Aortic Valve Replacement
Author Block: Mohiuddin Cheema, Robert Hagberg, Sabet Hashim, Raymond Mckay, Jeffrey Mather, Talhat Azemi.
Hartford Hospital, Hartford, CT, USA.
Abstract Body:
OBJECTIVE: Valve-in-Valve (VIV) transcatheter aortic valve replacement (TAVR) has been documented to be a safe and efficacious alternative to redo surgical aortic valve replacement. There are limited reports comparing long term VIV TAVR outcomes for balloon-expandable (BE) versus self-expanding (SE) bioprostheses.
METHODS: From a total cohort of 184 VIV TAVR procedures performed since 2012, we compared in-hospital and late outcomes in 39 patients treated with BE valves (Sapien [n=3], Sapien XT [n=3], Sapien 3 [n=33]) with 145 patients treated with SE valves (Corevalve [n=4], Evolut series [n=141]).
RESULTS:In comparison to SE patients, BE patients were more likely male (79.5 vs 62.1%, p=0.042), but otherwise the two cohorts were well matched for age (74.1±9.1 vs 75.9±10.7 years, p=0.161), STS risk Score (12.9±11.1 vs 10.4 ±8.2%, p=0.176), cardiovascular risk factors, comorbidities, pre-procedure echocardiographic and coronary angiographic findings, vascular access, fluoroscopy time, and contrast use.
BE and SE patients did not differ with respect to in-hospital mortality (0.0 vs 3.4%, p=0.246), stroke (0.0 vs 0.7%, p=0.603), procedural coronary obstruction (2.6 vs 0.0%, p=0.053), major vascular complication (0.0 vs 0.0%, p=1.000), composite bleeding (0.0 vs 2.1%, p=0.365) or permanent pacemaker implantation (5.1 vs 3.4%, p=0.626).
At 30-days post-TAVR, BE patients had higher mean aortic valve gradients (20.2±11.8 vs 12.5±6.4 mmHg, p<0.001), with no differences with respect to left ventricular ejection fraction, aortic valve area, and degree of aortic insufficiency.
Kaplan-Meier survival analysis following hospital discharge for the two cohorts demonstrated no significant difference in all-cause mortality at a mean follow-up time of 93.8 (82.2-105.5) months (p=0.535).
CONCLUSIONS: In comparison to SE VIV, BE VIV was associated with a higher post procedure mean aortic valve gradients, but no differences in effective orifice area, aortic insufficiency and in-hospital complications. BE and SE cohorts had similar survival rates at a mean follow-up time of 93.8 months.
Presentation Number: A4Publishing Title: Long-term Results Of Rapid Deployment Stented Bioprostheses In Minimally Invasive And Conventional Aortic Valve Replacement
Author Block: Romy M.J.J. Hegeman1, Ufuk B. Baldan1, Bart P. van Putte2, Geoffrey T.L. Kloppenburg3, Robert J.M. Klautz1, Patrick Klein1.
1Amsterdam University Medical Center, Amsterdam, Netherlands, 2St. Antonius Hospital, Nieuwegein, Netherlands, 3St. Antonius Ziekenhuis, Nieuwegein, Netherlands.
Abstract Body:
OBJECTIVE: Rapid deployment bioprostheses (RDBP) facilitate valve implantation especially in minimally invasive (MIS) surgical aortic valve replacement (SAVR) but are associated with increased risk of pacemaker implantation (PPI) and can be challenging in bicuspid aortic valves (BAV). We aimed to evaluate the outcome of RDSBP in both MIS and conventional SAVR, focusing especially on BAV.
METHODS: Between May 2015 and May 2023, all consecutive patients who underwent an isolated or combined SAVR procedure with the use of a RDBP in our center were included in a prospective database. Early and late outcome including mortality and reinterventions were assessed.
RESULTS: A total of 383 consecutive patients with a mean age of 72 ± 6 years (55% male) were included in this study. Overall survival was 89% at 8 years. MIS SAVR (N=183) was associated with significantly lower in-hospital mortality (p=0.011), while there was no difference in overall survival (p=0.838). 12 patients (3%) had to undergo a re-intervention of the aortic valve (9 for PVL closure, 2 for endocarditis and 1 for structural valve deterioration respectively), of whom 8 patients (67%) had a BAV (p=0.008). Significantly less patient prosthesis mismatch (PPM) occurred in patients with BAV (p<0.001). Type of BAV did not influence the incidence PPM (p=0.907). Both calculated moderate and severe PPM did not influence survival (p=0.834 and p=0.414 respectively) and neither did small valve size (p=0.751). PPI occurred overall in 8.4% but was not influenced by the presence of BAV (p=0.847).
CONCLUSIONS: The use of a RDBP in SAVR is associated with excellent long-term survival and freedom from reinterventions. It especially facilitates MIS SAVR, without compromising early risk. Although BAV pathology is a risk factor for re-intervention, it is also associated with less PPM and equal risk of PPI.
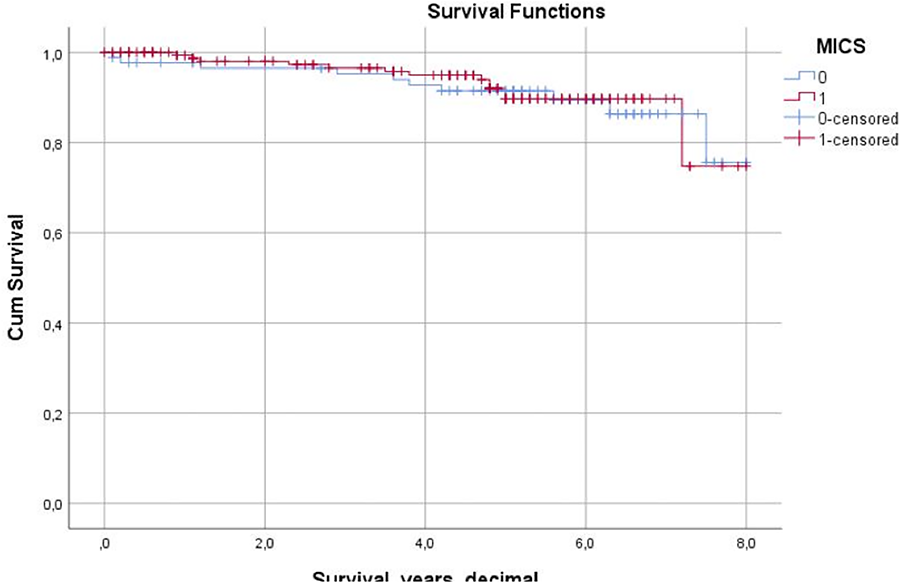
Presentation Number: A6Publishing Title: Prosthesis-Patient Mismatch Is Associated With Excess Long-Term Mortality In Young Adults After Aortic Valve Replacement
Author Block: Amine Mazine1, Anna Chu2, Rodolfo Rocha1, Terrence Yau1, Vivek Rao1, Philippe Pibarot3, Douglas Lee2, Tirone David1, Maral Ouzounian1.
1University of Toronto, Toronto, ON, Canada, 2Cardiovascular Program, ICES, Toronto, ON, Canada, 3Université Laval, Quebec City, QC, Canada.
Abstract Body:
OBJECTIVE: Prosthesis-patient mismatch (PPM) occurs when the indexed effective orifice area (iEOA) of a prosthetic valve is too small relative to patient body size. This study evaluates the impact of PPM on long-term outcomes in patients undergoing surgical AVR.
METHODS: We conducted a single-center observational study of patients undergoing first-time isolated AVR from 1990-2014. PPM was defined as iEOA <0.85 cm²/m², and severe PPM as iEOA <0.65 cm²/m². Demographics, surgical details, and in-hospital outcomes were collected prospectively. Cases were linked to provincial databases for long-term outcomes. The primary outcome was all-cause mortality; secondary outcomes were aortic valve reoperation and hospitalization for heart failure. Multivariable Cox regression analysis identified mortality risk factors.
RESULTS: Among 1,798 patients (no PPM: 770 [43%]; moderate PPM: 943 [52%]; severe PPM: 85 [5%]), mean age was 64±13 years, and 750 (42%) were female. Mechanical valves were implanted in 451 (25%) and bioprosthetic valves in 1,347 (75%). Aortic root enlargement was performed in 492 (27%). Mean follow-up was 13±7 years (max: 33 years). At 20 years, survival was 48% [95% CI: 43%-52%] in the “no PPM group” compared with 30% [26%-34%] and 25% [13%-39%] in the moderate and severe PPM groups, respectively (p<0.001) (Figure 1A). Larger iEOA was associated with lower long-term mortality (HR 0.95 per 0.10 increase in iEOA, 95% CI [0.91-0.98]; p=0.007). Smaller iEOA was associated with late mortality in patients <65 years (p<0.001) but not in those ≥65 (p=0.23). Readmission for heart failure was more frequent in patients with PPM (Figure 1B); no difference in reintervention was seen (p=0.654).
CONCLUSIONS: PPM is common after AVR and associated with late mortality and heart failure, especially in younger patients. These findings may have important implications for the lifetime management of aortic valve disease.
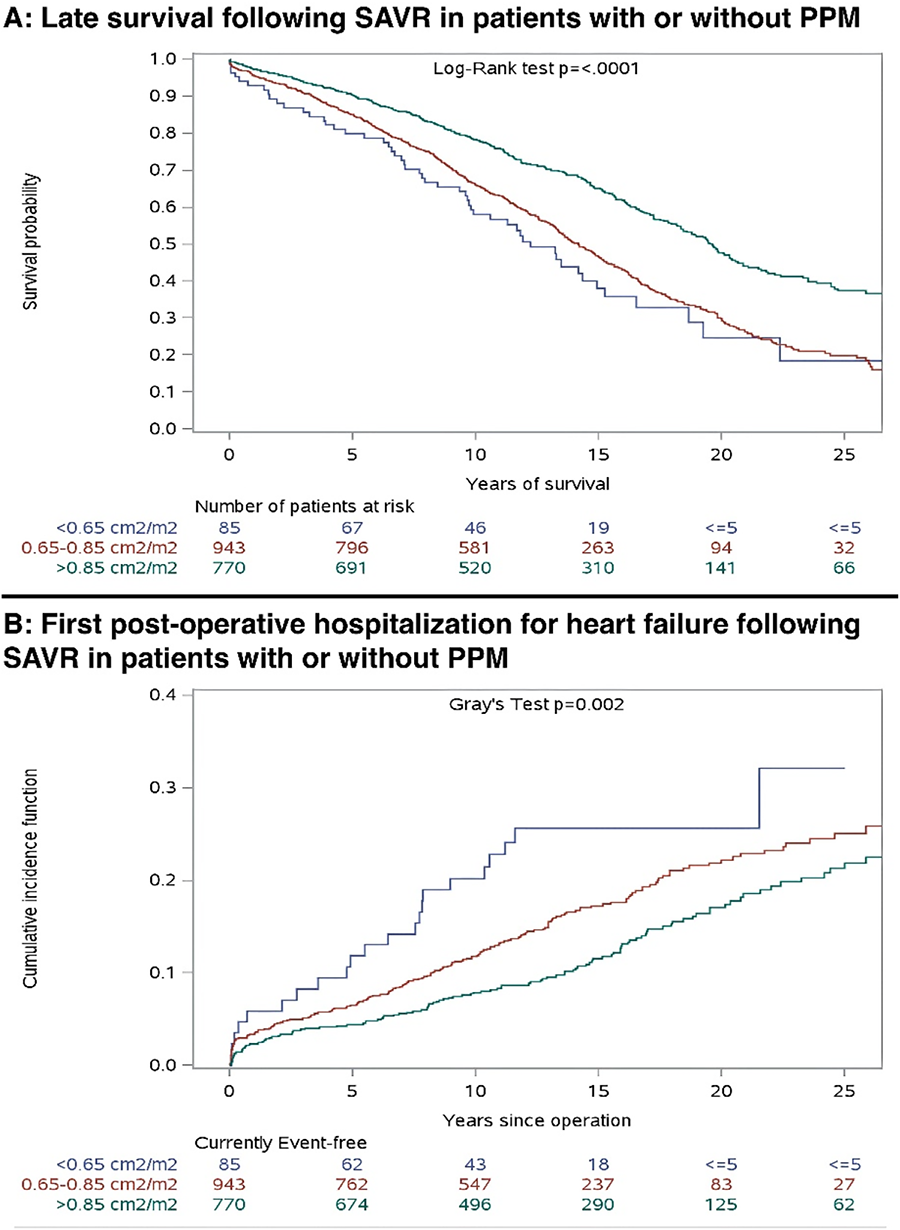
Presentation Number: A7Publishing Title: Incidence And Predictors Of Readmissions For Heart Failure In Patients Undergoing Surgical Or Transcatheter Aortic Valve Replacement
Author Block: Marcia Matilde Cortés, Martin Fasan, Juan Pedro Fescina, Maria Florencia Castro, Fernando Piccinini, Fernando Cura.
ICBA, Capital federal, Argentina.
Abstract Body:
INTRODUCTION: Heart failure (HF) readmissions in patients with severe aortic stenosis (SAS) undergoing aortic valve replacement (AVR) are common and linked to higher morbidity, mortality, and healthcare costs. There is limited data on this in South-America.
OBJECTIVE: To evaluate the incidence and predictors of HF readmissions in AVR patients.
METHODS: A prospective study analyzed patients with SAS undergoing AVR at a specialized cardiology center. The primary outcome was HF hospitalizations or unplanned emergency visits requiring intravenous diuretics. Multivariate analysis using Cox regression identified predictors.
RESULTS: The study included 441 patients (64% male, median age 76 years). Hypertension was present in 72%, 22% had a bicuspid aortic valve, and 26.5% were on diuretics. The median left ventricular ejection fraction (LVEF) was 60%. Of the patients, 57.6% had surgical AVR (SAVR) and 42% had transcatheter AVR (TAVR). The median follow-up was 364 days. During this period, 43 patients (9.8%) were readmitted for HF, with a median time to hospitalization of 25 days. Mortality was 9.3% for readmitted patients compared to 4.5% for those not readmitted. Risk factors for HF readmission included age over 80 years, hypertension, diabetes, pulmonary disease, prior diuretic use, and LVEF <50%. Procedure urgency and significant paravalvular leak were also associated. No significant differences in readmission rates were found between SAVR and TAVR. Multivariate analysis identified hypertension, urgent intervention, and significant paravalvular leak as independent predictors of readmission. Leak was present in 13% of TAVR patients but only 1.17% of those who had surgery.
CONCLUSIONS: HF readmission rates in AVR patients align with international data, predominantly occurring within the first 30 days post-procedure. Key predictors include hypertension, procedural urgency, and significant paravalvular leak. Improved monitoring of these risk factors during the initial 30 days could help reduce HF readmissions and their impact.
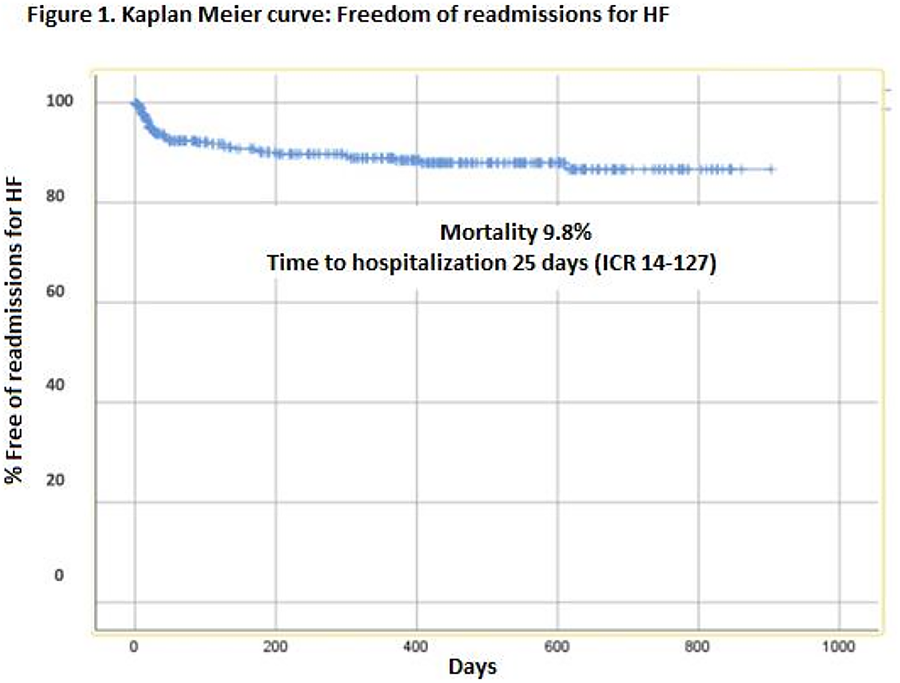
Presentation Number: A8Publishing Title: Transcarotid Approach To Transcatheter Aortic Valve Replacement As First-line Alternative Approach
Author Block: Andrew Cho, BS1, Tanya Rajabi, BS1, Andrew Jones, BA1, Hossein Amirjamshidi, MD2, Kazuhiro Hisamoto, MD2.
1University of Rochester School of Medicine and Dentistry, Rochester, NY, USA, 2University of Rochester Department of Surgery; Division of Cardiac Surgery, Rochester, NY, USA.
Abstract Body:
OBJECTIVE: Transcatheter aortic valve replacement (TAVR) is less invasive and requires shorter hospital stays when compared to surgical valve replacement. While transfemoral artery access for TAVR remains first line, it may not be feasible for patients with peripheral artery disease or small iliofemoral vessel size. In such cases, transcarotid vascular access has demonstrated more encouraging clinical outcomes than other alternative access sites. This approach, however, is less popular in the US, potentially due to less familiarity with carotid exposure among US-trained cardiothoracic surgeons. We aim to better understand the safety and outcomes of transcarotid TAVR in a US-based system.
METHODS: TAVR with a transcarotid approach between 2020 (when this institution began using transcarotid as first-line alternate access) and 2023 were identified and matched on age, sex, valve type, and, where possible, year of surgery in a 2:1 ratio with controls undergoing a transfemoral approach. 530 patients were screened. Complications and hospital stays were compared with chi-squared tests and t-tests.
RESULTS: No difference in rates of stroke, vascular complications, atrial fibrillation, or need for permanent pacemakers was noted between groups. Transcarotid TAVR procedures had a longer duration by 69 minutes, (184 mins vs 115 mins; p < 0.001) but median length of stay did not differ; both one day.
CONCLUSIONS: The transcarotid approach to TAVR is feasible and safe when transfemoral TAVR is contraindicated. While a transaxillary approach in these cases is more common in the US, this may be due to operator familiarity rather than evidence-based safety. Our institutional data showcase the successful use of a transcarotid approach as first alternative access for TAVR.
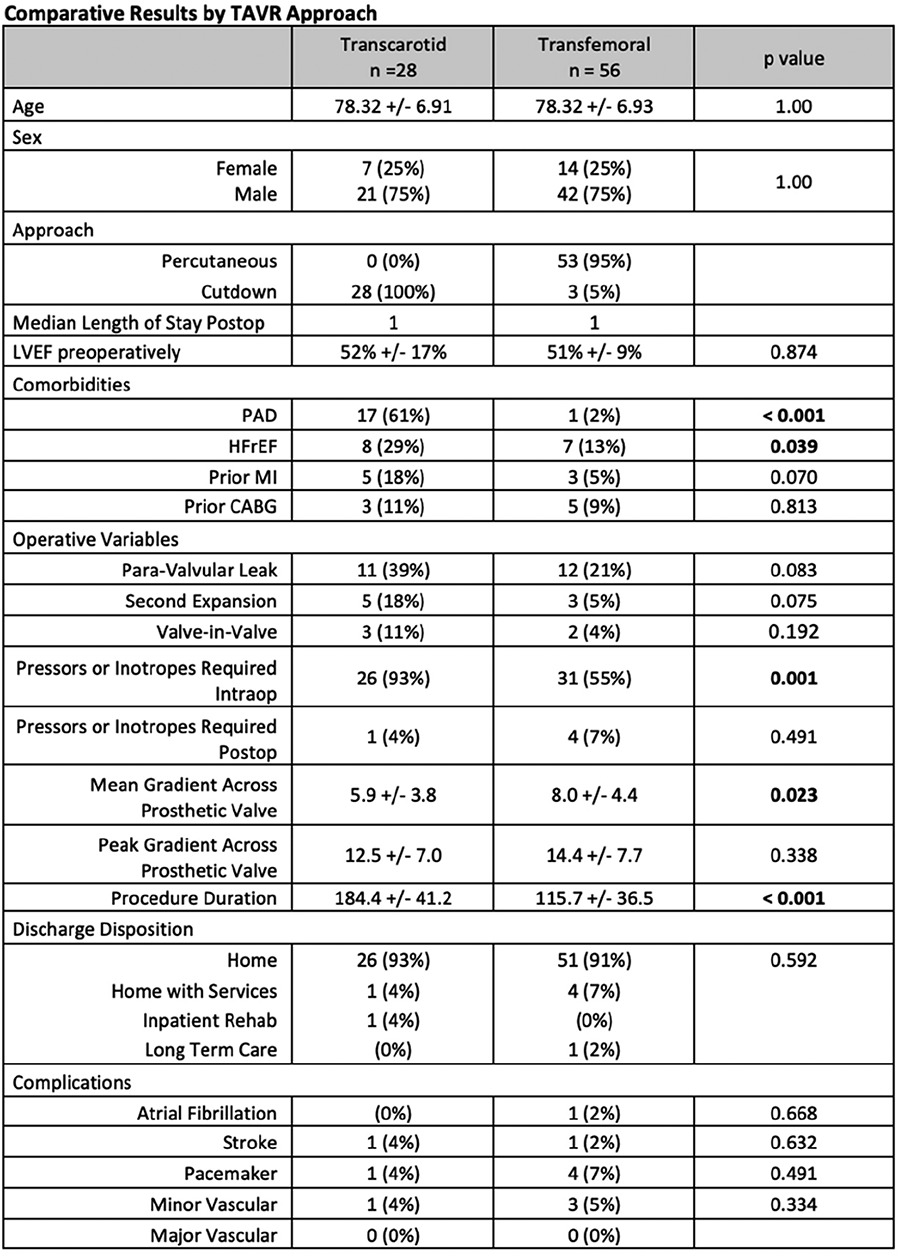
Presentation Number: A9Publishing Title: Impact Of Transcatheter Aortic Valve Replacement (TAVR) Program On Surgical Aortic Valve Replacement (SAVR) At A Veterans
Affairs Medical Center (VAMC):
Patient Risk Scores Vs.
Outcomes
Author Block: Neal Mukherjee1, Salvador A. Tello1, Aditya Dwivedi1, Manreet K. Dosanjh1, Joshua Xian1, Isaac Y. Kim1, Mitchka Mohammadi2, Axel Gomez-Casarez1, William P. Carroway1, Marko Boskovski1, Liang Ge1, Elaine Tseng1.
1University of California, San Francisco, SAN FRANCISCO, CA, USA, 2Oregon Health and Sciences University School of Medicine, Portland, OR, USA.
Abstract Body:
OBJECTIVE: Evaluate the impact of TAVR implementation at a VAMC on SAVR patient risk scores using Society of Thoracic Surgeons Predicted Risk of Mortality (STS-PROM), and outcomes by Valve Academic Research Consortium (VARC3).
METHODS: Nearly 350 SAVR patients since 2009 were reviewed for pre-operative characteristics relevant to STS-PROM and post-operative outcomes relevant to VARC3 criteria. Patients were compared between a pre-TAVR era from 1/1/2009-11/25/2013, the date of first TAVR at our VAMC, and a post-TAVR era from 11/26/2013-present. Both descriptive and inferential statistics were performed to determine significance.
RESULTS: Patient numbers and demographics remained similar across eras. Per Table 1, significant decreases in STS-PROM Operative Mortality and Morbidity & Mortality were observed between pre-TAVR and post-TAVR eras. Acute VARC3 outcomes, except for arrhythmias, improved post-TAVR, with significant reductions in relative frequencies of acute mortality, kidney injury, and bleeding requiring transfusion.
CONCLUSIONS: These findings suggest as TAVR was implemented fewer high-risk patients received SAVRs at this VAMC as they were likely switched over to TAVR. The patients that did undergo SAVR often had better outcomes likely due to a combination of improving technology/techniques and reduced operative risk. However, the significance of decreases in many VARC3 outcomes was limited by infrequent occurrences warranting additional data collection.
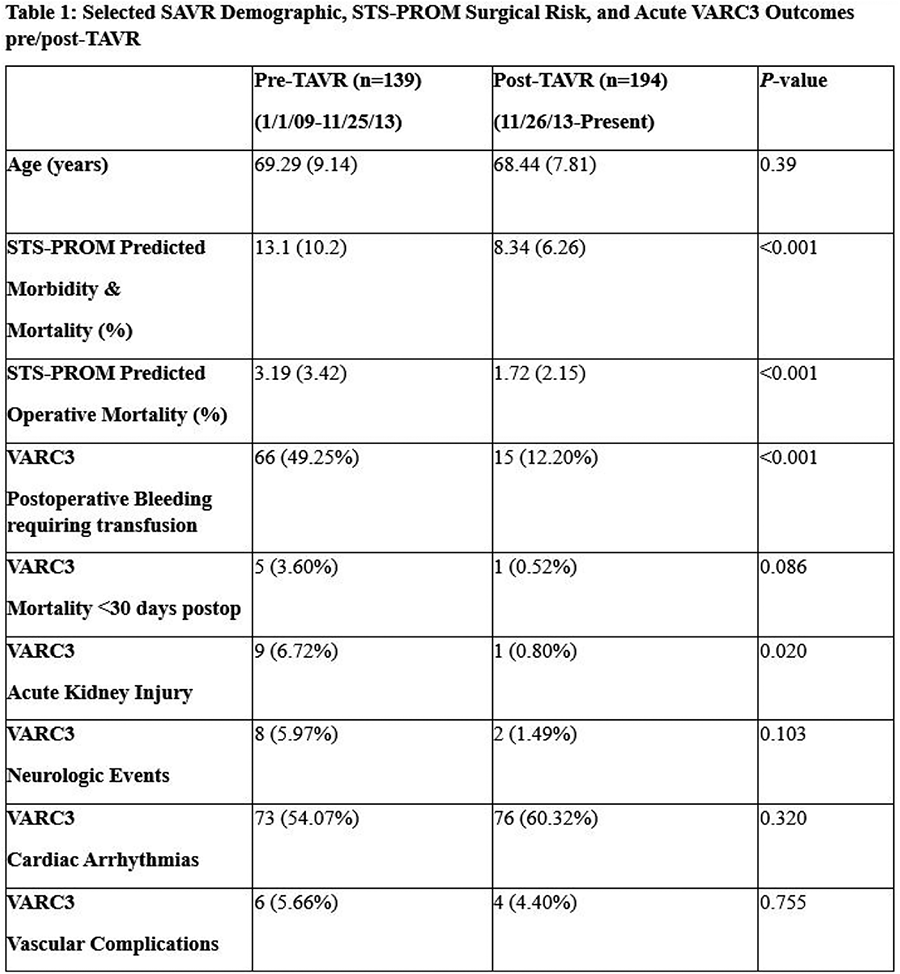
Presentation Number: A10Publishing Title: Assessment Of Valve Hemodynamics Following Transcatheter Versus Surgical Aortic Valve Replacement In Women With Small Aortic Annulus
Author Block: Elie Fadel1, Calvin Diep2, Eliza Calin2, Jean-Bernard Masson2, Jeannot Potvin2, Jean-François Gobeil2, Nicolas Noiseux2, Dimitri Kalavrouziotis3, Siamak Mohammadi3, Louis-Mathieu Stevens2, Jessica Forcillo2.
1McGill University, Montreal, QC, Canada, 2Centre Hospitalier de l’Université de Montréal, University of Montreal, Montreal, QC, Canada, 3Institut Universitaire de Cardiologie et Pneumologie de Québec, Université Laval, Québec, QC, Canada.
Abstract Body:
OBJECTIVE: Prosthesis-patient mismatch (PPM) has been shown to be related to worse survival and hemodynamic outcomes following valve replacement, and women with aortic stenosis (AS) are more susceptible than men. The objective of this study was to compare the incidence of PPM in a female population with small aortic annulus (SAA) undergoing TAVR vs. SAVR using the Carpentier Edwards Magna Ease bioprosthetic valves (19-21mm) and the Edwards Sapien 3 and Sapien 3 Ultra transcatheter valves (20-23mm).
METHODS: This retrospective study was conducted using harmonized databases from two high-volume cardiac surgery centers. Female patients with SAA (≤23mm) measured by echocardiography who underwent SAVR or TAVR between 2011 and 2022 were included. The primary endpoint was to compare the incidence of moderate to severe PPM, both measured and predicted, in women receiving TAVR versus SAVR. Secondary endpoints included various clinical outcomes.
RESULTS: A total of 426 women were included. 64.8% underwent SAVR (mean age:75) and 35.2% underwent TAVR (mean age:81). SAVR patients received 19- or 21-mm prostheses (32% and 68% respectively). Almost all TAVR patients (94%) were assigned a 23 mm prosthesis, with the others receiving a 20 mm prosthesis. While 53% of SAVR patients were predicted to have a moderate to severe PPM (P-PPM), 39% of TAVR patients were predicted to do so (p=0.005). When it came to measured PPM (M-PPM), 73% of SAVR versus 32% of TAVR patients had moderate to severe PPM (p<0.001). Proportions were lower when adjusting for BMI>30 (P-PPM - SAVR: 25%; TAVR: 19%; p=0.148; M-PPM - SAVR: 64%; TAVR: 23%; p<0.001).
CONCLUSIONS: In women with SAA, a larger proportion of SAVR patients had moderate to severe P-PPM or M-PPM compared to TAVR patients. Adjusting for BMI>30 showed similar trends, although overall proportions were lower.
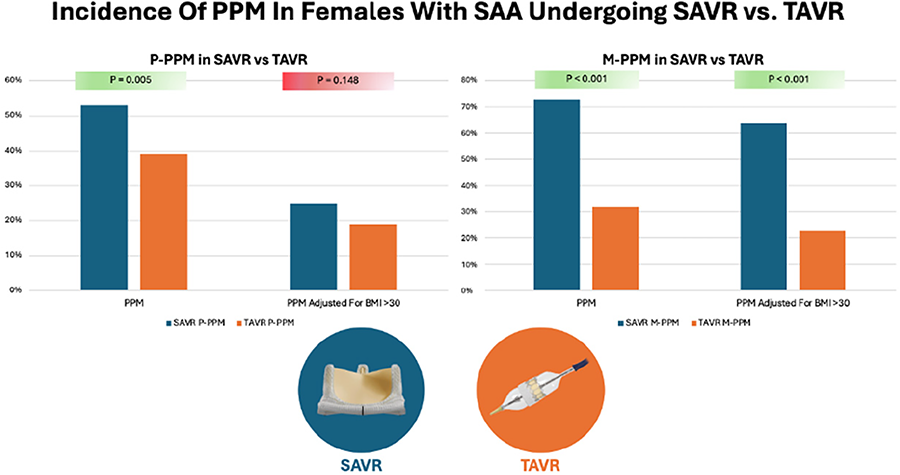
Presentation Number: A11Publishing Title: Aoritc Valve Leaflet Reconstruction For Type 0 Bicuspid Aortic Valve Case Designed By 3-d Virtual Reality Imaging Analysis
Author Block: Takeo Tedoriya.
Tokyo D Tower Hospital, Tokyo, Japan.
Abstract Body:
OBJECTIVE: Aortic valve leaflet reconstruction using three same-sized pericardial material have been performed for strictly selected cases of aortic valve diseaes. In the cases of unbalanced Valsava sinuses, aortic valve repair or aortic valve leaflet recontruction would be difficult to obtain ideal coaptation height. Threrefore, we introduced a unique 3-D virtual reality workstation in order to evaluate anatomical condition of the aortic root and simulate surgical procedures for complicated cases such as type 0 biscuspid aortic valve.
METHOD: We had a 53-year-old male with type 0 bicuspid severe aortic stenosis and regurgitation. The DICOM data of cardiac CT were installed to 3-D workstion to simulate the surgical procedure to accomplish our three same-sized leaflets reconstruction.
RESULT: In simulation of the surgery: 1) after observation of bicuspid native valve, we removed leaflets. 2) we marked new three commissures not to damage coronary orifices. 3) each leaflet-suture line was designed, one by one, LCC, RCC and NCC. During this stage of simulation, we realized that intra-leaflet triangle or ILT should be eliminated, because ILT is unfitted and too fragile for leaflet-stitching. 4) two ILTs were plicated and we could finally create leaflet-suture line. In our actual surgery: After measurement of the STJ diameter, both sides of ILT plication were completed then, we made crescent form the left Valsalva plication to create a new aortic root. Finally, we moved on to leaflet reconstruction, and completed the procedure. Postoperative echocardiography showed well-functioned new three leaflets without any leakage with mean pressure gradient of 6.0mmHg and aortic valve area of 2.34.cm2.
CONCLUSION: Aortic valve leaflet reconstruction for type 0 BA was successfully performed using 3-D VR analysis.
Presentation Number: A12Publishing Title: The Role Of Cd34 On The Calcification Of Human Aortic Valve Interstitial Cells Obtained Calcified Aortic Valve Stenosis Patients
Author Block: Zaiqiang Yu, Shihu Men, Kazuhiko Seya, Kazuyuki Daitoku, Masahito Minakawa.
Hirosaki University, Aomori, Japan.
Abstract Body:
OBJECTIVE: Calcified aortic valve stenosis (CAVS) is characterized by valve thickening and stenosis of the orifice area accompanied with valve calcification. Recently, we have demonstrated that human aortic valve interstitial cells (HAVICs) are positive on both mesenchymal stem cell markers (CD73, 90, 105) and endothelial cell marker (VEGFR2), then CD34-negative cells are responsible for aortic valve calcification. We aimed to confirm the pathophysiological role of CD34 in HAVICs obtained from calcified aortic stenosis patients by using various cytokines.
METHODS AND RESULTS: This study was approved by the institutional review boards of the Hospital of Hirosaki University. Calcified AV were obtained from CAVS patients performed SAVR. Human aortic valve interstitial cells (HAVICs) were isolated from AV by collagenase treatment. HAVICs were cultured in α-MEM with 10% FBS. The medium containing TNF-α (30 ng/ml) was replenished every 3-4 days. DNA microarray between CD34-positive and -negative HAVICs, separated by fluorescence-activated cell sorting, indicated that tenascin X (TNX) mRNA expression was significantly decreased in CD34-negative cells. We further confirmed that, in CD34-negative HAVICs, inflammatory cytokines, TNF-α and IL-1β significantly decreased the mRNA expression of CD34 in addition to TNX. While, TGF-β, a key cytokine of endothelial-mesenchymal transition, did not affect the HAVIC calcification. Overexpression of CD34 significantly inhibited TNF-α-induced HAVIC calcification, maintaining TNX mRNA expression.
CONCLUSIONS: These results suggest that CD34 is one of regulator for valve calcification and the loss of CD34-positive HAVICs by TNF-α and IL-1β pathophysiologically contributes to HAVIC calcification by decreasing the mRNA expression of extracellular matrix proteins such as TNX.
Presentation Number: A13Publishing Title: Evolution Of Quality Of Life Five-years After Minimally Invasive And Conventional Surgical Aortic Valve Replacement: Results From A Randomized Controlled Trial
Author Block: Idserd D.G. Klop1, Romy M.J.J. Hegeman1, Bart P. van Putte2, Geoffrey T.L. Kloppenburg2, Robert J.M. Klautz1, Pythia T. Nieuwkerk1, Patrick Klein1.
1Amsterdam University Medical Center, Amsterdam, Netherlands, 2St. Antonius Hospital, Nieuwegein, Netherlands.
Abstract Body:
OBJECTIVE: Surgical aortic valve replacement (SAVR) through conventional median sternotomy is safe and associated with an improvement in survival and quality of life (QoL). Minimally invasive SAVR is an equally safe alternative associated with potential additional advantages because of the reduced surgical trauma. This randomized controlled trial aimed to compare postoperative improvement and evolution in cardiac-related QoL five years after SAVR by upper hemisternotomy and conventional median sternotomy.
METHODS: Single-centre, investigator-initiated clinical trial that randomized patients to SAVR by upper hemisternotomy or conventional median sternotomy. Primary outcome was cardiac specific QoL, measured with the Kansas City Cardiomyopathy Questionnaire (KCCQ) at 5 years postoperatively. Secondary outcome were all other domains of the KCCQ, Short-Form 36 and survival. Predictors for change in cardiac specific QoL between one- and five-year follow-up were evaluated by multivariate logistic regression analysis.
RESULTS: QoL improvement after both procedures is excellent and sustained at 5 years follow-up, however patients experience important increase in physical limitations. Patients after minimally invasive SAVR had significantly higher physical limitation and total symptoms domain score (p=0.033). Overall survival at five years was 91.9% and did not differ between both approaches (p=0.417). Only baseline physical limitations (standardized beta: 0.35, p<.001) and age (standardized beta: -0.25, p=0.007) were significantly related to change in physical limitations domain scores. Only history of stroke was significantly related to change in total symptom domain score (standardized beta: -0.19, p=0.034).
CONCLUSIONS: Survival and QoL improvement after both minimally invasive and conventional median sternotomy is excellent and sustained at 5 years follow-up, however patients experience important increase in physical limitations. Patients after minimally invasive SAVR had a small but significant larger improvement in cardiac specific QoL. Better baseline physical condition and younger age are associated with greater and sustained improvement in physical limitations up at longer-term follow-up.
Presentation Number: A14Publishing Title: Robotic Coronary Revascularization And Transcatheter Aortic Valve Implantation In The Management Of Combined Coronary Disease And Aortic Stenosis For Moderate-high Risk Patients
Author Block: Mohamed Eldeiry1, Ashok Babu2, Amber Edwards3, Clayton Kaiser2, Mark Robbins2, Chandrashekhar Ramaiah2, Mark Stankewicz4, Michael A. Morse2, Evilio Rodriguez2.
1University of Washington, Seattle, WA, USA, 2Ascension St. Thomas, Nashville, TN, USA, 3Ascnesion St. Thomas, Nashville, TN, USA, 4Ascension St. Thomas, Nasvhille, TN, USA.
Abstract Body:
OBJECTIVE: This study aims to review the outcomes in patients with combined aortic valve and coronary disease who were managed using sternal-sparing approaches due to higher than average risk.
METHODS: Retrospective analysis was carried out from 2021 through 2024 looking at patients that had robot-assisted minimally invasive coronary artery bypass (R-MIDCAB) and transcatheter aortic valve implantation (TAVI) within 90 days. Pre-operative demographics and patient characteristics as well as post-operative outcomes, complications, and mortality were analyzed.
RESULTS: A total of 32 patients were included with 9 (28%) females and median age at initial procedure of 79 [interquartile range (IQR), 70-82]. Twenty-five had R-MIDCAB performed prior to the TAVI (78%). The mean time between procedures was 19 days [IQR 0-36] with 13 [41%] occurring in the same day. The median Society of Thoracic Surgeons' Predicted Mortality on initial presentation was 5% (IQR, 3-6%) and 13 (41%) patients had prior sternotomies. The incidence of smoking was 30% (6) active, and 70% (14) former with one patient (3%) on dialysis and two (6%) on home oxygen. The median New York Heart Association score was 3 (IQR 2-3). Successful myocardial revascularization was achieved in all patients. All patients had trace or less paravalvular regurgitation (PVL) post TAVI with the exception of one (3%) having a mild PVL. There were no strokes or transient ischemic attacks while one (3%) vascular access site bleeding was observed along with one (3%) pacemaker implantation. All patients were discharged and there were no 30-day mortalities.
CONCLUSIONS: Robotic coronary revascularization combined with percutaneous aortic valve implantation represents a viable therapeutic option for patients with aortic valve and coronary artery disease who present with elevated risk profiles.
Presentation Number: A15Publishing Title: Minimally Invasive Aortic Valve Replacement In Octogenarian In Okinawa Japan
Author Block: Masato Hayakawa, Ryo Ikemura, Satoshi Yamashiro, Kiyoshi Iha.
Chubu Tokushukai Hospital, Okinawa, Japan.
Abstract Body:
OBJECTIVE: In the era of transcatheter aortic valve replacement (TAVR), minimally invasive aortic valve replacement (mini-AVR) is challenging in octogenarian patients. Okinawa is located in the southernmost part of Japan and has the longest life expectancy among people over 75 as per 2020 statistics. Therefore, the need for mini AVR among octogenarians is expected to be higher than in other regions. The purpose of this study was to evaluate the effectiveness of mini-AVR in octogenarians.
METHODS: Among the 132 consecutive AVR performed in our hospital between January 2018 and December 2023, 27 patients aged above 80 years were isolated. Patients were divided into two groups, the median sternotomy group (median group, n=15) and the right mini-thoracotomy group (mini group, n=12), to assess preoperative comorbidities and postoperative outcomes, including long-term mortality and postoperative discharge target.
RESULTS: No significant differences were observed in preoperative characteristics between the two groups. Intraoperative characteristics were not significantly different between the two groups in terms of operation time, cardiopulmonary bypass time, aortic cross-clamp time, and blood loss; however, the mini group used more sutureless valves or rapid deployment valves (33.3% [n=5] in the median group vs. 83.3% [n=10] in the mini group). The 30-day mortality rates were 13.3% (n = 2) in the median group and 0% in the mini group. The 1-year survival rate was 73.3% (n=11) and 91.7 % (n = 11) in the median and minimum groups, respectively. In the mini group, 91.7% of patients (n=11) were discharged, while 8.3% (n=1) required transfer to a rehabilitation facility.
CONCLUSIONS: Our data add to the overall suggestion that patients aged above 80 years may be considered as candidates for mini-AVR if the preoperative evaluation is acceptable and should not be excluded based on age alone.
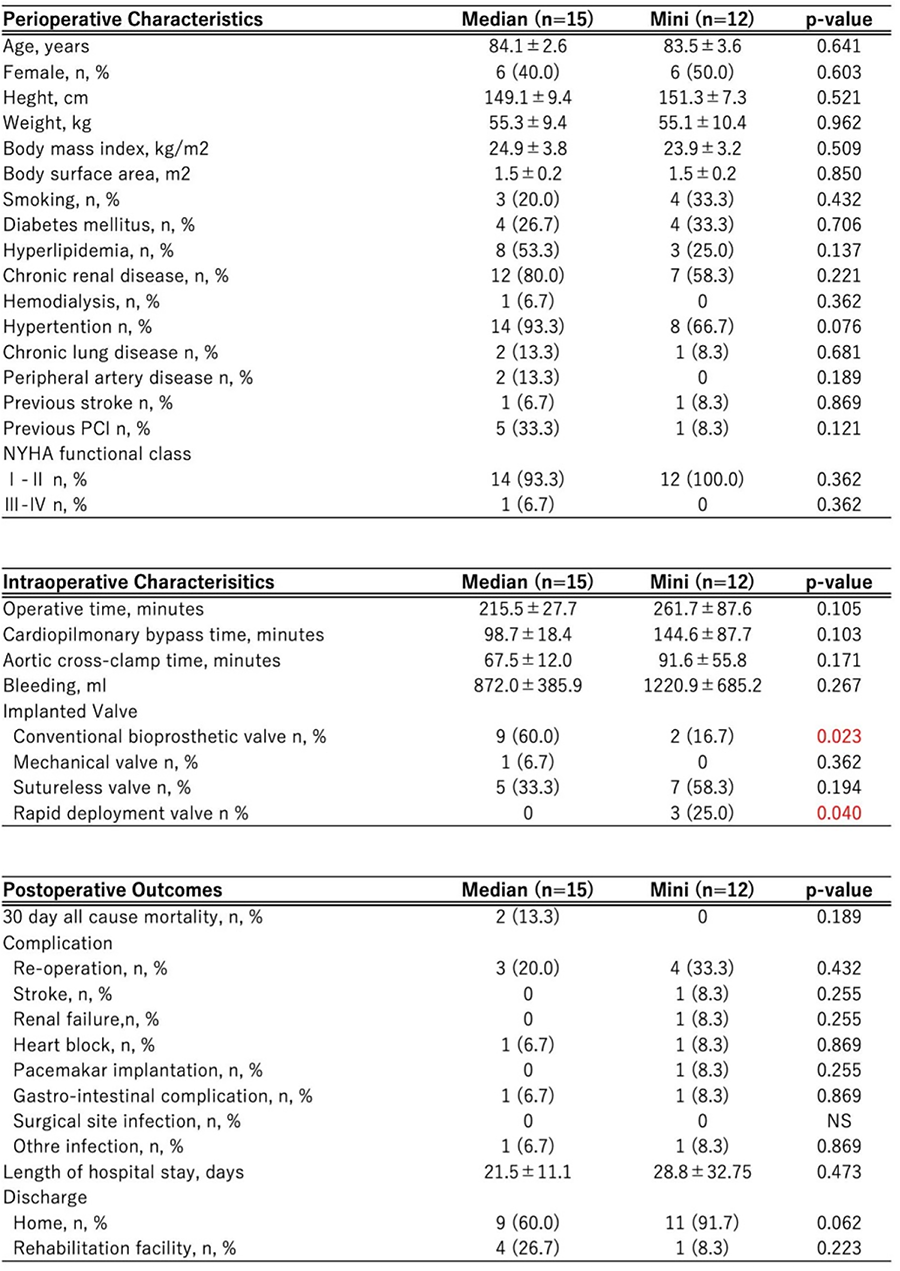
Presentation Number: A16Publishing Title: Valvular Expression Of Reelin Reveals Pathological Differences Among Calcific Aortic Stenosis And Aortic Regurgitation
Author Block: Mattie Garaikoetxea1, Eva Jover1, Ernesto Martin-Nuñez1, Miriam Goñi-Oloriz1, Susana San Ildefonso1, Paula Castillo1, Laurent Calvier2, Natalia Lopez-Andres1.
1Navarrabiomed, Pamplona, Spain, 2Center for Translational Neurodegeneration Research, Dallas, TX, USA.
Abstract Body:
OBJECTIVE: Reelin is a large extracellular glycoprotein that promotes atherosclerosis, a risk factor for aortic valve disease (AVD). Serum reelin mirrors the burden of vascular disease. Reelin might mediate inflammatory lymphangiogenesis. We investigated whether and how reelin is associated with AVDs.
METHODS: Reelin was studied in serum and aortic valves from patients with aortic stenosis (AS) (n=215, 59.5% men) or regurgitation (AR) (n=55, 76.36% men). In vitro calcification of human valve interstitial cells (VICs) (n = 18 donors, 50% men) was conducted for 2, 4 and 8 days as a relevant model of advanced forms of AS.
RESULTS: Serum reelin was correlated with the inflammatory and oxidative burden in AS. Expression of the RELN transcript was associated with angio/lymphangiogenesis, inflammation and osteogenesis markers only in aortic valves from AS patients, but not in AR. RELN expression was enhanced within the fibrocalcific areas of AS valves and the VIC was a cellular source of reelin along with inflammatory and valve endothelial cells. A higher expression in men agreed with a predominant presentation of calcific forms of AS. Such sex-dependent differences were reported in vitro. Calcifying male VICs had higher RELN expression than female’s and that was significantly associated with lymphangiogenesis, inflammation, and osteogenesis.
CONCLUSIONS: Valvular reelin emerges as a clinically relevant player of specific forms of AVD, with a sex-dependent contribution to the AS pathogenesis. Reelin seemingly mediates pathological mechanisms instrumental to the predominant calcific phenotypes in male stenotic AVs. Unlike for atherosclerosis, serum reelin does not mirror the valvular damage in AVDs.
Presentation Number: A17Publishing Title: A Role Of Sinus Plication To Prevent Aortic Stenosis After Bicuspid Aortic Valve Repair
Author Block: Takashi Kunihara1, Keiichi Ishiwari1, Takanori Tsujimoto1, Tomomitsu Takagi1, kosuke Saku2, Kay Maeda1, Nao Ichihara1, Akihiro Masuzawa1, Yoko Matsumura1, Michio Yoshitake1, Ryuichi Nagahori1.
1The Jikei University School of Medicine, Tokyo, Japan, 2Kurume University School of Medicine, kurume, Japan.
Abstract Body:
OBJECTIVE: Postoperative aortic stenosis after aortic valvuloplasty (AVP) for bicuspid aortic valve (BAV) is one of risk factors for recurrence. Sinus plication has emerged as promising tool to improve durability of BAV repair. However, its role on postoperative hemodynamics is still unknown. We evaluate hemodynamic differences between AVP for BAV and tricuspid aortic valve (TAV), and AVP for BAV with or without sinus plication.
METHODS: Patients with BAV (Group-B, n=42) and TAV (Group-T, n=70) undergoing AVP from 2014 to 2021 were enrolled. We also enrolled patients with BAV undergoing AVP with (Group-SP, n=14) or without (Group-NSP, n=27) sinus plication between 2018 and 2023. Mid-term outcomes and postoperative hemodynamics were compared within these groups.
RESULTS: Both 7-day and 1-year echocardiography showed higher peak/mean pressure gradient in Group-B than Group-T. When mid-term outcomes were compared within Group-B based on peak pressure gradient ≥ 20 mmHg (n=20) and < 20 mmHg (n=22), freedom from aortic regurgitation > II at 5 years was both 94.4% (p = 0.749) and freedom from reoperation was 94.4% and 100.0% (p = 0.317), respectively. Peak pressure gradient at 1 year was increased in group-NSP (19.4mmHg to 26.5 mmHg), whereas that in group-SP was decreased (17.3mmHg to 15.9mmHg) (P = 0.0036). Maximum systolic blood flow velocity at 1 year was also increased in group-NSP (2.21 m/s to 2.39 m/s), whereas that in group-SP was decreased (2.23 m/s to 1.90 m/s) (P = 0.0009).
CONCLUSIONS: AVP for BAV was associated with increased pressure gradient compared with AVP for TAV, however, peak pressure gradient ≥ 20 mmHg was not associated with inferior durability at 5 years. Sinus plication could improve hemodynamics at 1 year after BAV repair, however, its real role in improving long-term durability of BAV repair remains to be further evaluated.
Presentation Number: A18Publishing Title: Ozaki Aortic Valve Reconstruction: Our Experience
Author Block: Mohammed A. Sanad.
Mansoura University, Mansoura, Egypt.
Abstract Body:
OBJECTIVE: AV interventions achieved long durability with no anticoagulation and low risk of reoperation. Ozaki and colleagues started to publish the results in 2011. The procedure entails preserving the native annulus, extension of the coaptation zone, and enlargement of the orifice area by tricuspidization. It is a promising alternative to biological valves in low income countries.
METHODS: Our initial series includes 109 patients. Following standard median sternotomy. The pericardial patch is harvested and treated with 0.6 % glutaraldehyde solution for 10 minutes, then rinsed with normal saline. The cusps are fashioned using special template. Suturing is performed as standard. Assessment of the procedure with Trans-esophageal echo. Intermediate term Follow up was done.
RESULTS: Age ranges from 17 to 65 years. 63% of our patients were male. 20% of our patients had BAV. 50% of our patients have calcified valve, annulus and we had 2 patients with severe supravalvular stenosis. Mean CCT was 146 min. TEE results: Mean AVA 3.5, PPG 16 mmHg, MPG 7.6 mmHg, 1 case with mild AR and 2 case with trivial AR. We have only one case with suture rupture in the new Ozaki RCC. Challenging cases include undiagnosed ASD, small annulus 15 mm, small STJ 15 mm, midline pericardial tear after sternotomy, 2 huge AV mass diagnosed later as Libman Sacs endocarditis. We have minor complications in the form of 2 cases with high drainage, one case with diaphragmatic paralysis, 3 postoperative psychosis and one spontaneous pneumothorax.
CONCLUSIONS: Ozaki program was a challenge that provided a reasonable alternative for aortic valve replacement using biological valve. It is less costly. It can be applied in various pathologies. it avoids complications of anticoagulation. The technique is reproducible with a short learning curve. Patient satisfaction is obvious especially with young ages.
Presentation Number: A19Publishing Title: Upper Hemisternotomy: A Feasible And Safe Approach For Minimal Invasive Surgical Aortic Valve Replacement
Author Block: Ufuk Baldan, P Klein, R Klautz.
Amsterdam University Medical Center, Amsterdam, Netherlands.
Abstract Body:
Minimally invasive aortic valve replacement is increasingly recognized as a viable alternative to traditional surgical approaches, offering the potential for reduced recovery time and improved patient outcomes. Among the different techniques, this study identifies the upper hemisternotomy as one of the safest approaches, presenting minimal perioperative risk and being applicable across a broad patient population. Our findings indicate that this technique does not compromise procedural efficiency, as aortic clamp time and cardiopulmonary bypass duration are comparable to those of other approaches. Moreover, patient outcomes demonstrate no additional risk factors associated with this minimally invasive procedure. This analysis supports the broader adoption of this technique, emphasizing its potential to expand access to minimally invasive cardiac surgery.
The procedure is carried out with the following steps:
Marking costae and J-incision: A J-incision is made to provide optimal exposure of the surgical field.
External pacing wire and drain placement: An external pacing wire and drains is positioned substernal to avoid
Cannulation: Arterial cannulation is performed in the ascending aorta, and venous cannulation in the femoral vein.
Left ventricular vent: A vent is placed via the pulmonary artery to ensure adequate unloading.
Aortic valve excision: The aortic valve is excised under excellent visualization provided by the J-incision.
Barrel and replica sizing: Sizing is conducted with attention to both barrel and replica fit, ensuring proper placement while respecting the supra-annular valve position.
Suturing the knots: no issues with limited visibility due to the J-incision
Aortotomy closure: no issues with limited visibility due to the J-incision
External pacing wire placement: An external pacing wire is positioned following valve replacement.
Presentation Number: A20Publishing Title: Outcomes Of Valve-in-valve (viv) Transcatheter Aortic Valve Replacement (tavr) After Surgical Aortic Valve Replacement With Sutureless Surgical Aortic Valve Prostheses Perceval™: A Systematic Review Of Published Cases
Author Block: Tamer Owais.
auniversity hospitals Augsburg, Augsburg, Germany.
Abstract Body:
OBJECTIVE: Valve in Valve in transcatheter aortic valve replacment (TAVR) is a potential solution for malfunctioning surgical aortic valve prostheses, though limited data exist for its use in Perceval valves.
METHODS: searches were performed on PubMed and Scopus up to 31 July 2023, focusing on case reports and series addressing VIV replacement for degenerated Perceval bioprostheses.
RESULTS: Our analysis included 57 patients from 27 case reports and 6 case series. Most patients (68.4%) were women, with a mean age of 76 ± 4.4 years and a mean STS score of 6.1 ± 4.3%. Follow-up averaged 9.8 ± 8.9 months, the mean gradient reduction was 15 ± 5.9 mmHg at discharge and 13 ± 4.2 mmHgatfollow-up. Complications occurred in 15.7% of patients, including atrioventricular block III in four patients (7%), major bleeding or vascular complications in two patients (3.5%), an annular rupture in two patients (3.5%), and mortality in two patients (3.5%). Nocoronary obstruction was reported. Balloon-expanding valves were used in 61.4% of patients, predominantly the Sapien model. In the self-expanding group (38.6%), no valve migration occurred, with a permanent pacemaker implantation rate of 9%, compared to 5.7% for balloon-expanding valves.
CONCLUSIONS: VIV-TAVR using both balloon-expanding and self-expanding technologies is feasible after the implantation of Perceval valves; however, it should be performed by experienced operators with experience both in TAVR and VIV procedures.
Presentation Number: M1Publishing Title: Characterization Of Polycarbonate-based Polyurethane For Synthetic Mitral Valve Prostheses
Author Block: Farhad Sadeghi, Yasaman Zamani, Kaylee Lynn Bear, Arash Kheradvar.
University of California, Irvine, Irvine, CA, USA.
Abstract Body:
OBJECTIVE: Thermoplastic Polyurethane (TPU) is a high-performance medical-grade polymer widely used in implantable medical devices due to its exceptional mechanical properties. Hardness and surface morphology are critical characteristics of TPU that significantly influence its mechanical behavior and suitability as a heart valve prosthesis material. Our goal is to characterize these properties, as they are vital to the material's performance within the body.
METHODS: Two types of polycarbonate urethane resins—Chronoflex (CF) with a hardness of 65D and Carbothane (CB) with a hardness of 95A—were evaluated as potential materials for mitral valve prostheses. Films with a thickness of 150 microns were cast from these resins and characterized using tensile testing and dynamic mechanical analysis. Heart valves were then fabricated from both materials and tested in a heart valve flow simulator at varying flow rates.
RESULTS: At room temperature (22°C and 55% humidity), CF exhibited higher modulus and stiffness than CB due to its greater hardness. However, under physiological conditions (37°C and 100% humidity), the mechanical responses of the two polymers were similar. Moisture acted as a softening agent, reducing the strength and modulus of both, with a more pronounced effect on CF, leading to comparable modulus values. Hysteresis curves indicated that both materials recovered well within the elastic loading zone. Electron microscopy of cell cultures revealed that cell adhesion and growth were linked to the hard segment morphology of CF, suggesting that cells preferentially adhered to these areas.
CONCLUSIONS: The hardness of polyurethane (65D vs. 95A) significantly influenced mechanical properties at room temperature, but both polymers exhibited comparable responses under physiological conditions. Notably, cell growth was enhanced on the CF surface, with increased cell adhesion and anchorage linked to its higher hard segment content, suggesting potential advantages for mitral valve tissue engineering applications.
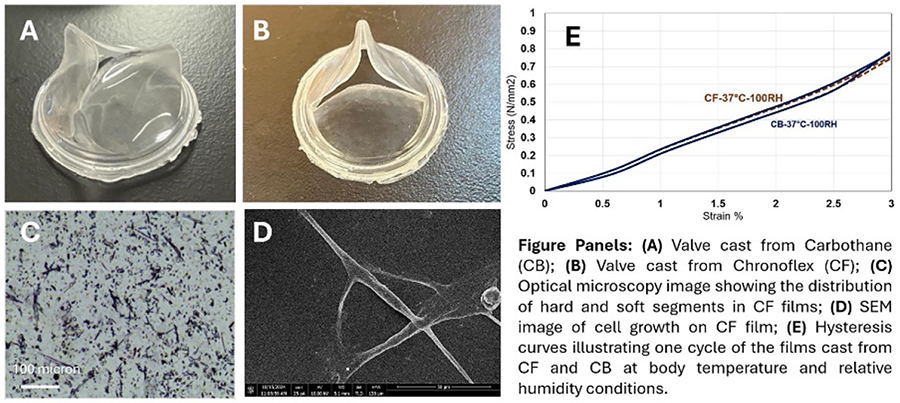
Presentation Number: M2Publishing Title: Contemporary 3-year Real-world Outcomes Following Mitral Valve Replacement With A Novel Mitral Tissue Bioprosthesis
Author Block: Denis Bouchard, Michel Pellerin, Philippe Demers.
Montreal heart Institute, Outremont, QC, Canada.
Abstract Body:
OBJECTIVE: Innovations in pericardial tissue valves are promising. Resilia bovine pericardial valves (Edwards Lifesciences) incorporate a novel tissue technology, including stable capping of free aldehydes to prevent binding with calcium. To date, mid-term outcomes of the COMMENCE trial investigating mitral valve replacement using bioprosthesis with Resilia tissue reported promising outcomes. However, the hemodynamics characteristics and potential durability of this new tissue treatment is still to be described in a real-world setting.
METHODS: A retrospective review was conducted on the first patients undergoing mitral (MVR) with the Mitris Resilia bioprosthesis between July 2021 and March 2024. Follow-up included clinical assessments and post-operative echocardiography and at follow-up. Statistical methods, including mean values and Kaplan-Meier survival curve were employed. A retrospective review was conducted among patients undergoing mitral replacement (MVR) with the Mitris Resilia ( July 2021 to March 2024). Clinical follow-up and echocardiography were recorded. Statistics, including mean values and Kaplan-Meier survival curve were employed.
RESULTS: 247 MVR patients were included. The mean age was 72.7 ± 9.3 years, and the STS predictive mortality and EuroSCORE II were 7.3 ± 6.3 and 8.7 ± 7.8, respectively. The 30-day mortality was 7.7%, while 30-day complications included 6 strokes (3.0%), 1 endocarditis (0.4%), and 2 reoperations (1%). Follow-up was 658 ± 233 days, the late mortality was 0.0 %, and the late complications included 1 stroke (0.5%), 1 endocarditis (0.5%), and 1 reoperation (0.5%). Post-operative and late mean gradient pressure ranged from 3.68 to 5.8 mmHg and 4.28 to 4.5, respectively.
CONCLUSION: This study demonstrated favorable hemodynamic and clinical outcomes in the short-term follow-up patients who underwent MVR using the novel bioprothesis. These findings highlight the potential of this new valve, particularly for difficult cases and irrepairable mitral valves. Further studies are needed and the Momentis trial, underway, will look more extensively at the long-term follow-up of these prostheses.
Presentation Number: M4Publishing Title: In-silico Multi-physics Model To Assist Biomimetic Polymeric Mitral Valve Double Component Deposition (DCD) Processing
Author Block: Ignazio Niosi1, Viktor Balashov2, Pietro Terranova2, Arianna Adamo2, Flaviana Falci1, Patrizia Caruso1, Antonio Pantano3, William Wagner4, Petra Mela5, Antonio D'Amore6.
1Università degli studi di Palermo & Fondazione Ri.MED, Palermo, Italy, 2Fondazione Ri.MED, Palermo, Italy, 3Università degli studi di Palermo, Palermo, Italy, 4University of Pittsburgh, Pittsburg, PA, USA, 5Technical University of Munich, Munich, Germany, 6Fondazione Ri.MED & University of Pittsburgh, Palermo-Pittsburgh, Italy.
Abstract Body:
OBJECTIVE: Engineering the mitral valve (MV) leaflets poses unique functional and structural challenges: leaflet asymmetry, thickness variation, and mitral dynamism render most polymer fabrication techniques ineffective. We developed Double Component Deposition (DCD) to prescribe scaffold anisotropy, fiber diameter, leaflet thickness, size, and shape. This work advances DCD with multiphysics analyses of fiber deposition mechanisms. Electrical field (EF) distribution allowed the identification of optimal surface Double Component Ratio (DCRs) for the collecting target, while fluid mechanics defined a mandrel rotation axis for anisotropic fabrication. These enhancements improved engineered MV accuracy in thickness distribution and anisotropy.
METHODS: In order to identify optimal DCRs in MV-shaped collectors, 29mm DCD targets were machined via 3D metallic/plastic printing. Electrostatic and aerodynamic simulations studied the EF distribution on the collector and air movement from MV-shaped collector rotation. Modeling results were used to calculate the full width at half centroid (FWHC) for EF distribution on three geometries with DCRs of (40, 45, 25) %. Eccentric and non-eccentric configurations were tested (Fig.1C). Thickness heatmaps of processed MVs(N=3) were obtained by averaging n=27 measurements. Functional anisotropy was quantified via biaxial mechanical testing, while structural one via Scanning Electron Microscopy, and digital image analysis (OrientationIndex (OI)=0.5_isotropic, OI=1_parallel fibers).
RESULTS: The lowest value of FWHC was obtained for DCD III (Fig. 1A), this corresponds to a more homogeneous EF. The aerodynamic simulation showed an increased symmetry in both pressure and relative airstream velocity which led to proper circumferential alignment of the fibers (Fig.1B). The engineered MV obtained with the eccentric set-up matched the desired range of thickness (400-600µm, average 525µm). Fibers anisotropy(OI=0.69) duplicated the OI=0.68 measured for native human MV(Fig.1D).
CONCLUSIONS: In this incremental study we demonstrated how DCD technology coupled with a electrostatic-aerodynamic simulation advances the level of control on structural and functional features that are considered critical in atrioventricular valve biomimicry.
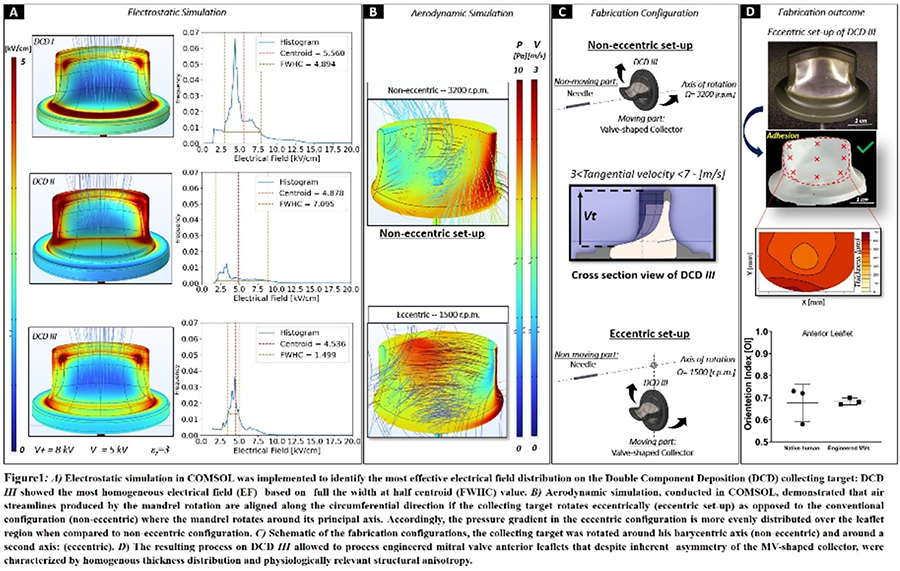
Presentation Number: M5Publishing Title: A Case Of Mitral Valve Repair For Mitral Regurgitation Due To Double Orifice Mitral Valve
Author Block: Takenori Kojima, Ryo Hirayama, Tomoya Miyamoto, Shuichi Urashita, Kenta Uekihara, Takeshi Sakaguchi, Mai Matsukawa, Ryusuke Suzuki.
Japanese Red Cross Kumamoto Hospital, Kumamoto, Japan.
Abstract Body:
OBJECTIVE: We report a case of mitral valve repair for mitral regurgitation caused by a double orifice mitral valve, a rare congenital heart anomaly, with considerations regarding preoperative diagnosis and surgical techniques.
METHODS: A 60-year-old woman presented with nocturnal dyspnea and was diagnosed with severe mitral valve regurgitation. The mitral valve had two orifices, with regurgitation noted from one of them. We performed mitral valve repair with artificial chordae and prosthetic ring using a minimally invasive right anterior minithoracotomy approach.
RESULTS: Postoperative echocardiography showed well-controlled mitral regurgitation without signs of mitral stenosis, and the valve orifice area was preserved.
Transesophageal echocardiography with 3D imaginag is recommended for preoperative diagnosis; however, diagnosis is also possible with transthoracic echocardiography if abnormalities in the subannular apparatus of the mitral valve are understood.
In surgery, while repair can be performed based on the same principles as standard mitral valve reconstruction, repairing the smaller orifice is more challenging when there is a size discrepancy between the orifices. In addition, it is also important to avoid postoperative mitral stenosis.
CONCLUSIONS: We successfully performed mitral valve repair for mitral regurgitation caused by a double orifice mitral valve, achieving favorable results. Understanding abnormalities in the subvalvular apparatus contributes to an accurate preoperative diagnosis. It is essential to perform the reconstruction in a manner that avoids postoperative mitral stenosis.
Presentation Number: M7Publishing Title: Robotic Mitral Valve Repair For Anterior Prolapse Made Easier
Author Block: Marc Gillinov, Tarek Malas.
Cleveland Clinic, Cleveland, OH, USA.
Abstract Body:
OBJECTIVE: To demonstrate a simplified approach to correction of anterior prolapse in robotic mitral valve repair.
METHODS: The video demonstrates a technique for correction of anterior leaflet prolapse utilizing pre-knotted, pre-measured, free-hand artificial chordae. A pre-knotted PTFE suture is passed through the free edge of the anterior mitral leaflet such that the knot engages the leaflet. The needle is then passed through the papillary muscle in a horizontal mattress fashion and supported by a felt pledget. The needle is next woven through the free edge of the prolapsing segment of the anterior leaflet, taking 2-3 passes. Chordal length is adjusted such that the free edge of the anterior leaflet can be lifted to the hinge point of the anterior leaflet at the annular level. Two sets of artificial chordae are placed: one to the medial portion of A2 and one to the lateral portion of A2. An annuloplasty completes the repair.
RESULTS: On post-repair echocardiogram, there is no residual mitral regurgitation.
CONCLUSIONS: This technique facilitates robotic repair of anterior mitral prolapse.
Presentation Number: M8Publishing Title: Rheumatic Mitral Valve Repair: “Ship Technique”: Excellent Results In Aggressive Mitral Valve Disease.
Author Block: Shipra Shrivastava1, Sandeep Shrivastava1, Shitij Shrivastava2, Shashwat Shrivastava3.
1Medanta Superspeciality Hospital, Indore, MP, India, Indore, India, 2BronxCare Health System, New York, NY, USA, 3Montefiore Medical Center, New York, NY, USA.
Abstract Body:
OBJECTIVE: To restore flexibility and functionality of the mitral commissures, improving valve area and achieving optimal coaptation of the mitral leaflets using the novel Ship Technique of commissural reconstruction.
METHODS: Mitral valve repair was performed in 125 patients at our center between January 2021 and September 2024. Among mitral repair cases, 66.4% were rheumatic in nature, with only 9.6% being degenerative, a stark contrast to Western centers where degenerative cases predominate. Mitral stenosis represented 67.5% of the cases, a rare finding elsewhere. Of the rheumatic repairs, 71% were females, and 96.4% pf patients were under 60 years of age. Hence, all of these patients were initially candidates for mechanical valve replacement. In the past two years, amongst rheumatic repairs, 66.66% of patients underwent, Ship Technique of commissural reconstruction, yielding excellent postoperative outcomes. In all patients, we closed the left atrial appendage, regardless of rhythm or left atrial size. We observed significant reduction in left atrial size and restoration to sinus rhythm in some patients, with appropriate medical therapy and cardioversion if necessary.
RESULTS: The "Ship Technique" of commissural reconstruction delivers outstanding results in treating aggressive rheumatic mitral valve disease at our center. It is effective in both mitral stenosis and regurgitation, providing a large valve area with minimal gradients and no leakage, ensuring optimal diastolic and systolic function. Strict adherence to dual rheumatic prophylaxis is maintained in these young patients. None of the patients have required repeat mitral valve intervention so far.
CONCLUSIONS: Commissural reconstruction restores the normal functioning of the mitral leaflets, enabling them to operate smoothly throughout the cardiac cycle. This technique achieves Type 1 valve function, ensures laminar blood flow, gives good valve opening, and coaptation, leading to excellent patient outcomes.
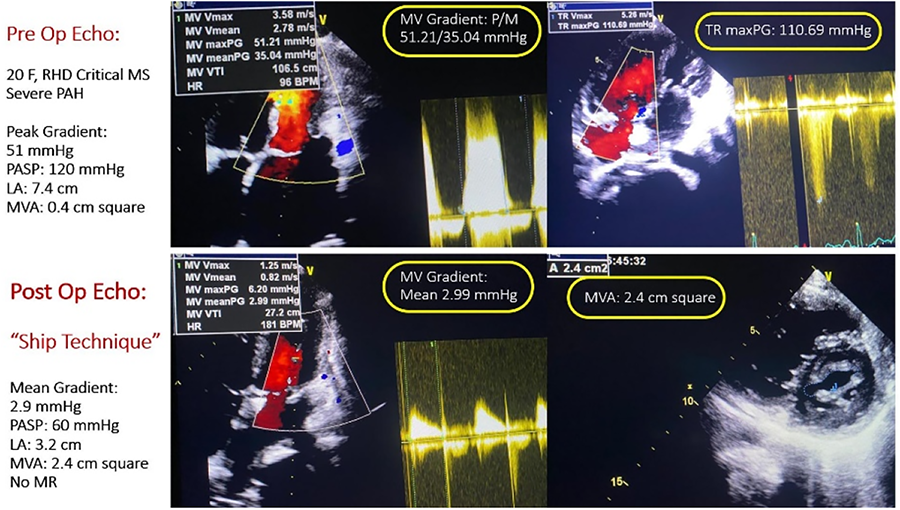
Presentation Number: M9Publishing Title: Mandrel-less Fabrication Of Biomimetic Engineered Chordae Tendineae
Author Block: Flaviana Falci1, Arianna Adamo2, Alfonso E. Castaneda Serrano3, Viktor Balashov2, Ignazio Niosi1, Pietro Terranova2, Valeria Vetri1, Giovanni Ferrari4, William R. Wagner5, Antonio D'Amore2.
1University of Palermo, Palermo, Italy, 2Fondazione Ri.MED, Palermo, Italy, 3University of Cagliari, Cagliari, Italy, 4Columbia University Irving Medical Center, New York, NY, USA, 5University of Pittsburgh, Pittsburgh, PA, USA.
Abstract Body:
OBJECTIVE: Current treatments for Chordae Tendineae (CT) replacement involve surgical repair with non-absorbable suture materials that have shown suboptimal results, particularly in replicating native chordae’s complex mechanical properties and structural integrity. To address these limitations, we introduce a novel bioengineered substitute for CT: BioChord. By employing a mandrel-less electrodeposition (MLD) technique, compatible with various polymers, we fabricate bioengineered CT that recapitulate macro- and microstructure of native CT with customizable mechanical behavior. We assessed BioChord’s regenerative capacity conducting an in vitro study to elucidate the impact of the ultrastructural cues and the mechanical conditioning on cell growth while exploring the underlying mechanisms of strain/stress signaling.
METHODS: BioChords were fabricated via MLD method (PCT/US2018/022863) (Fig.b) and compared to Human CT (HCT) in terms of structure and mechanical properties through scanning electron microscopy (SEM) and uniaxial tensile tests (UTT) (Fig.a and b). BioChords were seeded integrating NIH-3T3 fibroblasts suspension (106 cell/ml) during MDL fabrication. Cell-loaded BioChords were first cultured for 72 hours to allow cell attachment, followed by a dynamic conditioning in a bioreactor for 7 days. Histological analysis assessed fibroblast infiltration and proliferation (Fig.c).
RESULTS: SEM evaluation confirmed the ability to properly control diameter and microfiber arrangement. BioChords macro and microstructure successfully replicated the fibrous alignment of native CT, with no significant differences in Orientation Index between HCT (0.73±0.07) and BioChords (0.82±0.11). Mechanical testing showed comparable initial modulus values between BioChords (88.15±12.21 MPa) and HCT (91.05±6.28 MPa). Histology confirmed effective fibroblast infiltration after dynamic conditioning in an in vitro platform.
CONCLUSIONS: In vitro preliminary tests demonstrate that BioChords offers topological cues for enhanced cell infiltration, promoting new functional tissue regeneration while providing mechanical support, making them a promising candidate for valve repair.
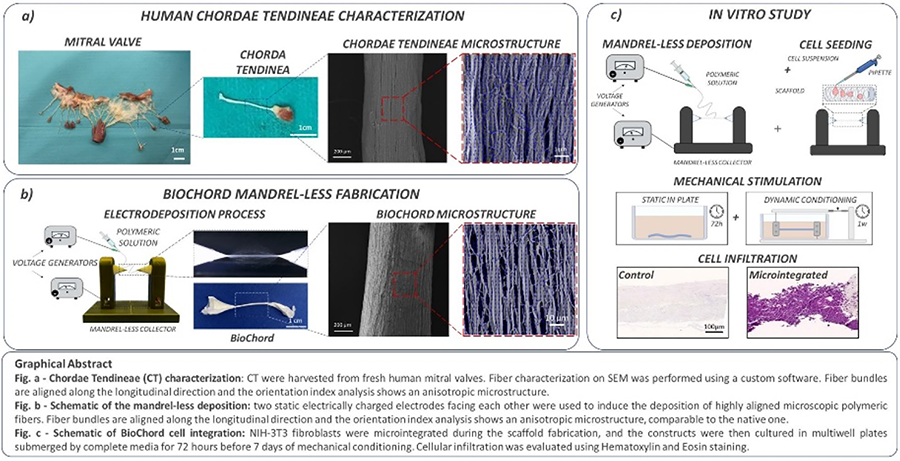
Presentation Number: M10Publishing Title: Transcatheter Mitral Valve Replacement With Tendyne. Early Spain And Portugal Experience. The Iberian Registry
Author Block: Christian Muñoz—Guijosa1, Luis Nombela—Franco2, Javier Cobiella Carnicer2, Ignasi Julia Amill3, Rui Teles4, Juan Jose Legarra5, Daniel Pereda6, Ignacio Amat7, Carlos Martin8.
1Hospital Universitario 12 Octubre, Madrid, Spain, 2Hospital Universitario Clinico San Carlos, Madrid, Spain, 3Hospital Germans Trias i Pujol, Barcelona, Spain, 4Hospital de Santa Cruz, Carnaxide, Portugal, 5Complejo Hospitalario Universitario Vigo, Vigo, Spain, 6Hospital Clínic i Provincial Barcelona, Spain, 7Hospital Clínico Universitario Valladolid, Valladolid, Spain, 8Hospital Universitario Puerta de Hierro, Madrid, Spain.
Abstract Body:
OBJECTIVE: Transcatheter mitral valve replacement (TMVR) is emerging as an alternative for patients with mitral valve disease who are not candidates for surgery or edge-to-edge repair (TEER). This study aims to evaluate the short- to mid-term procedural success and safety outcomes.
METHODS: This prospective registry included consecutive patients with symptomatic mitral disease who underwent TMVR using the transapical Tendyne* (Abbott) system at seven centers across the Iberian Peninsula between December 2020 and June 2022. Clinical data, cardiovascular imaging evaluations, procedural details, and follow-up assessments at one and twelve months were collected.
RESULTS: A total of 40 patients (mean age 78.5 years [IQR 76-82], 47.5% male) underwent TMVR. Most had significant surgical risk, comorbidities, and advanced functional class. Of the patients, 38 had mitral regurgitation (MR) and 2 had severe mitral stenosis. Prior mitral valve intervention and off-label implantation were present in 4 (10%) and 8 (20%) patients, respectively. Technical success was achieved in 100%, device success in 95%, and procedural success in 85% at 30 days. All-cause mortality was 2.5% at 30 days and 17.5% at one year. Reduction of MR to ≤1 and improvement in NYHA functional class to I-II were observed in 90.9% and 89.9% of survivors at one year, respectively.
CONCLUSIONS: TMVR demonstrated durable resolution of mitral valve disease and significant functional improvement at one-year follow-up. The procedure showed a satisfactory short-term safety profile. However, one-year mortality remained relatively high in this elderly, high-risk population.
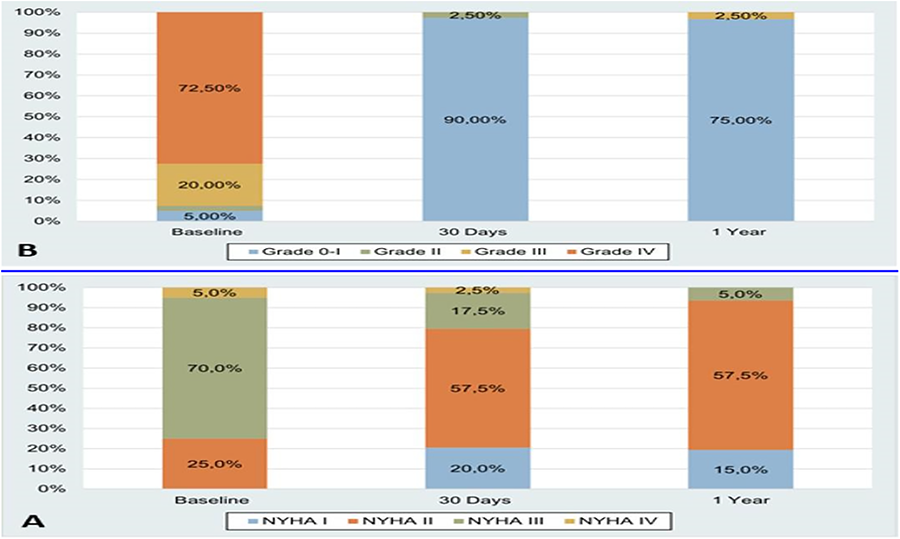
Presentation Number: M11Publishing Title: A Novel Bioprosthetic Mitral Valve For Valve Augmentation - Ovine Studies
Author Block: Hugh Stewart Paterson1, Dominic K. Ng2, Fiona C. Schnitzler1, Laurencie M. Brunel1, Mariko Yata3, Konstantin Yastrebov1, Lisa M. Partel1, Benjamin M. Robinson2, Paul G. Bannon1.
1The University of Sydney, Camperdown, Australia, 2Royal Prince Alfred Hospital, Camperdown, Australia, 3The University of Sdyney, Camperdown, Australia.
Abstract Body:
OBJECTIVE: To determine the extent of benefit of mitral valve augmentation with a novel asymmetric atrialised mitral bioprosthetic valve designed to allow full retention of the native valve without the risk of outflow tract obstruction.
METHODS: A novel mitral bioprosthetic valve was inserted in 6 normal sheep terminal studies using 3 techniques with complete retention of the native mitral valve. (1) Supra-annular (vertical mattress sutures), (2) intra-annular (horizontal mattress), and (3) intra-annular mal-rotated (a bioprosthetic stent post under the retained anterior leaflet (AML)). Releasable plication snares were placed around the AML and P3 chordae. A conductance catheter measured haemodynamic and contractility parameters, and a pulmonary artery flow probe measured cardiac output. Echocardiography demonstrated mitral valve function.
RESULTS: Supra-annular. The distance between the native and bioprosthetic valve coaptation points was 10mm with unrestricted native leaflet movement and normal trans-mitral flow. Intra-annular. There was unrestricted AML movement but partially restricted posterior leaflet movement. Plication of the AML was associated with impaired haemodynamic and contractility parameters (cardiac output 4.5%, systolic blood pressure 4.2%, stroke volume 6.6%, stroke work 15%, and independent contractility 9.6%, and an increase in ventricular end diastolic pressure 8.2%). With fixed plication of the P3 segment causing gross native valve incompetence prior to AML plication, the adverse effects in response to AML plication did not occur. Intra-annular mal-rotated. There was restricted movement of the AML by a prosthetic stent. In this situation, plication of the AML was not associated with haemodynamic or contractility changes. There was no evidence of left ventricular outflow tract obstruction with any technique.
CONCLUSIONS: AML movement supports left ventricular function but this is dependent upon a pressure gradient across the AML. A novel asymmetric bioprosthesis may augment a native mitral valve with functional regurgitation, preserving ventricular function without the risk of outflow tract obstruction
Presentation Number: M12Publishing Title: Papillary Muscle Approximation And Relocation Alter Ventricular Geometry But Not Contractility In A Normal Ovine Heart
Author Block: Hugh Stewart Paterson1, Dominic K. Ng2, Fiona C. Schnitzler1, Laurencie M. Brunel1, Mariko Yata1, Konstantin Yastrebov1, Lisa M. Partel1, Benjamin M. Robinson1, Paul G. Bannon1.
1The University of Sydney, Camperdown, Australia, 2Royal Prince Alfred Hospital, Camperdown, Australia.
Abstract Body:
OBJECTIVE: The mitral subvalvular procedures of papillary muscle approximation (PMA) or relocation by shortening the papillary annular distance (PAS) as adjuncts to annuloplasty for ischaemic mitral incompetence have improved outcomes compared to annuloplasty alone. The direct effects of these procedures on left ventricular function have not been determined.
METHODS: Adult sheep (PMA=5) and (PAS = 8) underwent left atriotomy and insertion of papillary muscle sutures to allow reversible and repeatable interventions on the normal beating heart. PMA: A pledgetted propylene suture passed through both papillary muscles and a trans-mural snare. PAS: A neochordal loop measured to the length of the ipsilateral anterior leaflet marginal chordae was attached 4mm below the tip of each papillary muscle. A propylene suture attached to the free end of the loop passed through the annulus at each ipsilateral trigone and immediately exited through the left atrial roof. Sonocrystals were attached to the trigones and papillary muscles. Haemodynamic and left ventricular contractility parameters were recorded immediately before and after each intervention. Echocardiography and intra-cardiac sonomicrometry data measured the effect of the interventions.
RESULTS: The haemodynamic parameters of systolic pressure, cardiac output, stroke volume and stroke work all decreased with both PMA and PAS but without changes in ventricular filling pressure or the independent measurements of ventricular contractility. PAS shortened the papillary trigonal distance by 4.58+0.65mm.
CONCLUSIONS: Both PMA and PAS cause an alteration in left ventricular geometry resulting in an immediate decrease in haemodynamic parameters but without changing contractility. On that basis, they are both appropriate subvalvular papillary muscle relocation techniques, albeit with different modes of ventricular geometric alteration. The anterior leaflet marginal chordal length can be used to determine the normal papillary-trigonal distance.
Presentation Number: M13Publishing Title: Tissue Engineering Models For Mitral Valve Calcification
Author Block: Agneta Simionescu, Joshua Wingold, Collin Owens, Dan Simionescu.
Clemson University, Clemson, SC, USA.
Abstract Body:
OBJECTIVE: Due to its structure, a discontinuous rim of fibrous tissue periodically interrupted by fat, the posterior annulus of the mitral valve is susceptible to degenerative calcification under conditions that increase the oxidative and mechanical stress on the mitral valve: hypertension, hyperglycemia, elevated triglycerides, and chronic inflammation. Mitral annulus calcification (MAC) is an active and regulated process of injury, and lipid deposition with spots of early mineralization, inflammation, and bone formation.
METHODS: We investigated the cell and extracellular matrix modifications in MAC, using tissue engineered mitral valves (TEMVs) mounted in bioreactors and compare with swine animal models.
RESULTS: TEMVs exhibited reduced orifice area after 2 weeks in bioreactor; cells expressed alpha-smooth muscle actin and osteocalcin and stained positive for Alizarin Red. Biaxial mechanical testing showed increased stiffness in the circumferential direction. The mitral valve annulus from swine models also showed signs of calcification and activated valvular cells.
CONCLUSIONS: Modifications in mitral valve annulus leading to calcification could be evaluated in 3D dynamic tissue engineering models that mimic the mechanical and biochemical environment of the valve.
Presentation Number: M14Publishing Title: Surgical Repair Of Isolated P2 Prolapse In A Single Institution; Comparison Between Resection And Artificial Chorda Reconstruction
Author Block: Tomohito Nakashima, Yusuke Yaku, Umpei Okamoto, Tatsuro Gondai, Kaichiro Manabe, Takuma Kobayashi, Hidetake Kawajiri, Satoshi Numata, Shinichiro Oda.
Kyoto Prefectural University of Medicine, Kajii-cho, Kamigyo-ku, Kyoto-city, Japan.
Abstract Body:
OBJECTIVE: The purpose of this study is to evaluate the feasibility of artificial chorda reconstruction for isolated posterior leaflet prolapse.
METHODS: We evaluated both the early and long-term outcomes between the group underwent resection and suturing (Group R) and the group underwent reconstruction using artificial chordae (Group A). Additionally, we examined the recurrence rate of more than moderate mitral regurgitation and the reoperation-free rate.
RESULTS: From 2010 to 2023, 107 cases of mitral valve repair for isolated P2 prolapse were performed at our institution. Group A consisted of 36 cases, and Group R consisted of 71 cases. There was no significant difference in the mean age between the two groups (A: 66.2 years, R: 61.8 years, p=0.1). Preoperative echocardiography including LVDd (A: 53.7 mm, R: 53.1 mm, p=0.70), and EF (A: 65.5%, R: 64.0%, p=0.41), showed no significant differences. No operative mortality was observed in either group. The predischarge echocardiography showed 1 case of residual moderate MR in each group. There was no significant difference in the mean pressure gradient across mitral valve between the two groups (A: 2.3 mmHg, R: 2.0 mmHg, p=0.12). The mean follow-up period was 3.3 years for Group A and 4.5 years for Group R. More than moderate MR was observed in 1 case in Group A and 8 cases in Group R. Kaplan-Meier analysis showed no significant difference between the groups (p=0.18). No reoperations were performed in Group A, while the reoperation-free rate in Group R was 97.1% at 5 years and 93.4% at 10 years.
CONCLUSIONS: Repair of isolated P2 prolapse using artificial chordae reconstruction achieved comparable control of mitral regurgitation in early and long-term to the resection-suture technique. Further investigation of long-term outcomes is mandatory.
Presentation Number: M16Publishing Title: Starting A Robotic Mitral Valve Program: Focus On Safety And Learning Curve
Author Block: Rahul A. Bhoera1, Anton Tomšič, MD, PhD1, Maurice A. P. Oudeman, MD2, Paulien C. Hoefsmit, MD, PhD2, Reinier H. Zandbergen, MD, PhD2, Jerry Braun, MD, PhD1, Linda de Heer, MD, PhD3, Robert J. M. Klautz, MD, PhD1, Meindert Palmen, MD, PhD1.
1Leiden University Medical Center, Leiden, Netherlands, 2Amsterdam University Medical Center, Amsterdam, Netherlands, 3Utrecht University Medical Center, Utrecht, Netherlands.
Abstract Body:
OBJECTIVE: Mitral valve repair through median sternotomy is the gold standard for treatment of severe primary mitral regurgitation. Robotic mitral valve surgery is an innovative minimally invasive approach that has been introduced with the aim of reducing surgical impact on patients while preserving safety and surgical outcome. Initiation of this program is accompanied by a learning curve for the entire surgical team and experience with port-access minimal invasive mitral repair may be advantageous.
METHODS: A dedicated robotic mitral repair team in a high-volume mitral repair center with no prior experience with port-access mitral valve repair, collectively followed an extensive training program. After training and performing a prospective risk analysis in order to identify possible risks in the initiation phase, the first 9 procedures were accompanied by an experienced proctor. A total of 81 patients underwent robotic mitral valve surgery.
RESULTS: The initial repair rate was 100% and no early mortality, postoperative stroke or myocardial infarction was observed. Over time, we observed a decrease in cardiopulmonary bypass times (first 20 cases: 299 minutes vs. last 20 cases: 204 minutes), aortic cross-clamp times (first 20 cases: 184 minutes vs. last 20 cases: 136 minutes) and operating times (first 20 cases: 415 minutes vs. last 20 cases 267 minutes). At mid-term follow-up, repair rates were excellent (MR < 1+ 95%, MR < 2+ 98%).
CONCLUSIONS: A robotic mitral valve repair program can be safely implemented in a high-volume mitral valve repair center with no port-access experience and with excellent short- and mid-term results. It may be considered a valuable alternative to port-access mitral valve repair for selected patients.
Presentation Number: M17Publishing Title: Double Valve Surgery In Infective Endocarditis: Mitral Valve Replacement Versus Mitral Valve Repair
Author Block: Ufuk Baldan1, Anton Tomsic2, Meindert Palmen3, Patrick Klein1, Robert J. M. Klautz1.
1Amsterdam University Medical Center, Amsterdam, Netherlands, 2Leiden University Medical Center, Leiden, Netherlands, 3Leiden University Medical Center, Amsterdam, Netherlands.
Abstract Body:
OBJECTIVE: To provide a clinical overview of our center compared to current literature regarding patients with infective endocarditis undergoing double valve surgery, specifically examining differences in mitral valve (MV) replacement or MV repair outcomes, as well as extracorporeal circulation (ECC) and aortic cross-clamp (AoX) durations.
METHODS: A multicenter, retrospective analysis was performed from January 2016 to June 2024.
RESULTS: Out of a total of 10,966 patients, 103 patients with infective endocarditis requiring double valve surgery (aortic and mitral valves) were identified, with an in-hospital mortality rate of 11% (n=11). The cohort comprised 79 men (77%) and 24 women (23%). Among them 43 patients (42%) presented with prosthetic valve endocarditis. Of the 103 patients, 40 patients (39%) underwent MV replacement, with an in-hospital mortality rate of 15% (n=6). Median ECC duration in this group was 300 minutes (IQR 180-366 minutes), and median AoX duration was 203 minutes (IQR 148-276 minutes). Conversely, 63 patients (61%) underwent MV repair, with an in-hospital mortality rate of 8% (n=5). Median ECC duration for MV repair was 294 minutes (IQR 234-361 minutes), and median AoX duration was 206 minutes (IQR 160-254 minutes). For patients undergoing MV replacement, the mortality rate was 15% (n=6), with an median ECC duration of 300 minutes (IQR 180-366 minutes) and an AoX duration of 203 minutes (IQR 148-276 minutes). For those who underwent MV repair, the mortality rate was 8% (n=5), with median ECC and AoX durations of 294 minutes (IQR 234-361 minutes) and 206 minutes (IQR 160-254 minutes), respectively.
CONCLUSIONS: Double valve procedures demonstrate an acceptable mortality rate given limited alternative treatment options. MV repair is associated with comparable ECC and AoX durations to MV replacement while showing lower mortality.
Presentation Number: M18Publishing Title: Re-operative Cardiac Valve Surgery: Low Mortality In High-risk Procedures
Author Block: Masashi Azuma1, Salman Khaledi1, M. Abul Kashem1, Yoshiya Toyoda2.
1Lewis Katz School of Medicine, Philadelphia, PA, USA, 2Temple University Hospital, Philadelphia, PA, USA.
Abstract Body:
OBJECTIVE: Re-operative open-heart surgery is associated with an elevated mortality risk, leading to ongoing debate among surgeons about which patients are acceptable operative candidates. This study aimed to evaluate the factors impacting mortality in patients undergoing re-operative cardiac valve surgeries.
METHODS: We performed a retrospective analysis of patients who underwent re-operative aortic, mitral, and tricuspid valve surgeries at our center between 2008 and 2023. The study included patients over 18 years old with previous cardiac valve surgery history. Data were extracted from the STS database and EMR for analysis, including demographics, prior cardiac procedures, and re-operative surgical variables. Kaplan-Meier curves assessed survival with p-values generated with log-rank tests, with statistical significance defined as p < 0.05.
RESULTS: Between July 2008 and December 2023, 187 patients underwent re-operative cardiac valve surgery, including 50 aortic valve re-operations, 85 mitral valve re-operations, and 30 tricuspid valve re-operations. The aortic valve group had a mean age of 62.9 ± 14.9 years and a mean BMI of 29.2 ± 6.9. The STS predicted mortality for this group was 32.4%, but our observed 5-year mortality was 30%. The mitral valve group has a mean age of 59.2 ± 13.4 years and a mean BMI of 28.5 ± 6.5. The STS predicted mortality was 36.53%, while our observed 5-year mortality was lower at 26%. The tricuspid valve group had a mean age of 42.5 ± 14.5 years and a mean BMI of 25.8 ± 6.3. There was no statistically significant difference in mortality between the three valve re-operation groups (p=0.177).
CONCLUSIONS: Our study shows that, despite the complexity of secondary re-operations, re-operative cardiac valve replacement or repair can be performed with relatively low mortality. These findings highlight the potential for successful outcomes in well-selected patients.
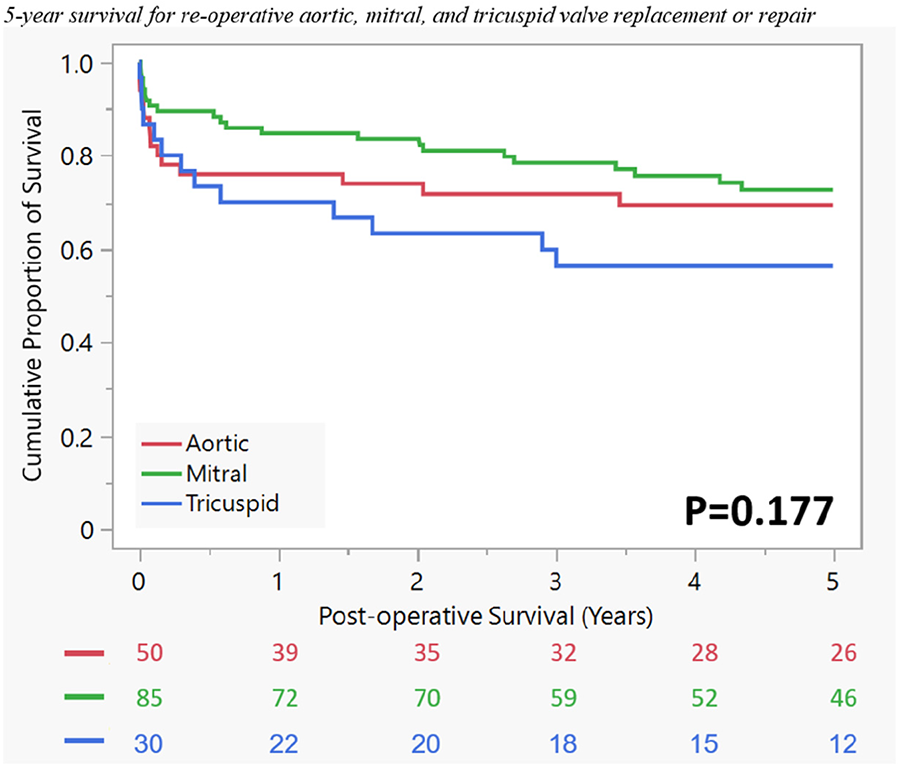
Presentation Number: M19Publishing Title: Single Institute Experience Of Suboptimal Anticoagulation Management After On-x Mechanical Mitral Valve Replacement
Author Block: Doosang Kim.
Veterans Health Service Medical Center, Seoul, Korea, Republic of.
Abstract Body:
OBJECTIVE: Prospective Randomized On-X Anticoagulation Clinical Trial (PROACT) showed the safety in reduced anticoagulation with warfarin after On-X aortic valve replacement. To show whether also feasibility in On-X mitral valve replacement with suboptimal anticoagulation management from single institute experience.
METHODS: We retrospectively observed the patients who were managed with reduced warfarin dose prescription for suboptimal INR range. 21 On-X mitral valve replacement patients were enrolled. Their follow-up INR and any hospitalization were reviewed. We compared the optimal INR range (more than 2.5) period and suboptimal INR range (less than 2.5) period.
RESULTS: Median follow-up duration was 2,252 days (75.1 months) and its range was 106 to 3,478 days (3.5 to 115.9 months). Proportion of optimal INR range period was just 17% of all follow-up period and median INR were 3.21 (range: 2.51-7.71). However, suboptimal INR range period were 83% and median INR were 1.52 (range: 0.92-2.46). During the follow-up period, there were three hospital visits (in 2 patients) for neurologic episode, two visits for management of PT prolongation, and one for GI bleeding among all 34 hospital visit episodes (The other reasons were for wound repair, ophthalmic surgery, rehab exercise, orthopedic problems, etc.).
CONCLUSIONS: Reduced anticoagulation with warfarin for suboptimal range in On-X mitral valve replacement is feasible and also safe as single institute experience.
Presentation Number: M20Publishing Title: Feasibility And Safety Of An Ultra-Fast-Track Robotic Program
Author Block: Elena Sandoval, Ignacio Morales-Rey, Francisco Javier Mancebon, M. Jose Arguis, Judith Prats, Miriam Cazalis, Albert Carramiñana, Daniel Pereda.
Hospital Clinic, Barcelona, Spain.
Abstract Body:
OBJECTIVE: We sought to investigate if an ultra-fast-track program is feasible and safe within a robotic mitral surgery program.
METHODS: An ultra-fast-track (UFT) program consisting in extubation in the operating room (OR), transfer to the recovery unit and direct transfer to the ward without intensive care unit (ICU) admission was developed and started in February 2023. Patients who were scheduled for isolated mitral repair since 02/2023 were included in the study (n=84). Patients were divided in 2 according to their UFT status. Data are presented as percentages and as median (IQR); comparisons between groups were made using the Chi-square test, the Fisher exact test or the Mann-Whitney U test, as appropriate.
RESULTS: During the study period, the UFT path had to be interrupted in 5 patients; the first patients had an episode of seizures after extubation with normal head tomography. Two patients suffered postoperative bleeding, one of them in the same OR. In one case the patient needed vasopressors for a few hours and in the last one logistics precluded to pursue the protocol. There were no significant preoperative differences between groups except for a higher prevalence of bileaflet prolapse in the UFT group (9.5 vs 30.9, p=0.02). None of the surgical times revealed any significant differences between groups. UFT group showed a higher rate of patients extubated in the OR and a shorter ICU (1 vs 0 days, p<0.0001) and hospital length of stay (3 vs 2.5 days, p=0.002). Table below summarizes the main preoperative and postoperative findings. Only two patients needed an early readmission (<30d).
CONCLUSIONS: Despite the study limitations, an ultra-fast-track program seems safe and feasible within an already stablished robotic mitral program.Further studies are needed to investigate the economical impact of this results
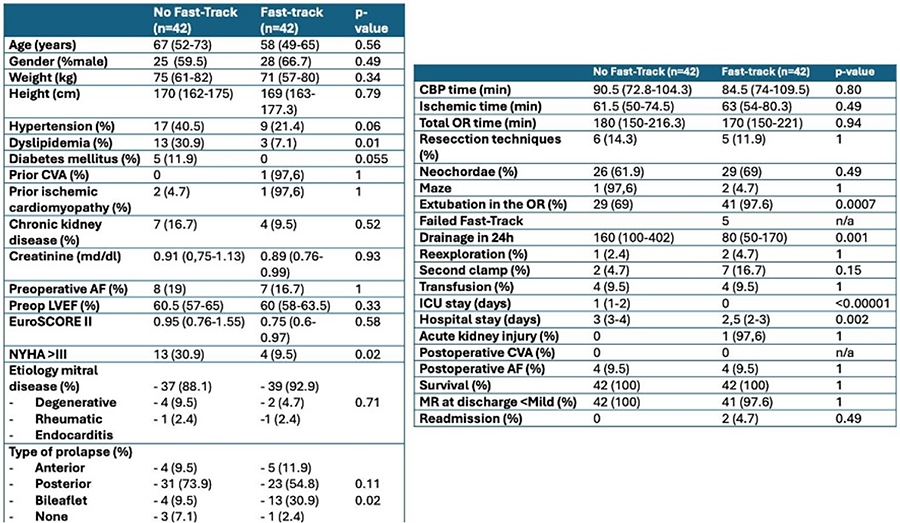
Presentation Number: H1Publishing Title: Distal Aortic Reoperation After Type A Dissection: Results From International Multicenter Registry
Author Block: Veronica Lorenz, Matteo Pettinari, Stefano Mastrobuoni, Gaby Aphram, Gebrine El Khoury, Laurent de Kerchove.
Clinique Universitaires Saint Luc, Bruxelles, Belgium.
Abstract Body:
OBJECTIVE: Data about distal aortic reoperation after type A dissection are mostly based on single center experience and often mix proximal and distal aortic reinterventions
We aimed to investigate the fate of the distal aorta after surgery for type A dissection from the ERTAAD multicenter registry.
METHODS: Data were extracted from an observational, multicenter, retrospective cohort study including 3902 patients who underwent surgery for TAAD at 18 tertiary hospitals.A total of 205 patients underwent reoperation at the level of the distal aorta. Freedom from reoperation was estimated with cumulative incidence survival and Fine-Gray competing risk regression model was used to identify independent risk factors for reoperation.
RESULTS: The median follow-up was 2.2 years (range, 0-17 years). Patients who had a distal reoperation were younger (60 vs. 65 years, p<0.01) and had higher prevalence of any malperfusion (42% vs 35%, p 0.02) at the time of dissection diagnosis. The overall incidence of distal aortic reoperation at 5, 10 and 15 years was 5.4%, 7.5% and 11% respectively. Distal aortic reoperation did not increase long term mortality. Factors associated with increased risk of distal reoperation were found to be younger age and increased abdominal aortic diameter
CONCLUSIONS: Type A aortic dissection repair was associated with a low rate of aortic distal reoperation. Younger patients and increased abdominal aortic diameter had higher risk of distal aortic reoperation. Distal aortic reoperation did not increase the risk of mortality during follow-up.
Presentation Number: H2Publishing Title: Mid-term Results Of Autograft Reinforcement By Inclusion In Dacron Graft
Author Block: Luca Zanella1, Stefano Mastrobuoni2, Gebrine El Khoury2, Laurent De Kerchove2.
1University of Bologna; Cliniques Universitaires Saint-Luc, Université Catholique de Louvain (UCL), Bologna; Brussels, Italy, 2Cliniques Universitaires Saint-Luc, Université Catholique de Louvain (UCL), Brussels, Belgium.
Abstract Body:
OBJECTIVE: The Ross procedure involves replacing the aortic valve with the patient’s pulmonary valve. Several reinforcements were described to manage autograft dilatation. This study investigates the mid-term outcomes of autograft inclusion in dacron grafts.
METHODS: Data concerning 314 Ross in adults was retrospectively gathered from 1991 to 2021: 202 free-standing roots and 112 inclusions in dacron. Cox regression was separately performed in the groups to identify predictors for mortality and autograft reintervention [Hazard Ratio (HR), Confidence Interval 95% (CI 95%)]. Kaplan-Meier method compared survival and freedom from reintervention until 10% of patients at risk remained.
RESULTS: The median follow-up was 8.85 years (Interquartile range 3.93-18.11): 12.87 years (5.78-19.31) for free-standing root; 3.9 years (0.87-6.05) for inclusion, since its introduction in 2005. The inclusion involved more treatments for aortic insufficiency and congenital malformations. In-hospital mortality was 1 case (0.5%) in free-standing and 1(0.9%) in the inclusion. Mortality risk was related to age [HR1,06 CI95% (1.02-1.11) p=0.004], diabetes [HR5,15 CI95% (1.46-18.15) p=0.011], severe kidney disease [HR10,37 CI95% (1.33-81.04) p=0.026], associated mitral surgery [HR6,65 CI95% (2.91-15.21) p<0,001]. While pre-operative aortic insufficiency and congenital malformations were risk factors for autograft reintervention in free-standing root [HR4.68 CI95% (1.61-13.62) p=0.005; HR3,21 CI95% (1,13-9,16) p=0,029], they were not for inclusion [HR2.01 CI95% (0.21-19.27) p=0.54; HR4.63 CI95% (0.65-32.94) p=0.13]. Four early reinterventions in the inclusions were related to the learning curve. Freedom from reintervention at 8 years was 95% in free-standing root and 96% in inclusion. Survival in the inclusions was excellent at 8 years (99% versus 95%). (Figure)
CONCLUSIONS: Autograft reinforcement inclusion in dacron graft was safe showing excellent survival. Despite the learning curve, reinterventions were very low. Mid-term results with inclusion were encouraging. This Ross technique became our standard in younger patients with unrepairable aortic insufficiency and annular or aortic dilatation. Further studies are required to evaluate the long-term function of autograft in dacron grafts.
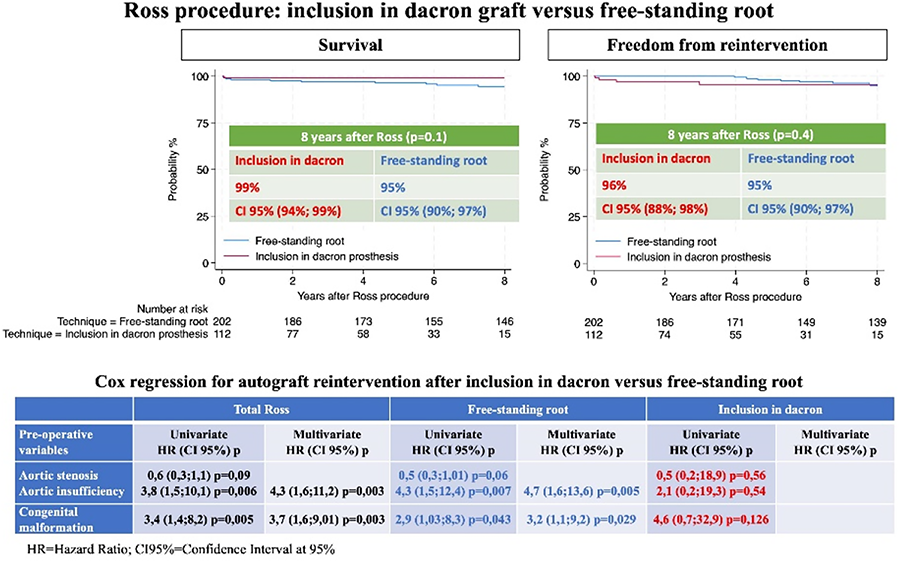
Presentation Number: H3Publishing Title: Ruptured Right Sinus Of Valsalva Aneurysm And Residual Congenital Ventricular Septal Defect Treated With Deconstructed David Valve Sparing Root Replacement
Author Block: Eric E. Roselli.
Cleveland Clinic, Cleveland, OH, USA.
Abstract Body:
OBJECTIVE: To demonstrate a novel technique for valve sparing root replacement (VSRR) that is helpful in very complex pathology such as the case presented with congenital heart and aortic disease.
METHODS: 29 y/o male with history of VSD repair as an infant and know small residual defect presented to an outside facility with severe acute heart heart failure secondary to a ruptured right sinus of Valsalva aneurysm communicating with the right ventricle, Qp:Qs of 2.5. He was optimized medically and transferred for definitive repair. He wished to avoid anticoagulation. Operation was performed via redo sternotomy with primary repair of the residual VSD under the right coronary cusp, and primary repair of the aorta to right ventricular fistula follow by valve sparing root reimplantation using a novel “deconstructed” technique.
RESULTS: Patient required veno-venous ECMO support postoperatively but was safely weaned on postoperative day 3 and discharged to home on postoperative day 14. At three months follow-up, the patient is doing well normal bi-ventricular function and no aortic insufficiency.
CONCLUSIONS: This novel technique of VSRR may help to expand the use of these operations to patients with more complex aortic root anatomy and pathology.
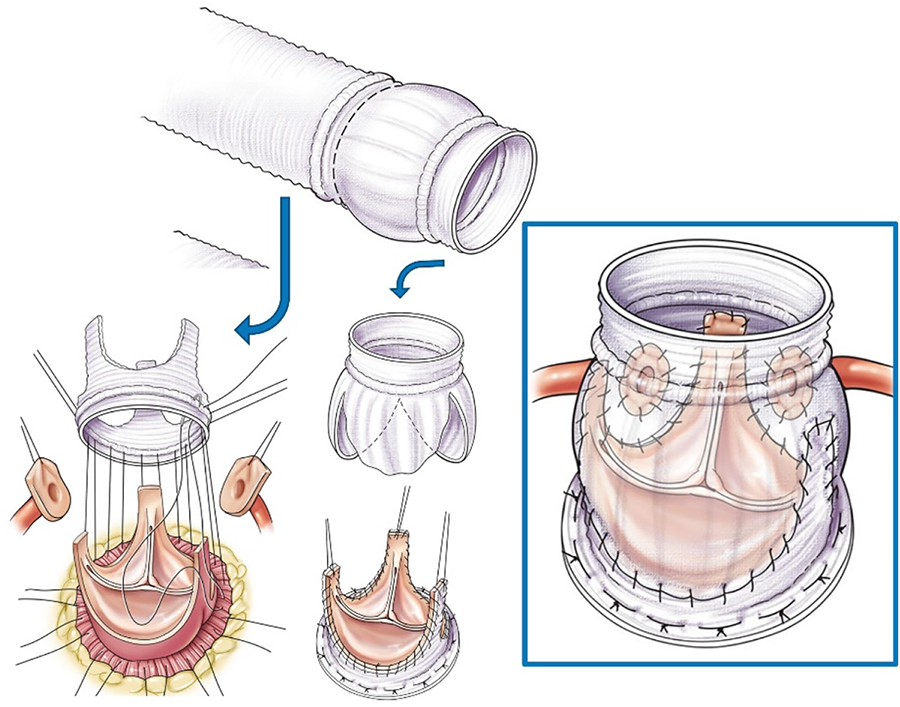
Presentation Number: H5Publishing Title: Early To Mid-term Results After Valve-sparing Root Surgery - Does Valve Morphology Affect Outcomes?
Author Block: George Gradinariu, Kezia Summers, Ahmed Shaheen, Ahmed Othman, Ayman Kenawy, Deborah Harrington, Jakub Marczak, Matthew Shaw, Manoj Kuduvalli, Mark Field, Omar Nawaytou.
Liverpool Heart and Chest Hospital, Liverpool, United Kingdom.
Abstract Body:
OBJECTIVE: To identify the short and mid-term results of valve-sparing root surgery and the impact of valve morphology on outcomes.
METHODS: The aortic valve repair program started in August 2017 in our unit. Consecutive patients undergoing valve-sparing root surgery between 2017 and 2024 were included. The primary outcome was a composite of survival, reoperation, and grade 2+ aortic regurgitation (AR) at follow-up. We also analyzed each component of the composite endpoint separately.
RESULTS: We included 334 patients with a mean age of 51±15 years. 81% (n=262) were male. Preoperative AR grade ≥2/4 was present in 64% (n=207). The aortic valve was tricuspid in 69% (n=225) and bicuspid in 31% (n=100). Most patients (90%, n=294) underwent David V reimplantation, 7% (n=24) had isolated valve repair with annuloplasty and 2% (n=7) had remodeling. Concomitant hemiarch replacement was performed in 10% (n=34) and total arch replacement in 6% (n=20). There were no early deaths. Intraoperative conversions to aortic valve replacement occurred in 3% (n=9). Median follow-up was 34 months [IQR 14-54]. Survival rates were 99%, 97%, and 96% at 1, 2, and 5 years, respectively. Valve-related reoperations were required in 1% (n=3), and freedom from significant aortic regurgitation (grade ≥3) was 99%. The composite endpoint occurred in 4% (n=14), with similar rates for tricuspid and bicuspid valves (p=0.60). Tricuspid valves had lower mean gradients than bicuspid valves (5.4 vs. 8.9 mmHg, p<0.001) measured with echocardiography during medium term follow-up.
CONCLUSIONS: Valve-sparing root surgery shows favorable short- and mid-term outcomes, with comparable results for tricuspid and bicuspid valves. Longer follow-up is necessary to confirm repair durability.
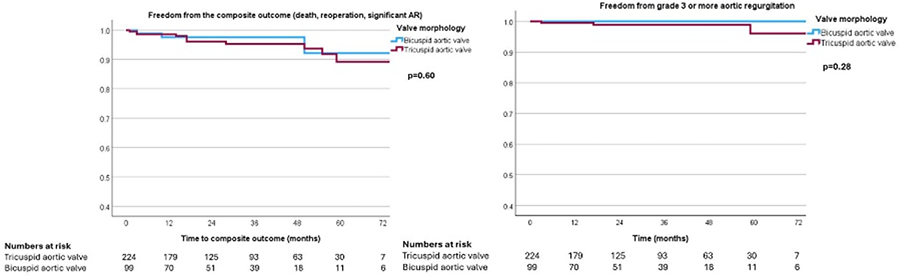
Presentation Number: H6Publishing Title: The Role Of Valve Endothelial Cells In Aortic Valve Calcification
Author Block: Daria Evensen1, Arsenii Zabirnyk2, Krizia Sagini3, Hanne Haslene-Hox4, Alicia Llorente3, Mari-Liis Kaljusto5, John-Peder Escobar Kvitting5, Kåre-Olav Stensløkken1, Jarle Vaage1.
1Section of Physiology, Department of Molecular Medicine, Institute of Basic Medical Sciences, University of Oslo, Oslo, Norway, 2Department of Research and Development, Division of Emergencies and Critical Care, Oslo University Hospital, Oslo, Norway, 3Department of Molecular Cell Biology, Institute for Cancer Research, Oslo University Hospital, Oslo, Norway, 4SINTEF, Trondheim, Norway, 5Department of Cardiothoracic Surgery, Oslo University Hospital, Oslo, Norway.
Abstract Body:
OBJECTIVE: Aortic valve calcification (AVC) is a leading cause of cardiovascular disease, affecting 25% of people over 75 years old. Valve interstitial cells (VICs) play a main role in calcification. Experimentally induced calcification in cultured VICs is a standard model to study AVC in vitro. It has been suggested that valve endothelial cells (VECs) may stimulate pro-osteogenic changes in the valve tissue. This study aimed to investigate the role and possible mechanisms of VECs in promoting calcification of VICs.
METHODS: A 2D co-culture system of human aortic VECs and VICs was established to study their interaction. In another model, extracellular vesicles (EVs) from VECs were isolated, characterized, and added to VICs. Proteomic analysis was performed on VECs from healthy and calcified valves to identify differentially expressed proteins.
RESULTS: Co-cultivation of VECs with VICs enhanced calcification in vitro compared to VICs monocultures with p value = 0.008. Addition of VEC-derived EVs to VICs undergoing experimentally induced calcification did not promote calcification. Proteomic analysis identified 3378 proteins across all samples, with 3342 proteins present in VECs from both healthy and calcified valves. Nitric oxide synthase 3 and Hedgehog-interacting protein were increased in VECs from calcified valves with p values = 0.005 and 0.002 respectively. Further bioinformatic analysis is ongoing.
CONCLUSIONS: VECs from calcified valves stimulated calcification of VICs. Extracellular vesicles did not mediate this effect. The proteomic profiles of VECs from healthy and calcified valves showed few differences. VECs may promote calcification in VICs by paracrine factors or direct cell-to-cell interaction.
Presentation Number: H7Publishing Title: In Vitro Physiological Reproduction Of A Patient-Specific Mitral Valve
Author Block: Katell Delanoë1, Erwan Salaun1, Régis Rieu2, Philippe Pibarot1, Viktoria Stanová1.
1Institut Universitaire de Cardiologie et de Pneumologie - Université Laval, Québec, QC, Canada, 2Aix-Marseille Université/ Gustave Eiffel Université, LBA-UMRT24, Marseille, France.
Abstract Body:
OBJECTIVE: To address mitral regurgitation in high-risk patients, percutaneous mitral valve treatments emerged in early 2000. Due to the novelty of these procedures, long-term hemodynamic and biomechanical consequences are still not well understood as well as the impact of patient anatomy/etiology on the device efficiency. Although both percutaneous repair and replacement are being extended to lower risk patients, there is a need for treatment individualization to improve the device's durability and the patient's quality of life. The aim of this study is to develop a patient-specific mitral valve with normal anatomy and function.
METHODS: Echocardiography images obtained during clinical examination were used to reproduce the patient's mitral valve (MV) in 3D. Then, a mold was 3D printed and MV was fabricated using a specific silicon combination that was examined in previous studies. To ensure sufficient tension, chordae were placed between silicon layers. The MV model was tested on a dual-activation simulator under the hemodynamic conditions of the patient acquired during clinical examination (Heart Rate = 70bpm, Stroke Volume = 40mL, Mean Aortic Pressure = 110mmHg). Doppler echocardiographic measurements were used to analyze hemodynamic behavior.
RESULTS: The silicon MV reproduced the patient's mitral valve anatomical characteristics successfully (Antero-Lateral Diameter=2.73+/-0.1cm vs 2.72+/-0.1cm, Commissural Diameter=3.34+/-0.1cm vs 3.34+/-0.1cm, Annulus Area=6.94+/-0.1cm2 vs 6.95+/-0.1cm2, respectively). Regarding the hemodynamic behavior, the silicone MV induced hermetic closing and parameters similar to those induced by the patient (Mean Pressure Gradient = 0.86+/-0.11 vs 0.63+/-0.11 mmHg, Geometric Orifice Area = 4.30+/-0.29cm2 vs 4.43+/-0.00cm2, respectively).
CONCLUSIONS: In vitro physiological reproduction of patient-specific MV can be a useful tool for patient-specific percutaneous procedures planning regarding patient’s anatomy, physiology, and hemodynamic profile. The next step is to develop patient-specific mitral valves with different types of pathologies and dysfunction in order to investigate, in vitro, the different potential therapeutic strategies to successfully correct these dysfunctions.
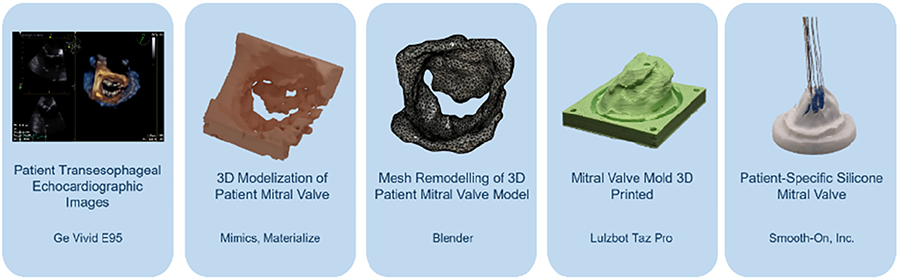
Presentation Number: H11Publishing Title: Numerical Simulation Study On The Effect Of Moving Pattern On The Dipping Manufacturing Polymer Prosthetic Heart Valve
Author Block: Haiyang Wei, Qianwen Hou, Yana Meng, Erhou Zou, Jianye Zhou.
Fu Wai Hospital, Beijing, China.
Abstract Body:
OBJECTIVE: Dip-coating technology is a manufacturing process for polymer heart valves. A more uniform thickness distribution in polymer valves helps extend their lifespan, but traditional dip-coating technique is hard to achieve even coating on the complex structure of valve leaflets. This numerical simulation study aims to explore the impact of specific moving patterns during the dip-coating process on the thickness distribution of polymer heart valves.
METHODS: A three-dimensional model of a typical tri-leaflet heart valve was established in SOLIDWORKS, and fluid dynamics simulations were performed in ANSYS Fluent with VOF (Volume of Fluid) model and EWF (Eulerian Wall-Film) model. The simulation assessed liquid flow behavior and thickness distribution under three type of movement patterns—vertical, horizontal, and circular, meanwhile each pattern undergoing rotation as well. Moving pattern parameters influencing thickness distribution were analyzed and subsequently adjusted to optimize the results.
RESULTS: The study found that different moving patterns led to distinct thickness distribution trends: the vertical pattern increased thickness non-uniformity between leaflets, with a coefficient of variation of 41.6%.; the horizontal pattern mainly affected the uniformity of individual leaflets; and the circular pattern, due to centrifugal forces, showed lower coefficient of variation compared to the vertical pattern, at 27.2%. Adjusting circular moving parameters reduced the coefficient of variation to 5.13%.
CONCLUSIONS: This numerical simulation results reveal how different moving patterns affect the thickness distribution in the dip-coating process of polymer heart valves. Strategic adjustment of moving parameters provides a scientific basis and technical pathway for optimizing valve thickness distribution, which is crucial for improving manufacturing quality
Presentation Number: H12Publishing Title: Numerical Investigation Of The Hemodynamics Of Aortic Valves And Their Surgical Treatments With A Focus On Fluid-Structure Interaction Mechanisms
Author Block: Tom Fringand1, Loic Mace2, Isabelle Cheylan1, Marien Lenoir2, Julien Favier1.
1M2P2, CNRS, Centrale Marseille, Aix Marseille Univ, Marseille, France, 2Department of Cardiac Surgery, La Timone Hospital, APHM, Aix Marseille Univ, Marseille, France.
Abstract Body:
OBJECTIVE: Demonstrate for aortic valve replacement the potential of numerical methods in daily clinical practice to predict and optimize procedures based on hemodynamics criteria. The long-term goal being to improve patient-specific considerations and outcomes.
METHODS: A novel fluid-structure interaction solver is introduced based on the Lattice Boltzmann Method for blood flow simulation and the Finite Element Method to calculate valve deformations. This solver is completed by an innovative process using landmark interpolation to obtain improved valve segmentation quality. The complete workflow is applied to a patient with aortic stenosis to determine the optimal replacement solution by comparing the quality of flows produced between a bioprosthetic valve and a neocuspidization procedure.
RESULTS: The numerical model provides meaningful results consistent with existing literature, accurately simulating physiological dynamics across a range of criteria. It also identified specific features, such as fluttering in the neocuspidization leaflets or increased velocity and wall shear stress in the bioprosthetic valve.
CONCLUSIONS: Numerical methods offer promising potential to predict outcomes of various valve replacement scenarios, providing surgeons valuable hemodynamics insights to inform and optimize patient-specific interventions before surgery.
Presentation Number: H13Publishing Title: Patient-Reported Outcomes Are Underutilized In Valvular Cardiac Surgery Randomized Clinical Trials: A Scoping Review
Author Block: Kenza Rahmouni1, Sami Aftab Abdul2, Nora Driscoll Szabo2, Nicole Hryciw2, Pierre Voisine1.
1University of Ottawa Heart Institute, Ottawa, ON, Canada, 2School of Epidemiology and Public Health, University of Ottawa, Ottawa, ON, Canada.
Abstract Body:
OBJECTIVE: The importance of patient-reported outcomes (PROs) in clinical trials is increasingly recognized. However, there is a paucity of knowledge on the extent to which PROs are incorporated and adequately reported in the cardiac surgery literature. This study aims to establish the proportion of recent randomized controlled trials (RCTs) in adult valvular cardiac surgery that include PROs and to evaluate the completeness of PRO reporting in these studies.
METHODS: A scoping review was conducted searching MEDLINE, EMBASE and Cochrane Central. Studies were eligible for inclusion if they were RCTs in cardiac surgery comparing valvular operations in adult patients (≥ 18 years old), and published between January 2014 and February 2024. Studies comparing valve surgeries to transcatheter procedures were excluded. RCTs including PROs as an endpoint were evaluated for completeness of reporting according to the Consolidated Standards of Reporting Trials (CONSORT) PRO guidelines.
RESULTS: Of the 51 trials included, one-third (31.4%) incorporated PROs (Figure 1). The most commonly reported PRO measure was the EuroQoL 5 dimensions (EQ-5D; 36.7%). Most PRO measures (73.3%) used were generic rather than disease-specific, and the majority were secondary endpoints (80.0%). Completeness of reporting in reference to the CONSORT-PRO guidelines was limited. Overall, only 7 of 14 trials reported 50% or more of the relevant CONSORT-PRO specific items. No studies met all reporting criteria. Quality of life was the PRO domain most frequently evaluated.
CONCLUSION: In this scoping review, the use of PROs in valvular cardiac surgery RCTs was low and PRO reporting was incomplete in reference to the CONSORT-PRO recommendations. Reported PROs primarily focus on quality-of-life measures, potentially missing other important domains relevant to designing patient-centered trials. The results of this study highlight the need for improvement in PRO incorporation and reporting in valvular cardiac surgery trials.
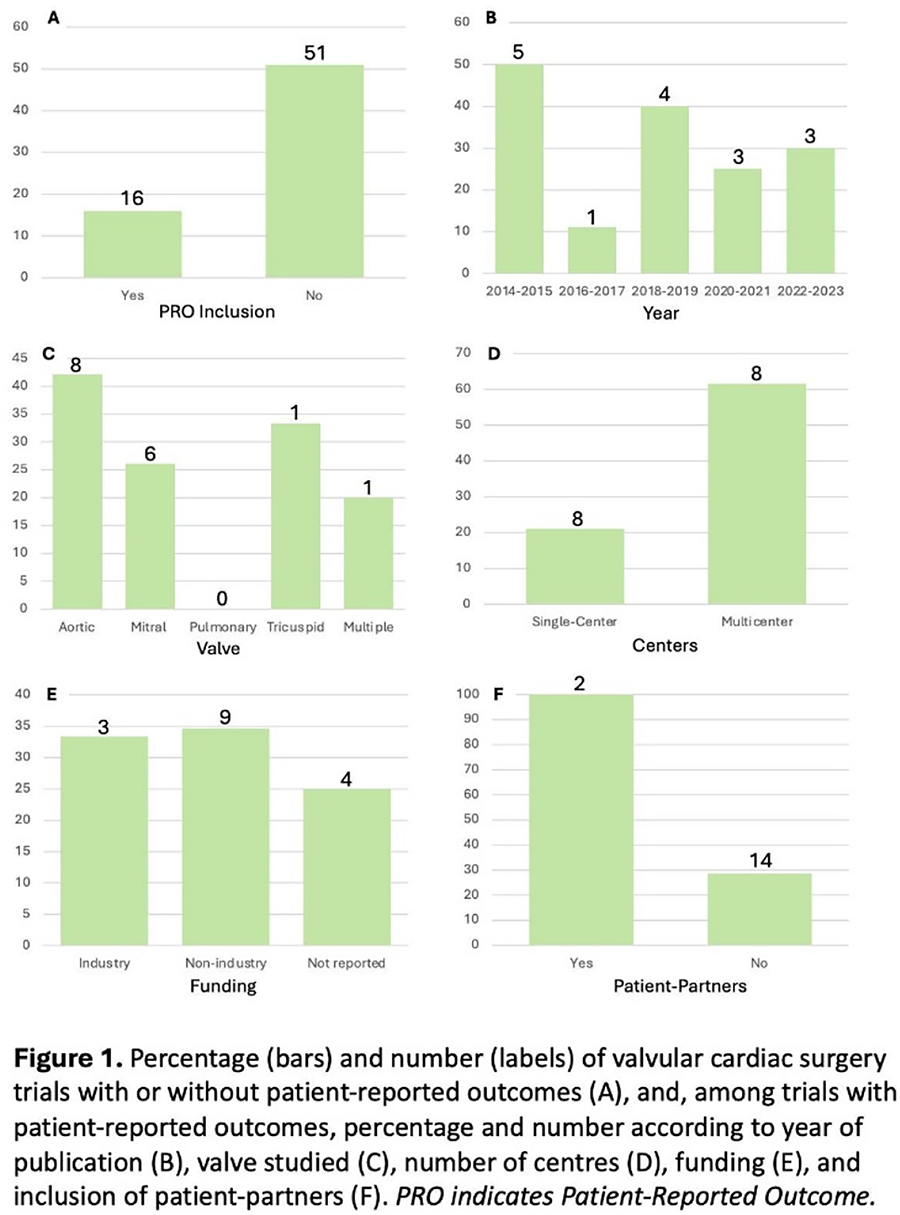
Presentation Number: H14Publishing Title: Cross-cultural Adaptation Of The Dutch Version Of The Heart Valve Disease Impact On Daily Life Questionnaire: An Interim Report
Author Block: Carlijn C.E.M. van der Ven1, Hajar Bofarid1, Kevin M. Veen1, Sabrina Siregar1, Kátia M. Padilha2, Maria-Cecilia B.J. Gallani3, Johanna J.M. Takkenberg1.
1Department of Cardiothoracic Surgery, Erasmus University Medical Center, Rotterdam, Netherlands, 2Faculdade de Enfermagem, Universidade Estadual de Campinas, Campinas, Brazil, 3Faculty of Nursing, Université Laval; Quebec Heart and Lung Institute Research Centre-UL, Quebec City, QC, Canada.
Abstract Body:
OBJECTIVE: The Heart Valve Disease Impact on Daily Life (IDCV) questionnaire is adisease-specific patient-reported outcome measure (PROM) designed to assess theimpact of heart valve disease (HVD) on patients’ daily lives. Currently, the IDCV exists only in Brazilian-Portuguese, limiting its global use. This study describesthe cross-cultural adaptation of the IDCV tool for the Dutch surgical cohort of patients with HVD.
METHODS: The IDCV consists of two parts with 14 items each: part A measures the perceivedimpact of HVD on health-related quality of life, while part B determineswhether patients experienced those impacts positively or negatively (Figure 1A). The cross-cultural adaptation followed five stages (Figure 1B). Contentvalidity was assessed by evaluating the level of agreement among experts in theexpert committee across five areas (semantic, idiomatic, experiential, consequential and total agreement) using a 4-point Likert scale. This produced a Content Validity Index (CVI) at both item (I-CVI) and scale levels (S-CVI), generating a pre-final version of the questionnaire, the Modified IDCV.
RESULTS: Atinterim analysis, forward translation, backward translation and review by anexpert committee were completed (Figure 1B). Several items initially failed toreach content validity (I-CVI < 0.78 and S-CVI < 0.90), mainly due to disagreements in idiomatic equivalence, and were revised. After adjustment, the Modified IDCV reached excellent content validity across all five areas (I-CVI and S-CVI of 1.00).
CONCLUSIONS: The Modified IDCV was constructed with excellent content validity. As part of the ICHOM standardized set of Patient-Centered Outcome Measures for HVD, thecross-cultural adaptation of the IDCV questionnaire is an important step toward implementing meaningful PROMs for patients with HVD and facilitates global outcome standardization. In a future study, the Modified IDCV will be used for pretesting, involving cognitive interviews with 30 patients scheduled foraortic or mitral valve surgery at Erasmus University Medical Center.
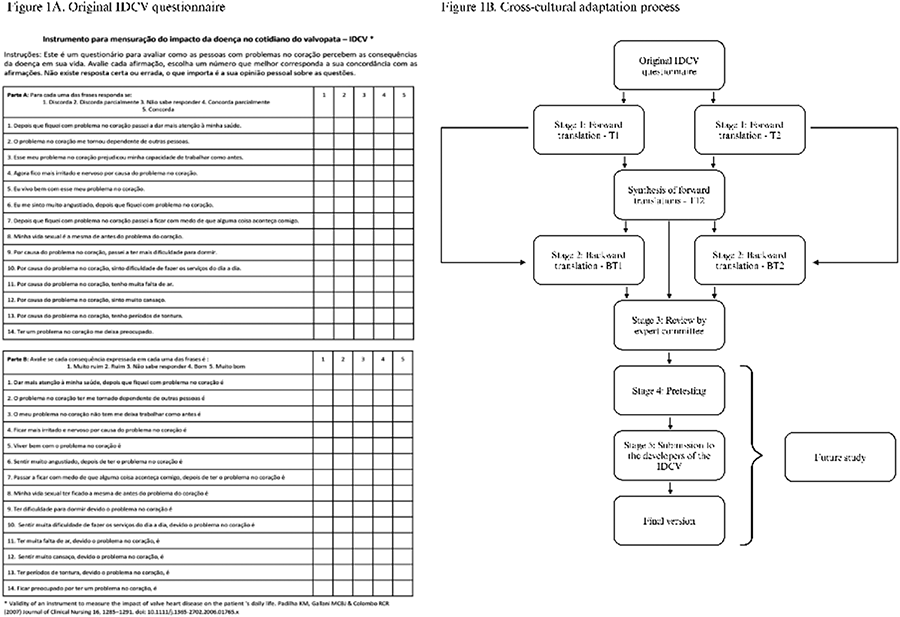
Presentation Number: H15Publishing Title: Thrombocytopenia After Implantation Of Sutureless Valves: An Unexplained But Temporary And Benign Phenomenon
Author Block: Marie Van den Bosch, Julie Van Durme, Marie Lambergits, Filip Rega, Peter Verbrugghe, Bart Meuris.
Cardiac Surgery, University Hospitals Leuven, Leuven, Belgium.
Abstract Body:
OBJECTIVE: The sutureless Perceval valve, used in aortic valve replacement (AVR), offers shorter cross-clamp times and facilitates minimally invasive surgery. However, postoperative thrombocytopenia has been reported. This study investigates the occurrence and extent of thrombocytopenia in a large, all-comers cohort receiving a Perceval valve.
METHODS: A retrospective study included 1030 patients who received a Perceval valve between May 2009 and February 2022. Three subgroups were created: Perceval S initial period (2009-2016; n=390), Perceval S second period (new sizing method; 2017-2019; n=481), and Perceval Plus (2.0 version; 2020-2022; n=159). Platelet counts from preoperative day to postoperative day 9 were retrieved from the UZ Leuven database. Thrombocytopenia was classified as mild (<150,000/μL), moderate (<99,000/μL), or severe (<50,000/μL). Statistical analysis included means ± SD for continuous variables, percentages for categorical variables, and repeated measures ANOVA with multivariate logistic regression (Statistica 14.0).
RESULTS: The mean age was 78 years, with 517 (50.1%) females, and mean EuroSCORE II of 6.1 ± 6.5. Combined surgery (CABG and/or multiple valves) occurred in 53%. Of the 1030 patients, 29.1% developed mild, 52.9% moderate, and 10.3% severe thrombocytopenia. The lowest platelet counts occurred on days 3-4 postoperatively, with none below 10,000/μL. By day 9, platelet counts increased to 210,000 ± 124,000/μL (vs 233,000 ± 72,000/μL preoperatively). Forty-three patients (4.2%) required revision for bleeding, though early postoperative platelet count was not a predictive factor. Platelet transfusions were administered to 5.5%. Female gender (p=0.04), cross-clamp time (p=0.04), and age (p=0.07) were key determinants of thrombocytopenia. No differences were found between the three cohorts over time.
CONCLUSIONS: Postoperative thrombocytopenia is common after Perceval sutureless valve implantation, but typically mild. Severe thrombocytopenia occurs in only 10% of cases and does not significantly increase bleeding rates. A conservative, watchful-waiting approach is recommended. The cause remains unknown, but does not affect morbidity or mortality.
Presentation Number: H16Publishing Title: Outcomes Of Transcatheter Pulmonary Valve Implantation To Treat Right Ventricular Outflow Tract Dysfunction Following The Ross Procedure
Author Block: Bana Samman, MSc1, Amine Mazine, MD, PhD1, Lee Benson, MD2, Jennifer Chung, MD, MSc3, Mark Osten, MD3, Maral Ouzounian, MD, PhD3, Eric Horlick, MD3.
1University of Toronto, Toronto, ON, Canada, 2The Hospital for Sick Children, Toronto, ON, Canada, 3Toronto General Hospital, Toronto, ON, Canada.
Abstract Body:
OBJECTIVE: Transcatheter pulmonary valve implantation (TPVI) offers a minimally invasive treatment option for right ventricular outflow tract (RVOT) dysfunction after the Ross procedure. Given the paucity of data regarding its clinical outcomes, we reviewed the safety, efficacy, and durability of TPVI in this context.
METHODS: This retrospective observational study was conducted at a tertiary academic centre. We identified all adult patients who underwent TPVI following a previous Ross procedure. Data collection included demographics, indications for TPVI, procedural details, and pre- and post-procedural echocardiography and right heart pressures. Outcomes assessed included technical success, changes in pressure gradients across the right ventricle to pulmonary artery (RV-PA) conduit, complications, and follow-up echocardiography.
RESULTS: Between 2009 and 2024, 162 patients underwent TPVI. Of these, 20 (80% male) had previously undergone a Ross procedure. Median age at index TPVI was 36 (IQR 24-56) years. Median interval from Ross procedure to index TPVI was 19 (IQR 5-24) years. Primary indications were conduit stenosis (n=14, 70%), regurgitation (n=4, 20%), or both (n=2, 10%). Technical success was achieved in 19 (95%) cases. One case was converted to a surgical pulmonary valve replacement due to valve embolization in the RVOT. Procedural hemodynamics showed a decrease in peak-to-peak RV-PA gradient from 34±16 mmHg to 9±6 mmHg (p<0.00001) and systolic RV-systemic pressure ratio from 0.6±0.1 to 0.4±0.1 (p<0.0001). No patient experienced major adverse cardiovascular events or clinically significant pulmonary valve regurgitation post-procedure. At a median of 23 (IQR 2-39) months, 19 patients were alive, and one had required reintervention via balloon valvuloplasty.
CONCLUSIONS: This study demonstrates that TPVI is a safe and effective intervention—with promising mid-term outcomes—for failing RV-PA conduits. Routine transcatheter treatment of RVOT dysfunction may further favour use of the Ross procedure by offering a minimally invasive strategy to address one of its main limitations.
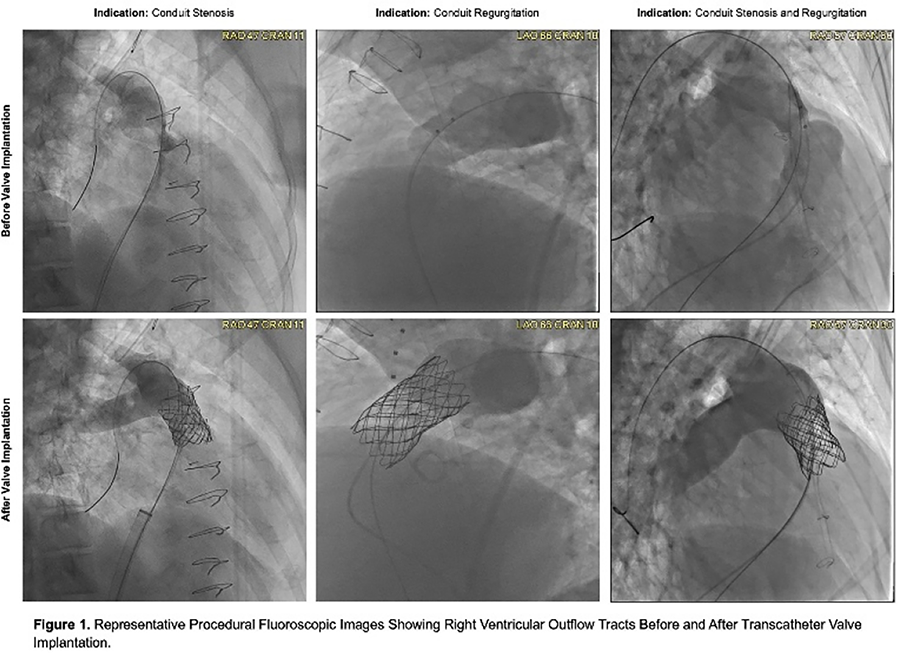
Presentation Number: H17Publishing Title: Quadruple Valve Replacement In A Patiemt With Metastatic Neuroendocrine Tumor
Author Block: Chand Ramaiah.
Ascension Saint Thomas, Franklin, TN, USA.
Abstract Body:
OBJECTIVE: Carcinoid syndrome affecting heart valve disease is rare. All 4 heart valve dysfunction from carcinoid is extremely rare. Here is a report of a case of successful quadruple cardiac valve replacement due to carcinoid.
METHODS: 55 y/o male with metastatic neuroendocrine tumor liver found to have severe regurgitation involving all cardiac valves. His cancer was in reportedly in remission after chemotherapy and embolization of liver masses. He was admitted to the hospital with heart failure exacerbation twice in 3 months period and not responding to diuretic therapy. He had moderate LV and RV dysfunction. With no other viable therapy, patient elected to proceed with high risk surgery.
RESULTS: After optimization as an inpatient for few days he underwent Aortic valve replacement with a 25 mm pericardial valve, Pulmonic valve replacement with a 23 mm pericardial valve, Mitral valve replacement with 29 mm Porcine valve and Tricuspid valve replacement with 31 mm porcine valve. Surgery was long with CPB time of 229 minutes and cross clamp time of 150 minutes. Intra aortic balloon pump was placed and required moderate doses of pressors and inotropes to separate from CPB. Left chest open with negative pressure dressings. Reoperated for due bleeding 12 hours later. Sternum closed 3 days later and bilateral moderate sized hemothorax evacuated. Extubated a few days later and discharged to rehab facility 4 weeks after surgery. His Liver and kidney function remained normal after surgery. He is alive and well with no recurrence of cancer and normal LV and RV function at 6 years.
CONCLUSIONS: Carcinoid involvement of all 4 valves is rare. Only a few cases rare reported in the literature with successful quadruple valve replacement surgery. With proper patient selection and peri-operative care procedure can be done with good results.
Presentation Number: H18Publishing Title: Identification Of Serum Markers To Predict Post-operational Atrial Fibrillation In Patients With Aortic Stenosis.
Author Block: Eva Jover, Oscar Alcalde, Rafael Sadaba, Natalia Lopez-Andres.
Navarrabiomed, Pamplona, Spain.
Abstract Body:
OBJECTIVE: Post-operative atrial fibrillation (POAF) is the commonest complication after cardiac surgery occuring in 40% of surgical valve replacements, consistently impacting morbimortality rates and financial liability. Drawing conclusions from biomarker studies is limited by the heterogeneity of POAF cohorts (e.g., coronary and valvular patients). We sought to identify whether serum markers may infer the underlying pathogenesis driving POAF.
METHODS: Pre-operative serum samples were collected from 382 patients undergoing elective surgical valve replacement for severe aortic stenosis (AS) (80.76% sinus rhythm, 19.23% previous AF/preAF). Development of POAF (22.44%) was reported. Discovery studies were conducted with Olink Proteomics® Proximity Extension™ Assay technology in n=41 patients (39.02% POAF) with subsequent functional annotation enrichment analyses. Selected targets along with systemic markers of inflammation, endothelial dysfunction, angiogenesis, clinical and demographic parameters were assessed.
RESULTS: Multivariate analyses revealed 11 targets significantly regulated in AS patients developing POAF. Enrichment analysis suggested that neutrophil degranulation (MPO, AZU1, PRTN3, CSTB, MMP-9) and thrombosis (vWF, AXL, OPN, CHD5) might be instrumental to POAF in AS. The neutrophil degranulation marker MPO (p=0.011) was validated in the whole cohort along with relevant markers for inflammation, endothelial dysfunction and angiogenesis. Only MPO was significantly up-regulated in POAF patients (p=0.028) and was correlated with additional neutrophil degranulation markers (AZU1, PRTN3, MMP-9, NGAL). MPO was also correlated with the expression of vWF and sVEGF-R2 (endothelial dysfunction) as well as with reelin and VEGF-D (lymphangiogenesis) that may support the development of atrial substrate and ulterior POAF. ROC analyses suggest a diagnostic potential for reelin (AUC 0.697, p=0.000, 76.7% precision) and VEGF-R2 (AUC=0.624, p=0.014, 37.7% precision). Logistic regression modelling including MPO, VEGFR2, VEGF-D and Reelin revealed the latter the best marker to forecast POAF occurrence (p=0.044), overall in women (p=0.012).
CONCLUSIONS: Pre-operational serum markers may infer the underlying pathogenesis driving POAF and assist on everyday decision-making strategies.
Presentation Number: H19Publishing Title: Analysis Of Mid-term Results Following Repeated Pulmonary Valve Replacement In Patients With Repaired Tetralogy Of Fallot
Author Block: Christina Chalvatzis, Cordula Wolf, Julie Cleuziou, Jürgen Hörer, Maria von Stumm.
Deutsches Herzzentrum München, Technical University Munich, Munich, Germany.
Abstract Body:
OBJECTIVE: Patients with repaired Tetralogy of Fallot (rTOF) often undergo pulmonary valve replacements (PVR) over their lifespan. However, data about timing of repeated PVR in rTOF patients remains scarce. This study aimed to evaluate the freedom from repeated PVR in rTOF patients.
METHODS: We identified all consecutive rTOF patients who underwent surgical PVR at our institution between 2004 and 2022. The primary study endpoint was occurrence of 2nd, or 3rd interventional or surgical PVR. Time-to-event-data was analyzed using log-rank test with Kaplan-Meier method; predictors of the primary endpoint were assessed by multivariate Cox regression analysis.
RESULTS: A total of 89 patients (42 females) were included. Mean follow-up time was 10±5 years. Median age at TOF repair and 1st PVR was 13 months and 20 years, respectively. At 1st PVR, 25 (28%) patients underwent implantation of porcine or bovine pericardial bioprosthesis and 64 (71%) patients received a homograft. Over the study period, 25 (28%) patients underwent 2nd PVR comprising 12 (13%) surgical and 13 (14%) interventional PVR. Freedom from 2nd PVR at 10 and 15 years was 90±4% and 65±8%, respectively. Freedom of 2nd PVR was similar in patients with homograft vs. bioprosthesis at 10 years (96±3% vs. 72±11%; p=0.2). Eight (9%) patients underwent 3rd PVR with median age of 12 years, resulting in a freedom from 3rd PVR at 10 and 15 years of 97±3% and 82±7%. Multivariable analysis identified age below 15 years at 1st PVR as an independent risk factor for repeated PVR (HR:3.8; 95%-CI 1.5-9.6; p=0.05).
CONCLUSIONS: In our cohort, repeated PVR was common in rTOF patients. Overall, 28% of rTOF patients underwent a 2nd PVR and 9% a 3rd PVR. Patients aged below 15 years at 1st PVR had an almost four-times higher risk for repeated PVR.
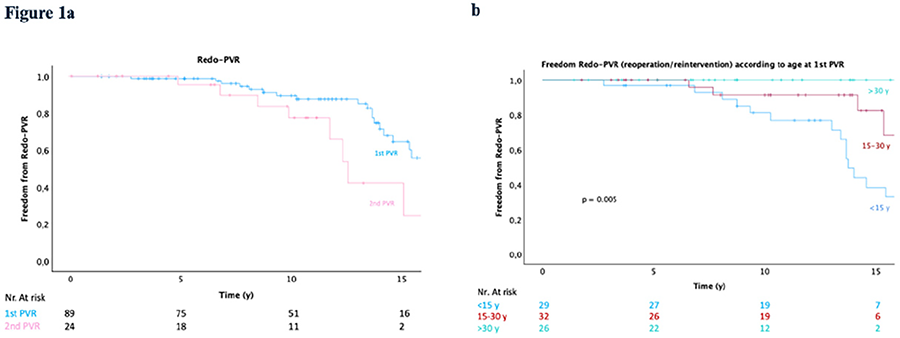
Presentation Number: H20Publishing Title: Successful Delivery Via Cesarean Section In A 19-year Old Primigravid Patient With Severe Uncorrected Isolated Pulmonic Stenosis With Right To Left Interatrial Shunting: A Case Report
Author Block: Cassius Kay Gapol Ramos1, Luke Matthew Mondares2, Fatima Dia Ahaja2, Pjeeco Bagasbas2, Valerie Ann Bering2, Khristine Buque2, Caryl Lou Cotejo2, Jeffrae Isaac Albert Damayo2, Gloria Leonisa Gabisan2, Maningo, Tanara Faye Maningo2, Miguel Tristan Rebalde2, Bernice Serquiña2.
1Vicente Sotto Memorial Medical Center, Cebu, Philippines, 2Cebu Institute of Medicine, Cebu, Philippines.
Abstract Body:
BACKGROUND: Pulmonic stenosis (PS) accounts for 7% to 12% of congenital heart diseases and isolated PS is even rare occurring in 1 per 2000 live births worldwide. Patients may remain asymptomatic even in cases of severe PS. However, the significant hemodynamic burden caused by the changes in pregnancy may precipitate symptoms related to the disorder. This poses a risk for adverse maternal and fetal outcomes. Thus, preconception planning and close intrapartum monitoring by a multidisciplinary team is very important.
CASE REPORT: This paper presents a case of an uncorrected isolated severe pulmonic stenosis in a 19-year-old primigravid female. The patient had an unplanned pregnancy. Nail clubbing was noted on her 4th prenatal visit at 30 2/7 weeks AOG, thus she was referred to a cardiologist who noted a grade 3 systolic ejection murmur. Pulmonic stenosis was suspected and 2D echocardiography done in the 3rd trimester revealed severe pulmonic stenosis with a peak pressure gradient of 218 mmHg. Intrauterine growth restriction was noted on OB ultrasound with persistent minimal variability thus cesarean section was immediately done. The patient had no complications after surgery and was advised to do a cardiac MRI for further assessment of the pulmonary valve and to plan for intervention.
CONCLUSIONS: Pulmonary stenosis may become symptomatic or aggravated due to hemodynamic changes in pregnancy, possibly leading to cardiac decompensation or adverse neonatal outcomes such as intrauterine growth restriction. Thus, prompt risk stratification must be done to tailor the therapeutic strategy to the needs of the patient and the fetus.
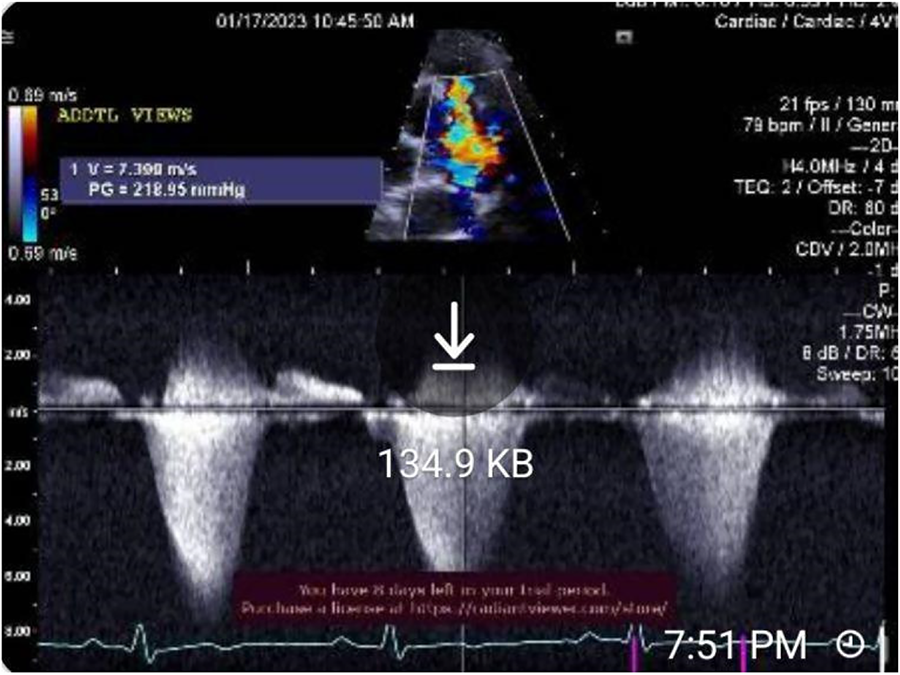
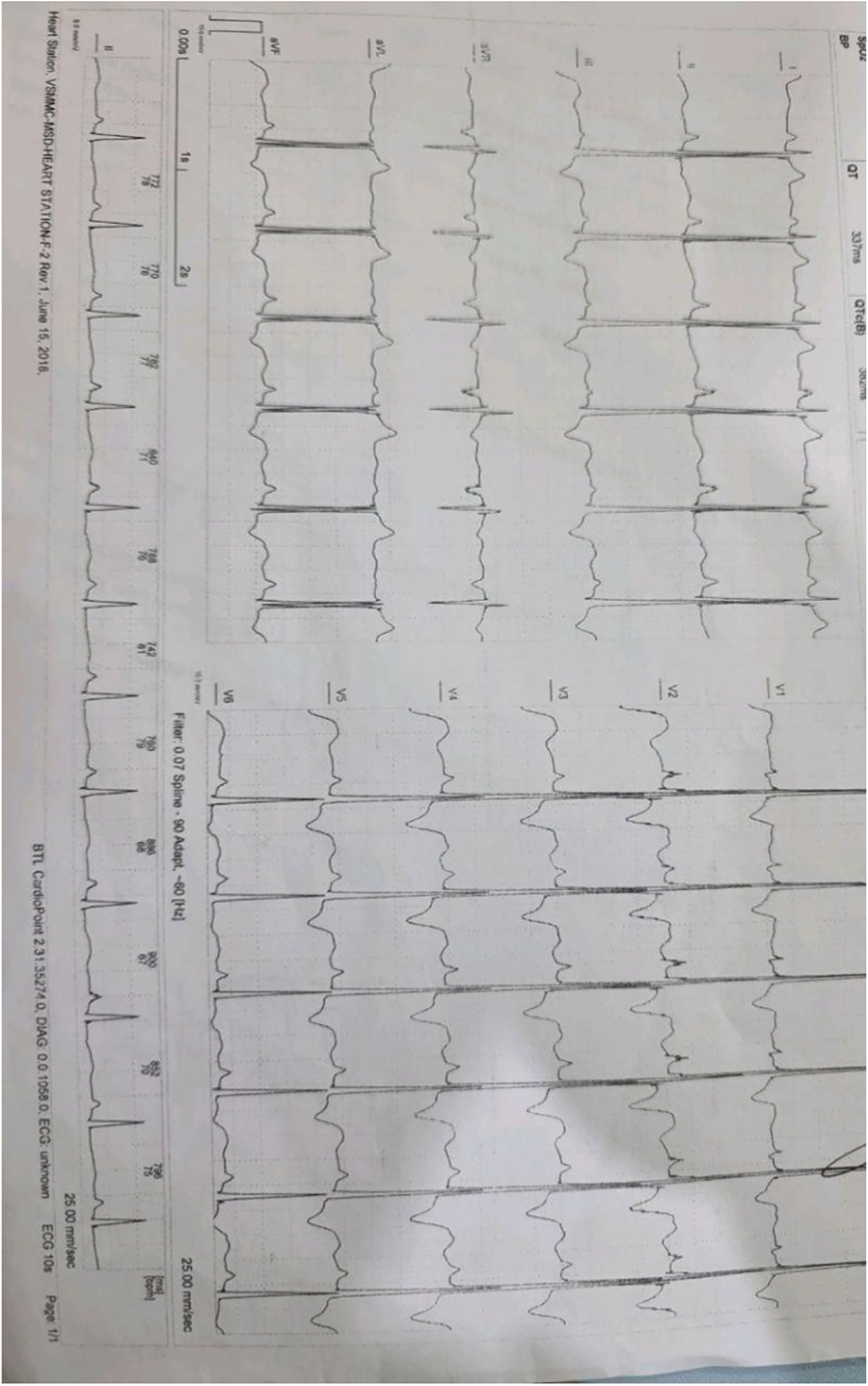
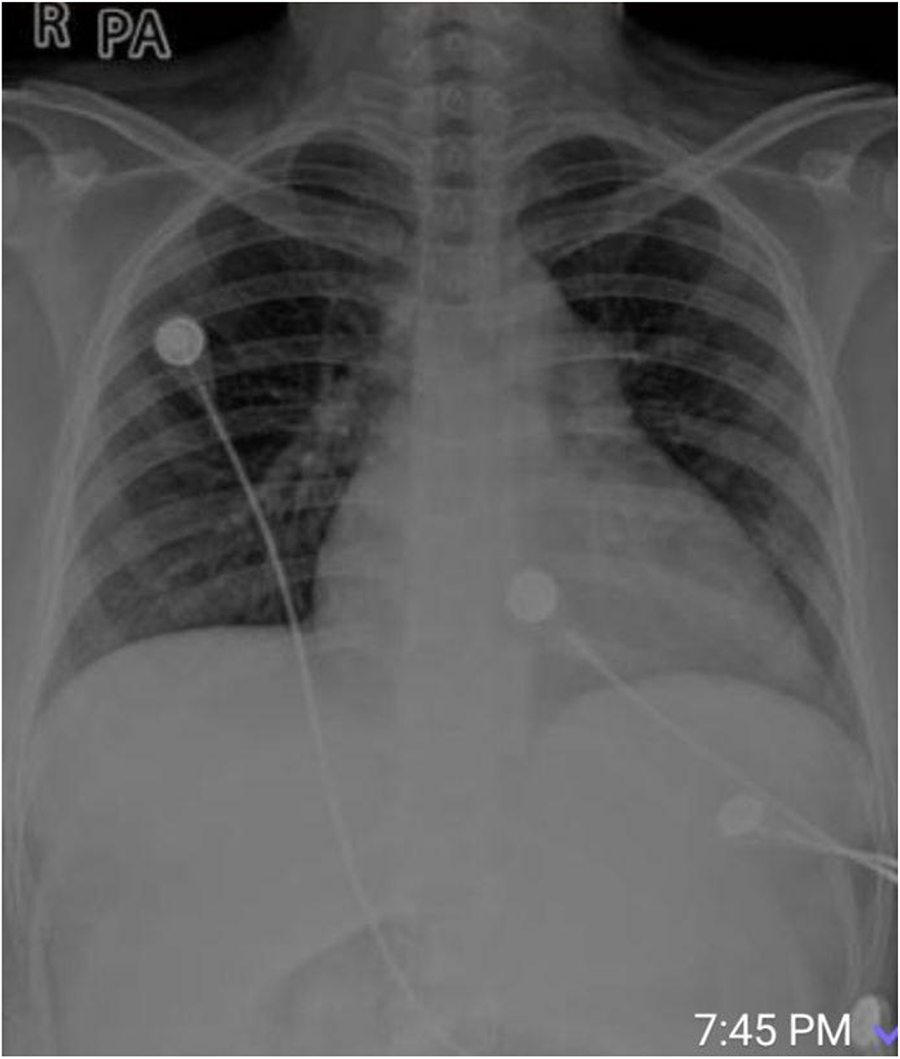

P1-P81 and T1-T7 are display posters
Presentation Number: P1Publishing Title: First In Man Use Of Percutaneous Endoclamp In Minimally Invasive Redo Mitral Surgery, A Prospective Study
Author Block: Vincent Doisy.
Medipôle Lyon, Villeurbanne, France.
Abstract Body:
OBJECTIVE: Evaluation of modification of previously described surgical introduction of the Intraclude Endoclamp by a percutaneous device. The aim is to eliminate local morbidities and improve reaching of ascending aorta to make this technique reliable, standardised and safe.
METHODS: After resolving technical point by using introducer Gore 18fr with preclosing by Proglide device. Percutaneous puncture is done under ultra-sound guidance; Control of guide in aorta under TEE survey. Improvement of balloon visualisation in ascending aorta is achieve by use of SonoVue contrast ultrasound agent. For patients needed mitral surgery with previous cardiac surgery , TAVI or unclampable aorta we systematically use this approach. From december 2022 to March 2024 30 patients were included in the study. Median age: 67,2. 12 patients underwent mitral replacement, 15 mitral plasty, 3 patients mitro-tricuspid procedure. Euroscore: 6,57, Clamping time: 74 mn, ECC: 113 mn.
RESULTS: Intent to treat: 100%. Perioperative mortality: 0%. Follow-up: 100% complete
Plasty: No leak > 1, none SAM, gradient: 3,2 mmHg, none reoperation Succes of plasty in mitral insufficiency: 93, 6%
Replacement: None leak, gradient: 5,1 mmHg
Back to Home: 6,93 Days (4 to 20)
Perioperative complications: 2 transient phrenic nerve paresis, 1 covered stent in iliac artery, None stroke, 1 Pace-maker
Follow-up: All patients are still alive. None reoperation , 1 endocarditis medically treated.
Functionnal status improved: 96%
CONCLUSIONS: In this population of high-risk patients, minimally invasive mitral surgery under percutaneous endoclamp improve results of surgery. Mortality is inferior to expected. Results on mitral valve are excellent. Procedure is safe, reproductible and need to be part of discussion in a Heart- Team strategy.
Presentation Number: A6Publishing Title: Routine Extubation In The Operating Room Following Minimally Invasive Aortic Valve Replacement
Author Block: MinHo Ju, Hyung Gon Je, Chee-Hoon Lee, Mi Hee Lim.
Pusan National University Yangsan hospital, Yangsan, Korea, Republic of.
Abstract Body:
OBJECTIVE: This study aimed to assess the safety of on-table extubation in patients undergoing aortic valve replacement via right anterior mini-thoracotomy because the safety of this procedure is unclear.
METHODS: We retrospectively reviewed the data of patients who underwent isolated aortic valve replacement via right mini-thoracotomy between February 2012 and December 2023. We compared patients who underwent on-table and intensive care unit extubation, excluding emergency or redo surgeries. Factors influencing on-table extubation were also analyzed using multivariable logistic regression.
RESULTS: In total, 423 patients underwent non-emergent isolated aortic valve replacement; Of these, 73.3% underwent on-table extubation. These patients were younger and had lower EuroSCOREII and higher preoperative serum albumin levels. The surgical procedures were similar; however, patients who underwent on-table extubation exhibited significantly shorter cardiopulmonary bypass times (84.0[68.0-104.0] vs. 104.0[85.0-131.5], p<0.001). Early clinical outcomes did not differ significantly, but intensive care unit (24.0[22.0-26.0] vs. 25.0[23.0-30.0], p<0.001) and hospital stays (5.0[4.0-6.0] vs. 6.0[5.0-8.0], p<0.001) were shorter in the on-table extubation group. A predictive model based on age, preoperative albumin level, and cardiopulmonary bypass time achieved approximately 78.4% accuracy for successful on-table extubation.
CONCLUSIONS: On-table extubation was safe and feasible for most patients undergoing isolated aortic valve replacement through right anterior mini-thoracotomy. It carried minimal risk of reintubation and was linked to shorter intensive care unit and hospital stays. These results advocate for the broader implementation of routine on-table extubation for isolated aortic valve replacement through right anterior mini-thoracotomy.
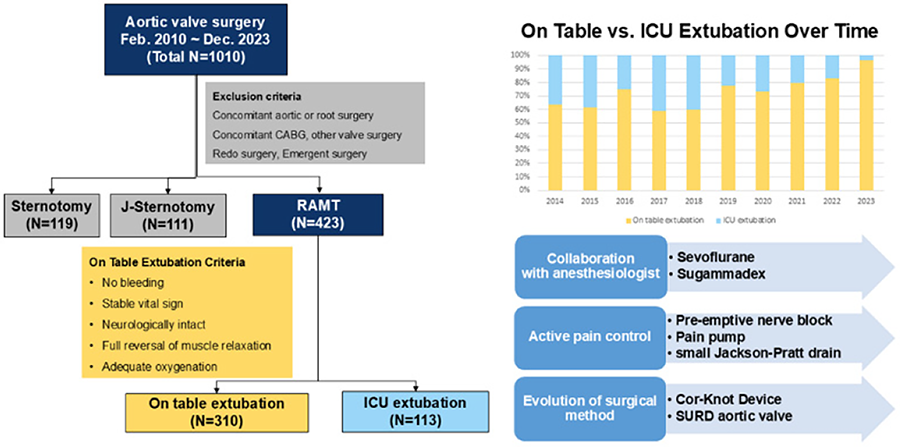
Presentation Number: P3Publishing Title: Impact Of Hand-tied Suture Vs. Titanium Fastener In Structural Cardiac Surgery: A Retrospective Single-center Study
Author Block: Laith Allaham1, Saeed Al Najar1, Yazan Elayan1, Mohammad Aweel1, Raed Rabadi1, Kyle Purrman2, Shaelyn Cavanaugh3, Ariana Goodman3, Mohammad Sajjad1, Mark Lutz4, Adnan Allaham5.
1Albasheer Hospital for Specialized Surgery, Amman, Jordan, 2LSI Solutions, Victor, NY, USA, 3University of Rochester Medical Center, Rochester, NY, USA, 4SUNY Upstate Medical University, Syracuse, NY, USA, 5Albasheer Hospital for Specialized Surgery, Amman, Jordan.
Abstract Body:
OBJECTIVE: When used to secure prosthetic sutures in surgical valve replacement procedures, titanium fasteners (TFs) have demonstrated benefits in both open and less invasive approaches. Using data from a single center’s early experience, this study compares the outcomes from patients whose valve sutures were secured with conventional hand-tied knots to those whose valve sutures were secured with TFs.
METHODS: A retrospective chart review was conducted to analyze the preoperative baseline characteristics and postoperative outcomes of 200 consecutive patients undergoing surgical valve replacement via median sternotomy between January 2020 and May 2023. Patients were grouped according to whether their valve was secured using hand-tied knots (HT group) or titanium fasteners (TF group) (COR-KNOT MINI® Device, LSI SOLUTIONS®, Victor, NY, USA). Patients with a history of prior cardiac surgery and patients undergoing urgent/emergent surgery were excluded.
RESULTS: There were no significant differences in baseline preoperative characteristics between the groups. Patients in the TF group had significantly shorter aortic cross-clamp and cardiopulmonary bypass times than patients in the HT group (p<0.05). The TF group also had shorter ICU time and overall hospital length of stay (p<0.05) compared to the HT group. Postoperative bleeding and paravalvular leak in the TF group were also less frequently observed than the HT group (p<0.05). And although not statistically significant, there was a trend toward fewer wound infections and lower mortality rates in the TF group.
CONCLUSIONS: In our single center’s early experience, the use of TFs in surgical valve replacement was associated with shorter operative times, hospital length of stay, and lower overall complication rate compared to hand-tied valve sutures. These results are consistent with the benefits of the COR-KNOT MINI® Device that have been previously well established in surgical literature.
Presentation Number: P4Publishing Title: Peri-procedural Complications After Percutaneous Aortic Implantation According To Prosthesis Type
Author Block: Marcia M. Cortés, Juan P. Fescina, Martin A. Fasan, Maria F. Castro, Fernando Cura.
ICBA, Buenos Aires, Argentina.
Abstract Body:
OBJECTIVE: Transcatheter aortic valve replacement (TAVR) has emerged as an effective and safe alternative to traditional surgery. Literature regarding its outcomes is limited in our context. We analyzed the incidence of periprocedural complications in patients with severe aortic stenosis undergoing TAVR, and compared according to the type of prosthesis.
METHODS: A prospective analysis of a cohort of patients undergoing TAVR between December 2021 and May 2023 at a cardiology center was performed.
RESULTS: A total of 223 patients were included, 53% were male, and the median age was 76 years. The median EUROSCORE II was 3.94% and the median left ventricle ejection fraction (LVEF) was 60%. Only 4.5% had bicuspid valve. Prior to the procedure, 14% had right bundle branch block, 5% left bundle branch block, and 7% permanent pacemakers. About the intervention, 85% were elective and 15% were urgent. Regarding the type of prosthesis, 67% received self-expandable prostheses (69% Evolut, 25% Acurate Neo, 2.7% Vitaflow, and 3.3% Navitor) and 33% balloon-expandable prostheses (93% Myval and 7% Edwards Sapien). In terms of post-procedural complications, 5% developed tachyarrhythmias, 3.6% suffered a cerebrovascular event, 3% had major bleeding, 22% presented new conduction disorders and 15% required permanent pacemaker placement. Significant paravalvular leak was detected in 11% of patients. During follow-up, none of the patients required reintervention. When comparing by type of prosthesis, there was a higher incidence of significant paravalvular leak in the self-expandable group (15% vs. 4%, p 0.011). No other significant differences were found.
CONCLUSIONS: Patients undergoing TAVR in a specialized center in Argentina had a low rate of periprocedural complications. Conduction disorders were the most frequent and many of them required pacemaker implantation. When compared by type of prosthesis, self-expandable prostheses had a higher incidence of significant paravalvular leaks.
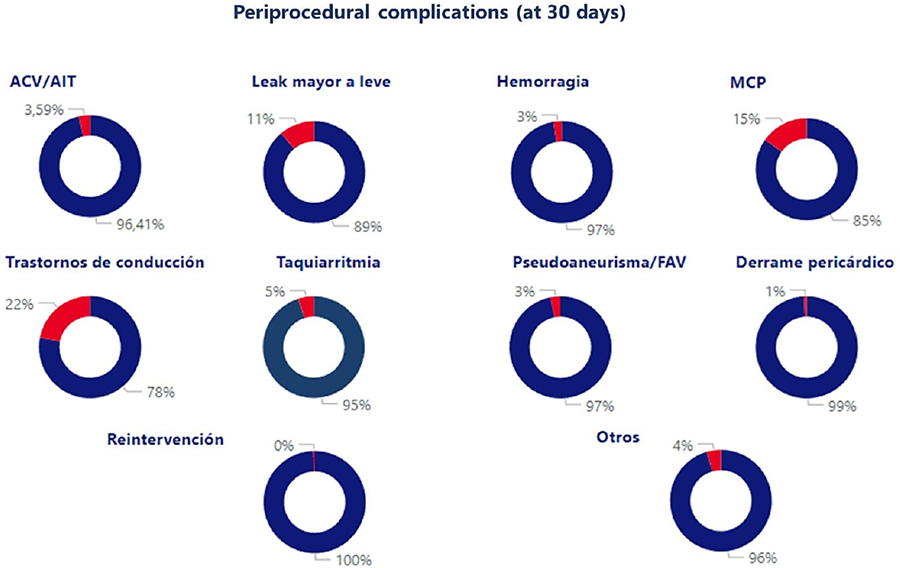
Presentation Number: P6Publishing Title: Fate Of Neoaortic Root After Supported Ross In Children And Young Adult: There Are Advantage Over Un-supported Ross Procedure? Single Center Experience
Author Block: Gianluigi Perri, Vincenzo Labriola, Gianluca Brancaccio, Enrico Cetraro, Sergio Filippelli, Matteo Trezzi, Sonia Albanese, Ermanno Bellanti, Antonio Amodeo, Adriano Carotti, Lorenzo Galletti.
Bambino Gesù Children Hospital, Rome, Italy.
Abstract Body:
OBJECTIVE: Supported Ross (SR) is used to mitigate neoaortic root dilatation that has been described after Ross procedure. There is limited literature assessing efficacy of SR in children. In this study, the fate of neoaortic root was compared between supported and unsupported Ross
METHODS: Between January 2014 and August 2024, 35 patients underwent Ross procedure at our Institution. Among these, 8 (22%) underwent SR by pulmonary autograft inclusion approach technique, that was recently introduced in our Hospital. Median age at operation was 20 years (range, 2 years to 27 years). In SR group, one patient (12.5%) underwent operation under 2 year of age and three (37.5%) undergone previous surgery. One patient (12.5%) need concomitant surgery on ascending aorta
RESULTS: Median follow-up time was 2 years (range 168 to 1596 days). No early or late deaths occurred with estimated overall survival of 100%. In SR group, no patient need reintervention: one patient underwent percutaneous pericardial drainage for pericardial effusion. In unsupported Ross, 3 patients (11,1%) need reintervention: 1 for infective aortic rupture, 1 for pulmonary homograft endocarditis and the last for peacemaker implantation. At follow-up, median neoaortic root diameter in patients undergoing SR was 2.73 cm, while in unsupported Ross was 3.65 cm. Moreover, in SR group, no patients developped neoaortic insufficiency
CONCLUSIONS: Progressive dilation of neoaortic root in Ross patients is significantly mitigated with SRs technique with excellent stability. SR is safe and effective and may play increasing role in the management of children with aortic disease
Presentation Number: P8Publishing Title: Complex Reoperation On Aorta And Aortic Valve
Author Block: Chand Ramaiah.
Ascension Saint Thomas, Nashville, TN, USA.
Abstract Body:
OBJECTIVE: Re-operation on ascending aorta and aortic valve can be complex and associated with high risk of morbidity and mortality. Accurate diagnosis and proper surgical technique can lead to good results.
METHODS: I will present 3 complex re-operations involving ascending aorta and aortic valve. First case is a 3rd time redo for a 10 cm root aneurysm from prior Ross procedure. Second one is a LV pseudo-aneurysm presenting with CAD following prior AVR for endocarditis. 3rd case is distal anastamotic disruption after prior hemiarch for Type-A dissection. Presentation will include TEE, Cath, CTA and intra operative photographs.
RESULTS: All 3 cases were successfully managed with good results and long term survival. Each case required different surgical strategy to achieve success. At followup all 3 patients were alive with no complications. Followup was up to 5 years.
CONCLUSIONS: With proper diagnosis and selecting the right operative approach good results can be obtained. Operative techniques are reproducible.
Presentation Number: P9Publishing Title: Long-term Outcomes Of Transcatheter Aortic Valve Replacement (TAVR) In Patients With Renal Failure On Dialysis
Author Block: Shree Manivel, James Wu, M.D., MBA.
Lehigh Valley Health Network, Allentown, PA, USA.
Abstract Body:
OBJECTIVE: This study aims to evaluate the long-term outcomes and valve durability in patients with pre-existing End-Stage Renal Disease (ESRD) on dialysis who underwent Transcatheter Aortic Valve Replacement (TAVR) for aortic stenosis (AS). The primary goal is to assess survival duration post-TAVR and examine bioprosthetic valve function over time in this high-risk population.
METHODS: We conducted a retrospective analysis of all patients with pre-existing ESRD on dialysis who underwent TAVR between January 2016 and April 2024 at Lehigh Valley Health Network. Patient data was obtained through electronic medical record review. The primary endpoint was duration of survival after TAVR. Secondary endpoints included assessment of bioprosthetic valve function over time, evaluated through post-TAVR echocardiogram findings including valve position, mean aortic valve gradient, left ventricle ejection fraction, and right ventricle ejection fraction.
RESULTS: A total of 39 TAVRs were performed on patients with ESRD on dialysis (38 hemodialysis, 1 peritoneal dialysis). Median survival was 16.2 months, with a mean survival of 22.55 months. At the time of analysis, 10 patients (25.64% of the cohort) remained alive. Long-term valve function appeared durable, with mean aortic valve gradient values staying in the mild AS range. At 5 years post-TAVR, the mean gradient was 8.76 mmHg (excluding one outlier).
CONCLUSIONS: TAVR in ESRD patients on dialysis is associated with improved survival compared to the expected 9-month median survival for untreated AS in this population. Long-term valve function appears durable, with minimal structural deterioration over time. However, overall survival remains limited compared to non-ESRD populations undergoing TAVR. Further long-term studies are necessary to fully evaluate the effects of hemodialysis on TAVR valve durability.
Presentation Number: P10Publishing Title: The Tissue Vs. Mechanical Valve Dilemma Revisited: Another Paradigm Shift?
Author Block: Mohammad Hasan Kalantar Motamedi, MD.
Bahman General Hospital, Tehran, Iran, Islamic Republic of.
Abstract Body:
OBJECTIVE: Heart valve disease continues to be a serious health problem throughout the world, especially in developing countries which continue to see rheumatic heart disease. Valve repair is often not possible and many patients require valve replacement. This study of over 1600 heart valve replacement patients aims to look at long term results, adverse events and quality of life in two major groups of mechanical vs. tissue heart valve patients.
METHODS: From Jan. 2003 to December 2023, 1640 patients underwent heart valve replacement by a single surgical team. 823 patients were male and 817 were female. Age ranged from 8 to 86 yrs of age. Patients were divided into two groups, A) 885 with mechanical and B) 755 with bioprosthetic valves. 234 cases were redo's and 648 cases were multiple valve surgery procedures. Long term outcome, major adverse events and quality of life were studied in the two groups.
RESULTS: Hospital mortality was similar in both groups (3.7 vs 4.5%, P=nonsignificant). However adverse events were more frequent in the mechanical valve group, despite their younger age (21.6% vs 11.5%, P<0.05). Major bleeding and stroke were significantly higher in the mechanical valve group (9.6% and 2.6% vs 3.2% and 1.5% respectively, P<0.05). Long-term survival did not significantly differ in the two groups, and quality of life was significantly higher in the bioprosthetic valve group.
CONCLUSIONS: We conclude that 1) long-term survival is similar in both groups, 2) mid- and long-term morbidity is worse and complications are more devastating in patients with mechanical heart valves, and 3) mechanical heart valves with associated life-long mandatory warfarin use has a substantial negative impact on daily quality of life of patients. Thus, it seems bioprosthetic valves may be suitable for younger age groups as well.
Presentation Number: P11Publishing Title: Minimally Invasive Commando+Maze+TVP Procedure
Author Block: Xinglong Zheng, Yang Yan, Yongxin Li, Heping Zhou, Jing Li.
The First Affiliated Hospital of Xi’an Jiaotong University, Xi'an, China.
Abstract Body:
OBJECTIVE: To report a case of minimally invasive Commando+Maze+TVP surgery for a patient with mitral and aortic valve stenosis.
METHODS: The patient was a 43 years old female who underwent percutaneous balloon mitral valve dilation 20 years ago. Echocardiography showed that the patient had severe stenosis of the mitral and aortic valves, with an aortic annulus diameter of 19mm. Electrocardiogram indicated atrial fibrillation rhythm. We performed minimally invasive aortic valve replacement (25# mechanical valve) +mitral valve replacement (27# mechanical valve) +aortic root mitral valve curtain widening+maze+TVP surgery on the patient through the right third intercostal space.
RESULTS: Surgical extracorporeal circulation time was 181 minutes, cardiac block time was 157 minutes. The drainage volume was 260ml 24 hours after surgery, the ICU stay was 2 days, and the patient was discharged 9 days after surgery. Postoperative echocardiography showed a peak velocity of 1.6m/s and a pressure gradient of 11mmHg in the aortic valve. The patient had sinus rhythm one month after surgery.
CONCLUSIONS: For patients with small aortic valve annulus, commando surgery can effectively widen the aortic root, thereby benefiting the patient. For suitable patients, minimally invasive commando surgery is safe and feasible, and can reduce patient’s trauma.
Presentation Number: P12Publishing Title: Dynamic In Vitro Calcification Testing Of Bovine Pericardium Patches With Titanium Coating
Author Block: Jan Fabian Drexler1, Rouven Tewes1, Sara Leal-Marin1, Marc Müller1, Norbert Guldner2, Birgit Glasmacher1.
1Leibniz University Hannover, Institute for Multiphase Processes, Garbsen, Germany, 2University Medical Center Schleswig-Holstein, Clinic for Cardiac and Thoracic Vascular Surgery, Lübeck, Germany.
Abstract Body:
OBJECTIVE: Pathological calcification is one of the major causes of failure of biological heart valve prostheses. In this publication, we present a method to reduce calcification by coating with titanium. Titanium-coated bovine pericardium patches were evaluated for calcification tendency using a novel compressed air-based in vitro method.
METHODS: Glutaraldehyde-crosslinked bovine pericardium patches were coated with thin titanium layers using plasma-assisted chemical vapor deposition. Three titanium-coated patches and three uncoated patches as a control group were tested for calcification in vitro. The patches were dynamically loaded in a calcification solution at 37°C using compressed air at a frequency of 1s-1 for nine weeks. The composition of crystalline phases was investigated by Raman spectroscopy. Hyperspectral imaging was performed to to visualize deposits of calcium phosphate. Calcium content of the patches was measured by ethylenediaminetetraacetic acid titration.
RESULTS: White crystalline phases could be observed on all patches after nine weeks of in vitro calcification. Crystalline phases exhibited peaks at wavenumbers of 959 to 962 cm-1 in Raman spectroscopy, indicating the presence of hydroxyapatite. Both extrinsic and intrinsic calcified areas of the patches could be localized through hyperspectral imaging (Figure). Calcium content of the patches according to titration was 0.21 ± 0.03 mg for the surface-modified patches and 0.66 ± 0.33 mg for the control group.
CONCLUSIONS: In vitro calcification was drastically reduced by the titanium coating. The test bench developed was able to reproduce the process of calcification in vitro, even at low loading frequencies of 1s-1. Our findings indicate that hyperspectral imaging is a promising approach for two-dimensional mapping of extrinsic and intrinsic calcified areas in biological heart valve prostheses or patches. Future work will address the translation of coating and testing methods from patches to bovine heart valve bioprostheses.
Presentation Number: P13Publishing Title: Long-term Outcomes Of Small Size Of On-x Aortic Valve In A Taiwan Single Center
Author Block: Yung-Szu WU, Ying-Cing Chen.
Taichung Veterans General Hospital, Taichung city, Taiwan.
Abstract Body:
OBJECTIVE: Prosthesis-patient mismatch was found in the small size of aortic prosthesis but did not affect the mortality. In the past decade, the importance of small size aortic mechanical prosthesis has diminished. However, larger size of aortic bioprosthesis might be beneficial in the future for valve in valve procedure. We aimed at reviewing the clinical outcome of small aortic mechanical valve size in our hospital, compared with larger size.
METHODS: We retrospectively collected data of patients who received aortic valve replacement with On-X mechanical valve from 2018 to 2023 in VGHTC. Patients were classified into two groups according to the size of valve larger than 19mm or not. Outcomes of intubation duration, ICU stay, aortic valve area, pressure gradient between aortic valve, and left ventricular ejection fraction were analyzed.
RESULTS: As a result, the duration of both ICU stay and length of stay were significantly shorter in patients with larger size of mechanical aortic prosthesis. Post-operative IABP or ECMO use was significantly higher in the patients who received the 19-mm On-X aortic valve. The trans-aortic pressure gradient was higher in patients with 19mm On-X mechanical aortic valves compared with valve size as 21mm or larger. There was no significant difference between two groups regarding left ventricular ejection fraction. In patients with larger size of aortic prosthesis, the peak pressure of tricuspid regurgitation was lower after operation.
CONCLUSIONS: Postoperative echocardiographic changes were more obvious in patients who received aortic valve replacement with the size of On-X mechanical valve as 21mm or above. Interpretation of echocardiographic changes should be practical with clinical correlation for further surgical planning including choosing larger aortic prosthesis or aortic root enlargement.
Presentation Number: P14Publishing Title: Impact Of Aortic Valve Calcium Score On In-hospital And 1-year Outcomes Of Tavr
Author Block: Mohiuddin Cheema, Robert Hagberg, Sabet Hashim, Raymond Mckay, Jawad Haider, Jeff Mather.
Hartford Hospital, Hartford, CT, USA.
Abstract Body:
OBJECTIVE: Prior studies examining the impact of aortic valve calcium score (AVCS) on outcomes of transcatheter aortic valve replacement (TAVR) have reported conflicting results.
METHODS: We assessed the association of AVCS calculated from pre-TAVR computed tomography with baseline clinical characteristics and adverse in-hospital and 1-year clinical outcome of 474 patients TAVR patients treated at a high-volume center. The study group included 209 females and 265 males with a mean age of 81.2±7.4 years. All patients were treated with new generation balloon-expandable (Edward Lifesciences S3; n=283) or self-expanding (Medtronic Evolut Pro Plus, FX; n=191) bioprostheses from either a transfemoral (n=417) or transcarotid (n=57) approach. Male and female patients were divided into four quadrants ranging from lowest to highest AVCS (Groups 1-4).
RESULTS: Groups 1-4 were well-matched with respect to age, gender, race, comorbidities, cardiovascular risk factors, prior cardiac history, STS risk score, vascular access and valve type. AVCS (Agatston units) ranges included: Group 1 (male: <1925; female: <1283; Group 2 (male: 1925-2715; female: 1283-1883); Group 3 (male: 2716-3565; female: 1880-2500); Group 4 (male: >3565; female: >2500)
Group 1 N=120 Group 2 N=118 Group 3 N=118 Group 4 N=118 p ValuePre-TAVR TestingMean AV Gradient (mmHg) 35.5±10.8 38.9±12.0 42.9±12.5 46.5±15.3 <0.001Peak AV Velocity (m/sec) 3.9±0.6 4.0±0.6 4.2±0.6 4.4±0.7 <0.001LV Ejection Fraction (%) 56.7±14.6 57.7±12.0 57.8±11.2 59.2±11.2 0.478In-Hospital OutcomesMortality 0 (0.0%) 0 (0.0%) 4 (3.4%) 0 (0.0%) 0.011Stroke 1 (0.8%) 3 (2.5%) 0 (0.0%) 0 (0.0%) 0.108Permanent Pacemaker 9 (7.5%) 10 (8.5%) 13 (11.0%) 9 (7.8%) 0.753Aortic Insufficuency>Mild 5 (4.4%) 5 (4.7%) 0 (0.0%) 1 (0.9%) 0.4181-Year OutcomesAll-Cause Mortality 4(3.3%) 7(5.9%) 10(8.5%) 6(5.1%) p=0.386Hospital Re-Admission 6(5.0%) 4(3.4%) 7(5.9%) 5(4.2%) p=0.81
CONCLUSIONS: Increasing AVCS is associated with increasing aortic stenosis severity in TAVR patients with preserved left ventricular systolic function, but is not associated with increasing adverse in-hospital or 1-year clinical events.
Presentation Number: P15Publishing Title: The Expand ValveTM: A Pediatric Pulmonary Heart Valve With Controlled Expansion Capabilities
Author Block: Dan Simionescu1, Martin Lautenschlager1, Erica Hoskins1, David Podolsky1, Agneta Simionescu1, Leslie Sierad2.
1Clemson University, Clemson, SC, USA, 2Aptus Bioreactors LLC, Clemson, SC, USA.
Abstract Body:
OBJECTIVE: In newborns, pulmonary valves are about 10+/-2 mm in diameter, growing and expanding naturally to 24+/-2 mm by age 20. A large number of children born with severe congenital heart defects require immediate valve replacement with an artificial valve. However, no device on the market exists that would expand in diameter in parallel with the patient’s natural growth. Due to this gap, surgeons perform several corrective surgeries, which are potentially detrimental to the patients and increase suffering, costs and mortality. A pediatric valve capable of expansion without the need for repeat surgery is a critical necessity.
METHODS: To address this need, we have developed the Expand ValveTM (patent pending), a sterile, off-the-shelf, 10-mm diameter, surgical pulmonary heart valve designed for pediatric patients. The device is constructed by suturing highly elastic valve tissue leaflets on a novel expandable stent. The biological tissue leaflets can stretch up to 100% in the circumferential direction and are chemically stabilized and treated with anti-calcification agents to ensure long-term durability. We expanded valves to 16- and 24-mm diameters using valvuloplasty balloons and tested their functionality in the Aptus Valve Bioreactor in pulmonary conditions.
RESULTS: The valve is easy to manufacture. Bioreactor testing results showed excellent round opening at all diameters, adequate systolic orifice areas, and good closing parameters, with minimal to moderate regurgitation at the larger diameter.
CONCLUSIONS: Implanting the Expand ValveTM early on in the life of a child has the potential to minimize the need for additional surgical interventions for babies born with heart defects. After the initial surgery, the implanted valve can be expanded as needed, using minimally invasive procedures until maturity is reached. Ongoing work is focused on optimizing design and manufacturing parameters to maximize functionality at larger diameters and preparations for pre-clinical testing and validation in a juvenile piglet model.
Presentation Number: P16Publishing Title: Rapid-Deployment Versus Stented Aortic Valve In Combined Aortic Valve-Coronary Artery Surgery: Towards A Tailored Therapy
Author Block: Rosanna Gambardella, Alberta Marcolini, Maria Lisa Nesta, Federico Cammertoni, Piergiorgio Bruno, Massimo Massetti.
Policlinico Universitario Fondazione Agostino Gemelli, Rome, Italy.
Abstract Body:
OBJECTIVE: Aortic valve replacement (AVR) and Coronary Artery Bypass Grafting (CABG) combined surgery has a mortality rate of 5-7%. Many studies have been done to compare rapid deployment AVR (RDAVR) to traditional AVR. No effort has been made to find which population can benefit the most by using each device. The aim of this study is to individuate this population, comparing short-term outcomes of RDAVR and AVR in higher risk patients undergoing combined AVR and CABG.
METHODS: We retrospectively selected 178 patients >75y/o and with an Euroscore II >4, who underwent combined surgery with at least two grafts between January 2013 and April 2020 (55 AVR cohort -Perimount Magna Ease- and 123 RDAVR cohort -Intuity Elite). After a Propensity Score Match, 41 patients from each group were compared. The primary end-point was the Major Adverse Cardiovascular Events (MACE). The secondary end-points were: ICU stay, death for all causes, acute myocardial infarct, stroke, PMK implantation, aortic mean gradient.
RESULTS: There were no significant differences in MACE percentage between the two groups (AVR 5% vs RDAVR 10%, p value 0,68). The mean gradient was significantly lower in RDAVR (AVR 14.7 mmHg vs RDAVR 9 mmHg, p value<0,01). ICU stay was shorter in patients treated with RDAVR (AVR 67 vs RDAVR 48, p value<0,01). No significant differences were found in postoperative PMK implantation between the two groups (AVR 0 vs RDAVR 7%, p value 0,24).
CONCLUSIONS: Even if RDAVR and traditional AVR in concomitant CABG have no significant difference in MACE rate, we have found a shorter ICU stay after RDAVR. This theoretically means a shorter time to recovery, which is more important in fragile patients. Furthermore, lower mean gradients would be associated with a longer symptoms-free interval. Further studies are necessary to clarify this aspect.
Presentation Number: P18Publishing Title: Impact Of Residual Pulmonary Valve Disease On Exercise Capacity In Patients Following Repair Of Tetralogy Of Fallot
Author Block: Lisa Kout1, Julia Hock2, Cordula Wolf2, Alfred Hager2, Julie Cleuziou1, Jürgen Hörer1, Maria von Stumm1.
1Department of Congenital and Pediatric Heart Surgery, German Heart Center Munich, Technical University of Munich, School of Medicine, Munich, Germany, Munich, Germany, 2Department of Congenital Heart Defects and Pediatric Cardiology, German Heart Center Munich, Technical University of Munich, School of Medicine & Health, Munich, Germany, Munich, Germany.
Abstract Body:
OBJECTIVE: Cardiopulmonary exercise testing (CPET) is an established tool to monitor functional capacity in patients with congenital heart disease. Patients with repaired Tetralogy of Fallot (rTOF) are known to show exercise limitation during CPET. We hypothesized, that exercise limitation in rTOF patients is associated with residual pulmonary valve disease (PVD) (i.e., pulmonary regurgitation), which is a common complication following ToF repair.
METHODS: We included all rTOF patients in this retrospective study who underwent two CPETs at our institution between 1/2006 and 12/2023. The primary study parameter was maximal oxygen uptake (peakVO2), which was indexed by weight or calculated as %predicted peakVO2. The primary study endpoint was a decline of indexed or %predicted peakVO2 between baseline and follow-up CPET. Types of residual PVD were graded using echocardiographic measurements: no PVD (PS < 30mmHg; PR < Grade3), PS (PS≥30mmHg;PR < Grade3), PR (PS < 30mmHg;PR≥ Grade3), and mixed PVD(PS≥30mmHg;PR≥Grade3).
RESULTS: 84 patients (37% females) underwent a baseline and follow-up CPET with mean age of 13±4 years and 20±7 years, respectively. Mean follow-up time between baseline and follow-up CPET was 7 ± 5 years. Residual PVD was found in 38 patients (45%) comprising patients with PS (n=18;21%), PR (n=14;17%) or mixed PVD (n=6;7%). Over the study period, 44 (52%) and 40 (48%) patients showed a decline in indexed and predicted peakVO2, respectively. Five-year freedom from decline of %predicted peakVO2 was significantly lower in patients with PR vs. PS (77±12% vs. 80±10%; log-rank test p=.02). Multivariate analysis identified PR as significant risk factor for decline of indexed (HR2.6;p=.04) and %predicted peakVO2 (HR2.9;p=.01).
CONCLUSIONS: Decline of exercise capacity is a common sequela in rTOF patients, especially in patients with PR. We suggest that - in terms of functional capacity - rToF patients might benefit from repair strategies which avoid PR by accepting a residual PS.
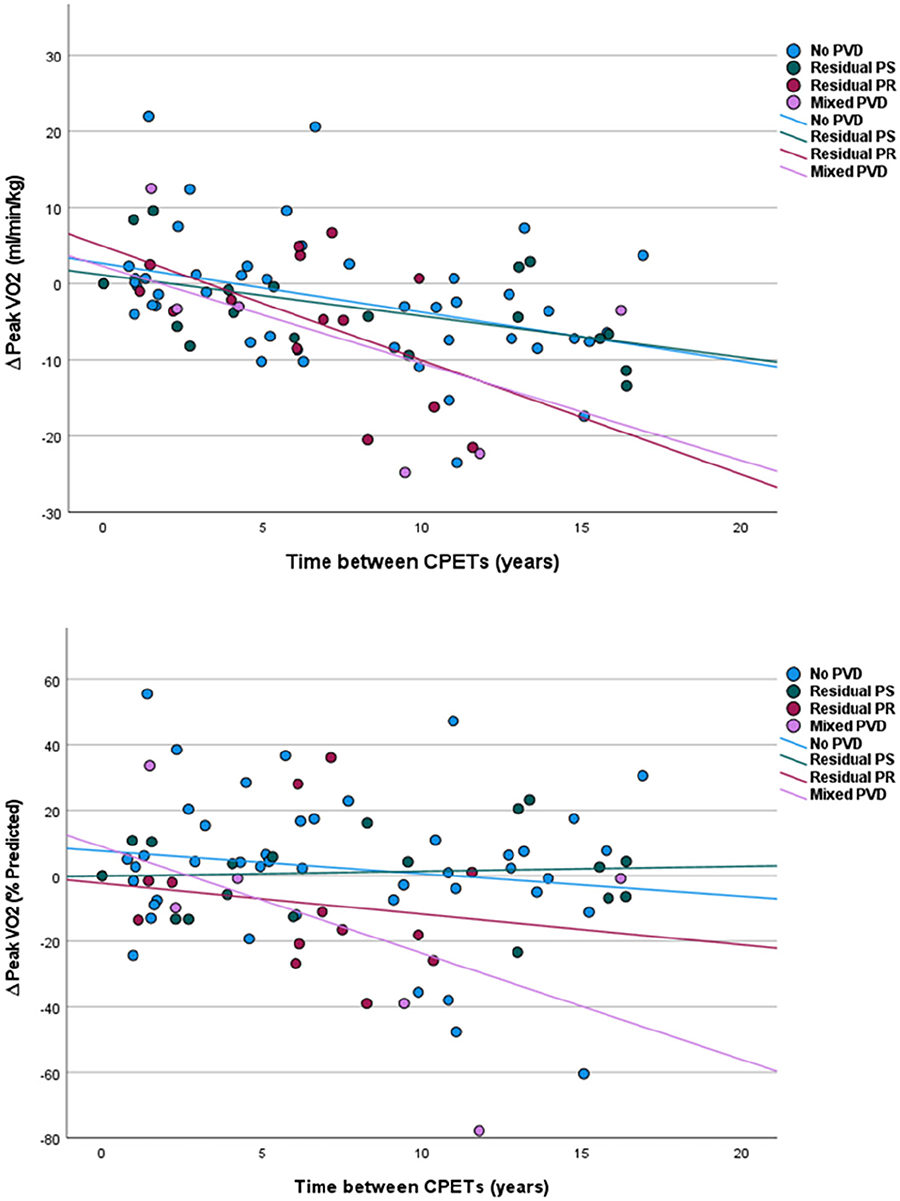
Presentation Number: P19Publishing Title: Complex Endocarditis With Gerbode Defect And Aortic Root Abscess: The Importance Of Imaging In Aiding Diagnosis And Management
Author Block: Marten AttaAlla, Hawazen Alherbawi, Ahmad Maswadeh, Sameh Mohamed, Wael Awad.
St Bartholomew's Hospital, London, United Kingdom.
Abstract Body:
OBJECTIVE: Infective endocarditis (IE) is associated with high mortality and morbidity. A Gerbode defect - an abnormal communication between the left ventricle (LV) and right atrium, is a rare complication. We present a complex case of aortic and mitral valve IE complicated by an aortic root abscess and Gerbode defect with interesting imaging.
METHODS: A 69-year-old man presented with leg swelling, orthopnea, fever and night sweats. He had complex cardiac murmurs and splinter hemorrhages. ECG showed first-degree block. TTE showed severe aortic and mitral regurgitation with vegetations, a Gerbode defect and a preserved LV. TOE confirmed these findings. Blood cultures were positive for Strep viridans. CT aortogram showed an aortic root abscess beneath the right and left coronary cusps and a Gerbode defect. Coronary arteries were unobstructed. Intraoperatively, the aortic valve had multiple vegetations and all three leaflets were destroyed. A large root abscess with a fistula into the right atrium was found just above the septal leaflet of the tricuspid valve and dehiscence of the aortomitral curtain with involvement of the anterior mitral valve leaflet. The tricuspid valve was normal. The aortic and mitral valves were replaced with 27mm mitral and 21mm aortic bioprosthetic valves. The aortic abscess cavity was debrided. The defect in the aortomitral curtain was patched with bovine pericardium. The Gerbode defect was closed with a bovine pericardial patch via a right atriotomy. He was transferred to the ICU on minimal support. Post-op TOE confirmed normal functioning valves without paraprosthetic leak or fistula.
RESULTS: The patient required a permanent pacemaker for heart block. He was discharged 31 days post-op after completing a 4 weeks course of intravenous amoxicillin and ceftriaxone. TTE at 8 months showed normal functioning valves with preserved LV function.
CONCLUSIONS: We present images highlighting the rare complications of infective endocarditis aiding successful surgical management.
Presentation Number: P20Publishing Title: Asymptomatic Antagonism Of Right Atrial Diverticulum And Atrial Septum Defect In 50years Old Woman
Author Block: Vadim Dalinin, MD, PhD, Igor Borisov, MD.
Sokolniki cardiac surgery center, Moscow, Russian Federation.
Abstract Body:
OBJECTIVE: Right atrial diverticulum (aneurysm) is a rare congenital pathology. And of course, this process go on with Right atrial enlargement and results in tricuspid valve insufficiency. This pathology could be found even after 30, when symptoms appear. But Right atrial diverticulum with atrial septum defect as accidental founding in 50-years old woman is unique case.
METHODS: Some extra cardiac tumour, which compresses right ventricle, has been found in 50-years old woman during routine examination before quitting from military. After admitting our hospital deep examination has been performed. During TEE giant right atrial (more than 300 ml) has been found. During MRI of right atrial diverticulum and secondary atrial septum defect has been found. It was verified that diverticulum during systole compress right ventricle area, exactly on the fibrous ring of tricuspid valve.
RESULTS: Patient has been operated. Diverticulum has been closed by purse-string sutures. Diverticulum wall was 1 mm. Atrial septum defect has been closed by purse-string suture. No any other congenital cardiac anomaly has been found. Follow up time is one year. All Echo data is normal. Woman returns to the quitting process.
CONCLUSIONS: Combination of large diverticulum with atrial septum defect is a unique case. Large right atrial diverticulum compressed the tricuspid valve fibrous ring and right ventricle during heart cycle and stops developing of atrial septum defect symptoms as right heart enlargement and pulmonary hypertension. The combination and antagonism of those pathologies makes them remains asymptomatic.
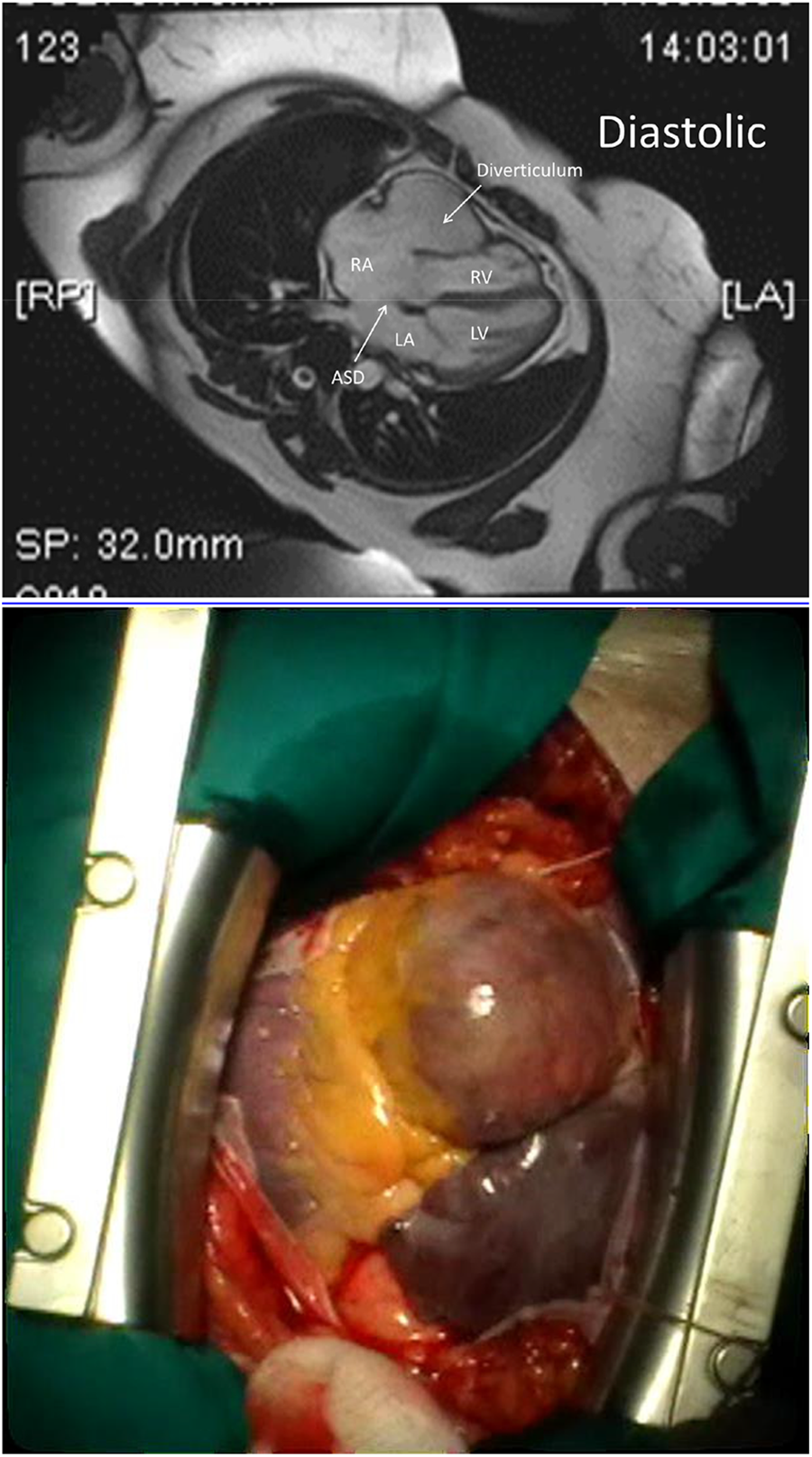
Presentation Number: P21Publishing Title: Aggressive Graft Downsizing During Valve-Sparing Root Replacement In Children And Young Adults Predicts Aortic Valve Reintervention
Author Block: Dominic Recco, Duc Giao, Matthew Schildmeier, Kimberlee Gauvreau, Pakaparn Kittichokechai, Gerald Marx, Christopher Baird, Pedro del Nido, Sitaram Emani.
Boston Children's Hospital, Boston, MA, USA.
Abstract Body:
OBJECTIVE: VSRR is an effective treatment for aortic root pathology +/- aortic regurgitation (AR) in adults. As data in pediatrics are limited, we analyzed midterm outcomes of VSRR in children and young adults to define risk factors for reintervention.
METHODS: From 2006-2023, 81 patients underwent VSRR at 15(11-20)y, with 37% having connective tissue disorders (18 Marfan, 12 Loeys-Dietz). Preoperative diameters were annulus 2.55±0.51cm, sinus 4.30±0.83cm, and ascending aorta 3.31±1.15cm. Thirty-four patients had concomitant >mild AR. Primary endpoint was mortality and secondary outcomes were complications, aortic valve (AoV) reintervention, and subsequent valvular dysfunction. Root and graft diameters were compared using Cox regression to determine effect of intraoperative sizing on endpoints.
RESULTS: Reimplantation technique was used in all but 2 patients with straight-tube (n=41) or Valsalva (n=40) grafts. Thirty-seven underwent concurrent valvuloplasty and 62 ascending aortic replacement. Only 2 patients had >mild AR at discharge with no perioperative mortality. Complications in >10% of patients included arrhythmia requiring medication or pacemaker (n=9 each). At 3.7(0.7-8.1)y follow-up, 4 patients died, 17 required reoperation (4 re-repair, 13 replacement), and 13 developed >mild AR. At 12y, freedom from death, reintervention, and recurrent AR were 92.2(80.4-97.0)%, 59.2(40.7-73.6)%, and 48.7%(25.1-68.7)%. For every 0.1 increase in the ratio of preoperative annulus diameter to graft size, risk of reintervention increased by 58% (HR 1.58[1.11,2.23], p=0.010). A ratio of ≥0.95 maximized model discrimination (HR 5.45[1.59,18.7], p=0.007, C-index 0.72).
CONCLUSIONS: VSRR is safe and effective for children and young adults with aortic root aneurysms. Early arrhythmias, late reintervention, and recurrent regurgitation remain concerns. Graft upsizing or annular reduction should be considered if the ratio of preoperative annulus to intended graft diameter is ≥0.95. Preoperative 3D modeling can guide appropriate graft selection and annuloplasty extent to mitigate reintervention risk associated with excessive downsizing.
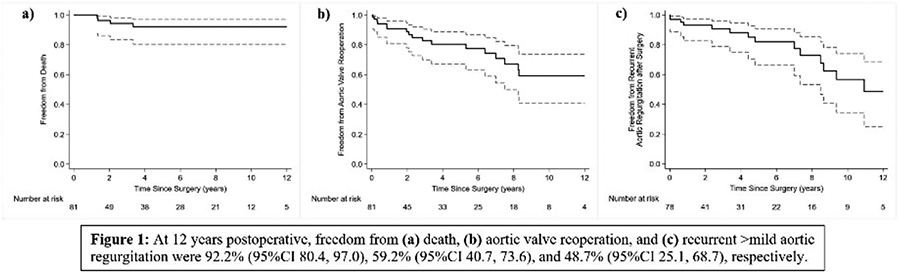
Presentation Number: P23Publishing Title: A Case Of Cor Triatriatum Sinister With Atrial Septal Defect Secundum Type On A 33 Year Old Female
Author Block: Cristoper Jay Pramio Tagalog, Neil Wayne Salces.
Chong Hua Hospital, Cebu, Philippines.
Abstract Body:
OBJECTIVE: Cor triatriatum is a rare case congenital heart disease rarely diagnosed during adulthood. This is to present a case of a 33 year old female who presented with palpitations and symptoms of heart failure was diagnosed with Cor triatriatum sinister associated with a secundum type ASD as seen on 3D-TEE.
METHODS: This is a case report.
RESULTS: We have a case of a 33-year old female with a relatively active childhood with unremarkable past medical history present with acute onset of palpitations and dyspnea with pulmonary congestion (BP 100/60 mmHg, heart rate 105 bpm, SO2 99%). Patient was Worked-up with transthoracic echocardiography showing a normal sized left atria with a linear echogenic density that divides the left atrium into a superior and inferior compartment. There were 2 echogenic drop out in the mid interatrial septum measuring 0.5cm and 1cm with 0.4cm gap between them with a Qp:Qs of 1.7:1. The right ventricle was dilated with evidence of pressure and volume overload, as well as a dilated right atrium. Heart valves were structurally normal, left ventricular systolic and diastolic function is normal. The patient was managed as congestive heart failure with resolution of dyspnea and pulmonary congestion. Surgical repair was advised but did not comply due to financial constraints.
CONCLUSIONS: Echocardiography especially Transesophageal Echocardiography is the mainstay in diagnosing this defect as well as to identify concomitant defects. Medical Management of CTS is limited only for symptomatic relief and definitive treatment involves surgical correction of the obstructing lesion as well as other associated defects.
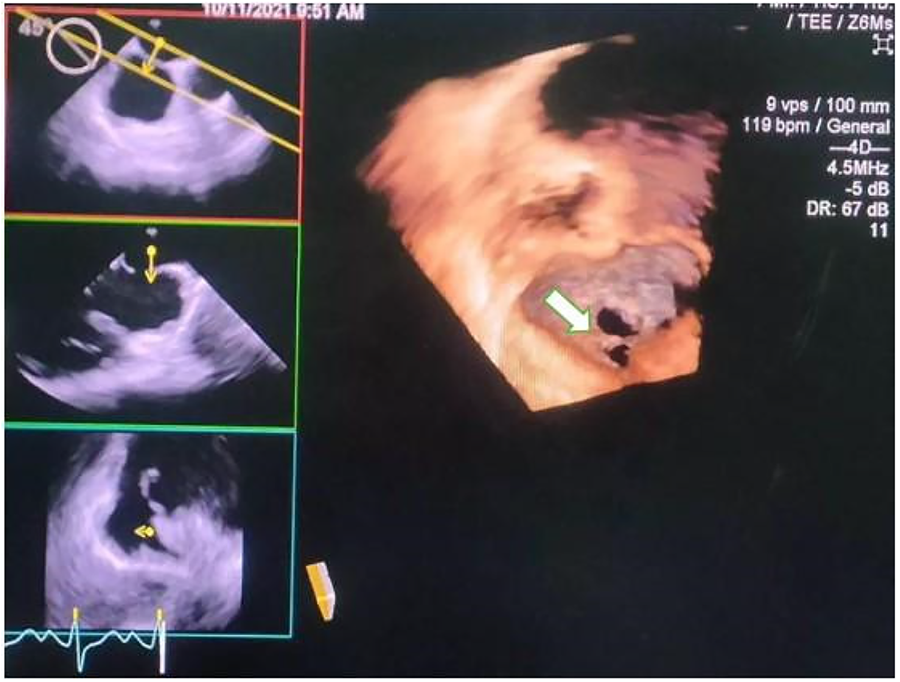
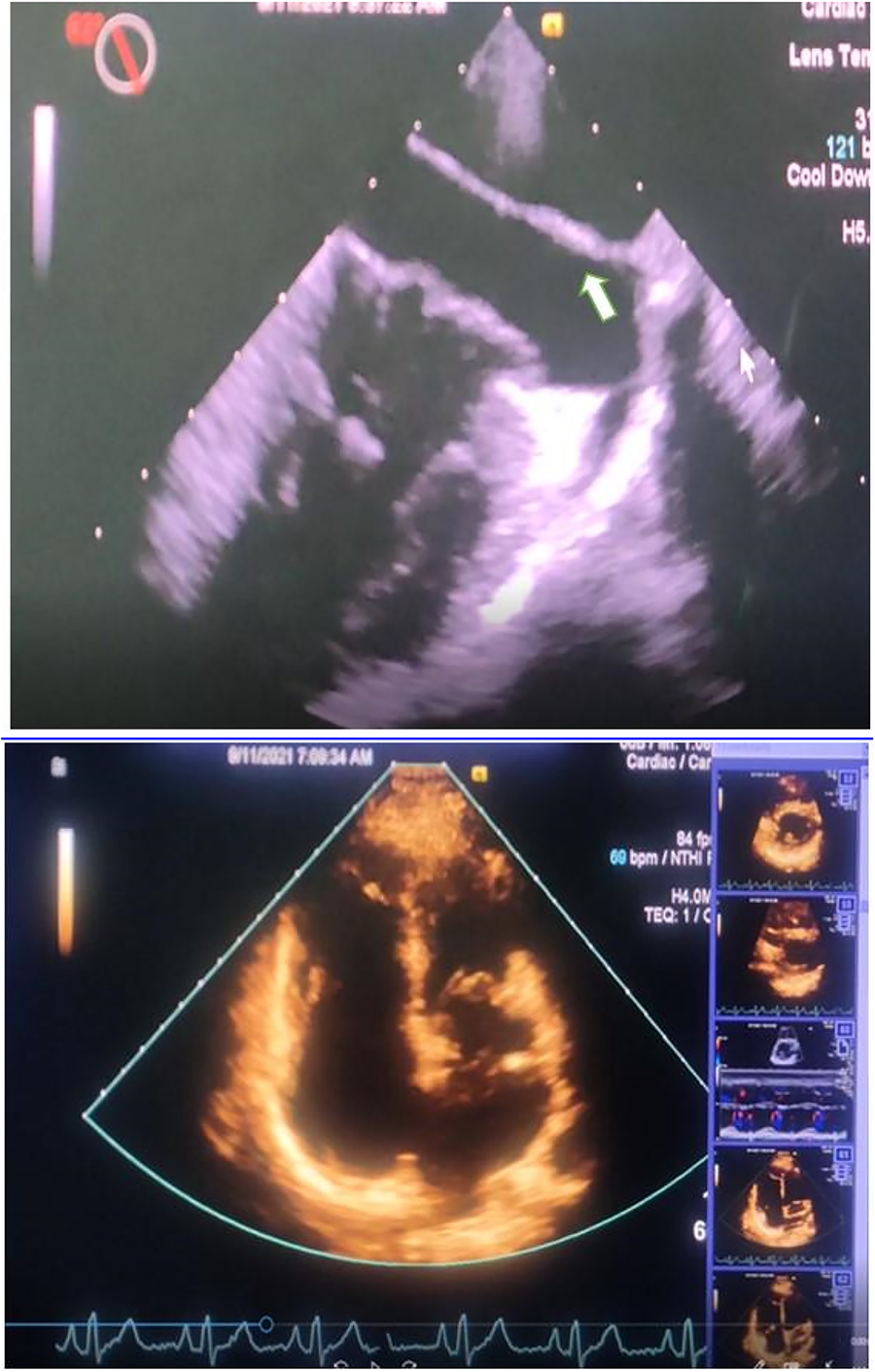
Presentation Number: P24Publishing Title: Thrombocytopenia Induced By Giant Atrial Thrombus Inrheumatic Valve Disease, A Case Report Of Successful Mitralvalve Replacement And Removal Of The Giant Thrombus.
Author Block: Mohammad Lokman Hossain.
Labaid Cardiac Hospital, Dhaka, Bangladesh.
Abstract Body:
OBJECTIVE: Thrombocytopenia can be associated with intracardiac masses, though giant left atrial thrombusis a rare complication. While anticoagulation is often effective for treatment, high-risk patientsmay require aggressive management with resection to prevent fatal outcomes. The casereported here developed thrombocytopenia along with giant thrombus formation in the leftatrium and management of this case was done by successful Mitral Valve Replacement andremoval of the giant thrombus.
METHODS: We report a 52-year-old female patient with thrombocytopenia induced by giant atrial thrombusin presence of pre-existing rheumatic mitral stenosis (MS). The patient presented withprogressively increased shortness of breath and fast atrial fibrillation (AF). Diagnosis wasconfirmed by transthoracic echocardiography (TTE). She underwent bioprosthetic mitral valvereplacement (MVR) and removal of the giant thrombus. The platelet counts graduallynormalized within one week of surgery and her post operative hospital course was uneventful.
RESULTS: A 52-year-old woman presented with bilateral basal crepitations and a fast, irregular pulse. Investigations revealed atrial fibrillation with rapid ventricular response, cardiomegaly,pulmonary congestion, thrombocytopenia (70×109/L), and elevated transaminases. NT-proBNPwas 4811 pg/ml. Transthoracic echocardiography (TTE) showed severe mitral stenosis, tricuspidregurgitation, pulmonary hypertension, and a giant left atrial thrombus infiltrating the pulmonaryvein. Coronary angiography revealed normal coronary arteries. She underwent successfulbioprosthetic mitral valve replacement and thrombus removal, and her postoperative coursewas uneventful. On the 5th postoperative day, her platelet count improved to 125×109/L andnormalized (390×109/L) three weeks after surgery.
CONCLUSIONS: While anticoagulation can treat giant left atrial thrombus, high-risk patients require aggressiveresection to prevent fatal outcomes. Due to the risk of embolization or complications, treatmentmust be individualized. The rise in platelet counts post-thrombus removal suggests aphysiopathological link between thrombocytopenia and giant thrombus.
Presentation Number: P25Publishing Title: Mastering Aortic Valve Repair: Proctoring And Teaching A Standardized Approach With External Annuloplasty
Author Block: Gabriel Saiydoun1, Saadé Saade2, Mohammed Alghamdi1, Pouya Youssefi3, Blaise Demine4, Pascal Leprince1, Emmanuel Lansac1.
1La Pitié Salpetrière, Sorbonne University, Paris, France, 2Strasbourg university hospital, Strasbourg, France, 3Royal Brompton & Harefield hospital, London, United Kingdom, 4Caen university hospital, Caen, France.
Abstract Body:
OBJECTIVE: Valve-preserving aortic root surgical techniques are gaining popularity for treating aortic root aneurysms and aortic regurgitation. However, the adoption of valve-sparing/repair procedures remains limited. This study aimed to evaluate the feasibility, reproducibility, and effectiveness of aortic valve repair performed by a surgical fellow proctored by an expert, compared to a procedure performed by an expert surgeon.
METHODS: In this 10-year retrospective cohort study (2013-2023), 653 patients were enrolled. The primary outcome was a composite criterion, including mortality, aortic valve reintervention, reintervention for bleeding, reclamping for aortic regurgitation (>2), and clamp time. Data were collected prospectively and reviewed retrospectively from Epicard and the Aortic Valve Repair International Registry.
RESULTS: Among 653 patients (aged 49±15 years, 85% male), 457 underwent standardized aortic valve repair, involving root remodeling with an aortic ring annuloplasty, performed by the same expert surgeon (Proctor group). Meanwhile, 196 patients had surgery performed by a fellow under the proctoring of the same expert (Fellow group). The primary outcome showed no significant difference between the two groups (HR=1.58, 95% CI: 0.96-2.6; P=0.07). At 1 year, freedom from mortality, reintervention, or reclamping was 89.25% in the no-proctoring group and 89.28% in the proctoring group. Rates of in-hospital mortality, overall mortality, bleeding, thromboembolic events, pacemaker implantation, myocardial infarction, postoperative creatinine levels, postoperative functional state (NYHA>III), and atrial fibrillation were similar between groups.
CONCLUSIONS: Aortic valve repair with external aortic annuloplasty is a reproducible, effective, feasible, and safe technique for fellows learning it under the supervision of an expert through proctoring.
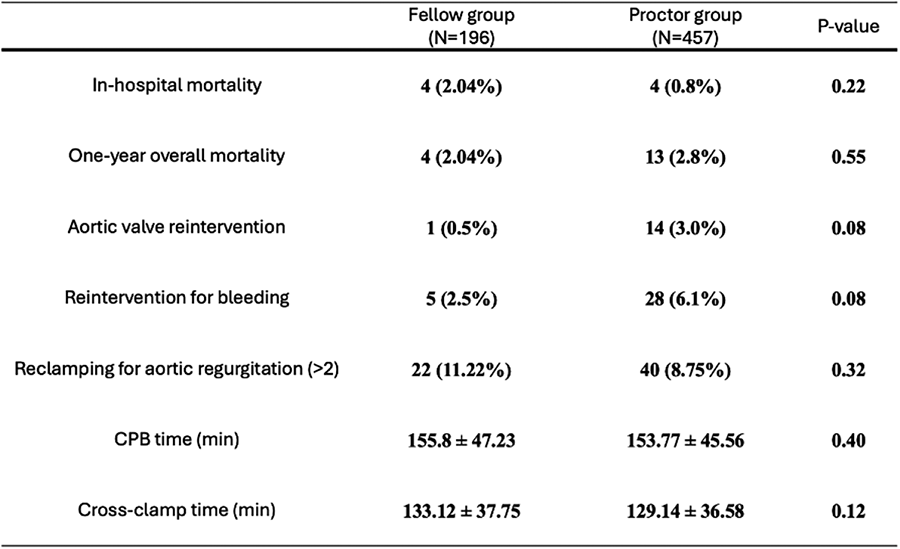
Presentation Number: P26Publishing Title: Minimally Invasive Mitral Valve Surgery Frome Start Of Programm Till Routine Practice
Author Block: Oleg Y. Pidanov, Kirill V. Tscherbatyuk, Boris L. Haes, Dmitry N. Kuzmin.
City Hospital named after I.V.Davidovsky, Moscow, Russian Federation.
Abstract Body:
OBJECTIVE: Minimally invasive mitral valve surgery is a real alternative approach of traditional sternotomy. The start and development of minimally invasive program in the non-specialized mitral valve Clinic is challenged and may associated with increasing of mortality and morbidity.
METHODS: First group, forty-five patients have been operated between March 2014 and March 2018. It was period introducing of minimally invasive program. Second group 187 patients have been operated after March 2018 till 2024. In all cases we used hypothermic extracorporeal perfusion (32 C) via femoral approach. Antegrade cold crystalloid cardioplegia with Custodiol (2000 ml) was used for myocardial protection. In the first group valve replacement and repair were performed in 13(29%) and 32 (71%) patients respectively. In the second group MV repair was performed in 94 % cases of degenerative disease. Concomitant maze procedure was performed in 10 patients (22.2%) and 49 (26.2%) respectively. In the second group was performed 14 transmitral myoectomy.
RESULTS: We observe increasing of proportion of minimally invasive mitral procedures from 10.7% first to 86.3 % in the second group. Mean time of procedure was 270±122.1minutes in the first group and 210±83 in the second. Cardiopulmonary bypass and aortic cross clamp mean time was 159±43.5 minutes and 93±17.4 minutes in the first group and 129±23.5 minutes and 81±12.4 minutes in the second. 30-days mortality is 2.2% in the first group and 1.6% in the second
CONCLUSIONS: Mitral valve surgery through right mini-thoracotomy is a perspective approach for treatment of patients with different type of mitral valve disease. Any type of surgery both safe and effective through minimally invasive approach. The start and development of minimally invasive program is possible in non-specialized mitral valve clinic without increasing morbidity and mortality
Presentation Number: P27Publishing Title: Transaxillary Access For Heart Valve Surgery: A Step-by-step Video Demonstration
Author Block: Abdel Hannan Diab, Alish Kolashov, Rashad Zayat, Phillipp Kolat, Assad Haneya.
Heart Centre Trier, Trier, Germany.
Abstract Body:
OBJECTIVE: The purpose of this video is to demonstrate the technical steps of the transaxillary access for heart valve surgery. Our minimally invasive technique offers an excellent alternative to traditional sternotomy, reducing recovery time and improving cosmetic outcomes. The video highlights key procedural aspects, patient selection criteria, and surgical tips for successful aortic valve (AV) access through the transaxillary route.
METHODS: The video showcases a 5-minute step-by-step guide to performing aortic valve replacement (AVR) through a transaxillary approach. The patient is positioned supine with the right arm elevated, and a 4-6 cm incision is made in the third or fourth intercostal space. Following exposure of the intercostal muscles and placement of a soft tissue retractor, the AV is accessed. A combination of standard and long-shafted minimally invasive instruments is used to perform the valve replacement, with clear visual guidance on maintaining optimal exposure and preventing complications.
RESULTS: The transaxillary approach provides excellent exposure to the AV, with minimal disruption to surrounding structures. This method results in superior cosmetic outcomes, shorter recovery times, and reduced postoperative pain. Our video includes intraoperative footage demonstrating the successful implantation of a bioprosthetic valve without the need for rib resection or sternotomy.
CONCLUSIONS: Transaxillary access for heart valve surgery is a viable and effective minimally invasive approach. The technique minimizes postoperative complications and provides a superior cosmetic result, making it a valuable option for selected patients. We believe that our minimally invasive technique is also well-suited for older patients for whom a TAVI implantation may not be appropriate. This video serves as an educational tool to enhance the reproducibility of the procedure among cardiac surgeons.
Presentation Number: P33Publishing Title: In-hospital And Long-Term Outcomes Of Isolated Surgical Aortic Valve Replacement Withand Without Aortic Root Enlargement
Author Block: Mohiuddin Cheema, Robert Hagberg, Sabet Hashim, Raymond Mckay, Susan Collazo, Deborah Loya, Jeffrey Mather.
Hartford Hospital, Hartford, CT, USA.
Abstract Body:
OBJECTIVE: Aortic root enlargement (ARE) with small annuli has been associated with less prosthesis-patient mismatch (PPM). We sought to compare outcomes of isolated SAVR with and without ARE treated at a large tertiary center.
METHODS: Retrospective analysis was made of an institutional database using STS definitions. Late clinical outcomes were assessed from the EMR.
RESULTS: From a total cohort of 848 isolated SAVR patients treated between 1/1/16 and 6/30/24, 51 had ARE. SAVR-ARE versus SAVR patients were more likely female (76.5 vs 34.5%, p<0.001), otherwise the two groups matched with respect to age (66.0±8.3 vs 65.5±10.7 years, p=0.743), cardiovascular risk factors, preoperative echocardiography, coronary angiography findings and STS risk score (2.0±1.7 vs 1.7±2.3%, p=0.360). The two groups likewise matched with respect to procedural acuity (elective vs urgent), first time vs re-do operations, use of concomitant procedures (MAZE, PFO closure), and valve replacement type (bioprosthetic vs mechanical). SAVR-ARE patients had longer cross-clamp (89.8±31.3 vs 68.5±18.3 mins, p<0.001) and perfusion (116.2±42.8 vs 90.0±28.4 mins, p<0.001) times, smaller prosthesis sizes (22.8±1.8 vs 24.1±2.4 mm, p<0.001). SAVR-ARE vs SAVR cohorts did not differ with respect to mortality (0.0 vs 0.5%, p=1.00), stroke (0.0 vs 0.6%, p=1.00), reoperation for bleeding (3.9 vs 2.3%, p=0.448) and postoperative atrial fibrillation (33.3 vs 26.9%, p=0.313). SAVR-ARE patients required longer intensive care unit stay, longer postoperative length of stay (6.7±10.6 vs 5.5±4.7 days, p<0.001) but similar ventilation times and intraoperative/postoperative blood transfusions. At a mean follow-up 39.9 months, there was no difference between cohorts for mortality, hospital re-admission, aortic valve re-intervention or endocarditis.
CONCLUSIONS: In this single center study, annular root enlargement in patients undergoing isolated SAVR was associated with longer operative times and hospital length of stays, with no increase in in-hospital and late adverse events.
Presentation Number: P34Publishing Title: Minimally Invasive Mitral Valve Repair With Memo 4d Rechord System: 5 Years Of Experience
Author Block: Claudia Calia, Gabriella Rovero, Luciano Barbato, Mauro Del Giglio.
Department of Cardiac Surgery- Maria Pia Hospital- GVM Care & Research, Torino, Italy.
Abstract Body:
OBJECTIVE: Due to its demonstrably superior long-term survival and freedom from valve-related complications in comparison with mitral valve (MV) replacement, MV repair is the recommended treatment in clinical guidelines. The importance of respecting the anatomy of the valve but also preserving the physiological movement of the leaflets is widely discussed. However, deciding the length of the chordal is not easy and time- dispensing. With the memo 4D ReChord system, it could turn artificial chordae replacement into standard procedure. The aim of our study is to show the results of our experience of minimally invasive repair of the MV with this device.
METHODS: From January 2020 to October 2024, a retrospective analysis was conducted on patients who underwent MV repair with MEMO 4D ReChord system through a minimally invasive approach.
RESULTS: 45 consecutive patients were included in the study. Mean age was 55,7 years and about 30% were females. Mean Logistic EuroSCORE-II was 1.1. Anteriore leaflet chords were used in 16 cases, posterior leaflet chords in 36. The most used annular size was 36 (42%). Cardiopulmonary bypass time and cross clamp time were respectively 83.9 and 68.2 minutes. Two reexploration for bleeding were necessary. Median ICU stay and Hospital stay were 1 and 7.5 days. Postoperative echocardiographic results showed no or 1+ (95.6%) mitral valve regurgitation. Only one 30-day mortality occurred. (Table 1)
CONCLUSIONS: The MEMO 4D ReChord system is a reliable choice with very satisfactory postoperative outcomes, promotes standardized chord implantation, offering a reproducible technique while accelerating procedure times.
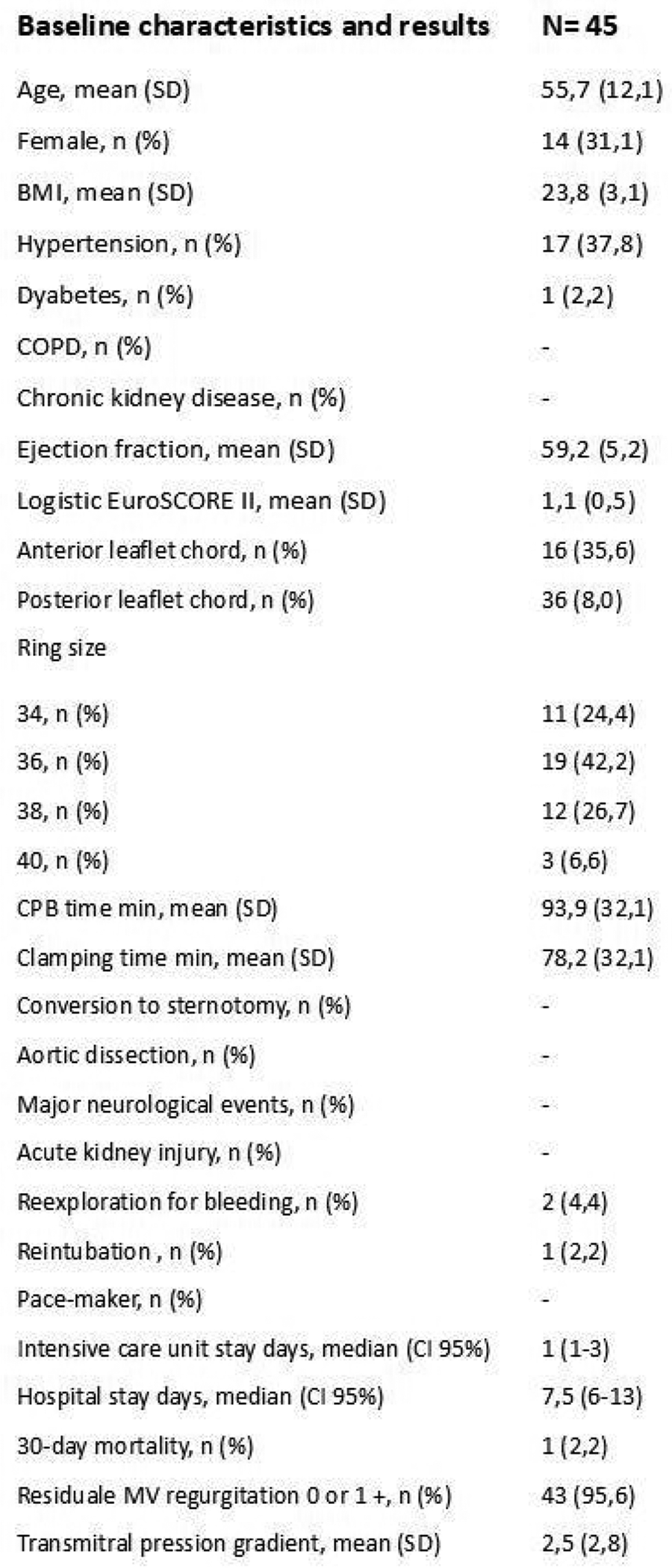
Presentation Number: P35Publishing Title: Completely Calcified Aortic Valve, Root And Ascending Aneurysm Replacement With A Pulmonary Autograft (ross Procedure) And Dacron Graft, Combined With Arterial Revascularization Of The Left Coronary Artery System: Case Presentation
Author Block: Antal Szabó-Bicók, Ali Shadmanian, Tamás Donauer, Miklós Bitay.
University of Szeged, Szeged, Hungary.
Abstract Body:
OBJECTIVE: A 53-year-old female was admitted with severe aortic stenosis. The cardiac ultrasound, CT scan, and coronary angiography revealed a completely calcified aortic valve and root, including the coronary periostial region, and an aneurysm of the ascending aorta. The heart team conclusion was that the TAVR procedure is unfeasible, because of the small caliber and the circumferential calcification of the aortic root.
METHODS: The aortic valve was bicuspid, and had a gradient of 97/56 mmHg, with 20, 22, 22 mm diameters. The CT scan revealed a completely calcified, small caliber aortic root, and an ascending aneurysm (50 mm), with regional calcifications. On the coronary angiography, the origin of both coronaries were calcified, but without any stenosis. Given the young age and the allergy on coumarines, as well as the contraindication for TAVR, we decided to perform a Ross procedure, combined with ascending replacement and arterial revascularization of the left coronary system, using a baby “Y”, followed by ligation of the left main stem. The right ostium was the place of the autograft. The patient was easily weaned of CPB, and transported to the ITU in a stable condition.
RESULTS: The postoperative period was uneventful, with a small amount of blood drainage. The patient was discharged on day 7, with good echocardiographic results and sinus rhythm at the 5th day postoperative check, as well as at the 2 months follow-up.
CONCLUSIONS: The intervention was successful, with a state-of-the-art strategy for a young patient with coumarin allergy, and with no other possible intervention plan.
Presentation Number: P37Publishing Title: Right Anterior Thoracotomy Approach For Aortic Valve Replacement And Subaortic Membrane Resection
Author Block: Ziyab K. Sarfaraz, Qasim Al Abri, Mahesh K. Ramchandani.
Houston Methodist, Houston, TX, USA.
Abstract Body:
OBJECTIVE: We present a case of a Subaortic membrane resection and Aortic valve replacement in a 56-year-old female patient with severely symptomatic left ventricular outflow tract obstruction and aortic valve insufficiency.
METHODS: A minimally invasive right mini-thoracotomy approach was employed to access the aortic valve and Subaortic membrane. The membrane causing the obstruction was resected, and the aortic valve was replaced with a bioprosthetic valve. Intraoperative Transesophageal echocardiography (TEE) was used to confirm membrane resection and evaluate valve function.
RESULTS: The patient experienced an uneventful recovery, with significant improvement in symptoms and no complications. Postoperative TEE showed an unobstructed left ventricular outflow and well functioning bioprosthetic valve.
CONCLUSIONS: Minimally invasive Subaortic membrane resection with aortic valve replacement offers a safe and effective alternative to conventional open sternotomy, providing symptomatic relief, reduced recovery time and improved outcomes in selected patients with combine left ventricular outflow tract obstruction and aortic valve pathology.
Presentation Number: P38Publishing Title: Aortic Valve Preservation In Acute Type A Dissection
Author Block: Veronica Lorenz, Matteo Pettinari, Gebrine El Khoury, Stefano Mastrobuoni, Gaby Aphram, Laurent de Kerchove.
Clinique Universitaires Saint-Luc, Bruxelles, Belgium.
Abstract Body:
OBJECTIVE: Repair and preservation of the aortic valve in Type A aortic dissection remains controversial. In literature there are only reports describing single center experiences. Therefore, we interrogate the Heart Valve society Aortic database to report clinical and echocardiographic outcomes of aortic valve repair in case of acute type A dissection.
METHODS: Data were extracted from the multicentric international Heart Valve Society Database. All patients who underwent ascending aorta or root replacement with or without aortic valve repair were included in the study. The study group was composed by patients operated for acute type A dissection, while the rest of the selected patients was used as control group. Patients with diagnosis of endocarditis were excluded. The primary outcome was long-term mortality, and the secondary outcomes were the incidence of moderate to severe aortic insufficiency and the reoperation rate. At the end of the investigation, competing risk analysis was performed for survival and reoperation.
RESULTS: 372 patients with type A aortic dissection underwent aortic valve repair. Survival at 5 and 10 year was respectively 81% and 66% in the dissection group. Valve sparing root replacement was performed in 53% of the patients. Aortic valve reoperation was similar in the two groups at 5 and 10 years (p=0.6). Moreover, the incident of more than moderate aortic insufficiency did not differ during follow up and the mixed model demonstrated that dissection was not associated with increase late aortic insufficiency
CONCLUSIONS: Preservation of the aortic valve in case of Type A dissection is feasible and can be performed with satisfying midterm results. The rate of reintervention and high degree of regurgitation is acceptable compared to patients without acute dissection.
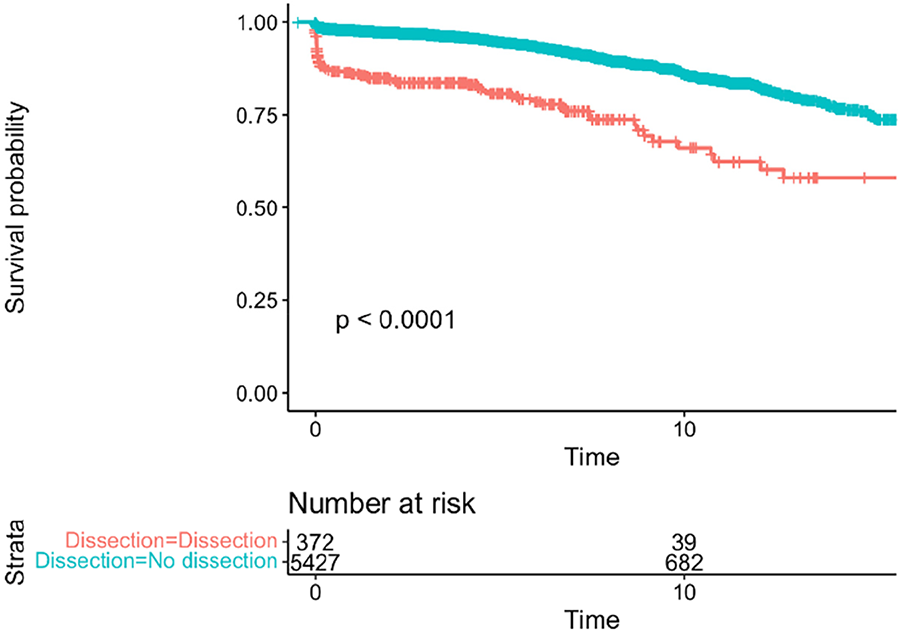
Presentation Number: P39Publishing Title: Evaluation Of Postoperative Outcomes Of Aortic Root Repair In Type-a Aortic Dissection Over A Decade: Insights From A Single Centre’S Specialized Aortic Team
Author Block: Faizus Sazzad, Vishvini Vijayakumaran, Qian Qi, Jai Ajitchandra Sule, Sorokin Vitaly.
National University of Singapore, Singapore, Singapore.
Abstract Body:
OBJECTIVE: Emergency surgery is crucial to improve outcomes in type A aortic dissection (TAAD). Despite advances in diagnostics, treatment, and surgical techniques, early mortality rates remain high. This study evaluates postoperative outcomes following TAAD surgery in a tertiary setting, hypothesizing that aortic root repair is effective when root dissection is present at initial presentation.
METHODS: A multivariate retrospective analysis was conducted from 2010 to 2023, comprising 988 patients from 1113 admissions who underwent aortic root surgery for TAAD. Data were extracted from the existing National University Heart Centre Singapore (NUHCS), Aortic Center’s database. Analysis was performed using IBM SPSS Statistics, focusing on postoperative complications as the primary outcome and hospital length of stay as the secondary outcome.
RESULTS: In this retrospective cohort, 122 patients underwent Bentall procedures, and 53 had aortic root repair surgery. The median patient age was 63.1±14.9 years, with 80% male. Common comorbidities included hypertension (80.5%), poor mobility (35.4%), stroke (13.5%), and diabetes (17.1%). Median times were 243.8±96.4 minutes for cardiopulmonary bypass, 142.2±66 minutes for aortic cross-clamping, and 33.7±25 minutes for circulatory arrest. Postoperative complications included stroke (6.1%), dialysis-requiring renal failure (9.2%), and 30-day readmission (19.7%). ICU stays averaged 5.1 days, hospital stays 16.3 days, with a 30-day mortality of 8.9% and a 10-year Kaplan-Meier survival rate of 73.6%. Multivariate analysis identified female gender, hypertension, poor mobility, existing AKI, and longer ICU stays as predictors of adverse outcomes, and longer hospital stays were correlated with renal failure requiring dialysis, strokes, and pre-existing poor mobility.
CONCLUSIONS: The study intends to improve patient outcomes after having aortic dissection surgeries by identifying potential risk factors to reduce hospital duration and post-operative complications. This will help improve institutional practice even though benefits to participants are limited.
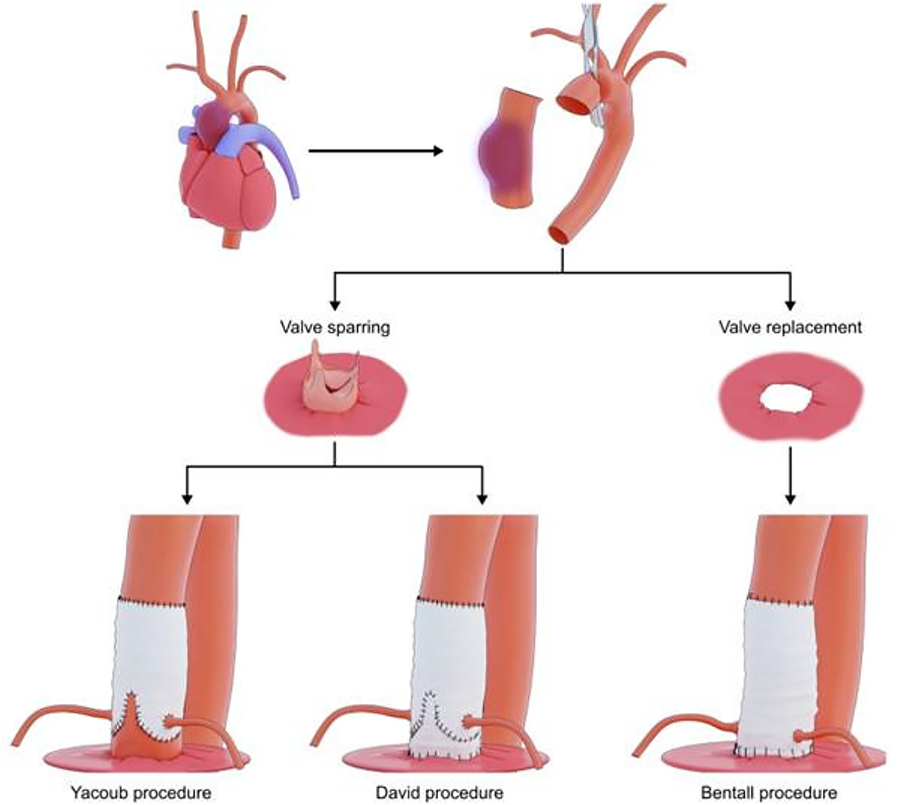
Presentation Number: P40Publishing Title: Feasibility And Performance Of A Novel Tricuspid Valve Prosthesis: Insights From An Acute Ovine Experiment
Author Block: Abdulrahman El Gohary, Ki Han Kim, Irwan Shah Bin Mohd Moideen, John C. Stevens, Theo Kofidis, Faizus Sazzad.
National University of Singapore, Singapore, Singapore.
Abstract Body:
OBJECTIVE: The study aimed to assess the feasibility, acute performance, and safety of a novel tricuspid valve prosthesis.
METHODS: A non-GLP acute animal study was conducted using one ovine subject. A preoperative evaluation was performed using a 3Mensio CT scan, while a post-procedure evaluation was conducted with transesophageal echocardiography and postoperative RA-RV fluoroscopy. Necropsy and macroscopic evaluation were performed following euthanasia.
RESULTS: During surgery, the prominent papillary muscle was identified intraoperatively, and the chordal structures of the prosthesis were anchored to this muscle. The valve prosthesis was successfully implanted, and the papillary muscle orientation facilitated optimal chord attachment. The peak pressure gradient is 5 mmHg, the mean pressure gradient is 3 mmHg, the maximum velocity is 1.1 m/s, the velocity time integral (VTI) is 0.40 cm, and there is trace central regurgitation along with trace paravalvular leakage in the anterior-posterior commissure.
CONCLUSIONS: This feasibility study demonstrates the potential for effective implantation of the tricuspid valve prosthesis with chordal connections.
Presentation Number: P42Publishing Title: Central Fibrous Body Reconstruction
Author Block: B Ufuk Baldan1, Meindert Palmen2, Patrick Klein1, Robert J M Klautz1.
1Amsterdam University Medical Center, Amsterdam, Netherlands, 2Leiden University Medical Center, Amsterdam, Netherlands.
Abstract Body:
In this case of central fibrous body reconstruction, also known as the Commando procedure, there are a few key considerations. One of the most important aspects includes gaining visualization through a Guiraudon incision, aggressively removing all infected tissue, using a double-folded xenopericardial patch, and use of an aortic root bioprosthesis.
Decalcification and debridement of aortic and mitral annulus, AMVL and LVOT
All infected tissue is extensively removed.
Mitral valve ring placement: first posterior annulus
The mitral valve (MV) ring is placed first on the posterior annulus to preserve space for the subsequent repair of the anterior mitral valve leaflet (AMVL).
Augmentation AMVL with Cardiocell patch
A cardiocell patch is chosen for its low rate of degeneration and sclerosis over time.
Anterior mitral annulus repair
Augmented AMVL is attached to the MV annulus.
Inspection coaptation mitral valve leaflets
Coaptation of the MV leaflets is inspected to ensure the free edges are non-pathologic. For coaptation in these cases, it’s preferable to have slight over-augmentation rather than insufficient repair.
Aortic-mitral curtain and roof left atrium: inlay double folded xenopericardial patch
An inlay of a double-folded xenopericardial patch is used to reconstruct.
Trimming boundaries of aortic-mitral curtain and roof left atrium
Roof left atrium repair
Repair of aortic-mitral curtain
Sizing the aortic root bioprothesis
Sizing the aortic root bioprosthesis does not require undersizing.
Using the sizer to identificate tip of the RCC/NCC commissure
The RCC/NCC commissure is identified using the sizer to ensure correct orientation of the bioprosthesis.
Aortic root bioprothesis implantation, positioning 120dg clockwise, LCC in NCC
The bioprosthesis is rotated 120 degrees clockwise, positioning the left coronary cusp within the non-coronary cusp of the bioprosthesis.
Left and right coronary button implantation
Closure anatomical buttons
Distal aortic root anastomosis
Closure of Guiraudon incision
Presentation Number: P44Publishing Title: Understanding The Presence Of Valvular Adipose Tissue In Aortic Regurgitation Patients. A Potential Role For Valve Interstitial Cells
Author Block: Mattie Garaikoetxea, Alba Sadaba, Carolina Tiraplegui, Paula Castillo, Ernesto Martin-Nuñez, Miriam Goñi-Oloriz, Susana San Ildefonso, Eva Jover, Adela Navarro, Natalia Lopez-Andres.
Navarrabiomed, Pamplona, Spain.
Abstract Body:
OBJECTIVE: Adipose tissue (AT) is present in aortic valves (AVs). Valve interstitial cells (VICs) could differentiate into an adipogenic lineage. We here characterize the presence of AT in the AV from patients with aortic regurgitation (AR). Moreover, we investigated VIC differentiation into adipocytes and its influence in AV alterations in AR.
METHODS: AVs (n=144) were analysed by histological and molecular techniques. VICs were cultured with adipogenic, pro-calcifying and a combination of both media. Adipocyte differentiated VICs were co-cultured with autologous VICs, analysing the supernatants with a proteome profiler.
RESULTS: 67% of AVs presented AT. Classical markers of AT were increased in AVs with AT. AT was composed mainly of white adipocytes within the spongiosa. AVs with AT presented increased levels of inflammatory mediators. Interestingly, the presence of AT was associated with greater AV thickness and higher fibrosis, which was characterized by increased collagen and proteoglycans. AV thickness positively correlated with markers of AT, inflammation and fibrosis. In vitro, VICs cultured in a combination of both media exhibited characteristics of adipose cells. Accordingly, adipocyte-differentiated VICs expressed higher white AT markers and increased inflammatory mediators as compared to control VICs. Co-cultured control VICs with adipocytic VICs showed higher expression of AT, inflammatory and fibrotic markers.
CONCLUSIONS: AVs presenting AT exhibit higher inflammation, fibrosis and thickness. Under pathological stimuli, VICs from patients with AR have higher potential to differentiate into adipogenic pathway, contributing to inflammation and fibrosis. VICs differentiation into adipocytes might be a new pathological mechanism involved in AR.
Presentation Number: P46Publishing Title: Unsupervised Machine Learning Analysis To Enhance Risk Stratification In Patients With Aortic Stenosis
Author Block: Marie-Ange Fleury1, Louis Ohl2, Lionel Tastet1, Mickaël Leclercq3, Frédéric Precioso3, Pierre-Alexandre Mattei3, Jérémy Bernard1, Mylène Shen1, Nancy Côté1, Arnaud Droit2, Philippe Pibarot1.
1Institut universitaire de cardiologie et de pneumologie de Québec - Laval, Québec, QC, Canada, 2Centre de recherche du CHU de Québec - Ulaval, Québec, QC, Canada, 3Inria, Maasai team - Université Côte d’Azur, Nice, France.
Abstract Body:
BACKGROUND: There is a lack of studies investigating the pathophysiologic and phenotypic distinctiveness of aortic stenosis (AS). However, this heterogeneity has important implications on identifying the optimal timing of intervention and potential medical therapies. This study seeks to find multiple phenogroups of AS using unsupervised machine learning to improve risk stratification and therapy development.
METHODS: A total of 349 patients with AS from the PROGRESSA study (NCT01679431) were included (median follow up of 7.4 years). Echocardiographic, clinical and blood data were used in the unsupervised agglomerative clustering process. Discriminative models were trained with the sparse generalised mutual information to find multiple sets of stable clusters. Longitudinal data was used to evaluate AS progression.
RESULTS: Five distinct clusters of patients (cluster 1: n=81, cluster 2: n=54, cluster 3: n=47, cluster 4: n=117, and cluster 5: n=50) were revealed using 18 variables selected by unsupervised machine learning. Amongst them, valvular phenotype, mean gradient (MG) and peak aortic jet velocity (Vpeak) were selected as discriminatory variables. Following the clustering process, many characteristics differed between clusters, including age, BMI, and the percentage of male patients (all p<0.001). Of note, cluster 0 showed increased AS severity at baseline with significantly higher initial Vpeak (344 [314; 376] cm/s) and calcium score (1257 [806; 1837]UA) (versus other clusters p<0.001). Patients from cluster 0 had a faster hemodynamic and anatomic progression of AS (delta Vpeak=22 [9; 39] and calcium score progression=+213 [111; 307], versus other clusters p<0.001). Cluster 0 was also associated with a higher composite risk of aortic valve replacement and mortality, even when adjusted for age, sex, and initial AS severity (p<0.001).
CONCLUSIONS: Artificial intelligence-guided phenotypic classification revealed 5 distinct groups and enhanced risk stratification of patients with AS. This phenogrouping may be useful to optimize and individualize therapeutic management of patients with AS.
Presentation Number: P47Publishing Title: Ring Annuloplasty And Sinotubular Junction Stabilization For A Dynamic Ross Procedure
Author Block: Pichoy Danial, emmanuel lansac.
Pitié-Salpêtrière hospital, Paris, France.
Abstract Body:
The Ross procedure offers better long-term survival and freedom from valve-related complications compared with prosthetic aortic valve replacement and is now considered as the first option in young patients. However, progressive autograft dilatation with concurrent regurgitation occurs in 10-30% particularly in aortic regurgitation as the primary indication with annular dilation (> 25 mm) which limits long-term durability. Various techniques have been described to avoid this complication, such as the inclusion Ross procedure. Recently, a more physiological approach was proposed with an extra-aortic annuloplasty and a short ascending aortic tube graft replacement as well as inclusion of the autograft within the remnant root tissue (ie non-coronary sinus and right-left commissure). In the absence of ascending aortic dilatation, we propose a technical modification to restore the sinotubular junction (STJ) and annulus ratio with a double external sub and STJ expansible ring annuloplasty preserving the endocardial continuity as well as root and ascending aortic dynamics.
Presentation Number: P49Publishing Title: David Procedure Via Right Anterior Minithoracotomy
Author Block: Claudia Calia1, Gabriele Tamagnini2, Gabriella Rovero1, Luciano Barbato1, Mauro Del Giglio1.
1Department of Cardiac Surgery, Maria Pia Hospital, GVM Care & Research, Torino, Italy, 2Department of Cardiac Surgery, Villa Torri Hospital, GVM Care & Research, Bologna, Italy.
Abstract Body:
OBJECTIVE: Minithoracotomy has been demonstrated to be a valid cost effective and cost saving strategy for valve surgery, being associated with excellent short term and long-term results, reduced morbidity and mortality, and thus becoming a feasible and popular alternative to the sternotomy approach. Tangible benefits include less pain, faster postoperative recovery, and better cosmetic results. As a result, Minithoracotomy has been increasingly used as a routine approach for both aortic and mitral valve surgery, but only few centers also apply it for aortic root surgery.
METHODS: Since the beginning of our experience of minimally invasive surgery we have opted for a total central cannulation (distal aorta/right atrium) to be as physiological as possible but also to avoid the potential damage of retrograde perfusion. We therefore also applied this setting to the aortic root surgery.
RESULTS:
CONCLUSIONS: In this video we show our tecnique to perform David procedure via right minitoracotomy.
Presentation Number: P50Publishing Title: Early Outcomes Of Miclats Versus Mics-avr. Single Center Retrospective Analysis.
Author Block: Elvin Farhad Rajabov, Rufat Khankishiyev, Jan Gummert, Sabine Bleiziffer.
Herz- und Diabeteszentrum NRW Bad Oeynhausen, Bad Oeynhausen, Germany.
Abstract Body:
OJECTIVE: Minimally invasive surgical aortic valve replacement via upper partial sternotomy (MICS-AVR) is a well-established technique. In contrast, the Minimally Invasive Cardiac Lateral Surgery (MICLATS) procedure provides access through the right 3rd or 4th intercostal space, allowing for a completely sternotomy-sparing surgery. MICLATS was recently established in our center, and here, an analysis of our initial 4-month data.
METHODS: We retrospectively analyzed data from patients who underwent isolated minimally invasive aortic valve replacement via MICS-AVR or MICLATS at our center from June to September 2024. Primary endpoints were 30-day mortality and postoperative neurological complications. Secondary endpoints were cardiac conduction disorders, cross-clamping times, early postoperative drainage volumes, blood transfusion, length of hospital stay and short-term follow-up.
RESULTS: During the 4-months period, we performed isolated minimally invasive aortic valve replacement in n=46 patients. N=18 were performed as MICLATS, n=28 as MICS-AVR. Comorbidities and BMI were comparable. Indication for surgery was severe aortic stenosis in n=43 patients, and severe insufficiency in n=3. There was no significant difference regarding 30-day mortality (MICLATS 0.05 ± 0.2 vs. MICS-AVR 0.0) and neurological complications (MICLATS 0.0 vs. MICS-AVR 0.0). No significant differences were noted in early postoperative drainage volumes (MICLATS 546 ± 443ml vs. MICS-AVR 606 ± 547ml) and blood transfusion (MICLATS 2.2 ± 3.3 RBC vs. MICS-AVR 1.2 ± 2.1 RBC). No patient after MICLATS, 1 Patient after MICS-AVR required a permanent pacemaker. The overall length of stay after MICLATS was not significantly shorter than after MICS-AVR (MICLATS 12 ± 3.3 days vs. MICS-AVR 13 ± 7.6 days). However, cross-clamping time was significantly longer (p<0.05) in the MICLATS group (MICLATS 105 ± 29 min vs. MICS-AVR 63 ± 13 min).
CONCLUSIONS: MICLATS is a safe alternative to MICS-AVR, offering enhanced patient comfort and aesthetic benefits by avoiding sternotomy. Further studies should provide additional insights into postoperative recovery and long-term outcomes.
Presentation Number: P52Publishing Title: Setting Up A Minimally Invasive Valve Surgery Program With Novice Team. A Systematic Approach.
Author Block: Qasim Al Abri1, Ziyab K. Sarfaraz2, Mohammad Bakoush1, Utba Al Mandhri1, Mahesh K. Ramchandani2.
1Royal Hospital, Muscat, Oman, 2Houston Methodist, Houston, TX, USA.
Abstract Body:
OBJECTIVE: We outline our approach to preparing a previously inexperienced team to launch a fully functional, efficient, and safe minimally invasive cardiac surgery (MICS) program.
METHODS: We submitted a proposal to heart center administration detailing the objectives and requirements for establishing a MICS program, followed by a grand round presentation for relevant departments. After acquiring the necessary surgical instruments and disposables, we assembled a multidisciplinary team, including surgical assistants, anesthesiologists, perfusionists, and scrub and circulating nurses. Preparation began with an online tutorial on MICS setup, followed by hands-on training using conventional open-heart surgery cases. This included double-lumen intubation, femoral cannulation with wire and echo guidance, and cardiopulmonary bypass through peripheral cannulation. Del Nido cardioplegia was also introduced in open cases in anticipation of its use in MICS. Individual meetings with each department addressed concerns and provided feedback. Eight patients with diverse pathologies were selected to expose the team to potential challenges and troubleshooting.
RESULTS: All cases were successfully completed by a single MICS-trained surgeon under the supervision of an experienced proctor, with no conversions to open surgery or adverse events. Only one patient required a blood transfusion. The average ICU stay was 14 hours, and most patients were discharged on postoperative day three. Team efficiency and turnover were closely monitored, with outcomes summarized in Table 1.
CONCLUSIONS: Our targeted training approach successfully transitioned a novice team into a competent MICS unit, proving effective in a resource-limited setting. This model has the potential to empower similar teams worldwide, broadening access to advanced cardiac care.
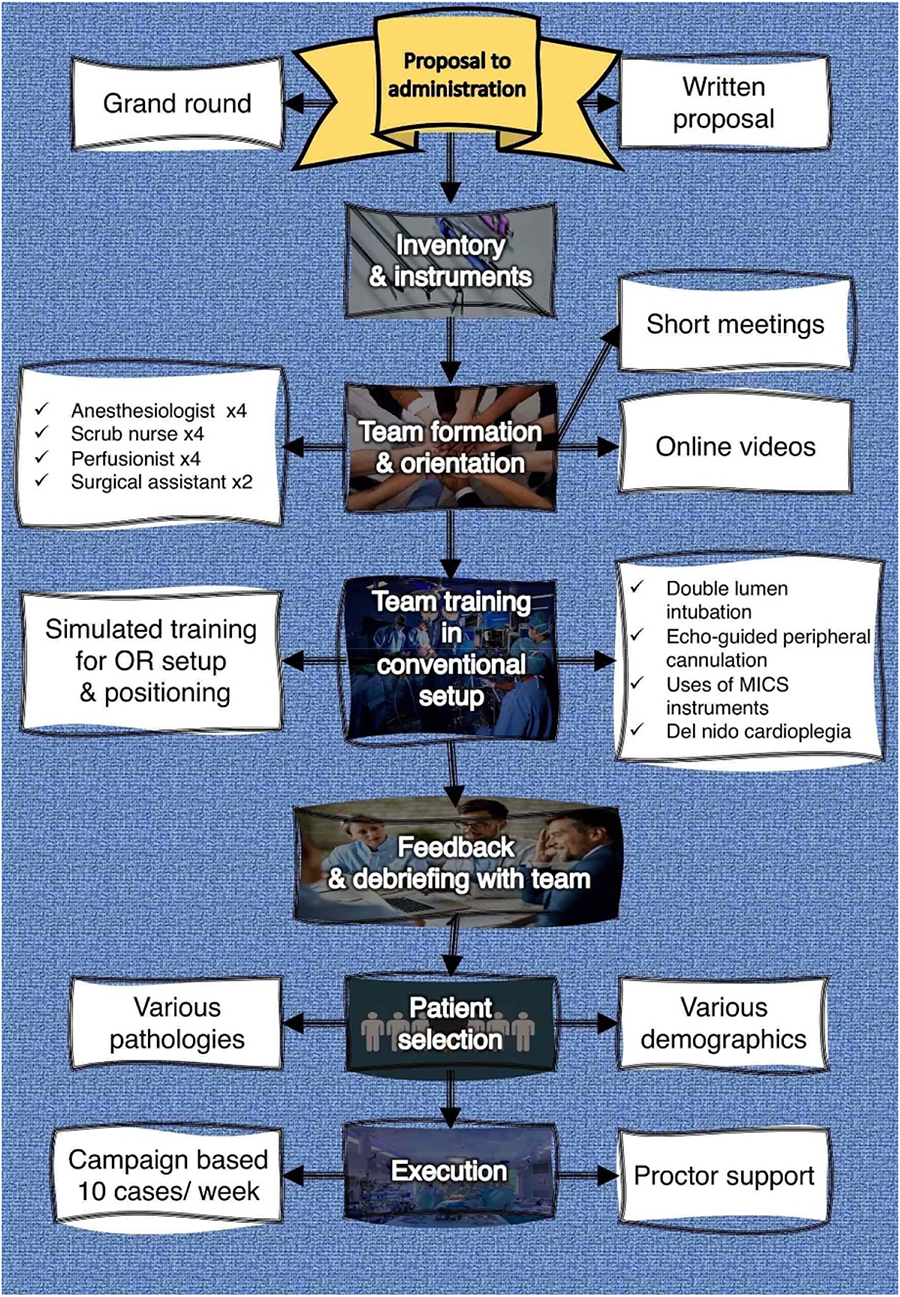
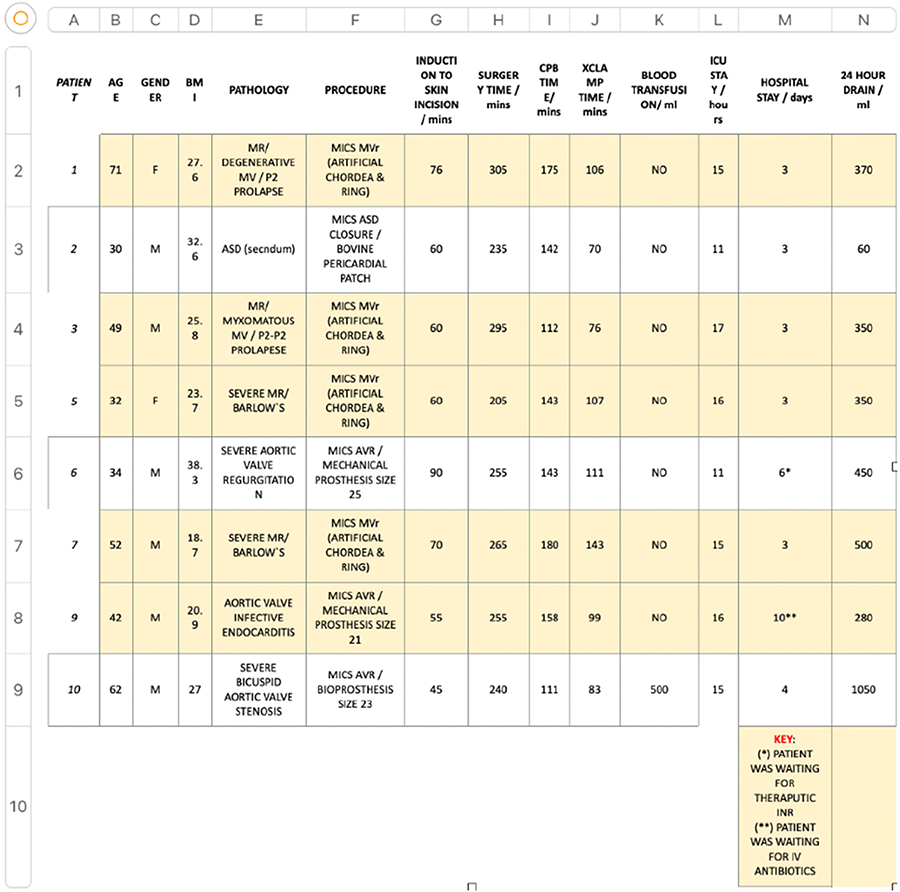
Presentation Number: P53Publishing Title: Clinical Mid-term Results Of Aortic Valve Replacement Using Sutureless Valve
Author Block: Soonchang Hong.
Wonju College of Medicine, Yonsei University, Wonju, Korea, Republic of.
Abstract Body:
OBJECTIVE: We describe the outcomes of patients with aortic stenosis who underwent aortic valve replacement (AVR) using a sutureless Perceval aortic bioprosthesis.
METHODS: We used the data of a retrospective cohort from a clinical database. Patients with symptomatic severe aortic stenosis who underwent surgical AVR with a sutureless bioprosthesis between August 2015 and september 2024 were enrolled. Two hundred thirty patients with severe aortic stenosis who underwent surgical AVR with a sutureless bioprosthesis were enrolled (mean age, 75.3±8.4 years; women, 57.5%; median Society of Thoracic Surgeons score, 9.7%; mean follow up period, 51.19±20.6 months). Eightytwo patients were octogenarian (35.6%), or nonagenarian (1.6%). Transthoracic echocardiography was performed to evaluate changes in ejection fraction (EF), left ventricular mass index (LVMI), mean pressure gradient (MPG).
RESULTS: In-hospital mortality was 2.1%. A permanent pacemaker was implanted in four patients (1.7%). Median intensive care unit stay was 1 day (interquartile range [IQR], 1-2), and median length of hospital stay was 12 days (IQR, 9.5-15). Overall survival was 95.9 % at 5 years. Postoperative LVMI, MPG was decreased, and postoperative EF was increased during followup period. No structural valve deterioration occurred, paravalvular leakage (more than trivial) did not develop during the followup priod.
CONCLUSIONS: A sutureless valve in the aortic position is safe and feasible, even for highrisk, elderly patients requiring surgical AVR. Postoperative LVMI, MPG was decreased, and postoperative EF was increased during follow-up period.
Presentation Number: P54Publishing Title: Betrayed By The Heart: A Case Study Of Rheumatoid Nodules Posing As Infective Endocarditis
Author Block: Zainab Alam, MS, OMSIII1, Gurtej Dhaliwal, MBBS2, Ravi Akula, MD, MBA2.
1Lake Erie College of Osteopathic Medicine, Elmira, NY, USA, 2Arnot Ogden Medical Center, Elmira, NY, USA.
Abstract Body:
OBJECTIVE: We present here a critical, often under-recognized cardiovascular manifestation of multivalvular rheumatoid heart valve disease, which necessitates precise differentiation from infectious etiologies like infective endocarditis to prevent misdiagnosis and inappropriate treatment. To date, this is the first case that was histopathologically proven in similar circumstances.
METHODS: Through an in-depth retrospective analysis of medical records, we evaluated this 60-year-old male patient with treatment refractory Rheumatoid Arthritis (RA) unresponsive to conventional DMARDs and biologics, managed primarily with high-dose prednisone. This patient has a history of extra-articular manifestations of RA namely splenic infarction as well as a non-healing ulcer on his left shin and presented with stroke symptoms. Initial cardiac workup found severe mitral regurgitation with flail leaflet, severe aortic insufficiency and severe aortic stenosis leading to transfer to a tertiary hospital. The original cardiac findings were confirmed along with suspected mitral valve abscess. Infectious disease started IV antibiotics. In light of the abscess, surgery was recommended. Surgical intervention with aortic valve and mitral valve replacement followed by histological analysis of the tissue specimen.
RESULTS: Histopathological findings revealed necrobiotic nodules characteristic of rheumatoid granulomas with central eosinophilic necrosis and surrounding palisading histiocytes—hallmarks of rheumatoid valvular involvement. In contrast to infective vegetations, these rheumatoid nodules lacked microbial colonization, confirmed through extensive staining.
CONCLUSIONS: This case underscores the critical need to recognize non-infective endocarditis in RA as a distinct condition with serious thromboembolic risks. In RA patients with advanced or refractory disease and cardiovascular involvement, close monitoring for rheumatoid valvular disease is essential. Advanced imaging and interdisciplinary management should be standard for RA patients with thromboembolic events, facilitating clear differentiation of rheumatoid nodules from infective vegetations. This distinction can significantly improve valvular disease management and enhance patient outcomes by proactively addressing RA-related cardiovascular risks.
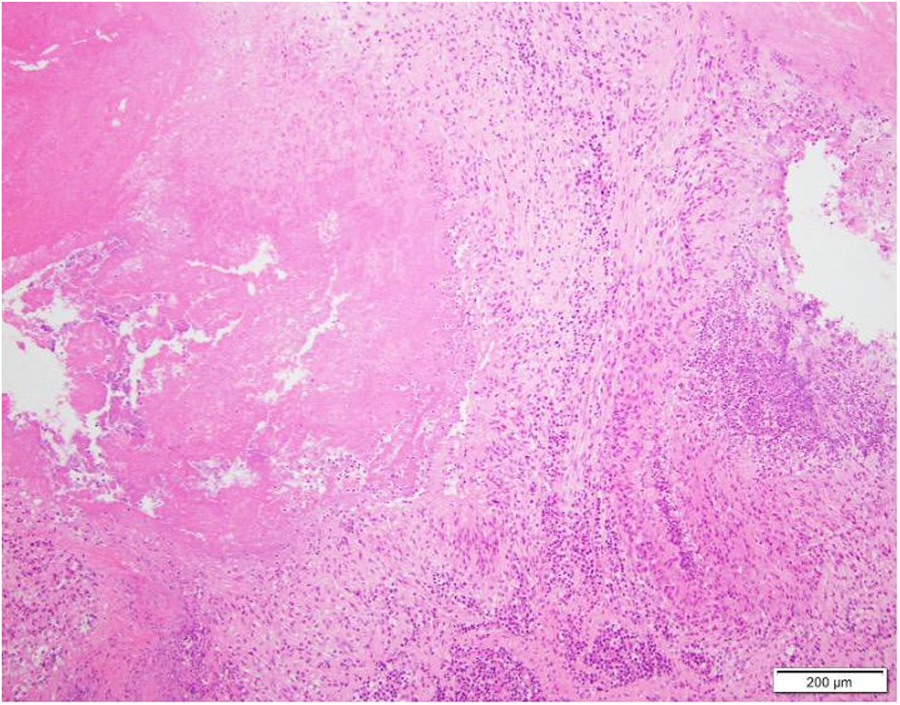
Presentation Number: P55Publishing Title: Tricuspidization Of Bicuspid Aortic Valve
Author Block: Yutaka Okita.
Takatsuki General Hospital, Takatsuki, Japan.
Abstract Body:
OBJECTIVE: The purpose of this study is to analyze outcomes of tricuspidization of the bicuspid aortic valve (BAV) in patients with aortic regurgitation (AR).
METHODS: From October 1999 to June 2024, out of 90 patients with BAV and AR who underwent aortic valve repair or valve sparing aortic root replacement, five patients with very asymmetrical aortic cusp and sinus had tricuspidization. Age at operation was 33.0±16.3 years (median 23, 22-60), and all patients had severe AR preoperatively. The fused valve was right + left in 4, and right + non in one and commissure angle of the non-fused cusp ranged from 130 to 140 degree. All had prolapsing cusps. Geometric height of the cusp was 20.3±2.8 mm, diameter of the basal ring was 29.5±2.7, Valsalva sinus 38.2±4.8, and ST junction 28.0±5.1. Central portion of the fused cusp was elevated to the level of the other commissures. All had resuspension of the non-fused cusp. Postoperative effective heigh 8.4±0.9 mm.
RESULTS: No early or late death was observed. Cardiopulmonary bypass time ranged from 216±20 minutes, and cardiac ischemia time was 173±13 minutes. Postoperative AR was trace in one, and mild in 4 at discharge. Follow-up duration was 5 to 34 months. AR was mild in 4 and moderate in one. Mean pressure aortic valve gradient was 6.9±2.1 mmHg and valve orifice area was 2.10±0.17 cm2.
CONCLUSIONS: Early outcomes of tricuspidization of bicuspid aortic valve with aortic regurgitation were acceptable in selected patients with a suitable anatomy.
Presentation Number: P58Publishing Title: Surgical Treatment Of Concomitant Aortic Valve And Carotid Artery Stenosis
Author Block: Igor Zivkovic1, Petar Milacic1, Zoran Tabakovic1, Ivan Soldatovic2, Bogdan Okiljevic1, Milos Matkovic3, Milos Jovanovic1, Petar Vukovic1, Slobodan Micovic1.
1Institute for Cardiovasculare disease, Belgrade, Serbia, 2Faculty of Medicine, University of Belgrade, Belgrade, Serbia, 3Clinical center of Serbia, Belgrade, Serbia.
Abstract Body:
OBJECTIVE: Neurological problems following heart surgery remain a significant risk for patients. Due to a lack of data, the recommendations do not provide a clear treatment plan for associated carotid and heart disease. Treatment options include surgical and percutaneous techniques that can be performed simultaneously or in two steps (staged). This research evaluated the surgical and percutaneous approaches to treating severe carotid artery disease in patients hospitalized for surgical aortic valve replacement.
METHODS: This retrospective study included 149 patients with significant concomitant carotid and aortic valve diseases. The first group (116 patients) was treated simultaneously by carotid endarterectomy and surgical aortic valve replacement. The second group (33 patients) was treated by same-day carotid artery stenting and surgical aortic valve replacement.
RESULTS: According to the preoperative characteristics of patients, groups were homogenous. There was no difference in the rate of postoperative neurological adverse events (transient ischemic attack and stroke) between Group 1 vs. Group 2 (5.2% vs. 6.1%, p = 0.65). All of the neurological events were nondisabling. The mortality rate was insignificantly higher in group 1. (6% vs. 0%, p = 0.34). Comparing the two groups, MACE was insignificantly higher in group 1. (10.3% vs 6.1%, p = 0.73). In-hospital stay was significantly longer in Group 1. (15±12.5 vs 10±5.1, p=0.02).
CONCLUSIONS: This group of patients is very complex when making decisions about treatment strategies. Regardless of the treatment strategy we used, there is a high rate of periprocedural adverse events. Appropriate preoperative selection is necessary to decrease the rate of adverse events. Percutaneous carotid artery interventions could be a good alternative surgical approach to accelerate postprocedural recovery.
Presentation Number: P60Publishing Title: Initial Palliation In Symptomatic Patients With Fallot Type Lesions: ventricular Outflow Tract Stenting Versus Arterial Duct Stenting
Author Block: Steven Bibevski, Mark Ruzmetov, Kak-Chen Chan, John Dentel, Frank Scholl.
Joe DiMaggio Children's Hospital, Hollywood, FL, USA.
Abstract Body:
OBJECTIVE: Patients with tetralogy of Fallot (TOF) with pulmonary atresia (PA) and severely hypoplastic pulmonary arteries require intervention in the neonatal period. This study set out to compare stenting of the right ventricular outflow tract (RVOT) versus the PDA for palliation in symptomatic patients of TOF/PA-type lesions.
METHODS: Retrospective review evaluating 29 patients (19 males) who underwent palliation with either RVOT (n=14) or PDA stent n=15). Differential left PA (LPA), right PA (RPA), and main PA (MPA) growth was assessed by serial echocardiograms at the pre-stent, pre-surgical repair and at last follow-up phases. Procedure-related morbidity, mortality and reintervention rates were assessed and compared.
RESULTS: There were no early deaths. The groups did not differ significantly in gender, age/weight/height at stent insertion, postoperative length of stay, genetic/syndromic abnormalities, cardiopulmonary and cross-clamp time during complete repair. Twenty-six patients (13 from RVOT group and 13 from PDA group) underwent complete TOF/PA repair; and three patients are awaiting repair. Use of RV-PA conduit during complete repair was significant higher in PDA group when compared to RVOT group (PDA, 100% vs RVOT, 31%; p=0.001). Redo surgery was performed in 31% of PDA patients and none in the RVOT group (p=0.11). Any type of reintervention was performed in 12 patients (RVOT, 31% vs PDA, 62%, p=0.24). The mean time to any reintervention was longer in PDA group (PDA, 5.3+5.3 years vs RVOT, 1.6+0.9 years; p=0.09). Echocardiographic follow-up was available for all patients at a mean of 5.5 years. There were no differences between groups when comparing the MPA at all three timeline periods.
CONCLUSION: RVOT stenting promotes less conduit insertion compared with PDA stenting in symptomatic patients with Fallot-type lesions.
Presentation Number: P61Publishing Title: Trapezoid Modification Of The Y-incision Aortic Root Enlargement
Author Block: Andrew D. Wisneski, Elaine E. Tseng, Marko T. Boskovski.
University of California, San Francisco, San Francisco, CA, USA.
Abstract Body:
OBJECTIVE: The Y-incision aortic root enlargement has become a popular method for root enlargement that accommodates prostheses up to four sizes larger. In very small roots, however, the width of the rectangular patch is limited by the distance between the left fibrous trigone and the membranous septum, and may not allow for sufficient root enlargement. Here we describe a modification to the Y-incision root enlargement using a trapezoid patch that allows for enlargement of the root beyond the limit imposed by left trigone and membranous septum.
METHODS: A mini-aortic valve replacement requiring root enlargement was recorded and edited for presentation.
RESULTS: A transverse aortotomy is made 2cm above the sinotubular junction, terminating above the left-non commissure. If a root enlargement is necessary, the aortotomy is continued down the left-non commissure. It is then split into Y-fashion under the annulus to the right just shy of the membranous septum and to the left extending to the left fibrous trigone. A trapezoidal Dacron patch is fashioned with the short end corresponding to the distance between the membranous septum and left fibrous trigone. The patch is implanted in standard fashion with running suture. Non-everting, non-pledgeted valve sutures are placed along the native annulus and along the widened aspect of the Dacron patch. The valve is then seated and secured in standard fashion. The distal aspect of the patch is then trimmed in triangular fashion, and the aortotomy is closed with running 4-0 Prolene suture incorporating the trimmed end of the patch.
CONCLUSIONS: In cases where the Y-incision aortic root enlargement does not yield sufficient enlargement, a trapezoid patch can be used to further increase the root diameter and allow implantation of larger valve sizes.
Presentation Number: P62Publishing Title: Over Twenty Years’ Experience With Aortic Homograft Implantation For Acute Infective Endocarditis
Author Block: Antonio Davide Conserva1, Andrea Rapagnani1, Stefano Mastrobuoni1, Veronica Lorenz1, Matteo Pettinari1, Gaby Aphram1, Ramadan Jashary2, Gebrine El Khoury1, Laurent De Kerchove1.
1Clinques Universitaires Saint-Luc, Université Catholique de Louvain, Bruxelles, Belgium, 2European Homograft Bank, Clinques Universitaires Saint-Luc, Université Catholique de Louvain, Bruxelles, Belgium.
Abstract Body:
OBJECTIVE: Complex acute aortic valve infective endocarditis (IE) still represents a challenging scenario for surgeons, despite medical and surgical improvements in IE management. Cryopreserved aortic valve homograft (AH) provide an alternative option to prosthetic valves in this situation with a certain versatility, better hemodynamics and higher resistance to relapse and reinfection. Aim of the study was to evaluate early and long-term outcomes of over two decades of experience with AH implantation in IE in our center.
METHODS: All adult patients who underwent aortic valve surgery for infective endocarditis with homograft implantation at St Luc’s Hospital in Brussel from January 2000 to December 2022 were enrolled in the study.
RESULTS: During the study period 176 patients underwent an AH implantation (mean age 62+/- 13 years, 81% male gender). A prosthetic valve endocarditis (PVE) was present in 101 (57.3%) of cases and an annular abscess in 48.8% of all cases (58% of PVE and 36% of NVE). Early mortality occurred in 25 (14.2%) patients. Median follow-up duration was 7.9 years (IQR: 4.7-15.1). During follow-up 17 patients (11.3%) required a reintervention on the homograft of whom only one for reinfection. Freedom from reoperation on the aortic homograft was therefore 99.3%, 95.4% and 84.7% at 5,10 and 15 years, respectively. Long-term survival was 87.3%, 77.5% and 57.6% at 1, 5, and 10 years respectively.
CONCLUSIONS: Complex infective endocarditis of the aortic valve still shows a high perioperative mortality. Replacement of the aortic valve with a cryopreserved homograft shows a very low rate of relapse/reinfection. Although the degeneration of the homograft occurs over the years, however freedom from reintervention is high. Aortic homografts provide excellent resistance to infective endocarditis and good durability over time.
Presentation Number: P63Publishing Title: Dacron Annuloplasty For Bicuspid Remodeling Valve-sparing Root Replacement
Author Block: Mohammad Arammash, Elaine E. Tseng, Marko T. Boskovski.
University of California, San Francisco, San Francisco, CA, USA.
Abstract Body:
OBJECTIVE: The reimplantation procedure is the dominant valve-sparing root replacement (VSRR) operation in the United States, and remodeling has been criticized for its lack of annuloplasty and potential lower long-term durability. Here we present a remodeling VSRR with Dacron annuloplasty and bicuspid aortic valve repair.
METHODS: A bicuspid VSRR was recorded and edited for presentation.
RESULTS: The aortic root is deconstructed and the coronary buttons are harvested. A deep root dissection is carried out, with dissection of the right ventricular outflow tract being most difficult as it can require dissection into the septum to reach the annular level in order to achieve an appropriate annuloplasty. Six pledgeted subannular sutures are placed in planar fashion. A straight graft is cut symmetrically along the two marking lines to fashion two neo-sinus tongues. The remodeling anastomosis is started at the sinus nadirs and carried up to the commissures. Near the nadirs, the bites are small and even to avoid bleeding, but subsequently the bites travel more on the Dacron graft compared to the aortic rim. This creates neo-sinuses and maximizes the height of the commissures. The annuloplasty is completed with a Dacron ring that is secured with the previously placed annuloplasty sutures. For bicuspid repair, the non-fused cusp is plicated to an effective height ≥9mm if needed. The fused cusp edge length is then plicated to the same length as the non-fused cusp. The repair is completed when the two cusp edges are equal with symmetric coaptation. Finally, the coronary buttons are reimplanted using a double biting technique to increase hemostasis.
CONCLUSIONS: Remodeling VSRR with annuloplasty and associated aortic valve repair is an effective and reproducible root replacement operation that allows for ongoing dynamism of the aortic root while robustly securing the aortic annulus.
Presentation Number: P65Publishing Title: Our Experience Of Country Made Ttk Chitra Valve In India
Author Block: Amanullah Ansari, Ram Manuj, Rahul Debdas, Perwaiz Alam.
Brahamananda Narayana Multispeciality Hospy, Jamshedpur, India.
Abstract Body:
OBJECTIVE: To assess and evaluate the efficacy of TTK Chitra valve
METHODS: TTK Chitra valve is countrymade prosthetic mechanical valve of tilting disc mono leaflet type, made in India and very cheap in price as compared to other mechanical prosthetic valve emported from western countries. In our study, 623 TTK Chitra valve were used in 500 consecutive patinents either in mitral or aortic or both positions.
RESULTS: The mean gradient across prosthetic mitral valve is 3.6+_0.4 mmHg and at aortic position is 22+3.2 mm Hg. In hospital mortality is 1.8%. 5 year follow up is 87%. The incidence of stuck valve is 2.1% and anticoagulant related haemorrhage is 1.6%. Only one party required Redo surgery for stuck valve while all other patients responded well with thrombolysis.
CONCLUSIONS: TTK Chitra valve is cost effective for Indian patients with satisfactory outcome in terms of haemodynamics, complications and short and long term follow up.
Presentation Number: P66Publishing Title: Biological Prostheses In Patients Younger Than 65 Years Old: A Propensity Score Matching Analysis Between Two Different Tissue Preservation Methods
Author Block: Alessandra Francica, Fabiola Perrone, Irene Maffei, Cecilia Rossetti, Francesco Onorati, Giovanni Battista Luciani.
University of Verona Medical School, Verona, Italy.
Abstract Body:
OBJECTIVE: No real-world comparisons between the new and the previous generation of bioprostheses are reported in young patients. This study aimed to compare five-year outcomes of two generations of bioprostheses in ≤65 years old patients.
METHODS: From 2017 to 2023, clinical and echocardiographic data of patients receving ThermaFix process or RESILIA tissue prostheses for isolated or combined aortic valve replacement were prospectively collected. Propensity score (PS) matching was performed to obtain two comparable populations. Kaplan-Meier estimation was performed to compare time to events analysis. Prosthetic haemodynamics were compared at different time points up to 6 years using ANOVA for repeated measures. The statistical analysis was performed using SPSS Version 27.0. A p-value of <0.05 was considered significant.
RESULTS: A total of 1602 patients receiving ThermaFix (TF) processed valves were older (mean age 72.3 ± 8.8 vs 59.5 ±9.6 years old), reporting higher EuroSCORE II (5.8 ± 8.3% vs 2.7 ± 5.4%, p<001) than patients implanted with RESILIA tissue valves. After propensity-score matching, 224 matched pairs of ThermaFix process or RESILIA tissue valves patients. Total bioprosthesis explants: TF valves 8 (3.6%) vs RT valves 9 (4%); p 0.8. Only 1 case explanted for SVD in TF valves and 1 for PPM in RT valves. The main cause of explant was endocarditisin both populations. Lower freedom from cardiovascular mortality was observed in patients receiving TF valves. After an initial lower transproshtetic mean gradients and peak velocity in RT valves, the two generation of bioproshtesis showed comparable hemodynamic during 6 years of follow-up (Figure 1).
CONCLUSIONS: In patients younger than 65 years old with similar risk profile, the new RT bioprostheses showed comparable 6-years clinical and echocardiographic outcomes compared to previous generation of valves treated with TF process.
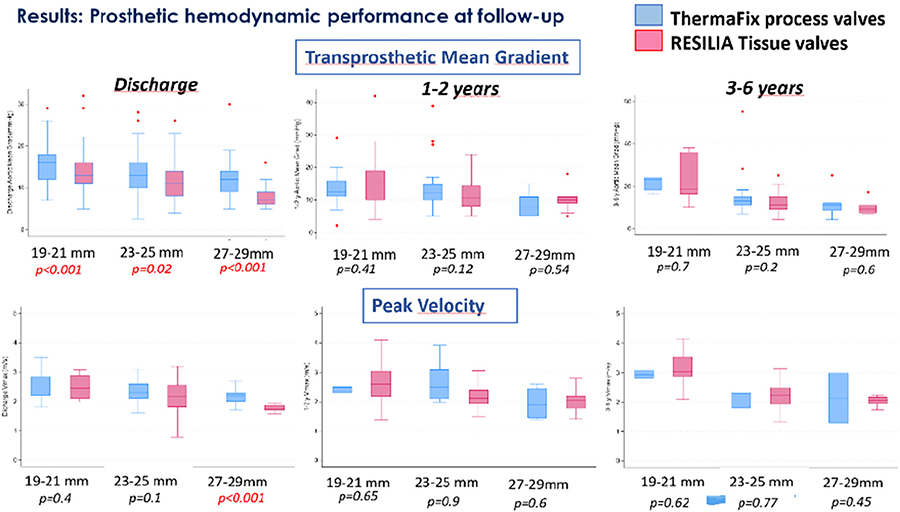
Presentation Number: P69Publishing Title: Levosimendan In Patients With 'Border Line' Left Ventricular Dysfunction Undergoing Cardiac Surgery
Author Block: Ahmed A. Desoky, PhD, Daniele Maselli, PhD.
Clinica Mediterranea, Naples, Italy.
Abstract Body:
OBJECTIVE: First end point was the assessment and evaluation of the potentiality of using GLS (GLS ≤ -17) as an early preoperative indicator of borderline left ventricular dysfunction with high risk of developing postoperative complications, independently of the EF value, in cardiac surgery patients; our second end point was the assessment and evaluation of preconditioning with levosimendan on the postoperative complications in patients with EF ≥ 41% in the immediate postoperative period.
METHODS: Our project was a prospective, randomized, case-control study, where 50 patients underwent elective cardiac surgery including patients with echocardiographic findings of borderline or mid-range left ventricular dysfunction with GLS ≤ -17. From April 2021 until September 2023, all patients who fulfilled eligible criteria were randomized into two groups: the levosimendan group (LG) and the control group (CG). In the LG, patients received a levosimendan (Simdax®; Orion Pharma, Espoo, Finland) infusion at a rate of 0.2 μg/kg/min for 24 h before the intervention. Statistical analysis was performed with IBM SPSS Statistics 27.0 (IBM Corp). For all analyses, a p-value < 0.05 was considered statistically significant.
RESULTS: During the intensive care unit stay, 21 (42%) post-operative complications occurred, 16 in the control group with a statistical significance of P-value 0.02. The postoperative lactate peak levels in the first 24h were statistically lower in the LG, and a statistical significance was found with a P-value 0.01.
CONCLUSIONS: The postoperative complications were higher in the control group compared to the levosimendan group. Assessment of global longitudinal strain in cardiac surgery patients is beneficial and superior to LVEF because of the ability to detect early cardiac dysfunction in asymptomatic patients due to compensation by other groups of strain. Preconditioning with levosimendan in patients with compromised left ventricular function appears to reduce significantly the early postoperative complications.
Presentation Number: P70Publishing Title: Urgent Ozaki Procedure For Huge Aortic Valve Mass
Author Block: Mohamed Ahmed Gabr, Mohammed Sanad, PhD.
Mansoura University, Mansoura, Egypt.
Abstract Body:
OBJECTIVE: Aortic valve bioprostheses are prone to degeneration in adults and more rapidly in young patients. Ozaki procedure involves creation of new aortic valve leaflets from the patient’s pericardium. Short and mid-term results of Ozaki are promising in various aortic valve diseases.
METHODS: A 45-years-aged lady with primary Anti-phospholipid Syndrome, history of DVT, pulmonary embolism and COVID-pneumonia, presented with recurrent syncopal attacks and acute pulmonary edema. Workup revealed a huge aortic valve mass totally obstructing the AV orifice with sever AS in setting of small aortic annulus. After patient-centered, shared decision-making, the patient chosen Ozaki procedure. Urgent Ozaki procedure was done according to the standardized protocol. After median sternotomy, pericardial harvesting and preparation according to the standard Ozaki protocol, a huge fleshy mass was found totally obstructing the AV orifice, non separable from the leaflets and protruding deeply into the LVOT. The mass was excised and standard AV neocuspidization was performed.
RESULTS: TEE after weaning off CPB revealed a well functioning neo-AV. Postoperative course went uneventful. Histopathological examination of the mass revealed the diagnosis of Libman-Sacks Endocarditis. 1 year follow up TTE revealed a well functioning AV with no AR and very low gradients.
CONCLUSIONS: Libman-Sacks Endocarditis is a rare immunological entity and describes a broad spectrum pathologies ranging from very small microscopic particles to huge vegetations (sterile) on previously normal cardiac valves. AVNeo is an innovative surgical procedure to treat a wide spectrum of AV pathologies. AVNeo has impressive mid-term outcomes. In case of Libman-Sacks endocarditis, AVNeo is a creative procedure in this setting; due to the non-immunogenicity, non-thrombogenicity when compared to xenograft prostheses. Moreover, in this specific patient with small annulus, it provided an easy out-of-box solution alternative to conventional solutions, with very impressive hemodynamics.
Presentation Number: P73Publishing Title: Impact Of Bicuspid Valve Morphology On Outcomes Of Valve-sparing Root Surgery - Is It All About Symmetry?
Author Block: George Gradinariu, Kezia Summers, Ahmed Shaheen, Ahmed Othman, Ayman Kenawy, Deborah Harrington, Jakub Marczak, Matthew Shaw, Manoj Kuduvalli, Mark Field, Omar Nawaytou.
Liverpool Heart and Chest Hospital, Liverpool, United Kingdom.
Abstract Body:
OBJECTIVE: To evaluate the role of commissural symmetry in outcomes of bicuspid aortic valve (BAV) repair and identify additional outcome-influencing factors.
METHODS: We included consecutive BAV patients who underwent valve repair or valve-sparing root surgery. The primary outcome was a composite of: early and late death, valve-related reoperation, moderate aortic regurgitation (AR) or moderate stenosis (AS) during follow-up.
RESULTS: 99 patients were included, with a mean age of 45±12 years. 90% were male. 95% (n=94) underwent David V reimplantation, 3% (n=3) had remodeling and 2% (n=2) had valve repair with annuloplasty. Commissural orientation was symmetrical in 60% (n=59) of patients and asymmetrical in 17% (n=17) or very asymmetrical in 23% (n=23). Mean annular diameter was 29±4mm. The mean geometric height for the conjoined cusps was 21±3mm and 24±3mm for the non-fused cusp.
Median follow-up was 24 months. There were no early postoperative deaths or intraoperative conversions. The primary outcome occurred in 9 patients (2 deaths, 2 reoperations, and 5 patients with moderate AS/AR). Commissural symmetry was not associated with the composite outcome (figure) or moderate AR/AS (p=0.62). However, lower geometric heights of fused and non-fused cusps (OR 0.53, p=0.01; OR 0.65, p=0.01), anterior leaflet calcium (OR 8.3, p=0.03) were predictors for the composite outcome. Anterior leaflet plication had a beneficial effect (OR 0.21, p=0.03). Aortic annular dimensions, graft size, and other repair factors showed no association. Mean aortic gradient on discharge predicted the composite outcome (OR 1.17, p=0.02) and moderate AS/AR at follow-up (OR 1.35, p=0.04).
CONCLUSIONS: While commissural orientation was not a significant predictor, we identified anatomical and surgical technique-related factors which were associated with negative outcomes after BAV repair. Longer follow-up and larger series are needed to confirm these findings.
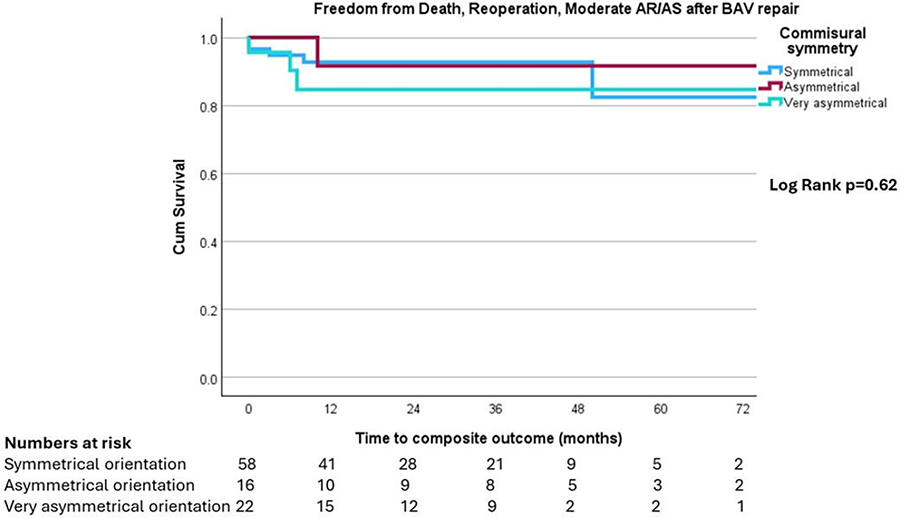
Presentation Number: P75Publishing Title: Early And Mid-term Results Following Valve-sparing Aortic Root Replacement In Type A Aortic Dissection
Author Block: Kezia Summers, George Gradinariu, Ahmed Shaheen, Ahmed Othman, Ayman Kenawy, Deborah Harrington, Jakub Marczak, Matthew Shaw, Manoj Kuduvalli, Mark Field, Omar Nawaytou.
Liverpool Heart and Chest Hospital, Liverpool, United Kingdom.
Abstract Body:
OBJECTIVE: To assess short- and mid-term outcomes of valve-sparing root replacement (VSRR) in patients with type A aortic dissection.
METHODS: Consecutive patients undergoing VSRR for type A aortic dissection were included. The primary endpoint was survival at follow-up. Secondary endpoints were 30-day survival, short-term morbidity, and freedom from valve-related reoperation.
RESULTS: From January 2019 to September 2024, 36 patients were included. 27 were males (75%) and 9 females (25%). Mean age was 50±13.17 years. 11% (n=4) had a bicuspid aortic valve, and 89% (n=32) had a tricuspid valve. All patients underwent the standard David V reimplantation procedure. 13% (n=5) required additional aortic valve repair. Acute type A dissection repair was performed in 81% (n=29) of cases, and chronic type A dissection repair in 19% (n=7). Additional procedures included total arch replacement in 25% (n=9) and hemiarch replacement with hypothermic circulatory arrest in 47% (n=17). Survival rates were 97.1% at 6 months (34/35), 97.0% at 1 year (32/33), and 95.7% at 3 years (22/23). Freedom from valve-related reoperation was 100% at all follow-up points (6 months, 1 year, and 3 years), with outcomes similar to our non-dissection cohort (p=ns). Complications occurred in 41% (n=15) of patients, including re-exploration (14%, n=5), atrial fibrillation (11%, n=4), cerebrovascular accident (17%, n=6), reintubation (8%, n=3), continuous veno-venous hemofiltration (8%, n=3), and permanent pacemaker placement (3%, n=1).
CONCLUSIONS: These midterm results support the use of valve-sparing root replacement in the setting of type A aortic dissection in selected cases. The risks of postoperative complications need to be balanced when extensive procedures are planned.
Presentation Number: P76Publishing Title: Huge Aortic Valve Mass: Rare Case Reports
Author Block: Mohammed A. Sanad.
Mansoura University, Mansoura, Egypt.
Abstract Body:
OBJECTIVE: Aortic valve bioprostheses made with heterologous tissue are prone to degeneration in adults and more rapidly in young patients. The major mechanism of degeneration is the immunologic reaction against xenoantigens in the graft. Young patients have both higher phosphocalcic metabolism and more reactive immune systems. The Ozaki procedure involves templated creation of new autologous aortic valve leaflets from the patient’s pericardium Short and mid-term clinical and echocardiographic results of Ozaki technique are promising.
METHODS: On-pump aortic valve neocuspidization was urgently performed via full sternotomy. The aortic root sinuses of Valsalva space were nearly occupied by a reddish shreddy mass attached to all of the three AV leaflets with near total obstruction of the valvar orifice. Dissection of the AV mass en-bloc with excision of the AV leaflets and dissection of the mass from the AMVL were done. Aortic valve leaflets were fashioned via treated autologous pericardium using the standard technique of Ozaki aortic neocuspidizaiton.
RESULTS: AV-Neo was performed: R: 23 mm L: 23 mm N: 23 mm Post procedure TEE: AR: none - Coaptation: 15 mm - PPG: 10 mmHg - MPG: 7 mmHg - EF: 60% - FS: 40% EDD: 42 mm ESD: 30 mm Uneventful postoperative course. Pathology revealed Libmann-Sack`s Endocarditis (NBTE) with no atypical or malignant cells.
CONCLUSIONS: Libman-Sacks endocarditis describes a broad spectrum of immunological pathologies ranging from very small particles to large vegetations on normal heart valves (mostly aortic and mitral). Ozaki Procedure is a surgical procedure that is used to treat people with aortic valve pathologies with good short and midterm results. it is a good alternative for AVR for Libman Sacks endocarditis as it evades risk of immune degeneration, thrombogenicity as compared to xenografts or mechanical valves.
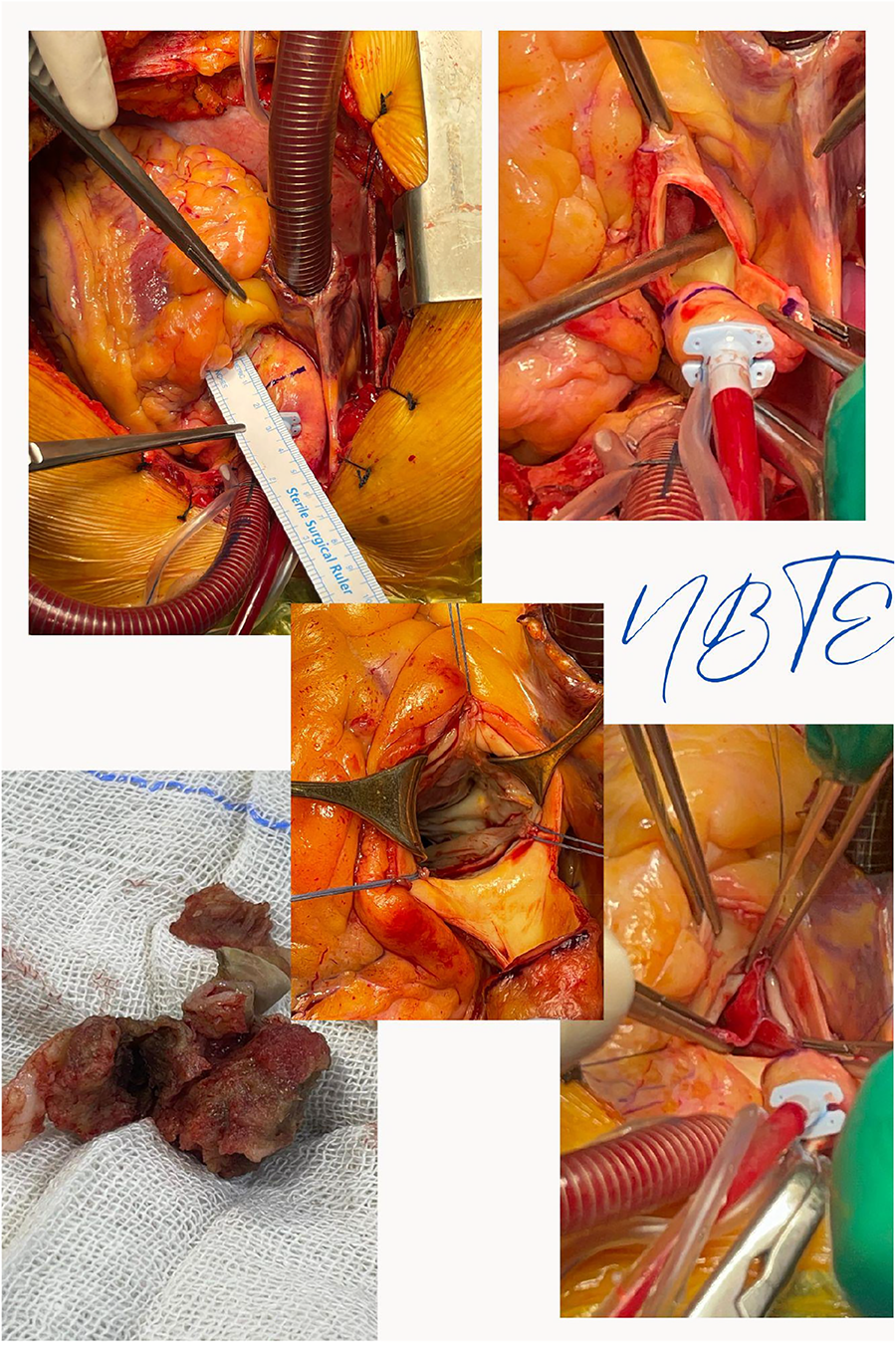
Presentation Number: P77Publishing Title: Influence of the Incision in the Lower Part of the Valsalva Graft in David-type Reimplantation Surgery
Author Block: Hiromasa Kira, Takehiko Matsuo, Takahide Takeda, Fumie Takai, Masahide Kawato, Kazuhiro Takatoku, Yasuyuki Fujimoto, Haruka Fujimoto, Ryo Nakanishi, Kazuyoshi Kanno, Tadashi Ikeda, Kenji Minatoya.
Kyoto University Hospital, Kyoto, Japan.
Abstract Body:
PURPOSE: We experienced several cases of relativelyearly recurrence of aortic regurgitation (AR) after valve sparing rootreplacement (VSRR, reimplantation), which raised the suspicion of annularenlargement at the time of reoperation. When a Valsalva graft was used, weinvestigated whether an incision was made in the lower part of the graft toalign the top of the original valve commissure with the sinusoidal junction ofthe graft, which would affect the recurrence of AR.
SUBJECTS AND METHODS: We retrospectively compared 32cases who underwent VSRR between October 2016 and March 2024, with 15 cases whohad an incision made at the bottom of the graft (Group A) and 17 cases who didnot have (Group B).
RESULTS: The average age of Group A was 51.6 years, with 46.6% having connective tissue abnormalities and 6.2% having bicuspidvalves, while the average age of Group B was 53.2 years, with 47.0% havingconnective tissue abnormalities and 0% having bicuspid valves (p=0.78, 1.00,0.21). The preoperative Ventriculo-aortic junction (VAJ) diameter, the diameterof the graft used, and the postoperative VAJ diameter were 25.0 mm, 27.3 mm, and 20.5 mm in Group A, and 26.0 mm, 27.7 mm, and 20.6 mm in Group B (p=1.00,0.51, 0.76), respectively. There were no cases in either group with more than moderateAR at the discharge. The recurrence-free rate for more than moderate AR was 74%in Group A and 88% in Group B at 3 years (p=0.36), and 59% in Group A and 88%in Group B at 4 years (p=0.16).
CONCLUSIONS: There was no correlation between early ormid-term AR recurrence and incision of the lower part of the graft. Despite ofthe incision, the size of the VAJ was reduced and stabilized.
Presentation Number: P78Publishing Title: Anomalous Circumflex From The Right Sinus During Redo Root Replacement After Previous Limited Dissection Repair
Author Block: Eric E. Roselli.
Cleveland Clinic, Cleveland, OH, USA.
Abstract Body:
OBJECTIVE: To demonstrate managing an anomalous circumflex from the right sinus of Valsalva during root replacement.
METHODS: Pt is a 62y/o one year post limited ascending replacement for acute type A dissection now with severe aortic regurgitation and root aneurysm noted to also have a large circumflex artery originating in the right sinus that is also aneurysmal.Redo sternotomy was performed, coronaries were all mobilized extensively including the circumflex artery throughout its course behind the aortic root. Biologic Bentall procedure is performed with three coronary buttons - LAD, Cx transposed above the STJ, and RCA.
RESULTS: Patient tolerated the procedure well with widely patent coronaries.
CONCLUSIONS: Anomalous circumflex from the right sinus of Valsalva can be be addressed with an in-situ reconstruction in patients requiring root replacement surgery.
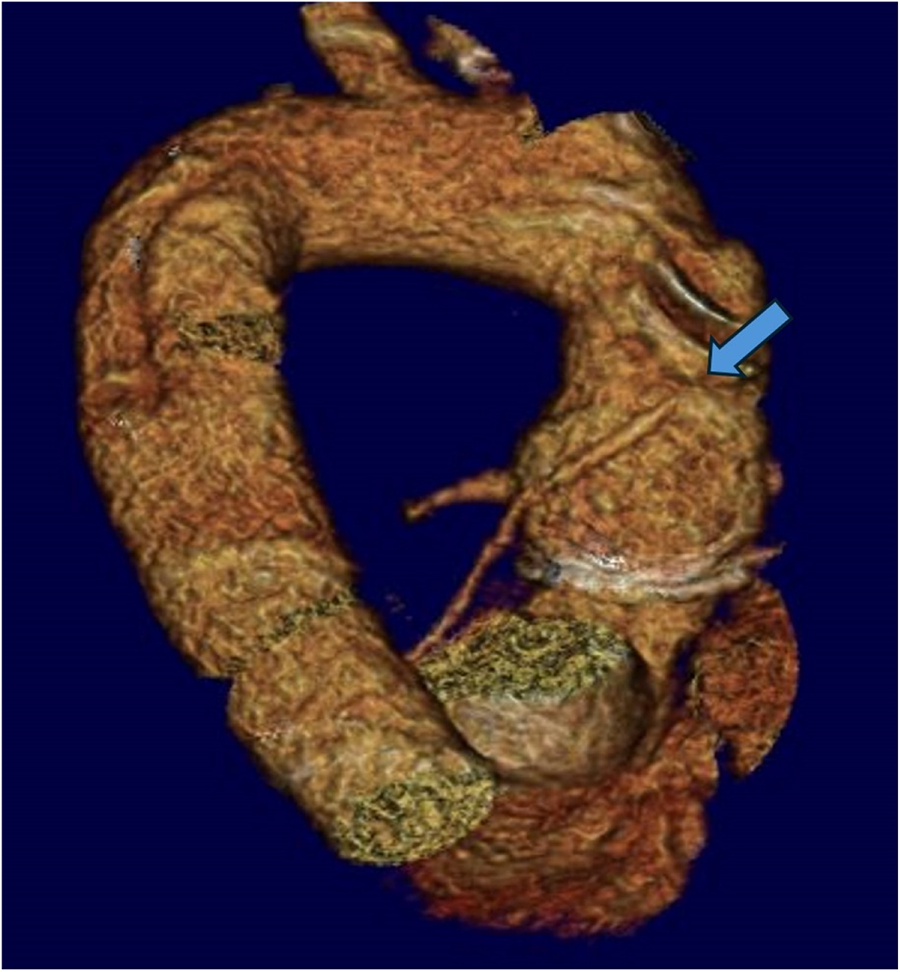
Presentation Number: P79Publishing Title: How To Deal With Congenitally Abnormal Supra-commissural Left Coronary Ostia During Aortic Valve-sparing Procedure?
Author Block: Luca Zanella1, Gebrine El Khoury2, Laurent De Kerchove2.
1University of Bologna; Cliniques Universitaires Saint-Luc, Université Catholique de Louvain (UCL), Bologna; Brussels, Italy, 2Cliniques Universitaires Saint-Luc, Université Catholique de Louvain (UCL), Brussels, Belgium.
Abstract Body:
OBJECTIVE: The left congenitally abnormal supra-commissural coronary ostia is a rare condition. However, it could be a challenge during aortic valve-sparing surgery. This manuscript aims to suggest how to deal with this.
METHODS: The technique is presented through an emblematic case of a 25-year-old male with severe aortic insufficiency and congenitally abnormal supra-commissural left coronary ostium in a tricuspid aortic valve. The surgery consisted of a valve-sparing aortic root surgery and aortic valve repair. The graft used for the root replacement was cut accurately in correspondence with the supra-commissural coronary ostium to let it settle inside a hole at the top of the incision without distortions. The stitches at the level of the ventricular-aortic junction embraced the abnormal coronary ostium. They were placed on either corresponding side of the vertical incision on the graft. Then, they were tied to close the gap on the dacron graft, passing one of the two arms of the suture under the coronary trunk to join the other arm. Moreover, reimplantations of both the valve and the misplaced ostium were performed following their contours. In addition, shaving and plications of the aortic cusps were performed. Finally, an external aortic annuloplasty was carried out.
RESULTS: Post-operative echocardiography showed a good result of the surgery. The patient experienced a full recovery from the intervention. At our institution, three patients presented with left congenitally abnormal supra-commissural coronary ostia. They were all treated with aortic valve-sparing root replacement using the technique described, with good results.
CONCLUSIONS: The left congenitally abnormal supra-commissural coronary ostia should not be a contraindication for the valve-sparing aortic root surgery, because it could be managed with a modified technique of implantation of the graft used for the root replacement. Further studies are required to verify the long-term outcome of this kind of surgery.
Presentation Number: P80Publishing Title: Results Of Continuous Suturing For Bentall Operation
Author Block: Sepideh Banar, Saeid Hosseini, Alireza Alizadeh Ghavidel, Hamideh Khesali, Soheila Salari, Zahra Ghaffarinejad, Asal Karimi, Maryam Pourmojib.
Rajaie Cardiovascular Medical and Research Center, Tehran, Iran, Islamic Republic of.
Abstract Body:
OBJECTIVE: This study aims to evaluate the safety and efficacy of the continuous suturing (CS) technique in the Bentall procedure by analyzing postoperative complications, particularly bleeding, in a large patient cohort. Additionally, this study seeks to provide a detailed description of the CS technique to assess its advantages over the traditional interrupted suture method in heart valve surgery.
METHODS: We conducted a retrospective analysis of 468 consecutive patients who underwent the Bentall procedure using the continuous suturing technique at a single medical center from April 2004 to December 2022. Clinical outcomes were assessed, with a particular focus on postoperative complications such as bleeding. Additionally, 221 patients (47.2%) in the cohort underwent concomitant procedures alongside the Bentall operation. Data were extracted from electronic medical records, and outcomes were analyzed to evaluate the safety and efficacy of the continuous suturing technique in this patient population.
RESULTS: A total of 468 patients were included in the study, with a mean age of 45.5 ± 14 years, and 392 patients (83.7%) were male. The mean aortic cross-clamp time for the pure Bentall procedure was 84.2 minutes. Among the patients who underwent concomitant procedures, the most common interventions included mitral valve repairs, coronary artery bypass grafting, and aortic arch surgeries. Notably, in-hospital mortality was recorded in 8 patients (1.3%) within the pure Bentall procedure group, indicating a favorable safety profile for the continuous suturing technique.
CONCLUSIONS: The continuous suturing technique utilized in the Bentall procedure demonstrated a low in-hospital mortality rate, reflecting its safety and effectiveness in a diverse patient population. The technique also allowed for efficient surgical performance, even when combined with other cardiac procedures. These findings support the integration of continuous suturing into clinical practice, highlighting its potential to enhance surgical outcomes and reduce complications in patients undergoing cardiac surgery.
Presentation Number: P81Publishing Title: Mid-term Results Of New Heart Valve Tissue Bioprosthesis For Pulmonary Valve Replacement
Author Block: Gianluigi Perri1, Maria Grandinetti2, Gianluca Brancaccio1, Sergio Filippelli1, Matteo Trezzi1, Enrico Cetraro1, Francesca Graziani2, Victoria D'Inzeo1, Antonio Amodeo1, Lorenzo Galletti1.
1Bambino Gesù Children Hospital, Rome, Italy, 2Gemelli University Hospital, Rome, Italy.
Abstract Body:
OBJECTIVE: To evaluate haemodynamic performance and midterm durability of Inspiris Resilia Valve (IRV) in pulmonary position in patients with different congenital cardiac anomalies.
METHODS: We retrospectively reviewed medical records of 45 patents that underwent pulmonary valve implantation (PVI) with IRV between January 2018 and August 2023. Demographic data included primary diagnosis, age at surgery, intraoperative and follow-up data. Primary outcomes are bio-prosthesis dysfunction (BD) and prosthesis-related reintervention. BD was defined as moderate or severe bio-prosthesis insufficiency or trans-prosthesis peak gradient >50 mmHg
RESULTS: Most common primary diagnosis was Tetralogy of Fallot (26 pts) followed by pulmonary valve stenosis (10 patients). Indication to surgery was in all severe pulmonary regurgitation with severe right ventricle dilatation with mean pre-operative RVEVi of 160.8 +/- 31.3 ml/m2. Median age and weight at surgery were 18 (range 15-30) years and 62 (range 47-72) kg. All patients, except 5, underwent at least 1 previous sternotomy. Mean cardiopulmonary bypass time was 98.4 +/- 50,2 min. Follow-up data was complete in all cases (100%). The most common size of IRV implanted was 25 mm (31 pts), followed by 27 mm (11 pts). After a median time of 33 (range 18-45) mos, 6 patients (13,3%) developed BD and one needed trans-catheter reintervention. All these patients underwent implantation of IRV 25 mm size. Our statistical analysis showed that higher peak gradient and high RV systolic pressure were associated with higher occurrence of BD (p value < 0.001). Moreover, bioprosthesis regurgitation was mainly cause of BD than stenosis (p value < 0.001).
CONCLUSIONS: Despite the short-medium term follow-up, our results suggest that durability of IRV in pulmonary position is concerning. Further discussion and collaboration are needed to evaluate this prosthesis in pulmonary position on a larger scale and with a longer follow-up.
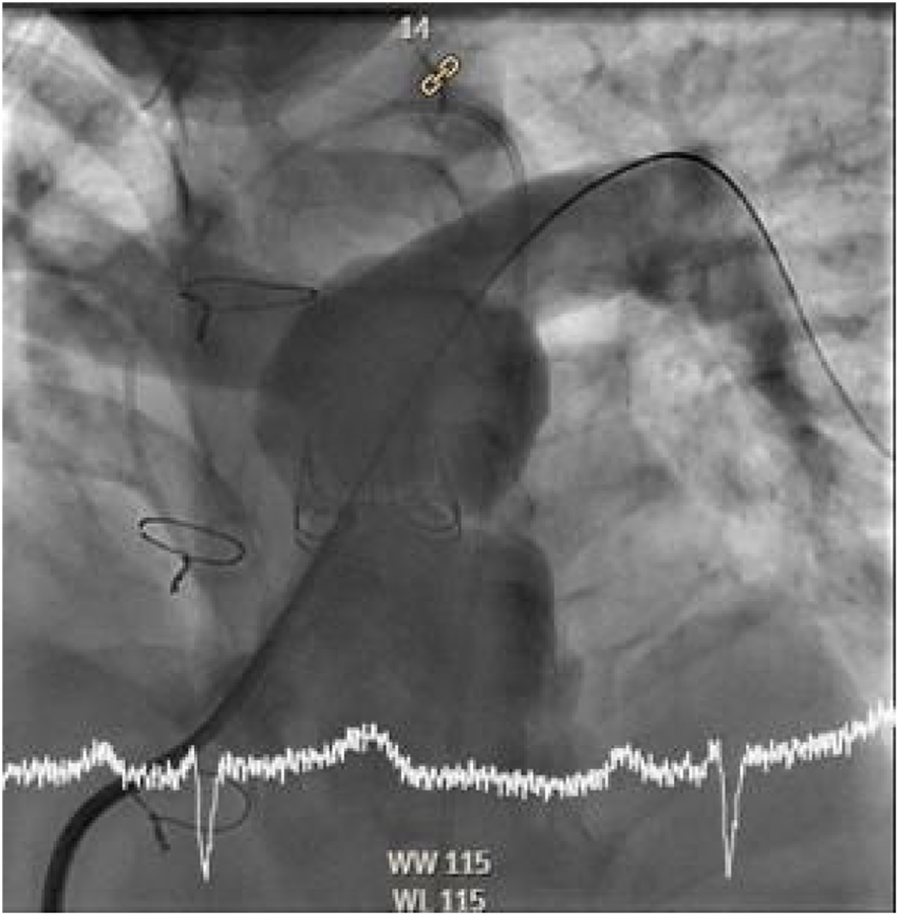
Presentation Number: T1Publishing Title: Plasma-treated Chronoflex Polyurethane Films Exhibit Superior Biocompatibility Over Carbothane For Enhanced Heart Valve Tissue Engineering
Author Block: Yasaman Zamani, Farhad Sadeghi, Arash Kheradvar.
University of California, Irvine, Irvine, CA, USA.
Abstract Body:
OBJECTIVE: Current research in heart valve engineering faces challenges in finding materials that balance biocompatibility and mechanical durability. An ideal material has yet to be established. In this study, we aimed to evaluate the biocompatibility of two polycarbonate polyurethane resins, Carbothane (CB) and Chronoflex (CF), as potential materials for heart valve leaflets. We focused on cytotoxicity, cell proliferation, and the effects of plasma treatment.
METHODS: Two types of polycarbonate polyurethane resins, namely Carbothane (CB) and Chronoflex (CF) films, were used in this study as potential materials to be used as heart valve leaflets. Cytotoxicity of the films was studied using L929 cells. The CB and CF films were plasma treated and Normal Human Lung Fibroblasts were seeded on the films. Cell proliferation was studied after 7 days of culture. Live/dead staining was performed after 3 and 7 days of culture.
RESULTS: For both the CB and CF films, cell viability was higher than 70%, which is the acceptable range for cytotoxicity measurement. There was no significant difference in cell viability between CB and CF films. Only the plasma-treated CF sample showed increased cell proliferation from day 1 to day 7. For all other samples, there was no significant increase in cell number from day 1 to day 7. A more homogeneous distribution of live cells was observed on the plasma-treated CF film compared with the other samples. Cell aggregates were only observed on CB film.
CONCLUSIONS: The absence of cell aggregates on the CF film compared to the CB film suggests better surface characteristics and cell-material interactions for CF after plasma treatment. The findings of this research indicate that plasma-treated CF films may provide a more favorable environment for cell proliferation and distribution, which is crucial for developing tissue-engineered heart valves.
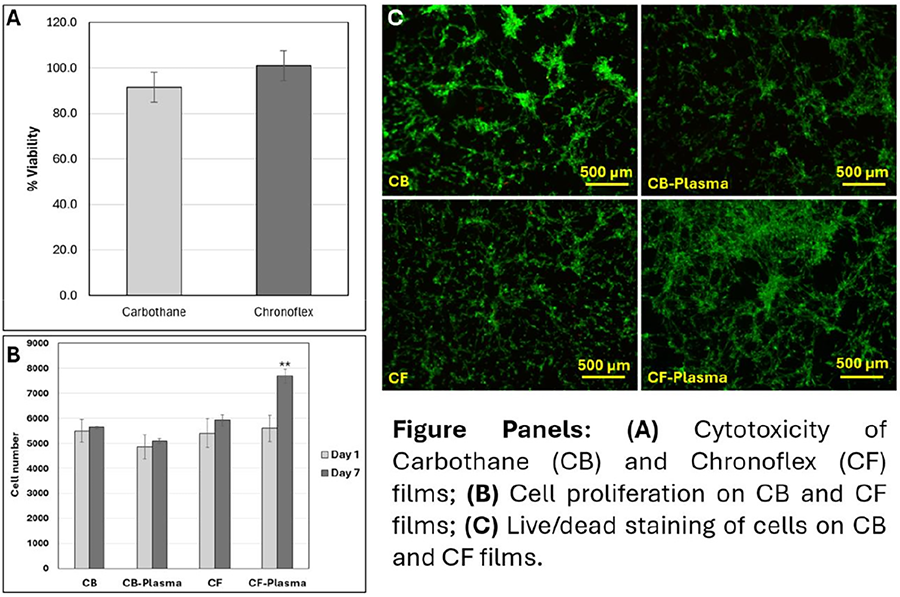
Presentation Number: T2Publishing Title: Biomechanical And Degradation Characteristics Of A Bioresorbable Heart Valve Replacement
Author Block: Julia R. Toma, Sanchita S. Bhat, Ph.D, Lakshmi Prasad Dasi, Ph.D.
Georgia Institute of Technology, Atlanta, GA, USA.
Abstract Body:
OBJECTIVE: Pulmonary atresia, affecting 1 in 7000 live births, is a congenital heart defect lacking long term solutions. Current percutaneous treatments to restore flow in fetal and neonatal patients have high re-intervention rates, and subsequent pulmonary valve replacements have limitations regarding size, availability, and durability. Tissue engineered heart valves have grown in popularity to treat valvular diseases due to regenerative and remodeling capabilities-properties necessary to address the needs of fetal and neonatal patients. This study aims to manufacture and characterize degradation and biomechanical properties of a bioresorbable heart valve replacement.
METHODS: Valve prototypes (N=2) were manufactured using previous methods,1 and a bio-resolvable polymer stent (polycaprolactone, PCL). They underwent accelerated degradation in a sodium hydroxide (NaOH) solution to analyze degradation patterns, which will inform design modifications for the stent and leaflets. Prototypes were removed from this solution every 24 hours to measure weight loss and qualitatively assess degraded regions. PCL samples were made using established1 leaflet concentrations-0.75% PCL and 5% PCL in chloroform. N = 2 were degraded in NaOH to the following time points: 2.5h, 4h, 18h, and 24h. They were further subjected to biaxial testing and microscopic analysis using scanning electron microscopy (SEM).
RESULTS: Observations indicated degradation of the valve began at leaflet commissures, with only the 5% PCL skirt remaining intact after 72 hours. Total mass loss was 45% (+/- 4%). Biaxial testing showed peak stiffness at 4 hours and a noticeable loss of mechanical properties in 0.75% PCL as degradation time increased. Ongoing microscopic analyses will provide insight to microstructural changes.
CONCLUSIONS: This study will provide insight into design considerations of a bioresorbable heart valve replacement by improving the understanding of (1) manufacturing techniques to optimize degradation patterns and (2) microstructural and biomechanical changes of polymer leaflets.
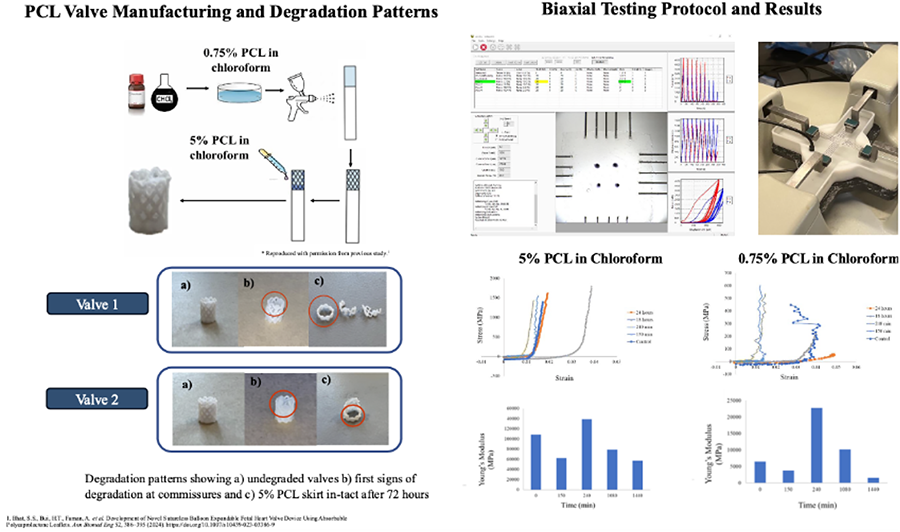
Presentation Number: T3Publishing Title: Characterization And Clinical Applications Of Controlled Cross-linked Bovine Pericardial Bio-patches And Artificial Heart Valves
Author Block: Tongtong Wu, Can Jin, Xiaoxue Zhang, Tiwen Li, Yingjie Wang, Yuxin Wang, Congchong Chen, Liyan Li, Jia Wu, Kangjian Wu, Lei Jin.
Beijing Balance Medical Technology Co., Ltd, Beijing, China.
Abstract Body:
OBJECTIVE: Over recent years, research on biomedical materials have focused on ensuring biological safety and enhancing efficacy in tissue and organ repair through the development of advanced biomaterials. However, there is a translational gap between fundamental research and clinical practice due to the variation and specificity of biomaterials. We admitted and developed controlled cross-linked acellular bovine pericardial (CCABP) bio-patches and heart valves at large industry scale, which have been successfully applied in neurosurgery, thoracic surgery, hernia surgery, cardiovascular surgery, and etc, for over 20 years. Here we comprehensively described the features of those biomaterials and the state-of-art engineering strategy as an approach for clinical applications.
METHODS: A controlled cross-linked technique was utilized to process the CCABP bio-patches and heart valves. The resulting biomaterials were characterized by various methods, including histochemistry, SEM, TEM, thermal shrinkage temperature, melting point, tensile test, FTIR, UV, and LC-MS. A side-by-side comparison of anti-calcification property was conducted in an animal model for CCABP materials and glutaraldehyde cross-linked materials used as heart valves. Furthermore, clinical safety and effectiveness data were collected and summarized for the CCABP based medical devices applied in clinic.
RESULTS: The CCABP bio-patches and heart valves exhibited unique physical and chemical properties suitable for corresponding clinical applications. The CCABP heart valves showed the highest mechanical strength followed by CCABP cardiac, hernia/ thoracical, and neurosurgical patches, respectively. The crosslinked sites within CCABP materials exist not only intra and inter collagen molecules but also among collagen and other extracellular matrix components. This crosslink feature resulted in a significant enhancement of anti-calcification property in a subcutaneous rat model. Moreover, the safety and effectiveness profiles were also proved clinically for the CCABP bio-patches and heart valves.
CONCLUSIONS: These CCABP materials performed excellent physical, chemical and biological features suitable for soft tissue repairing in various implantation sites clinically.
Presentation Number: T4Publishing Title: Interaction Between Scaffold Degradation And Propensity Of Calcification In Tissue Engineered Heart Valves - An In Vitro Study.
Author Block: Claudia Zacchini, Dewy van der Valk, Anthal I.P.M. Smits, Carlijn V.C. Bouten.
Eindhoven University of Technology, Eindhoven, Netherlands.
Abstract Body:
OBJECTIVE: In situ heart valve tissue engineering offers an alternative to mechanical and bioprosthetic valves by creating living, adaptable prostheses capable of growth. Electrospun synthetic scaffolds promote tissue regeneration at the implantation site by triggering a wound-healing response, facilitating immune cell infiltration, recruitment of tissue-producing cells, and regeneration of functional, native-like tissue. A crucial requirement is balanced scaffold degradation over time, allowing healthy new tissue to form while preventing chronic inflammation and fibrosis. The latter aspects are linked to calcification in living valves, such as calcific aortic valve disease, making tissue-engineered heart valves (TEHVs) potentially susceptible to calcification. Indeed, minor degrees of calcification have been observed in over one-third of preclinical animal models to test TEHVs. The present study aims to explore the relationship between scaffold degradation and calcification, specifically examining whether scaffold degradation byproducts contribute to a pro-calcific environment.
METHODS: Electrospun polycaprolactone-bis urea (PCL-BU) scaffolds, successfully used for TEHVs, and PCL controls, are seeded with induced pluripotent stem cell-derived smooth muscle cells (ivSMCs, the precursors of valvular cells), cultured to mimic the onset of calcification. This is combined with hemodynamic loading and scaffold degradation using enzymatic methods. Analyses include neo-tissue formation and inflammation (qPCR, immunofluorescence, matrix assays), calcium assays, and quantification of scaffold degradation (physical (fiber morphology, mass loss, scaffold thickness) and mechanical properties (biaxial tensile testing)).
RESULTS: Initial experiments focus on determining whether enzymatic degradation using lipase is suitable to accelerate in vitro scaffold degradation and if the enzyme affects calcification. Validating (accelerated) in vitro degradation against in vivo scaffold resorption will provide insight in the physiologically relevance of the model.
CONCLUSIONS: This study aims to enhance understanding of the interaction between scaffold degradation and calcification. The findings could advance new strategies to prevent calcification in TEHVs applications, improving their long-term functionality.
Presentation Number: T5Publishing Title: Comparison Of Biomechanical And Hydrodynamic Properties Of Tissue Engineered Heart Valve To Bovine And Porcine Pericardium Tissue Valves
Author Block: Jacob Benkofske, Abrielle Prunty, Mariah McMahon, Rick Murphy, Jeffrey Lawson, MD PhD, Zeeshan Syedain, PhD.
Vascudyne Inc., St. Paul, MN, USA.
Abstract Body:
OBJECTIVE: Tissue engineered heart valves (TEHV) offer the potential for lifelong durability compared to current animal derived tissue valves. Engineered tissue is capable of recellularizing, remodeling, and repairing to maintain mechanical integrity and resist calcification. However, to ensure engineered tissue has initial mechanical durability to withstand early performance in vivo, reference biomechanical properties should be established.
METHODS: Using fixed bovine and porcine pericardium as a reference, this study measured biaxial tensile properties and suture retention using an Instron tensile testing system to compare against engineered tissue created in a bioreactor using cell produced extracellular matrix. Additionally, trileaflet valves of identical designs were manufactured using porcine fixed pericardium and engineered tissue and hydrodynamically tested in pulse duplicator system to evaluate performance.
RESULTS: Each valve was imaged using Faxitron (Figure a-f) showing no major calcification. Calcium content was measured through mass spectrometry quantification. Preimplant tissue had a value of 0.181μg/mg dry weight. Explants at 18 months had average values of 0.141 and 0.158μg/mg dry weight indicating no significant increase in calcium content (Figure g). After 18 months, evidence of regeneration through endothelial coverage was observed in significant portions of the conduit with lack of endothelialization visualized only in localized inflammation or thrombus-attached areas (Figure h-j). Analysis showed interstitial cell migration from root into leaflets and full cellularization by interstitial cells in tissue within the frame (Fig k-n). There was evidence of elastin deposition near leaflet roots which potentially indicates healthy regeneration rather than fibrotic tissue formation, as seen with fixed pericardium leaflets.
CONCLUSIONS: Tissue engineered pulmonary valve derived from human cells has been shown to allow for endothelization and reduce immunological response that can lead to deterioration and calcification. These implant results suggest the material has potential to regenerate and provide longer-term solution for younger patients.
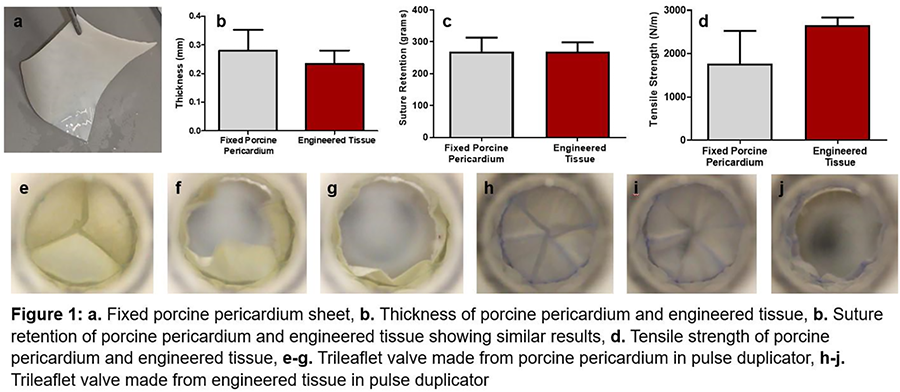
Presentation Number: T6Publishing Title: Development And Evaluation Of Self-tissue Engineered Artificial Heart Valves For Congenital Heart Disease
Author Block: Yusuke Inoue, Yasushi Sato, Takeshi Terazawa, Yuuki Yoneda, Kento Yamada, Yoshiaki Takewa.
Asahikawa Medical University, Asahikawa, Hokaido, Japan.
Abstract Body:
OBJECTIVE: We have developed the Biovalve, an artificial valve with high anti-thrombogenicity and durability, which can be fabricated in any shape required by the patient and rarely causes immune rejection because it is made from autologous tissue. The purpose of this study was to implant the Biovalve as a pulmonary artery valve in large animals and to evaluate its safety and efficacy.
METHODS: The Biovalve is fabricated using the encapsulation phenomenon in living organisms. The mold was implanted subcutaneously and removed 3 months to obtain the Biovalve. A self-expandable stent is inserted into the gap between the molds to obtain a stent-integrated valve. An adult goat weighing about 60 kg was implanted with the Biovalve catheterically at the pulmonary artery valve site through the apex of the heart under X-ray guidance, and the patient was followed up for 6 months. No anticoagulation therapy was administered during follow-up.
RESULTS: Two animal studies were performed and completed at 6 months. No significant regurgitation or incidents occurred. Anatomic findings showed no thrombus or inflammation in the Biovalve. Histologic evaluation revealed donor recellularization of the Biovalve and no calcification.
CONCLUSIONS: The Biovalve functioned as a pulmonary artery valve for 6 months, allowing us to evaluate its efficacy and safety. Future studies will extend the number of experimental cases and the duration of the experiments to evaluate the longer-term durability and growth potential of the Biovalve.
Presentation Number: T7Publishing Title: Meso-scale Topological Cues To Promote Endothelial Cell Proliferation On Macro-scale, Blood-contacting Polymeric Substrates
Author Block: Marta Baccarella1, Federica Cosentino2, Pietro Terranova2, Marianna Barbuto1, Enrica Romano1, Vincenzo La Carrubba3, Francesco Lopresti3, Claudio Arnone4, William R. Wagner5, Antonio D'Amore6.
1University of Palermo and Fondazione Ri.MED, Palermo, Italy, 2Fondazione Ri.MED, Palermo, Italy, 3University of Palermo, Palermo, Italy, 4Microtech srl, Palermo, Italy, 5Departments of Surgery, Bioengineering, University of Pittsburgh, Pittsburgh, PA, USA, 6McGowan Institute for Regenerative Medicine, University of Pittsburgh, Pittsburgh, PA, USA.
Abstract Body:
OBJECTIVE: Mesoscopic-topological-cues are a challenging and promising alternative to promote a stable endothelial cell layer formation able, long-term, to impact the thrombogenicity of medical devices. The use of polydimethylsiloxane (PDMS)-micropatterned-films and substrates has shown limitations, such as slow degradation rate, low surface-to-volume ratio, low permeability, and a rather limited scalability which all affected biocompatibility. In this preliminary study, we introduce a hybrid lithography/electrodeposition method to fabricate permeable, large, fiber-based substrates with mesoscale patterns putatively able to mimic basement membrane and promote functional endothelium formation.
METHODS: Lithography was performed through a direct-laser-writing-system(LW405E, Microtech srl) that selectively removed the photoresist and engraved the pattern on a three-layer substrate composed of soda-lime-glass, AZ1518-photoresist, and chrome. The conductive chrome-layer enabled the wafer to serve directly as a collector for the electrodeposition. The alternated conductive/non-conductive regions of the target were designed to attract the electrospun fibers selectively, processing values were investigated in the range V(Δ14kV),d(10cm),t(30min), T(22°C),HR(35%),Q(0,4ml/hr),needle(21G). Two different patterns depths were evaluated: 1µm, and 4µm. Patterns were investigated via SEM and quantitative analysis (%patterns on polymer substrate/patterns on CAD model) to prove the method capacity to prescribe a mesoscale pattern regardless of its shape: square and honeycombs both with a side of 60µm and 20µm gaps. Scaffolds were seeded with vascular smooth muscle cells to assess topological cues impact on cellular metabolic activity via Alamar blue test.
RESULTS: Qualitative and quantitative analysis of SEM images confirmed the ability to transfer a pattern geometry regardless of its shape with an accuracy of 84% and 98% respectively for 1µm and 4µm. This proprietary technique (US2024/0016983A1) demonstrates higher cellular activity than casted-non-fibrous patterns.
CONCLUSIONS: This study showed how photolithography and electrodeposition can be combined to process micro-fiber-based substrates 4cmx4cm with mesoscale-patterns of desired shape feasible for applications at organ level scale enhancing cellular viability.