
Abstract
Despite widespread use of advanced technology by children with type 1 diabetes mellitus (T1DM), there is little data on the use of diabetes technology by schools in managing T1DM in children. Four hundred seventy-six parents of school age (K-12) children with T1DM in the United States were surveyed regarding the use of diabetes technology at home and in school. Parents also answered questions regarding their experience with T1DM care in school during the prior school year. Nearly all children with T1DM (99.8%) wore a continuous glucose monitor (CGM), and 95% of parents received remote CGM data, yet only 47% of children had remote alert monitoring by someone at school who could respond to an emergency. This study explores barriers to the varied adoption of diabetes technology for T1DM care in schools and provides insight into school experiences for parents of children with T1DM.
Keywords
Introduction
Type 1 diabetes mellitus (T1DM) affects 1 in 400–600 children. 1 Wearable technology for T1DM management is expanding at a rapid pace. Continuous glucose monitor (CGM) devices are standard of care for children with T1DM and allow for tighter glycemic control with early identification of both hypoglycemia and hyperglycemia through customized alerts. 2 These devices permit remote, real-time glucose monitoring with customizable alarms via companion apps. Prior to CGM, blood glucose and A1C targets for children were higher due to the risk of hypoglycemia with tighter control, especially with younger children. 3
Children with T1DM in the school setting require appropriate support from trained staff to promote safety and learning. 2 Prior to the widespread adoption of technology in T1DM management, when compared with their healthy siblings, children with T1DM had lower academic skill ratings, poorer classroom attention, and higher rates of school absences.4,5 Both hypoglycemic and hyperglycemic episodes cause transient attention and information processing difficulties.6–13
Remote CGM monitoring allows proactive glucose monitoring without interrupting classroom instruction. Critical alerts can reach staff supervising the classroom, playgrounds, or cafeterias, and prompt intervention helps prevent emergencies and reduces class disruption. 2 The National Institute of Health and American Diabetes Association (ADA) support CGM use in schools, and in April 2025 the ADA updated its Diabetes Medical Management Plan to include the option for clinicians to indicate if remote monitoring by on-site school staff is recommended or medically necessary.14–16
We analyzed survey data from parents of children with T1DM to assess use of diabetes technology at home and in U.S. schools, to identify barriers to adopting this technology, and to better understand the school experience for parents of children with T1DM.
Methods
Study design and participants
This study is an analysis of a cross-sectional, web-based survey of parents and caregivers of school-aged children with T1DM in the United States. Eligible participants were ≥18 years old, resided in the United States, and were the parent or primary caregiver of a child with T1DM enrolled in grades K–12 during the 2023–2024 academic year.
The Naval Medical Center San Diego Institutional Review Board approved the study protocol for use of de-identified data. Because all data were anonymized prior to analysis, informed consent was waived.
Survey instrument
The survey was a 29-item questionnaire that addressed four major domains: (1) child demographics and diabetes characteristics, (2) use of diabetes technology (CGM, insulin pump, and remote alert features), (3) school diabetes care practices (school staff involvement, monitoring, and emergency response), and (4) caregiver experiences and perceptions of school support. Questions were yes/no, Likert scale, or multiple-choice with predefined response options, along with several free-text fields included to capture qualitative responses.
Survey administration
The survey was designed and conducted by the market research company dQ&A (San Francisco, CA). The survey was administered online between September 12 and October 2, 2024. Participants were recruited from two sources: (1) email invitation to dQ&A’s established national research panel of people with diabetes and their caregivers, and (2) social media posts in U.S.-based online T1DM caregiver groups on Facebook (Parents of type 1 diabetics—37,000 members, Moms of Type 1 Diabetics—32,000 members, Type 1 together—2800 members, 504-Diabetes—3700 members, FOLLOWT1Ds—953 members). Invitations contained a brief description of the study and a secure survey link. Participation was voluntary, anonymous, and uncompensated. Duplicate responses were minimized by restricting submissions from the same IP address. dQ&A did not provide funding for this work, was not involved in data analysis, and did not contribute to the article.
Data management and analysis
Survey responses were anonymized before they were released to the investigators. Responses with >50% missing data were excluded from analysis. Descriptive statistics were used to summarize child demographics, technology use, and caregiver experiences. Categorical variables were reported as counts and percentages, and continuous variables as means (standard deviations) or medians (interquartile ranges), as appropriate.
Results
A total of 491 surveys were received. Of these, 15 were excluded due to incomplete responses, leaving 476 surveys for analysis. Surveys were received through (1) dQ&A’s national research panel (n = 96) and (2) U.S.-based online caregiver communities and social media groups for T1DM (n = 380). Nearly all children with T1DM wore a CGM to monitor blood glucose levels (99.8%), and most (86%) children used an insulin pump (Table 1). While 96% of parents remotely monitored their child’s CGM while at school, only 47% of children had remote CGM monitoring by school staff (Table 1). Parents considered their children mostly independent in diabetes care in only 30% of cases (Table 1), and the majority of those (95%) were in high school (Table 2). Parents who requested remote CGM monitoring by the school were denied due to policy or liability (65.1%), staffing/time constraints (16.9%), or privacy concerns (6%) (Fig. 1). For students without remote CGM alerts at school, 153 (61.5%) were not independent in diabetes care (Table 2). Twenty percent of parents did not ask for remote CGM monitoring by the school (Table 1). Parents reported concerns about the quality of care provided by schools and the need for in-school parental support (Table 1). Most parents (88%) had to respond in person to a diabetes situation at least once in the prior year; 56% had to go more than four times, and 20% had to go at least 10 times (Table 1). Even among mostly independent students, 80% of parents still went to school at least once (Table 2). Seventy-two percent of parents specifically reported rushing to school due to a diabetic emergency in the prior school year (Table 1). Eight percent of students with T1DM changed schools due to inadequate care, and 17% of parents reported quitting a job to provide diabetes care (Table 1). More than half of parents (64%) reported helping train school staff in diabetes management to ensure their child was receiving proper diabetes care at school (Table 1). Nearly all parents (94%) worried about diabetes affecting their child’s academic performance (Table 1). Parents were least confident in the ability of someone at school to recognize hyperglycemia and hypoglycemia (Fig. 2).

School remote CGM monitoring refusal reasons n = 154. CGM, continuous glucose monitor.

Parent confidence in diabetes care at school n = 476.
Patient Characteristics and Diabetes Support at School n = 476

Missing question response in two surveys.
Excludes participants currently in kindergarten.
CGM, continuous glucose monitor; T1DM, type 1 diabetes mellitus.
Diabetes Care Support at School Based on Student Level of Independence and Grade n = 476
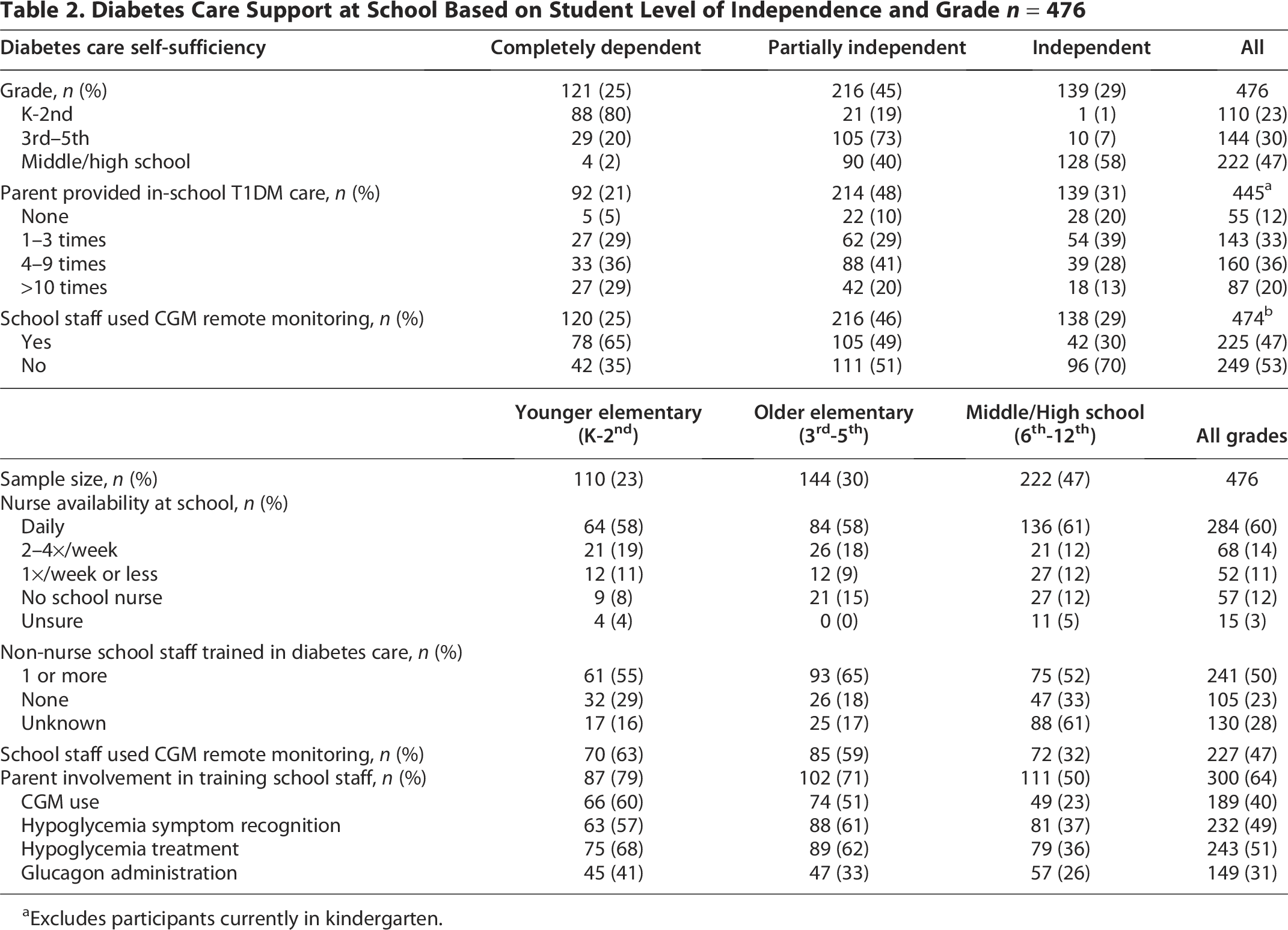
Excludes participants currently in kindergarten.
Discussion
This cross-sectional survey of parents of children with T1DM provides an updated perspective on self-reported parent experiences with school-based diabetes care across the United States. Half of students with T1DM were reported to not receive the full benefits of advanced monitoring technology in the school setting. Nearly all parents reported providing T1DM care at school during the prior school year, including for students who are independent.
School nurses report difficulties adopting CGM technology due to district policies that limit their ability to properly monitor children.18,19 Endocrinologists agree that differences in school policies and practices are a barrier to diabetes care.18,19 In schools and daycares that use CGM remote alerts, staff report increased reassurance when remotely monitoring CGM.19,20 National professional organizations have underscored the obligation of schools to provide safe and equitable care for children with diabetes. The American Academy of Pediatrics emphasizes that every child with diabetes deserves coordinated care and support within the school environment, including appropriate technology use. 21 Similarly, the ADA asserts that schools must provide safe and effective diabetes management, including access to diabetes technology. 22 The reported variability in schools’ adoption of remote CGM technology may represent missed opportunities to enable timely responses to hypoglycemia, minimize classroom interruptions, and reduce some of the parental burden of care while children are at school. There is opportunity for schools and families to work together toward integration of technology into school T1DM care.
Limitations
This survey has several limitations that should be considered when interpreting the findings. The subjective interpretation of survey questions and reliance on parent-reported outcomes may introduce reporting bias. While capturing data from most states, the total survey population was relatively small compared with the number of school-aged children with T1DM. The potential for selection bias due to recruitment from online diabetes communities may result in over- or underestimation of technology use by schools depending on which caregivers were motivated to respond. In addition, caregivers needed access to technology to complete the survey, potentially underrepresenting families without access to technology.
In addition, U.S. public schools are required to provide accommodations to students with medical needs for equal access to education, whereas private schools are not held to the same standard. Potential geographic differences exist due to varied state laws and school policies that have the potential to affect the care that can be provided. Furthermore, biases in regional sampling may limit generalizability of these findings.
Future multicenter, prospective studies with objective measures are needed to confirm these findings.
Footnotes
Acknowledgments
This study was conducted by dQ&A. The authors thank Trevor Bell, PhD, Richard Wood, and Kim Gerber of dQ&A and Kerry Murphy of FOLLOWT1Ds for contributions to survey development, data collection and their commitment to making life better for children with diabetes. dQ&A did not contribute to the drafting of this article. The authors received no payment related to the development of the article.
Authors’ Contributions
T.I.: conceptualization (equal), resources (lead), formal analysis (equal), supervision (lead), visualization (equal), writing—original draft (lead), and writing—review and editing (equal). N.R.: conceptualization (equal), visualization (equal), and writing—review and editing (equal). P.O.-R.: conceptualization (equal), formal analysis (equal), visualization (equal), writing—original draft (supporting), and writing—review and editing (equal). All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Institutional Clearance
This work has been approved for publication. PAO approval granted through Naval Medical Center San Diego.
Disclaimer
The views expressed in this article are those of the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. Government.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
The authors received no financial support related to the development of the article.
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.