
Abstract
Background
Sleep-related disorders are common among older adults with chronic obstructive pulmonary disease (COPD). Breathing exercises, a key component of pulmonary rehabilitation programs, may improve sleep quality. However, there is a paucity of research on the impact of breathing exercises on sleep quality in elderly patients with COPD.
Objective
This study aimed to compare the effects of diaphragmatic breathing (DB) and pursed-lip breathing (PLB) exercises on sleep quality in elderly patients with COPD.
Design
Crossover clinical trial.
Methods
In this study, 60 elderly patients with COPD were randomly assigned to two groups: DB followed by PLB (Group 1) and PLB followed by DB (Group 2). Each exercise was performed for 4 weeks. Participants completed the Pittsburgh Sleep Quality Index (PSQI), Abbreviated Mental Test Score (AMTS), and COPD Assessment Test (CAT) questionnaires before training. Data were analyzed using descriptive and inferential statistics in SPSS version 21, with a significance level of 0.05.
Results
Both DB and PLB exercises significantly improved sleep quality in elderly patients with COPD (P < 0.05). No significant difference was found between the two exercises. However, the sequence of exercises in Group 1 (DB followed by PLB) resulted in greater improvement in average sleep quality compared to Group 2.
Conclusion
This study demonstrates that DB and PLB exercises enhance sleep quality in elderly patients with COPD. These exercises are recommended as an effective non-pharmacological approach to improve sleep quality in this population.
Plain Language Summary
Background
Sleep-related disorders are common in older adults with chronic obstructive pulmonary disease. The breathing exercises gives some benefits to these patients. However, the literature attests to the scarcity of research on the impact of breathing exercises on sleep quality among elderly patients. This study aimed to determine the impact of breathing exercises on the sleep quality among elderly patients with chronic obstructive pulmonary disease in Guilan, the north of Iran.
Methods
In this study, a total of 60 elderly patients were assigned to two groups (group 1: 4 weeks of abdominal (diaphragmatic) breathing followed by 4 weeks of tightly pressed (pursed) lips breathing exercises; group 2: 4 weeks of tightly pressed lips breathing exercises followed by 4 weeks of abdominal breathing). After completing demographic information and questionnaires, training was conducted on how to perform breathing exercises.
Results
Both abdominal and tightly pressed lips breathing exercises individually had an effect on the sleep quality of elderly patients with chronic obstructive pulmonary disease. However, there was no difference in the impact on sleep quality between the two types of breathing exercises. Nevertheless, the arrangement of the breathing exercises in the first group, starting with 4 weeks of abdominal breathing followed by 4 weeks of tightly pressed lips breathing exercises, led to a greater improvement in sleep quality of these patients compared to the arrangement in the second group.
Conclusion
The results of this study indicated that abdominal and tightly pressed lips breathing exercises improve the sleep quality of older adults with chronic obstructive pulmonary disease.
Quick Look
Current knowledge
Chronic obstructive pulmonary disease (COPD) is more prevalent in the elderly, with a higher incidence of complications and mortality in this age group. Breathing exercises, part of lung rehabilitation programs, have garnered attention from researchers. There is a scarcity of research on the impact of breathing exercises on sleep quality in elderly patients with COPD, highlighting the need for further investigation. This study shows that diaphragmatic breathing (DB) and pursed-lip breathing (PLB) exercises improve sleep quality in elderly patients with COPD. These exercises are recommended as a non-pharmacological method to enhance sleep quality in elderly patients with COPD.
What this paper contributes to our knowledge?
Introduction
Today, a significant portion of the population consists of elderly individuals. 1 Studies have shown that chronic obstructive pulmonary disease (COPD) is more prevalent in the elderly, and the incidence of complications and mortality due to the disease is higher in this age group.2–4 COPD is characterized by progressive and irreversible airway obstruction and chronic airway inflammation. 5 One common feature in COPD patients is poor sleep quality, with over 50% of patients reporting undesirable sleep. 6 Sleep in a normal course to a certain extent impairs breathing in normal individuals. Recumbency and sleep decrease oxygen stores in the body and sleep depresses response to hypoxia and hypercapnia. In COPD, hypoxemia is more during sleep as compared to wakeful pattern. During sleep, increased hypoxemia is seen in rapid eye movement sleep. The major causes are hypoventilation, increased ventilation–perfusion mismatching, and a decrease in functional residual capacity. 7 Nocturnal dyspnea is common in COPD patients, leading to sleep disturbances and fatigue. 8 These patients often complain of sleep problems. 9 Despite this, sleep problems are often overlooked by physicians in COPD management. 10
Pulmonary rehabilitation is a crucial component of COPD management, leading to positive outcomes in patient symptoms and functioning. 11 Pulmonary rehabilitation includes chest physiotherapy techniques, such as breathing exercises, postural drainage, spirometry, clapping, vibration, and breathing techniques. 12 Breathing exercises, part of the lung rehabilitation program, offer benefits to patients with COPD, including improved breathing patterns, increased arterial oxygen saturation, and enhanced lung volumes.13,14 These exercises also improve pulmonary function, respiratory muscle strength, exercise capacity, dyspnea, and health-related quality of life in COPD patients. 15 As a complementary and non-pharmacological therapy, breathing exercises can reduce sleep deprivation and stimulate body and brain function, sympathetic–parasympathetic systems function, and relaxation. 16 Research has shown that slow, paced breathing can enhance vagal activity and improve sleep quality, particularly in insomniacs.17,18
Diaphragmatic breathing (DB) and pursed-lip breathing (PLB) exercises are two commonly used respiratory exercises that can be performed individually or in combination. 19 PLB is an important aspect of respiratory exercise training for COPD patients, promoting maximum exhalation and improving patency. 20 PLB can strengthen respiratory muscles, improve oxygen saturation, and prevent bronchiolar collapse. 13 DB increases asynchronous and paradoxical ribcage motion, which may account for the work of breathing. 12 The mechanisms responsible for the improvement in dyspnea following these exercises are not fully understood, but several hypotheses have been suggested, including reduction of minute ventilation, slowing of inspiratory flow rates, improvement of ventilation–perfusion relationships, diminution of the work of breathing, and promotion of a feeling of well-being. 21
Several studies have demonstrated the positive effects of DB and PLB exercises on patients with COPD. Yang et al. 22 found that a combination of these exercises significantly improved pulmonary function and exercise capacity in COPD patients. Izadi-Avanji and Adib-Hajbaghery 23 observed improvements in lung function and activities of daily living in COPD patients following PLB exercise. Budiman and Garnewi 24 further supported these findings, showing a significant reduction in breathlessness in COPD patients after DB exercise. However, limited research has been conducted on the effect of these exercises on sleep quality in elderly patients with COPD. Pedramrazi et al. 5 demonstrated that controlled respiratory exercises improved sleep quality in COPD patients. Given the scarcity of research on the impact of breathing exercises on sleep quality among elderly patients with COPD, particularly in Guilan province, the oldest province in Iran, this study aimed to investigate the effect of DB and PLB exercises on sleep quality in elderly patients with COPD.
Materials and Methods
Study Design, Setting, and Participants
This clinical trial employed a crossover design and was conducted between February and November 2022 at public hospitals with respiratory and internal medicine departments in Guilan, northern Iran. A total of 60 participants were recruited based on predetermined inclusion criteria and randomly assigned to one of two intervention groups: Group 1, which received 4 weeks of DB exercise followed by 4 weeks of PLB exercise, and Group 2, which received the reverse sequence.
The inclusion criteria were as follows: age 60 and older, diagnosis of COPD by a treating physician, an Abbreviated Mental Test (AMT) score of 7 or higher, a COPD Assessment Test (CAT) score of 20 or lower, and a STOP-BANG questionnaire score of 2 or lower, the ability to perform respiratory exercises, proficiency in reading and writing in Persian, no history of participation in pulmonary rehabilitation programs, no use of sleep-inducing and sedative medications, and a body mass index less than 35.
In Iran, the disease is diagnosed by a physician. Some patients visit clinics and hospitals, and after a consultation with a lung specialist physician, they are admitted to the relevant department. Some other patients visit the lung specialist's office and, after examination and spirometry, are referred to the hospital with the diagnosis of COPD. Spirometry devices are widely available in clinics and teaching hospitals in the center of Guilan province, but hospitals in the east of Guilan do not have these devices. The spirometry data of the patients are available in the lung specialist physician's office.
The exclusion criteria were: participating in similar programs during the implementation of the intervention, exacerbation of the disease, and occurrence of complications following breathing exercises. Non-cooperation of the patient to continue participating in the study, migration, and death of the patient were reasons for study withdrawal.
It is necessary to mention that, according to the evidence mentioned in the introduction, breathing exercises have no risks or complications. However, holding the breath for a long time may have side effects such as decreased lung function, decreased heart rate, accumulation of CO2 in the bloodstream, and alveolar hemorrhage, or pulmonary hemorrhage. Therefore, the assessment of the potential risks of breathing exercises in these patients was considered.
Research Instruments
The research instruments included the AMT, the CAT, the STOP-BANG questionnaire, and the Pittsburgh Sleep Quality Index (PSQI). These instruments are explained in detail below:
– AMT: This tool consists of 10 simple and short questions used to assess orientation, concentration/attention, and short- and long-term memory.
25
In this questionnaire, one point is assigned to each correct answer, and the total score is 10 points. A score of 0–3 indicates severe cognitive impairment, 4–6 indicates moderate cognitive impairment, and a score of 7 and above indicates a normal cognitive state. The psychometric properties of this test, as evaluated by Foroughan et al. in Iranian elderly individuals, resulted in a Cronbach's alpha reliability coefficient between 0.88 and 0.91.
26
– CAT: This is an assessment tool designed for the first time by Jones et al. It consists of eight questions. Each question is scored on a 0–5 scale, with a total score of 0–40.
27
Based on the obtained score, patients are placed in one of four groups in terms of the impact of the disease on their health status: low impact (CAT score 1–10), medium impact (11–20), high impact (21–30), and very high impact (31–40).
28
The psychometric evaluation of this questionnaire was conducted by Sigari et al. The Cronbach's alpha coefficient for this questionnaire was 0.87.
29
– STOP-BANG questionnaire: This questionnaire is a two-part questionnaire used to assess the likelihood of obstructive sleep apnea.30,31 The scoring system for the questionnaire is binary, with “yes” scoring 1 and “no” scoring 0. The total score can range from 0 to 8. There is a high risk of obstructive sleep apnea in patients who answer (yes) to three or more of the eight items in this questionnaire.32,33 The validity and reliability of this questionnaire were assessed in the Iranian population by Sadegh niiat-Haghighi et al.
31
– PSQI: This is an assessment tool created in 1989 by Buyss et al. at the Pittsburgh Psychiatric Institute.
34
The questionnaire originally consisted of nine items, but because question 5 includes 10 sub-items, the total questionnaire comprises 19 items. Each item is scored on a 4-point Likert scale ranging from 0 to 3.
35
The 19 self-rated items are combined to form seven component scores, each of which has a range of 0–3 points. In all cases, a score of “0” indicates no difficulty, while a score of “3” indicates severe difficulty. The seven component scores are then added to yield one “global” score, with a range of 0–21 points, “0” indicating no difficulty and “21” indicating severe difficulties in all areas.
Higher scores indicate worse sleep quality
34
(see questionnaires as Supplementary File 1).
Buysse et al. reported internal consistency with a Cronbach's alpha of 0.83 for the PSQI. 36 This questionnaire was psychometrically validated by Farrahi Moghaddam et al. in Iran, with a reported Cronbach's alpha of 0.77. 37 Hosseinabadi et al. utilized this questionnaire in an elderly population and found its reliability to be 0.74 according to Cronbach's alpha. 38
Sampling Method
A simple random sampling method was used for the selection of individuals for the two intervention groups, namely, intervention group 1 and intervention group 2. The sample size for each group was calculated based on a previous similar study,
5
considering a test power of 90% and a significance level of 0.05. According to the formula below, the sample size was initially determined to be 26 individuals for each group. Taking into account the possibility of attrition, the final sample size was determined to be 30 people for each group.


The CONSORT flowchart of participant allocation to study groups.
As shown in Figure 1, out of 95 eligible patients, 35 were excluded due to lack of inclusion criteria, death, and reluctance to follow up or cancel cooperation. Finally, 60 patients (30 in the first intervention group and 30 in the second intervention group) participated in this study.
Intervention
The intervention consisted of a combination of DB and PLB exercises. Following the random allocation of participants into the intervention groups (1 and 2), a crossover design was implemented. Here's how it was carried out:
In the initial phase, over 4 weeks, intervention group 1 engaged in DB exercise while intervention group 2 performed PLB exercise. After a suitable 1-week washout period to clear the effects of the previous exercises, during the subsequent 4-week period (from the beginning of the sixth week to the ninth week of the study), the two groups switched interventions. In other words, those in intervention group 1 received PLB exercise, and those in intervention group 2 received DB exercise (a crossover design).
A simple random selection was used to start the intervention first with DB or PLB exercises. To perform PLB, a person simply needs to breathe in nasally for about 2 s while shaping the lips as if about to blow out. Then, a person should breathe out more slowly for about 4–6 s. This technique is limited to 3–5 breaths per day. To perform this breathing exercise, the subject was asked to breathe slowly and steadily through the nose with a count of three; take the time needed to say “Smell the flower.” Then, while closing his/her lips and engaging his/her abdominal muscles, he/she should exhale slowly and with pressure. He/she was told to count slowly up to 6 to prolong the exhalation through pursed lips. The duration should be similar to saying “Blow out the candle.” DB is also known as deep breathing or slow abdominal breathing. To perform this breathing exercise, the subject was asked to place one hand on his/her abdomen, just below his/her ribcage, and the other hand on the middle of his/her chest to become aware of his/her diaphragm's position and function during breathing. He/she was told to breathe slowly and deeply through his/her nose and let his/her abdomen rise as much as possible. Then, while his/her lips are pursed, and his/her abdominal muscles are firm (contracted), exhale through his/her mouth. The subject had to do this breathing as six breaths for 6 min (each breath in one minute), and twice a day (see trial protocol and pamphlet as Supplementary File 2).
For sampling, the researcher introduced herself to the participants and explained the objectives of the research to the participants. She emphasized that participation in the research was completely voluntary. Additionally, participants were assured that their information would remain confidential, and their informed consent was obtained. Participants were also assured that they had the option to withdraw from the study if they no longer wished to participate.
To implement the intervention, patients were instructed to perform each breathing exercise for 4 weeks, totaling 8 weeks for the entire intervention period. At the end of each session, instructional contents for the breathing exercises were provided to the patients in the form of an educational pamphlet. The quality of sleep for both groups was assessed using the PSQI questionnaire before and after the intervention at two time points (once at the end of the first 4 weeks of the study and again at the end of the second 4 weeks of the study).
To ensure the proper execution of exercises by the elderly participants, they were asked to perform the exercises in the presence of the researcher, a caregiver, or a family member before being discharged from the hospital. This was done to address any issues or difficulties they might encounter. These exercises were performed in their homes after the discharge of the patients until the end of the research period. Throughout the research, daily contact was made with the patients, and their questions were addressed. Additionally, the caregiver or a family member who was part of the educational program was requested to supervise the elderly individuals' exercise routines and to communicate any questions or issues that arose during the exercises with the researcher.
Data Analysis
For assessing the homogeneity of demographic variables in the two study groups, the chi-square test was used when the variables were qualitative. In the case of quantitative variables, an independent t-test or Mann–Whitney U test was employed. To compare sleep quality before and after the intervention within each group and in each sequence separately, the non-parametric Wilcoxon test was used. To examine the effect of interventions on sleep quality, the time effect, and the interaction effect of time and intervention, a repeated measures analysis was employed. Normality was assessed using the Kolmogorov–Smirnov test. Calculations were performed considering a significance level of less than 0.05. Data analysis was carried out using SPSS software version 21. Excel software was used for drawing diagrams.
Results
The results showed that the majority of the research participants were female, and most patients fell within the age range of 60–74 years. The groups were gender-matched, with 10 males and 20 females in each group. None of the variables examined showed a significant difference between the two intervention groups (P > 0.05). In other words, the two groups were homogeneous in terms of demographic characteristics (Table 1).
Comparison of demographic characteristics of elderly patients with COPD.

Other diseases consist of stroke, thyroid disease, cancer, etc.
The results of the sleep quality assessment for both intervention groups before and after the DB exercise are presented in Table 2. In both groups, the subjective sleep quality scores showed significant improvements, with a 5% significance level in intervention group 1 and a 1% significance level in intervention group 2, before and after the DB exercise. Furthermore, the total sleep quality scores demonstrated a significant effect of the DB exercise in both groups, with a 1% significance level.
Comparison of sleep quality dimensions before and after DB exercise in two intervention groups for elderly patients with COPD.

Note. SD = standard deviation; P-value = statistical estimation.
*P < .05, **P < .001.
The results regarding the sleep quality of the two groups before and after the PLB exercise are shown in Table 3.
Comparison of sleep quality dimensions before and after PLB exercise in two intervention groups for elderly patients with COPD.

Note. SD = standard deviation; P-value = statistical estimation.
*P < .05, **P < .001.
PLB exercise had a significant effect on sleep quality in the first intervention (P < 0.001). This exercise also significantly improved sleep latency in the second group (P < 0.01). Furthermore, PLB exercise had a significant effect on sleep duration in the first group (P < 0.05). Overall, this exercise significantly improved sleep quality in both groups, with a greater effect observed in the first group (P < 0.001) compared to the second group (P < 0.05).
The mean and intervention effect size, period, and the interaction effect of period and intervention on the sleep quality of elderly patients with COPD based on a cross-over study design were investigated, and the results are reported in Tables 4 and 5 and Figures 2 and 3.
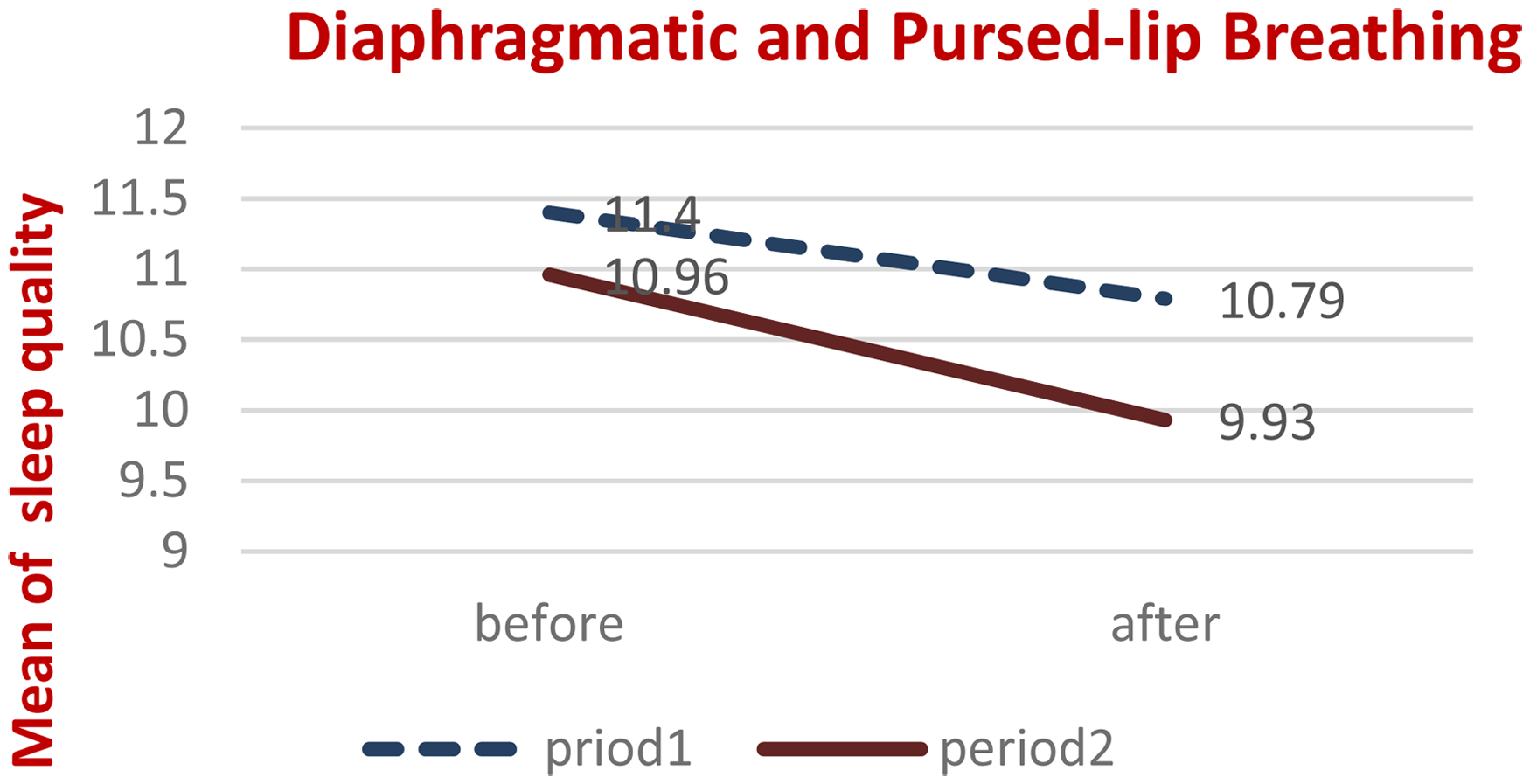
Mean sleep quality of elderly patients with COPD before and after intervention, in two separate periods, for the first intervention period (DB followed by PLB).
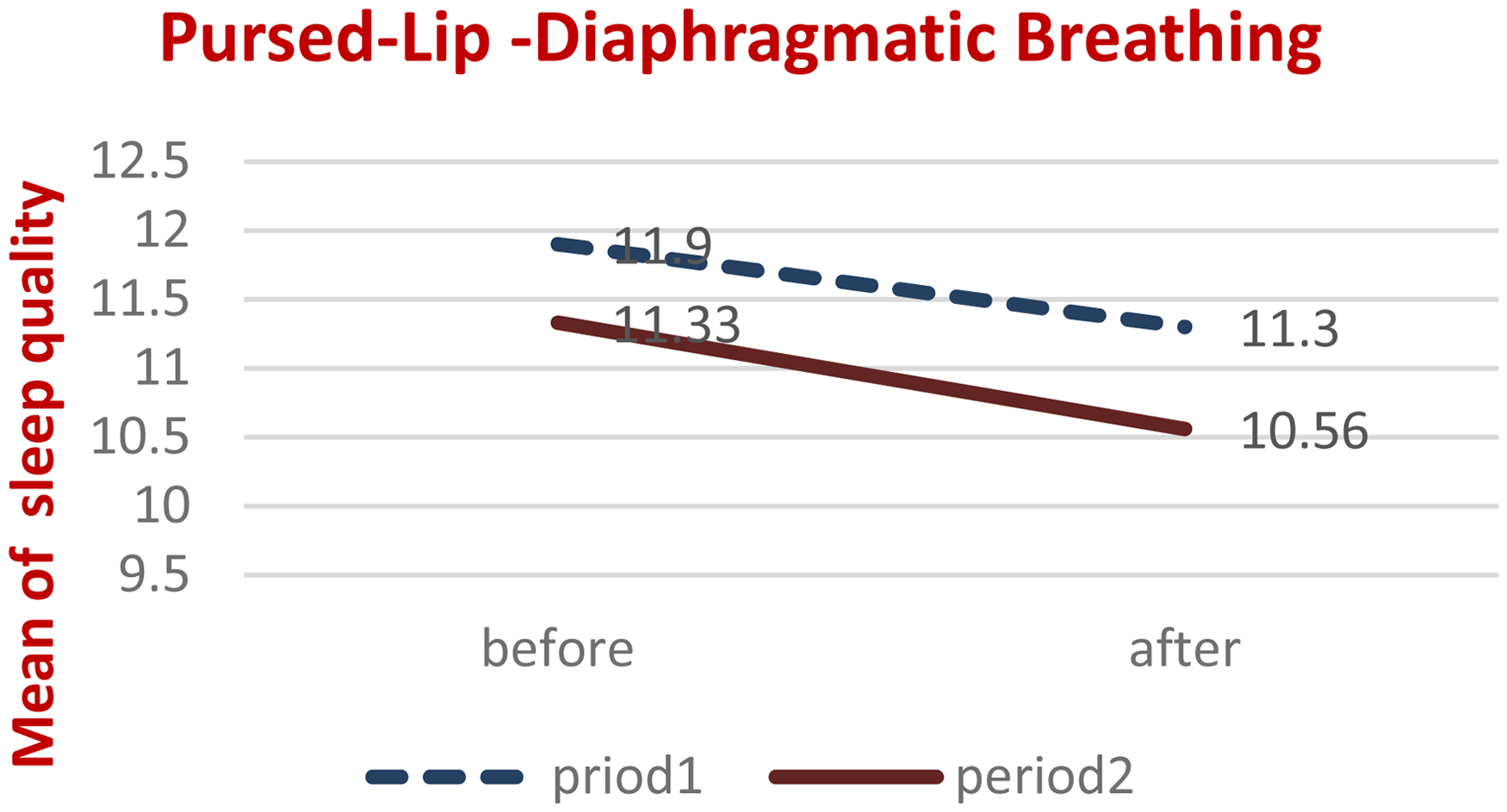
Mean sleep quality of elderly patients with COPD before and after intervention, in two separate periods, for the second intervention period (PLB followed by DB).
Mean and effect size of intervention (respiratory exercises), period, and the interaction effect of period and intervention on sleep quality in elderly patients with COPD.

Note. SD = standard deviation; df = degrees of freedom; P-value = statistical estimation.
*P < .05.
Mean and standard deviation of sleep quality in intervention groups.

Note. SD = standard deviation; SE = standard error.
Based on the results of Table 4, there was no statistically significant difference at a 5% level between the two methods of DB and PLB exercises on the sleep quality of hospitalized elderly patients with COPD. Different breathing exercises had no different effects on the sleep quality of elderly patients with COPD. However, the interaction effect of the intervention method with time was found to be significant in affecting the changes in the sleep quality of the study participants. In other words, the order of implementing respiratory exercises impacts the sleep quality of hospitalized elderly patients with COPD. Table 5 reports the mean and standard deviation of sleep quality in the first and second intervention groups.
The mean and standard deviation of changes in sleep quality within each group were calculated as follows:
As shown in Figures 2 and 3, the mean sleep quality of elderly patients with COPD improved significantly after both intervention periods. Specifically, the mean sleep quality score decreased from pre-intervention to post-intervention in both the first and the second periods. This suggests that both sequences of exercises were effective in improving sleep quality in this population.
Discussion
This study aimed to investigate the effect of respiratory exercises on the sleep quality of elderly patients with COPD. The results showed that DB exercise significantly improved sleep quality in both intervention groups 1 and 2. This finding is consistent with previous studies that have reported poor sleep quality in individuals with chronic respiratory diseases. In Nobesch et al., Soler et al., and Lan et al., most individuals with chronic respiratory disease had poor sleep quality.9,10,40 Additionally, the severity of insomnia in elderly patients with COPD has been found to be at a moderate level. 41
The results of this study are also in line with previous research that has demonstrated the positive effects of DB exercise on improving sleep quality in patients with COPD. For instance, Lan et al. 10 found that respiratory exercises were effective in improving sleep quality, increasing sleep duration, and reducing sleep disturbances in patients with COPD. Similarly, Nobesch et al. 40 reported that a gradual-intensity pulmonary rehabilitation program could be beneficial in improving sleep quality and reducing daytime sleepiness in COPD patients. Oh et al. investigated the effects of respiratory rehabilitation programs on sleep quality in elderly individuals with COPD and found that respiratory rehabilitation significantly improved sleep quality in patients with COPD. 42 Furthermore, studies have shown that pulmonary rehabilitation programs can enhance sleep quality in patients with COPD. 10 Similarly, respiratory exercises have been found to have a positive effect on improving sleep quality in hospitalized patients. 16
However, the findings of this study are not consistent with the results of McDonnell et al., who found that pulmonary rehabilitation had no impact on improving sleep quality in patients with COPD. The reason for this discrepancy may be due to the strong correlation between sleep quality, health status, and depression scores in the study's entry, which raised the expectation that if the quality of life or mood also improved in the intervention group, sleep might also improve. 43
The results regarding determining and comparing the sleep quality of elderly patients with COPD in two intervention groups 1 and 2 before and after PLB exercise showed that, in general, considering all dimensions of sleep quality, both intervention groups 1 and 2 had inadequate sleep quality before PLB exercise. Regarding the impact of PLB exercise on improving the sleep quality of elderly patients with COPD, the results of the present study are consistent with findings from other research. In a study by Zuriati et al., it was found that PLB combined with tripod positioning in COPD patients can increase oxygen saturation and reduce breathlessness. 44 In a study by Serçe et al., the results showed that PLB and DB exercises are effective in reducing sleep apnea in patients with obstructive sleep apnea syndrome. 45 Furthermore, the results of this study support previous studies that have demonstrated the positive effects of PLB on increasing oxygen saturation, 46 improving functional capacity, 47 reducing breathlessness, 48 and decreasing fatigue 49 in patients with COPD.
The findings of this study also demonstrated that different respiratory exercises (DB and PLB) did not have significantly different effects on sleep quality in elderly patients hospitalized with COPD. However, the interactive effect of the intervention method with time was found to be effective in influencing changes in sleep quality. These findings are in line with previous studies that have emphasized the importance of combining different exercises to improve respiratory function and sleep quality in patients with COPD. In the study by Mendes et al., a comparison of the effects of DB with and without PLB in individuals with COPD showed that a combination of exercises could be beneficial. 19 The study by Yang et al. also emphasized the use of a combination of PLB along with DB, introducing this dual exercise as a low-cost physiotherapy intervention for improving respiratory function and as an essential daily exercise for patients with COPD. 22 In the study by Pedramrazi et al., aimed at determining the effect of controlled breathing exercises on the sleep quality of hospitalized patients with COPD, sleep quality improved in the intervention group after the intervention. 5 Thapamagar et al. also highlighted the complex interactions between COPD, sleep, and exercise. 50
One possible explanation for why the sequence of exercises led to better results in the first group (DB followed by PLB) is that the DB exercise may have helped to optimize respiratory function and reduce symptoms of COPD, such as dyspnea and fatigue, thereby creating a more favorable environment for the subsequent PLB exercise to have a greater impact on sleep quality. By improving lung function and reducing symptoms, the DB exercise may have allowed the PLB exercise to be more effective in promoting relaxation and reducing sleep disturbances, leading to improved sleep quality. Additionally, the DB exercise may have also helped to increase oxygenation and reduce inflammation, which may have further contributed to the improved sleep quality observed in the first group. This order effect has important clinical implications, as it suggests that the sequence of exercises may be a critical factor in determining the effectiveness of pulmonary rehabilitation programs for improving sleep quality in patients with COPD. By incorporating DB exercise as a precursor to PLB exercise, healthcare providers may be able to enhance the benefits of pulmonary rehabilitation and improve sleep quality in this population.
This study had several limitations. The first limitation was the inability to precisely control biological factors that affect sleep quality, such as dietary habits, which were beyond the researcher's control. The second limitation was that this research was conducted without blinding, which was not feasible due to the nature of the intervention. The third limitation was the small sample size, the implementation of the study at a single center, and the short-term follow-up, all of which could impact the generalizability of the results. The fourth limitation was that the principle of overload in DB exercises to strengthen the diaphragm was not applied due to the difficulty of determining the exact amount of resistance before DB exercises. The fifth limitation was self-reported adherence to exercises, which may have affected the accuracy of the results. For this reason, as explained in the method, family members were involved in the patient's exercise program. The support of family members can encourage the patient to adhere to the prescribed exercises. Also, behavioral techniques such as stating specific goals and providing positive reinforcement in telephone follow-ups were used to encourage compliance. The sixth limitation was that post-hospitalization can affect patients' overall recovery related to respiratory status, functional status, and quality of sleep. Continuing with prescribed breathing exercises can help improve lung function. Regular telephone follow-ups can help monitor recovery and address any emerging problems that were considered in this study. The seventh limitation was the presence of comorbidities, which can significantly impact sleep quality. To overcome their influence on the study results, the two groups were homogenized in terms of comorbidities. Finally, the lack of necessary information on the clinical severity of COPD (eg mild, moderate, severe), baseline lung function (eg FEV1, FVC. In the context of pulmonary function tests, the Forced Expiratory Volume in 1 second (FEV1) and Forced Vital Capacity (FVC) are two key metrics employed to evaluate lung function. Specifically, FEV1 quantifies the volume of air exhaled during the initial second of a maximal exhalation maneuver, whereas FVC measures the total volume of air expelled from the lungs following a maximal inhalation. Collectively, these parameters are utilized in the diagnosis and management of various respiratory diseases, including chronic obstructive pulmonary disease (COPD) and asthma, as well as other conditions that impact lung function), the reason for hospitalization (eg COPD exacerbation, or for another diagnosis), which may have affected the results of the study. Patients with different severity levels may respond differently to treatments, leading to variability in outcomes. For these limitations, the results may not be generalizable for the broader patient population.
Conclusion
The research findings showed that the difference between the two respiratory exercise methods, DB and PLB, was not statistically significant in terms of improving sleep quality in elderly patients with COPD. However, the arrangement of the respiratory exercise methods in the first intervention group resulted in a more substantial increase in sleep quality. Based on these results, it is recommended to focus on educational initiatives for nursing staff and other healthcare providers (respiratory therapists, chest physiotherapists, physical therapists, pulmonologists, and hospitalists), especially those following the patients after discharge regarding the effects of respiratory exercises on sleep quality and how to perform them. Nursing managers could rely on these findings to develop suitable intervention programs that incorporate this technique and oversee its implementation in the daily care of COPD patients admitted to hospitals or residing in elderly care facilities. Future research should consider using objective sleep testing methods, such as actigraphy, pulse oximetry, and home sleep testing, and conducting long-term studies to assess the sustainability of sleep quality improvements.
Supplemental Material
sj-doc-1-cra-10.1177_29768675241302901 - Supplemental material for Comparison of the Effects of Diaphragmatic Breathing and Pursed-lip Breathing Exercises on the Sleep Quality of Elderly Patients with Chronic Obstructive Pulmonary Disease (COPD): A Clinical Trial Study
Supplemental material, sj-doc-1-cra-10.1177_29768675241302901 for Comparison of the Effects of Diaphragmatic Breathing and Pursed-lip Breathing Exercises on the Sleep Quality of Elderly Patients with Chronic Obstructive Pulmonary Disease (COPD): A Clinical Trial Study by Zahra Dodange, Azar Darvishpour, Mohamad Javad Ershad and Bahare Gholami-Chaboki in Therapeutic Advances in Pulmonary and Critical Care Medicine
Supplemental Material
sj-rar-2-cra-10.1177_29768675241302901 - Supplemental material for Comparison of the Effects of Diaphragmatic Breathing and Pursed-lip Breathing Exercises on the Sleep Quality of Elderly Patients with Chronic Obstructive Pulmonary Disease (COPD): A Clinical Trial Study
Supplemental material, sj-rar-2-cra-10.1177_29768675241302901 for Comparison of the Effects of Diaphragmatic Breathing and Pursed-lip Breathing Exercises on the Sleep Quality of Elderly Patients with Chronic Obstructive Pulmonary Disease (COPD): A Clinical Trial Study by Zahra Dodange, Azar Darvishpour, Mohamad Javad Ershad and Bahare Gholami-Chaboki in Therapeutic Advances in Pulmonary and Critical Care Medicine
Supplemental Material
sj-docx-3-cra-10.1177_29768675241302901 - Supplemental material for Comparison of the Effects of Diaphragmatic Breathing and Pursed-lip Breathing Exercises on the Sleep Quality of Elderly Patients with Chronic Obstructive Pulmonary Disease (COPD): A Clinical Trial Study
Supplemental material, sj-docx-3-cra-10.1177_29768675241302901 for Comparison of the Effects of Diaphragmatic Breathing and Pursed-lip Breathing Exercises on the Sleep Quality of Elderly Patients with Chronic Obstructive Pulmonary Disease (COPD): A Clinical Trial Study by Zahra Dodange, Azar Darvishpour, Mohamad Javad Ershad and Bahare Gholami-Chaboki in Therapeutic Advances in Pulmonary and Critical Care Medicine
Footnotes
Acknowledgments
The researchers would like to express their sincere gratitude to the Vice Chancellor for Technology and Research for approving this research project. They also extend their thanks to the elderly participants who took part in the study.
Author Contribution(s)
Data Availability
Due to ethical concerns, the complete dataset cannot be publicly shared. However, the datasets used and/or analyzed during the current study, with all confidential information removed, are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
This study is the result of a master's thesis approved by the Ethics Committee of Guilan University of Medical Sciences in Rasht, Iran (Approval ID: IR.GUMS.REC.1399.111; Approval Date: 2020-06-10), and the Iranian Registry of Clinical Trials (No: IRCT20190315043062N2; Approval Date: 2020-07-05). This study was performed under the ethical standards as laid down in the Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.