
Abstract
Carbon capture, utilization and storage (CCUS) is critical for decarbonizing in hard-to-abate industries, while it may impede air quality improvements and associated health co-benefits by delaying fossil fuel phase-out. Here we evaluate the trade-offs between CCUS deployment and health co-benefits in China’s pathway to carbon neutrality 2020–2060 by an integrated modeling framework. We show that, CCUS increases the national PM2.5 concentration, leading to an additional 658,800 (95% confidence interval: 532,300–780,800) premature deaths, with uneven distributions in terms of health outcomes and populations. Our findings highlight tensions between the Sustainable Development Goals (SDGs) of climate action (SDG 13) and health (SDG 3). To maximize health co-benefits resulting from carbon neutrality, we propose to deploy CCUS with stricter air pollutant emissions control measures in regions with significant population aging, and to incorporate health co-benefits losses into the cost-benefits analysis of CCUS deployment. Our study provides novel insights into enhancing synergies between carbon neutrality and sustainable development objectives.
Keywords
Introduction
Achieving carbon neutrality, which requires drastically cutting greenhouse gas emissions, with phasing out fossil fuels being central, can generate substantial environmental co-benefits (Jia et al., 2022; Swart et al., 2004). In China, fossil fuels are the primary source of both greenhouse gases and harmful air pollutants, including sulfur dioxide (SO2), nitrogen oxides (NOX), and fine particulate matter (PM2.5; Wu et al., 2023; Zheng et al., 2024). Exposure to these pollutants undermines public health, such as increased mortality from respiratory and cardiovascular diseases (Guan et al., 2016; Liang et al., 2020; Shah et al., 2013; Wang et al., 2019). As carbon neutrality drives substantial reductions in these emissions, reducing air pollution, in turn, generating significant health co-benefits. The decarbonization pathway thus presents a great opportunity to simultaneously address SDG 13 and SDG 3.9 (reducing deaths from air pollution; Creutzig et al., 2019).
Carbon capture, utilization and storage (CCUS) is crucial for carbon neutrality, which is a process that involves capturing CO2 emissions from various sources, utilizing the captured CO2 for commercial application, or storing it away from the atmosphere (Hanson et al., 2025; Jiang et al., 2020). CCUS, including conventional CCUS and carbon dioxide removal (CDR), such as bioenergy with carbon capture and storage (BECCS) and direct air carbon capture and storage (DACCS), is an essential decarbonization option for hard-to-abate industries, such as steel, cement, and chemical manufacturing (Creutzig et al., 2019). By allowing existing fossil fuel-based infrastructure to continue function while reducing CO2 emissions, CCUS alleviates the need for immediate and extensive transitions and investments to renewables. However, by extending the functional life of fossil fuels, CCUS potentially diminish anticipated environmental and health co-benefits, thus raising a notable trade-off between SDG 13 and SDG 3 (Jacobson, 2019; Liu et al., 2025).
Although this trade-off has been fully recognized by prior studies (Cobo et al., 2022; Kiesewetter et al., 2024; Lin et al., 2023; Sun et al., 2024; Xu et al., 2024; Zhang et al., 2021), these research only confirmed the trade-off at a global or national scale and thus cannot provide practical insights into relevant policy-making. In terms of downscaling of CCUS impacts on climate-health, there remains a research gap in assessing the heterogeneous impacts of CCUS in terms of regions and population groups. At the regional level, variations in economic development, energy structures, and local air quality may lead to different effects of CCUS implementation on the health co-benefits (Zhang et al., 2021). At the population level, groups with different income levels, ages, and health conditions show varying sensitivity to air pollution exposure risks (Xu et al., 2024; Zhang et al., 2021).
By recognizing tension between CCUS implementation and air quality improvements, our research aims to answer three key questions: (1) How CCUS influence health co-benefits under carbon neutrality goals? (2) How CCUS unevenly impact health co-benefits across different diseases, population groups, and geographic regions? (3) How to maintain health co-benefits while meeting carbon neutrality targets? Our study provides evidence-based guidance for designing policies to bridge health co-benefits and climate action.
Methods
Methodological framework
To address these questions, we developed an integrated modeling framework to quantify the health co-benefits of CCUS deployment under China’s carbon neutrality scenarios (2020–2060). Based on the causal link where climate policy can generate health co-benefits by reducing fossil fuel use and improving air quality, we integrated multi-scenario PM2.5 concentration projections under different CCUS-deployed scenarios with gridded population data and baseline mortality rates through the Environmental Benefits Mapping and Analysis Program-Community Edition (BenMAP-CE) platform. Applying well-established exposure-response functions, we estimated changes in PM2.5-attributable premature mortality across scenarios, then monetized these health outcomes using the Value of a Statistical Life (VSL) approach (Figure 1).
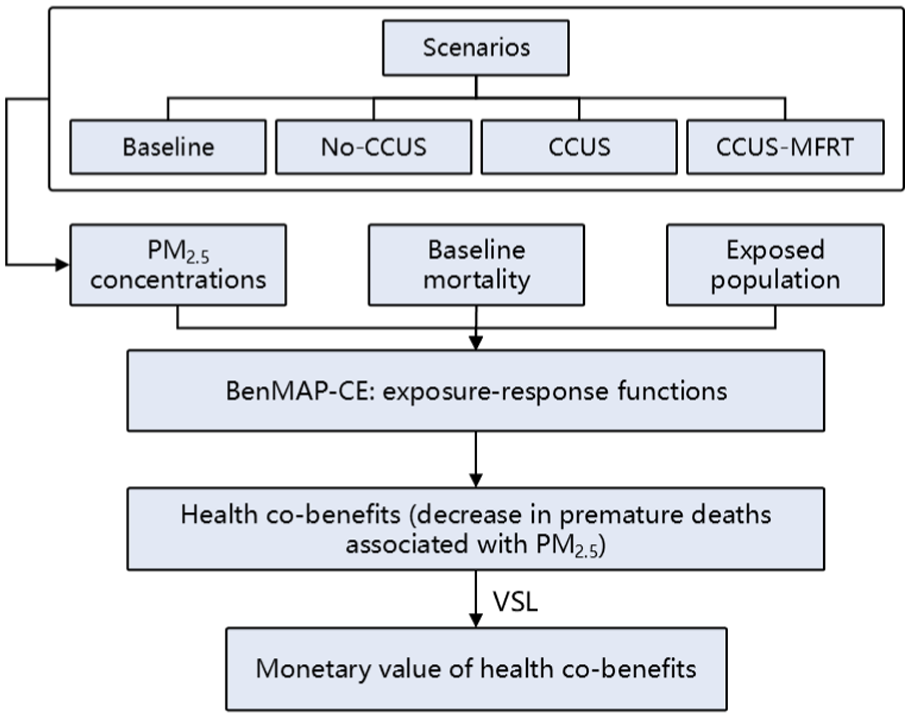
Methodological framework.
Multi-scenario PM2.5 concentration projections
To model the impacts of climate policy on energy transitions and associated changes in air quality, we utilized the multi-scenario PM2.5 concentration projection dataset calculated by Liu et al. (2025) for analyzing health co-benefits. First, we examined future energy structures through systematic analysis of carbon budget variations across different carbon neutrality scenarios, combined with China’s primary energy consumption from the Global Change Analysis Model (GCAM). An accept-reject Monte Carlo simulation was conducted to allocate national-level fossil fuel consumption to the provincial/sectoral-level. In downscaling using the Monte Carlo simulations, random sampling was repeated 1,000,000 times to reduce uncertainty. The allocation process was guided by historical fossil fuel consumption patterns, where provinces with higher historical consumption levels were proportionally allocated greater shares of future fossil fuel usage quotas.

where
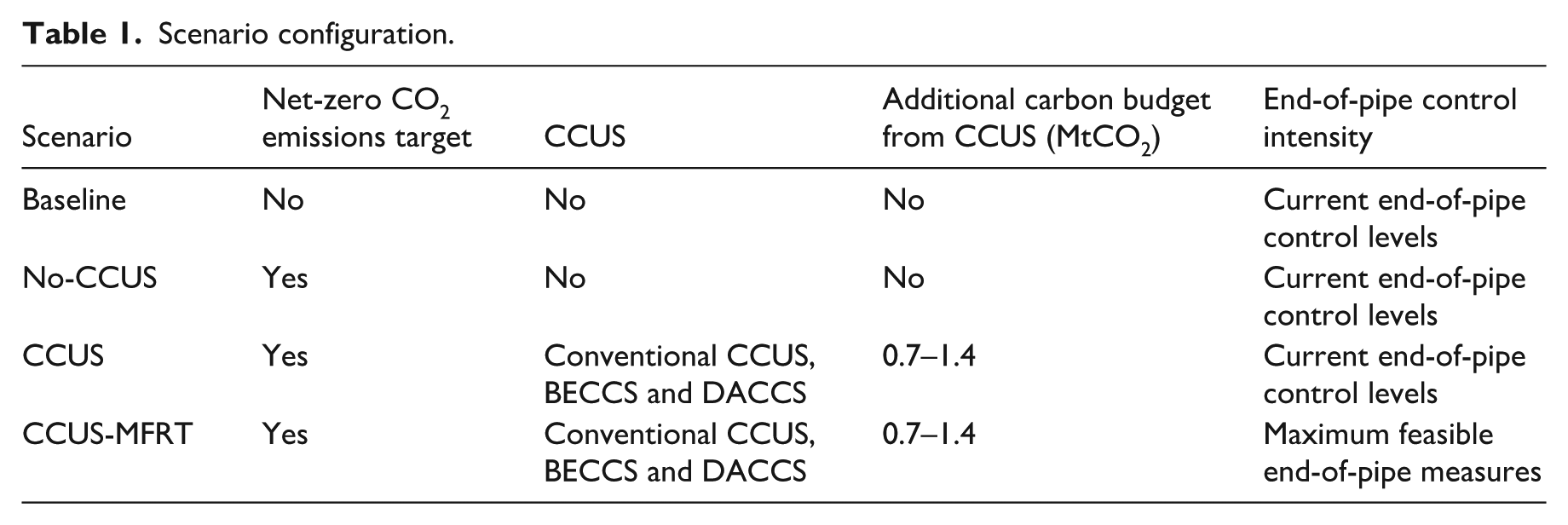
The No-CCUS scenario represents a pathway only relying on natural carbon sinks (e.g. forests and oceans) without the large-scale CCUS deployment. This scenario is counterfactual, given the extreme difficulty of eliminating all emissions. The CCUS scenario incorporates technological carbon removal based on China’s CCUS technical potential estimated from the China CCUS Annual Report (2021; Cai et al., 2021).The CCUS-MFRT scenario further combines CCUS deployment with maximized feasible reduction technologies for air pollutants (MFRT), requiring all sectors to adopt the strictest end-of-pipe measures: With respect to SO2, circulating fluidized bed-flue gas desulfurization deployed in all non-power sectors with a removal rate of 90%. With respect to NOX, selective catalytic reduction deployed in all industrial sectors with a removal rate of 80%. With respect to PM or dust, filter dedusting deployed in all non-power sectors with a removal rate of 95%. (Ministry of Science and Technology and Ministry of Environmental Protection, 2014). The scenario configuration is shown in Table 1.
Scenario configuration.
Estimation of health co-benefits
We employed the BenMAP-CE model to assess health co-benefits. Developed by the Environmental Protection Agency of USA, BenMAP-CE serves as an open-source software tool widely used to evaluate the health impacts of air pollution changes and quantify their associated economic benefits (Grabow et al., 2012; Li et al., 2018; Wang et al., 2020). The model integrates air quality data, demographic statistics, and exposure-response relationship, utilizing a built-in geographic information system to assess health effects across specific regions and demographic group (Sacks et al., 2018).
We evaluated the health co-benefits from PM2.5 reduction under different carbon neutrality scenarios, using exposure-response relationships to quantify associated declines in population health risks. Considering data availability and reliability, we selected the following health endpoints: all-cause mortality (A00-Z99), along with cause-specific mortality from circulatory diseases (I00-I99), respiratory diseases (J00-J99), and lung cancer (C30-C39). Health effects were calculated using the exposure-response coefficient (β): a key parameter typically derived from relative risk (RR) values:

The RR values were sourced from reference (Chen and Hoek, 2020; Yang et al., 2020). ΔC represents the change in pollutant concentration. As the RR values used in this study correspond to a 10 μg/m3 PM2.5 increase, ΔC is standardized at 10 μg/m3.
Health impacts were quantified using exposure-response functions, with uncertainty analysis with 95% confidence intervals (95% CIs) based on Monte Carlo simulations. We apply BenMAP-CE’s log-linear exposure-response function to estimate health effects from air quality changes:

where ∆
According to the health co-benefits at each time point, the cumulative health co-benefits from 2020 to 2060 are calculated as follows:

where CHB represents the cumulative health co-benefits; HB denotes the function of annual avoided PM2.5-related deaths versus time; and t represents a given time point.
We accounted for the co-benefits of fulfilling the dual carbon goals under different scenarios by monetizing the estimated avoided premature deaths using the VSL, which was extracted from reference (Zhang et al., 2021).

Results
CCUS-induced changes in PM2.5 concentrations
Regional PM2.5 distribution varies significantly due to factors like economic development, industrial structure, and energy use. Figure 2a shows that under the baseline scenario, provinces such as Xinjiang, Hebei, Shandong, and Liaoning exhibit higher PM2.5 levels, while southwestern regions maintain lower concentrations.
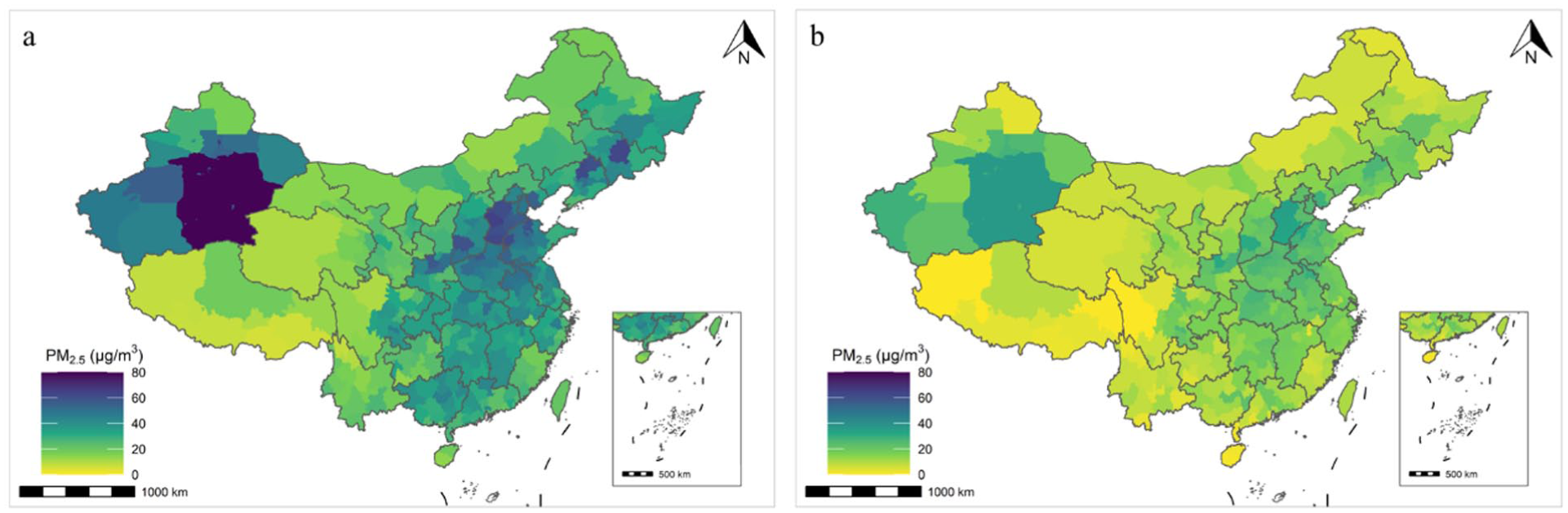
Changes in PM2.5 concentrations by the mitigation pathway to carbon neutrality under No-CCUS. (a) Regional PM2.5 concentrations in 2020. (b) Regional PM2.5 concentrations in 2060 under the No-CCUS scenario. All maps in this study are generated from the Standard Map Service (GS (2024) 0650) provided by the Ministry of Natural Resources of the People’s Republic of China, with unmodified base maps (http://www.nrsis.org.cn).
To evaluate the impact of achieving carbon neutrality on air quality, we compare PM2.5 concentrations under the No-CCUS scenario against the baseline scenario (Figure 3b). The results demonstrate that achieving carbon neutrality can significantly mitigate PM2.5 pollution nationwide. The most substantial reductions occur in provinces with the highest baseline pollution, particularly those with intensive industrial activity such as Xinjiang, Hebei, Shandong, Liaoning, Henan, and Jiangsu. These provinces face the most demanding energy transition due to their fossil-fuel-dependent industries. In contrast, provinces like Tibet and Yunnan experience relatively smaller decreases in PM2.5 concentrations, reflecting their lower baseline pollution levels and smaller energy transition requirements.
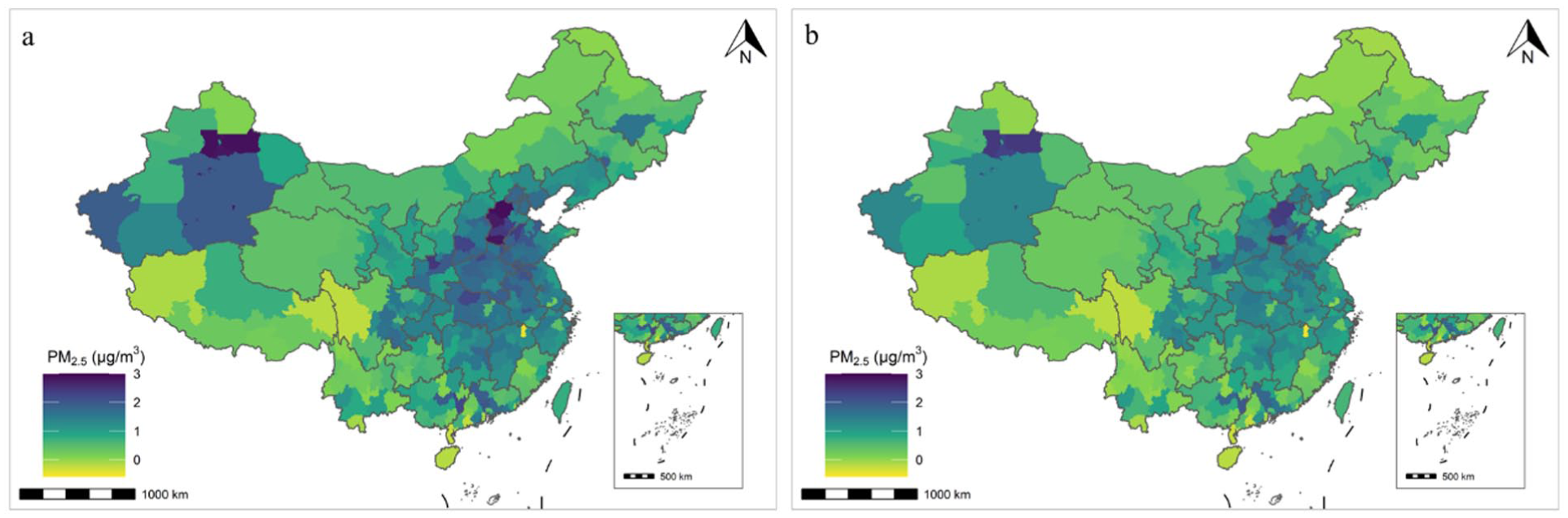
Changes in regional PM2.5 concentration induced by CCUS deployment. (a) Differences in PM2.5 concentrations in 2060 between the CCUS and No-CCUS scenarios. (b) Differences in PM2.5 concentrations in 2060 between the CCUS-MFRT and No-CCUS scenarios.
To separate the impact of CCUS deployment on PM2.5 reduction, we compare scenarios with CCUS deployment (CCUS and CCUS-MFRT) against the No-CCUS scenario. Notably, deploying CCUS technology results in higher PM2.5 concentrations compared to the No-CCUS scenario, regardless of end-of-pipe control stringency. This effect partially offsets the air quality improvement resulting from carbon neutrality. The most significant PM2.5 increases due to CCUS deployment occur in highly industrialized provinces with great reliance on fossil fuels, such as Hebei, Shandong, Henan, and Xinjiang (Figure 3). Furthermore, the PM2.5 increase under the CCUS deployment scenario relative to No-CCUS scenario is greater than the increase observed between the CCUS-MFRT scenario and No-CCUS scenario.
This adverse outcome is primarily due to the complex energy transition in these key industry-based provinces. While pursuing carbon neutrality through reduced fossil fuel use and increased renewables, their large existing fossil energy consumption creates substantial transition pressure (Shindell and Smith, 2019). Consequently, they are allocated larger CCUS-derived additional carbon budgets to maintain both economic stability and energy security (Table S1). This allowance enables continued, albeit reduced, reliance on coal and natural gas in the short term. However, this incomplete shift away from high-pollution fuels indicates that emissions of conventional air pollutants are not sufficiently curtailed. Therefore, although CCUS effectively captures CO2, the lack of primary pollutant emissions cuts leads to higher PM2.5 levels under CCUS scenarios compared to pathways without it, thus undermining the potential air quality co-benefits of carbon neutrality. Notably, improved end-of-pipe measures can partially mitigate the adverse impacts associated with large-scale CCUS deployment. The CCUS-MFRT scenario demonstrates that even with maximum feasible end-of-pipe measures, residual PM2.5 levels remain high compared to the No-CCUS scenario. This underscores the need of end-of-pipe measures that serve as a supplementary to energy transitions.
Declines in health co-benefits induced by CCUS
We evaluate the impact of CCUS deployment on health co-benefits during China’s carbon neutrality transition by comparing PM2.5-related premature mortality under two CCUS deployment scenarios against the No-CCUS scenario, as shown in Figure 4. While CCUS adoption contributes to carbon mitigation, it partially offsets expected health co-benefits from reduced air pollution. Specifically, the CCUS scenario leads to an additional 658,800 (95% CI: 532,300–780,800) PM2.5-attributable premature deaths from 2020 to 2060 compared to the No-CCUS scenario, translating to economic losses of 7.26 trillion CNY (95% CI: 5.87–8.60 trillion; Table S5). These findings highlight critical trade-offs between CCUS-driven decarbonization and health co-benefits by improving air quality, underscoring the need for integrated policy design.
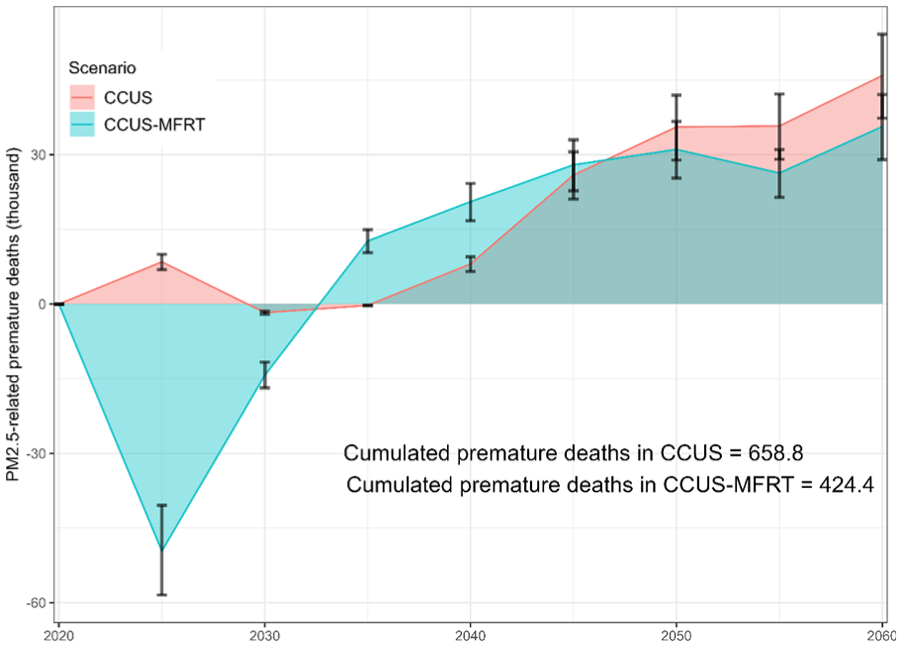
Change in premature deaths due to CCUS deployment compared to the No-CCUS scenario (thousands).
Enhanced end-of-pipe controls temporarily mitigate these health losses, showing net health benefits before 2030. However, by 2060, even with stringent controls, the CCUS-MFRT scenario still results in 35,600 (95% CI: 29,000–42,100) excess deaths annually relative to the No-CCUS scenario. Cumulatively from 2020 to 2060, this contributes to an additional 424,400 (95% CI: 246,900–599,400) premature deaths and economic costs of 4.68 trillion CNY (95% CI: 2.72–6.61 trillion; Tables S4 and S5). This temporal divergence reveals a critical limitation of pollution control strategies: While strengthened end-of-pipe measures can effectively reduce emissions and lower ambient PM2.5 concentrations in the short term, yielding immediate reductions in PM2.5-attributable premature mortality (pre-2035), their long-term efficacy (by 2060) proves insufficient to offset the health co-benefit losses by CCUS. The persistent mortality gap is attributable to the inherent constraints of end-of-pipe technologies. These end-of-pipe measures reduce air pollutants after generation but before environmental release, achieving rapid air quality improvements. However, their effectiveness approaches a technological ceiling (Frondel et al., 2007), making marginal gains increasingly difficult as control intensities near maximum feasible levels. Consequently, while valuable for transitional mitigation, end-of-pipe measures cannot fundamentally eliminate pollution sources. Sustainable air quality improvement and associated health co-benefits ultimately require transformative energy transitions to renewables by phasing out fossil fuel at scale.
Impacts of CCUS on health co-benefits of different subgroups
Health co-benefits under carbon neutrality scenarios exhibit significant demographic heterogeneity. Under the No-CCUS scenario, cumulative avoided premature deaths from circulatory diseases reach 9.96 million (95% CI: 7.82–11.94 million) during 2020–2060, accounting for 71.9% of total PM2.5-attributable mortality reductions across all disease categories. In contrast, respiratory diseases and lung cancer contribute relatively smaller shares, accounting for 15.5% and 12.6% of total avoided deaths, respectively (Table 2). This primarily reflects differences in baseline disease mortality rates, as circulatory diseases in China had a substantially higher baseline mortality (0.30% in 2019) compared to respiratory diseases (0.07%) and lung cancer (0.05%). The greater absolute health benefits observed for circulatory diseases align with established epidemiological principles-conditions with higher baseline burdens typically demonstrate stronger mortality response elasticity to environmental improvements like PM2.5 reduction.
Health co-benefits across different subgroups under the No-CCUS scenario.
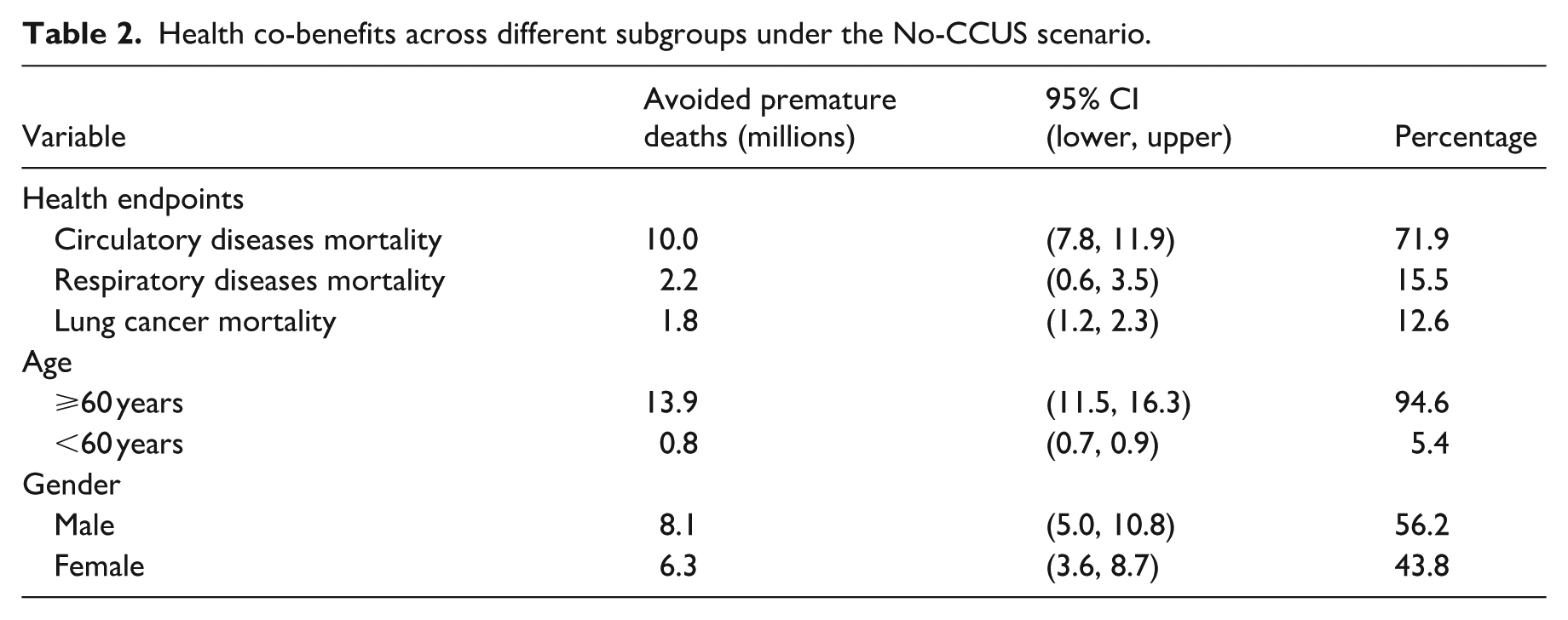
Under the No-CCUS scenario, elderly populations (⩾60 years) account for 13.94 million (95% CI: 11.48–16.26 million) avoided PM2.5-attributable premature deaths, representing 94.6% of total mortality (Table 2). This disproportionate health outcomes among the elderly reflect their heightened physiological vulnerability to air pollution, as aging populations typically exhibit higher prevalence of chronic conditions (e.g. hypertension, diabetes, cardiovascular diseases) and weakened immune function, which collectively amplify their sensitivity to long-term PM2.5 exposure (Chanda et al., 2024; Hu et al., 2023; Li et al., 2023). The notable sensitivity stems from age-related declines in organ capacity and increased baseline inflammatory states, making older individuals more responsive to both the detrimental effects of pollution exposure and the health improvements from air quality interventions compared to younger age groups.
Gender differences show a moderate disparity, with males avoiding 8.06 million premature deaths (56.2% share; 95% CI: 5.04–10.81 million) compared to 6.28 million (43.8% share; 95% CI: 3.62–8.67 million) among females (Table 2). The observed gender disparity in the absolute health co-benefits primarily stems from males’ higher baseline mortality rates for PM2.5-related diseases and their greater population size.
The CCUS deployment undermines these co-benefits unevenly across subgroups. Compared to the No-CCUS scenario, CCUS results in 454,800 (95% CI: 347,500–558,500) additional deaths from circulatory diseases, accounting for 71.8% of all excess mortality. Respiratory diseases and lung cancer show comparatively smaller increases, contributing 15.4% and 12.8% of total excess deaths respectively (Table 3). The elderly population (⩾60 years) experience the most severe impacts, with approximately 625,000 (95% CI: 505,200–740,800) excess deaths under CCUS deployment, representing 97.1% of all premature mortality increases. This pattern remains consistent under the CCUS-MFRT scenario (411,300 excess deaths with 95% CI: 244,600–575,600). Gender disparities are modest, with males showing only slightly higher sensitivity than females. Male populations suffer 359,300 (95% CI: 214,500–499,400) additional deaths (55.7% of total excess mortality), compared to 282,600 (95% CI: 153,800–407,500) in females (44.3%).
Health co-benefits across different subgroups under the CCUS and CCUS-MFRT scenarios.
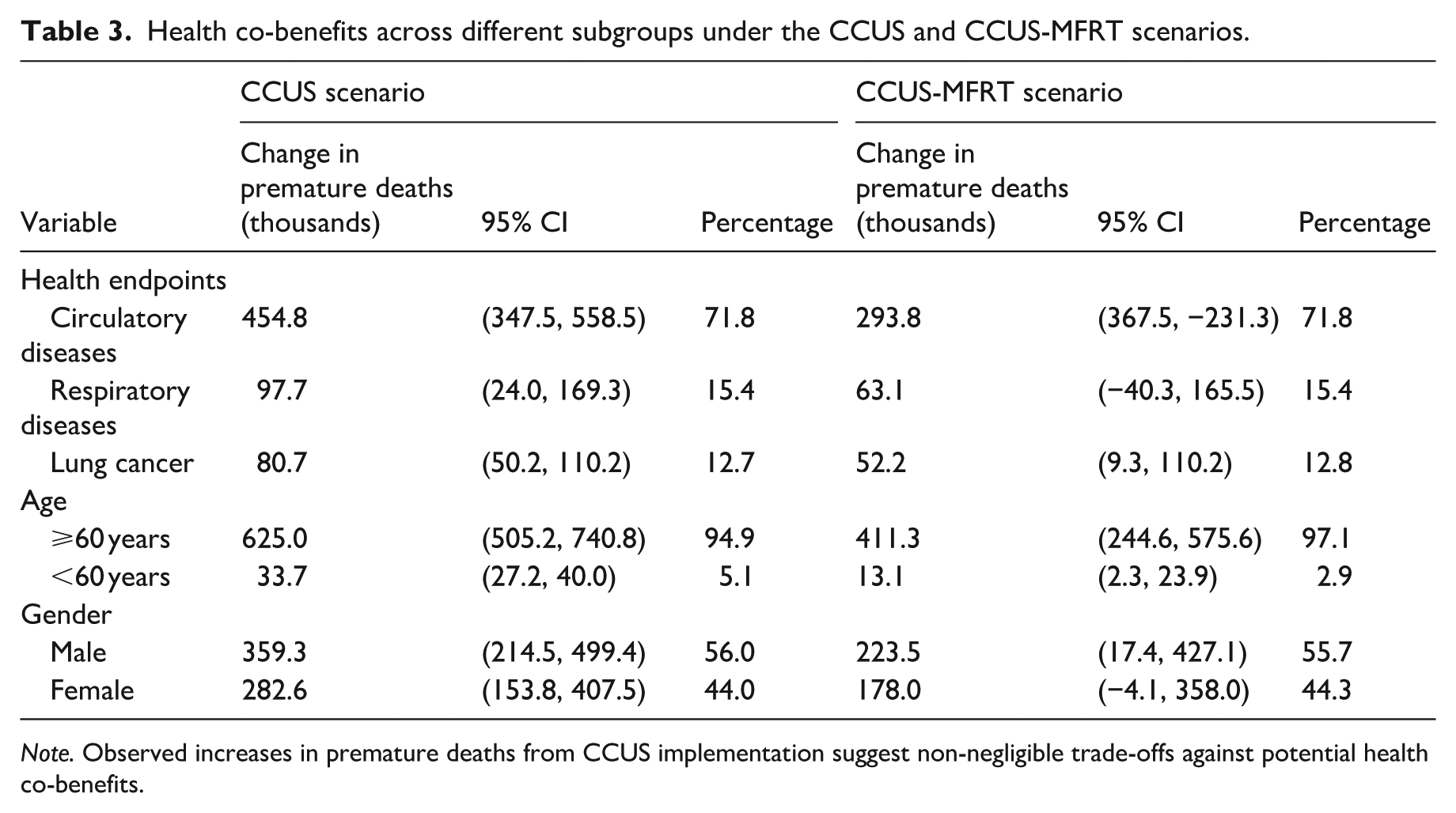
Note. Observed increases in premature deaths from CCUS implementation suggest non-negligible trade-offs against potential health co-benefits.
These findings identify high-risk populations requiring targeted protection from CCUS-related PM2.5 concentration increases. Elderly individuals (⩾ 60 years) and those with circulatory diseases show exceptional vulnerability (Table 3). Public health strategies should prioritize these groups through enhanced air quality monitoring, adaptive healthcare services for pollution-sensitive conditions, and community-level exposure reduction measures. Such tailored interventions would mitigate disproportionate health losses, while ensuring equitable benefits during the low-carbon transition.
Differential impacts of CCUS on health co-benefits across provinces
Health co-benefits resulting from carbon neutrality exhibit substantial regional heterogeneity. From 2020 to 2060, provinces like Henan, Shandong, Hebei, Jiangsu, and Hunan are projected to obtain the most significant health co-benefits, potentially avoiding ~1.60 million (95% CI: 1.32–1.86 million), 1.43 million (95% CI: 1.18–1.66 million), 1.19 million (95% CI: 0.99–1.38 million), 0.87 million (95% CI: 0.72–1.02 million), and 0.84 million (95% CI: 0.69–0.98 million) PM2.5-related premature deaths, respectively. In contrast, regions such as Qinghai, Hainan, and Tibet have limited potential of obtaining health co-benefits, with estimated avoided premature deaths of 35,700 (95% CI: 29,200–41,900), 13,300 (95% CI: 10,800–15,600), and 5200 (95% CI: 4300–6100) cases during the same period (Figure 5). This spatial heterogeneity highlights the uneven distribution of air quality improvements in carbon neutrality.
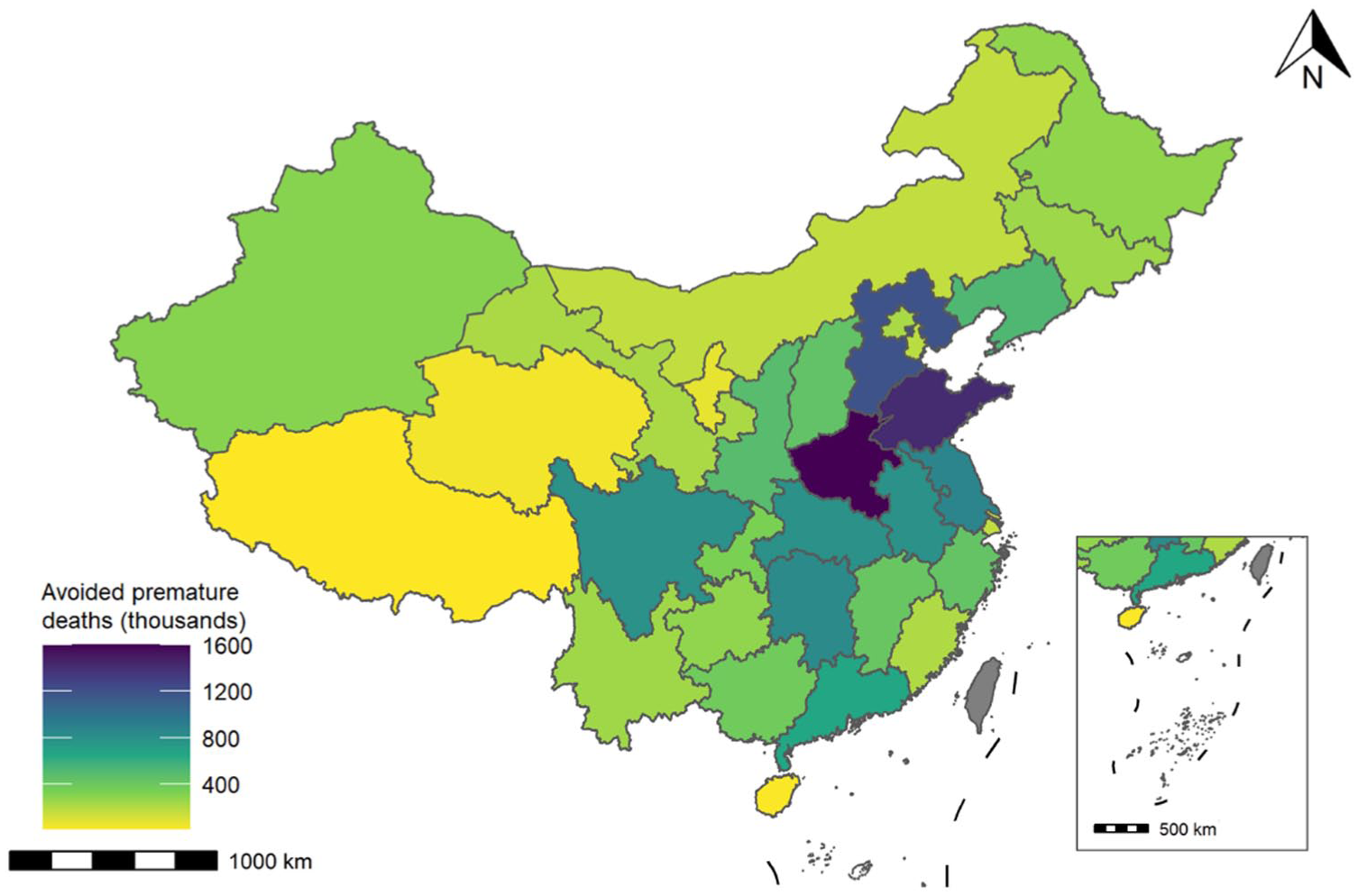
Provincial health co-benefits resulting from carbon neutrality. Health co-benefits are quantified as avoided PM2.5-related premature deaths over 2020–2060. Hong Kong, Macao, and Taiwan are excluded.
The deployment of CCUS reduces both net CO2 emissions and health co-benefits resulting from carbon neutrality, with significant spatial heterogeneity (Figure 6). The largest reductions in health co-benefit are observed in Henan, Shandong, Hebei, and Jiangsu provinces, where PM2.5-attributable premature deaths increase by 77,500 (95% CI: 63,000–91,400), 64,300 (95% CI: 52,400–75,900), 59,200 (95% CI: 48,100–69,900), and 41,500 (95% CI: 33,800–49,000), respectively. In contrast, carbon budget allocation is limited in regions with small fossil fuel consumption, such as Hainan, Tibet, and Qinghai, resulting in minimal adverse impacts on health co-benefits in these regions. Although enhanced end-of-pipe measures partially alleviate these negative effects, residual health losses remain substantial, particularly in heavily industrialized provinces. Under the CCUS-MFRT scenario, premature deaths caused by increased CCUS remain significantly in Henan (45,300; 95% CI: 36,800–53,500), Hebei (42,600; 95% CI: 34,600–50,300), Shandong (36,700; 95% CI: 29,800–43,300), and Sichuan (25,600; 95% CI: 20,800–30,200; Table S6).
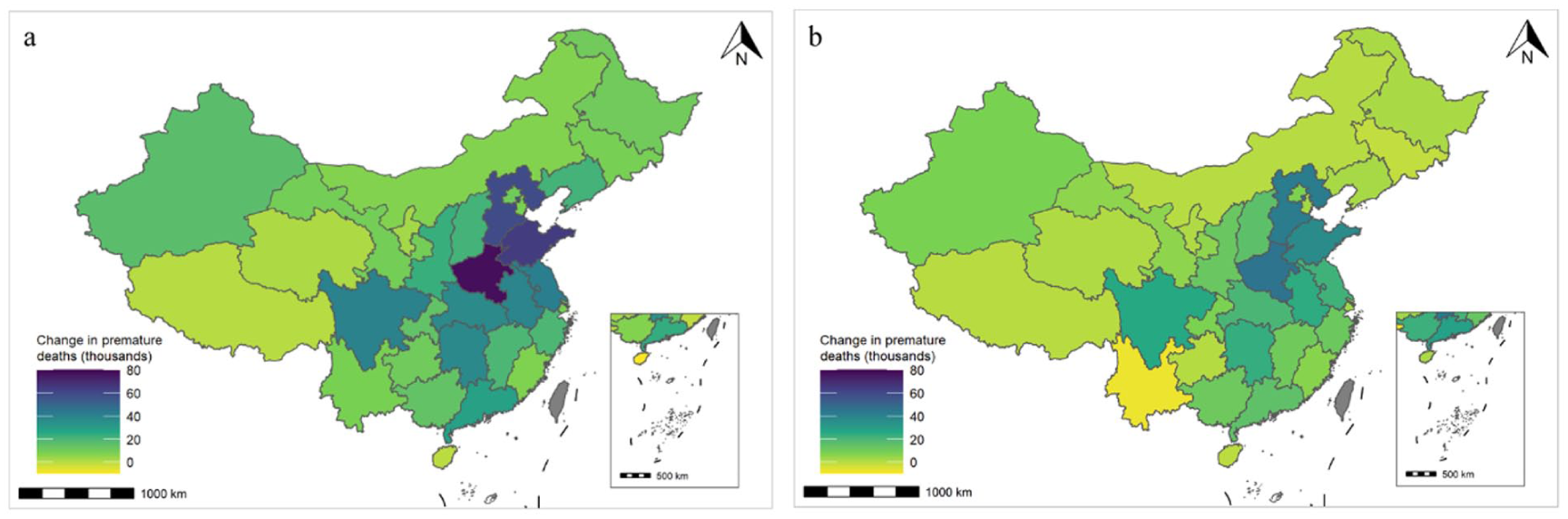
Rises in health co-benefits when transitioning from No-CCUS to CCUS (a) and CCUS-MFRT (b) scenarios. Hong Kong, Macao, and Taiwan are excluded.
Compared to the No-CCUS scenario, the reduction in health co-benefits across provinces broadly aligns to the rise in carbon budgets by CCUS (Tables S1 and S6). This occurs because provinces with notable agglomeration of heavy industry, such as Shandong, Hebei, Jiangsu, and Henan, develop based on the large consumption of fossil fuels and receive larger carbon budgets for energy transitions. Consequently, a larger carbon budget allocation slows fossil fuel phase-out, leading to more pronounced declines in expected health co-benefits from carbon neutrality. In contrast, because of low population density, regions such as Xinjiang and Inner Mongolia experience relatively smaller health co-benefit reductions, despite receiving substantial carbon budgets.
We introduce a CCUS sensitivity coefficient, defined as health co-benefits declined by per unit of additional carbon budget enabled by CCUS (unit: deaths/MtCO2). A higher coefficient indicates greater sensitivity to CCUS deployment and a larger health co-benefits loss due to each unit of carbon budget allocated. Sichuan, Henan, Beijing, Hunan, and Hubei are identified as “CCUS-sensitive” regions, where moderate carbon budget increases lead to substantial health co-benefit losses (Table 4). This is primarily due to their high population density and baseline mortality rates. In Sichuan, the basin’s enclosed topography further amplifies health risks by trapping air pollutants, leading to higher air pollutant concentrations (Wang et al., 2018). In contrast, regions such as Hainan, Inner Mongolia, Ningxia, Fujian, and Xinjiang show limited sensitivity to CCUS deployment, with minimal health co-benefit losing per unit of carbon budget (Table 4). These “CCUS-insensitive” regions benefit from high atmospheric environmental capacity (e.g. Hainan and Inner Mongolia) and low population density (e.g. Xinjiang), all of which mitigate health impacts by CCUS deployment and associated air pollutants. Furthermore, differences in income and access to healthcare also contribute to such heterogeneity across those provinces (Xu et al., 2021; Yang et al., 2023). For example, residents in developed regions are more accessible to advanced healthcare, leading to lower local mortality rates, despite severe air pollution induced by CCUS.
CCUS sensitivity coefficients in 31 provinces.
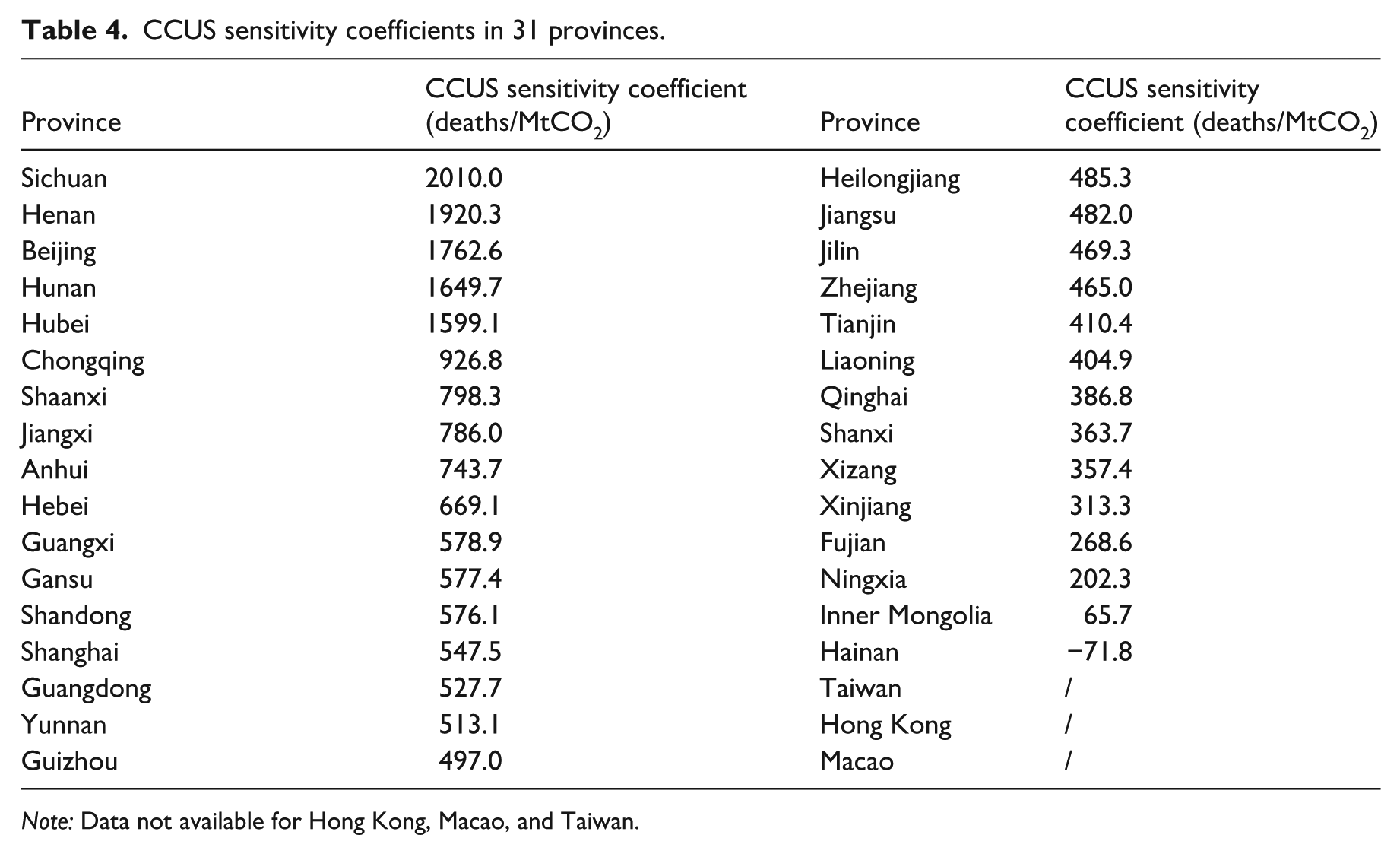
Note: Data not available for Hong Kong, Macao, and Taiwan.
Discussion
This study demonstrates that achieving carbon neutrality can generate substantial health co-benefits by reducing ambient PM2.5 concentrations, consistent with existing research findings (Cheng et al., 2023; Kiesewetter et al., 2024; Li et al., 2024; Zhang et al., 2021). However, the large-scale deployment of CCUS technology, which is critical for hard-to-abate sectors, diminishes these health co-benefits by postponing fossil fuel use and associated PM2.5 emissions cuts. We reveal that elderly populations and patients with circulatory system diseases emerge as particularly vulnerable groups to the health impacts of CCUS deployment. Regional variations show that industrialized provinces with higher CCUS-related carbon budget allocations experience more pronounced health co-benefit reductions, while “CCUS-sensitive” regions like Sichuan, Henan, and Beijing suffer from disproportionately larger health impacts due to their dense populations, high baseline mortality rates, and unfavorable geographic conditions. These findings highlight how geographic and demographic factors shape the health-climate trade-offs of decarbonization strategies.
The demonstrated health trade-offs of CCUS in carbon neutrality necessitate policy tools that incorporate climate action (SDG 13) with public health protection (SDG 3). Given the disproportionate impacts across regions and vulnerable populations, policymaking should prioritize health equity alongside emission reductions. We propose two measures for achieving carbon neutrality, while maximizing health co-benefits:
(1) Carbon budget should be allocated according to the sensitivity of local health co-benefits to CCUS deployment. While allocating carbon budget to fossil-dependent provinces (e.g. Shandong, Hebei, Jiangsu, and Xinjiang) to reduce pressure on energy transitions, fossil fuel phase-out should be facilitated at the same time. For “CCUS-sensitive” regions, the deployment of CCUS should be informed by the consideration of health co-benefits declines.
(2) The cost-effectiveness of CCUS deployment should be re-evaluated based on monetized health co-benefits declines. By this approach, despite agglomerated hard-to-abate sectors, such as transportation and buildings, policymakers may focus on energy transitions to renewables in regions with high population densities. In addition, health equity could be further improved by crafting a holistic evaluation framework, where regional cost-effectiveness of CCUS is adjusted for vulnerable groups and health co-benefits should be explicitly defined in carbon neutrality. For example, the cost-effectiveness of CCUS could decline in regions with significant population aging, and energy transitions to renewables could be facilitated as a priority.
Conclusion
We evaluate the trade-offs in regard to CCUS deployment decreasing the expected health co-benefits resulting from carbon neutrality, with four major conclusions:
Developing CCUS increases the national PM2.5 concentration, decreasing the expected health co-benefits resulting from carbon neutrality by leading to an additional 658,800 (95% CI: 532,300–780,800) premature deaths over 2020–2060.
The deployment of CCUS yields significantly heterogeneous impacts in terms of regions, population groups, and diseases. The most notable adverse impact of CCUS occurs by increasing the circulatory diseases in the elder group in coal-based regions of Henan, Hebei, and Shandong.
End-of-pipe measures are essential to balance the trade-off regarding CCUS, which significant mitigates the adverse impacts on health co-benefits.
Health co-benefits in Sichuan and Henan exhibit the most notable sensitivity to CCUS deployment, with 2010.0 and 1920.3 premature deaths occurring, respectively, when 1 million ton of CCUS is deployed.
There remain several limitations in our study. (1) Health co-benefit declines by CCUS might be underestimated, as we only focus on the mortality due to exposure to PM2.5, while morbidity and mortality caused by ozone and other air pollutants are excluded. However, PM2.5-related mortality accounts for the lion’s share of air pollution-related mortality and these underestimation might not jeopardize our conclusion. (2) Due to data limitations, we employ proxy inputs (e.g. 2019 baseline mortality rates) for 2020–2060 projections. This represents a conservative approach that introduces minor uncertainty. Future research should enhance data accuracy through multi-stakeholder collaboration, sharing of integrated monitoring data, and applying of more sophisticated modeling for health co-benefit assessments. (3) Monetization of premature deaths based on a gross domestic product-based value may trigger some moral and ethical concerns (Aldy and Viscusi, 2007). Despite VSL used in our study, it may result in another uncertainties, where declines in monetized health co-benefits would be underestimated in developed provinces like Beijing and Shanghai. (4) Despite Monte Carlo simulations used in energy consumption downscaling, our modeling framework cannot capture all uncertainties. For example, future meteorological conditions have not been addressed in PM2.5 concentration modeling, resulting in some uncertainties in air pollutant concentration modeling and associated health impact assessment.
Supplemental Material
sj-docx-1-tss-10.1177_29768632251397734 – Supplemental material for Trade-offs between CCUS deployment and health co-benefits in China’s carbon neutrality
Supplemental material, sj-docx-1-tss-10.1177_29768632251397734 for Trade-offs between CCUS deployment and health co-benefits in China’s carbon neutrality by Zuhui Zhang, Zeyuan Liu and Kai Fang in Transactions in Energy and Sustainability
Footnotes
Ethical considerations and consent to participate
Not applicable. This study utilized exclusively open-access/publicly available data with no individual identifiers. All analyses were performed in compliance with relevant institutional guidelines for non-human subjects research.
Author contributions
Zuhui Zhang: Methodology, Data Curation, Formal analysis, Visualization, Writing – Original Draft.
Zeyuan Liu: Methodology, Data Curation, Conceptualization, Validation, Writing – Review & Editing.
Kai Fang: Conceptualization, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Key R&D Program of China (2024YFC3712900), the National Natural Science Foundation of China (72074193, 42341205), the Key R&D Program of Zhejiang Province (2022C03154), and the Postdoctoral Fellowship Program and China Postdoctoral Science Foundation (2024M762837, BX20250329).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be made available on request except the public data already indicated in the text.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.