
Abstract
Background:
This study aimed to investigate the complex relationships between smokeless tobacco (SLT) consumption behaviors, socio-demographic factors, and oral health status among patients in Bangladesh, using Structural Equation Modeling (SEM).
Methods:
A cross-sectional study was conducted from December 2021 to June 2022 with 156 participants included via purposive sampling from a dental outpatient department. Data were collected using a semi-structured questionnaire, translated and piloted for validity, covering socio-demographics, detailed SLT behaviors, and oral health status assessed by clinical dentists using the WHO Oral Health Assessment Form for Adults. Data analysis was performed employing descriptive statistics, Spearman correlations, and SEM to evaluate associations.
Results:
SEM analysis revealed a strong positive relationship between SLT using behavior and oral health status (path coefficient = 0.99), while the path from socio-demographic factors to oral health was moderately positive (path coefficient = 0.59). Key specific associations included a significant relationship between the duration of SLT use and the need for more urgent treatment interventions (P < .001), with over 70% of participants having used SLT for more than a decade. Furthermore, earlier age of initiation (P = .016), higher frequency of daily use (P = .015), and specific SLT types (P = .022) were significantly associated with treatment urgency. The SEM model demonstrated an acceptable overall fit based on ULS-appropriate indices, including the Root Mean Square Residual (RMR = 0.079), Goodness of Fit Index (GFI = 0.986), Adjusted Goodness of Fit Index (AGFI = 0.981), and Normed Fit Index (NFI = 0.916), indicating a reasonable representation of the observed data.
Conclusions:
The use of SLT is a major and direct factor associated with poor oral health outcomes, and the length of usage is a crucial risk factor. Although less important, sociodemographic traits are also important.
Keywords
Introduction
The use of smokeless tobacco (SLT) is a significant public health concern, particularly in regions where cultural practices support its consumption. Unlike conventional smoking, SLT products—such as chewing tobacco, snuff, and betel quid—are often perceived as less harmful, leading to widespread underestimation of their health risks.1,2 Despite the clear evidence linking SLT to various health issues, including cardiovascular diseases, respiratory problems, and oral health complications, public awareness remains insufficient.3,4
Evidence suggests that SLT use is associated with serious oral health problems, including periodontal disease, dental caries, and oral cancers.5,6 The World Health Organization (WHO) has recognized SLT as a significant risk factor for non-communicable diseases, urging member states to adopt comprehensive tobacco control measures. 7 Despite these recommendations, SLT use continues to be prevalent, particularly among specific demographics such as youth and individuals in lower socio-economic groups.8,9
In Bangladesh, a diverse range of smokeless tobacco products are commonly used, including Zarda (tobacco mixed with spices and lime and often chewed with betel leaf), gul (finely powdered tobacco applied to the gum), and Sada Pata (sun-dried raw tobacco leaf). 10 Among adults, zarda alone or in combination with other ingredients is the most frequently consumed form, followed by other products such as pan masala with tobacco (which may increase addictive exposure).11,12 These products vary in composition and usage patterns, which can influence both dependence potential and oral health risk profiles.11,12
Additionally, studies conducted in Bangladesh have shown that, independent of tobacco use, sociodemographic traits are significantly linked to oral health outcomes. For instance, among Bangladeshi university students, variations in oral health knowledge, attitudes, and practices had a significant relationship with gender, household income, and parental education. 13 According to Nagata et al (2025), disparities in dental service utilization in Bangladesh were also found to be influenced by age, education level, and urban versus rural residence, with higher education and better socioeconomic status consistently associated with greater use of dental services. 14 These results justify the inclusion of social determinants in analytical models of oral health by demonstrating their wider significance in determining oral health status in the Bangladeshi context.
Although often misperceived as a safer alternative to conventional smoking, smokeless tobacco products—including chewing tobacco, snuff, and related forms—pose considerable health risks. The World Health Organization has identified SLT as a major etiological factor in dental caries, periodontal diseases, and oral cancers. 7 The abrasive and sugar-containing nature of many SLT products contributes directly to dental decay and erosion.2,15 Furthermore, epidemiological evidence indicates that SLT users exhibit a markedly higher risk of developing oral malignancies, in some cases surpassing that associated with cigarette smoking.16,17 The carcinogenic compounds within SLT, which maintain prolonged contact with the oral mucosa, constitute the primary pathogenic mechanism behind these outcomes.16,17
Socioeconomic variables such as education, income, and access to healthcare have an important impact on smokeless tobacco usage. The socioeconomic model of health (SEAM) emphasizes that individual behaviors are impacted by wider socioeconomic settings, such as education, money, and access to healthcare facilities. 18 Various studies have demonstrated that socio-demographic characteristics—such as age, gender, and educational attainment—significantly influence tobacco use patterns and health outcomes.19-21
In response to the multifaceted nature of smokeless tobacco (SLT) practices and their implications for oral health, this research is designed to quantitatively dissect these relationships among SLT users within a tertiary dental care setting using Structural Equation Modeling (SEM) analysis. A key component of this study is the integration of socio-demographic factors to better understand their modulating effects on oral health. The findings are anticipated to provide specific insights for dental practitioners regarding patterns, intensity, and duration of SLT use, which can inform patient counseling, prevention strategies for nonusers, and cessation support for current users, rather than general public health policy.
Materials and Methods
Study Design, Setting, and Participants
A cross-sectional study was conducted at a tertiary dental care facility in Dhaka, Bangladesh, between December 2021 and June 2022. The target sample size was calculated as 172, using the single population proportion formula:

Where, n is desired sample size, when the study population >10 000, Z is the standard normal distribution set as 1.64, which corresponds to a 90% confidence interval, prevalence of oral effects due to SLT consumption (P = .80).22,23
Based on this, n = (1.64)^2 × (0.80) × (0.20)/(0.05)^2 = 172.
A purposive sample initially comprised 172 eligible patients. Sixteen participants subsequently withdrew consent prior to completing the questionnaire and oral health assessment, yielding incomplete data and necessitating their exclusion. Consequently, the final analytical sample included 156 participants. Enrollment was contingent upon the following inclusion criteria: age 18 years or older, possession of a minimum of 10 natural teeth, and current use of smokeless tobacco. While the patients who were not eligible as per inclusion criteria, having mental health conditions, speech disability, and withdrew SLT consumption, were excluded.
Data Collection and Instrument
A semi-structured questionnaire, incorporating the WHO Oral Health Assessment Form for Adults (2013), was used to collect data on socio-demographic characteristics, smokeless tobacco use, and oral health status. 24 The instrument was translated and culturally adapted through forward- and back-translation procedures and piloted on 10% (n = 16) of the target sample. No new items were added to the standard WHO OHFA; the adaptation involved linguistic translation only to ensure cultural and contextual clarity. Assessment of dental treatment need was conducted exclusively using the standardized WHO OHFA clinical criteria. Oral health examinations were conducted by professional Dentists holding at least Bachelor degree in Dental Surgery (BDS) and other professional training, following WHO guidelines. Socio-demographic and tobacco-use–related information was collected through interviewer administration for participants with limited literacy and self-completion for literate participants, under interviewer supervision. Completed forms were reviewed daily by the examining dentists to ensure completeness and accuracy of clinical assessments.
Data Analysis
Data were analyzed in IBM SPSS and AMOS (v25.0). Analytical methods included descriptive statistics, chi-square tests for bi-variate analysis and Structural Equation Modeling (SEM) with path coefficients to evaluate associations between variables, and goodness to fit.
To prepare OHFA items for Structural Equation Modeling (SEM) analysis, all responses were converted into numeric scores reflecting increasing severity of oral health problems. For example, the dental intervention item was coded as 1 = No treatment needed, 2 = Preventive or routine treatment, 3 = Prompt treatment including scaling, 4 = Immediate/urgent treatment due to pain or infection, and 5 = Referred for comprehensive evaluation or systemic condition. Enamel fluorosis, overall dental status, and dental erosion were recoded into ordinal scales, with higher values indicating worse conditions. The denture item, originally a yes/no question, was coded as a binary variable (1 = Yes, 2 = No). These recoding steps standardized the OHFA items, allowing them to serve as observed indicators of the latent oral health construct in the SEM model.
Given the modest sample size (n = 156) and the categorical nature of the observed indicators (binary and ordinal), Structural Equation Modeling (SEM) was conducted using Unweighted Least Squares (ULS) estimation in AMOS. 25 ULS is recommended for models with ordinal indicators and does not rely on multivariate normality assumptions. 46 To reduce the risk of overfitting and unstable estimates, we (a) modeled a single latent variable for “Oral Health,” (b) ensured each latent construct had a modest number of indicators, and (c) evaluated model fit using residual-based and incremental fit indices appropriate for ULS estimation (GFI, AGFI, RMR, NFI, RFI). Composite reliability and factor loadings were also evaluated to confirm indicator quality and measurement precision. Model fit was evaluated using a multi-index approach consistent with current recommendations for Structural Equation Modeling (SEM) involving categorical indicator types. Given that the OHFA indicators included a combination of binary and ordinal variables, model estimation was conducted using unweighted least squares (ULS) in AMOS, and fit statistics were interpreted cautiously. Overall model adequacy was assessed using fit indices appropriate for Unweighted Least Squares (ULS) estimation, including the Root Mean Square Residual (RMR), Goodness of Fit Index (GFI), Adjusted Goodness of Fit Index (AGFI), Normed Fit Index (NFI), and Relative Fit Index (RFI). The values of RMR <0.08 and GFI, AGFI, and NFI ⩾0.90 were considered indicative of acceptable model fit. 47
Chi-square-based and likelihood-based indices (eg, χ2, RMSEA, CFI, TLI) are not available under ULS estimation and were therefore not interpreted. Given the categorical nature of the observed indicators and the modest sample size, the use of ULS and reliance on residual-based and incremental fit indices is consistent with methodological recommendations for SEM with ordinal data. 46
Ethical Considerations
The study protocol was approved by the Ethical Review Committee of Daffodil International University (Ref: FHLS-REC/DIU/2021/0026). Institutional permissions were secured from the participating site, and written informed consent was secured from all participants.
Results
Socio-Demographic Characteristics
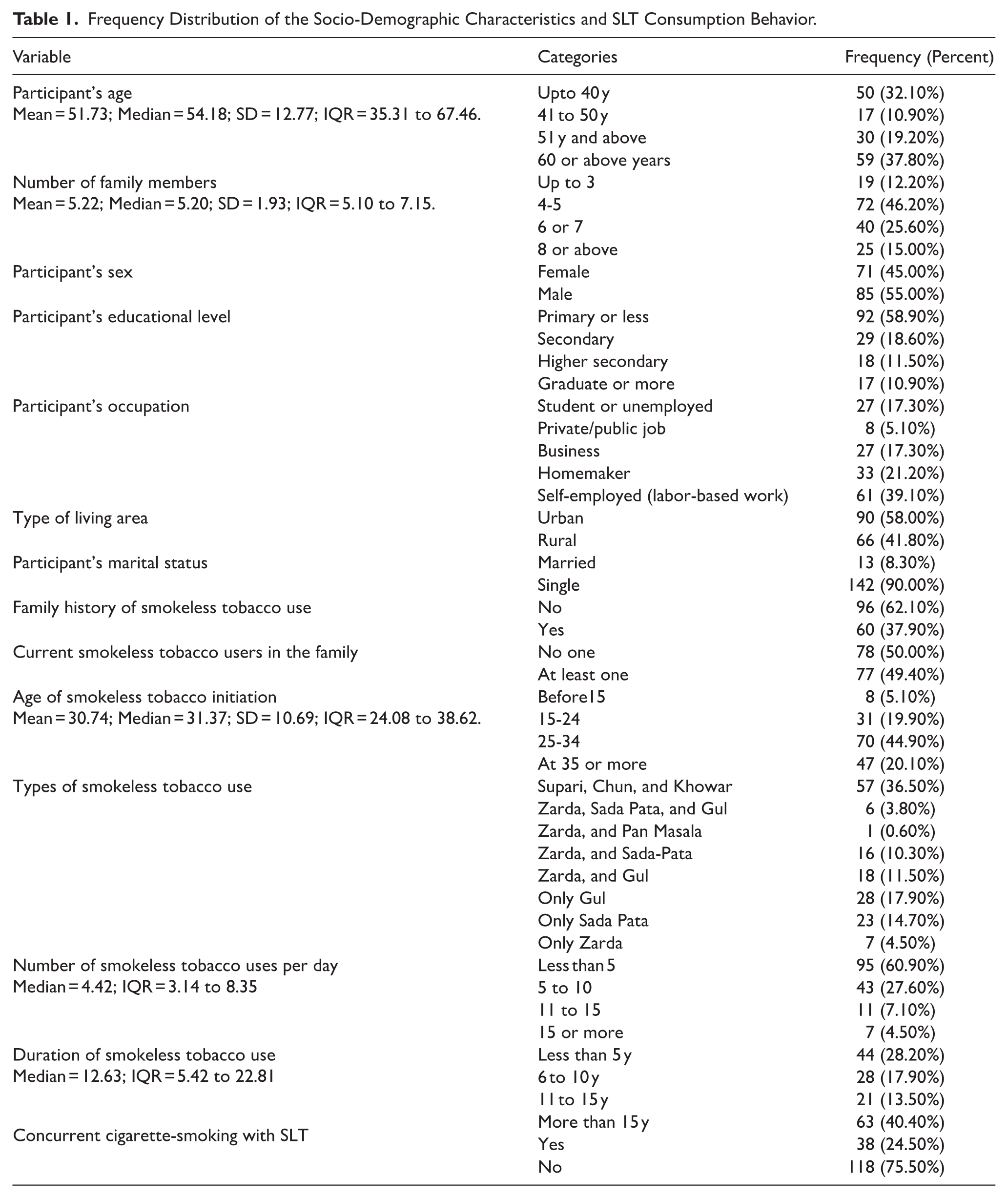
A wide variety of sociodemographic backgrounds were represented among the participants (Table 1). Men made up a small majority of the sample, and the majority were middle-aged or older. Most of the participants lived in urban areas, and households were typically large. The distribution of occupations showed a tendency toward low educational attainment, with homemaking and labor-based work being the most common types of employment.
Frequency Distribution of the Socio-Demographic Characteristics and SLT Consumption Behavior.
Smokeless Tobacco (SLT) Consumption Behaviors
The smokeless tobacco uses patterns of the participants varied (Table 1). A significant percentage stated that there was at least one active SLT user in the household or that there was a family history of SLT use. The majority of participants started using SLT after the age of 25, with initiation typically occurring in early to mid-adulthood. Numerous SLT products were reported, with some traditional preparations and mixed formulations being used more often than others.
The distribution of daily SLT consumption was skewed, with a low median number of uses and significant individual variability. Participants reported both relatively short-term and long-term patterns of use, and the duration of SLT use showed significant dispersion. Furthermore, almost 25% of the sample reported using SLT and smoking cigarettes at the same time.
SLT Using Behavior and Treatment Intervention Status
Spearman’s correlation analysis showed that greater urgency of dental intervention was significantly associated with earlier initiation of smokeless tobacco use (ρ = .328, P < .001), higher daily frequency of use (ρ = .176, P = .028), and longer duration of SLT consumption (ρ = .354, P < .001). In contrast, types of smokeless tobacco used and the presence of other SLT users in the family were not significantly correlated with treatment urgency (Table 2).
Association Between SLT Using Behavior and Status of Treatment Intervention.

Summary of Structural Equation Modeling (SEM) Results
Path Coefficients and Factor Loadings
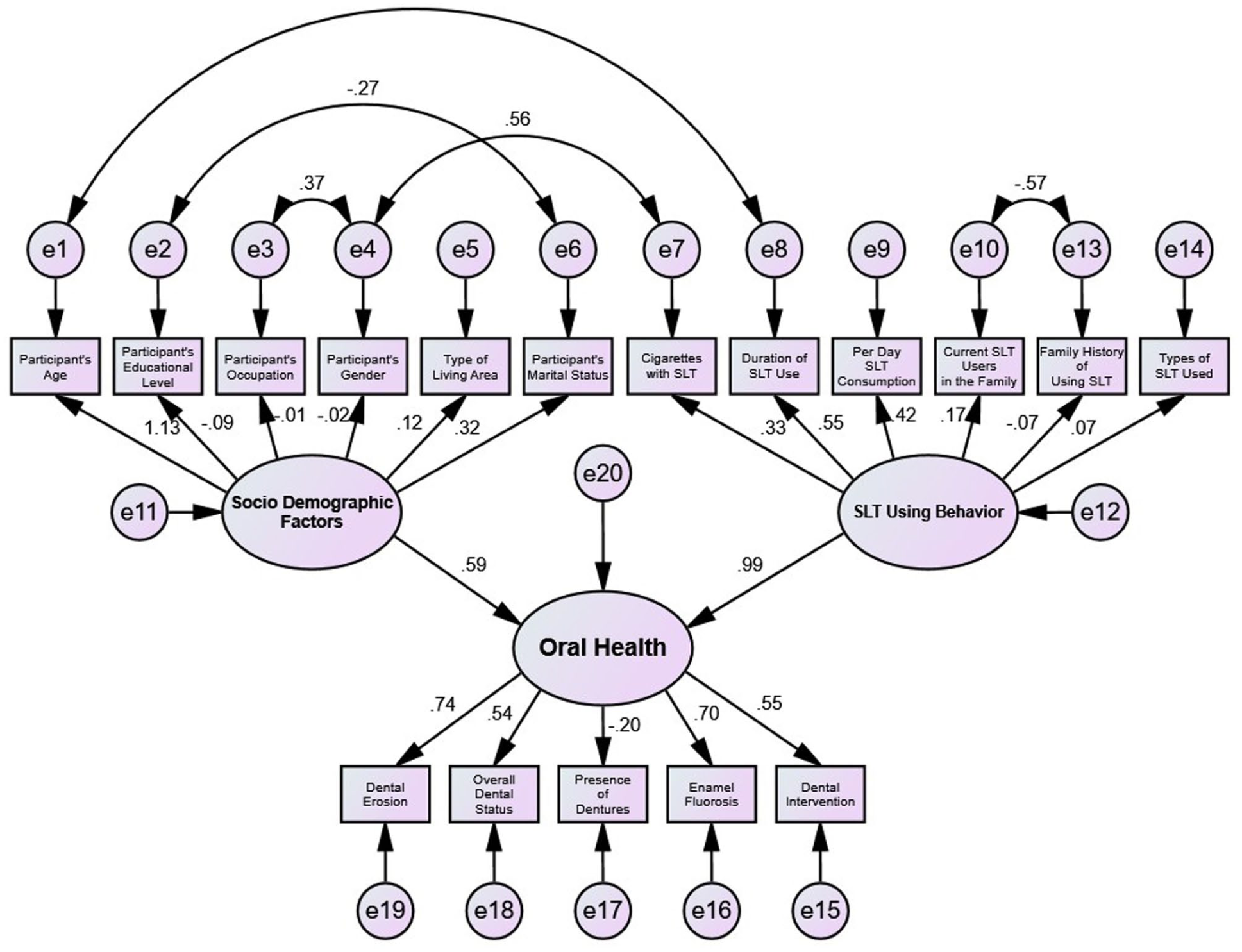
The standardized path coefficients for the proposed model (Figure 1) are detailed in Table 3. Within the constraints of a cross-sectional design and modest sample size, the analysis indicated a moderate positive association (standardized path coefficient = 0.59) between socio-demographic factors (Y1) and oral health (Z). In contrast, a comparatively stronger positive association (standardized path coefficient = 0.99) was observed between SLT using behavior (Y2) and oral health (Z). These coefficients should be interpreted as indicative associations rather than causal effects.
Association of socio-demographic factors and SLT using behaviors with oral health outcomes in structural equation modeling.
Each Component’s Standardized Path Coefficients.

Table 4 presents the standardized factor loadings for the latent constructs. For SLT using behavior (Y2), duration of use (0.55) and daily consumption frequency (0.42) showed the strongest positive loadings. For the oral health construct (Z), dental erosion (0.74), enamel fluorosis (0.70), overall dental status (0.54), and dental intervention need (0.55) exhibited substantial loadings, while denture status showed a small negative loading (−0.20). All loadings are reported as standardized estimates derived from the specified ULS-based model.
Identification of Significant Factors Related to Oral Health.

Model Fit Indices
The goodness-of-fit of the SEM was evaluated using multiple indices (Table 5). All but the Relative Fit Index (RFI) achieved recommended cut-offs. Although RFI is very close to the necessary level, which is acceptable. Consistent with current methodological guidance for SEM with mixed indicator types and smaller samples, model adequacy was therefore assessed using a holistic, multi-index approach rather than reliance on a single fit statistic. Overall, the pattern of fit indices suggests a reasonable representation of the observed data.
The Fitness Indices for Model in Figure-1.

Discussion
The present study underscores smokeless tobacco (SLT) use as a critical public health concern, particularly due to its detrimental effects on oral and dental health. The findings reveal a significant association between SLT consumption patterns and adverse dental outcomes among patients attending a tertiary dental care facility, thereby reinforcing the existing body of evidence on the oral health consequences of SLT use.
Socio-Demographic Determinants of Dental Health
The analysis identified significant correlations between socio-demographic characteristics such as education attainment, occupation, gender and overall oral health status among SLT users. Marital status, and occupational background were significantly associated with dental erosion severity, supporting the socio-economic model of health (SEAM), which posits that health outcomes are shaped by individual behavior in conjunction with structural socio-economic determinants.26,27 Notably, younger adults—particularly those under 40 years of age—exhibited a higher prevalence of dental erosion. This pattern is consistent with global trends indicating a rise in SLT consumption among youth, influenced by social acceptance and limited awareness of SLT’s adverse health implications.23,28 Marketing strategies that normalize SLT use among adolescents further perpetuate this behavior.29,30 Moreover, occupational disparities were evident, with housewives exhibiting comparatively poorer dental health outcomes. This may reflect gendered inequities in healthcare access, oral health literacy, and prioritization of personal health within lower socio-economic strata. 15
SLT Consumption Behaviors and Oral Health Impacts
Behavioral attributes of SLT consumption—including age of initiation, type of SLT, frequency, and duration of consumption—were significantly associated with overall oral health. Individuals consuming SLT more than 5 times per day demonstrated substantially higher rates of dental erosion and a greater need for clinical intervention. These findings align with prior studies establishing a dose-dependent association between SLT use intensity and oral pathology.31-33 The observed trends can be explained by cumulative exposure theory, wherein prolonged and repeated SLT use is linked to progressive oral tissue degradation. 15 Furthermore, the social embeddedness of SLT use—often occurring within communal or peer settings—reinforces habitual patterns and perpetuates dependence, particularly in cultural contexts where SLT use is normalized.34,35
Insights From Structural Equation Modeling (SEM)
The Structural Equation Model (SEM) analysis explored the interrelationships among behavioral and socio-economic dimensions in relation to SLT-related oral health status, highlighting the multifactorial structure underlying the observed associations. Rather than inferring causality, the model was used to illustrate pathways and covariation patterns that may be informative for hypothesis generation and programmatic planning. The findings underscore the potential relevance of tailored interventions focusing on younger populations and individuals from lower socio-economic backgrounds. Public health initiatives incorporating education, behavioral counseling, and accessible cessation support may be aligned with the patterns identified.36,37 The strategic use of social media platforms can enhance outreach to younger demographics, 38 while community engagement involving local leaders and healthcare professionals may strengthen social support for cessation efforts. 39
Educational Interventions and Health Literacy
A clear association was observed between lower educational attainment and poorer oral health, underscoring the pivotal role of health literacy in shaping SLT-related health behaviors. Broad, population-wide educational interventions that are suitable and reasonable for different demographic groups and aimed at enhancing awareness of SLT’s risks and promoting oral hygiene are warranted.40,41 Evidence suggests that well-designed health education programs significantly improve knowledge and influence positive behavioral change. 42 To maximize efficacy, such programs should be demographically tailored with age-appropriate content and delivery, particularly for adolescents and young adults, and disseminated through culturally sensitive and accessible channels, including school curricula and digital media. 43
Policy Implications for Tobacco Control
The findings strongly indicate the need for comprehensive tobacco control frameworks encompassing both smoking and SLT use. Given the observed association between age of initiation, duration of use, and treatment intervention status, policy measures should focus on restricting the availability and marketing of SLT products, particularly to minors. Historically, tobacco control efforts have disproportionately targeted smoking, leaving critical gaps in the regulation of SLT products. 44 Policy strategies such as taxation, advertising bans, and the integration of SLT cessation programs into broader tobacco control initiatives could significantly reduce consumption rates. 44
Future Research Directions
This study highlights specific patterns of SLT use and their association with oral health behaviors and outcomes among the target population, offering some insights into risk factors that may not have been fully characterized previously. Further longitudinal research is warranted to elucidate causal relationships and long-term effects. Future investigations should assess the efficacy of intervention strategies, explore behavioral determinants across different cultural contexts, and evaluate community-specific perceptions of SLT products. Such research will be essential in developing nuanced, evidence-based interventions that effectively address this persistent public health challenge.44,45
Limitations
Several methodological constraints should be noted. First, the cross-sectional design means the relationship between socio-demographic characteristics and oral health cannot be interpreted causally. Second, the model’s modest fit indices suggest the possible omission of relevant mediating variables, such as specific oral hygiene behaviors and salivary factors. The reliance on self-reported socio-behavioral data also introduces the potential for recall bias, which may have diluted the strength of the observed associations. Third, the study did not include a SLT non-user comparison group; therefore, oral health differences could not be contrasted with SLT non-users, limiting contextual interpretation of SLT-related findings. Fourth, although a target sample size of 172 was calculated, 16 participants withdrew consent after enrollment, resulting in a final sample of 156; this reduction may have slightly decreased statistical power and introduced selection bias. Finally, the SEM was conducted with a relatively small sample size, which may affect the stability and generalizability of parameter estimates despite efforts to limit model complexity and apply multiple fit indices. Overall, generalizability is further constrained by the hospital-based study setting, which may over-represent individuals seeking care and limit external validity.
Conclusion
In summary, this study indicates that smokeless tobacco (SLT) consumption is associated with adverse oral health outcomes, with the duration of use appearing as a particularly important risk factor. These results underscore the imperative for public health initiatives to prioritize SLT cessation as a primary intervention strategy. The application of Structural Equation Modeling provides a validated empirical framework for identifying high-risk demographic profiles. Consequently, policy should be directed toward developing tailored literacy programs and early clinical interventions designed to prevent initiation and curtail prolonged use, thereby alleviating the significant oral health burden attributable to SLT. Moreover, the statements about the urgent need for intervention are warranted given the observed associations.
Supplemental Material
sj-doc-1-sat-10.1177_29768357261425434 – Supplemental material for Association of Dental Status and Smokeless Tobacco (SLT) Using Behavior Among Bangladeshi Dental Patients: A Structural Equation Modeling (SEM) Analysis
Supplemental material, sj-doc-1-sat-10.1177_29768357261425434 for Association of Dental Status and Smokeless Tobacco (SLT) Using Behavior Among Bangladeshi Dental Patients: A Structural Equation Modeling (SEM) Analysis by Nasima Akter Mukta, Syed Billal Hossain, Kazi Mahfujur Rahman, Md. Hazrat Ali and Mst. Kamrun Nahar Sorna in Substance Use: Research and Treatment
Supplemental Material
sj-docx-2-sat-10.1177_29768357261425434 – Supplemental material for Association of Dental Status and Smokeless Tobacco (SLT) Using Behavior Among Bangladeshi Dental Patients: A Structural Equation Modeling (SEM) Analysis
Supplemental material, sj-docx-2-sat-10.1177_29768357261425434 for Association of Dental Status and Smokeless Tobacco (SLT) Using Behavior Among Bangladeshi Dental Patients: A Structural Equation Modeling (SEM) Analysis by Nasima Akter Mukta, Syed Billal Hossain, Kazi Mahfujur Rahman, Md. Hazrat Ali and Mst. Kamrun Nahar Sorna in Substance Use: Research and Treatment
Footnotes
Ethical Considerations
Ethical approval was obtained from the ethical review committee of the Faculty of Health and Life Sciences of Daffodil International University, Bangladesh (Ref: FHLS-REC/DIU/2021/0026).
Consent to Participate
All the study participants were informed about the objective of the study and their written consent was obtained. The confidentiality of the information was maintained strictly.
Authors Contributions
N.A.M.: Conceptualization, Writing - original draft, and Writing - review & editing; S.B.H.: Conceptualization, Supervision, Formal analysis, Writing - original draft, Visualization, and Writing - review & editing; K.M.R: Formal analysis, Writing - original draft; M.H.A.: Formal analysis, and Writing - original draft; M.K.N.S.: Writing - original draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.*
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.