
Abstract
Introduction
Smokeless tobacco (SLT) is a prevalent tobacco-consuming form. It was popular in Asian countries and also in Africa. During the 20th century, it emerged in the USA and European countries. 1 Usually, SLT is consumed nasally or orally (without burning). Oral SLT goods are consumed by chewing as loose leaf, plug, or twist form. Snuff is another form (powdered) of SLT that can be taken as moist or dry, and consumed orally by applying to the teeth or gums. Dry one can be also inhaled nasally. 2 Nicotiana tabacum and N Rustica are used for most SLT products. Along with other tobacco alkaloids, nicotine is about 85-95% of total alkaloids in SLT. Mainly leaves with stems are blended to gain nicotine content, pH, and flavor. Worldwide, various SLT products are consumed usually consumed only or with other products. The occurrence of SLT consumption can vary noticeably across the countries, and also within the countries.
Tobacco use has been proven as one of the predominant public health concerns that the whole world has ever challenged. Around six million losses a year are responsible for the frequent use of tobacco. 3 The ease of getting processed or unprocessed forms of raw tobacco goods also leads Bangladesh to the worst position that possibly exposes the underprivileged people further to the health risks of SLT goods. Several toxic, mutagenic, and carcinogenic constituents were reported to be present in those products of SLT. 4 The lack of awareness and knowledge on the critical effects of SLT are the key reasons to be exposed to addictive smokeless tobacco use. Smokeless tobacco consumption is related to numerous adverse health consequences such as cancer, hypertension, cardiovascular disease, and many other diseases including life-risk complications during pregnancy as well as different antagonistic results of pregnancy. 5
Some states of South Asia are the main tobacco producers and net exporters. About 90% of the world’s smokeless tobacco consumers live in South-East Asia. In Bangladesh, India, Pakistan, and Sri Lanka, men as well as women are habituated culturally in the consumption of SLT as the form of betel quid. 6 Among the countries of South Asia, the position of Bangladesh as a tobacco grower is also central. In this country, tobacco leaves are easily accessible for use as smokeless tobacco. 7 In Bangladesh, the usual forms of SLT intake are betel quid, tooth powder (tobacco), and tobacco with lime. In any small and large social get-togethers, it is customary to use SLT in the form of betel quid after having the food. 8 A chewable form of smokeless tobacco use is a pervasive form of SLT consumption in Bangladesh. Women about 39%, and men about 22% were reported to practice that form of SLT in this country. 9 Not only men and women but young and children are also habituated to several newly packed forms and flavored forms of smokeless tobacco products. Usual forms such as Sada–pata (sun-dried, typically at home), Gul, and Zorda (processed industrially), are economical, and thus amounts of use are comparatively higher in low-earning urban entities. 10 As these products are beyond the concern of regulatory authorities there is no warning on the label about the constituents such as nicotine percentage as well as its health risks. Adversely, there are public misunderstandings amongst diverse demographic regions of people in Southeast Asia as well as Bangladesh that this form of tobacco consumption is not as unsafe as cigarettes and worth it for the gums and teeth thus subsequently being used in the form of Gul (dentifrice). 11 Because of such misrepresentation of chewing SLT, a large number of people practice it to clean teeth, as an oral refresher, and to get relief from several pains. Some users keep betel quid in touch with the oral mucosa used for prolonged periods, even the whole night.
Consumption of this form of tobacco varies with gender, age, indigenous origin, and socioeconomic features. 12 Intake of SLT with the mixture of betel leaf, slaked lime, areca nut, and some spices (known as betel quid) has been now integrated into the cultural life in some countries which is the most frequently used form of smokeless tobacco. The occurrence of smokeless tobacco usage was revealed as more in the rural areas and was advanced amongst socioeconomically underprivileged people. 4 Though the mouth is the access to a health condition, we infested this entry by using SLT (Zarda and Gul). 13 More than twenty-seven percent of adults 15 years old or older than this age practice smokeless tobacco in Bangladesh and the usage of smokeless tobacco is correlated with the sociodemographic status of the individual. The Occurrence of health risks such as oral cancer, stroke, and heart disease has increased reflected in the life loss of about three lacks and twenty thousand within 2010 in Bangladesh. 14
A few studies are known that focused on the exposure of a particular sociodemographic group to smokeless tobacco ingestion behaviors and allied health values, mostly targeted to rural and underprivileged populations.8,13 The worldwide prevalence of oral cancer is increasing and about seven thousand subjects are identified yearly in Bangladesh. 15 Therefore, the objective of this study was to determine the association of sociodemographic characteristics and smokeless tobacco consumption behavior among dental patients.
Methods
Study Design
It was a cross-sectional study conducted from 24 April 2024 to 15 September 2024.
Study Sample
All the participants were patients attending outdoor services (OPD) of the selected tertiary dental hospital named, Dhaka Dental College and Hospital. The sample size was determined using a single proportion formula for a population,

Based on this- n = (1.64)^2*(0.80)*(0.20)/(0.05)^2 = 172
Sample size was estimated 172, however, 156 participants were included in the study by Purposive sampling method, due to incomplete response by the remaining participants.
Selection Criteria
Dental patients of 18 years and above with at least 10 natural Teeth, who visited at the Outdoor department in the selected dental hospital for treatment were the population of the study. Apparently healthy dental patients both smokers and non-smokers, who consume either form of smokeless tobacco were included for this study. Patients less than 18 years, and who were not willing or/and unable to attend the survey questionnaire administration due to physical or mental causes were excluded.
Data Collection Tool and Methods
A semi-structured questionnaire was prepared which comprised items focusing on socio-demography, smokeless tobacco-using behavior, oral hygiene-related clinical information, and duration of SLT Taking, including “WHO Oral health assessment form for adults 2013”. 18 To validate, the prepared questionnaire was pilot-tested among 16 randomly selected participants (10% of the sample size) among selected population, prior to the main survey and adjusted some of the coding categories of the variables for collecting data from included participants. Data were collected by both interviewing and self-administration depending on the patient’s educational status.
Data Quality Control Measures
The questionnaire was translated into Bengali and back-translated to English to conform to its original meaning and to maintain an unbiased response. The filled questionnaire was checked daily for completeness. The questionnaire was evaluated for its content and modification was done for some literacy questions by adding oral health status questions specific to our society to the relationship between oral hygiene and smokeless tobacco related questionnaire.
Data Analysis Method
All of the interview data was double-checked for mistakes, then coded into the database and analyzed by using statistical software named IBM SPSS (version 25.0), and IBM SPSS AMOS (version 25.0). The study objectives were the focus of the analysis, and so were the indicators. To evaluate the association among variables, we used statistical tests such as Fisher’s exact χ2 test, Structured equation modelling (SEM) including specific path coefficients of the association of the variables.
Ethical Considerations
The study protocol was reviewed and approved by the Ethical Review Committee of the Faculty of Health and Life Sciences, Daffodil International University (DIU), Dhaka, ethical approval Number: FHLS-REC/DIU/2024/0007. Permission was also taken from all the educational institutions of the participants responded in the study. Additionally, during survey, after a brief explanation of research objectives and methods, written informed consent were taken before interview from each study participant.
Results
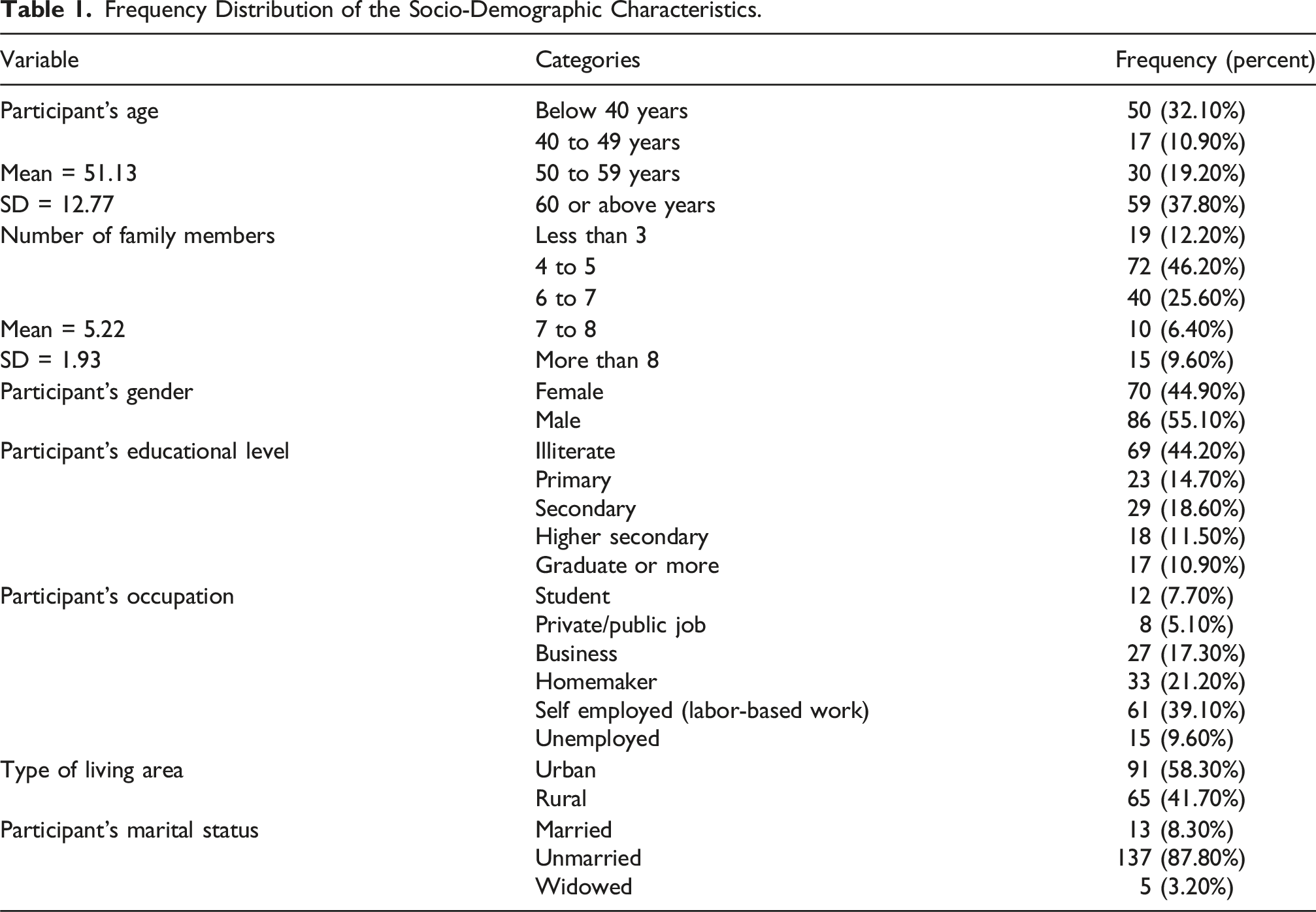
Frequency Distribution of the Socio-Demographic Characteristics.
Frequency Distribution of the Information Regarding SLT Consumption Behavior.

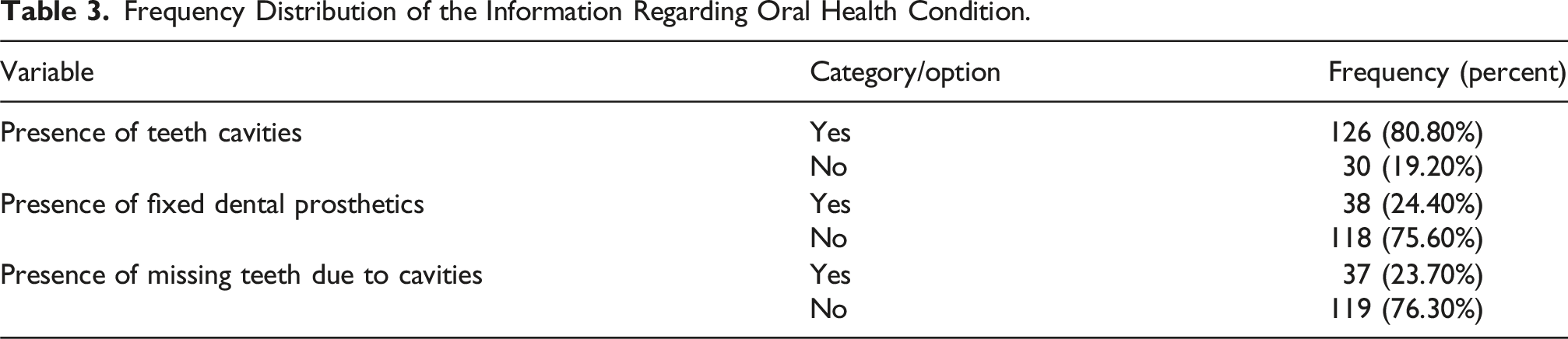
Frequency Distribution of the Information Regarding Oral Health Condition.
Association Between Socio-Demographic Status and SLT Consumption With Smoking.

Association Between Socio-Demographic Status and Duration of SLT Consumption.

The number of children also plays a crucial role, with a highly significant P-value of .000. Those with no children or more than four children tend to use SLT for longer durations. Age is another important factor, with a P-value of .000, indicating a significant association. Those below 40 years of age are more likely to use SLT for extended periods. Family size demonstrates significance, with a P-value of .010. Larger families tend to have individuals who use SLT for shorter durations. Lastly, the educational level does not appear to have a significant impact on SLT usage duration, with a non-significant P-value of .684. This table underscores the importance of considering socio-demographic factors when examining SLT usage duration. Marital status, the number of children, age, family size, and living area all appear to play a role in influencing how long individuals engage in SLT use. These findings can inform targeted interventions and public health campaigns to address SLT usage (Table 5).
Figure 1 and Table 6 presents the results of the structural equation model (SEM) for the relationship between socio-demographic factors (Y1) and SLT (Smokeless Tobacco) using behavior (Z). The construct “Socio-demographic Factors” is denoted by Y1, and the construct “SLT Using Behavior” is represented by Z. The path coefficient between socio-demographic factors and SLT-using behavior is 0.839. The path coefficient of 0.839 indicates a strong positive relationship between socio-demographic factors and SLT-using behavior. This suggests that as socio-demographic factors increase, there is a corresponding increase in SLT-using behavior. The positive sign of the coefficient implies that higher levels of socio-demographic factors are associated with a higher likelihood of engaging in SLT use. Association Between SLT Consumption Behaviors and Socio-Demographic Factors. Specific Path Coefficients of the Association of Socio-Demographic Characteristics and SLT Consumption Behavior. [Significance of Coefficients: **: P < .001 (highly significant); *: P < .05 (Statistically significant); ns: P > .05 (not significant);].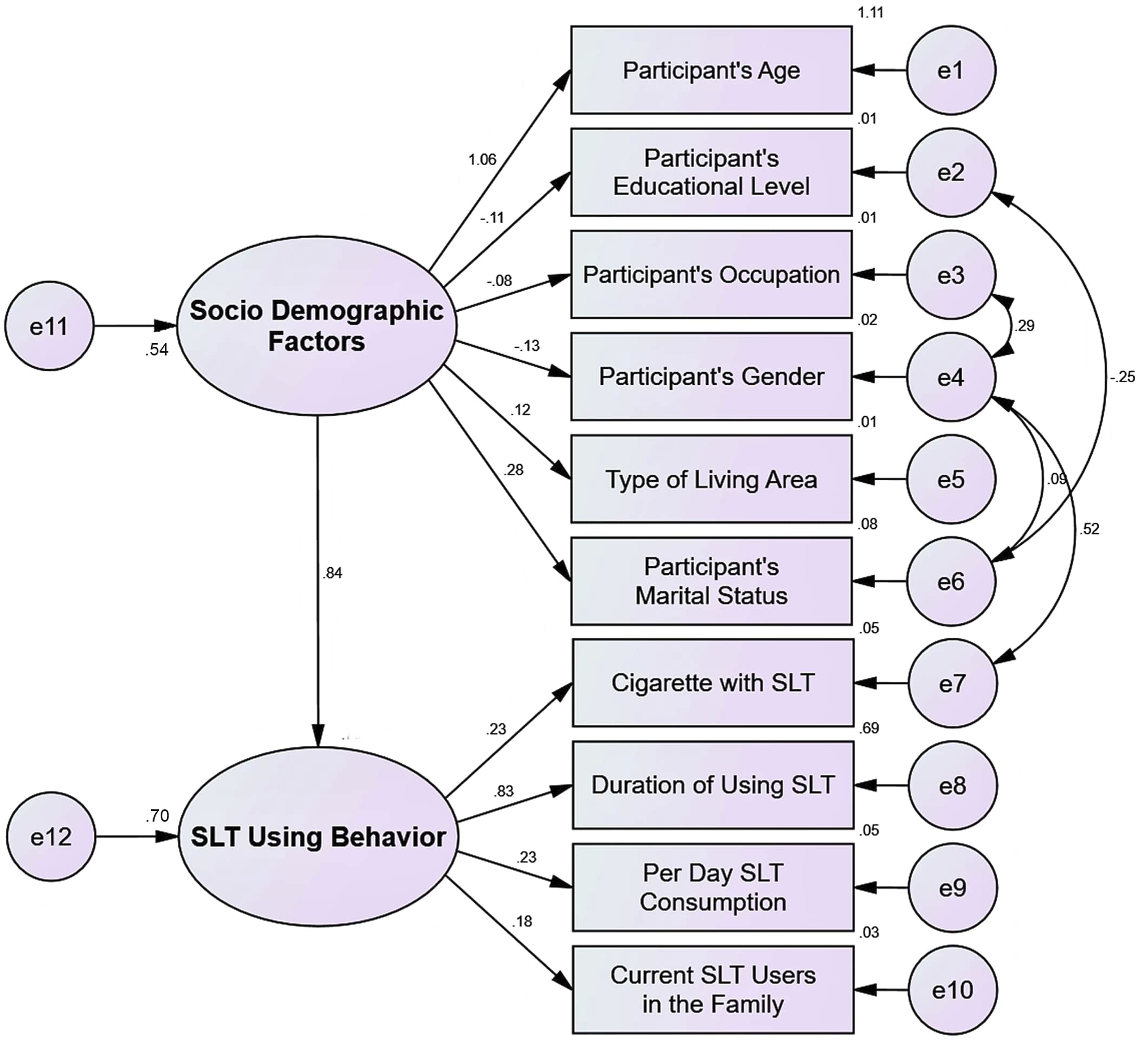
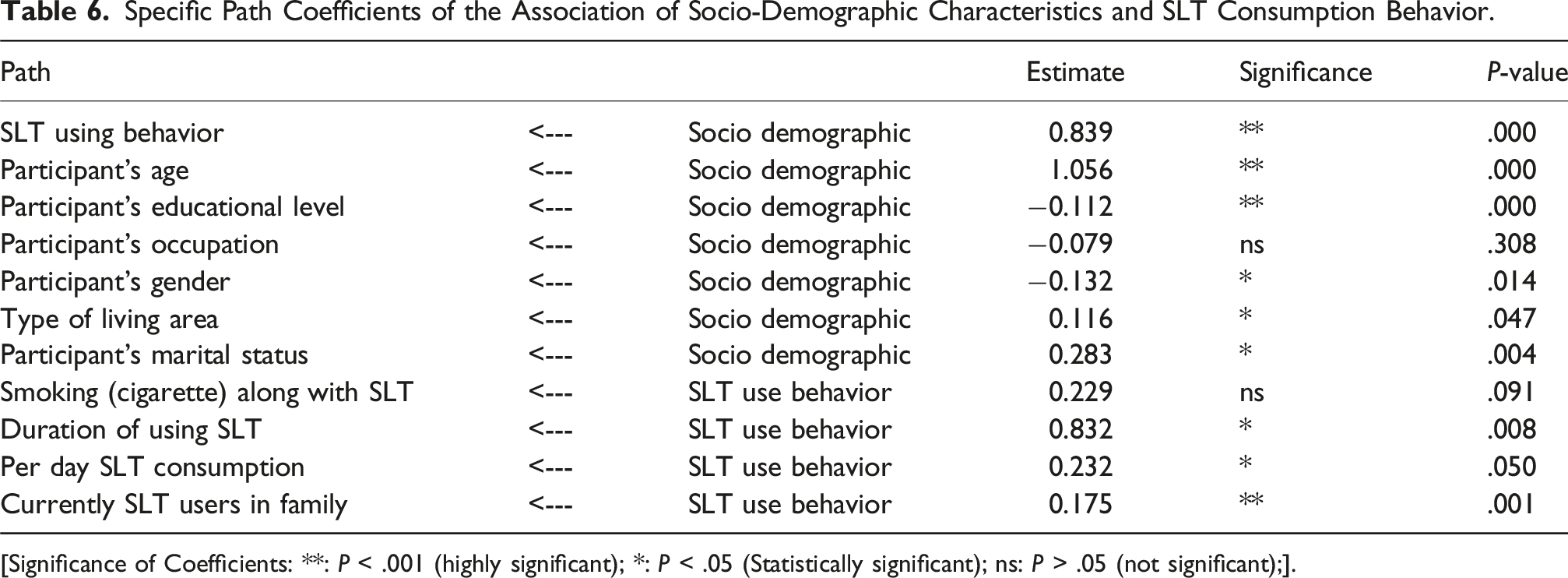
Table 6 presents the specific association of socio-demographic factors and SLT consumption behavior through path estimation. The analysis shows that participant’s age has a significant positive effect on SLT using behavior (Estimate = 1.056, P < .001), suggesting that as participants age, their likelihood of using SLT increases. Participant’s educational level has a significant negative effect on SLT using behavior (Estimate = −0.112, P < .001), indicating that higher education is associated with a reduction in SLT use, acting as a potential protective factor. However, participant’s occupation does not have a significant effect on SLT use behavior (Estimate = −0.079, P = .308), meaning that occupation alone does not strongly influence SLT usage. Participant’s gender shows a significant negative effect (Estimate = −0.132, P = .014), suggesting that male participants are more likely to engage in SLT use than females. Type of living area has a significant positive effect on SLT use behavior (Estimate = 0.116, P = .047), indicating that individual’s living area influence the use of SLT. Participant’s marital status has a significant positive effect on SLT consumption behavior (Estimate = 0.283, P = .004), indicating that married individuals are more likely to engage in SLT use compared to those who were unmarried.
Regarding the SLT using behavior factors (Table 6), smoking along with SLT has a positive effect on SLT consumption (Estimate = 0.229), but this effect is not statistically significant. The duration of SLT use shows a significant positive effect (Estimate = 0.832, P = .008), suggesting that the longer an individual uses SLT, the more likely they are to continue its use. The per day SLT consumption has a marginally significant positive effect (Estimate = 0.232, P = .051), meaning that individuals who consume more SLT daily tend to use it more frequently, although the effect is marginal. Lastly, having current SLT users in the family has a significant positive effect on SLT using behavior (Estimate = 0.175, P < .001), indicating that individuals with SLT users in their family are more likely to engage in SLT consumption, highlighting the influence of family dynamics.
Besides, the R2 indicator (Figure 1) for SLT using behavior (0.70), provides a moderate indication of explained variance, which indicates the independent variable Socio-demographic factors explain 70% of the variation of the dependent variable, SLT using behavior.
The Fitness Indices for Structural Equation Model (SEM).

Discussions
This research work studied for whether the relationship between socio-demographic characteristics and smokeless tobacco (SLT) usage behavior among patients be the outdoor department of a dental tertiary hospital. This research was conducted outdoors in a tertiary dental hospital which represents patients from different socio-demographics which could be the reason for non-significant gender discrimination in SLT consumption. The study reveals that the percentage of families where at least one male member practices SLT is greater (51%) than that of families in which at least one female member (48 %) uses the same, there is no significant difference (P > .05) in the same between the male and female members. A previous study reported that smokeless tobacco intake was estimated as 29% in Bangladesh, and the prevalence is greater in females (33%) than in males (23%) which was found to be more than the national prevalence in rural areas of the country. 19 SLT consumption as a chewing form in males is lower than that of females. Gender disparity in SLT consumption was reported to differ with the socioeconomic status and also with the locality but was not reported as significant in Bangladesh as well as other Southeast Asian countries. 20 Prevalence of SLT consumption is increasing as customarily in Bangladesh, there is no disapprobation of using smokeless tobacco, irrespective of whether men or women. Many people practice smokeless tobacco which is culturally not forbidden. SLT use in people of rural areas is greater than the SLT use in people of urban areas. This trend is also observed in unmarried, widows, students, and unemployed people or those who are staying at home, people of age more than 60 years, and between 40-49 years. 21
In this study, education was found to be not associated with SLT consumption behavior, however, variations in SLT usage due to educational factors were observed as more prominent in India (urban regions) and Bangladesh (rural regions). 22 The study finds a significant correlation (P ≤ .05) between the number of children and smokeless tobacco use as well as the family members and use of SLT. Prevalence of the SLT usage is highest in the person who had no children followed by the respondent who had four or more than four children. Similarly, the occurrence of SLT use is greater in comparatively larger family sizes rather than smaller ones. An earlier study on low socio-economic people in Bangladesh revealed that family size had a non-significant relationship with SLT usage. 13 This endeavor also focuses on the consumption of SLT with cigarettes (smoke form) and it reveals that all socio-demographic parameters such as gender, marital status, age, family size, no. of children, and occupation except living area, and education are significant (P ≤ .05) allied with the ingestion of cigarettes and SLT. No noticeable difference was found in the occurrence of tobacco use (smoke) between the people of rural and urban regions but the usage of SLT was higher in the people of rural areas. 23 Another study compared the use (at home in Bangladesh) of tobacco in urban and rural zones which revealed the rural usage of smoking and smokeless tobacco is higher than the usage of urban areas. 24
Regardless of gender, occupation (labor-based) is found to be associated with a higher occurrence of smoking in the studies. 25 However, in this study, participant occupation showed no significance with SLT consumption. Male and unmarried respondents are more prone to use both cigarettes and SLT than female and married participants. Whereas widows show no use of both forms of tobacco together. This may be due to the cost of cigarettes and considering the social tattoos against the use of cigarettes rather than SLT products. In addition, people of age less than 40 years old, who have a family size of four to five members, and who have two children are more inclined to tobacco use both cigarettes and SLT. Students and self-employed (labor-based) are more susceptible to both forms of tobacco usage than the participants of other occupations. The existing smoking (tobacco) occurrence in Bangladeshi students (university) was reported as over 60%. 26 The prevalence of SLT instigation in the Bangladeshi population (age 15-24 years) is increasing evidently. 27 However, socio-demographic parameters such as age, living area, marital status, family members, and number of children significantly (P ≤ .05) vary with the duration of the use of smokeless tobacco. SEM analysis of the study found the path coefficient of 0.84 indicates a strong positive relationship between socio-demographic factors and SLT-using behavior. This suggests that as socio-demographic factors increase, there is a corresponding increase in SLT-using behavior. The positive sign of the coefficient implies that higher levels of socio-demographic factors are associated with a higher likelihood of engaging in SLT use. A comprehensive work in Pakistan accompanied by patients visiting tertiary care hospitals revealed that the ingesting of SLT was increased in the poor socio-economic group with insufficient income. 28 SLT users especially older people, housewives, widows, females, illiterate, and people with poor socio-economic conditions had a noteworthy relationship with several health hazards. 19
All of these findings among a group, where 81% of the participants hade tooth cavities, 75% with dental prosthetics and about 24% were missing tooth due to cavities clearly indicates that, SLT consumption not only associated with socio-demographic factors, it also affects oral health.13-15
Aside from a few unique findings, the study had certain limitations. As Because this was a cross-sectional study in which both the outcome and the exposure were assessed concurrently, the time-course connection between the outcome and the exposures could not be determined. The study only included patients from only one tertiary dental hospital, limiting the generalizability of the findings. While about 9.3% of the estimated participants couldn’t include for their incomplete responses. Another downside of this study was the limited number of participants due to financing and time constraints.
Conclusion
Socio-demographic variables are strongly linked with smoking cigarettes during SLT usage and the duration of SLT use. In Bangladesh, smoking and SLT may be the subjects of campaigns to increase public awareness of tobacco usage. The findings clearly indicated that, socio-demographic factors influence the SLT consumption behavior and associated with Oral health conditions. The tobacco consciousness attempts in this country might involve setting prominence on SLT as well as smoking. It can be proposed from the study that organized and collaborative efforts of the organizations, directing both smoking and smokeless tobacco use lessening and end, may be adjusted to reach a population comprising who are female, students, and ageing population. Majority of the Tobacco control plans mark mainly smoking, corresponding attempts are desirable that will also comprise smokeless tobacco usage in the tobacco regulating policy and inhibition approaches.
Supplemental Material
Supplemental Material - Smokeless Tobacco (SLT) Consumption Behavior and Associate Socio-Demographic Factors Among Bangladeshi Dental Patients
Supplemental Material for Smokeless Tobacco (SLT) Consumption Behavior and Associate Socio-Demographic Factors Among Bangladeshi Dental Patients by Syed Billal Hossain, Tabasum Ferdous, Md. Hazrat Ali, Md. Nawal Sarwer, Akibul Islam Chowdhury, Mir Apel Mahmud, Lipi Rani Mondal, and Nasima Akter Mukta in Tobacco Use Insights
Footnotes
Authors’ Note
The study was conducted to fulfill an academic purpose.
Acknowledgements
Pleased to thanks the Department of Public Health, University of Science and Technology Chittagong (USTC) and Department of Public Health, Daffodil International University, for their assistance in Sampling and Data collection process of the study.
Ethical Statement
Author Contributions
Syed Billal Hossain: Conceptualization, Formal analysis, Supervision, Formal analysis, Writing - original draft, and Writing - review & editing; Tabassum Ferdous: Conceptualization, Formal analysis, and Writing - original draft; Md. Hazrat Ali : Formal analysis, and Writing - original draft; Md. Nawal Sarwer: Writing - original draft; Akibul Islam Chowdhury: Writing - original draft; Mir Apel Mahmud: Formal analysis, Writing - original draft; Lipi Rani Mondal: Writing - original draft, and visualization; Nasima Akter Mukta: Conceptualization, Supervision, and Writing - review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Study data will be given on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.