
Abstract
Background:
Rural communities face significant implementation challenges addressing the overdose epidemic, including limited treatment capacity, pervasive stigma toward people who use drugs, and social and political opposition to evidence-based interventions.
Objectives:
Rather than implementing prescribed harm reduction services that may face community resistance, the Ohio Opioid Project adopted a capacity-building approach to address structural barriers and enhance community readiness for future harm reduction and treatment innovation across 3 rural Appalachian Ohio counties.
Methods:
This applied implementation project used the Evidence-Making Intervention framework with process evaluation. Mixed-methods formative research included interviews with stakeholders (n = 34) and people who use drugs (n = 30), respondent-driven sampling surveys with people who use drugs (n = 258), organizational network analysis, and surveillance data review. A 9-member Community Leadership Board – including health commissioners, treatment providers, and harm reduction program representatives – co-developed interventions targeting 3 structural barriers: substance use-related stigma, interagency fragmentation, and inadequate provider capacity. Community members served as leadership board representatives, implementation staff, intervention consultants, and data collectors, democratizing research involvement and building local public health capacity. Implementation followed an adaptive approach, allowing activities to evolve based on emerging needs, policy changes, and the COVID-19 pandemic.
Results:
The service delivery plan included 20+ activities across stigma reduction, interagency coordination, and provider capacity building. Key activities included peer recovery supporter training, law enforcement harm reduction seminars, faith-based stigma reduction forums, conflict resolution processes, establishment of drug court buprenorphine protocols, and HCV telehealth partnerships. Multiple activities were sustained by community partners beyond the research period, including resource clearinghouses, new regional partnerships, and organizational protocols integrating harm reduction into existing services.
Conclusions:
Capacity-building implementation science can address structural barriers to community-based harm reduction in resistant rural settings. By prioritizing community co-creation and adaptive implementation, this approach created foundational conditions for sustainable harm reduction innovation while respecting local contexts and readiness for change.
Keywords
Introduction
More than 1 million Americans have died from overdose in the past 25 years. 1 Rural areas face unique challenges in addressing the overdose epidemic, including substance use treatment capacity, social and political opposition to harm reduction, and pervasive community stigma toward people who use drugs.2-6 In 2017, four federal agencies, led by the National Institute on Drug Abuse, established the Rural Opioid Initiative (ROI) to characterize the landscape of the epidemic in 8 rural regions and to implement demonstration projects that address regionally defined needs. 7
The Ohio Opioid Project (OHOP) aimed to build community capacity for evidence-based intervention (EBIs) rather than conducting formal implementation trials of EBIs. The impetus for this approach came from a series of discussions with local leaders who felt that their communities would be resistant to EBIs that were still culturally stigmatized or lacked necessary infrastructure, including syringe service programs, harm reduction mobile units, and overdose response teams.6,8 In other words, readiness for change was deemed a community-level barrier to implementation of these initiatives.9,10
Rather than impose prescribed best practices on these communities, we opted to co-create a package of intervention activities that met their identified priorities and readiness for change, with the expectation that these activities would accelerate local capacity to build and sustain more difficult and culturally tenuous solutions in the long term.11-13 In doing so, we adopted principles from the Evidence-Making Intervention (EMI) framework. EMI acknowledges that interventions are “never fixed nor stable or universal but always in process” 14 (p. 6). Implementation science within an EMI framework permits flexibility and adaptiveness rather than adherence to protocol. 14 Community members are treated as co-creators of evidence in this process, and interventions become mutable objects that can unfold and adapt to local context.
This paper describes the process of selecting, implementing, and evaluating a package of community-based capacity-building interventions in 3 rural counties in Appalachian Ohio. As a high-level case study drawn from a broader, multi-component project, it focuses on the key processes that shaped implementation rather than providing a comprehensive report of all activities or outcomes. We begin by outlining the local context and processes of community engagement. We next describe the selection of priority topic areas and intervention activities within each topic area. We conclude by sharing implementation outcomes and key lessons for applied implementation projects in substance use service delivery.
Methods
The Ohio Opioid Project (OHOP) was an applied implementation project initially designed to improve access to HIV and HCV screening and harm reduction services in a tri-county area in southern Ohio facing high rates of overdose and HCV. OHOP was 1 of 8 projects of the Rural Opioid Initiative (ROI), a consortium of research institutions addressing outcomes of the overdose epidemic. 7 The consortium intended to address both opioid use and injecting drug use; most ROI participants who used opioids also used other drugs, primarily methamphetamine. 15 OHOP drew from the Exploration, Adoption/Preparation, Implementation, and Sustainment (EPIS) model for evidence-based implementation. 16 This model incorporates outer factors (social, cultural, political environment) and inner factors (organizational environments, characteristics of service providers and recipients) that can affect effective implementation. Using this framework as a guide, OHOP proceeded in phases with data collection from people who use drugs, key public health actors, and agencies. Initial data were interpreted with community input and plans for relevant intervention activities developed. Planning and implementation were grounded in the Evidence-Making Intervention framework, which facilitated quick pivots in a constantly changing opioid landscape in rural Ohio. After implementation, process evaluation data were collected. Details of the methods for each project phase are summarized below. Project phases aligned with the NIDA UG3/UH3 funding mechanism; exploration and adaptation occurred concurrently over a 2-year period (UG3, 2018-2020), while implementation and evaluation occurred over the following 4 years, which included a 1-year extension due to the COVID-19 pandemic (UH3, 2020-2024).
Exploration (Phase 1)
We first used a mixed-methods approach to explore the landscape of the opioid epidemic in southern Ohio, identify barriers to care, and plan for implementation. We collected, analyzed, and triangulated data from a variety of sources, including interviews with key participants and people who use drugs (PWUD), organizational surveys to assess interagency dynamics, and respondent-driven sampling surveys with PWUD.
In-Depth Interviews
We conducted in-depth interviews with PWUD (n = 30) and key participants (n = 34) including health department personnel, health care and substance use treatment providers, law enforcement officers, and judicial officials to assess barriers to service provision and local substance use culture. Methods and results of these interviews have been described in detail elsewhere.17-19
Key participants were individuals providing or supporting health- or drug-related services and were recruited through referral by community-based collaborators. The semi-structured interview guide addressed: (1) perceptions and attitudes toward PWUD, (2) perceptions and attitudes toward medications for opioid use disorder (MOUD), (3) barriers and facilitators to providing services for PWUD. 17 The interviewers used probing questions to understand the underlying elements of the risk environment contributing to participants’ perceptions and attitudes.20-22
People who use drugs, including individuals with a history of illicit opioid use or any injection drug use, were recruited mainly from harm reduction programs or through peer referral. The semi-structured interview guide was collaboratively designed by investigators with qualitative expertise representing each ROI site during a series of meetings organized by the consortium’s data coordinating center. The guide was designed to elicit barriers to substance use treatment and uncover opportunities for intervention. The interview guide addressed substance use experiences, interactions with law enforcement, and health care access.
All in-depth interviews were conducted by 2 graduate student interviewers with training in qualitative methods. All participants provided informed consent. Interviews were audio-recorded, transcribed verbatim, then coded based on a mixed inductive-deductive codebook derived from a priori research questions and emergent themes using thematic analysis. 23 Codebook iteration and analysis were pragmatic, focusing on identifying intervention areas of apparent need to share with stakeholders during Phase 2. Matrices were developed to identify the economic and social context of drug use in the community, efforts in the community to address the opioid epidemic, attitudes toward drug users and harm reduction approaches, and barriers to implementing services for drug users.
Agency Relationships
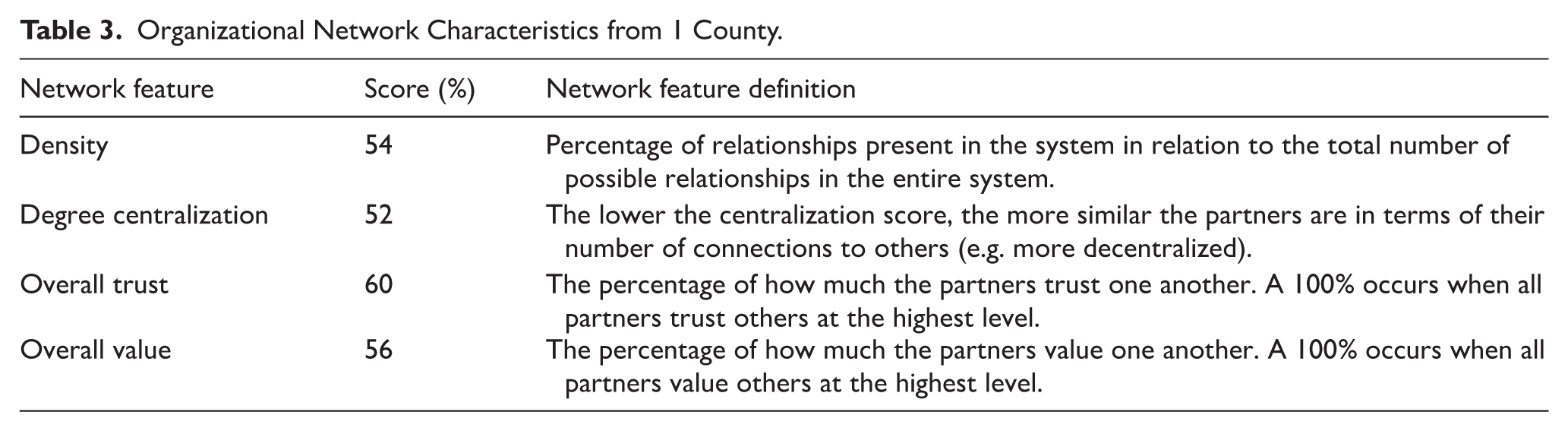
To assess the strength and quality of interagency relationships within each county, we collaborated with Visible Network Labs and used the Program to Analyze, Record, and Track Networks to Enhance Relationships (PARTNER) Tool. This tool uses social network analysis to examine interorganizational characteristics across 4 domains: density, centralization, trust, and value. The PARTNER methodology uses a bounded network survey where each agency receives a complete roster of identified organizations and indicates which ones they collaborate with and how, addressing potential awareness gaps about possible connections. Density reflects the percentage of actual reported connections divided by all mathematically possible connections, centralization measures whether the network depends heavily on 1 or a few highly connected organizations (high centralization) versus having partnerships distributed more evenly across many organizations (low centralization), while trust and value are measured through Likert-scale ratings of relationship quality between organizations. 24 Agencies were identified through consultation with local community leaders and public health officials and included syringe service programs (if present), treatment and rehabilitation centers, pharmacies dispensing naloxone, infectious disease testing centers, and nonprofit organizations. The goal of this survey was to understand whether essential partners are at the table, identify gaps in partnerships, agency perceptions of strengths and benefits, agency connectedness, and interagency value and trust. Data collection and analyses were conducted by the Visible Networks Lab. Visualizations and descriptive statistics were generated for all network characteristics. Brief reports were shared with community leaders in each county.
Surveillance Data Review
Multiple sources of data related to MOUD and naloxone access; overdose deaths; HIV, HCV, and syphilis infection; drug seizures; and neonatal abstinence syndrome births were obtained from public sources or through data use agreements with Ohio governmental agencies. The surveillance data were triangulated and reviewed in simple frequencies, graphical representations, and maps.
Legal Mapping and Policy Surveillance
The Health Policy Institute of Ohio, a non-profit, non-partisan agency based in Columbus, Ohio, conducted the Addiction Evidence Project that assessed 3 domains of state and local policy: prevention, treatment, and recovery; harm reduction; and law enforcement and criminal justice systems. 25 No additional assessment was performed.
Respondent Driven Sampling Survey of PWUD
We conducted surveys with PWUD (n = 258) using a modified respondent-driven sampling approach with initial seeds derived from a local syringe service program. Participants were incentivized to recruit up to 4 peers. Inclusion criteria included: (1) 18 years of age or older, (2) injection of any drug or non-injecting use of opioids to get high in the past 30 days, and (3) residing in 1 of the 3 study counties. Participants were excluded if they were unable or unwilling to provide informed consent. Surveys were completed using computer-assisted self interview (CASI) in REDCap. Surveys were standardized across ROI projects and included demographics and validated psychosocial measures.26-28 Topics included drug use (including networks and injection practices), substance use treatment, healthcare access, criminal justice involvement, harm reduction utilization, stigma, and infectious disease awareness, diagnosis, and treatment (Supplemental Material). Participants were reimbursed $25 for completing the survey and $10 per recruited peer. Participants also received $15 for completing rapid tests for HCV, HIV, and syphilis, and $20 if they underwent confirmatory testing after receiving a positive rapid test. Methods have been described in detail elsewhere. 7 The RDS survey was powered for n = 420 participants, assuming α = .05 and a conservative design effect of 4 to ensure adequate precision of prevalence estimates, and this calculation incorporated surveys planned for a second set of counties not examined here. The present implementation-focused analysis draws only from the tri-county study area and does not report the broader outcome analyses planned for the parent study.
Triangulation of Exploration Data
We conducted iterative data analysis during the data collection process. Repeatedly throughout data collection and analysis, we reviewed our findings and interpretation with local and state key participants. This review provided context for our findings and highlighted existing efforts to address the opioid epidemic.
Adoption/Preparation (Phase 2)
The goal of the Adoption/Preparation phase was to co-develop feasible and acceptable intervention strategies with community stakeholders guided by findings from the Exploration phase. First, we developed an interactive ArcGIS StoryMap (https://arcg.is/1L9b5C) – describing the local overdose crisis, summarizing key findings, and outlining leverage points for intervention – in order to engage partners and garner community support. 29 We next formed a nine-member community leadership board (CLB) with cross-county representation including health commissioners, public health staff, and representatives from treatment, health care, and harm reduction programs. The CLB was charged with collaboratively and iteratively informing our service delivery plan (ie, package of intervention activities). Planning efforts were guided by the principles of Collective Impact (CI), a framework for collaboratively solving community problems. 30 CI emphasizes a common agenda, mutually reinforcing activities, continuous communication, data and measurement, and the backbone support of a separate organization (eg, academic institution) to convene members and organize implementation. 31 The CLB developed mission and vision statements to guide the overall process (Table 1). We facilitated a series of eight CLB meetings between November 2018 and March 2019. In planning meetings, research team members presented triangulated findings and prospective evidence-based interventions, then solicited feedback from members on feasible, acceptable, and priority strategies; recommended partnerships; and barriers and facilitators to implementation (Figure 1). Priority issues and intervention activities were iteratively refined by CLB members with research staff support across successive meetings.
Community Leadership Board Mission and Vision Statements.


Intervention planning process presented to Community Leadership Board.
We explicitly sought to develop plans that would be sustainable for local partners without substantial external support. We compared proposed activities to ongoing activities in the community to minimize duplication. The process enabled us to recognize similarities and differences across the 3 counties. Most importantly, CLB members noted that larger interventions, like starting a mobile syringe service program in any of the counties, were likely infeasible given the local implementation climate, for example, low readiness for change in the community. 10 The CLB gave preference to smaller capacity-building activities that had a greater chance of community buy-in and success and could ultimately create a more favorable implementation climate for larger-scale harm reduction programs in the future. After conclusion of the CLB planning process, we developed a service delivery plan that identified thematic intervention categories, associated activities, community partners, and expected outcomes. This plan aligned with the principles of the Evidence-Making Intervention framework (EMI), which recognizes that implementation is contingent on dynamic local contexts and interventions should be responsive and flexible, rather than static and universal.14,32 Given the fluid implementation climates within and across counties, and constantly shifting local harm reduction ecosystems, the EMI approach allowed the service delivery plan and its activities to adapt to evolving needs, resources, and contexts. The service delivery plan was reviewed and approved by the CLB as a whole and with each county health commissioner individually.
Implementation (Phase 3)
The service delivery plan comprised a series of activities that focused on 3 salient targets for intervention identified in the triangulated formative data and confirmed by CLB members: (1) substance-related stigma, (2) public health interagency fragmentation, and (3) inadequate treatment provider capacity. These barriers, along with the interventions and the rationale for their inclusion, are described in greater detail in the results.
To implement the service delivery plan, we identified a team of intervention experts from the community and from the 2 lead research institutions. With input from the CLB, we identified and hired key harm reduction experts from the 3 counties as part of our intervention team. These experts served as consultants, liaisons, and community champions for all intervention activities, providing insights and critical connections to local communities, including substance use treatment providers, PWUD, law enforcement leaders, judicial officials, and news media (Table 2). In line with the EMI framework, the experts also kept the study team informed on changes in local treatment and harm reduction programing to prevent duplication and facilitate collaboration between the study team and relevant organizations.
Community Member Roles and Responsibilities.

Activities were implemented variously by study team members, consultants, and contractors, in close collaboration with our local partners, as described in the results.
Evaluation (Phase 4)
We conducted a process evaluation of intervention activities focused on reach, defined by proportion who attended or were exposed to the activity, and dose delivered, defined as implementation completeness. Attendance sheets and tracking logs were used to collect data from activity implementers and participants. Descriptive analyses were performed for each activity.
Planned outcome evaluations included changes from baseline in PWUD attitudes, beliefs, and behaviors as reflected in a repeated cross-sectional RDS survey, and comparative shifts in population-level health outcomes (eg, overdose, infectious disease rates) through regression point displacement analysis (RPDD). Intervention activities occurred during the COVID-19 pandemic, complicating inferences related to the impact of the service delivery plan on community outcomes. In particular, internal validity was threatened by secular trends in public health during the early stages of the pandemic, including surges in overdose, disrupted services, and worsening psychosocial health, especially in PWUD.33-35 RDS and RPDD evaluations were not completed. Implementation outcome data are described in further detail below.
Results
Exploration Phase
Detailed results from the exploration phase are being reported elsewhere.7,17-19,36,37 Formative data, specifically from stakeholder interviews, indicated that a combination of social, cultural, economic, and historical factors contributed to the pervasive belief that problematic substance use is a choice, a general mistrust of the medical community and MOUD, and a widespread endorsement of abstinence only, 12-step programs as the only path to full recovery. In contrast, a minority of people, primarily those in the health sector, supported harm reduction approaches including MOUD, emphasizing the complex social, structural, and biological factors contributing to addiction. These contrasting perspectives resulted in tensions within and between law enforcement, judicial, health care, and substance use treatment sectors, contributing to a fragmented response to the overdose crisis in the region. Fragmentation was corroborated by the PARTNER Tool, exemplified in 1 county (Table 3) whose scores indicated missed opportunities for collaboration (ie, density score), low trust between organizations, and low perceived value of other organizations.
Organizational Network Characteristics from 1 County.
The most salient barriers underpinning opioid-related morbidity fell into 3 categories: (1) Stigma: High levels of stigma directed toward PWUD, MOUD, and harm reduction combined with lack of community support; (2) Interagency fragmentation: Lack of awareness, coordination, and collaboration between organizations; and (3) Inadequate provider capacity: Lack of training and resources for providers to address opioid use disorder, overdose, and related morbidities, eg, infectious disease.
Adoption/Preparation Phase
Using an iterative process with the CLB, we developed a relevant, feasible, acceptable, and sustainable service delivery plan (SDP) to address these 3 barriers (Table 4). A more detailed operational matrix indicated target counties, implementation complexity (low, medium, high), proposed partners, implementation steps, and process and outcome measures for each activity (Supplemental Material). With advisement from the CLB, activities were selected that would not be redundant with ongoing or planned programing in the community. In most cases, activities were newly developed (eg, conflict resolution seminars), while in others, activities enhanced existing programs (eg, promoting MOUD in established drug courts). The CLB members helped identify relevant partners for implementation of each activity. In several cases, these partners were hired as part-time consultants given their local credibility and time contributed to the project. For instance, a community faith leader provided ad hoc consulting to help the research team identify religious organizations, develop training materials, and deliver training content to congregations. Two harm reductionists from 2 local health departments were also hired as part-time research staff to aid with relationship building, intervention implementation, and ensuring proposed activities were complementary to ongoing efforts. As a capacity-building intervention, all activities were executed with grant funding and intended to be sustained with minimal investment by the community post-intervention.
First Iteration of Service Delivery Plan.
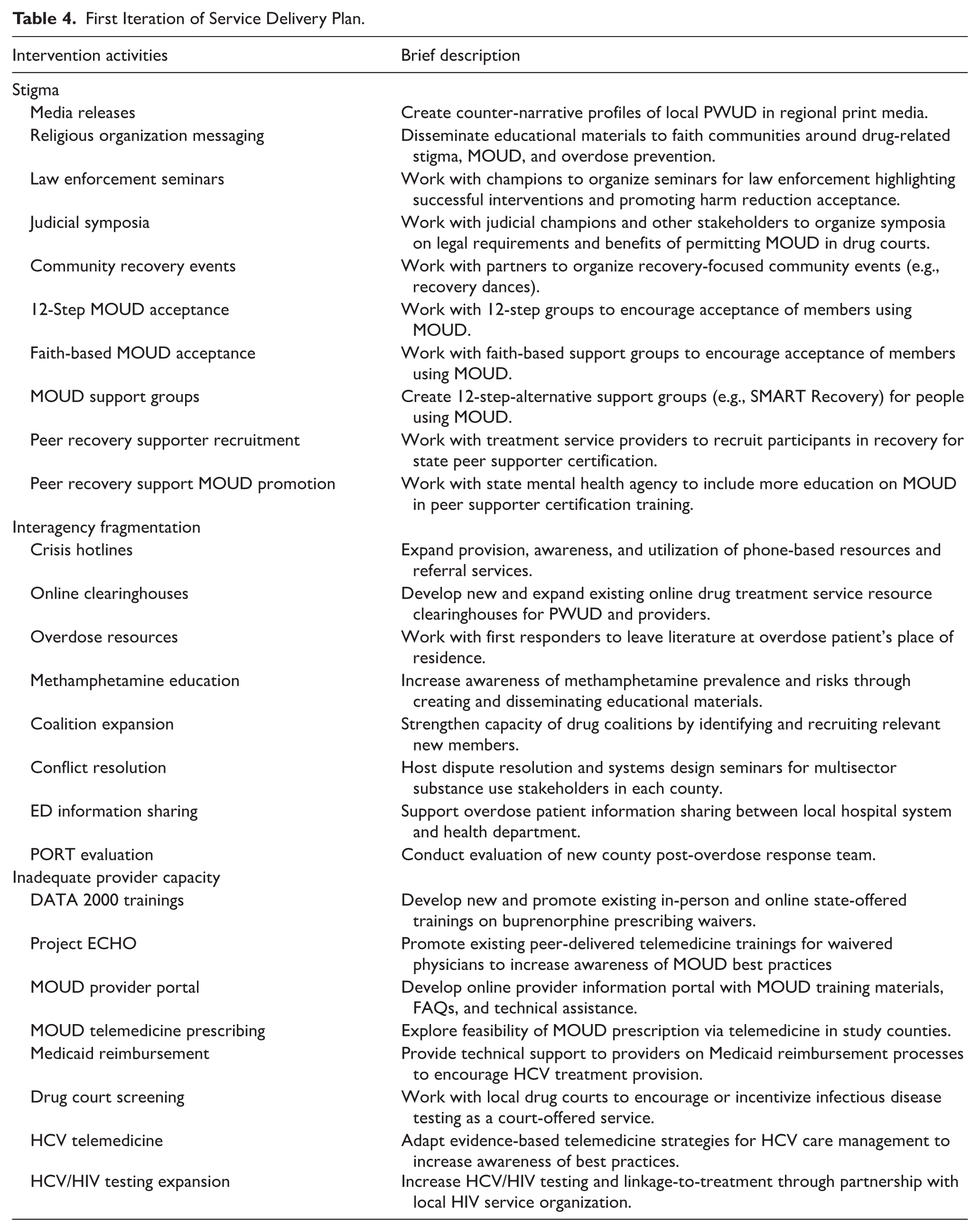
Stigma
Stigma-related interventions focused on community education, acceptance, and support around addiction and harm reduction approaches including MOUD. Some activities aimed to address misconceptions about substance use in the broader community, including positive profiles of PWUD disseminated through local newspapers (Table 4, “media releases”). Others targeted stakeholder groups with potentially stigmatizing behaviors (law enforcement seminars) or untapped capacity to disseminate education and resources (“faith-based MOUD acceptance”). Such activities invited gatekeepers (eg, regional law enforcement and religious leaders) to deliver programing and were tailored to address CLB-identified opportunities and barriers (eg, compassion fatigue and burnout among police officers). Finally, activities aimed to increase limited local capacity for and quality of peer support, an evidence-based resource for reducing internalized stigma. 38
To ensure sustainability, our proposed stigma interventions built on existing resources when possible. For example, for the activity “Peer Recovery Supporter Recruitment,” we proposed to raise awareness among the recovery community and facilitate an existing state-sponsored training and certification. Ohio’s mental health and addiction services board had limited success recruiting for and convening trainings in southern Ohio. Such an intervention would be low complexity, require few resources, and potentially benefit both peer supporters and PWUD: Peers would receive an employable credential and the opportunity to build self-esteem and reinforce their own recovery, while PWUD would have greater access to peer support in harm reduction, treatment, and recovery services. 39
Interagency Fragmentation
Interagency fragmentation interventions aimed to facilitate cooperation in the epidemic response by raising service awareness, increasing coordination of efforts, and ultimately encouraging collaboration between organizations. Proposed activities included increasing resource awareness for stakeholders and community members through an online, GIS-enabled resource hub (“online clearinghouses,” Table 4) and dissemination of physical educational materials to organizations and individuals (“overdose resources,” “methamphetamine education”); facilitating cross-sector collaboration through a series of conflict resolution forums hosted by systems design experts from the Divided Community Project 40 (“conflict resolution”); and encouraging data sharing between hospitals and public health agencies (“ED information sharing”). Certain activities were response to CLB-initiated requests, like a formal evaluation of a proposed post-overdose response team (“PORT evaluation”) which itself was a new interagency collaboration.
Inadequate Provider Capacity
Provider capacity in the tri-county area was deemed inadequate, with CLB members citing limited screening and linkage-to-care services and a shortage of substance use and infectious disease treatment providers. To build MOUD capacity, we aimed to increase the proportion of eligible providers prescribing MOUD through promoting and facilitating existing DATA 2000 (“X-waiver”) trainings, coordinating with a regional medical university to recruit for a continuing education webinar for MOUD providers (“Project Echo,” Table 4), and producing a report on the feasibility of tele-prescribing MOUD based on demonstration programs in other parts of the country. 41 In the realm of infectious disease, proposed capacity-building activities included introducing infectious disease screening into drug court protocols (“Drug court screening,” Table 4), expanding HCV and HIV screening and linkage services in partnership with a regional non-profit healthcare agency (“HCV testing expansion,” “HIV testing expansion”), and developing HCV telemedicine infrastructure through The Ohio State University’s infectious disease clinic (“HCV telemedicine”). 42
Implementation & Evaluation Phases
The final service delivery plan, ultimately comprised of 18 sets of activities, included trainings, seminars, technical support, acquisition of materials and resources, and partnership development activities (Table 5). Overall, given the scope and range of the proposed service delivery plan, the final suite of activities was well-received.
Completed Intervention Activities and Key Process Measures.

Data provided by treatment provider Central Outreach for 2022Q1 to 2023Q2 for residents of study counties. Numbers not disaggregated by substance use status.
Intervention as Emergent and Contingent: SDP Adaptation
Although many activities were conducted with fidelity to the service delivery plan (eg, media releases, law enforcement seminars, drug court screening), the package of activities evolved during implementation, keeping with the EMI principle that community-situated interventions should be fluid and emergent. 14 We note 4 kinds of adaptations (Table 6): omitted activities (those attempted but left incomplete due to feasibility issues), redundant activities (those rendered superfluous during the course of implementation), modified activities (those changed to address a related outcome in light of emerging needs and opportunities), and added activities (those not appearing in the original SDP but added in light of emerging needs and opportunities).
Intervention Adaptations.

Removed: Implementation was attempted but unsuccessful. Redundant: Implementation was deemed unnecessary due to secular trends. Modified: Activity was changed but reflected similar outcomes. Added: Activity did not appear in original service delivery plan.
Most adaptations were a direct outcome of the COVID-19 pandemic and the shifting drug policy landscape. Most notably, the elimination of the Drug Enforcement Agency’s “X-waiver” in June 2023 (formerly a requirement for prescribing buprenorphine) 43 allowed our team to deprioritize DATA2000 trainings for healthcare providers. Other activities were modified for similar reasons. For instance, given increased flexibility for telehealth during the pandemic, we worked with regional partners to expand HCV tele-prescribing rather than burdening the under-resourced local infectious disease treatment system. 44 COVID-19, counterintuitively, also made educational activities easier to implement insofar as the communities became more adept and familiar with video conferencing options like Zoom, allowing our team to develop and deliver additional activities (eg, stigma reduction seminars) that would have been burdensome to attend in-person, given the geographic spread across these rural counties.
In other cases, SDP adaptations arose from our team’s growing recognition as a quasi-backbone organization 30 in the region (ie, substance use stakeholders from outside the region occasionally approached our team to broker partnerships within the communities). This included partnering with a start-up non-profit to introduce overdose text alerts in the study counties (in lieu of the planned crisis hotline activity) and securing $350 000 in unallocated passthrough funding through the federal CARES Act for 2 local addiction services boards.
Finally, a few activities were omitted from the SDP due to unforeseen feasibility barriers. For instance, although the CLB requested greater promotion of MOUD in 12-step circles, neither our team nor the CLB had existing partnerships, nor could we establish buy-in with these groups to implement this activity.
Several activities were sustained by community partners, including the Scioto Connect resource clearinghouse, which has since become the brand identity for the regional opioid prevention consortium. New partnerships forged with state and regional organizations, including telehealth clinics and harm reduction suppliers, further enhanced local capacity for overdose and infectious disease prevention into the near future. Many other activities remain integrated into organizational policy and practice, including MOUD training for peer supporters and infectious disease screening in drug courts.
Discussion
In this paper, we present an applied implementation research project aimed at enhancing regional capacity for overdose response in rural Appalachian Ohio. Our formative research revealed that pervasive public stigma, fragmented service delivery systems, and rural infrastructural limitations undermined the likely feasibility and acceptability of traditional harm reduction trials in these communities. Instead of imposing externally developed interventions, we adopted a community-guided capacity-building approach that addressed foundational barriers while respecting local readiness for change.
Community capacity is a critical, though often neglected, foundation for public health innovation that can be strengthened through formative research and deliberate implementation science activities.45,46 While many implementation science efforts focus on building organizational capacity to deliver specific EBIs, our approach emphasized working across a community ecosystem to facilitate collective readiness for innovation. In this project, stakeholders shared broader community barriers that precluded the feasibility of multiple interventions, requesting instead support toward building a local culture amenable to and prepared for future harm reduction interventions. Below, we share lessons learned from our approach that may be of value to implementation researchers aiming to strengthen community foundations for sustained intervention success.
Transferrable Lessons for Applied Implementation Research Studies
Problematizing Fidelity: Meeting Emergent Need Through Adaptive Implementation
Implementation followed an Evidence-Making Intervention approach, which emphasizes pragmatism and adaptability in rapidly evolving public health contexts.14,32,47 We developed a service delivery plan that was not static, continuously soliciting community input to understand changes in the substance use landscape and pivot to reduce duplication of efforts or fill in new gaps. This approach proved crucial during the overlapping COVID-19 pandemic, which interrupted essential services for PWUD and rendered many planned activities infeasible due to social distancing guidelines, reallocated public health resources, and emerging issues and priorities.
Flexibility runs counter to traditional notions of implementation fidelity, which calls for faithful adherence to protocol, that is, implementation strategies should be delivered as intended. 48 In our EMI approach, process and outcomes were iterative and contingent on a dynamic implementation context during a global health emergency. In emergent situations, as barriers shift, adhering to an original plan may be ineffective when the original implementation strategy may no longer relevant. Our approach prioritized the questions that needed answering (ie, the 3 community-identified barriers) rather than the answers themselves. In this way, fidelity meant less so adherence to processes than faithfulness to process.
One key adaptation was shifting away from providing technical assistance for local HCV treatment capacity toward facilitating partnerships with a regional healthcare organization with tele-prescribing capabilities, which allowed us to leverage external support in light of minimal local resources. Rather than compromising fidelity to the implementation strategy, this shift represented a pragmatic adaptation in the delivery approach itself – adjusting the plan to local context while maintaining alignment with the core goals of the initiative. Elsewhere, planned activities were abandoned (eg, MOUD waiver trainings) and unplanned activities were created (eg, online stigma reduction seminars) that acknowledged secular trends (eg, MOUD policy changes) and capitalized on emerging opportunities (eg, widespread adoption of teleconferencing technology). From the EMI standpoint, when community interventions are entangled amongst each other – as they often are – their effects are not isolatable from each other or from their environments.14,47 Acknowledging that our interventions were part of an assemblage, rather than isolated activities, allowed us to refocus our efforts from finding “what works” 47 within the service delivery plan to iteratively reimagining the plan as a cohesive and fluid evidence-making experiment.
Democratizing Community Research Involvement
Local and regional partners were instrumental in establishing community buy-in, forging partnerships, implementing culturally relevant interventions, and advising on shifts in the local treatment and harm reduction ecosystems. Recognizing that sustainability depends upon the continued efforts of multiple actors after research ends, community engagement was a multi-stage endeavor aimed at giving residents control over the processes and products of the intervention. 49 Community members inhabited 4 roles: Community leadership board representatives, data collectors, implementation team members, and ad-hoc consultants (Table 2). Our implementation team included 2 health department staff members and several ad-hoc consultants with local credibility (eg, pastors, sheriffs) to lead trainings and other activities. Champions have long been recognized as levers for promoting innovation in health systems by enhancing researcher credibility and fostering organizational support.50,51 This approach may be especially important in rural areas where networks are compact and trust is needed to gain access.52-54 Data collectors were also lifelong residents of the region, which fostered credibility with research participants and facilitated peer survey referral. 55
A benefit of extensive community involvement is that public health capacity can be built not only through intervention but through the community engagement process itself. Implementation staff were part-time health department employees whose salaries were topped off to an effective full-time rate, an ancillary benefit for rural agencies that are often under-resourced and experience high turnover rates. 56 The timing of their hiring was critical, as health departments nationwide turned their attention to the COVID-19 pandemic, often deprioritizing substance use and harm reduction services. 34 Implementation staff also gained exposure to academic research, harm reduction practitioner networks, and training in implementation science. Our community involvement efforts further positioned our team as a quasi-backbone organization, which attracted the attention of state agencies with weak ties to our catchment area and improved state-local partnerships for funding and training opportunities. These outcomes were unplanned and exemplified the benefits of an adaptive, emergent approach to capacity-building.
Rethinking Needs Assessment: An Argument for Asset-Based Approaches
Public health science is historically built on identifying needs or deficits in populations – where communities fall short – in order to allocate resources toward appropriate interventions. Asset-based community development (ABCD) recognizes the inherent strengths and opportunities in communities. 57 Formative research should focus not only on documenting community risk profiles and resource shortages but also on capturing and enhancing what already works. Several intervention activities capitalized on existing resources, including a clearinghouse of local harm reduction and treatment services that unexpectedly spawned an overdose stakeholder consortium, providing new avenues for coordination and collaboration. In contrast to a needs-based mindset, thinking with assets can help uncover opportunities that already exist in communities.58,59 Our team facilitated an unrealized partnership with a regional HCV treatment provider, made possible through awareness of existing PWUD-serving organizations able to screen and refer clients. This activity required few implementation resources but resulted in sustained programmatic improvements. Of course, the researcher team’s role as a quasi-backbone organization is a temporary solution to identifying and connecting community assets. However, social network approaches, like the PARTNER tool, could be used to identify partnership opportunities in an ABCD framework. 60 For example, “bridge” organizations could be targeted for linking disparate networks in a community, 61 while organizations with high centrality can serve as “hubs” of knowledge exchange and collaboration. 62 Regional mental health and addiction service boards – like the ones who received passthrough federal funding during our intervention – are candidates for such roles, given their ties to multiple PWUD-serving organizations in their respective communities.
Limitations and Future Directions
This paper does not present a formal outcome analysis; however, examining these implementation processes is essential for understanding how capacity-building unfolds in low-resource rural environments. High-level case studies such as this one illuminate the contextual, relational, and structural dynamics that shape feasibility and sustainability – factors often obscured in outcome-focused research. Documenting these processes offers critical insights for scholars and practitioners designing community-engaged interventions in similarly complex settings.
Our approach faced certain challenges that should be considered in future adaptive capacity-building interventions. Some activities were altered or developed after implementation had begun, requiring flexibility in the evaluation protocol as well. However, developing new process measures (eg, acceptability post-surveys for seminars) is time-intensive and often requires ongoing approvals from research ethics committees, which can delay implementation. Researchers considering an adaptive approach will need to find a balance between meeting emerging opportunities for intervention and collecting comprehensive evaluation data. In keeping with the EMI philosophy of valuing multiple ways of knowing, 14 one option is to emphasize qualitative evaluation and develop interview guide templates to capture community perspectives across a diversity of intervention activities. While our implementation team helped connect fragmented systems and catalyze change, the sustainability of these connections beyond the research lifecycle remains uncertain. Future work should prioritize embedding leadership, coordination, and evaluation into existing community organizations to ensure long-term continuity. Asset-mapping and network analysis tools, discussed above, could help communities identify pathways for responsibility setting.
A major limitation of our research is that the COVID-19 pandemic obfuscated the impact of our interventions and disrupted our ecological evaluation design; though our process measures suggest some positive results, the actual health and social impacts on people who use drugs is undetermined. Finally, our project overlapped with the HEALing Communities Study (HCS), a large-scale substance use prevention and treatment implementation study across 4 states which included one of our study counties and initiated during OHOP’s implementation phase. 63 It is likely that HCS researchers partnered with many of the same stakeholders and implemented similar activities. While this overlap is a positive testament to investment in rural overdose research, it also points to the threat of redundancy and research burden on small communities. Our field staff maintained contact with HCS field staff during the study; nonetheless, the lack of effective coordination between our projects is a reminder that researchers risk reinscribing fragmentation within the very systems they aim to strengthen when multilevel implementation efforts unfold without shared governance structures.
Conclusions
This study demonstrates how applied implementation science can support communities in building the foundations needed to engage with and sustain harm reduction innovation. Rather than imposing predefined interventions, we developed a collaborative, adaptive, and iterative approach that acknowledged the material realities and readiness for change of the community. This work underscores the importance of community capacity-building not just as a means to support specific interventions, but as a strategy in its own right for addressing the structural roots of the overdose epidemic.
Supplemental Material
sj-docx-2-sat-10.1177_29768357251413412 – Supplemental material for Building Community Capacity for Harm Reduction: An Adaptive Implementation Science Approach in Rural Appalachian Ohio
Supplemental material, sj-docx-2-sat-10.1177_29768357251413412 for Building Community Capacity for Harm Reduction: An Adaptive Implementation Science Approach in Rural Appalachian Ohio by Adams L. Sibley, Christine A. Schalkoff, David C. Colston, Hannah M. Piscalko, Abby G. Spears, William C. Miller and Vivian F. Go in Substance Use: Research and Treatment
Supplemental Material
sj-xlsx-1-sat-10.1177_29768357251413412 – Supplemental material for Building Community Capacity for Harm Reduction: An Adaptive Implementation Science Approach in Rural Appalachian Ohio
Supplemental material, sj-xlsx-1-sat-10.1177_29768357251413412 for Building Community Capacity for Harm Reduction: An Adaptive Implementation Science Approach in Rural Appalachian Ohio by Adams L. Sibley, Christine A. Schalkoff, David C. Colston, Hannah M. Piscalko, Abby G. Spears, William C. Miller and Vivian F. Go in Substance Use: Research and Treatment
Footnotes
Acknowledgements
We wish to thank all research participants, Community Leadership Board members, and consultants for their invaluable contributions to this study. We are particularly grateful to those with living experience of substance use for their vulnerability and bravery in research participation. This study would not be possible without the efforts and expertise of our local collaborators and consultants, and in particular, Abby Spears, Cathy Neal, Renee McDowell, Staci Mercer, and Anyssa Wright.
Ethical Considerations
The study received ethical approval from The Ohio State University IRB (#2017B0328) and the relying institution, University of North Carolina-Chapel Hill IRB (#17-1887).
Consent to Participate
All participants in formative research procedures (surveys, interviews) provided written informed consent.
Consent for Publication
Not applicable.
Author Contributions
ALS: Conceptualization, methodology, formal analysis, investigation, supervision, project administration, writing – original draft; CAS: Conceptualization, investigation, project administration, writing – review and editing; DCC: Investigation, writing – review and editing; HMP: Investigation, writing – review and editing; AGS: Conceptualization, project administration, writing – reviewing and editing; WCC: Conceptualization, methodology, supervision, funding acquisition; VFG: Conceptualization, methodology, supervision, funding acquisition, writing – review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Drug Abuse (UG3/UH3 DA044822). No funders were involved in the preparation of this manuscript or the decision to submit for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Formative research data and intervention materials are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.