
Abstract
Objective:
Pain is a significant clinical challenge among patients with opioid use disorder (OUD), and management strategies remain diverse and controversial. This scoping review aimed to describe and evaluate the different types of pharmacologic pain management strategies for patients who are prescribed extended-release buprenorphine (BUP-XR) for OUD and experiencing pain.
Methods:
The databases Ovid Medline, EMBASE, CINAHL, Web of Science, and PsycInfo were searched from their inception to February 2025 for relevant articles. All articles that discuss the treatment of acute or chronic pain among patients receiving BUP-XR were included. Data on the key outcomes of pain severity, related functioning, patient satisfaction, and adverse events were extracted and study quality was rated independently by the authors.
Results:
The initial search yielded 980 articles. Of those, 56 were assessed for full-text review and a total of 6 articles met inclusion criteria for the study. The overall strength of the evidence was poor, consisting mainly of case series and case reports. Most studies achieved adequate pain control through the continuation of BUP-XR and the combination of full opioid agonists and non-opioid adjuncts, adjunct use of nonsteroidal anti-inflammatory drugs, conversion to sublingual buprenorphine, or performing surgery at trough serum buprenorphine concentration. No cases of respiratory depression or toxicity were observed.
Conclusions:
This review confirmed that clear guidelines on how to support pain management in BUP-XR treatment have yet to be identified. The majority of clinicians favored a multimodal analgesic approach combining opioids, non-opioid analgesics, and regional anesthesia. Further studies, including high-quality evidence through randomized controlled trials, are needed to find and evaluate optimal adjunctive medications and define overall strategies.
Introduction
Opioid use disorder (OUD) and opioid-related overdose rates remain at epidemic levels across the globe. Despite the known efficacy of available opioid agonist medications, 1 numerous barriers impede the access, utilization, and retention to care among those with OUD, including the frequent requirement for daily dosing. 2 To mitigate these concerns, long-acting depot buprenorphine formulations have recently been introduced to the range of treatments. Extended- or prolonged-release buprenorphine (hereby referred to as BUP-XR) consists of a subcutaneous depot used for the treatment of moderate to severe OUD. In North America, a once-monthly subcutaneous polymer-based injection formulation (Sublocade®) was first approved by the United States’ Food and Drug Administration in late 2017, shortly followed by Health Canada in late 2018. In Europe and Australia, a once-weekly and once-monthly subcutaneous lipid-based injection formulation (Buvidal®) was approved in 2018. In efficacy studies, BUP-XR at a 300 mg dose was shown to produce a blockade of opioid subjective effects and reinforcing efficacy of intramuscular hydromorphone for the 4 weeks after the first dose. 3 Compared to placebo, BUP-XR has also demonstrated significantly improved abstinence from non-prescribed opioids, with mean abstinence rates of 41.3% and 42.7% in 2 dosing groups versus 5.0% in the placebo group over 24 weeks (P < .0001). 4 In another randomized controlled trial comparing depot and sublingual buprenorphine, the depot group reported higher treatment satisfaction, greater convenience, and lower treatment burden. 5 Since its introduction as an alternative treatment option to methadone and sublingual or buccal buprenorphine-naloxone, both patient interest and uptake related to BUP-XR have been increasing,6,7 alongside the application of various forms of buprenorphine for treatment of acute and chronic pain.8 -11 One population-based study demonstrated a moderate uptake rate of BUP-XR across Canada, with more than 6500 people treated since its approval in early 2020. 12 Despite these benefits and overall tolerability, BUP-XR is also associated with mild to moderate adverse events related to the injection, consisting of local pain, itching, or erythema. 13 A 12-week-long multicenter trial among 527 patients had 13.2% of participants report injection-site pain, with mean pain scores of 44 out of 100 within the first hour of injection. 14 Further limitations of BUP-XR have also been revealed through qualitative studies with individuals who use opioids, including fears about potential coercive treatment and the incompatibility of long-acting formulations for those who still wish to use opioids recreationally. 15 Moreover, access to BUP-XR as well as other OAT options remain impeded due to ongoing systemic and psychosocial barriers, such as high medication costs, 16 lack of training for providers who will perform the injection, as well as ongoing stigma toward patients and prescribers. 17
Pain is a frequent and disabling condition in individuals with OUD. In 1 sample of patients in primary care, 80% were found to have a pain disorder. 18 Similar prevalence rates for pain were found in another sample of those who use fentanyl, with nearly 3-quarters (73%) of its participants to report ongoing pain in the past 6 months. 19 Moreover, pain intensity is more frequently moderate to severe in patients receiving opioid agonist therapy (OAT), occurring in 23% to 44% of individuals with OUD compared to the 12% to 29% reported in the general population.20,21 Despite pain affecting a substantial portion of this population, pain management strategies for OAT patients continue to be a subject of debate. The urgency of patients’ needs, the demonstrated effectiveness of opioid analgesics for the management of acute pain, and the limited therapeutic alternatives for chronic pain have combined to produce an overreliance on opioid medications. 22 The long-term use of opioids, either prescribed or non-prescribed, is associated with addiction, overdose, and diversion, and can often lead to higher tolerance and increased pain sensitivity in patients from opioid-induced complications such as allodynia and hyperalgesia. Together, these factors can create barriers or challenges to achieving adequate analgesia with opioid therapy. 23 This may further be exacerbated in OUD patients, who more often than not have co-occurring conditions that also result in both acute and chronic pain.24,25 Increasing evidence shows that undertreated pain is a common barrier to OUD treatment, hindering all of entry, retention, and relapse prevention.26,27 Additional challenges also exist from the perspective of health care providers. Physicians are naturally concerned about inadvertently promoting opioid misuse, addiction, and public health risks or the potential to face legal repercussions for overprescribing narcotics, particularly for chronic pain where the benefits are more questionable. 28 Moreover, given the propensity of opioids to cause respiratory depression, the potential for adverse events when prescribing additional opioids in the context of OAT remains an important safety concern. Among available opioids, buprenorphine as a partial agonist confers greater safety over full agonists like methadone by exhibiting a dose-ceiling effect on respiratory depression, but not on analgesia. 29 Further clarity and precision regarding the analgesic effects of buprenorphine is vital given its implication for pain management.
To date, few studies have systematically examined pain management strategies among individuals with opioid use disorder, and publication have focused mostly on methadone or sublingual buprenorphine30,31 and specific to surgical, 32 critical, 33 or perioperative care 34 settings. Recent formulations such as BUP-XR have yet to be studied in relation to how it may positively impact, but also complicate, acute and chronic pain management for OUD patients. Maintenance opioids prescribed for addiction treatment are typically understood as being unable to provide adequate pain control on their own. 31 In particular, the core issue of pain control with buprenorphine comes from its partial opioid agonism and high receptor binding affinity that limit additional opioid doses to little or reduced efficacy. 35 Previous work has associated buprenorphine with the dose-dependent attenuation of morphine and other full agonists, and in some cases, nullifying their analgesic effects while increasing the potential for toxicity.36,37 However, recent literature has found support for the use of buprenorphine in managing both acute 38 and chronic pain. 39 Specific buprenorphine formulations indicated solely for chronic pain were also observed with efficacy in reducing pain in various populations.40,41 Given the relative novelty of the BUP-XR and limited evidence in this setting, there is a strong need to explore the potential for the long-acting formulation’s analgesic potential. This scoping review aims to determine and evaluate the effectiveness of the different types of pain management strategies that exist for patients taking BUP-XR.
Methods
Search Strategy
The present review was carried out completing the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines that were extended for scoping reviews (PRISMA-ScR). 42 Electronic searches were conducted in the databases Ovid Medline, EMBASE, CINAHL, Web of Science, and PsycInfo from August 2024 to February 2025. The following search terms and related queries were used, with Medical Subject Headings (MeSH) terms when possible (in Ovid Medline, EMBASE, CINAHL, and PsycInfo): “pain management,” “extended-release buprenorphine” and “opioid use disorder.” Forward and backward reference searching were also performed to avoid missing relevant papers meeting the inclusion and exclusion criteria.
Inclusion and Exclusion Criteria
All articles that discussed the treatment of acute or chronic pain among patients receiving BUP-XR were included. Despite their being separate entities, acute and chronic pain were collectively grouped as pain in order to obtain all papers related to pain management in the search and identify potential differences. Studies that reported methadone or other buprenorphine formulations were excluded as they require different treatment goals and trajectories. All study types that reported primary data in English were included. With the ongoing discussion about the importance of including conference abstracts in reviews, 43 conference abstracts that met the same inclusion and exclusion criteria as articles were also included. Further, the references of any reviews addressing pain management in patients on buprenorphine therapy were hand-searched by reviewers to find any original articles not otherwise identified. No animal or in vivo studies were included. The full search details for Medline are included in Appendix 1 (Table A1).
Screening
Two independent reviewers screened each title and abstract against the predefined inclusion and exclusion criteria using the Covidence software. 44 Disagreement between authors was resolved with discussion. The methodological quality of the included studies was assessed using the JBI Critical Appraisal Checklist for case reports (Table A2).
Data Extraction
Data were extracted independently by the authors using a data extraction form designed for this study, including patient demographics; clinical history; pain severity; pain-related functional outcomes; patient satisfaction; and adverse events. Extracted data from the final pool of articles were analyzed and summarized qualitatively to assess strengths of evidence as well as how pain was managed, measured, and reported in individuals prescribed BUP-XR. No statistical analyses of results were possible with the large number of case reports and heterogeneity in the data reported, only allowing for a descriptive summary. Data extraction revealed clinical heterogeneity from differences in participant characteristics (eg, sex, age, OUD severity, ethnicity, comorbidities) as well as intervention characteristics (eg, dose and frequency of dose).
Data Synthesis
A thematic synthesis approach was used to analyze and synthesize qualitative data, with the overall aim to provide practical implications to inform healthcare professionals. Thematic synthesis was conducted collaboratively, with data coded independently by 2 separate reviewers and compared between each other through iterative processes of developing themes in pain management.
Results
Our search yielded 980 articles after removal of duplicates. 893 articles were excluded during the title and abstract screening, and of the remaining 56 articles assessed for eligibility, only 6 met the inclusion criteria for the study (Figure 1). Back-searching of the retrieved articles did not yield any additional studies, resulting in a total of 6 articles after abstract and full-text screening.

The flow diagram of study inclusion and exclusion.
Table 1 provides an overview of these articles, including characteristics, patients examined, pain management strategies, results, and any follow-ups. The overall quality of evidence was poor, with 4 case reports, 1 letter to the editor, and 1 conference abstract, with the latter 2 each describing a single case.
Characteristics of the included studies.
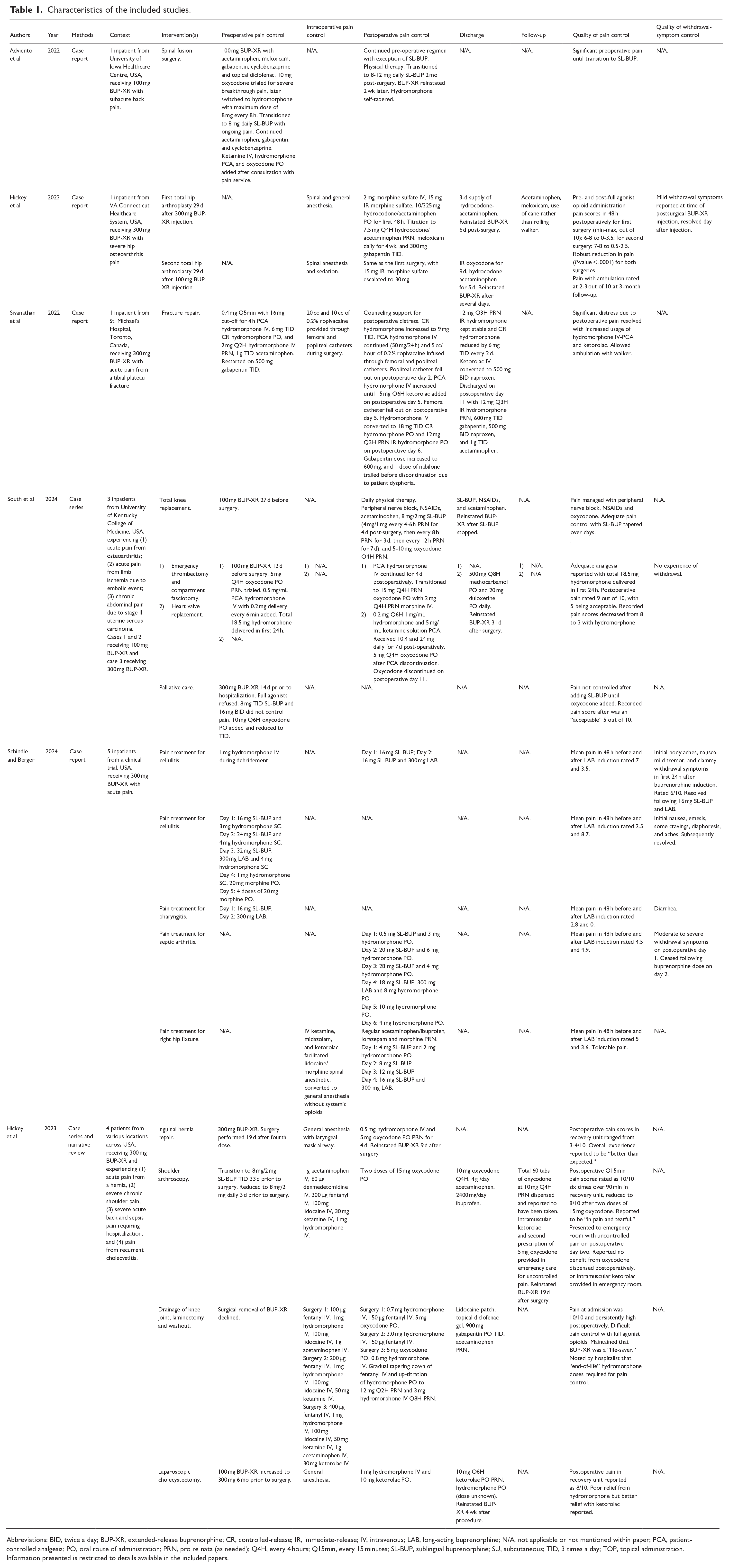
Abbreviations: BID, twice a day; BUP-XR, extended-release buprenorphine; CR, controlled-release; IR, immediate-release; IV, intravenous; LAB, long-acting buprenorphine; N/A, not applicable or not mentioned within paper; PCA, patient-controlled analgesia; PO, oral route of administration; PRN, pro re nata (as needed); Q4H, every 4 hours; Q15min, every 15 minutes; SL-BUP, sublingual buprenorphine; SU, subcutaneous; TID, 3 times a day; TOP, topical administration.
Information presented is restricted to details available in the included papers.
All articles were conducted with monthly formulations in either the United States or Canada. All addressed acute postsurgical pain,34,45 -49 acute emergent surgery pain 48 or chronic pain34,48 in a total of 15 distinct patient cases with ages ranging between 24 and 74 years. All participants received either 100 or 300 mg monthly doses of BUP-XR between the years 2021 to 2024, with the number of received injections ranging from 1 to 24.
Interventional Strategies
Treatments typically included a multimodal approach with the continuation of BUP-XR.
Combined use of full opioid agonists and non-opioid adjuncts: Ten cases used both full opioid agonists and non-opioid adjuncts for pain management (Table 1). Full agonist opioids used included oxycodone, hydrocodone, hydromorphone, and morphine. Oral acetaminophen was commonly prescribed as an adjunct to hydrocodone 46 or hydromorphone.45,48,49 In one case where full agonist opioids were initially refused, sublingual buprenorphine (8 mg given 3 times or 16 mg given twice daily) failed to adequately control pain until oral oxycodone was added. 48 Most cases saw a reduction in pain scores before and after opioid administration, particularly with oxycodone or hydromorphone patient-controlled analgesia (PCA).46 -48 High doses of hydromorphone were required in the setting of opioid tolerance, in one case increasing to a peak of 24-hour hydromorphone-oral-equivalent of 243 mg/24 hours, 47 and in another, to a peak of 108 mg oral hydromorphone and 3 to 6 mg intravenous hydromorphone as a typical 24-hour requirement. 34 Despite their high opioid doses, no abnormal values for vitals were recorded or mentioned.
Use of nonsteroidal anti-inflammatory drugs: Nonsteroidal anti-inflammatory drugs (NSAIDs) used included meloxicam, ibuprofen, ketorolac, and diclofenac. Other non-opioid adjuncts used included ropivacaine, cyclobenzaprine, gabapentin, duloxetine, and regional anesthesia with peripheral nerve blocks provided as needed. One study described using nabilone; however, this was promptly discontinued due to the patient experiencing dysphoria. 47 Intraoperative analgesics including acetaminophen, dexmedetomidine, fentanyl, lidocaine, ketamine, and hydromorphone were used for surgical procedures. Post-surgery, intravenous PCA with either hydrocodone, morphine, or hydromorphone was initiated for cases with breakthrough pain.47,48 When pain coverage was inadequate with either oxycodone or hydromorphone, 1 patient was transitioned from 100 mg BUP-XR to 8 mg daily sublingual buprenorphine with ongoing hydromorphone and non-opioid adjuncts. Sublingual buprenorphine was later discontinued due to inconsistent dosing and BUP-XR reinitiated 2 months after surgery. 49 Physical therapy was prescribed as an adjunct for 2 cases related to mobility.48,49 Only 1 study provided counseling support on top of medications in relation to uncontrolled pain. 47
Interventions related to surgeries: Timing of surgeries varied from 3 to 33 days after the last injection. One patient awaiting surgery was converted to sublingual buprenorphine due to concerns of poorly controlled postoperative pain. 34 Surgical removal of the depot was discussed with 1 patient requiring multiple surgeries, but was eventually declined. 34 Another strategy included performing surgery at trough serum buprenorphine concentration, when the next regularly scheduled maintenance dose would have occurred, as opposed to administering BUP-XR immediately before surgery or delaying surgery until sufficient time has passed since the last dose. Breakthrough pain in the postoperative periods was managed with full agonist opioids, mostly consisting of hydromorphone or morphine sulfate in intravenous or oral immediate release formulations. 46
Outcome Measurements
Twelve cases reported the effects of their interventions on pain intensity through quantitative measurements taken before and after.45 -48 All used a linear numeric scale with 10 representing maximal pain to measure the severity of pain in patients. Other cases included verbal confirmations from patients about their satisfaction with pain control (“better than expected”). 34 One study reported that their intervention resulted in a statistically significant reduction in pain scores and included follow-up pain measures at 3 months. 46 No other study included follow-up measures for pain or OUD-related outcomes after discharge.
Discharge and Follow-Up
Pain management strategies after discharge were varied. Two cases prescribed sublingual buprenorphine, which were either gradually tapered off or sustained until death in hospice care. 48 Two cases only prescribed short-term opioid analgesics including oxycodone, hydromorphone, or hydrocodone with acetaminophen, while another case after valve replacement surgery only prescribed methocarbamol and duloxetine. 48 Five cases used multimodal pain regimens incorporating opioids as needed, acetaminophen, NSAIDs, and other non-opioid adjuncts. Prescribed NSAIDs included ketorolac, meloxicam, naproxen, ibuprofen, and topical diclofenac, while non-opioid adjuncts included gabapentin, cyclobenzaprine, lidocaine, and duloxetine.34,47 -49 Majority did not report on pain levels after discharge. One postsurgical case discharged with oxycodone, acetaminophen, and ibuprofen returned to the emergency room on the second day with uncontrolled pain, requiring a total of 60 tabs of 10 mg oxycodone dispensed. 34 The patient was provided with intramuscular ketorolac but reported no benefit. 34 No other cases mentioned uncontrolled pain after discharge. Only 1 case mentioned follow-up at 3 months, where reported pain levels of 2 to 3 out of 10 was managed with acetaminophen, meloxicam, and a cane for ambulation. 34 Papers generally did not report on non-prescribed opioid use after discharge, with only 1 case explicitly denying any use. 34
Thirteen cases reported the reinitiating or administering of the next scheduled dose of BUP-XR, ranging between 24 and 74 days after surgeries.34,47 -49 Mild opioid withdrawal was observed in 1 patient whose maintenance dose occurred 72 days after their first 300 mg dose, 46 which were resolved the day after the injection. Only 1 case explicitly mentioned the lack of withdrawal, worsening cravings, and uncontrolled pain. Another study transitioned 5 patients with acute pain from full opioid agonists to solely 300 mg BUP-XR and discharged all with no signs of relapse or withdrawal. 45
Discussion
To our knowledge, no other reviews have been published with a focus on pain management in patients prescribed BUP-XR for OUD. Given the relative novelty of depot buprenorphine, most studies found were case reports or other gray literature, resulting in an overall lack of evidence-based data and consensus. Of the 6 included studies, most consisted purely of pharmacological interventions. While pain control was adequate for the vast majority of cases, there is insufficient evidence to draw conclusions on the relative effectiveness of the various approaches used. As increasing numbers of OUD patients are being initiated or maintained on BUP-XR, the clinical management of concurrent pain is an emerging, relevant, and important issue.
This review highlighted several challenges related to the issue of pain management among patients on extended-release buprenorphine. The product monograph for Sublocade® recommends that patients be treated with non-opioid analgesics whenever possible to bypass the tightly bound receptors and for full agonist opioids to only be used under supervision. 50 In turn, patients with acute pain during the continued use of Buvidal® are suggested a combination of opioids, non-opioid analgesics, and regional anesthesia. 51 In all included studies, non-opioid analgesics alone were unable to manage perioperative or breakthrough pain and were supplemented with full agonist opioids. Titrating short-acting opioid analgesics to effect is one of the only feasible ways to mitigate the blockade when buprenorphine cannot be discontinued, converted, or have its doses divided due to a depot formulation. 31 Higher doses of full opioid agonists can theoretically outcompete buprenorphine for receptor binding; this displacement allows the full agonist to activate the opioid mu receptors and thus elicit an opioid effect and response. 52 However, higher doses can also increase the risk of opioid-related adverse effects, such as respiratory depression and oversedation, adding to the challenges of adequate pain control and safety. 53
Of note, our review found no instances of adverse events due to high doses of opioid agonists. The likely explanation for the absence of abnormal vital signs despite high doses of opioids lies in the pharmacological phenomenon of cross-tolerance, specifically between buprenorphine and full mu-opioid receptor agonists. 54 Buprenorphine has a high binding affinity for the mu-opioid receptor and dissociates slowly, which can lead to prolonged receptor occupancy even after its clinical effects wane. This tight binding may result in a form of receptor desensitization or downregulation, where the receptors become acclimatized to the partial agonist effects of buprenorphine. Consequently, when a full agonist like hydromorphone is later administered, its ability to activate those receptors is reduced, requiring significantly higher doses to achieve equivalent analgesic effects. This attenuated response may help explain both the need for higher opioid doses and the relative hemodynamic stability observed, as the typical adverse effects associated with opioid toxicity are blunted due to this pharmacological cross-tolerance. Moreover, given that all pain types included in the review were transient, all opioids used were narrow spectrum with their analgesic actions limited to the mu opioid receptor. They were additionally given either in controlled-release formulations or with an acetaminophen or NSAID for a ceiling effect on the maximum dose administered.55,56 Patient-reported pain levels as high as 10 out of 10 are consistent with studies suggesting that opioid-using patients are more likely to be prescribed higher-dose opioid therapy compared to those who do not use opioids due to tolerance.57,58 Future work should seek to delineate opioid dosing guidelines that can balance adequate pain control without the risk of toxicity in long-term opioid patients.
Depending on the expected or observed level of pain, other agents such as NSAIDs, gabapentinoids, anticonvulsant and antidepressant drugs, muscle relaxants, and local anesthetics were often added for their analgesic and opioid-sparing effect. Ketorolac was specifically highlighted in 2 separate cases as an effective measure of pain control,46,47 but also failed to be beneficial when administered intramuscularly in another case. Approaches incorporating drugs with distinct mechanisms of action are expected to reduce side effects and target pain pathways in an additive and complementary action.59,60 Given the tight binding of buprenorphine to mu-opioid receptors and resulting blunted opioid responsiveness, administration of non-opioid agents are expected to improve analgesia by acting on other distinct receptors involved in pain signaling, acting synergistically with the residual effects of BUP-XR. This multimodal approach helps circumvent the limited opioid receptor availability and offers a complementary mechanism for more effective pain control. In particular, studies have indicated the potential synergy between cannabinoids and opioids in producing analgesia through G-protein coupled receptor activation,61,62 but dysphoric side effects have been observed at high doses. Future studies should carefully document any adverse effects from cannabinoid administration in those already prescribed opioids, with careful attention on dose range and tolerability. One other potential adjunctive treatment to OAT is ketamine, the use of which was limited to interoperative settings in the included studies. Ketamine is a N-methyl-D-aspartate (NMDA) receptor antagonist with analgesic and anti-hyperalgesic effects. These properties are advantageous in OUD patients at risk of developing opioid-induced hyperalgesia and tolerance. 63 Opioid-induced hyperalgesia can arise from chronic opioid receptor activation leading to central sensitization, partly mediated by NMDA receptor activation and increased glutamatergic signaling. Ketamine counteracts this pathway by inhibiting the excitatory effect from glutamate, thereby reducing hyperalgesia and providing analgesia through non-opioid mechanisms. This makes it particularly useful in patients maintained on buprenorphine, as it improves pain control without further activating opioid receptors, while also targeting the NMDA receptor activation that contributes to opioid-induced hyperalgesia. 23 Given its current role in acute pain management, opioid sparing effect, and potential to reduce opioid withdrawal symptoms, 64 continued research on ketamine therapy through experimental and clinical studies is needed in this setting.
Drawing conclusions on the clinical utility of multimodal pain regimens remains extremely challenging due to the heterogeneity of the patient population, treatment, and reported pain outcomes, and importantly, the lack of controlled trials. Selection of each treatment was dependent on clinician decision and documentation of how separate components were initiated in relation to their timing and dosing were unclear. Further studies investigating the different combinations of analgesic agents will help further evaluate effective approaches of pain control.
Our findings align with expert consensus recommendations regarding continuing buprenorphine to support patients’ recovery from OUD.10,65 In the limited evidence available, no cases of respiratory depression or toxicity were observed with the exception of mild withdrawal. Alongside adequate pain relief, a contingency plan should be in place to ensure that patients do not experience withdrawal by observing their OUD-related outcomes, including the use of non-prescribed opioids. Additional considerations may include functional recovery plans, post-discharge taper and follow-up plans, as well as hospice care for end-of-life support in palliative settings. Majority of the studies in this review did not specify the use of objective measurements for pain intensity or durations of follow-up. As pain is often an experience extending beyond acute management, the continual assessment and reporting on pain control after discharge will provide further insight into the longer-term effectiveness of the strategies employed and help assess the sustainability of relief for patients beyond the initial treatment period.
Limitations of this review merit discussion. A primary limitation across all studies is the small sample size and focus on specific patient cases, which likely include confounding factors that limit our ability to fully understand the impact of these approaches on pain management. Particularly, the significant clinical heterogeneity in analgesic regimens observed makes it difficult to determine the causality of the effect from the interventions. Given the relative novelty of BUP-XR, relevant studies were few in number, with all industry-led clinical trials having excluded patients with pain. Variability in the identified interventions precluded pooling of data and conclusions are predominantly based on narrative synthesis. Much work is needed to consolidate the disparate protocols and treatment paradigms that exist toward an ongoing effort to enable interoperability and efficient exchange of data. This is especially the case with our observed lack of published literature on BUP-XR and pain management, which would largely benefit from quantitative data collection from chart or administrative data reviews, as well as the use of same scale notations to collect reported scores. Other potential limitations include the inclusion of manuscripts only in English and the grouping of acute and chronic pain. Nonetheless, this review has produced an overview of the current evidence base for pain management in individuals receiving BUP-XR and highlights the clear need for larger-scale studies.
Despite the variations in procedures, the consensus seems to support BUP-XR continuation, multimodal non-opioid analgesia, and full agonist opioids as needed following collaborative treatment planning with the individual. Some specific factors to be considered in such planning include but are not limited to symptom severity, patient preference and goals, and mental comorbidities. In clinical practice, strategies should prioritize minimal discomfort for the patient with the ongoing aim to avoid opioid withdrawal while minimizing safety concerns. Given the large overlap between OUD and pain, it is imperative that definitive treatment guidelines are developed to improve individuals’ quality of life and functional outcomes. More studies are necessary to develop optimal strategies to manage acute pain in OUD patients on BUP-XR therapy.
Conclusion
This scoping review confirmed that clear guidelines on how to support pain management in BUP-XR treatment have yet to be identified. The best available evidence, limited as it may be, suggests combining buprenorphine continuation, non-opioid adjuncts, regional anesthesia, and full opioid agonists as needed is a clinically reasonable approach to provide synergistic analgesia and protection against withdrawal for OUD patients. Priority areas for future research include controlled study designs to compare the safety and efficacy of specific treatment regimens, as well as chart or data reviews to quantitatively summarize previous work. As the use of opioids becomes more prevalent and the opioid crisis continues to worsen, optimizing pain management strategies and identifying ways to retain patients in treatment are becoming increasingly relevant and important.
Footnotes
Appendix 1
The protocol was pre-registered on PROSPERO (ID: CRD42024581719).
Consent for Publication
Informed consent for information published in this article was not obtained because it was a review of previously published studies.
Author Contributions
PA: Conceptualization, Methodology, Validation, Investigation, Writing—Review & Editing, Supervision. JK: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Writing—Original Draft, Writing—Review & Editing. FA: Data Curation, Validation, Investigation, Writing—Original Draft, Writing—Review & Editing. KS: Data Curation, Validation, Investigation, Writing—Review & Editing. JM: Validation, Investigation, Writing—Review & Editing. AL: Validation, Investigation, Writing—Review & Editing. JS: Validation, Investigation, Writing—Review & Editing. MI: Validation, Investigation, Writing—Review & Editing. JM: Validation, Investigation, Writing—Review & Editing. MK: Validation, Investigation, Writing—Review & Editing, Supervision.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PA is a consultant for Indivior-led extended-release buprenorphine studies, however, the data from these studies are not included in this review. PA, JM, and MI have also received honoraria for educational presentations organized by Indivior. The other authors have no disclosures or conflicts of interest.
Data Availability Statement
The data used in this study is publicly available.