
Abstract
Background:
This study considers how the COVID-19 pandemic impacted individuals recovering from a substance use disorder (SUD).
Method:
Fifty individuals recovering from SUD in Vermont, a rural New England state (U.S.), were recruited for an interview from 12-step recovery meetings (Alcoholics Anonymous, Narcotics Anonymous) as well as via word-of-mouth. Interviews were transcribed and coded, and qualitative analyses were performed.
Results:
Many of the participants who were in recovery prior to the pandemic starting remained substance-free and in recovery throughout the pandemic period. Some individuals used substances during the pandemic period, although not typically in the context of a relapse caused by negative emotions (eg, distress over a loved one contracting COVID-19). The majority of those individuals indicated that the risk of catching COVID-19 did not alter their substance use.
Conclusions:
Many individuals already in SUD recovery before COVID-19 remained in recovery despite the challenges of pandemic era. The role of peer support in recovering individuals managing negative emotions caused by COVID-19 is considered.
Introduction
This study examines how the COVID-19 pandemic with its social distancing requirements affected people recovering from a substance use disorder (SUD). Recovering from SUD was defined as the use of substances (eg, alcohol, marijuana, cocaine) that had crossed a line from use to abuse, and had begun to severely and negatively impact the individual’s life (work, relationships) such that they felt a need to seek out assistance to halt their abuse. This research considers the COVID-19 pandemic as a mass trauma-inducing experience1 -5 likely to have disrupted and harmed individuals’ recovery efforts. The COVID-19 virus upended all areas of life. Activities that would normally be undertaken indoors – work, events, school – shifted to remote participation; or in-person, socially distanced, masked-up events. This includes attendance at 12-step recovery meetings.
This paper explores how recovering individuals fared during the pandemic, emotions during the pandemic period, and whether study participants relapsed. An earlier paper 6 of some preliminary findings – specifically participants’ feelings about whether the terms “addict” and “alcoholic” are stigmatizing – was published in Substance Abuse: Research & Treatment in 2023. The findings presented in the current paper are different from those in the 2023 article.
Literature Review
Substance use among adults,7 -9 relapse 10 and drug overdoses 11 increased during the pandemic. Pandemic-era stress and anxiety, combined with disruption to treatment programing, increased the risk of substance misuse and relapse. 12 A 2020 survey by the Addiction Policy Forum 13 of individuals with a substance use disorder (n = 1079) found that one-third of respondents experienced disruptions to recovery services during the pandemic. Among respondents’ concerns were the lack of access to support group meetings, including 12-step fellowship meetings. 13
Other research 14 found that some recovering individuals adapted to lock-down protocols by substituting one addiction (eg, alcohol) for another (pornography). In addition to the heightened risk of catching COVID-19 as compared to people that do not use substances, 15 individuals with SUD also face greater health and mental health issues6,16 (eg, mood disorders, depression, anxiety, overdose). Social distancing requirements presented challenges for recovering individuals, 17 whose recovery may depend on in-person support from peers.18,19 Strong social networks are a key to substance use recovery. 20 Economic and social shifts caused by COVID-19 adversely impacted access to treatment for substance abusing individuals, likely worsening their addictions.21,22 In a 2022 study 11 of 21 U.S.-based drug treatment and harm reduction programs, individuals receiving treatment reported a 27% point reduction in group counseling meetings. The pandemic necessitated outpatient clinics reducing the number of in-person appointments, compounding an already existing gap in treatment implementation. 8
One question the PI had at the onset of the study was whether individuals with pre-COVID-19 fragile recovery status (ie, the person often thought about substances and felt “on the fence” about whether they would continue to abstain from using alcohol or drugs) would be more likely to relapse, either due to the inability to attend meetings in person or because of negative emotions. Prior research 20 found that while some participants in a harm reduction program experienced isolation and loneliness during the pandemic, others found that isolating nature of the COVID-19 era was peaceful and lowered their stress. Continuing in this vein, it is plausible that some participants in the present study would feel similarly; that is, some would feel lonely and anxious while others would feel at peace.
This study also considered whether strong negative emotions about COVID-19 and all that came with it (eg, closing of in-person AA/NA meetings, sheltering in place) influenced any relapse with substances. Past research 23 has shown high levels of lifetime trauma among individuals seeking treatment for opioid addiction. As per one prior study, 24 the vast majority of patients recovering from a substance use disorder had experienced at least one traumatic event; and that relapse with substances was more common among individuals with past histories of interpersonal violence victimization. Qualitative research 25 on individuals seeking treatment for a substance use disorder, who also had untreated post-traumatic stress disorder, found that the patients craved substances and self-medicated after a trauma trigger. A 2021 review 26 of research found that the brain’s prefrontal cortex is “involved in drug seeking behavior as well as the extinction of fear conditioning, playing a role in both addiction” and post-traumatic stress disorder. The author’s own prior research 27 suggests that a past trauma experience increases individuals’ smoking.
The present study considered how the COVID-19 pandemic impacted individuals recovering from substance addiction. The study also makes the novel contribution of examining how individuals who continued to use substances during the pandemic navigated the risk of catching COVID-19 while acquiring drugs or alcohol.
Method
Sampling
Fifty individuals recovering from a substance use disorder were interviewed by the PI over the course of 18 months, beginning in June 2022 and concluding in December 2023. A primarily purposive sampling approach was employed with the goal of recruiting as many individuals as possible within the study timeframe. The PI also asked participants if they knew anyone else recovering from SUD to whom they would recommend the PI reach out (ie, snowball sampling). The study was primarily qualitative in nature, and in keeping with other qualitative research aimed to shed light on the diversity and nuances of different individuals’ experiences. Saturation of themes and insights in qualitative research is achieved around the 24th interview. 28
Participant recruitment
Participants were recruited by the PI from different socio-economic areas throughout Vermont, a rural state 29 in the New England region of the United States. The PI announced the study at 12-step meetings of the Narcotics Anonymous (NA) and Alcoholics Anonymous (AA) fellowships that were classified as open to the public. In other words, an attendee (eg, the study’s PI) did not need to be in recovery themselves to attend. Twelve-step meeting locations and times were gathered through two apps downloaded to the PI’s phone. The PI also hung informational flyers about the study in recovery centers and clubhouses where 12-step meetings sometimes convene. The decision to recruit from 12-step meetings was made because they are widely available and easily accessible throughout the state, and a key element of these types of fellowships is support from fellow recovering people. A fundamental part of these types of fellowships was likely to be greatly impacted by the mandated closure of in-person meeting facilities such as churches and clubhouses.
A $20 Amazon gift card was offered to participants as an incentive to be interviewed. It should be noted that individuals did not have to be 100% substance-free in order to enroll in the study. As long as they self-identified as being in recovery, they were eligible to enroll as a participant. Any subject who had seemed under the influence of a substance at the time of the interview would have been excluded. (This did not happen.) Interviews took place in a variety of locations (eg, coffee shops, libraries), with the participants’ comfort level being the main consideration in choosing a day, time and location to conduct the interview.
Informed Consent
Approval from the university’s institutional review board (IRB) was received in advance of participant recruitment starting. Participants were given two copies of a written informed consent form, one to keep, and the other to read, sign and return to the PI. At the conclusion of interviews participants were handed a written debriefing form, reviewing the purpose of the study and including contact information for the PI as well as the PI’s university’s IRB.
Interview protocol
All interviews were conducted by the study’s PI. No other individuals were present for the interviews. While some interviews took place in public settings (eg, coffee shops), the PI made an effort to secure a table not too close to other people present in the setting. The PI also double-checked with the participant that they were comfortable with the location for the interview. Interviews took on average 25 minutes, although the length varied depending on how talkative a participant was. The shortest interview was 9 minutes long and the longest interview lasted for 62 minutes. Subjects were asked about how their recovery experience was during the pandemic period. They were asked about substances they had use(d) (ie, tobacco, marijuana, alcohol, heroin, opioids, cocaine, methamphetamines, and “other” drugs); and whether and how their substance use patterns changed during the pandemic. Respondents were asked about how solidly they felt they were in recovery both at the time of the interview and before COVID-19; and if they relapsed with any substances during the COVID-19 period. For individuals that did relapse, they were asked about which factors of the COVID-19 era contributed to their relapsing.
To account for COVID-19 as a traumatic event, items informed by trauma symptom instruments such as the Trauma Symptom Inventory30,31 were included. (A copy of the interview protocol is included as an Supplemental Appendix to this paper.) For individuals that did relapse, or had not yet begun their recovery at the time of COVID-19, they were asked about experiences acquiring substances during the pandemic (eg, if the risk of contracting COVID-19 made them hesitate). Respondents were also asked about their fear, if any, of contracting COVID-19; and how this may have impacted their participation in recovery, and/or (if applicable) their seeking out drugs for a relapse. The perseverance to access substances despite environmental risks was of interest. In a study 9 of Canadian people who use drugs (PWUD), among those who continued to use drugs during the COVID-19 era, the PWUD reported changes in their drug supply (eg, contamination) – and yet they persisted in seeking out drugs, underscoring the powerful pull of addiction.
The “COVID-19-as-a-traumatic-event” related questions (see Supplemental Appendix) were informed by existing trauma instruments.30,31 Other protocol questions were originally written by the study PI based on her prior research on substance addiction. Questions were grounded in the study’s research questions, and were pilot tested with three recovering individuals (not part of the study’s sample) who attend 12-step meetings in advance of going “live” with the interviews.
Participants were not initially asked for their age as it was not directly relevant to the study’s questions. It became apparent at the mid-study reporting point that the study’s funder, the National Institutes of Health, was requesting certain demographic data including age. The PI thus backed into the participant database and retroactively added estimated ages. From that point forward, the PI continued to record estimated age ranges (or enter an exact age, if the participant proactively volunteered their age). For continuity, the PI opted not to start asking future interviewees their age, as this had not been done with past participants.
Data, coding and qualitative analyses
Subjects’ interviews were recorded and then transcribed using an outside transcription service. Participants’ answers to open-ended questions were coded using a code list created based on the interview protocol using Atlas Ti qualitative analysis software, which has been used in other qualitative public health research.32,33 Coding from a code list is an initial step in conducting a content analysis34,35 of responses to open-ended questions (eg, “How would you say COVID-19 and everything that came with it [sheltering in place] affected you in your recovery?”). The broad code list for the qualitative data (words and phrases from the interviews) was as follows: recovery status-now, recovery status-pre-COVID-19, trauma, emotions. Three student research assistants independently performed the initial coding of the qualitative data (ie, words and phrases) in the transcripts, and for interrater reliability reviewed each other’s coding. The PI then checked the research assistants’ coding. Once all the transcripts were coded, the PI performed searches in Atlas Ti on the various codes, looking for common themes.
Results
Participants
Twenty-nine participants were male and 18 were female. Three individuals self-identified as gender fluid or transgender. Forty-eight of the subjects were Caucasian, in keeping with the primarily Caucasian state population. The mean age range was 40s, although subjects ranged from being in their 20s to being in their 70s. The youngest participant was 21 years old. Forty percent of the participants said they attend AA exclusively; 30% attend NA exclusively; and 20% indicated that they attend both 12-step fellowships. Five participants use other or additional mechanisms (eg, therapy, church) to support their recovery. Eight percent of the sample indicated that they currently or in the past participate in medication-assisted treatment such as using doctor-prescribed suboxone to ease addiction to an opioid such as fentanyl or heroin. The mean age of respondents starting to use substances was 16 years old. Respondents had used substances for various lengths of time, for as short as 2.5 years to as long as 54 years.
Recovery status
Individuals’ length of time in recovery ranged from short (under 1 year) to long (10 years or longer; see Table 1 below). How an individual conceptualized being “in recovery” was left to them, but generally corresponded with their initial efforts to stop or reduce their use of substances, sometimes with 12-step fellowship support and other times not. Being in recovery was not framed as being the same thing as being substance-free. For instance, some participants indicated that they had been on their recovery journey for many years, but had relapsed with substances a few months prior. One participant said that she had two recovery dates, the first for when she stopped using heroin and transitioned to using suboxone; and the other – her “real” recovery date – when she got off suboxone for good.
Length of time in recovery.

Information is not available for one individual.
Alcohol and marijuana were the most commonly used substances over the course of participants’ lifetimes. The majority of respondents had used or did currently use tobacco, primarily cigarettes. Other substances used included prescription drugs, Quaaludes, secobarbital, inhalants (eg, huffing nitrous), “a lot of different pills. . . like benzos,” angel dust, Ritalin, amphetamines, Adderall, and Xanax. Preferred substances were across the board and included alcohol, cocaine, crack cocaine, marijuana, heroin, opioids, pain killers, and valium.
The majority of respondents (80%) classified their current recovery status as
Impact of the pandemic on recovery and substance use
Many participants had negative comments about the impact of COVID-19 on their recovery (see Table 2, below). Others also provided some positive perspective about the time, and/or that the pandemic was minimally impactful on their recovery and life.
Impact of the pandemic on recovery.

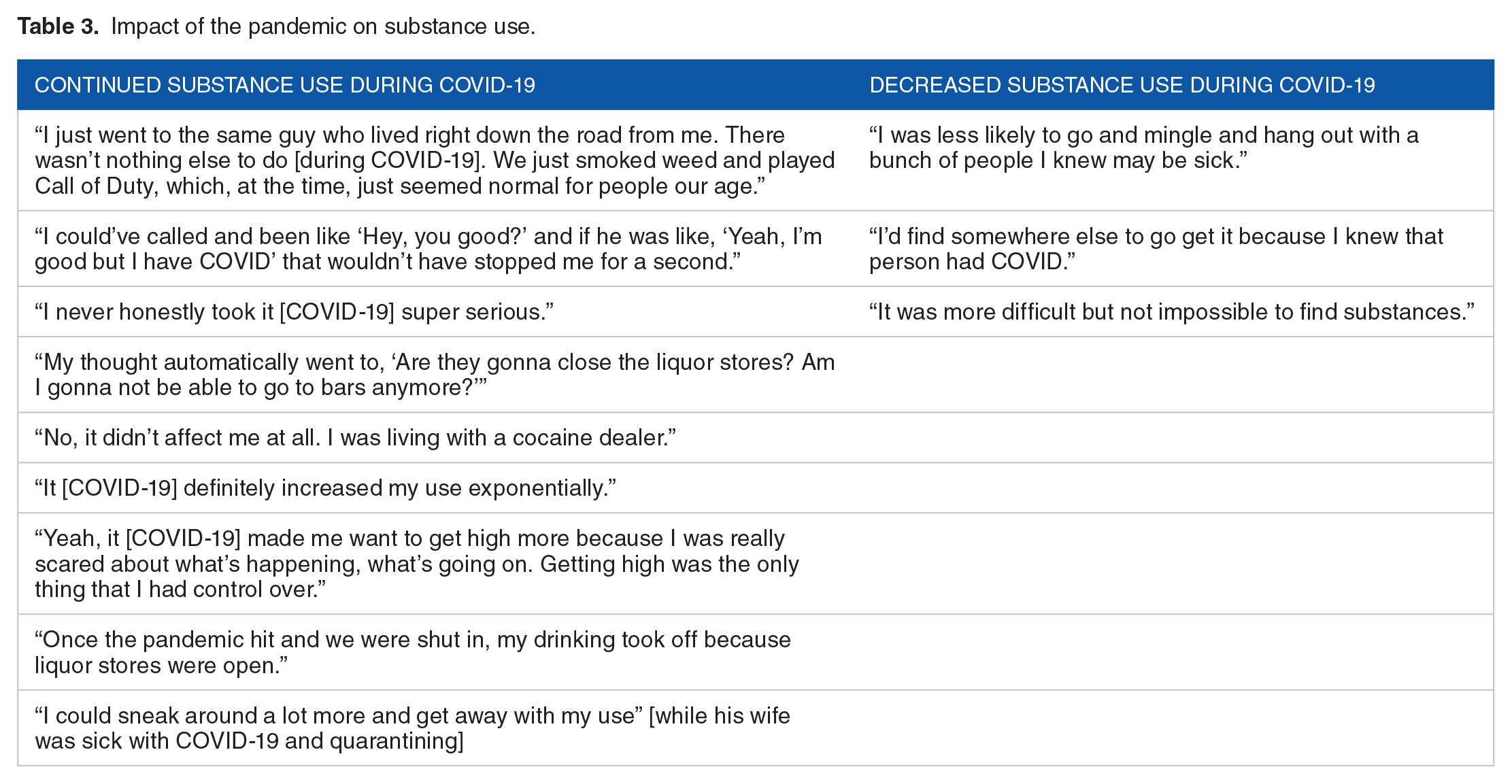
Of the fourteen individuals who used substances during the pandemic, most indicated that they sought out substances regardless of the risk of catching COVID-19. A few individuals said that the risk of catching COVID-19 impacted their seeking out and abusing substances in that they decreased their use. Examples of comments are shown in Table 3.
Impact of the pandemic on substance use.
Emotions during the COVID-19 pandemic
As seen in Table 4, the majority of respondents indicated they had felt anxious, sad, and depressed often or sometimes during the pandemic period. More than half indicated that they felt lonely. Fewer respondents said they sometimes or often felt “anger” emotions (ie, rage, wanting to hurt someone).
Emotions during COVID-19.

In terms of other emotions during the pandemic, participants mentioned some
Emotions and (thoughts of) relapse
Eleven participants (n = 11) indicated that they had had a recent relapse. While subjects expressed a variety of pandemic-era emotions, only three individuals connected their emotions to a subsequent relapse. As one participant explained, “Yeah, that [drinking] was like the most helpful thing for me at the time [when their friends were sick with COVID-19] because there was no real like support that I felt. . . those resentments built too, and then wanting relief from that kind of validated my [alcohol] use at the time.” Another interviewee thought about relapsing, but did not end up turning to substances, because of fears for their mother. “My biggest fear before she actually did pass away was my mom passing away. . . . I was in Vermont, not in San Diego yet when she had it, and just knowing her health and stuff, yeah, it was definitely triggering [of wanting to use drugs].” Another participant explained that turning back to alcohol provided some comfort during the pandemic “because there was no real support that I felt [for front-line workers]. I also felt really misunderstood and really taken for granted.” One participant explained that while they did not end up relapsing, they began to have “very vivid dreams” about relapsing. “During the COVID pandemic, I started having dreams about use to the point where I’d wake up and I can still taste the drug. You know, I used to snort meth and there’s this taste. . . . I mean, the taste is that vivid. And so, there were times that I really had crystal clear vivid dreams that I haven’t had in a long time. The only thing I can think of is stress.”
Emotions around loved ones contracting COVID-19
Slightly more than half of the sample caught COVID-19, and nearly everyone had friends or family that had contracted the virus. In describing how their friends and family catching COVID-19 affected them emotionally, subjects’ responses tended to fall into one of two categories. First, some comments reflected the fact that loved ones’ illnesses
Discussion
This study examined the impact of the COVID-19 pandemic and everything that came with it (eg, sheltering in place) on the substance use recovery experience. There are a number of key findings. First, in terms of the pandemic’s impact on recovering individuals, while COVID-19 presented challenges, many of the respondents maintained their recovery throughout the pandemic period. Some participants did not experience much of a COVID-19 impact on their recovery, either because they had a strong pre-COVID-19 recovery foundation, were used to being alone, or got into recovery during the pandemic period and had never experienced in-person meetings and as such had no sense of losing something. These findings echo those of Smith et al 20 who determined that while some patients in a harm reduction program felt lonely and isolated during the pandemic, others found that isolating nature of the COVID-19 era to be peaceful and stress-lowering.
While the majority of participants felt their recovery was solid at the time of the interview, some individuals continued to use substances during the pandemic period. The majority of those individuals indicated that the risk of catching COVID-19
This study is part of a body of research on the myriad emotions processed by individuals recovering from a substance use disorder during a traumatic time in life.23 -25 In a qualitative study 25 of patients with comorbid substance use disorder and posttraumatic stress disorder, patients sometimes relapsed with substances following a trauma intrusion when they saw no other avenue for coping with their emotions. In contrast, participants in the current study experienced both negative feelings (frustration, stress) and positive emotions (gratitude, sense of hope). This may be due to the peer support offered through 12-step programs, which continued to exist albeit in a virtual format.
Limitations
As with any research study, there are a number of limitations that must be acknowledged. The results presented are based on qualitative analyses of data from a modest sample (50 individuals) recruited primarily from 12-step recovery fellowships. The biggest challenge to conducting the study was subject recruitment. Given the rural nature of Vermont, the long geographical distance to some 12-step meetings, and massive rains and subsequent flooding of cities that occurred during the summer of 2023, participant recruitment remained challenging throughout the study period. Even with the $20 Amazon gift card as an incentive, some prospective subjects – men in particular – remained wary about being interviewed, or initially agreed and then changed their mind. Additionally, individuals still struggling with addiction and not actively seeking recovery would not have been candidates for the study. As such, the findings cannot easily be generalized to the larger population of individuals dealing with a substance use disorder.
It should also be acknowledged that the interview protocol was originally created for this study and not previously validated through prior research, although the trauma emotion questions were informed by existing trauma scales,30,31 as was mentioned in the method section. The reason for creating original questions was that the pandemic was a new event and no interview protocols existed that asked about specifically what the PI wanted to know. The interview protocol was pilot tested with three recovering individuals (not part of the study’s sample) in advance of the study “going live.”
Finally, while the PI believes that a sample size of 50 is sufficient to achieve saturation of the study’s main themes and question – the impact of the COVID-19 pandemic on individuals’ substance abuse recovery journey – a formal power calculation regarding sample size was not conducted as it is unusual to do so with a qualitative study. A review of prior literature 28 on sample size in qualitative research supports the sufficiency of a sample of 50 recovering individuals for an interview project of this nature.
Implications for Practitioners
While some research36,37 has found that 12-step fellowships lack effectiveness in reducing substance use, the present study suggests that individuals participating in 12-step meetings may access resources (eg, peer support) that are helpful in managing negative emotions, which may in turn contribute to non-relapse during a trying period. The pandemic is but one difficult life event, and an individual recovering from substance addiction may also experience divorce, death of a loved one, or job loss – all of which can cause acute distress and threaten one’s recovery. Having similarly situated peers to share the pain with can help alleviate the distress. In keeping with the National Institutes of Health current framework, being “clean” (ie, drug and/or alcohol free) frames recovery in a stigmatizing way 38 and is not necessarily reflective of an individual’s recovery journey, which may involve multiple relapses while a person nonetheless remains tethered in some small or large way to network of recovering peers. Even if a person has a “slip” with substances, having a support network of non-judgmental friends may help bring them back to recovery sooner. Participation in 12-step fellowship meetings is an option as a sort of low-cost outpatient recovery resource 39 that can connect individuals with a support network.
Supplemental Material
sj-docx-1-sat-10.1177_29768357241287405 – Supplemental material for The Impact of the COVID-19 Pandemic on Recovery From Substance Use Disorder: Findings From a Qualitative Study
Supplemental material, sj-docx-1-sat-10.1177_29768357241287405 for The Impact of the COVID-19 Pandemic on Recovery From Substance Use Disorder: Findings From a Qualitative Study by Connie Hassett-Walker in Substance Abuse: Research and Treatment
Supplemental Material
sj-docx-2-sat-10.1177_29768357241287405 – Supplemental material for The Impact of the COVID-19 Pandemic on Recovery From Substance Use Disorder: Findings From a Qualitative Study
Supplemental material, sj-docx-2-sat-10.1177_29768357241287405 for The Impact of the COVID-19 Pandemic on Recovery From Substance Use Disorder: Findings From a Qualitative Study by Connie Hassett-Walker in Substance Abuse: Research and Treatment
Supplemental Material
sj-pdf-3-sat-10.1177_29768357241287405 – Supplemental material for The Impact of the COVID-19 Pandemic on Recovery From Substance Use Disorder: Findings From a Qualitative Study
Supplemental material, sj-pdf-3-sat-10.1177_29768357241287405 for The Impact of the COVID-19 Pandemic on Recovery From Substance Use Disorder: Findings From a Qualitative Study by Connie Hassett-Walker in Substance Abuse: Research and Treatment
Footnotes
Acknowledgements
The PI is grateful to all the study participants for sharing their recovery experiences during the pandemic with the PI. The author is also grateful to her colleagues at the Vermont Biomedical Research Network for their ongoing support of this research. The PI expresses gratitude to the study’s student research assistants for their work in coding the interview transcripts.
Author Contribution
The PI is the sole author of the manuscript and is responsible for 100% of the analyses presented, and the writing of the manuscript.
Funding:
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number P20GM103449 to the Vermont Biomedical Research Network (VBRN). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NIGMS, NIH or VBRN.
Declaration of conflicting interests:
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Connie Hassett-Walker, the study PI and author of the paper, has no conflicts of interest in conducting this study or writing this manuscript.
Ethical Approval
The study was initially approved by the PI’s Institutional Review Board on November 30, 2021. Two IRB renewals were sought and obtained on December 19, 2022 and again on January 2, 2024. All participants received and signed written informed consent forms prior to being interviewed.
Informed Consent
Approval from the Norwich University’s institutional review board (IRB; IRB #00005859) was received in advance of participant recruitment starting. Participants were given two copies of an informed consent form, one to keep, and the other to read, sign and return to the PI.
The chair of the Norwich University IRB is Dr. Mark Stefani,
IRB Statement
This study was approved in advance by the Norwich University Institutional Review Board (IRB; IRB #00005859) on November 30, 2021. Two IRB renewals were sought and obtained on December 19, 2022 and again on January 2, 2024. The chair of the IRB is Dr. Mark Stefani,
Trial Registration Number/Date
Not applicable
Data Availability Statement
A deidentified version of the database used in the analyses of this paper is available upon request from Dr. Connie Hassett-Walker (
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.