
Abstract
Introduction:
Tobacco use is the major preventable cause of premature death worldwide, responsible for about 8 million deaths per year, mostly in low- and middle-income countries, such as Morocco. Adolescents’ tobacco use is a matter of concern, because early initiation increases the risk of becoming a lifelong user. There exists a notable gap in the synthesis of evidence concerning tobacco use among Moroccan adolescents. Thus, the purpose of this study was to provide a comprehensive view of the prevalence of tobacco products’ use and associated factors among adolescents in Morocco.
Methods:
We systematically searched PubMed, Scopus, Web of Science and ScienceDirect for relevant studies reporting prevalence rates of tobacco products’ use among Moroccan adolescents, published until June 2024, using inclusion and exclusion criteria in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. Additional searches were completed on other sources to reach unpublished reports. The Joanna Briggs Institute Critical Appraisal Checklist was used to assess the quality of included studies.
Results:
After the final screening, 22 papers met the inclusion criteria. Life-time prevalence of tobacco use ranged from 7.8% to 20.4% for cigarettes smoking, from 10.6% to 21.9% for waterpipe, from 7.9% to 9.1% for chewing tobacco and from 9.2% to 12.4% for snuff. The last 12-month prevalence of cigarette smoking was comprised between 6.9% and 10.8%. As for the prevalence of current use, ranges of (1.8%-16.4%) and (4.9%-8.4%) were noted for cigarettes and waterpipe, respectively. The most commonly highlighted risk factors for tobacco use included male sex, older age, having friends or family members who use tobacco and low perception of risk associated with tobacco use.
Conclusion:
Our findings reveal an alarming situation of tobacco use among Moroccan adolescents. Therefore, it is crucial that all stakeholders engage in concerted efforts to develop and implement evidence-based preventive interventions among early adolescents.
Introduction
Tobacco use is one of the greatest public health threats the world has ever encountered, already responsible for about 8 million deaths annually. 1 More than 85% of those deaths are the result of direct tobacco use, while around 1.2 million results from being exposed to second-hand smoke among non-smokers. 1 The World Health Organization (WHO) has computed 1.3 billion tobacco users worldwide with around 80% of them living in low-and-middle income countries (LMICs). 1 Financially, this imposes a heavy burden on countries. Economic costs arising from tobacco use amount to around $US 1.85 trillion, including the healthcare-needs costs, and the productivity losses due to tobacco-related morbidity and mortality. 2 In the Casablanca region of Morocco, 9.7% of all adult deaths (aged 35 years or older) were attributable to cigarette smoking in 2012, 3 representing the latest available data.
Adolescence, the transitional stage from being a child to an independent adult, is considered as a crucial period in human development, during which physical, cognitive, social and emotional changes occur. 4 Thus, adolescents are a relatively vulnerable and high-risk population for tobacco use initiation, since the majority of tobacco users begin their use during this life stage. 5 According to the WHO, globally, at least 1 in 10 adolescents aged 13 to 15 years use tobacco. 6 Studies have shown that young users are more likely to develop severe levels of nicotine addiction. Consequently, they are more likely to maintain tobacco use habit into adulthood. Furthermore, early use initiation correlates with the risk of cessation failure; those who start using tobacco early in their adolescence have more difficulty quitting, smoke more heavily and longer, than those who get involved in tobacco use later.5,7
In addition to its direct harmful effects, tobacco is designated as a “gateway substance,” according to the “gateway hypothesis,”8 -10 that describes a sequential order in drug use and claims that people who are already licit drug users can become more inclined to use “harder” drugs or illicit drugs thereafter than are non-users. Furthermore, studies demonstrated a clear link between young people’s tobacco use and their engagement in a wide range of risky behaviors that can compromise their health and well-being, such as illicit drug use, delinquency, risky driving or drunk-driving, early sexual activity, physical violence, school drop-out, unhealthy eating, etc., and argued that these risk behaviors tend to “cluster” and coexist constituting what is labeled “risk behavior syndrome.” So, those reporting one behavior are more likely to experience other risk behaviors.11 -14 Therefore, attempting to prevent tobacco use among adolescents might have a significant indirect impact on preventing many other risk behaviors, which subsequently promotes their physical and mental health.
Over the past few years, several studies have been conducted on the prevalence of tobacco use behavior among Moroccan adolescents. A synthesis of existing data on the subject is useful to help inform healthcare managers and policymakers and provide them with evidence that serves as a basis for adequate strategies and interventions to prevent and control tobacco use in Morocco. To the best of our knowledge, there is no comprehensive synthesis of data on tobacco use among Moroccan adolescents. Therefore, in order to fill in this knowledge gap, we conducted a systematic review of studies reporting the prevalence of tobacco use and associated factors among adolescents.
Although cigarette smoking is the most common form of tobacco use, 1 this review considers data on other tobacco products as well, such as smoking a product other than cigarettes (e.g. waterpipe or e-cigarette) and consuming smokeless tobacco (chewing tobacco and snuff). Moreover, tobacco use behaviors are reported across 3 time periods: lifetime use, last 12-months’ use and last 30-days’ use (or current use).
Methods
Study registration and reporting
The present systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews. 15
Search strategy
Four international databases (PubMed, ScienceDirect, Scopus, and Web of Science) were searched from inception to June 18, 2024, to identify all relevant literature reporting prevalence rates of tobacco products’ use among Moroccan adolescents.
We developed a search strategy using 4 groups of key-terms which were combined using Boolean operators (“AND” and “OR”):
Additional studies that fulfilled the inclusion criteria were identified by scanning references of included studies, as well as from Internet searches of the websites of the World Health Organization and the Moroccan Ministry of Health.
Inclusion and exclusion criteria
Were considered for this review, studies that:
Our aim was to report data for adolescents; therefore, we excluded studies conducted with a combination of adolescents and adults, when we could not disaggregate the data for adolescents age groups. Studies targeting specific populations (patients, students of vocational institute, doctors and paramedical staff, fishermen, construction workers, dockers, taxi drivers, etc.) were also excluded. Finally, the following manuscript types were rejected: case studies, qualitative studies, scales validation studies, conference papers, theses, systematic reviews, and meta-analyses.
Identified studies were independently reviewed for inclusion by 2 researchers (S.M and B.Z). When discrepancies arose, consensus was reached on inclusion or exclusion by discussion.
Data extraction
Data extraction was performed by a reviewer (SGM) and checked independently by another (BZ). For each eligible study, we extracted the following data; study design, year of the study, region of study, study population, included sample size, sex distribution, age characteristics, associated factors with tobacco use, sampling method, sample size calculation, response rate, administration method, measure or assessment tool, validity of tool and pilot testing.
Quality assessment
The Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data 17 was used to assess the methodological quality of the included studies. The checklist consisted of 9 items addressing the following issues; (1) appropriateness of target population, (2) sampling methods, (3) adequacy of sample size, (4) study subjects and setting description, (5) if coverage of identified sample was adequate, (6) the use of a valid method to identify the condition, (7) if the condition was measured in a standard, reliable way for all participants, (8) appropriateness of statistical analysis, and (9) adequacy of the response rate. Each study was assessed across each of these areas, with results reported as “Yes,” “No,” or “Unclear.” Studies were assigned an overall score, reflecting the number of questions with a “Yes” response. The quality assessment was performed by two reviewers (SGM and BZ) and reported in Supplemental File 2.
Results
Search results
As shown in Figure 1, a total of 657 articles were identified from searched databases. After duplicates were excluded, 598 records were screened by title and abstract. Other 585 records were excluded after reading the title and abstract, and the remaining 13 articles were screened further for eligibility by full-text reading. From these, 6 articles were excluded for the reasons shown in the PRISMA diagram (Figure 1). Fourteen additional reports were identified from gray literature repositories (WHO website, Ministry of health website and MedNET website and other sources). Also, the examination of the reference lists of the reviewed articles resulted in the inclusion of another article. Finally, 22 publications were admitted for this systematic review. From those 22 publications, 218,19 generated from the same study (addressed the same sample) and both were included. Thus, 21 studies were included in this review. The PRISMA checklist is in Supplemental File 1.

PRISMA flow diagram.
Characteristics of included studies
All included studies were cross-sectional studies. Twelve were conducted nationwide,20 -31 while 5 were carried out at a regional level; 1 in Beni Mellal region, 32 1 in Fez-Boulemane region, 33 1 in Fez-Boulemane and Taza Taounate El Hoceima regions18,19 and the fifth one in the Gharb-Chrarda-Béni Hssen region. 34 The remaining studies were conducted at city level; in Casablanca, 35 Rabat, 36 Marrakech, 37 Kenitra, 38 and Taza city. 39 All studies were conducted between 2001 and 2021, in middle and/ or high school or university settings, except one study done in households. 21 Three studies addressed urban, sub-urban (or peri-urban) and rural areas,29,33,35 and 15 studies addressed both urban and rural areas.18 -28,30-32,34 The setting for the 4 remaining studies was only urban area.36 -39
There was a wide sample size difference among the studies ranging from 450 36 to 7055 22 adolescents. The majority of the studies included relatively large sample sizes (>1000 participants, range 2670-7055 participants). Only 6 studies (out of 20) included smaller samples (range 450-764 participants). All included studies addressed both males and females. The major characteristics of included studies are showed in Table 1, while the methodological characteristics are displayed in Table 2.
Characteristics of included studies reporting Moroccan adolescents’ tobacco use prevalence.
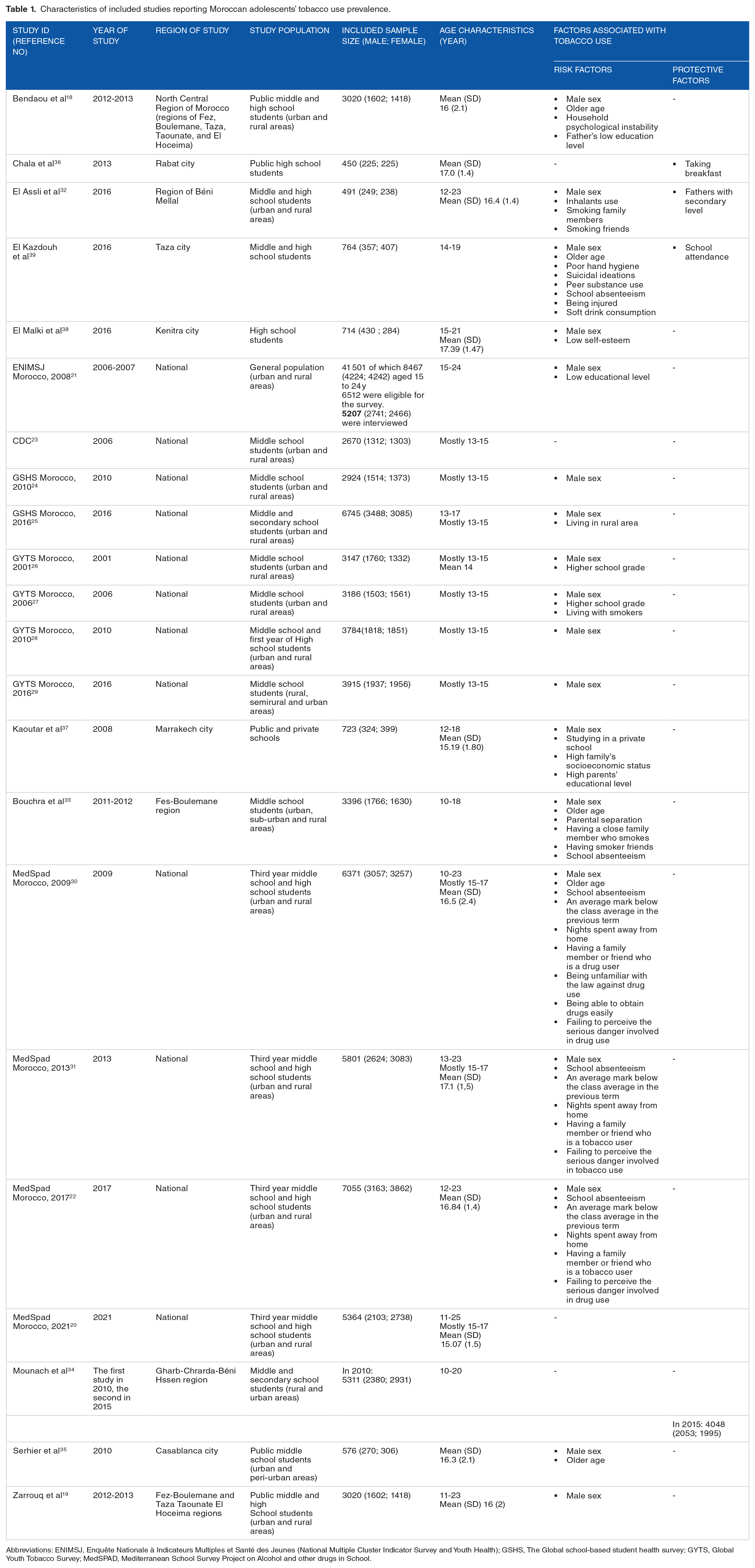
Abbreviations: ENIMSJ, Enquête Nationale à Indicateurs Multiples et Santé des Jeunes (National Multiple Cluster Indicator Survey and Youth Health); GSHS, The Global school-based student health survey; GYTS, Global Youth Tobacco Survey; MedSPAD, Mediterranean School Survey Project on Alcohol and other drugs in School.
Methodological characteristics of included studies reporting Moroccan adolescents’ tobacco use prevalence.
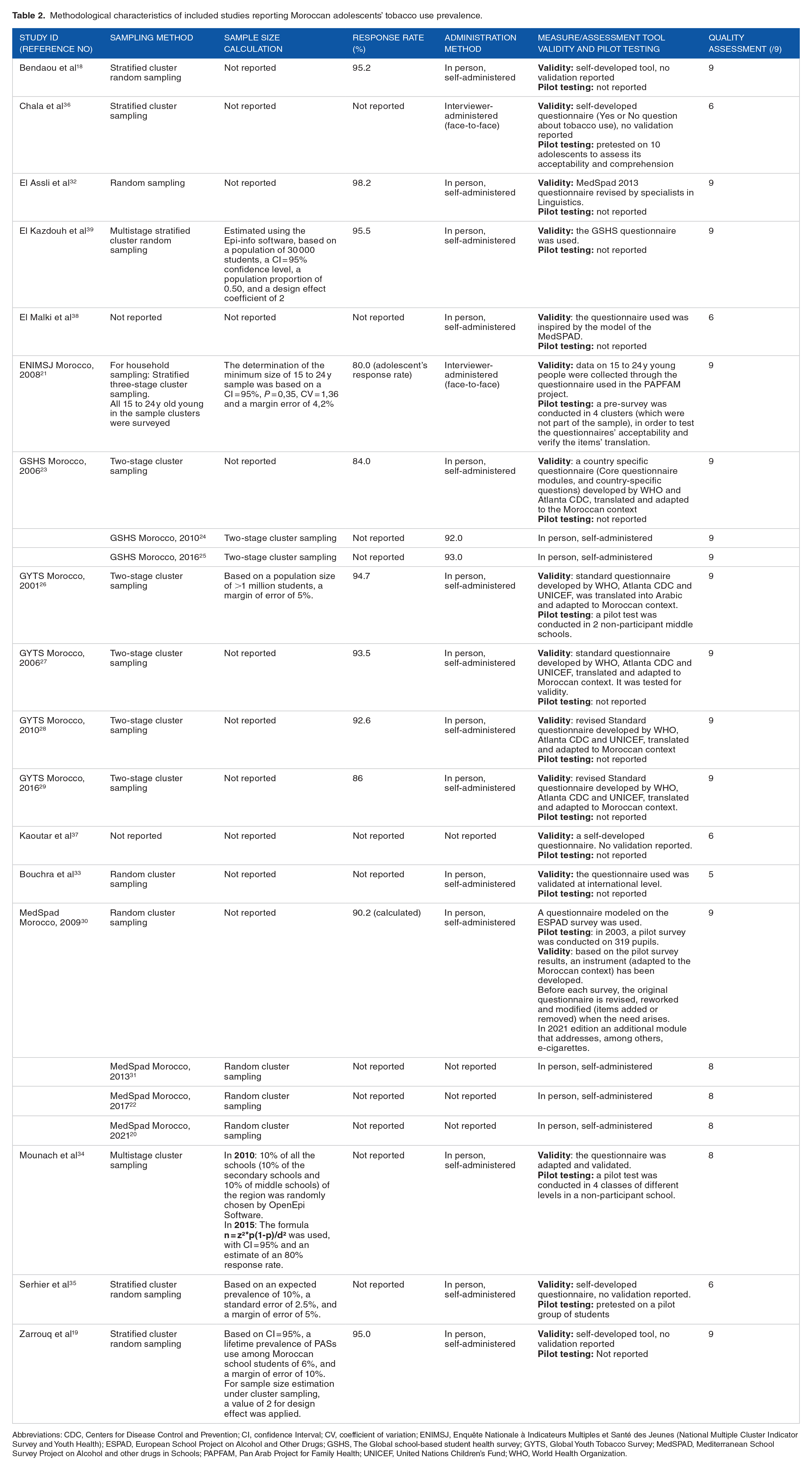
Abbreviations: CDC, Centers for Disease Control and Prevention; CI, confidence Interval; CV, coefficient of variation; ENIMSJ, Enquête Nationale à Indicateurs Multiples et Santé des Jeunes (National Multiple Cluster Indicator Survey and Youth Health); ESPAD, European School Project on Alcohol and Other Drugs; GSHS, The Global school-based student health survey; GYTS, Global Youth Tobacco Survey; MedSPAD, Mediterranean School Survey Project on Alcohol and other drugs in Schools; PAPFAM, Pan Arab Project for Family Health; UNICEF, United Nations Children’s Fund; WHO, World Health Organization.
Quality assessment
The quality of the studies was examined based on the 9 quality areas. Total quality ratings ranged from 6 to 9 (M = 8.04, SD = 1.3; Table 1). Sixteen studies received a total score of 8 or higher. All studies addressed the target population adequately (criterion 1), considered an adequate sample size (criterion 3), described the study subjects and the setting in detail (criterion 4), and collected data in a reliable way for all participants (criterion 7). In 18 studies, the sampling was conducted appropriately (criterion 2), and the statistical analysis was performed in an appropriate way (criterion 8) in 20 studies. All but 2 studies used a valid method to identify the condition (criterion 6). In 5 studies, data analysis was performed without sufficient coverage of the identified sample or not clearly described (criterion 5). Finally, 9 studies received an “unclear” on the criterion 9 because they did not report and discuss the response rate (Supplemental File 2).
Prevalence of tobacco use (Table 3)
Tobacco use prevalence.

Any tobacco form/product use
Based on a total of 21 studies, the highest overall lifetime prevalence of any tobacco product use among Moroccan adolescents was 21.9% and the lowest one was 6.2%. The prevalence of use in the last 12-month reported ranged from 6.3% to 10.8%. As for the prevalence of current use of any tobacco product, 32.4% and 1.8% were noted as the highest and lowest prevalence, respectively.
Cigarette use
Cigarettes were the most studied form of tobacco; all included papers reported its prevalence of use. From these papers, 95.4% reported the current cigarette smoking prevalence, 54.5% reported the lifetime prevalence and only 31.8% reported the last 12-months prevalence. There was a huge heterogeneity within studies; the lifetime prevalence of cigarette smoking was comprised between two values; 7,8% 28 and 20.4% 30 ; while the last 12-moths prevalence was between 6.3% 20 and 10.8%. 30 Current cigarette smoking was between 1.8% in a study conducted among secondary and middle school students in the Gharb-Chrarda-Béni Hssen region 34 and 16.4% in a study conducted among secondary school students in Kénitra city. 38
Other tobacco products (other than cigarettes)
GYTS and GSHS studies reported the prevalence of current other tobacco products (other than cigarettes) use. Data from the GYTS showed a decline of current other tobacco products use; the prevalence rates reported were 9.2% in 2001, 9% in 2006, 9% in 2010, and 2.8% in 2016. Contrary to the GYTS findings, the GSHS studies showed rather an increase in the prevalence rate which went from 5.9% in 2006 to 10.8% in 2016.
Water pipe/hookah use
The results indicate hookah/waterpipe as the second most predominantly reported form of tobacco after cigarettes; 8 studies out of 21 reported its prevalence of use. From these studies; 6 studies provided the lifetime prevalence and 4 studies provided the current use prevalence. The lifetime prevalence values of hookah use varied between 10.4% 20 and 21.9%. 30 The current use prevalence ranged between 4.9% 28 and 8.4%. 39
Chewing tobacco/snus use
Three studies, out of 21, looked at the lifetime prevalence of chewing tobacco/snus. A nationwide study conducted in 2013 among middle and high school students 31 reported that 9.1% of participants have ever used chewing tobacco, while a similar study conducted in 2017 22 found a prevalence rate of 8.9%. The third study, 32 done in Béni Mellal region in 2020, revealed that 7.9% of students have used this tobacco form in their lifetime.
Snuff use
Three studies investigated the lifetime prevalence of snuff use among adolescents. A nationwide study 31 revealed that 12.4% have used this substance at least once in their life. Another nationwide study 22 showed a prevalence rate of 10.6%. El Assli et al 32 assessed psychoactive substances use prevalence among school adolescents in Béni Mellal region and found that the overall prevalence of snuff use was 9.2%. These studies took place in 2013, 2017, and 2020 respectively.
Electronic cigarettes use
Two nationwide studies covered e-cigarettes use among adolescents. About 1 in 10 students (10.7%) reported having tried e-cigarettes. 20 The prevalence of e-cigarettes current use was found to be 5.3% (6.3% among boys and 4.3% among girls) 29 in a nationwide study conducted in 2016. 29 A close prevalence (4.8%) was reported in the latest Moroccan MedSpad edition. 20
Age of tobacco use initiation
Out of twenty-one studies, thirteen discussed the age of “initiation.19,20,22,24 -28,30 -33,35 Only 5 provided the mean age of initiation.19,22,30,31,33 A remarkably young mean age of tobacco use initiation reported was among a population of middle school students in 2014 in the region of Fez-Boulemane, where students started smoking very early at the age of 11 years, 33 while the latest mean age of tobacco onset reported was 15 ± 1.2 years. 22
Besides, 3 other nationwide studies provided the percentages of tobacco users who began smoking before the age of 10. The percentages reported were 24.3% ± 6.0 in 2001, 26 24.2% (95% CI, (18.2-31.4)) in 2006, 27 and 30.6% ((95% CI, (22.1-40.6) in 2010. 28 The GSHS showed that, in 2010, among adolescents who have ever smoked cigarettes, 18.2% had tried their first cigarette by the time they were 14 years or less. 24 In 2016, the percentage reached 63.3%, 25 while in 2021, the percentage decreased to 53.2%. 20 In the later study, it is also revealed that 12.9% of ever-smoking adolescents smoked their first cigarette at age 9 and less. 20 El Assli et al revealed that >50% of tobacco users initiated the consumption between 14 and 18 years old, and added that the majority of students (>50%) experimented snuff and snus for the first time at an age between 12 and 16 years. Similarly, Serhier et al 35 concluded that 52.5% of smokers began smoking between the ages of 14 and 18 years.
For shisha, the age of initiation of >50% of users was between 14 and 18 years old, 32 while the latest nationwide study showed that a proportion of 40.2% initiated shisha before the age of 14 years old. 20
Concerning e-cigarettes, the majority of users (approximately 60%) initiated at 15 years and over, 23.4% started between 13 and 14 years old, and 9.8% started very precociously at 10 years or younger. 20
Factors associated with tobacco use
Factors associated with Tobacco use identified from findings are summarized in Figure 2. Risk factors are broken down into four domains; the sociodemographic factors, individual factors, family-related factors and community-related factors.

Factors associated with tobacco use among Moroccan adolescents.
Discussion
The current systematic review provides an overview of tobacco products’ use among adolescents in Morocco, as well as the associated risk and protective factors.
The results of included studies showed that between 6.2% and 21.9% of Moroccan adolescents had ever used tobacco (any tobacco product) during their lifetime. This finding was slightly lower than the prevalence reported by the recent MedSpad surveys in other Maghreb countries; such as Algeria (24.6%) 40 and Tunisia (25.1%). 41 However, much higher values were noted in northern countries of the Mediterranean Region; Cyprus (36%), Portugal (37%), Greece (39%), France (55%), Italy (58%), always according to the MedSpad survey. 42 Considering the last 12 months, we found that the prevalence ranges between 6.9% and 10.8%, while the prevalence rates noted in Algeria and Tunisia are 14.3% and 14.9%, respectively.40,41 There are only small differences between prevalence rates in Maghreb countries and this may be due to the commonalities between the countries (predominantly Muslim countries, culturally close, same mother tongue, etc.).
This appraisal also revealed that the current tobacco use (any tobacco product) among Moroccan adolescents was ranging between 1.8% and 32.4%. The wide difference noticed may be due to variations in the sample size, participants’ age, and study settings or location of data collection. The prevalence of current tobacco use revealed by this systematic review is relatively higher than what was reported in reviews from other Arabic World countries. A review that investigated the prevalence, patterns, and determinants of tobacco use in Sudan, reported a prevalence between 1% to 25% among children and adolescents. 43 Likewise, in Saudi Arabia, Al-Mutairi et al 44 found in his review 22% as the highest prevalence rate of current tobacco use among adolescents. Besides, the upper range of our finding appears to be higher than a result of an analysis of the prevalence of tobacco use among school-going adolescents in 22 African countries (Morocco was included), where an overall prevalence of 19.1% was found. 45 The disparity noticed seems justified, since the analysis was conducted using the GYTS (2013-2018) datasets for adolescents aged 11 to 17 years, whereas our review considered a wider range age, up to 25 years old. The prevalence of current tobacco use largely differed across WHO regions. Using GSHS data from 2006 to 2013, Xi et al 46 reported prevalence rate of 12.3% in Africa, 13.2% in Americas, 14.0% in Eastern Mediterranean, 6.3% in Europe, 8.9% in Southeast Asia, and 17.6% in Western Pacific. Making direct comparison between findings seems difficult and meaningless, as there are many differences that warrant caution in making any comparison; (1) difference in data sources (Xi et al considered only GSHS data, while we considered all studies reporting prevalence of adolescents’ tobacco use in Morocco), (2) duration of considered studies (Xi et al used data from 2006 to 2013, while our systematic review covered a period from 2001 to 2017), (3) age of participants (in the study of Xi et al only young adolescents aged 12-15 years were considered).
Cigarettes was the most reported tobacco product. Findings of this study showed that between 7.8% and 20.4% had smoked cigarettes at least once in their lives. Considering the last 12 months, the prevalence of use of cigarettes ranged from 6.9% and 10.8%. The prevalence of current use of cigarettes was between 1.8% and 16.4%. In comparison with other reviews from Arab World countries, a review investigating tobacco use among Sudanese found that the prevalence of current cigarette use among adolescents ranged between 3.8% and 13.6%, 43 which is slightly high but less extreme than our finding. Another review from Saudi Arabia reported an extreme prevalence range of current cigarette use (2.4%- 39.6%). 47 Substantially higher prevalence rates were noted in previous studies from Arab countries, such as in Egypt (17.4%) 48 and KSA (48.2%). 49
The current review showed that between 10.6% and 21.9% of Moroccan adolescents have already tried waterpipe in their lifetime. It means that waterpipe is more frequently tried compared with cigarettes (7.8%-20.4%). In fact, another study concluded that waterpipe is increasingly becoming the first tobacco product ever tried by youth. 50 This may be attributable to the diversity of attractive flavors which motivate adolescents to experiment with waterpipe. Also, the various appealing smells and tastes make “waterpipe smoking” every time a new experience. Furthermore, there is a common misconception that waterpipe smoking is less harmful than cigarettes, and more socially acceptable.51,52
In this appraisal, only 5 studies investigated smokeless tobacco use. The lifetime prevalence reported was comprised between 7.6% and 12.4%. It was comprised between 7.9% and 9.1% for chewing tobacco, and between 9.2% and 12.4% for snuff use. Our finding is consistent with prevalence values from other Arab countries such as Algeria (7,8%), 40 Tunisia (10.1%), 53 and Mauritania (12.6%). 54
Unfortunately, few studies investigated the current smokeless tobacco use. The only 2 studies that provided data on current smokeless tobacco use, showed a prevalence of 3.1% among Moroccan adolescents’ national sample in 2016, and a prevalence of 8.8% in a city-based study in 2019. Based on the latest data from 138 countries in 2010to 2019, 55 the overall prevalence of current smokeless tobacco use was 4.4% among adolescents aged 12 to 16 years, and varied significantly across all 138 countries ranging from 0.0% in Tokelau to 51.6% in Kiribati. Notably, the prevalence was highest in lower-middle income countries (5.5%), compared with in high-income countries (2.8%). In Morocco, this tobacco form has relatively received little attention from researchers. Therefore, research efforts should be strengthened in order to spot and monitor smokeless tobacco use especially among adolescents, because these products seem to become “their favorites” since they can be used discreetly, without being noticed by adults, and without smoke smell on clothes. Also, smoke-free tobacco products can be used even in places where smoking is prohibited (workspace, schools, etc.).
While e-cigarettes use has become a major public health concern, that is becoming increasingly prevalent worldwide,56,57 research in Morocco remains scarce and only 2 studies examined e-cigarette use. These studies placed ever use of e-cigarettes at 10.7%, 20 and current e-cigarettes use at 5.3% 29 and 4.8%. 20 A recent systematic review and meta-analysis 57 revealed that the global lifetime and current prevalence of e-cigarettes vaping among adolescents and school students were 25% and 11%, respectively. It stated that current prevalence rates vary widely across countries. For example, a prevalence of 1% was noted in Mexico, and 3.5% in Canada and 9.9% in the United States. This study also demonstrated the upward trend of the prevalence of lifetime and current e-cigarettes vaping among adolescents and school students from 2011 to 2019.
Even if the prevalence rates reported in Morocco are lower than the global pooled prevalence, a notable finding which is “nearly 10% of ever users have vaped their first e-cigarette before the age of 10” was reported. This finding emphasizes the urgent need for further comprehensive research to track the trend of e-cigarettes use among Moroccan youth, understand its use patterns and identify its associated factors so that appropriate preventive measures could be developed and implemented.
According to the studies reporting the mean age of initiation to tobacco products, the provided mean age was comprised between 11 and 15 years. The lower limit of this interval indicates an earlier onset in comparison with results of similar studies from other countries, such as Saudi Arabia (12.96 years for males and 12.49 years for females), 58 Tunisia (13,6 ± 0,09 years), 41 Nigeria (12.0 ± 3.32 years), 59 United States (12.6 years), 60 India (12.4 ± 1.9 years), 61 Congo (14.1 ± 1 years). 62 However, other studies’ results align with ours. A study conducted in Sudan revealed an initiation age of 11 years. 63 Another one, among Algerian adolescents showed that 57% of those aged 15 started using tobacco before the age of 13 years old. 40 Similarly, 58% of European adolescents reported the onset of ever-smoking under the age of 14. 64
Even more worrisome, some included studies reported that between 24.2% (95% CI, (18.2-31.4)) and 30.6% ((95% CI, (22.1-40.6) of tobacco users started smoking before the age of 10 years old, which agrees with the finding of a systematic review on smoking initiation among adolescents carried out in Asia, where the age of tobacco initiation ranged between 10 and 14 years. 65
Overall, the different values of initiation age support the need for development of early preventive interventions against tobacco use that reach teenagers aged 10 years and even younger, with the aim of delaying the age of initiation. In this regard, studies argued that delaying the age of the first use is an effective way to prevent tobacco use behaviors. 66
The focus on factors associated with tobacco use among Moroccan adolescents is key for building tailored prevention strategies. Numerous factors were reported in the included studies as correlated to tobacco use among Moroccan adolescents, but we found that the most commonly highlighted were: (1) male sex, (2) older age, (3) having friends or family members who smoke, and (4) low perception of risk associated with tobacco use.
The male sex was, unsurprisingly, a recurrent associated risk factor with tobacco use. This sex disparity was common with other studies’ findings both in Arab countries40,41,43,47,67,68 and even elsewhere,45,69 -72 that indicates a significantly higher prevalence of tobacco use among males. But it is noteworthy that in Morocco, as in other Arab-Muslim countries, tobacco use is more disapproved among women than men. It is perceived as a male-specific behavior which is opposed to femininity norms. Thus, even women who smoke, choose to do it secretly and refuse to disclose it. As a result, the girls’ level of honesty (or veracity) during investigations into their smoking status may have been influenced.
Consistent with previous studies,45,47,71,73 it was shown that the prevalence of tobacco use gradually increased with increasing grade or age. This can be explained by the fact that an older age means more freedom or more denial of restrictions and a desire to get independence. Thus, their curiosity to experience new things including high-risk behaviors or situations get greater.
Another factor; peers or friends’ tobacco use, was reported as a factor shaping adolescents’ initiation to tobacco use and its maintenance. Young adolescents express “getting older and mature” by spending more time with their peers, especially outside the home. Thus, their influence on each other becomes more noticeable. Non-users can become users only by friends’ imitation. In addition, young people may get involved in substance use just to be accepted by their friends’ group. This factor was commonly cited in many other studies.43,44,47,71 -74
Similarly, family members’ tobacco use, including parents and siblings, influences substantially adolescents’ behavior. This family influence may be explained by the fact that adolescents consider adult family members (especially parents) as role models to whom they look up to and want to be like, so they imitate their behaviors, even the risky ones, thinking that these are a sign of adulthood. Otherwise, the availability of tobacco products at home (owned by tobacco-using older family members) may motivate adolescents to try. The present finding follows other systematic reviews that have showed that tobacco use by parents or family members is a predictor of tobacco use among adolescents.43 -45,47,71 -74 This result emphasizes the importance of considering parents’ attitude when developing policies and interventions for tobacco use prevention among adolescents.
A low-risk perception made adolescents more likely to get involved in tobacco use. Pupils who are unaware or not sufficiently informed about tobacco-use may underestimate its side effects, so they don’t take tobacco-related problems seriously. This factor was well investigated in many other studies.43,65 A longitudinal study examined to what extent perceptions of smoking-related risks and benefits influence adolescent smoking initiation. Participants with the lowest perceptions of long-term smoking-related risks were 3.64 times more likely to start smoking than were participants with highest risk perceptions. Similarly, participants with the lowest perceptions of short-term smoking-related risks were 2.68 times more likely to take-up smoking than were adolescents with highest risk perceptions. 75 Moreover, believing that smoking provides benefits such as increasing popularity and social connections or improving mood, reducing anxiety, boredom and depression makes the adolescent at a higher risk of tobacco initiation. The previous study reported that adolescents who had the highest perceptions that smoking brings benefits were 3.31 times more likely to start smoking. Another study showed a higher risk of becoming tobacco smoker among participants who believed that smoking would be relaxing (HR = 6.95, 95% CI: 3.60;13.43), and those who believed that smoking is enjoyable (HR = 4.74, 95% CI: 2.58;8.72); who feel more comfortable at gathering with friends (HR = 4.29, 95% CI: 2.33;7.92); who think that smoking would give them something to do when they were bored (HR = 3.42, 95% CI: 1.91;6.13); and would help to deal with problems or stress (HR = 3.19; 95% CI: 1.76;5.79). 76
Academic performance and school bonding were reported as involved in tobacco use risk. Poorly engaged students who do not have a sense of belonging to school, with a poor level of academic achievement are more likely to engage in tobacco use behavior.77,78 A study examined which comes first (tobacco use habit or school-related problems) found that theses variables influence each other mutually; smoking may precede the low school engagement and poor academic achievement, as it may be the result. 79
Conversely, school attendance was pointed out to be associated with a lower risk of tobacco use. Fathers’ higher educational level and taking breakfast were additional protective factors.
In our review, only a few studies have examined protective factors of tobacco use among adolescents, thus, future studies are needed to explore more factors and understand their influence on delaying the initiation and impeding maintenance of tobacco use in this population.
Regardless of the different percentages from one study to another, our findings spotlight that tobacco use is worriedly prevalent among adolescents in Morocco. The variations noted can be the result of different sample size, study setting or participants’ age range. In the same vein, it is significant to point out that almost all included studies (except one) were conducted in a school context, so out-of-school adolescents are not represented. The choice of school as a framework for such surveys can be justified by the fact that adolescence coincides with the age of compulsory schooling, so in order to reach the maximum number of adolescents, researchers opt for schools. However, this may result in an underestimation of the prevalence of tobacco use, while the situation is much alarming than what has been expected. Out-of-school youths (dropouts or those who never attended school or high school graduates not enrolled in higher education “non-university goers”) are more vulnerable to substance-use issues and other risky behaviors as studies have stated that higher prevalence rates were recorded among this category.80,81
The most effective way to reduce tobacco use is to prevent its initiation among youths. The early age of onset values highlighted are disturbing and call clearly for implementing evidence-based preventive interventions from the primary school. Indeed, the lack of school-based prevention programs in Morocco is blameworthy. More progress should be made in order to design and develop school-based programs adapted to Moroccan context considering risk and protective factors among Moroccan adolescents. To achieve optimal outcomes and ensure tobacco use reduction, these programs must involve all stakeholders, especially parents, peers, and educational authorities. Studies, evaluating the impact of anti-tobacco use school interventions, reported that school-based programs can reduce smoking onset by 25% to 30%. 82 Well-designed prevention programs based on health education and life-skills development have shown positive effects. They strengthen youths’ life-skills and develop protective factors against tobacco initiation, change the social norms and perceptions about this behavior, and reinforce the negative attitude toward it. Well-designed programs have proven their effectiveness.83,84 Also, other preventive measures must be strengthened, for instance, prohibiting the sale of tobacco products to minors and the verification of the customer’s age by the seller, by requiring an identity document, increasing promotion of smoking cessation services, protecting young people, especially children from exposure to second-hand smoke, engaging Non-governmental Organizations in awareness-raising campaigns on the harmful and deadly effects of tobacco use, and limiting the availability of tobacco products near schools.
Strengths and limitations
Some limitations suggest a cautious interpretation of our findings. First, the cross-sectional design of all included studies. It rules out the inference of cause-effect relationships between tobacco use and its associated factors. Second, nearly all studies were carried out in a school setting, which implies that our findings are representative of school-going adolescents only. Thus, the future studies should give more attention to out-of-school adolescents when investigating tobacco use related issues. Third, as included studies collected data using self-reported form, these data can be affected by recall bias or social desirability bias (especially since tobacco use can be a taboo and related questions may be sensitive and private). Fourth, because of the diversity of methodologies and heterogeneity of data across studies, we could not perform an analysis of the trends of tobacco use among Moroccan youths. Therefore, we settled on performing a narrative systematic review.
Nevertheless, this review is the first one to systematically report prevalence of tobacco-products use among Moroccan adolescents and its associated factors, examined across 21 studies that include 75 662 participants. The strengths of the present study include information on a variety of tobacco products and the focus on an expanded age range of 10 to 24 years. Hence, it provides a comprehensive picture of adolescents’ tobacco use situation in Morocco that can be the cornerstone for building effective preventive interventions.
Conclusion
The current study’s findings indicate the serious situation of tobacco products use among adolescents in Morocco. We deplore the absence of school-based prevention programs targeting this vulnerable population and we advocate and encourage dialog between policymakers, public health professionals and other stakeholders in order to develop policies and programs focused on tobacco-use prevention and implement them earlier as much as possible.
Supplemental Material
sj-docx-1-sat-10.1177_29768357241272370 – Supplemental material for Prevalence of Tobacco Products’ Use and Associated Factors Among Adolescents in Morocco: A Systematic Review
Supplemental material, sj-docx-1-sat-10.1177_29768357241272370 for Prevalence of Tobacco Products’ Use and Associated Factors Among Adolescents in Morocco: A Systematic Review by Salma Ghofrane Moutawakkil, Abdelfettah EL-Ammari, Hicham EL Malki, Mohammed El Amine Ragala, Karima EL Rhazi and Btissame Zarrouq in Substance Abuse: Research and Treatment
Supplemental Material
sj-docx-2-sat-10.1177_29768357241272370 – Supplemental material for Prevalence of Tobacco Products’ Use and Associated Factors Among Adolescents in Morocco: A Systematic Review
Supplemental material, sj-docx-2-sat-10.1177_29768357241272370 for Prevalence of Tobacco Products’ Use and Associated Factors Among Adolescents in Morocco: A Systematic Review by Salma Ghofrane Moutawakkil, Abdelfettah EL-Ammari, Hicham EL Malki, Mohammed El Amine Ragala, Karima EL Rhazi and Btissame Zarrouq in Substance Abuse: Research and Treatment
Footnotes
Acknowledgements
This research work was supported by Abu Dhabi National Oil Company (ADNOC), Emirates NBD, Sharjah Electricity Water & Gas Authority (SEWA), Technology Innovation Institute (TII) and GSK as the sponsors of the 4th Forum for Women in Research (QUWA): Sustaining Women’s Empowerment in Research & Innovation at University of Sharjah. We would like also to thank Mr. El Mostafa MOUTAWAKKIL, retired English language teacher, and Mr. Yassir Lazrak, a Professor of English Studies at the University of Sidi Mohamed Ben Abdellah, for proofreading an earlier version of the manuscript.
Abbreviations
$US, United States dollar; CDC, Centers for Disease Control and Prevention; CI, confidence Interval; CV, coefficient of variation; ENIMSJ, Enquête Nationale à Indicateurs Multiples et Santé des Jeunes (National Multiple Cluster Indicator Survey and Youth Health); ESPAD, European School Project on Alcohol and Other Drugs; GSHS, The Global school-based student health survey; GYTS, Global Youth Tobacco Survey; HR, Hazard ratio; MedSPAD, Mediterranean School Survey Project on Alcohol and other drugs in Schools; PAPFAM, Pan Arab Project for Family Health; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; SD, Standard Deviation; UNICEF, United Nations Children’s Fund; WHO, World Health Organization.
Authors’ Contributions
SGM and BZ conceptualized the study, designed the extraction templates, performed the quality assessment. SGM and BZ extracted and interpreted data. SGM wrote the manuscript. AEA and HEM critically reviewed the manuscript. BZ, MEAR and KER supervised this work, and provided methodological support and feedback throughout revisions. All authors have read and approved the final manuscript.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article and its Supplemental Information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.