
Abstract
Objectives:
Veterans with substance use disorder (SUD) can show high severity and are at high risk of relapse due to trauma histories and other comorbid conditions. However, evidence-based SUD therapies may not be available to many veterans due to geographic or transportation constraints. Telehealth approaches have shown promise to improve access to different SUD therapy formats but have not been well-studied in open (rolling-admission) group therapy of in-person patients as administered by a single on-screen therapist.
Methods:
Social distancing required by the COVID-19 pandemic forced the transition of delivery of Transcending Self Therapy (TST) from an in-person therapist to a single remote (on-screen) therapist. In this virtual model, veterans continued to receive TST but the therapist was off site and provided therapy to veterans who were together in the same room during a 28 day residential Veterans Affairs treatment program. In a program evaluation, we compared their changes in quality of life (QoL), treatment satisfaction ratings and group therapy treatment outcomes with those of Veterans who received TST from an in-person therapist.
Results:
In both groups, there was a significant increase in QoL Inventory scores from baseline to post-treatment, with no difference in improvement between treatment modalities (i.e., in-person group vs telehealth-delivered group). Veterans professed knowledge of therapy-driven skills at the end of treatment in both groups and overwhelmingly rated TST as helpful and understandable.
Conclusions:
These data extend previous findings of patient acceptability of remotely-delivered SUD treatment, here with a remote therapist administering open group therapy, as evidenced by improvement in QoL and positive patient feedback about the remote intervention.
Keywords
Introduction
Substance use disorders (SUDs) incur substantial psychosocial and economic costs. In 2022, 48.7 million Americans aged 12 or older (17.3%) were classified with SUD in the past year 1 per DSM-5. 2 The annual costs to the U.S. economy associated with SUD are estimated to exceed $600 billion. 3 Environmental stressors and related mental health issues, such as post-deployment civilian reintegration challenges, financial stressors, PTSD, depression, and loneliness put U.S. military veterans particularly at risk for developing SUDs. Indeed, a review of prior studies from 2017 revealed that more than 1 in 10 Veterans were diagnosed with SUDs, while data from 2012 to 2013 National Epidemiologic Survey on Alcohol and Related Conditions (NESARC-III) revealed a 25% lifetime incidence of Alcohol Use Disorder (AUD).4,5 Moreover, roughly 30% of completed suicides in veterans followed alcohol or drug use, while about 20% of deaths by high-risk behavior were attributed to alcohol or drug overdose.4,6 These findings collectively underscore the urgency of advancing access to SUD in veterans.
Fortunately, engagement in SUD treatment has been shown to reduce substance use severity7 -9 better employment outcomes, 10 more favorable legal outcomes, 11 reduced overdose rates, 12 and reduced mortality.12,13 Although evidence based SUD treatment programs that support improvements in quality of life (QoL) are available, the implementation of these programs, especially among vulnerable populations, is lacking. Veterans also struggle considerably with clinical, financial, social, and geographic access to in-person mental health care.4,14 To greatly expand access to SUD treatment for veterans, the U.S. Department of Veterans Affairs (VA) began promoting technology-based remote access to healthcare even before the onset of COVID-19, with such incentives drastically accelerating during the pandemic. 15 Indeed, SUD therapy and other mental health treatments are well-suited to telehealth due to their predominant reliance on extended verbal communication with providers and peers, and relatively lower reliance on biomarkers (e.g., serum chemistry, vital signs, diagnostic imaging).
Despite how some studies have demonstrated that patients are highly satisfied with telehealth interventions when available and accessible, 16 not all providers and patients are equally ready to engage in telehealth services, resulting in treatment disparities. 17 Research findings on telehealth interest and acceptability in veterans with SUDs are mixed.18,19 The factors contributing to these mixed findings have not been closely investigated. For example, patient impressions of telehealth may depend on technology access, where telehealth adoption, use, and treatment adherence are less common in Black, Latino, and other non-White veterans, compared to White veterans, and in those with lower socioeconomic backgrounds or with more chronic conditions.14,15,18 -22 Most prior telehealth engagement studies are focused on one-on-one telehealth interactions with patients, with patients connecting from their own home. This format thus places the responsibility of successfully using the necessary technology on the patient, requiring the patient to have access to a video-capable device, a reliable internet connection, relevant technological training, and adequate comfort level with technology—factors affected by racial and SES disparities in some studies. 23
To mitigate these barriers, researchers have called for raising the level of technological access, training, and awareness among patients. Alternatively, in residential group-based SUD treatments, many of these technological barriers may be lifted if a remote group therapy provider is connected to all the residential patients through a single telehealth screen maintained by the facility, while the patients can interact with each other face-to-face. This particular hybrid form of telehealth treatment delivery may allow patients to reap the benefits of in-person interactions and support of group members (e.g., bonding with other Veterans with similar lived experiences), while mitigating consequences of provider scarcity and unavailability in particular patient locations. This format of telehealth treatment could be applied in both residential and non-residential group/community settings and may allow 1) overcoming the barrier of provider shortage in rural areas, 2) lifting the requirement of providing technological training to each patient, 3) treating active-duty personnel when deployed and staff at their job site, and 4) cutting the cost of technology distribution and patient training.
Not well-understood, however, is the impact of removal of actual (physical) provider presence on a manualized cognitive behavioral therapy (CBT) that is reliant on provider-facilitated interactions between patients who have who themselves remain together in physical proximity as they engage in the material. It may be that CBT that is heavily reliant on inter-patient mentoring and collective problem-solving exercises may suffer from the physical absence of the therapist/facilitator. How well telehealth approaches work in “open group” therapy program formats is also poorly understood. In contrast to a “closed” group format wherein the group of patients is essentially static throughout the program, a common occurrence in the Veterans Health Administration and other hospital systems is to have “rolling” group formats wherein modular psychoeducation content presents the same total content to each individual patient, but where the patient would experience each concept at different points in his/her treatment. This format enables more experienced patients to mentor and assist new admissions to the program. When the program also features workbook-based homework, physical proximity of more experienced patients can also leverage the shared lived experiences of patients (military service and SUD).
The COVID-19 pandemic introduced a natural experiment to evaluate the impact of removing the physical proximity of a provider who must educate and facilitate a rolling-admission, in-person patient group. To reduce virus transmission, early in the pandemic, VA providers were advised to convert in-person services to telehealth when possible. 24 To ease this transition, many barriers to telehealth were eliminated. HIPAA Security and Privacy Rule requirements were relaxed, and reimbursement structures were expanded to support telehealth for both behavioral health and medical providers. 25
We conducted a program evaluation to examine the impact on SUD care of the rapid transition to remote-provider delivery of cognitive behavioral therapy (CBT), here in an understudied format, wherein: 1) the telehealth intervention consisted of a single remote therapist interacting on-screen with a group of patients all in proximity to each other, and 2) the therapy content was administered in a modular format to an open/rolling group. The CBT approach used was Transcending Self Therapy: Group Integrative Cognitive Behavioral Treatment (Group TST-I-CBT), an integrative and modular 20-session group intervention previously demonstrated effective for in-person residential programs. 26 Specifically, we determined whether COVID-era hybrid-group format TST-I-CBT delivery showed patient acceptability and evidence of effectiveness akin to in-person group TST-I-CBT administered prior to restrictions. Based on previous reports of successful implementations of other telehealth-based SUD therapies, and because the hybrid format retained the dynamic of in-person inter-patient mentoring, we hypothesized that individuals receiving Group TST-I-CBT SUD treatment in the hybrid-group telehealth delivery format would also show improved quality of life (QoL) post-treatment relative to pre-treatment, with no difference from treatment/time effects observed in pre-COVID in-person group patients, such that the two groups combined would show an overall main effect of time and TST-I-CBT treatment to improve QoL.
Methods
The Richmond VA Medical Center Institutional Review Board (IRB) determined this analysis to be a programmatic evaluation of treatment impact using extant standard-of-care assessments used in the treatment program, and thus not human-subject research requiring informed consent. Participants were not randomized into treatment groups as they received the modality offered at the time they were enrolled in residential treatment.
Participants
This program evaluation featured the electronic medical records review of N = 299 consecutive veterans with one or more SUDs who received SUD treatment in the Substance Abuse Residential Rehabilitation Treatment Program (SARRTP) of a large, Mid-Atlantic VA Medical Center just before and during the COVID-19 pandemic. Incidence of different (and non-mutually-exclusive) SUD in patients is shown in Table 1, where alcohol was the primary substance with disordered use in n = 180 patients, with stimulants n = 56, opioids n = 49, tobacco n = 6, cannabis n = 4, other substances n = 3, PCP n = 1, and undetermined n = 1. The SARRTP is a 28-day residential treatment program for veterans with SUDs that includes group psychotherapy, individual case management, peer recovery support, spirituality groups, 12-step facilitation, vocational therapy, occupational therapy, and pharmacotherapy. All participants received Transcending Self Therapy as the primary program, delivered in one of two formats: traditional, in-person, receipt of TST prior to the pandemic (N = 189) or telehealth receipt of TST during the pandemic (N = 110). Although subject to some disruption from the pandemic, there were no changes to the referral process in the transition to telehealth, nor in the psychoeducation content. Thus, the only distinctions between the two groups were the pandemic versus non-pandemic context of their SUD and therapy and the modality of treatment (in person pre-pandemic vs telehealth on weekdays during pandemic).
Demographics and SUDs of the complete sample of program evaluation patients.

Measures
The following variables were collected from manual electronic medical records review.
Demographics
Patients’ self-reported race, ethnicity, age, and gender were collected from their medical records.
Substance use disorder diagnoses
Patients’ substance use disorder diagnoses as determined by intake clinician(s) were retrieved from their medical records.
Quality of life inventory
The Quality-of-Life Inventory (QOLI) is a 32-item measure of life satisfaction and well-being across 16 domains, where each item is weighted by that respondent’s valuation of that particular quality of life domain, and shows a reliability = 0.80). 27 The QOLI was administered at intake and/or admission to the SARRTP program. QOLI data that most closely aligned with program onset were taken for this analysis. Responses to the QOLI were entered into Mental Health Assistant, a program used by the VA system of care to facilitate administration and scoring of assessment measures. The automatically generated score reports followed the guidelines as recommended by the test publisher. A standardized score is provided in the score report, a weighted life-satisfaction T-score, which was used for this analysis. This score is calculated by multiplying the raw score within each domain of the measure by the relative importance of each domain, which are then standardized using normative data provided by the publisher. With this scale, a T-score of 50 is considered “average,” and a score between 40 and 60 is considered to be within “normal range.”
Treatment retention
Participants’ SARRTP completion status (completed or not completed) was retrieved from their medical records.
Treatment receipt
Participant receipt of IOP treatment between intake and admission was recorded.
The TST-I-CBT intervention
The TST-I-CBT treatment for both groups (e.g., psychoeducation concepts, homework) was the same for all patients, with the exception of modality, with the same SARRTP Coordinator overseeing both in-person and telehealth care. The features and approach of TST is presented in detail in Supplemental Online Information. In brief, Group TST-I-CBT consisted of 4 modules, each containing five 50-minute sessions, totaling 20 sessions over a 4-week (~28 days) period, and supplemented with four 50-minute individual weekly sessions. 28 The four TST modules encompass: 1) cognitive conceptualizations, 2) behavioral interventions, 3) cognitive interventions, and 4) obstacles to sustained recovery. Combined, they address improving participants’ understanding of their past experiences, the development of their core beliefs about self and their current thought patterns, how these patterns influence emotional state and substance use, and how to change thought structures to cultivate healthy emotions and behaviors that could help move towards recovery. The sessions also address identifying external situations and relationships that promote substance use and relapse, and proactively selecting and engaging in situations, social relationships, communications styles, and daily activities that promote recovery. TST-I-CBT group treatment was designed to be conducted in an open-group modular structure, which permits new participants to join any day of the modular cycle as their first session during the treatment. Each session of a module also functions independently, without the requirement of knowing the prior session. The open-group format was designed to allow potential clients to access treatment faster, and thus improve access. The open group format also allows newly-admitted patients to learn concepts, skills, commitment, and vulnerability navigation through modeling clients who joined earlier and also receive peer support and encouragement from more experienced peers. All TST-I-CBT providers were supervised by or consulted with Dr. Reisweber (TST-ICBT co-developer) who has experience in previous trials monitoring therapist fidelity as a research director directly under Aaron T. Beck.
In addition to TST-I-CBT, patients in both groups received one 50-minute session of Acceptance and Commitment Therapy (ACT) and Seeking Safety each week. ACT sessions integrate components that leverage mindfulness to help maintain a flexible relationship with maladaptive personal narratives (e.g., cognitive diffusion) and guide participants toward value-based behaviors to live a meaningful life. The Seeking Safety sessions involve discussions of various quotes and psychoeducation about skills that orient participants towards practicing greater honesty, identifying red flags in their lives that promote substance use (e.g., trauma reminders, loneliness) and adaptively handling such red flags; they also train to recognize signs of danger, create safety plans, and cultivate skills (e.g., “recovery thinking”) to accurately interpret and resolve emotionally difficult situations.
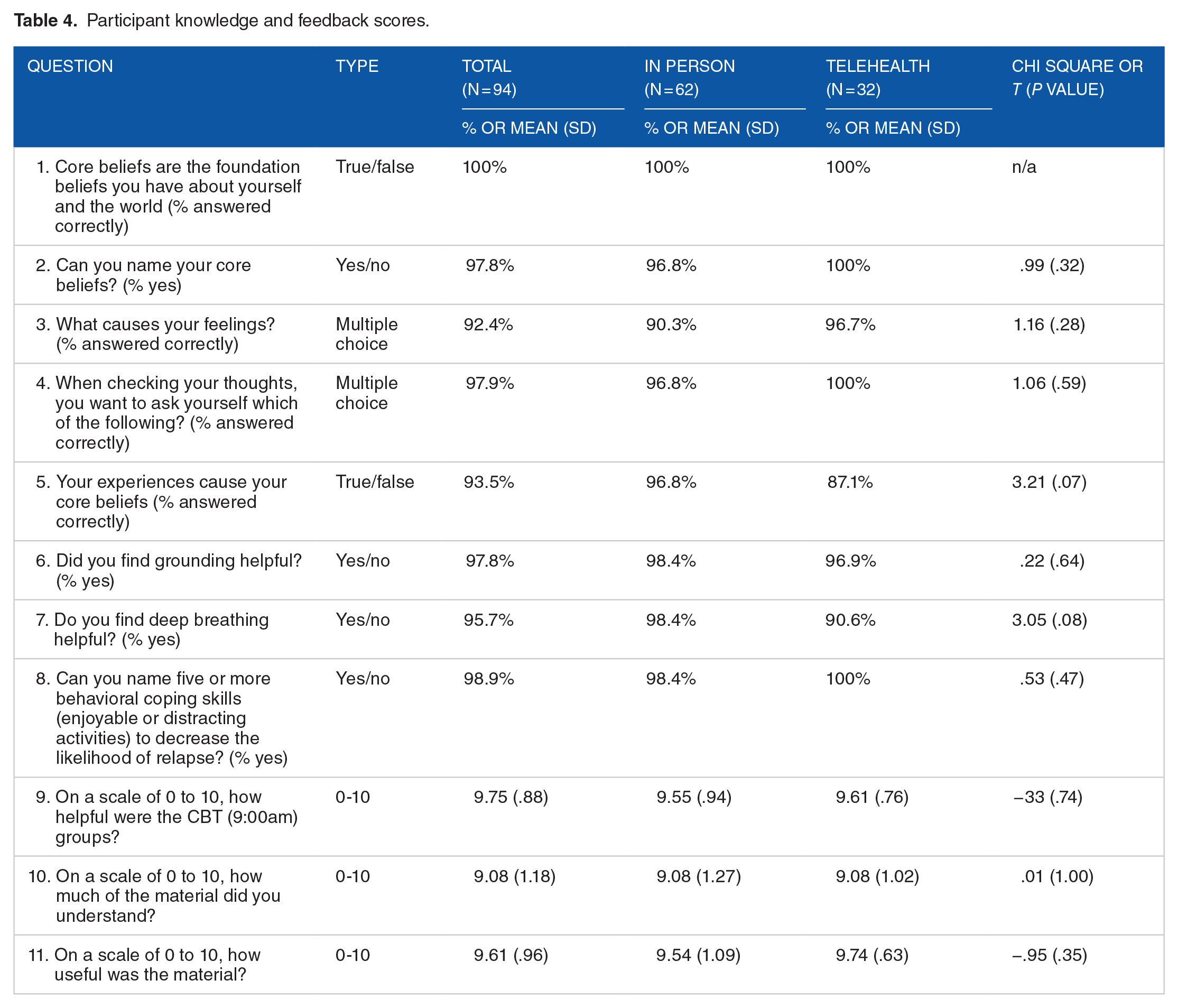
At the conclusion of treatment, patients were invited to complete a survey about the TST-I-CBT therapeutic content. Some questions probed patient comprehension of TST-I-CBT concepts, others invited the patient to provide his or her subjective impressions of TST-I-CBT. Some questions were true/false, others multiple choice, while impression items invited the patient to rate on a Likert scale (see Table 4, which presents the questionnaire items verbatim). Patient completion of forms was part of standard of care, voluntary, and anonymous. Patients received the form within two business days of discharge and were asked to place it in the nursing station should they choose to complete the form.
Data analysis plan
Chi-square analyses and independent t-tests were used to determine if demographic characteristics, SARRTP treatment completion rates, time between QOLI completion and admission, and SUD diagnoses differed between the 2 treatment groups. For each individual analysis, the pool of patients was limited to the subset of the 299 total patients for which data were available for that particular metric in electronic medical records. For example, in analyses directly comparing within-patient changes in QOLI scores between treatment delivery groups, analyses were limited to those individuals who had pre and/or post QOLI scores available in their chart (N = 124 for in person, N = 20 for telehealth). A paired t-test was used to evaluate within-patient change in QOLI T-scores pre- to post-treatment for each patient. Two-way Mixed ANOVA was used to determine presence of any treatment modality interaction effect with pre- to post-treatment QOLI scores. All analyses were carried out using SPSS version 27.
Results
Sample demographics and type of SUDs at intake
Sample demographics and types of SUDs at intake for 28-day residential care are shown in Table 1. In brief, the sample was almost all male (88.6%), roughly half Black (54.8%) and half white (42.8%). The mean age was 53.28 years (SD = 12.89). There was no difference between groups in terms of Age, Gender, Race, or SUD diagnoses at intake, nor in the time interval between the intake evaluation and admission to the residential program.
Mode of therapy delivery and treatment outcomes
Patients who received telehealth treatment were more likely to have participated in other VA treatment before SARRTP admission than those who attended in person treatment, but there was no significant group difference in treatment completion (see Table 2). There were no incidents of an unexpected drug-positive urine sample in either group.
Treatment engagement differences between groups.

The majority of participants were evaluated using the QOLI (Table 3) as our metric of treatment effectiveness. Baseline QOLI scores did not differ between patients who did versus did not engage in other VA treatment prior to residential admission. In order to assess whether each patient group experienced a change in QoL score, a paired samples t-test was run separately for each group, with both the in-person (N = 124; t = 9.67, p < .001) and the telehealth (N = 21; t = 3.93, p < .001) scores significantly increasing from their first assessment to the second. The pre- and post-scores for the sample overall were significantly different, with an overall mean score change of +14.15 on the QOLI (SD = 16.37; t = 10.41, p < .001; N = 145). A two by two within-subjects ANOVA was performed to identify if there was an interaction effect of time and treatment group on QoLI scores and found that the improvement in QoLI scores between groups did not differ significantly (F = .66, p = .42). There were also no significant differences between black and white patients in completion rates of the QoLI or in change in QoLI from pre to post.
Changes in Quality of Life Inventory scores.

Patient acceptability and comprehension of treatment
A total of 94 patients of the 299 completed the TST-I-CBT rating form. As displayed in Table 4, these patients generally displayed knowledge about CBT skills at the end of treatment. There was no significant difference in knowledge or satisfaction between those who received care from a provider who was in-person or via telehealth. These patients also rated TST as helpful, understandable, and useful, with mean scores ranging from 9.08 to 9.75 (out of 10). There was no significant difference between the in-person and telehealth groups in ratings of how helpful, understandable, or useful the material was.
Participant knowledge and feedback scores.
Discussion
Principal findings
The present project was a program evaluation of the impact on patient acceptability of the transition to remote provider in the group-based delivery of Transcending Self Therapy compared to its traditional in-person clinician format, as well as an evaluation of veteran impressions and potential impact of TST-I-CBT itself in a more recent patient sample. Consistent with our hypothesis, at a group level, individuals participating in treatment who had available scores demonstrated significantly improved QOLI T-scores from pre- to post-treatment generally. When comparing the provision of treatment by a therapist in-person with a remote therapist, there was no significant difference in change in score pre-to-post treatment in QOLI scores. Due to the small sample size of individuals with both pre- and post-scores in the telehealth group, these results should be interpreted with caution. Nonetheless, these results do suggest that it is possible to successfully administer CBT treatment for SUDs to a face-to-face patient group in a residential setting using a therapist who is located remotely. Additionally, the participants demonstrated a knowledge of CBT skills at the end of treatment, and rated TST as helpful, understandable, and useful per patient satisfaction survey results. These current findings when coupled with results from previous studies investigating the use of this type of therapy in this population and setting, both with individuals and with groups, demonstrate the potential versatility in application of TST, and also its acceptability in this population.
The patients of this program analysis found TST-I-CBT to be helpful, understandable, and useful, consistent with previous findings.26,28,29 It is also noteworthy that no patients in either group used illicit drugs or alcohol while in treatment, as evidenced by the absence of any (unexpected) positive urine drug screen or endorsement of having used drugs during the treatment period. A previous program evaluation of Group TST-I-CBT versus treatment as usual (TAU) in the same setting found that Group TST-I-CBT clients had fewer positive urine samples during treatment and within one-month post-discharge compared to TAU, as well as significantly improved QOLI T-scores from pre- to post-treatment, and better CBT mastery at the end of treatment. 26 The current and previous program evaluations also demonstrate that it is possible to develop an evidence-based integrative CBT for SUDs with an “open group” modular rolling format that is well suited for residential care. Under this format, each patient can begin treatment at different times than others with whom they are in treatment yet still attain the same skills across their residential stay. Most importantly, the current findings both bolster previous findings regarding the use of TST in the population, while providing preliminary evidence that rolling-admission group therapy can be used effectively in a telehealth format as well.
This natural experiment was a consequence of the drastic increase (e.g., 20-fold 30 ) in uptake of telemedicine overall among medical providers, where daily tele-mental health encounters via videoconferencing within the VA increased from 1739 on March 11, 2020 to 11 406 on April 22, 2020 (556% increase), with 114 714 patients seen via telehealth and 77.5% first-time users; telephone appts also saw substantial growth (442% increase). 20 That patients in our sample generally improved regardless of the treatment modality (in-person vs remote provider) reflects previous findings that for the most common modalities of telehealth services (i.e., video, phone) delivered for physical and mental health issues since the start of pandemic, responses from a large number of Veterans generally demonstrated telehealth’s acceptability, feasibility, and improved rate of patient retention, with other outcomes similar to in-person services.31,32
Previous studies have noted, however, the potential limitations of the provision of telehealth treatment in patients with SUDs. A review of randomized controlled trials investigating the effectiveness of telehealth for SUDs in papers published between January 2015 and August 2021 found that evidence is “very uncertain” that telehealth is similar to in-person care for SUD outcomes. 33 In one recent study investigating the use of telehealth among individuals with SUD, the majority of individuals were satisfied with the quality of telehealth care in the context of individual therapy, but fewer were satisfied with group therapy in this format. 34 However, compared to group therapy in person, participants were more satisfied with group therapy in a telehealth format. One concern patients who received group therapy noted in that previous study was feeling less able to connect with the therapist as well as other group members via telehealth or the potential to be interrupted by a family member when in the home. 34 It is important to note that these concerns were not applicable in the current study because group members were located in the treatment facility together with one another, preventing them from interruption in the home and ensuring they are able to connect with one another.
Limitations
There are several limitations to the present study. First, the sample size was small, and was limited to veterans in residential treatment at a single VAMC in the Mid-Atlantic Region. These features may potentially limit the power, generalizability or reproducibility of study findings. The rapid provision of telehealth treatment necessitated by the COVID-19 pandemic likely resulted in inconsistency in staffing, to impair rates of intakes as new procedures were established. A larger sample size admitted across the time period of pandemic distancing may have enabled detection of treatment modality differences in QOLI improvement or in TST-I-CBT perceptions, though such differences would likely have modest effect sizes. Despite this limitation, this overall sample size is larger than that of previous evaluations 31 and provides additional support for the use of Group TST-I-CBT. For example, the hybrid remote therapy may not be as acceptable or effective in more unsupervised group contexts or outside of structured, recovery-focused facilities. Nevertheless, given the previous studies investigating the use of this treatment in the same VAMC, this appeared to be an appropriate initial population for evaluation of Group TST-I-CBT provided in person and via telehealth.
Regarding generalizability, it may be worthwhile to consider the context of residential treatment in the time of the pandemic. Residential treatment offers an insulated, consistent, safe community of care, which, more often than not, is a setting not replicated in the personal lives of the patients being seen in the program, many of whom face housing instability. In non-pandemic times, discharge may be a hopeful occasion to anticipate, but discharge into the world during a pandemic may not be as celebratory an occasion. As previously stated, it is possible that the COVID-19 pandemic may have impacted the quality of life of participants at the time, which is consistent with trends in mental health noted among more vulnerable populations, like those with SUDs, during the pandemic. Given the paucity of data, this difference may not have been adequately reflected.
Second, this program evaluation was completely observational, and relied upon available clinical information. Consequently, clients were not randomly assigned to treatment groups (in person vs telehealth). However, the groups were similar demographically and in the distribution of different SUD diagnoses, though patients in the telehealth group were more likely to have received VA treatment between intake and admission to the residential program. Third, the data available were limited to what is typically seen in retrospective analyses of standard of care, and so we did not prospectively collect metrics of feasibility as traditionally understood in frameworks of implementation research. 35 Future prospective studies of telehealth-delivered TST-I-CBT could include both feasibility metrics and a broader array of outcome assessments. A related limitation to be noted is that, unfortunately, there was a marked discrepancy in the amount of available data for the in-person groups as compared with the telehealth groups. Finally, we note that only a minority of patients completed their exit rating forms about TST-I-CBT. It may be that the subpopulation of patients who took the time to respond may have been skewed toward patients who perceived the program favorably.
Conclusions and Future Directions
The use of telehealth for the treatment of SUD has exploded in recent years, out of necessity for continuity of treatment in the face of a global pandemic and to improve accessibility, such as for rural patients. It is therefore important for clinicians and researchers alike to investigate its provision. This program evaluation utilized real world clinical data to determine the patient acceptability of remote provider-administered Group TST-ICBT among veterans receiving residential SUD treatment. Key findings were that regardless of treatment modality, patients demonstrated CBT knowledge, and rated the treatment approach as helpful, understandable, and useful, and also reported significantly higher quality of life scores from before to after treatment. Our results provide preliminary evidence supporting the potential effectiveness of Group TST-I-CBT to enhance geographically remote or underserved SUD treatment programs. Future investigations into Group TST-I-CBT for the treatment of SUDs could include a formal RCT and implementation at multiple sites and as part of different types of treatment programs (e.g., in-person, remote/virtual).
As the present study builds on previous evidence of the potential effectiveness of Group TST-I-CBT for treating SUDs in a sample of veterans, a formal randomized controlled trial (RCT) of Group TST-I-CBT may be warranted. An RCT design that makes use of a larger sample with randomized provision of rolling group treatment via telehealth with an equal in-person comparator would be ideal. An RCT would allow for uniform data collection, and a greater array of outcome variables beyond instruments used as standard of care. Additionally, incentivized brief exit interviews could assess the subjective experience of a greater portion of patients in receiving either in-person or telehealth treatment. This in turn would inform the development of a treatment protocol for telehealth Group TST-I-CBT with necessary modifications if needed. Finally, to fully reflect the reality of providing these services remotely, multisite trials can be developed, wherein the treatment is provided by an outside provider to patients in a residential program elsewhere, which could have wide ranging implications for the implementation of evidence-based treatment within the VAMC health system nationally.
Supplemental Material
sj-docx-1-sat-10.1177_29768357241255437 – Supplemental material for Virtual Hybrid Versus In-Person Administration of Transcending Self Therapy for Veterans with Substance Use Disorders
Supplemental material, sj-docx-1-sat-10.1177_29768357241255437 for Virtual Hybrid Versus In-Person Administration of Transcending Self Therapy for Veterans with Substance Use Disorders by James M. Bjork, Jaclyn S. Sadicario, Nabila F. Jahan, Espn Curiel, Lillia Thumma and Jarrod Reisweber in Substance Abuse: Research and Treatment
Footnotes
Author Contributions
JMB co-wrote the article and oversaw manuscript edits. JSS co-wrote the article and performed statistical analyses, NJ performed statistical analyses. LT and EC performed literature review, and JR designed the TST therapy and formulated the hypotheses.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
Dr. Jarrod Reisweber has the potential to receive future royalties from the sales of Transcending Self Therapy. The author(s) declared no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.