
Abstract
Objectives:
Substance Use Disorders (SUDs) are increasingly prevalent among Veterans. Effective interventions for SUDs that also meet the clinical reality of open treatment groups are needed. Transcending Self Therapy: Group Integrative Cognitive Behavioral Treatment (Group TST-I-CBT) was developed to address this need. Group TST-I-CBT is a four-module, 20-session treatment designed so that a person can enter at any point in the treatment. We conducted a program evaluation of Group TST-I-CBT for veterans with SUDs.
Methods:
Participants were N = 68 veterans enrolled in the 28-day Substance Abuse Residential Rehabilitation Treatment Program at an urban Veterans Administration Medical Center who received either Group TST-I-CBT (N = 34) or treatment-as-usual (TAU; N = 34). Medical records were reviewed and participant treatment outcome data was retrieved. Group TST-I-CBT clients completed a knowledge and feedback form at treatment completion.
Results:
Compared to TAU participants, Group TST-I-CBT participants were significantly less likely to have a positive urine drug screen (UDS) during treatment (17.6% versus 0%; P = .01) and within one month post-discharge (50% versus 17.6%; P = .04). Among Group TST-I-CBT clients, Quality of Life Inventory scores significantly increased by an average of 14 points from pre- to post-treatment, t(15) = –3.31, P = .005, d = 0.83. Group TST-I-CBT clients displayed cognitive-behavioral therapy knowledge (mean correct answers ranged from 92%-100%) and rated Group TST-I-CBT as helpful, understandable, and useful (mean scores ranged from 9.3-9.6 out of 10).
Conclusions:
These preliminary data indicate that Group TST-I-CBT may be an effective group therapy as part of SUD treatment. A formal randomized controlled trial of Group TST-I-CBT may be warranted.
Keywords
Introduction
Effective interventions targeting Substance Use Disorders (SUDs) among veterans are desperately needed. Substance misuse is a serious public health concern, with 20.3 million Americans 12 years and older meeting criteria for a SUD. 1 Veterans are particularly vulnerable to developing certain SUDs (eg, Alcohol Use Disorder) compared to the general population, and 17.1% of veterans meet criteria for a past-year SUD.2-5 Lifetime SUD rates among veterans range as high as 39.2% for alcohol use and 5.7% for drug use in Vietnam veterans. 6 Veterans also have lower physical and mental health functioning than nonveterans. 5 This is especially concerning as SUDs are associated with substantial psychosocial and health consequences as well as increased psychiatric comorbidity.7,8
One of the major struggles in mental health has been in bringing scientific research to clinical practice.9,10 The gap between the two was originally considered mono-directional, from research to practice, and clinical practitioners were seen as being resistant to change. 11 There was a predictable backlash from practitioners insisting that clinical researchers needed to learn from frontline clinicians, and eventually a bidirectional relationship was proposed, with science and clinical practice each informing the other. 12
Bridging the gap between science and clinical practice has been particularly difficult in the area of SUD treatment.13,14 Effective treatments for SUDs are of critical importance, but only a minority of individuals in need of addiction services receive any or adequate treatment.15,16 Many SUDs clinicians use treatment approaches that have not demonstrated effectiveness.17,18 Even if they have, that does not mean that these evidence-based treatments (EBTs) are being implemented in the manner in which they were designed. It is common for community-based treatment organizations to modify SUD EBTs to fit their setting, even though there are no guidelines for doing so. 19 For example, Motivational Interviewing, one of the most widely studied EBTs for SUDs, has been implemented with a wide range of effectiveness in community settings. 20 Such modifications call into question their effectiveness.
Some EBTs such as Motivational Enhancement Therapy 21 are usually delivered in individual psychotherapy, while others such as Motivational Interviewing,22,23 12 Step Facilitation Therapy,24,25 and Cognitive-Behavioral Therapy for Substance Use Disorders (CBT-SUD)26,27 have both individual and group formats. The Veterans Health Administration (VHA) has successfully implemented individual CBT-SUD by including elements of Motivational Interviewing and providing clinicians with both an initial training and six months of weekly group supervision to ensure that the treatment is implemented as designed. 28 Most residential treatment centers (RTCs) and intensive outpatient programs (IOPs) for SUDs are based primarily on group therapies, partly stemming from a belief that group therapies are more effective in people suffering from addictions, 29 partly because of high demand in Veterans, and partly because it is less expensive to provide the same treatment to multiple individuals at the same time. The group versions of CBT-SUD, 12 Step Facilitation, and Motivational Interviewing are sequential; that is, each lesson or group of lessons build on the ones before them. These EBTs were designed, tested, and demonstrated to be effective when lessons or phases of treatment are delivered in order.
The problem is that SUD group treatment is typically not provided in its intended sequential order, regardless of whether treatment is conducted in a weekly outpatient, intensive outpatient, or residential setting. This is partly due to the need to “strike while the iron is hot,” when a client is most motivated to engage in treatment. However, it is also driven by a financial imperative and high demand for SUD treatment: RTCs need to fill beds each time one opens; IOPs need to fill desks; and weekly outpatient groups need to fill their slots as well. These groups are open groups, not cohorts in which all participants start and finish at the same time. The combination of these two factors mean that group SUDs EBTs are frequently not delivered as designed. Those who start later in the sequence lack the building blocks to use the skills and tools of later lessons. The mixture of timings when different clients start a group EBT may compromise treatment integrity, making that treatment potentially no longer evidence-based for a significant proportion of the participants in the group. 30 There has been one recent attempt to create a rolling admissions group version of an EBT. That trial used an open enrollment version of Mindfulness-Based Relapse Prevention (MBRP). 31 However, MBRP is designed as a substance misuse treatment aftercare program, not an initial treatment program. 32
Transcending Self Therapy: Group Integrative Cognitive Behavioral Treatment (Group TST-I-CBT) was developed to solve this problem. 33 It arose from a dialog between science (CBT for SUDs) and the clinical reality of open SUDs treatment groups, which are common in the VHA despite the implementation of individual CBT-SUD. TST-I-CBT is a manualized integrative, holistic Cognitive-Behavioral Therapy,34,35 incorporating elements of Interpersonal Therapy, 36 Motivational Interviewing, 22 Self Psychology, 37 and Acceptance and Commitment Therapy. 38 TST-I-CBT is based on a biopsychosocial-spiritual model that posits the centrality of a person’s need to live a meaningful life in accordance with one’s values. 33 TST-I-CBT adheres to a client-centered perspective and acknowledges the need to better connect to others and develop a passionate pursuit that is in line with one’s moral compass and/or spiritual beliefs. The TST-I-CBT model itself is not spiritual, it simply operates in a culturally sensitive way to acknowledge the spiritual or moral beliefs of clients (similar to Pearce et al. 39 ). Incorporating discussions of spirituality when clinically indicated is perceived by clients to be appropriate and helpful. 40
One of the first versions of TST-I-CBT was Transcending Self Therapy: Four-Session Individual Integrative Cognitive Behavioral Treatment (Individual TST-I-CBT). 41 Individual TST-I-CBT was designed to be provided weekly as part of group-based intensive SUD treatment programs. A pilot randomized clinical trial found that Individual TST-I-CBT participants were twice as likely to complete treatment and to be abstinent in the final week of treatment compared to TAU participants. 42 Individual TST-I-CBT clients showed significant reductions in depression over time, while TAU clients did not. Compared to the TAU group, the Individual TST-I-CBT group also showed trends toward being less likely to transition to a higher level of SUD care and for quality of life scores to increase more over time. 42 The success of Individual TST-I-CBT, the use of treatment groups as the primary treatment modality for SUDs, and the problem of the lack of fit between design and implementation of SUDs group therapy, particularly in IOPs and RTCs, spurred the development of Group TST-I-CBT, which is a different and much-expanded version of TST-I-CBT.
This investigation was designed to collect preliminary evidence regarding the effectiveness of Group TST-I-CBT for clients with SUDs. It was conducted to help inform SUDs treatment programming in a Veterans Administration Medical Center (VAMC) and other VAMCs as well. Based on prior results from Individual TST-I-CBT, 42 we hypothesized that: Group TST-I-CBT participants would be more likely to complete treatment as well as have fewer positive urine drug screens (UDSs) during treatment and within one-month post-discharge than TAU participants; Group TST-I-CBT participants would show significant gains in quality of life from pre- to post-treatment; and Group TST-I-CBT participants would show substantial knowledge acquisition about the treatment and find Group TST-I-CBT to be helpful, understandable, and useful.
Methods
Participants
Participants were N = 68 veterans with SUDs who received substance misuse treatment at the Hunter Holmes McGuire VA Medical Center in Richmond, Virginia. They were enrolled in the Substance Abuse Residential Rehabilitation Treatment Program (SARRTP), a 28-day residential treatment program for veterans with SUDs that includes group psychotherapy, individual case management, peer recovery support, spirituality groups, 12-step facilitation, vocational therapy, occupational therapy, and pharmacotherapy. Participants received either Group TST-I-CBT (N = 34) or treatment-as-usual group therapy (TAU; N = 34) as part of SARRTP treatment. Approximately 5% of SARRTP clients are mandated to treatment (C. Paul, email communication, April 2020). As a result, both treatment groups included those who were mandated to treatment and those who participated voluntarily. There were no changes to the referral process and thus no expectation of differences in referrals between groups.
Procedures
An IRB waiver was sought and granted because Group TST-I-CBT was developed and implemented as a SUDs treatment program improvement pilot. Clients were not randomized into treatment groups as they received the group therapy (Group TST-I-CBT or TAU) offered at the time they were enrolled in residential treatment. All data used for this project were collected as part of standard care. Medical records were reviewed for all participants in the two treatment groups. Information collected from these records included the following: demographic information, UDS results, Quality of Life Inventory (QOLI) scores, and treatment completion status. For both therapy groups, sessions were approximately 50 minutes long and were conducted by one to two providers per session at 9 am, Monday through Friday. The same SARRTP Coordinator oversaw both the TAU group and the Group TST-I-CBT group. Accordingly, the same philosophy governed the response to use while in treatment for both groups, which was to proceed as clinically indicated using relapse sensitive care.
Intervention group
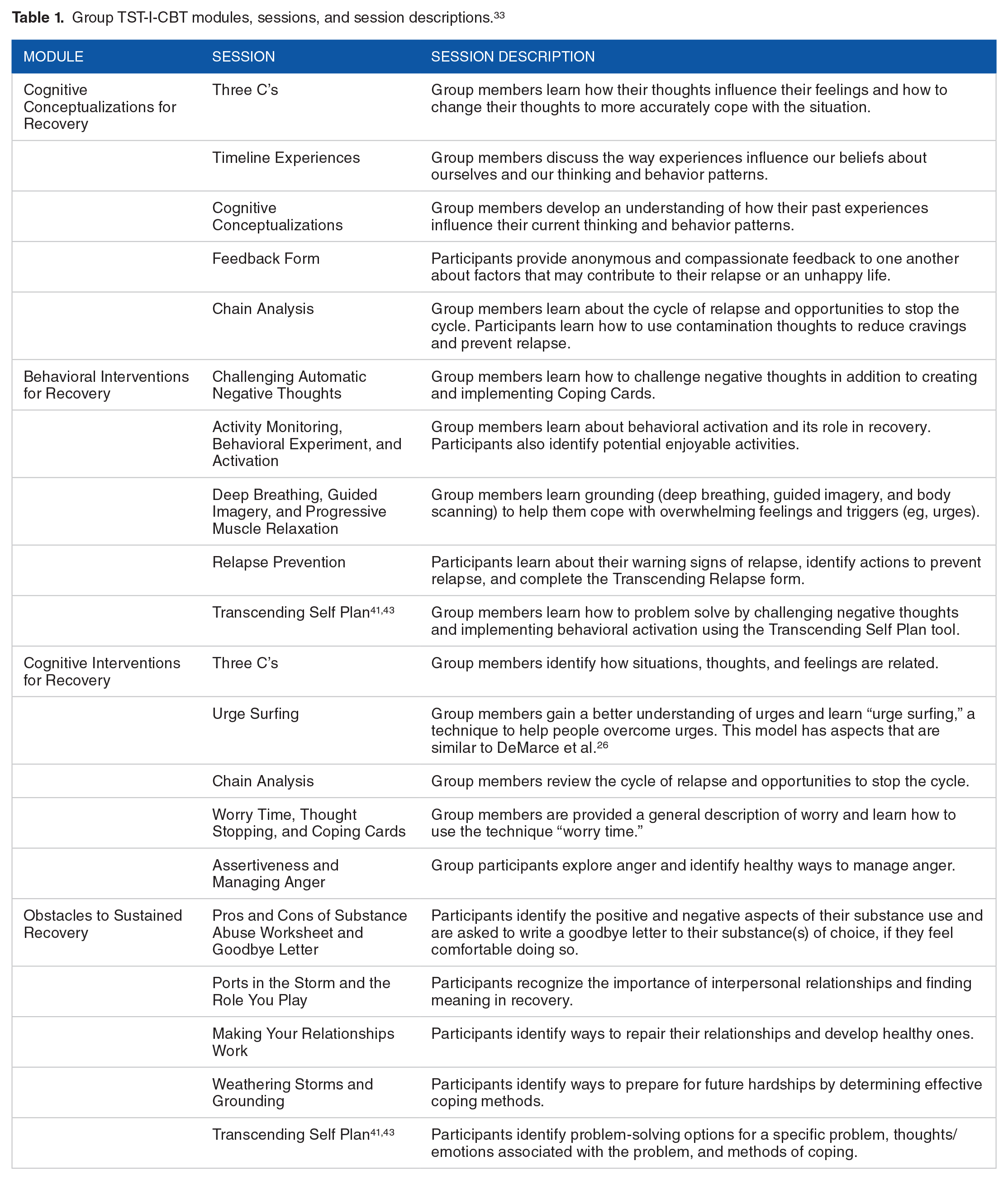
The structure of Group TST-I-CBT is modular with an “open” group (or “rolling admission”) format, allowing participants to join the group at any point during the protocol. No lesson requires any knowledge from the previous lesson. The combination of subject repetition, mirroring of concepts across treatment modules, and having newer participants taught some concepts by clients who have been in the treatment longer is designed to provide each client the same overall treatment experience regardless of which lesson is their first. Group TST-I-CBT sessions begin by asking group members the following two questions: “What do you remember from our last session?” and “What is the cognitive-behavioral therapy model?” These questions help to reinforce previously learned concepts and skills and introduce new members to important concepts while modeling a sincere investment in the process. Group TST-I-CBT participants who have been in treatment for longer are frequently called upon to describe behaviors and reactions from a CBT vantage point. These participants are encouraged to make themselves available to help newer participants with home practice of concepts and skills, which is assigned at the end of each session.
As detailed in Table 1, there are four modules in Group TST-I-CBT, each containing five one-hour sessions for a total of 20 sessions provided over a four-week period. In addition to the structured content at each session, Group TST-I-CBT involves in-the-moment processing of interactions and dynamics while utilizing CBT constructs. For example, clients are frequently asked to process their hot cognitions as they arise in session. Participants apply CBT in real time and when they do so incorrectly, the facilitator intervenes to show them the errors in the application of CBT and how to overcome said errors.
Group TST-I-CBT modules, sessions, and session descriptions. 33
Group TST-I-CBT participants were provided with a client manual and groups were conducted by therapists who practiced in accordance with what is outlined in the facilitators book. TST-I-CBT providers consulted with or were supervised by Dr. Reisweber (Group TST-I-CBT co-developer) and all received a score of “Meets Expectations” or higher on their biannual clinical evaluations. Group TST-I-CBT sessions were facilitated by licensed clinical social workers, a licensed clinical psychologist, psychology interns, and psychology externs.
After the last session of Group TST-I-CBT, participants were asked to complete an optional knowledge and feedback form. The purpose of the form was to assess group comprehension and provide feedback on the provision of Group TST-I-CBT. Participants were instructed not to write identifying information (eg, name) on the form, and to return completed forms to their social worker prior to discharge. Responses to anonymous forms were entered into a spreadsheet for aggregate data analysis.
Comparison group
We selected a comparison group of veterans, referred to as the TAU group, who did not have Group TST-I-CBT yet otherwise received almost identical care to the Group TST-I-CBT participants. The TAU participants were chosen for being the most recent veterans enrolled in SARRTP who did not receive Group TST-I-CBT. The TAU group received treatment prior to the arrival of the invention of Group TST-I-CBT, and thus had no exposure to the Group TST-I-CBT protocol. Whereas Group TST-I-CBT was designed to be an open group, the TAU group was an open group as a function of the fact that all groups in SARRTP have to be open groups (as is typical of “real-world” treatment programs); the TAU group was not specifically designed for open enrollment. Instead of receiving Group TST-I-CBT, TAU clients received a non-manualized psychoeducational group that consisted of reading from handouts covering various topics (eg, CBT concepts, such as identifying and challenging maladaptive thoughts and behaviors; coping skills; and communication patterns), followed by group discussion. Similar to the Group TST-I-CBT group, TAU sessions were facilitated by licensed clinical social workers, a licensed clinical psychologist, as well as psychology and social work trainees. Aside from the change in the provision of Group TST-I-CBT, there were no other significant staffing or treatment changes for Group TST-I-CBT and TAU participants in SARRTP. The only notable programmatic change was that TAU participants were more frequently allowed the option to obtain weekend passes, whereas Group TST-I-CBT participants were less likely to obtain weekend passes.
Measures
Demographics
Participants’ self-reported race/ethnicity, age, and sex were collected from their medical records.
Urine drug screen (UDS)
Results of UDSs collected during treatment and within one month post-discharge were reviewed. UDSs were collected as part of standard care for Aftercare, other SUD treatment, and/or through primary care and the Emergency Department. Positive UDS results included any measure exceeding standard thresholds for drug concentrations or exceeding standard detection time given the date of intake.44,45 For example, a UDS indicating the presence of cocaine within 24 hours of entry to treatment was not considered a positive UDS. However, if a UDS indicated the presence of cocaine 10 days after entry into residential treatment, it was coded as a positive UDS given that the standard detection time for cocaine metabolites is two to four days. 44 Positive UDS results were then assessed for possible false positives; for example, the antidepressant sertraline can produce a false positive for benzodiazepines.46,47 Prescribed medication for SUDs and other conditions was also accounted for in the drug screening process.
Quality of life inventory
The Quality of Life Inventory (QOLI) is a 32-item measure of life satisfaction and well-being across 16 domains (reliability = 0.80).48,49 Group TST-I-CBT participants were administered the QOLI at intake and upon discharge from SARRTP. QOLIs were not administered to the TAU group. Responses to the QOLI were entered into Mental Health Assistant, a program used by the VA system of care to facilitate administration and scoring of assessment measures. The score reports are automatically generated following the guidelines recommended by the test publisher. 49 The score report includes a weighted life-satisfaction T-score, which is derived by multiplying the raw score within each domain by the relative importance of each domain. The weighted scores are then standardized using normative data provided by the publisher. A T-score of 50 is considered average, and 40 to 60 is considered within normal range.
Treatment retention
Participants’ SARRTP completion status (completed or not completed) was retrieved from their medical records.
Knowledge and feedback form
After their last session, Group TST-I-CBT participants were asked to complete an anonymous knowledge and feedback form. Completion of this form was voluntary. The questions assessed their level of comprehension of the Group TST-I-CBT material and how useful, understandable, and helpful they found various aspects of treatment.
Data analysis plan
Chi-square analyses and independent t-tests were used to determine if differences existed for demographic characteristics, SARRTP treatment completion, and UDS data between the two treatment groups. A paired t-test was used to compare QOLI T-scores pre- to post-treatment for Group TST-I-CBT participants. Descriptive statistics were used to examine Group TST-I-CBT participant knowledge and feedback. All analyses were carried out using SPSS version 24. Individuals with missing information were excluded from analyses involving that specific item.
Results
Sample demographics and types of SUDs at intake
As shown in Table 2, the sample was almost all male (86.8%), roughly half African American (51.5%) and half Caucasian (45.6%). The mean age was 48.9 years (SD = 13.9).
Client demographic characteristics and types of SUDs at intake (N = 68).

Only n = 5 participants met criteria for an other Substance Use Disorder.
At intake, the sample predominantly met criteria for Alcohol Use Disorder (72.1%), followed by Stimulant Use Disorder (50%), Opioid Use Disorder (35.3%), Cannabis Use Disorder (25%), and Other Use Disorder (7.4%). No significant differences were found between groups for demographic or type of SUD variables. However, TAU clients showed trends toward being more likely to have an Alcohol Use Disorder (82.4% versus 61.8%; P = .06) and Cannabis Use Disorder (35.3% versus 14.7%; P = .05) at intake compared to Group TST-I-CBT participants.
Substance use and treatment outcomes
As shown in Table 3, compared to TAU participants, Group TST-I-CBT participants were significantly less likely to have a positive UDS during treatment (17.6% versus 0%; P = .01) and within one month post-discharge (50% versus 17.6%; P = .04). No difference in residential treatment retention was found between groups. Among Group TST-I-CBT clients, QOLI T-scores significantly increased by an average of 14 points from pre- to post-treatment, t(15) = –3.31, P = .005, d = 0.83.
Substance use and treatment variables by treatment group.

P < .05.
P ⩽ .01.
33 clients (n = 17 Group TST-I CBT participants and n = 16 TAU participants) did not provide a UDS within one month post-discharge.
Group TST-I-CBT knowledge and feedback
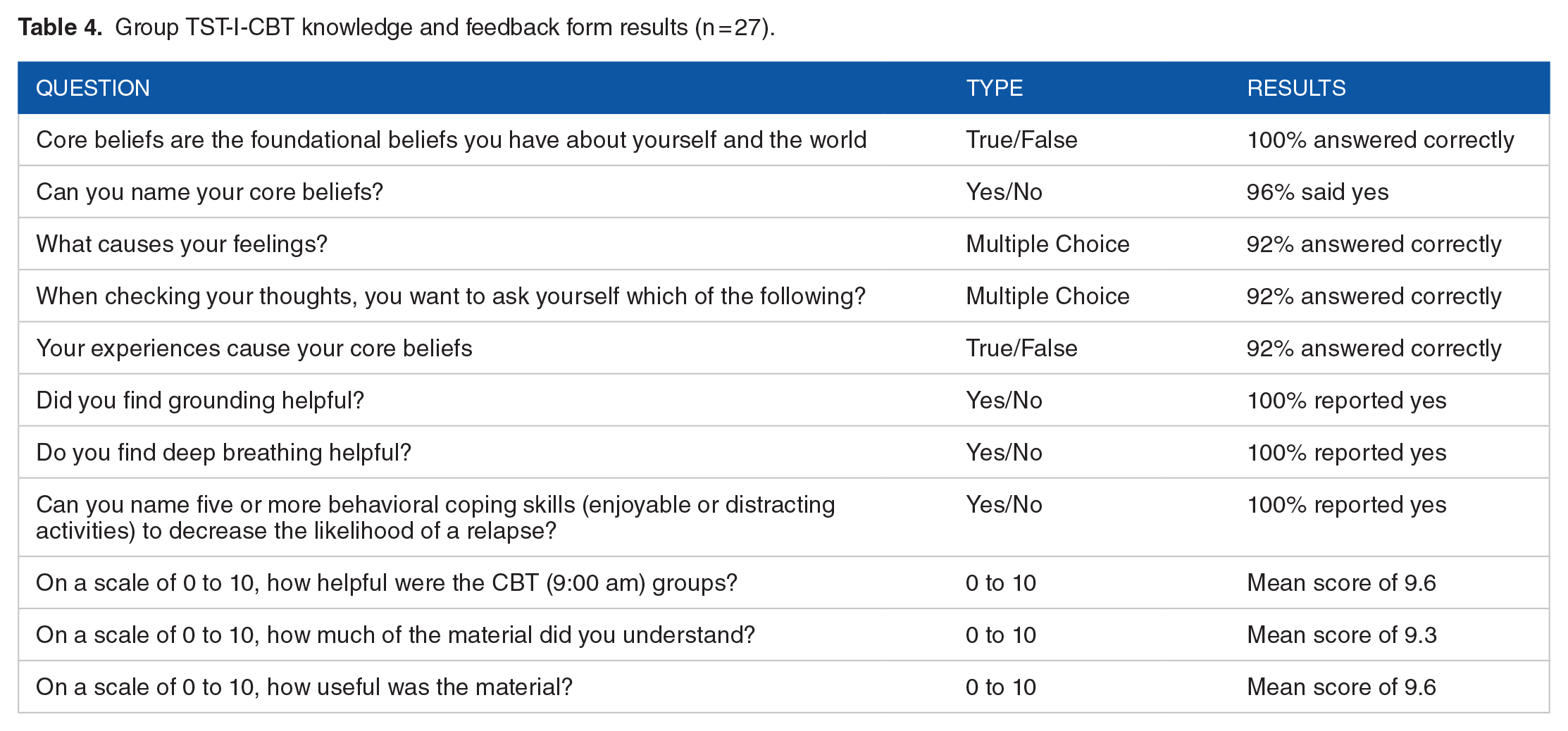
As displayed in Table 4, Group TST-I-CBT clients displayed knowledge about CBT skills at the end of treatment, with mean correct answers across items ranging from 92% to 100%. These clients also rated Group TST-I-CBT as helpful, understandable, and useful, with mean scores ranging from 9.3 to 9.6 (out of 10). A total of 27 of 34 clients (79.4%) provided answers to the questions. Clients who did not complete the form either declined or did not have time to complete the form at the end of group.
Group TST-I-CBT knowledge and feedback form results (n = 27).
Discussion
Principal findings
The present project was a program evaluation of Transcending Self Therapy: Group Integrative Cognitive Behavioral Treatment (Group TST-I-CBT). 33 Consistent with our hypothesis, Group TST-I-CBT clients were more likely to have fewer positive UDSs during treatment and within one month post-discharge compared to TAU clients. Group TST-I-CBT clients reported significantly improved QOLI T-scores from pre- to post-treatment. Additionally, Group TST-I-CBT clients displayed CBT knowledge at the end of treatment and found Group TST-I-CBT to be helpful, understandable, and useful. These results suggest that it is possible to develop an evidence-based modular integrative CBT treatment for SUDs with an “open group” format that is effective in a residential setting, the first one of which we are aware. Group TST-I-CBT treatment can be provided in a manner that is consistent with real-world settings in which SUDs clients begin treatment at different times than others with whom they are in treatment.
The current findings are similar to results from a previous clinical trial of Individual TST-I-CBT treatment. 42 Findings from that investigation showed that Individual TST-I-CBT clients were more likely to have reductions in substance use, decreases in depression, and trend-level increases in QOLI T-scores compared to TAU clients in a SUDs Intensive Outpatient Program. 42 Our current findings, combined with those from the previous study, suggest TST-I-CBT is potentially an effective treatment for SUD. These results provide further support for the continued application and investigation of TST-I-CBT as part of VAMC treatment. Our findings also provide support for investigation of TST-I-CBT treatment effectiveness in other settings and with other SUDs populations.
However, unlike the previous investigation of Individual TST-I-CBT, we found no difference between groups for treatment retention. It was previously found that Individual TST-I-CBT clients were twice as likely as the TAU group to complete treatment. 42 One possible reason for this inconsistency is that Individual TST-I-CBT study participants were enrolled in an intensive outpatient treatment program while the current project focused on clients in residential treatment. Retention rates are higher in inpatient SUD treatment programs than outpatient programs, 50 possibly as a result of barriers to treatment (eg, transportation) that are eliminated by residential treatment. 51 Another possible is that the individualized attention provided by the Individual TST-I-CBT format was the key factor in increasing treatment retention.
There are several possible reasons why TST-I-CBT was effective. We believe that the theoretical foundation of integrative-CBT, the adherence to the biopsychosocial-spiritual model, and the modular format in which a person can begin treatment at any point in the treatment sequence and receive the same therapeutic benefits are possibly critical elements explaining the potential effectiveness of TST-I-CBT. Consistent with our belief that the CBT component of Group TST-I-CBT is a likely reason why it was effective is the recent finding by DeMarce and colleagues 28 that large-scale training and implementation of individual CBT-SUD in the VA was linked with improvements in substance use and other outcomes (eg, quality of life).
In accordance with the biopsychosocial-spiritual model, TST-I-CBT therapists view their clients as needing to seek meaning and develop a lifestyle and sense of self that is in line with their moral compass. This appears to be a powerful process that promotes recovery. For some clients, this process includes discussions of spiritual beliefs. Discussing spirituality when clinically indicated is supported by the findings of Martinez, Smith, and Barlow 40 that clients appreciate these discussions. TST-I-CBT therapists also process their clients’ hot (emotional) cognitions 52 as they arise in session. This may help to facilitate the identification and adjustment of maladaptive thinking and behavior patterns that restrict their ability to connect to others and develop a more meaningful lifestyle or occupation.
We believe the open group design is possibly central to the effectiveness of Group TST-I-CBT as it accommodates the reality of rolling admissions SUD treatment programs. Group TST-I-CBT allows for clients to receive the same therapeutic benefit regardless of starting session because the model does not require prerequisite knowledge at any session. Furthermore, the modular format was designed so that clients who have been in treatment longer can relay knowledge to newer clients. This may help to maintain the positive therapeutic benefits for all group members. Our belief in the importance of open SUD groups is consistent with a recent finding by Roos and colleagues 31 who conducted a non-randomized open trial of rolling admission MBRP in residential SUD treatment. While total sessions attended did not predict end-of-treatment outcomes, attending at least two sessions predicted better mental health and higher mindfulness. 31 Furthermore, when sequential group therapies are implemented in treatment programs that require open groups, participants that start in the middle of the sequence miss the information and skills from earlier sessions. These participants therefore cannot benefit from treatment the same way someone would who began treatment in the beginning of the sequence. Such changes compromise treatment integrity, potentially rendering treatment no longer evidence-based. 30 However, it should be noted that these possible reasons why TST-I-CBT was effective are hypotheses that should be explored in future research.
Limitations
There are several limitations to the present study. First, the sample was exclusively veterans at one VAMC in Virginia, potentially limiting the generalizability of study findings. Virginia is one of the most religious states in the United States. 53 This could have contributed to the success and acceptability of Group TST-I-CBT, which adheres to the biopsychosocial-spiritual model. 33 However, Group TST-I-CBT operates in a culturally sensitive way to acknowledge the need to better connect to others and develop a passionate pursuit that is in line with one’s moral compass and/or spiritual beliefs. 33 Accordingly, being religious does not necessarily mean someone is more likely to benefit from this model. Additionally, given both the increased rates of substance use and problems observed among veterans 2 and that Group TST-I-CBT was developed at a VAMC, this appeared to be an appropriate initial population for evaluation of Group TST-I-CBT.
Second, this was a program evaluation in which clients were not randomly assigned to treatment groups and the data available were exclusively collected as part of standard care. As a result, important differences between the two treatment groups could have potentially contributed to our findings. For example, we found trend-level differences between groups for prevalence of Alcohol Use Disorder and Cannabis Use Disorder at intake. Despite this limitation, this design was determined to be suitable for an initial evaluation of Group TST-I-CBT, though future randomized clinical trials would improve our understanding of the efficacy of this treatment.
Third, as this was a program evaluation, therapist fidelity was not formally assessed. However, all TST-I-CBT providers were supervised by or consulted with Dr. Reisweber (TST-I-CBT co-developer). These providers all received a designation of at least “Meets Expectations” on their biannual clinical evaluations.
Fourth, there were minor programmatic changes between the two treatment groups. The TAU group was more frequently allowed the option to obtain weekend passes, whereas Group TST-I-CBT clients obtained passes only under special circumstances. As a result, TAU clients who had more weekend passes were potentially more likely to have the opportunity to use substances and thus have a positive UDS during treatment. However, the likelihood of a positive UDS within one month after treatment concluded would not have been impacted by this policy. Additionally, both the QOLI and the knowledge and feedback form were administered only to Group TST-I-CBT clients, which eliminated the possibility of comparing results to the TAU group and raises the possibility that QOLI T-score changes were due to the full residential treatment program and not just the implementation of TST-I-CBT. Beyond those changes, there was remarkable consistency between the other areas of the SUDs residential treatment program for the two treatment groups.
Future research
As the present study provides preliminary evidence of the potential effectiveness of Group TST-I-CBT for treating SUDs in a small sample of veterans, a formal randomized controlled trial (RCT) of Group TST-I-CBT may be warranted. An RCT design would increase internal validity and a larger sample size would allow for subgroup analyses (eg, comparing treatment outcomes based on the starting session or module). This design would also allow for the collection of additional SUD treatment outcome variables, which would help in evaluating the effectiveness of Group TST-I-CBT. A randomized controlled dismantling study could be valuable for evaluating the contribution of each component of Group TST-I-CBT to the overall treatment. Lastly, to evaluate generalizability, future trials could include implementation at multiple sites and as part of different types of treatment programs with different populations.
Conclusion
Our investigation examined the effectiveness of Group TST-I-CBT among veterans receiving residential SUD treatment. Key findings were that, compared to the TAU group, Group TST-I-CBT clients were less likely to have a positive UDS during treatment (17.6% versus 0%) and within one month post-discharge (50% versus 17.6%). Group TST-I-CBT clients also reported significantly higher QOLI T-scores from pre- to post-treatment; demonstrated CBT knowledge; and rated Group TST-I-CBT as helpful, understandable, and useful. Our results provide preliminary evidence supporting the potential effectiveness of Group TST-I-CBT as part of SUD treatment programs. Future investigations into Group TST-I-CBT for the treatment of SUDs could include a formal RCT and implementation at multiple sites and as part of different types of treatment programs.
Footnotes
Acknowledgements
We would like to thank the staff of the Hunter Holmes McGuire Veterans Administration Medical Center Substance Abuse Treatment Program who contributed to the outcome of this study and manuscript.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a VA Innovators Network Spark Grant to Drs. Reisweber and Meyer.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jarrod Reisweber, Psy.D. and Brian Meyer, Ph.D. at times receive a percentage of the royalties from sales of Group Transcending Self Therapy books.
Author Contribution
JR and BM developed Group TST, conceived of the program evaluation project, and were in charge of overall direction and planning. ZN collected data for the project. KP performed the analyses and took the lead in writing the manuscript, with significant contributions to the writing from all authors. All authors provided critical feedback and helped shape the final version of the manuscript.