
Abstract
Background:
In the United States, methadone for opioid use disorder is limited to opioid treatment programs. Increased methadone access is necessary, and community pharmacies may be a logical option for expansion. The objectives of this study were to explore opioid treatment program (OTP) staff members’ perceptions of and anticipated barriers and facilitators to implementing pharmacy-based methadone dispensing via medication units.
Methods:
Participants in this study were purposively sampled from OTP staff in North Carolina who completed a previous quantitative survey on the perceived acceptability, appropriateness, and feasibility of pharmacy-based methadone dispensing and agreed to be contacted for an interview. Thematic analysis was conducted to identify salient and main themes, and relationships among and between themes, as well as areas of divergence.
Results:
OTP staff (n = 10) endorsed increased access and OTP-pharmacy collaboration as benefits of pharmacy-based methadone dispensing. OTP staff were concerned about community pharmacy stigma, the suitability of the pharmacy setting for methadone treatment, and loss of counseling and felt that lack of pharmacy interest would be a barrier to implementation. OTP staff identified 5 implementation facilitators, including OTP willingness and pharmacist capability to provide the service, telehealth, clear communication, and reimbursement.
Conclusion:
Results from this study demonstrate moderate interest from OTP staff towards pharmacy-based methadone dispensing. Researchers and other vested parties should consider conducting a pilot study to identify how best to implement medication units in the pharmacy setting.
Highlights
Despite concerns, opioid treatment program (OTP) staff see benefits to methadone access at pharmacies.
OTP staff anticipate pharmacists will be unwilling to dispense methadone.
OTP staff are willing to collaborate with pharmacies to increase methadone access.
Clear OTP-pharmacy communication may facilitate pharmacy-based methadone implementation.
Introduction
Non-prescribed opioid overdose deaths represent the majority of overdose deaths in North Carolina, with an estimated three-fourths being from non-prescribed opioid use in 2024. 1 Medications for opioid use disorder (MOUD), including methadone and buprenorphine, are used to treat opioid use disorder (OUD) and can decrease non-prescribed opioid use.2,3 Methadone, compared with no medication, reduces mortality and OUD hospitalizations, and has a lower risk of treatment discontinuation than buprenorphine.4-6
In the United States, methadone for OUD can only be provided at federally registered opioid treatment programs (OTPs) due to a Nixon-era law from over 50 years ago, which sought to regulate addiction treatment and which, despite many efforts at reform, has not been significantly updated.7,8 OTPs are nonresidential treatment facilities that provide methadone, counseling, and other services for people with OUD, of which there are 97 throughout North Carolina. 9 Although OTPs provide essential care to people with OUD, patients have reported experiencing stigma and difficulty with the restrictive dosing hours, take-home policies, and inaccessibility of OTPs.10-13
Multiple studies have found community pharmacies are more accessible for patients with OUD compared to OTPs.14-16 In addition, community pharmacies serve many patients with OUD, including those who are prescribed buprenorphine. However, pharmacists’ stigmatizing beliefs toward MOUD and people who use drugs limit access to buprenorphine in community pharmacies.17-19 Outside of the United States, pharmacists have observed dosing of and dispensed methadone for OUD for decades; yet, patients also report stigma and lack of privacy at these international pharmacies.20-23 Despite these barriers to pharmacy-based MOUD services, increased methadone access in the United States is necessary, 24 and the abundance of pharmacies in the United States, and North Carolina specifically, warrants exploring a pharmacy-based methadone-dispensing model. Two recent studies in the United States demonstrated the feasibility of community pharmacists to observe methadone dosing and dispense take-home doses25,26; additional research is needed to explore key informant perspectives on pharmacy-based methadone treatment.
There are several methods by which pharmacy-based methadone dispensing may be implemented in North Carolina. The first is proposed federal legislation, called the Modernizing Opioid Treatment Access (MOTA) Act, which would allow addiction medicine providers to prescribe methadone to be dispensed at the pharmacy for unsupervised use. 27 However, the American Association for the Treatment of Opioid Dependence (AATOD), which represents OTPs nationally, currently opposes this bill, and there has been little congressional movement on it since being introduced in 2023. 28 In addition to MOTA, recent changes to North Carolina state regulation created a pathway for community pharmacies to operate as medication units. 29 Medication units are geographically separate entities from OTPs that function as satellite sites and must comply with the same regulations as OTPs. Despite the possibility of pharmacy-based medication units, there is currently no state or federal guidance nor published research of which we are aware which provides logistical guidance for implementing a pharmacy-based medication unit.
Study Objectives
Given the lack of evidence on how to implement medication units in community pharmacies, research is needed to better understand perspectives from OTP staff who may be involved with implementing this model. Thus, the objectives of this study were to explore OTP staff members’ perceptions of and anticipated barriers and facilitators to implementing pharmacy-based methadone dispensing via medication units.
Methods
Ethics
The University of North Carolina at Chapel Hill Office of Human Research Ethics reviewed a protocol for this study and determined it exempt from further review (IRB #24-3111). All participants provided verbal consent to participate after reviewing an IRB-approved study fact sheet.
Study Design
This study is part of a larger mixed-methods project on key informant (community pharmacists, OTP staff, addiction medicine providers, and people with lived/living experience [PWLLE] of opioid use and/or OUD) perspectives toward expanding methadone access through community pharmacies in North Carolina. As part of the research, 4 advisory boards (clinical, policy, and 2 PWLLE) worked with researchers to inform research goals and assessment tools.
The qualitative dataset reported here is from a nested sample of participants identified through a larger survey sample. 30 The semi-structured interview guide focused on a pharmacy-based medication unit model and was developed to gain in-depth insights on survey findings (ie, interview participants were prompted to provide additional insights on the key perceived benefits, negative consequences, and barriers to methadone dispensing identified in the survey) as well as exploring potential implementation facilitators, which were not a focus of the survey. The interview guide can be found in Supplemental File 1.
Participants
Participants were purposively sampled from OTP staff (primarily program directors) in North Carolina who earlier completed a quantitative survey on the perceived acceptability, appropriateness, and feasibility of pharmacy-based methadone dispensing and agreed to be contacted for an interview. 30 The survey sample consisted primarily of OTP program directors, or another staff member who could speak to the OTPs’ program operations, upon recommendation from our clinical advisory board. For the interviews, we used survey responses to ensure sample representation from different geographic areas (rural/non-rural), and those with a range of attitudes (from very negative = 1 to very positive = 5) toward expanding methadone access through MOTA, as a proxy for general attitudes toward pharmacy-based methadone dispensing.
As a nested subset study intended to gain further insight from survey respondents, and with pragmatic considerations based on the study budget and timeline, 31 we sought to interview up to 10 OTP staff. Out of 24 survey participants who expressed interest in completing an interview, 22 prospective interview participants were contacted up to 4 times via email, 2 of whom no longer wanted to participate; 7 did not respond; and 3 of whom did not attend their interview and did not reschedule, resulting in 10 participants.
Data Collection
Prior to the start of data collection, 2 pilot interviews were conducted over Zoom with OTP staff located in other states, recruited with assistance from our clinical advisory board, to assess and refine the interview guide for clarity. Both interviewees understood the questions being asked, and no changes were made to the guide. Both pilot interviewees received a $75 gift card.
A research associate (M.A.N.), with a Master of Public Health degree and years of qualitative research experience, conducted all interviews. Interviews lasted from 28 to 68 minutes and were conducted and audio-recorded over Zoom from June to August 2025. Participants received a $75 gift card.
Data Analysis
The Consolidated Framework for Implementation Research (CFIR) (2009) was used to develop the codebook. 32 CFIR includes constructs related to Innovation Characteristics, Outer Setting, Inner Setting, Individual Characteristics, and Process that researchers can use to identify barriers and facilitators related to implementation outcomes. Three researchers (C.S., M.A.N., G.M.) reviewed and added relevant CFIR constructs to the codebook. Interview guide concepts unrelated to CFIR were also added to the codebook. The codebook can be found in Supplemental File 2.
Interviews were transcribed verbatim and de-identified using transcription software (https://www.3playmedia.com/) and uploaded to MAXQDA 2024 (VERBI Software, Berlin, Germany) for analysis. Two coders (M.A.N. and C.S.) coded 1 interview together, then coded 2 more transcripts independently and met to reach consensus. No inductive codes were added during the coding process. The remaining 7 transcripts were split between the coders and coded independently. Coders met to compare coding and reconcile any uncertainties. One researcher (C.S.) conducted thematic analysis, composing memos to summarize coded sections of transcripts and grouping sections of interviews with emerging thematic agreement together to observe overarching trends in agreement. This allowed the researcher to identify salient and main themes, and relationships among and between themes, as well as areas of divergence.
Results
Participant Characteristics
Table 1 describes the characteristics of participants and the OTPs at which they worked. All participants reported their OTPs are primarily Medicaid-funded. Nine participants described their role at the OTP as “program director,” while one participant was a “consultant.”
Participant (n = 10) and OTP Characteristics.
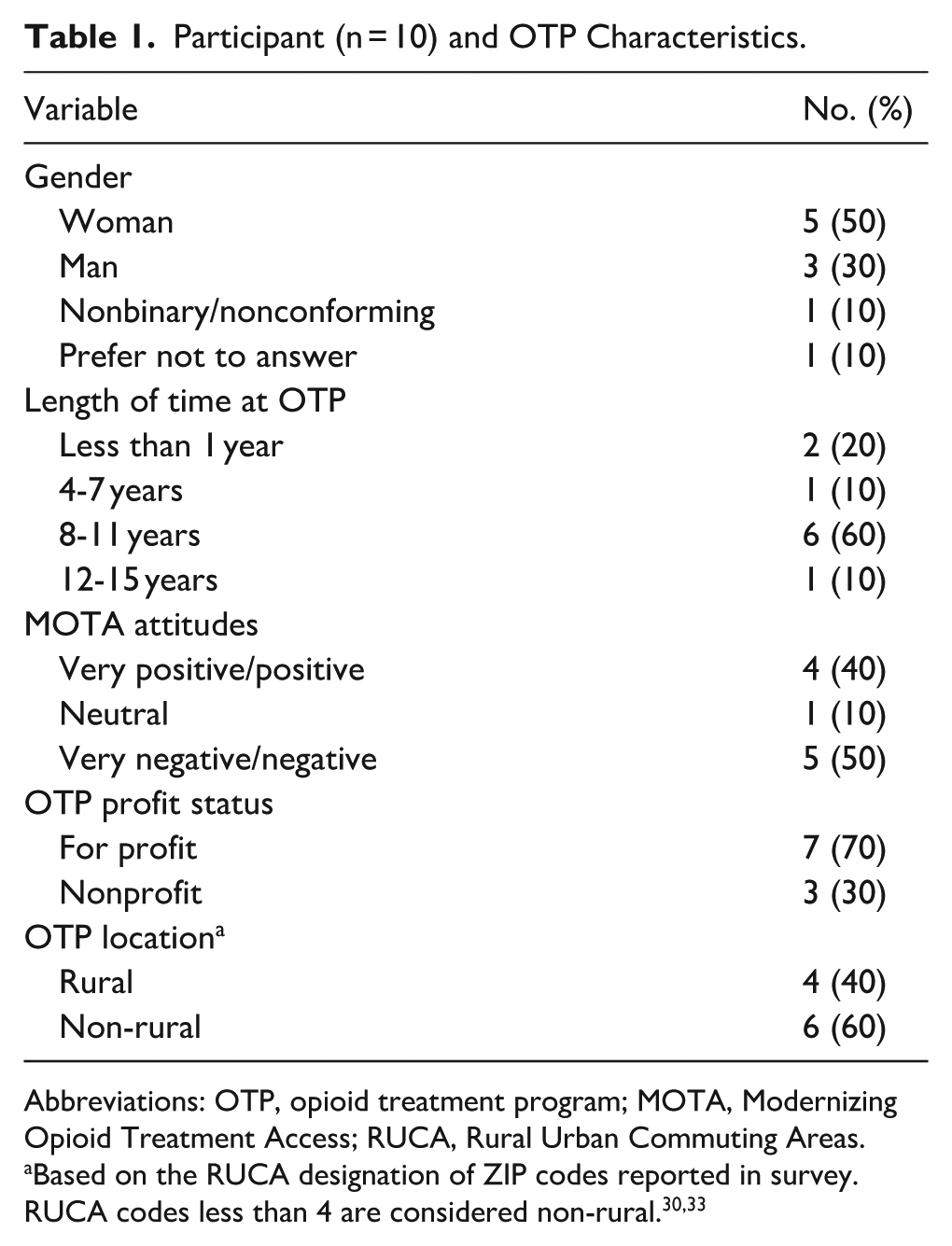
Abbreviations: OTP, opioid treatment program; MOTA, Modernizing Opioid Treatment Access; RUCA, Rural Urban Commuting Areas.
Thematic Findings
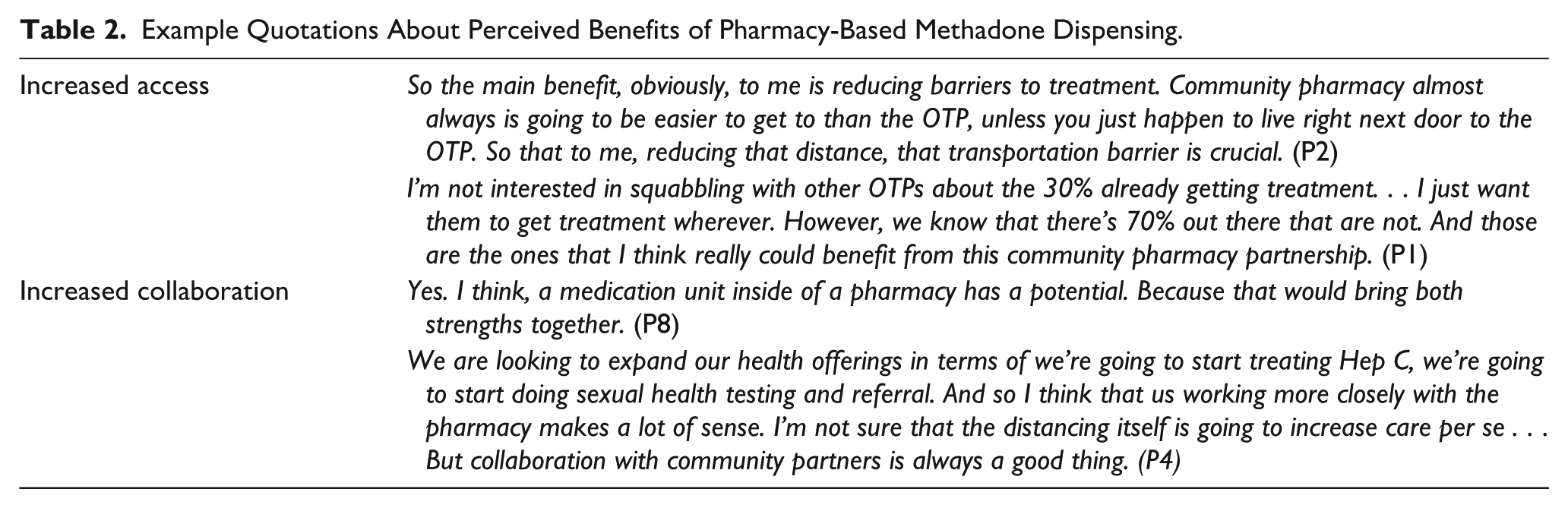
We categorized identified themes under the following categories: perceived benefits of pharmacy-based methadone dispensing (Table 2); perceived concerns about pharmacy-based methadone dispensing (Table 3); implementation barriers; and implementation facilitators (Table 4).
Example Quotations About Perceived Benefits of Pharmacy-Based Methadone Dispensing.
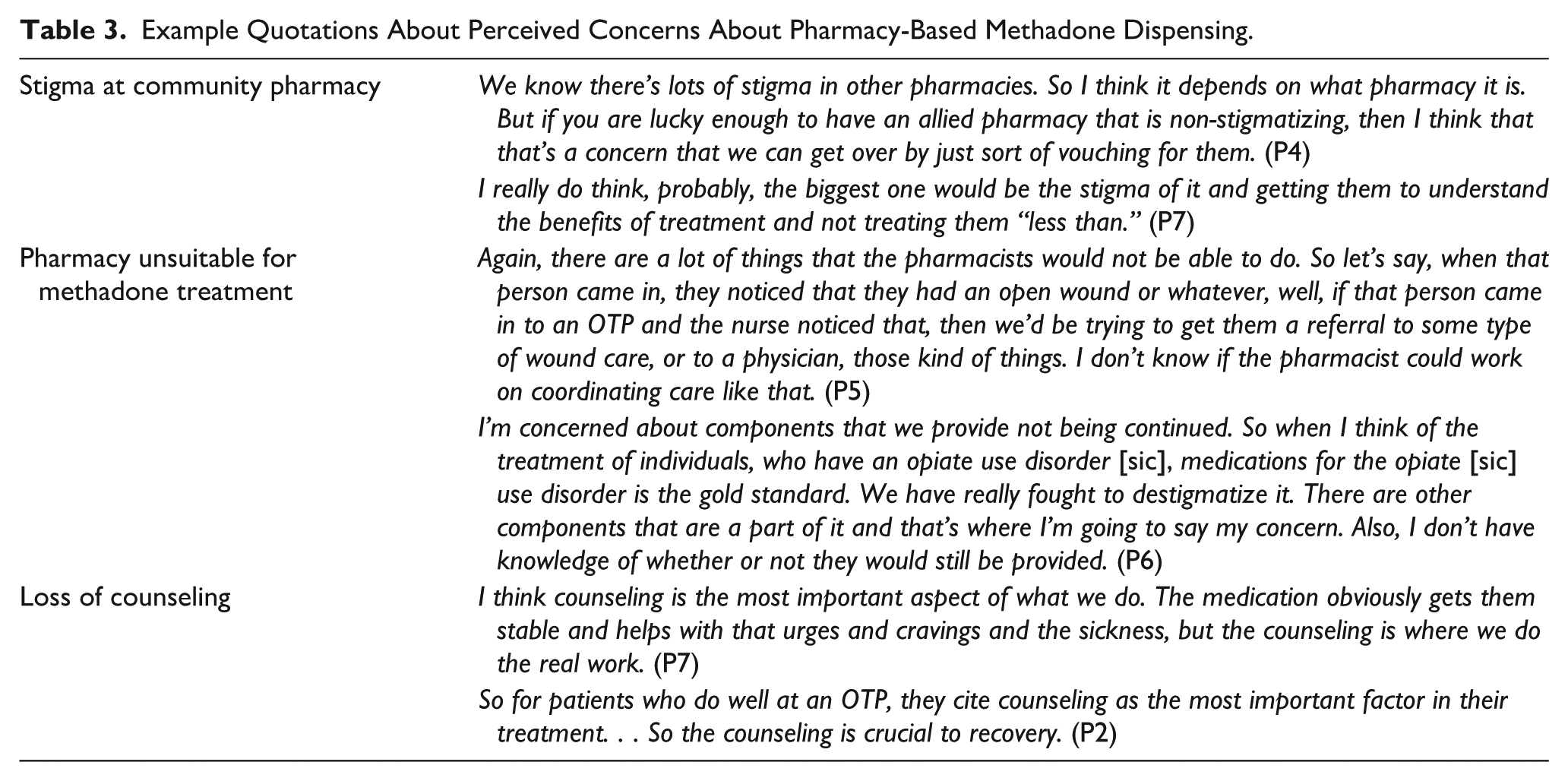
Example Quotations About Perceived Concerns About Pharmacy-Based Methadone Dispensing.
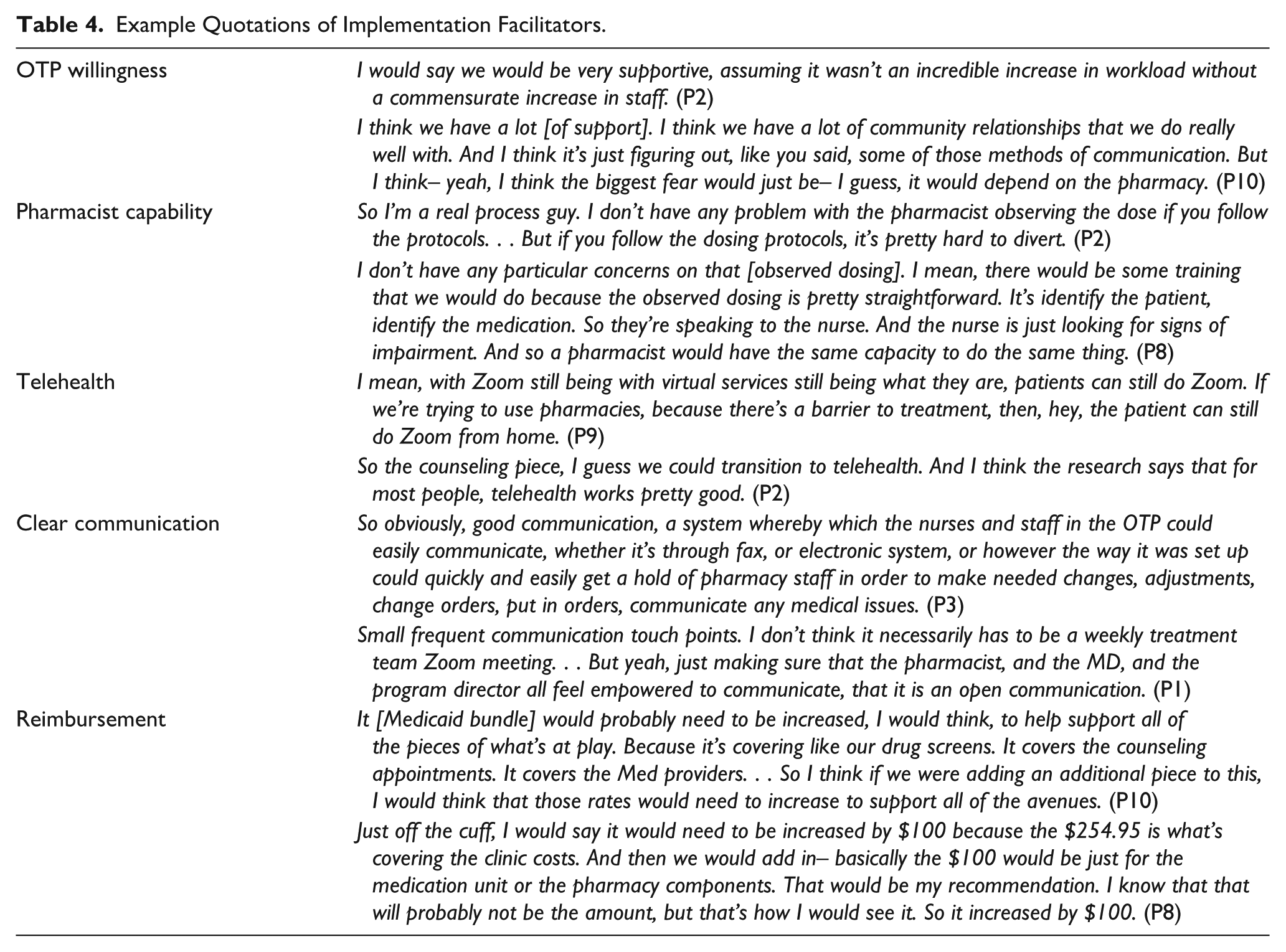
Example Quotations of Implementation Facilitators.
Perceived Benefits of Pharmacy-Based Methadone Dispensing
Increased Access
All participants agreed that dispensing methadone in community pharmacies could increase access to methadone for people with OUD. Examples of increased access mentioned by participants included reducing transportation barriers, having an alternative option to the OTP, and being able to reach people not currently receiving methadone treatment.
Increased Collaboration
OTP staff endorsed increased collaboration as a benefit of pharmacy-based methadone dispensing through medication units. Participants thought OTP-pharmacy collaboration would benefit patients by connecting them to over-the-counter remedies, utilizing pharmacists’ knowledge about drug interactions, and reducing stigma.
Perceived Concerns About Pharmacy-Based Methadone Dispensing
Stigma at Community Pharmacy
All but one participant expressed concern about stigma in the community pharmacy. Participants described stigmatizing conversations they had with pharmacists related to OUD or MOUD, and negative interactions they had personally witnessed between pharmacists and patients but also acknowledged that stigma toward people with OUD is pervasive across health professions, can vary between community pharmacies, and that education may be able to mitigate stigma.
Pharmacy Unsuitable for Methadone Treatment
Similarly, most OTP staff believed that the pharmacy was not the best place for a person to receive methadone. They perceived patients taking methadone for OUD needed specialized care, such as having a structured program, observed drug screens, staff that know them well, case management, and referrals, that they believed a pharmacy would not be able to provide.
Loss of Counseling
OTP staff were concerned about the potential loss of patient access to counseling. OTP staff perceived that counseling is the most important part of treatment and widely stated they would want patients to be able to maintain counseling if pharmacy-based methadone dispensing was implemented.
Implementation Barriers
Lack of Pharmacy Interest
The key implementation barrier that OTP staff anticipated was a lack of pharmacist interest or willingness to dispense methadone. Participants thought that pharmacists would need to be convinced to dispense methadone or that they would not want to incorporate a new service into their practice.
I’m going to have to go, or someone’s going to have to go to these neighborhood guys and convince them that it’s financially worth it, or someone with the state is going to have to say, look, here’s the financial packet that you’re going to get as a result of offering methadone. . . So I think that there’s going to have to be a lot of work on the front end. And I think, even– I think that’s the thing is the AATOD people think the pharmacies are all going to be like, yay, methadone. I don’t think that’s going to happen at all. (P3) Have we talked to any pharmacies that would actually do it? [LAUGHTER] I mean, I can’t imagine them taking time to make all these special arrangements. They don’t do that with any other medication. So what, are they going to build their own dosing room? Who’s going to pay for that? Who’s paying for the time of the pharmacist to do this? (P7)
Implementation Facilitators
OTP Willingness
Despite concerns about pharmacy-based methadone dispensing, most participants expressed a willingness to try an OTP-pharmacy partnership. Participant willingness varied from “We’re all for it” (P4), to “Well, we certainly would be willing to talk with them about it. Like I said, I have some concerns” (P6).
Pharmacist Capability
In addition, several participants felt that elements of dispensing methadone in the pharmacy were within pharmacists’ scope of practice and felt confident that pharmacists could provide the service. This included aspects such as observed dosing, assessing patients for withdrawal symptoms, and preventing diversion.
Telehealth
Most participants mentioned that if pharmacy-based methadone dispensing were to occur, patients could utilize telehealth for counseling. Participants described that in a “post-COVID” world, telehealth has become normalized and can facilitate expansion of methadone treatment into community pharmacies by satisfying counseling requirements and provider communication without requiring patients to travel to the OTP.
Clear Communication
Nearly all participants identified adequate communication between the OTP and pharmacy as important to implementing pharmacy-based methadone dispensing. However, there was a lack of consensus on how best to communicate. Some OTP staff thought that pharmacists could participate in team meetings to discuss patients, while others thought that calling or secure messaging would suffice.
Reimbursement
Half of participants felt the Medicaid bundled rate should be increased to accommodate pharmacy-based methadone dispensing through medication units, while the other half did not know or thought billing should be separated. Among participants that felt the Medicaid bundled rate should be increased, there was no consensus on the amount by which it should be increased, but suggestions included 50 or 100 USD.
Discussion
This study adds to a small but growing body of literature that gathers OTP staff perspectives on expanding methadone treatment through community pharmacies.30,34,35 Our previous survey with this same population found OTP staff are unsupportive toward observed dosing and dispensing methadone in the community pharmacy and cited concerns about patients losing access to counseling and care coordination, community pharmacist stigma, and lack of pharmacist training on methadone. 30 This qualitative study builds off the survey and adds to existing literature by focusing specifically on the medication unit model of dispensing in North Carolina.
Increased access to methadone was the main perceived benefit of pharmacy-based methadone dispensing identified in our previous survey, reinforced during the interviews, and is consistent with other literature from OTP staff and patients.13,30,34,35 Specifically, OTP staff recognize the benefit of increased access to methadone for patients, and think pharmacies are a practical option due to their accessibility. Likewise, OTP staff thought an OTP-pharmacy collaboration could benefit patients and saw it as a compromise between no access in the pharmacy (the current model) and MOTA-based dispensing. While our previous survey found that OTP staff had negative attitudes toward expanding methadone through MOTA, 30 the medication unit model would increase access to methadone while mitigating concerns about patients losing other access to care provided by the OTP. Future research should seek to implement pharmacy-based medication units and identify best practices for a sustainable partnership.
Unsurprisingly, OTP staff described stigma as a main concern regarding pharmacy-based methadone dispensing. Community pharmacist stigma toward MOUD is well-documented17-19; however, if pharmacies were to operate as medication units, OTPs could proactively address stigma by offering pharmacy staff training and education prior to implementation. Furthermore, pharmacist stigma may not be a deterrent to patients.36 In a forthcoming paper on PWLLE perspectives toward pharmacy-based methadone dispensing, patients expressed interest in receiving methadone in the pharmacy despite previous stigmatizing experiences in community pharmacies. 36 This, combined with research that shows patients also experience stigma at the OTP,10,37 suggests that PWLLE anticipate pharmacy-based methadone dispensing to be a comparable, if not preferred, method for obtaining their methadone.
OTP staff also expressed concerns about loss of care coordination and counseling in a pharmacy-based methadone-dispensing model. Participants felt the pharmacy would be unsuitable for methadone treatment because of the complex patient population. These perspectives are congruent with research from other countries where pharmacy-based methadone dispensing is allowed, in which heavy workload related to patient care impacts pharmacists’ willingness to provide methadone-dispensing services. 38 However, this stance contradicts some patient perspectives, who find restrictive OTP policies to be counterproductive to their recovery.11,12,39 Likewise, concerns about the loss of counseling may stem from personal opinions on the treatment model and not evidence-based practice. In North Carolina, OTP patients are currently required to attend counseling twice a month for the first year of treatment, and once a month following that, although there is a proposed bill that would eliminate this requirement.40,41 Other states do not have counseling requirements, 42 and research has found counseling to have little impact on patient outcomes for those taking methadone,3,43,44 which reflects the need to make counseling both optional and individualized to best fit patient needs.
Lack of pharmacy interest was the main implementation barrier identified. However, recent research has found that community pharmacists support expanding methadone access for OUD to community pharmacies.35,45 Although previous literature has documented lack of willingness to dispense buprenorphine among pharmacists,18,46-48 training and proper reimbursement could further facilitate pharmacy buy-in, as mentioned by pharmacists from other countries where pharmacy-based methadone dispensing is legal. 38
Over half of participants expressed willingness to explore an OTP-pharmacy partnership through a medication unit, which aligns with perspectives from OTP staff who participated in a 2020 pilot study in North Carolina. 35 In addition to their willingness to explore OTP-pharmacy partnerships, participants also thought pharmacists would be capable of observed dosing and dispensing methadone, despite our previous survey finding that OTP staff had negative views on the acceptability, feasibility, and appropriateness of observed dosing and dispensing methadone in the pharmacy. 30 These seemingly discordant findings warrant further investigation. Regardless, efforts to further improve OTP staff perceptions on pharmacy-based methadone dispensing may require successful implementation and subsequent uptake of pharmacy-based medication units.
Clear communication was identified as the most important aspect to ensure OTP-pharmacy partnerships would work. However, participants did not reach consensus on a preferred mode or frequency of communication, so future implementation studies should explore how to tailor communication between the pharmacy and OTP to ensure successful collaboration. The importance of communication speaks to a larger need for a comprehensive protocol for OTP-pharmacy collaboration, as identified by OTP staff and pharmacists who participated in a 2020 pilot study. 35 Key components of the protocol may include processes for dispensing and administration, assessing withdrawal, and overdose prevention, as well as those related to communication between OTP and pharmacy staff with an emphasis on patient-centered care. Furthermore, telehealth was also identified as an implementation facilitator, aligning with other research that has found telehealth to facilitate health care and MOUD access, including in rural North Carolina.49-51 With a pharmacy-based medication unit, telehealth would reduce patient visits to the OTP, thereby increasing the convenience of methadone treatment. Finally, proper reimbursement for pharmacy-based methadone dispensing has consistently been identified as necessary for successful implementation and has been endorsed by OTP staff and pharmacists alike.34,35,38
Limitations
The small sample may limit the generalizability of results. In addition, OTP staff attitudes may vary state to state given differences in OTP state regulations and requirements. Our sample consisted primarily of program directors, as suggested by the clinical advisory board; however, OTP staff more familiar with dispensing and observing methadone doses (eg, dosing nurses) might have different perspectives on potential barriers and facilitators to incorporating pharmacy-based methadone dispensing into the pharmacy workflow. Although individuals were purposively sampled to capture a range of opinions, individuals in the nested sample may have been more open to pharmacy-based medication units than survey respondents not interested in interview participation.
Conclusion
Results from this study demonstrate moderate interest from OTP staff toward pharmacy-based methadone dispensing. Despite various concerns around pharmacy-based methadone dispensing, OTP staff recognized the potential benefits for people with OUD, expressed willingness to explore an OTP-pharmacy partnership, and felt pharmacists could provide the service. Building off research conducted by Wu et al. (2022) 25 and Brooner et al. (2022) 26 that established proof of concept, researchers, and other vested parties should consider conducting a pilot study to identify how best to implement medication units in the pharmacy setting.
Supplemental Material
sj-docx-1-saj-10.1177_29767342261449037 – Supplemental material for Expanding Methadone Access Through Community Pharmacies: A Qualitative Study Exploring Opioid Treatment Program Staff Perceptions of Pharmacy-Based Medication Units
Supplemental material, sj-docx-1-saj-10.1177_29767342261449037 for Expanding Methadone Access Through Community Pharmacies: A Qualitative Study Exploring Opioid Treatment Program Staff Perceptions of Pharmacy-Based Medication Units by Caroline Shubel, Mary Ava Nunnery, Grace T. Marley, Delesha M. Carpenter and Bayla Ostrach in Substance Use & Addiction Journal
Supplemental Material
sj-docx-2-saj-10.1177_29767342261449037 – Supplemental material for Expanding Methadone Access Through Community Pharmacies: A Qualitative Study Exploring Opioid Treatment Program Staff Perceptions of Pharmacy-Based Medication Units
Supplemental material, sj-docx-2-saj-10.1177_29767342261449037 for Expanding Methadone Access Through Community Pharmacies: A Qualitative Study Exploring Opioid Treatment Program Staff Perceptions of Pharmacy-Based Medication Units by Caroline Shubel, Mary Ava Nunnery, Grace T. Marley, Delesha M. Carpenter and Bayla Ostrach in Substance Use & Addiction Journal
Footnotes
Acknowledgements
The authors would like to thank the clinical advisory board: Amanda Isac, Cheryl Viracola, Eric Morse, Michael Kidorf, Nathan Mullins, Nicole Franklin Ross, Steve Adkins, and Zoe Weinstein, for their feedback on the interview guide. The authors also honor the memory of Louise Vincent and Jessica Weisner, 2 members of the clinical advisory board whose recent passing they mourn.
Ethical Considerations
The University of North Carolina at Chapel Hill Office of Human Research Ethics reviewed a protocol for this study and determined it exempt from further review (IRB #24-3111).
Consent to Participate
All participants provided verbal consent to participate after reviewing an IRB-approved study fact sheet.
Consent for Publication
All participants provided verbal consent to participate after reviewing an IRB-approved study fact sheet.
Author Contributions
Caroline Shubel: Conceptualization, investigation, formal analysis, writing original draft; Mary Ava Nunnery: Project administration, investigation, writing—review & editing; Grace T. Marley: Conceptualization, writing—review & editing; Delesha M. Carpenter: Conceptualization, funding acquisition, supervision, writing—review & editing; Bayla Ostrach: Conceptualization, funding acquisition, writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the North Carolina Collaboratory. The content is solely the responsibility of the authors and does not necessarily represent the official views of the North Carolina Collaboratory.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Per the approved human subjects research and ethics review protocol, and the consent process undertaken with research participants, data from this study cannot be made available as this would compromise participant confidentiality.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.