
Abstract
Background:
Within office-based addiction treatment (OBAT) for opioid use disorder, routine urine drug testing (UDT) has been a near-universal practice, despite concerns about increased stigma and limited evidence on improved patient outcomes. During the COVID-19 pandemic, routine UDT was suspended in many settings as care transformed to telehealth, providing an opportunity to explore viewpoints about routine UDT and the implications of its absence.
Methods:
We explored patient and provider perspectives through qualitative interviews conducted from May 2021 to May 2022 within an urban, low-threshold OBAT program. Semi-structured interview guides and thematic analysis explored opinions on traditional routine UDT and experiences with its discontinuation during the COVID-19 pandemic.
Results:
Based on perspectives of 25 patients and 16 providers, we identified three themes regarding routine UDT and its decreased use during the COVID-19 pandemic: (1) the general utility of UDT within traditional models of care, (2) burdens that routine UDT could present to care engagement, and (3) impacts of UDT on trust within patient–provider relationships.
Conclusions:
Our findings support the need for reconsideration of routine UDT in OBAT, as well as the needs for improved care standards. Selective use of UDT can be implemented in a patient-centered manner, including offering it upon patient request (eg, for personal “accountability”) and discontinuing it when appropriate and to reduce barriers to care. In place of routine UDT, our findings also highlight the need for alternative, non-stigmatizing clinical tools that can support patients and providers within OBAT care settings.
Highlights
Patients and providers described experiences with routine urine drug testing (UDT) in opioid use disorder treatment.
UDT can pose barriers to continued care engagement for many patients.
UDT can reinforce power dynamics between providers and patients.
Findings support patient-centered, selective use of UDT and a need for alternative clinical tools.
Introduction
Opioid use disorder (OUD) and related mortality continue to threaten public health in the United States. Alongside rising use of synthetic opioids like fentanyl, 1 opioid overdose deaths increased 289% between 2011 and 2021. 2 Buprenorphine is a highly effective treatment for OUD that reduces overdose risk and improves quality of life.3-5 As a first-line OUD treatment, buprenorphine can be prescribed in generalist outpatient settings known as office-based addiction treatment (OBAT). Across OBAT programs, urine drug testing (UDT) is a common practice, often involving rapid qualitative immunoassay screenings for major drug classes (including buprenorphine as for monitoring treatment adherence) and confirmatory testing and quantification via gas chromatography-mass spectrometry (GC/MS).6,7
With the widespread contamination of unregulated drug supplies with fentanyl, 8 the American Society of Addiction Medicine expert guidance recommends “frequent” (eg, weekly) UDT during the early stages of treatment for augmenting inaccurate patient self-report and detecting unintentionally ingested substances. 9 Prior studies have demonstrated “unexpected” UDT results including undetectable levels of prescribed buprenorphine and presence of non-prescribed substances.10,11 However, a recent systematic review found no strong evidence of positive impacts on patient outcomes (eg, reduced overdose risk) and significant limitations of existing research. 12 Furthermore, there is little guidance or consensus on how to implement UDT (eg, when to decrease UDT frequency following patients’ clinical stabilization, whether to directly observe specimen collection or not), resulting in wide variation in clinical practices and debates surrounding the utility of UDT.13-15 While it could supplant or supplement self-reported substance use, there is little published evidence that providers change treatment plans when UDT results and self-report diverge. 16 Furthermore, a Norwegian study found that low-threshold OUD treatment programs that do not require UDT or abstinence from substance use can be as safe and effective as traditional models, with comparable rates of treatment retention, non-prescribed opioid use, overdose, and death. 17
Debates surrounding UDT include concerns about its potential negative impacts, including the perpetuation of stigma, mistrust, and power dynamics between patients and providers, 18 which may impact patients’ perceptions of care quality and decisions to engage with care. 19 People who use substances have been historically marginalized, and UDT has contributed to their surveillance and stigmatization.20,21 UDT may also be used in a biased manner, perpetuating structural racism. 22 Coupled with limited training on how to utilize UDT effectively for improving patient care, providers have increasingly questioned its inclusion in OUD treatment with buprenorphine. 13 With transitions to telehealth during the COVID-19 pandemic, routine UDT became impractical and was vastly decreased or eliminated in many OBAT programs, leading experts to posit its routine UDT would go “down the drain.”14,15 However, to date, the literature lacks systematic investigation of providers’ and patients’ perspectives on the benefits and drawbacks of routine UDT in OUD treatment. To inform ongoing debates and current care recommendations, we leveraged data collected from a pandemic-era study 23 to explore these views on the utility of routine UDT.
Methods
Study Setting, Design, and Sample
As previously described, 23 during the COVID-19 pandemic, we conducted qualitative interviews with patients and providers in an urban primary care-based OBAT clinic with a harm reduction focus. In this clinic, nurse care managers share clinical management responsibilities with prescribers and coordinate support from medical assistants and other team members.24-26 The clinic traditionally relied on frequent in-person visits, with UDT involving a screening immunoassay test for amphetamines, barbiturates, benzodiazepines, cocaine, fentanyl, methadone, opiates, and oxycodone; positive fentanyl screens were reflexively sent for quantitative GC/MS fentanyl and norfentanyl levels. Starting in March 2020, the clinic transitioned to telehealth, later evolving into a hybrid model incorporating some in-person appointments. For these qualitative interviews, patients’ eligibility included: confirmed OUD diagnosis, previously prescribed buprenorphine, having at least one OBAT clinic encounter since January 2020, being ≥18 years of age, and able to speak English. We used purposive sampling to maximize diversity in patients’ gender, race/ethnicity, age, and time in treatment. OBAT providers’ eligibility included OBAT employment for ≥3 months prior to March 2020; purposive sampling ensured a variety of job responsibilities and roles were represented. All recruitment contacts with prospective participants occurred by phone (patients) or secure email (providers). Participants provided verbal informed consent and were compensated $50 (via debit card) for completing qualitative interviews. The Boston University Medical Campus Institutional Review Board reviewed and approved all study protocols.
Data Collection
From May 2021 to May 2022, trained, graduate-level interviewers conducted semi-structured interviews by phone or video conferencing. Relevant to this analysis, open-ended questions for patients included: “Do you find it helpful to do regular urine drug tests? Why or why not?” and “What has it been like to
Data Analysis
We developed deductive and inductive codes through an iterative, collaborative codebook development process engaging multiple individuals across our interdisciplinary team.27,28 We first read transcript selections independently to develop and test codes, then met as a team to discuss and revise draft codebooks, repeating this process several times until reaching consensus (through regular team meetings) on our codebooks. We then double-coded 2 to 3 full transcripts in the patient and provider datasets using NVivo software (Lumivero, version 13 [Release 1]) 29 and discussed and resolved coding discrepancies to establish consistency. Single analysts then coded all transcripts, meeting regularly to discuss coding progress and emerging themes. Following coding, we used the framework method with thematic analysis to summarize coded data and document representative quotes into matrices (ie, spreadsheets). 30 After reviewing matrices, we developed higher-level interpretive memos for each code, which the lead author compared between patients and providers for thematic analysis. Relevant codes for this analysis, which were defined similarly for patients and providers, included overarching codes for “Changes in Care Processes” and subcodes for “Urine Toxicology Screening.” Other codes examined included “Patient-Provider Interactions,” “Patient Access and Engagement in Care,” and “Stigma.” Key themes identified in our analysis are supported with representative, anonymized quotes.
Results
Overall, we interviewed 25 patients (characteristics shown in Table 1) and 16 providers representing seven prescribers (physicians, nurse practitioners) and nine non-prescribers (seven nurses, two program staff members). Thematic analysis identified the following themes regarding routine UDT within OBAT: (1) the general utility of routine UDT in traditional models of care, (2) the burden to continued engagement in care posed by routine UDT, and (3) the impacts of UDT on trust within patient–provider relationships.
Characteristics of Patient Interview Participants (n = 25). a
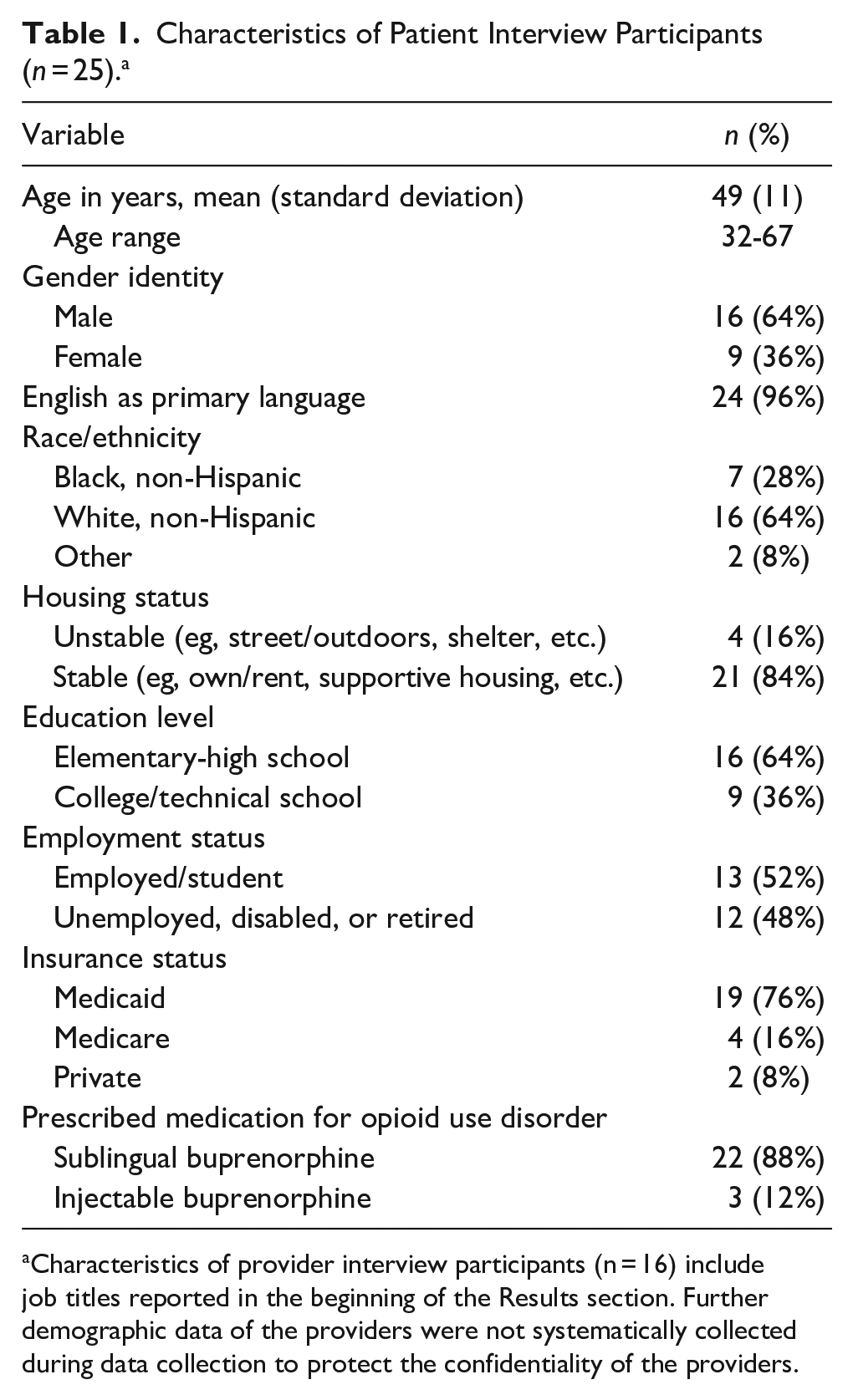
Characteristics of provider interview participants (n = 16) include job titles reported in the beginning of the Results section. Further demographic data of the providers were not systematically collected during data collection to protect the confidentiality of the providers.
General Utility of Routine UDT in Traditional Models of Care
Participants described various ways that routine UDT had utility in traditional models of OBAT. Some providers described UDT as providing important information about the appropriate use of medication and potential medication diversion: “If there’s a risk that they’re not taking the medication, [UDT is] really important. . .for being able to frame that conversation and help patients get the care they need. . .also, [to] not be giving them something they can sell to subsidize other [substance] use.” (Provider #1)
While some providers felt that UDT could influence prescribing decisions, others said that they would likely not change their prescribing decisions if other substances were present in patients’ urine samples. Instead, most providers described UDT as a helpful tool for identifying patients who could benefit from additional clinical supports (eg, medication dosing adjustments, referrals to mental health services). Additionally, some providers felt that UDT was particularly beneficial for facilitating conversations related to harm reduction: It’s not super common I see something [in UDT] that is outside of the range of what someone’s telling me. Sometimes, early in care, [patients] don’t know if they can trust us yet, maybe because they had bad experiences with other places [so] they may not disclose everything. [UDT] can lead to a conversation about how we can help them with safer use behaviors, so it’s really an opportunity to engage in risk reduction. (Provider #1)
Patients described the utility of detecting drug supply contamination and other ways UDT was helpful to them, such as documenting abstinence from substances for child custody cases and probation requirements. Notably, some patients described using UDT results as an objective source of information on their progress in treatment: “I actually like to do [UDT] because. . .say my family was ever doubting me. . .I like the fact that I did urines [to] support the fact that I’m not using.” (Patient #1)
Finally, many patients viewed UDT as supporting their “accountability” and motivation to abstain from substance use (eg, if they knew they were scheduled for routine UDT). As one patient, reflecting on the impact of the pandemic, explained, “I like to be held accountable [by giving] the urine [but] COVID took that away. . .I’m no longer accountable. Anything could be in my urine. . .essentially, I can do anything I want, [and] that’s not a good thing for an addict to know in his head.” (Patient #2) Additionally, even though providers in this clinic explained that they would not use UDT in a punitive way, a few patients held the belief that they could “lose” their access to buprenorphine if they repeatedly “failed” UDT, and as one patient commented, “knowing that keeps me straight and narrow.” (Patient #3)
The Burden to Continued Engagement in Care Posed by Routine UDT
Despite the utility of routine UDT in traditional models of care, some participants also described ways that it could present challenges to continued engagement in care. Providers expressed concerns that routine UDT could be burdensome for many patients, particularly prior to the pandemic when patients were scheduled for frequent in-person visits involving routine UDT that were time-consuming, requiring arrangements for transportation, childcare, and employment responsibilities. Providers felt that telemedicine (without UDT) decreased these burdens on patients, which felt appropriate because UDT was not affecting their clinical decision-making, especially for more “stable” patients: Bringing someone in only for [UDT], if I have no clinical concerns, is not going to provide long term clinical benefit for that person. So I think the ongoing access and flexibility that telemedicine offers is potentially reaching [more patients] and will enable continued retention, especially for stable patients. (Provider #2)
Some patients felt reduced need for the “accountability” provided by routine UDT as they progressed in their recovery and viewed UDT as an “inconvenience.” One patient also expressed suspicion of financial motivation for UDT, saying “I think [the clinic] gets paid for every urine sample [so] the only thing that matters is how many urine samples they could get in a month. . . [they should] stop putting so much emphasis on urine samples and start treating people.” (Patient #4) In addition to questioning the purpose behind UDT, some patients explained how the copays associated with frequent testing, in combination with visits or other laboratory testing, posed a financial burden: “I’m not [sure] I can continue going [to OBAT]. I’ve somehow racked up over a thousand dollars [in] medical bills [with] insurance. . .it almost is impossible to get treatment [and] it’s expensive because of all the testing.” (Patient #5)
Providers also expressed concern that UDT could feel stigmatizing to patients, especially those with a history of trauma, possibly leading to a problematic “us vs. them” dynamic between patients and providers and ultimately challenging patients’ engagement in care: We’re using tele-visits to our advantage and also to the patients’ advantage, and engagement has improved drastically. . . [If you] come to the clinic and have to provide urine, it’s a little dehumanizing, even though it’s for the greater good and for us to track [progress] with treatment and support them. For some of them, I think it feels like there’s “them,” and then there’s “us,” and nobody wants to feel that way. (Provider #3)
Some patients expressed some discomfort but compared practices in this clinic to others where they had received care: “It’s private [here]. They let you go in the bathroom by yourself, nobody watching you. You’re more comfortable; you can urinate just like that. With somebody standing over you, it’s hard to do.” (Patient #6) Another patient who held generally negative feelings towards UDT also explained how, in this clinic, UDT was used to support and not penalize them: “I would fall off and [not] want to go into the clinic and give my urine because I was kind of embarrassed. . .But, one time when I [gave] an [unexpected] urine. . .we just talked about it and [my provider asked], ‘What happened?’ but not in a bad way. . .just like she was truly concerned.” (Patient #7)
The Impacts of UDT on Trust Within Patient–Provider Relationships
Participants described specific impacts of UDT on trust between patients and providers, noting changes that occurred following the pandemic-related suspension of UDT. Some patients described how the routine use of UDT in traditional models of OBAT provided them with opportunities to demonstrate their willingness to engage with treatment and gain trust from their providers, as one patient explained: “You have to build their trust; you have to earn it. The better you do and the more consistent and responsible you are, they’ll [have] more room to trust you.” (Patient #8)
Some providers felt that patients’ trust was more limited prior to the pandemic when patients were trying to use UDT to prove commitment to treatment as described above. Some patients were fearful of losing “privileges” such as longer prescription lengths and less frequent in-person appointments due to unexpected UDT results, and this extended into fear of disclosing substance use during telehealth appointments during the pandemic when routine UDT was suspended. Some providers felt that patients were more honest and open about their substance use once they acclimated to the relaxation of the clinic structure with the telehealth transition: [Some patients] really wanted to hold onto their spot [in the old structure], but there was hesitancy to really talk about things. . .Once we became unfurled from that structure, I think people started talking more. So I have a huge amount of relief that we’re not [UDT] screening people all the time. (Provider #1)
In reflecting on pandemic-related changes to care, another provider commented on the trust-enhancing implications of discontinuing routine UDT: I think one of the biggest things that we’ve seen come out of COVID is this understanding that [UDT is] just not a critical piece of addiction care. . . . OBAT held that sort of global “we’re gonna check your urine because we’re not gonna necessarily believe what’s coming out of your mouth.” And so really seeing that we could provide really great supportive care to our patients and our patients continue to receive care and do really well, despite not coming in every week and giving urine. (Provider #4)
This provider described how a lack of UDT allowed patients to feel trusted by providers because they didn’t have to “prove” their sobriety with UDT, also enabling providers to provide effective medical care without objective tests to verify patients’ self-reported behaviors.
Conversely, a few providers felt that, after discontinuing routine UDT, patients were less “forthcoming” and providers had “no way to gauge what’s going on” (Provider #5), potentially raising concerns about negative outcomes for patients, at least initially: My perception was that a lot of people were going to overdose and die. . .We lost a huge tool to figure out where our patients were at in their recovery process. . .it was difficult to do my job not having that tool. (Provider #6)
However, another provider described more effective, preemptive methods of increasing patient knowledge of drug supply contamination: I had a group of patients. . .who were insistent that. . .they weren’t exposed to fentanyl. And so, there was utility [in UDT] to say “No, there is fentanyl coming through.” [But] from a standpoint of safety, and having patients understand what they’re using. . .a better system [would be one in which] they can test their drugs instead of us testing their urine. (Provider #1)
Many providers, including Provider #6 (quoted above), described other methods for assessing patients’ needs, including examining appointment attendance and “no show rates,” emergency department and pharmacy records, and relationship-building through close and open communication. Providers found that developing good rapport with patients could be most helpful in identifying their specific needs.
Patients’ interviews also reflected the importance of strong, trusting relationships with providers for supporting their recovery trajectories, enabling some to openly and proactively disclose substance use ahead of or in the absence of UDT results: You’re not judged. . .So it’s not something I fear, and I always tell [them] beforehand, this is what you’re gonna find [in my UDT]. . .And then they sit me down and want to talk about what’s going on, why did I feel the need to use that particular substance that day? As long as I’m honest with them. . .regardless of [the UDT], I know I have that support. (Patient #9)
Providers indeed hoped that patients felt empowered to discuss their recovery and make such disclosures on their own terms: It is more useful for a patient to feel comfortable talking about [their substance use] and for them to be the one that brings it up and be ready for that [conversation]. There is also more trust when [patients] feel like we’re in it [together] versus looking [for] something negative. And while that’s not our perception of [care], that’s the patient perception of it. (Provider #3)
Discussion
Our interviews with patients and providers identified specific perceived benefits and drawbacks of routine UDT in OBAT, generating practical implications for optimizing clinical practice in the context of recent debates surrounding the utility and optimal utilization of UDT in OUD treatment (Table 2). Overall, in reflecting on the suspension of routine UDT during the pandemic, which occurred in the context of significant transitions towards telehealth, our participants acknowledged some benefits of UDT while describing how it also posed a burden for some patients and could hinder trust between patients and providers when not implemented with patients’ individual needs in mind.
Practical Implications for Opioid Use Disorder Treatment Providers for Use of UDT in Clinical Care.
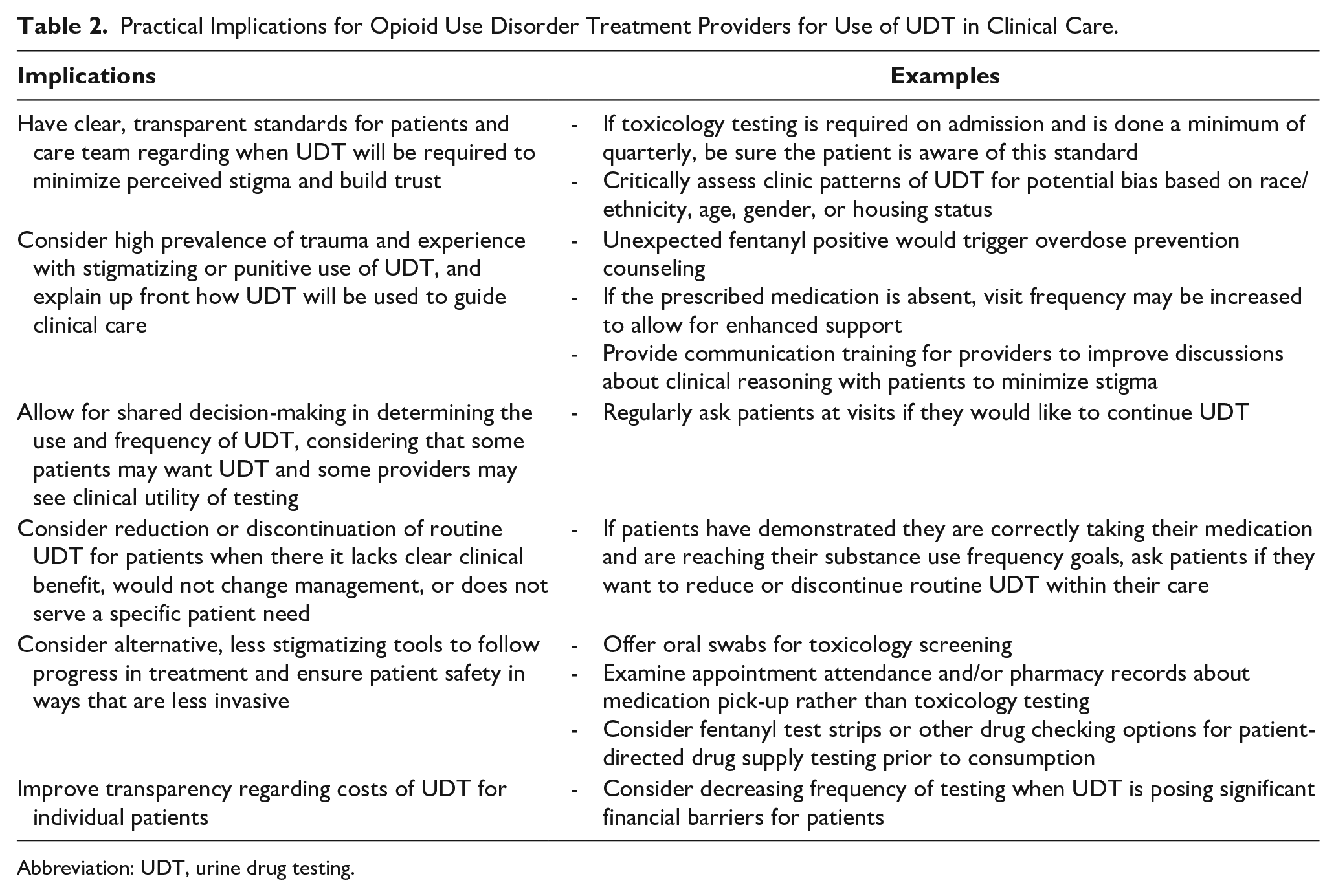
Abbreviation: UDT, urine drug testing.
Regarding the positive benefits of UDT in OBAT, some patients felt strongly that its routine use supported their “accountability” in treatment, particularly in the early stages, aligning with previous research. 18 Some providers also felt that UDT could provide helpful clinical information to guide decision-making, while others felt that “unexpected” UDT results would not change their buprenorphine prescribing, contextualizing prior quantitative research. 16 In our sample, instead, providers guided by a harm reduction lens could use UDT results to have open conversations about ongoing substance use and needs for additional recovery supports (eg, unexpected positive toxicology for benzodiazepines could prompt discussion of undertreated anxiety symptoms) 18 or the unpredictability of unregulated drug supplies (eg, fake pressed pills, which could be contaminated with toxic and potent fentanyl analogs).
Many patients and providers in our sample also described how UDT could pose a burden for some patients and reinforce stigma, as identified in research on methadone in which patients providing urine samples experienced embarrassment and shame. 18 These and other drawbacks of UDT (eg, financial burdens on patients) can reduce treatment initiation and retention, 31 leading us to pose several recommendations for improving patients’ perceptions and experiences of quality care and ultimately supporting their care engagement (Table 2). For example, our findings highlight a possible communication gap even in low-threshold settings, as patients feared punitive repercussions for unexpected UDT results despite provider reassurance against this. As such, it is imperative for providers to consider the high prevalence of trauma patients may have experienced in treatment settings with enforced surveillance or more punitive approaches to addiction care (Table 2, Row 2). Additionally, considering prior qualitative research and the findings of this study, providers should consider cost as a factor when planning the frequency of testing (Table 2, Row 6).
In addition to the significance of trauma-informed approaches, contrasting our study setting with the literature highlights the poorly defined standards surrounding UDT implementation. There is wide variation in UDT implementation, which depends in part on providers’ abilities to select appropriate technologies and effectively interpret results. In an evaluation of UDT training for internal medicine residents, pre-program surveys found that despite almost all of the residents utilizing UDT in their practice, 81.8% had no prior formal training in UDT interpretation (despite 22.7% reporting that they used UDT results to deny medication refills in the past month). 32 UDT results can have far-reaching consequences for specific populations (eg, those with criminal legal involvement), underscoring the need for training in test selection and interpretation, and transparent clinic standards to prevent bias with UDT use (Table 2, Row 1).
Providers in our sample were also concerned about potential negative impacts of UDT on trust within patient–provider relationships, explaining that UDT imposed or reinforced power dynamics, which has been documented in other studies.17,33 Providers in our sample also emphasized the need for building rapport and having open conversations with patients (Table 2, Row 3), which could support patient disclosure of substance use or requests for additional clinical supports. While some providers expressed discomfort when lacking objective UDT data, others in our sample pointed to alternative indicators of patient stability in treatment, such as appointment attendance and emergency department visits (Table 2, Row 5), accessible through a unified electronic health record system, which may not be available to all providers. Another provider suggested drug supply testing for providing objective, accurate information on fentanyl and other contaminants prior to ingestion. Fentanyl test strips (inexpensive and easy to use immunoassay tests) and more advanced point-of-care testing, if available in local communities, could be provided directly or through supportive referrals.34,35 These more upstream, prevention-oriented approaches can empower patients to reduce their overdose risk, 36 potentially improving patient safety more directly than UDT results discussed in clinical settings after ingestion (Table 2, Row 5).
Limitations
Our study had several limitations. We recruited participants from a single low-threshold OBAT program within an urban academic medical center, limiting generalizability. This particular clinic had a harm reduction orientation, which may have resulted in less punitive practices (eg, it does not engage in directly observed urine samples or discharge patients for unexpected UDT results or self-reported substance use), leading to more positive patient experiences of UDT than what might be encountered elsewhere.24-26 Views regarding UDT may have been very different if this study had been conducted in settings that continued or even increased UDT or if the study was conducted closer to the start of the pandemic. This clinic is also located in a Medicaid expansion state with a high rate of health insurance coverage, which may provide a buffer from some of the financial impacts of UDT. 37 As such, patients in our sample may feel more positively about the potential “support” of UDT relative to its costs or other burdens. Further research including quantitative surveys could help confirm our findings in other settings.
Conclusion
Overall, our findings support the need for a thorough reconsideration of routine UDT in OBAT, including the need for more patient-centered standards. UDT has the highest perceived utility during the early stages of treatment or when requested by patients for certain reasons (eg, desires for “accountability”). Based on our data, it seems that UDT would be most helpful if implemented in contexts with appropriate provider training on test interpretation and communication of results. Outside of these specific circumstances, the utility of UDT as a treatment tool should be judged in light of patient goals and barriers to treatment. Our results suggest it could be appropriate to discontinue routine UDT in clinical scenarios where providers and patients determine with shared clinical decision-making that UDT is posing a burden to continued engagement in care and not having significant clinical benefit (Table 2, Row 4). As buprenorphine is a life-saving medication, the use of UDT or any other clinical tests that challenge engagement should be carefully weighed against alternative, less intrusive or more upstream sources of information to promote patient safety.
Footnotes
Acknowledgements
The authors thank Alexander Y. Walley, MD, MSc and Colleen T. LaBelle, MSN, RN-BC, CARN for their assistance with study design and the OBAT clinical team for their support of recruitment and research activities.
Author Contributions
JT: Conceptualization, Formal Analysis, Writing—Original Draft, Writing—Review and Editing. ARB: Supervision, Conceptualization, Writing—Review and Editing. SB: Formal Analysis. JB: Project Administration, Formal Analysis. AC: Formal Analysis. MD: Conceptualization, Methodology, Formal Analysis, Investigation, Writing—Review and Editing. SF: Investigation, Formal Analysis. KMM: Conceptualization, Project Administration, Writing—Review and Editing. RS: Funding Acquisition, Conceptualization. ASV: Conceptualization, Writing—Review and Editing. ZMW: Conceptualization, Writing—Review and Editing, Supervision, Funding Acquisition.
Data Availability Statement
Data generated and analyzed during the current study are not publicly available due to its sensitive nature and to protect participant confidentiality but may be available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR001430. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The supporting organization had no further role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Compliance,Ethical Standards,and Ethical Approval
The Boston University Medical Campus Institutional Review Board reviewed and approved all study protocols and provided a waiver of documentation of consent.
Consent to Participate
Participants provided verbal informed consent; the Boston University Medical Campus Institutional Review Board reviewed and approved all study protocols and provided a waiver of documentation of consent.
Consent for Publication
Not applicable.