
Abstract
Background:
Despite increasing research on substance use among migrants and refugees, little attention has been paid to the instruments assessing substance use in these populations. This systematic review examines the suitability of substance use instruments for use in migrant and refugee populations and the quality of the instruments.
Methods:
A systematic search of the electronic databases PubMed, Web of Science, PsychINFO, and EMBASE was performed. Articles were eligible if they assessed substance use among refugees using a standardized instrument. Instrument properties were assessed using a standardized checklist, and the measurement properties were evaluated according to Terwee’s criteria.
Results:
In total, n = 2654 studies were retrieved. Of those, we included n = 55 studies. The most frequently used instrument was the Alcohol Disorder Identification Test (n = 20, 36.4%) followed by the CAGE/CAGE4M and the Mini International Neuropsychiatric Interview (n = 7 studies each, 12.7%). Out of 24 instruments, 18 (75%) were developed in English. Content validity, cross-cultural validity, and criterion validity were unreported for most instruments (n = 13, 54.2%). None of the instruments were developed with input from refugees. Completion time of the instruments ranged from 1 to 120 minutes. Psychometric properties were either not assessed in refugees or were moderate.
Conclusion:
None of the assessed instruments met all the psychometric criteria sufficiently. Therefore, it will be necessary to develop a rationale for instruments to better fit the needs of diverse groups of migrants and refugees. Accordingly, these instruments fitted to specific groups will allow for better measurement of substance use, diagnosis, and monitoring of treatment.
Highlights
The prevalence of substance use among migrants and refugees is largely unknown.
In order to ensure the reliability of the data collected, it is essential to implement instruments that are sensitive to the specific needs of refugees and migrants. Our findings indicate that instruments measuring substance use have been predominantly developed in English-speaking countries.
According to the quality criteria, some instruments, however, have better psychometric properties than others and have been widely used in refugee and migrant populations.
No substance use instrument so far has been developed together with migrants and refugees.
Introduction
Substance use in migrant populations is a significant Public Health challenge.1-4 The risk for substance use disorders among persons forcibly displaced from their home country, referred to as refugees, increases with the length of residence in the host country. The longer refugees stay in a host country, the more their risk of substance use converges with that of the native population. 5 However, findings depend on the quality of the measures used to assess substance use including their cultural validity. As of 2021, there were 89.3 million forcibly displaced persons. Eighty-three percent of the world’s forcibly displaced persons live in low- and middle-income countries, as reported by the Global Trends Report. 6 Accordingly, the number of refugees affected by substance use is likely to increase in the next years, alone due to the increase in refugees. By 2021, the number of individuals using substances is estimated to have increased to 296 million worldwide. 7 According to the Global Burden of Disease Study, 30.9 million years of healthy lives were lost and approximately 494.000 deaths were attributable to substance use in 2019. In 2018, 132.6 million disability-adjusted life years and 3 million deaths (5.3% of all deaths) were reported as a result of harmful alcohol consumption. 8
Studies suggest that prevalence rates of substance use and substance use disorders (SUDs) among refugees range from 2% to 60% for alcohol and 0.66% to 31% for other substances. 9 While research shows that substance use among refugees is significantly lower compared to the general population, it is unclear to what extent instruments capture aspects of substance use that are relevant to refugee populations, and whether available instruments are valid and reliable for the specific groups. Migrant and refugee populations are heterogeneous groups. The course and symptoms of SUDs are linked to differing cultural backgrounds and conditions in host countries. 10 This implies a need for culture-specific measures to be developed or for existing measures not only to be translated but also to be adapted to the specific contexts of particular populations. 11
Differences in prevalence rates might be related to the measures used.12,13 At the moment, some instruments are widely used, such as the Alcohol Disorder Identification Test (AUDIT), the Cut Down, Annoyed, Guilty, Eye-Opener (CAGE), or the Mini International Neuropsychiatric Interview (MINI). Some measures assess the use of one substance, while others assess various substances. In some cases, measures include specific domains or frequency and intensity of use. 14 This heterogeneity of instruments hampers the ability to compare study outcomes. Another issue that limits the ability to generalize study findings is the use of different types of instruments. Substance use instruments can be generic or population-specific. Generic instruments allow for comparisons across populations (refugees and non-refugees), while population-specific instruments measure aspects that are relevant to refugees or a specific group of refugees (e.g., integration into the host community). Instruments can also be uni or multidimensional. Unidimensional measures provide a global assessment of substance use, whereas multidimensional measures assess dimensions of substance use.
While studies suggest that substance use among refugees varies, it is unclear to what extent instruments capture aspects of substance use that are relevant to refugee populations, and whether they are valid and reliable measures for this population. Evaluation of instruments is of utmost importance, as they may affect the accurate detection of mental health conditions in this population group.
This comprehensive systematic review examines the suitability and psychometric properties of substance use instruments for migrants and refugees. The scope of this review is limited to the use of non-prescribed substances, especially drugs and alcohol. It does not include prescribed substances (e.g., opioid dependence in people with chronic pain). We identify substance use instruments that have been used in migrant and refugee populations and evaluate the item content relevance to this population, as well as the instruments’ properties. In line with expert recommendations, that the way forward in substance use research is a holistic and multidimensional approach, 15 single-item measures are excluded from this review, as they are unidimensional and their psychometric values are unspecified. We aimed (1) to summarize existing instruments for measuring substance use and SUDs among migrants and refugees and then to classify them according to their utilization in research and/or in clinical practice, (2) to evaluate the quality of instruments in terms of their measurement properties, and finally (3) make recommendations for the selection of instruments based on best evidence synthesis.
Methods
Search Strategy
We identified articles by searching the electronic databases PubMed (NCBI), Embase (Elsevier, 1974), PsycINFO (EBSCO), CINAHL (EBSCO), Web of Science Core Collection (Clarivate Analytics), and PTSDPubs (ProQuest). The searches, developed by a medical librarian (P.A.B.), covered the key domains of refuge, forced migration, and substance use (Supplemental Table 1). Controlled vocabulary terms were included if available. Searches were carried out between September 19 and 25, 2019. No date or language restrictions were applied. In addition to electronic searches, we screened the references and citations of included full-text reports.
Study Selection
Three researchers (S.A., L.M.S., M.J.) independently screened titles and abstracts of the included records for potential inclusion and independently evaluated full texts for eligibility. Discrepancies in eligibility decisions between the reviewers were resolved by a consensus method. Studies were considered eligible for inclusion in the review if they reported findings related to alcohol or drug use among refugees and migrant populations. Inclusion criteria for articles were as follows: (1) substance use was assessed. (2) a validated substance use instrument was used. (3) Substance use was self-reported by refugees or migrants. Articles were excluded if they were not original peer-reviewed research, did not clearly identify the population as migrants or did not provide separate results for refugees or migrants, did not report any relevant findings, or used single-item instruments to assess substance use. Multiple reports from the same study were excluded unless they reported additional relevant data.
Data Extraction
Basic information (author, year, country where the study was conducted, participants’ original country, type of migrant population, number of participants, their gender, age range, mean age and standard deviation [SD], mental health measures used, setting) and information about substance use measures (instrument name, type, substance, domain, recall period) were extracted from included articles. Before assessing the measurement properties of an instrument, descriptive variables of the instruments used in the included studies were extracted, including the short name of the instrument, country and language of questionnaire development, country in which the questionnaire was used, focus (drugs, alcohol, drug/alcohol, health, other) and type of measure (standardized, individualized, hybrid), delivery format (self-report, interview, mixed), response options (Likert scales, nominal scales, number of days/times, other), and translation modes. Data were extracted into an Excel sheet by S.A., L.M.S., M.J., and K.B. and independently reviewed by J.L.
Assessment of Content Relevance
We assessed the item content relevance of the substance use instruments used in the included studies by examining the extent to which items reflected domains relevant to refugee and migrant populations and measured substance use and SUDs, therefore indicating suitability. A thematic analysis was conducted in order to evaluate the content of the instruments that are available in the peer-reviewed literature. Information on item content was derived from the studies included in this review, from the first publication of the instruments, and from manuals. The content of substance use instruments was systematically differentiated by content analysis by 2 researchers. The researchers (K.-J.B. and S.A.) independently coded the instrument items. Differences in the codings and themes were discussed iteratively until a consensus was reached. The following decision rules were developed during the discussions:
The codings are intended to represent meaning, rather than the exact wording of the items.
If items are subdivided by domains in the original instrument, it is not necessary to automatically code the items according to the given domain.
If the instrument instructions indicate that an item should be considered within a specific context, it is necessary to adopt that context when coding.
Evaluation of Psychometric Properties
The methodological quality of the included studies was evaluated using recommended minimum standards that measures must meet to be considered suitable for use in scientific studies based on the criteria for psychometric properties developed by Terwee et al.16,17 The assessment was based on the information provided in the studies included in this review, first publications, and manuals. Cross-cultural validity aimed to determine the performance of the items on a translated or culturally adapted instrument and whether or not the adapted instrument adequately reflects the performance of the items of the original version of the instrument.
Best evidence synthesis was performed by applying an assessment property scoring summarized in the Supplemental Table 2, by integrating the results of the studies’ methodological qualities and the results of measurement properties of instruments. The rating included an evaluation of 6 domains (conceptual and measurement model, instrument development methodology, interpretability of scores, measurement error, internal consistencies, and validity) to rate different aspects of the measurement properties of the instruments. Each domain contains 3 items measured on a 3-point scale (2, 1, 0). A higher score indicates stronger evidence.16,17
Results
The electronic database search returned 2654 unique records. From these, 216 full-text documents were selected for full-text review, of which 55 met our inclusion criteria (Figure 1).
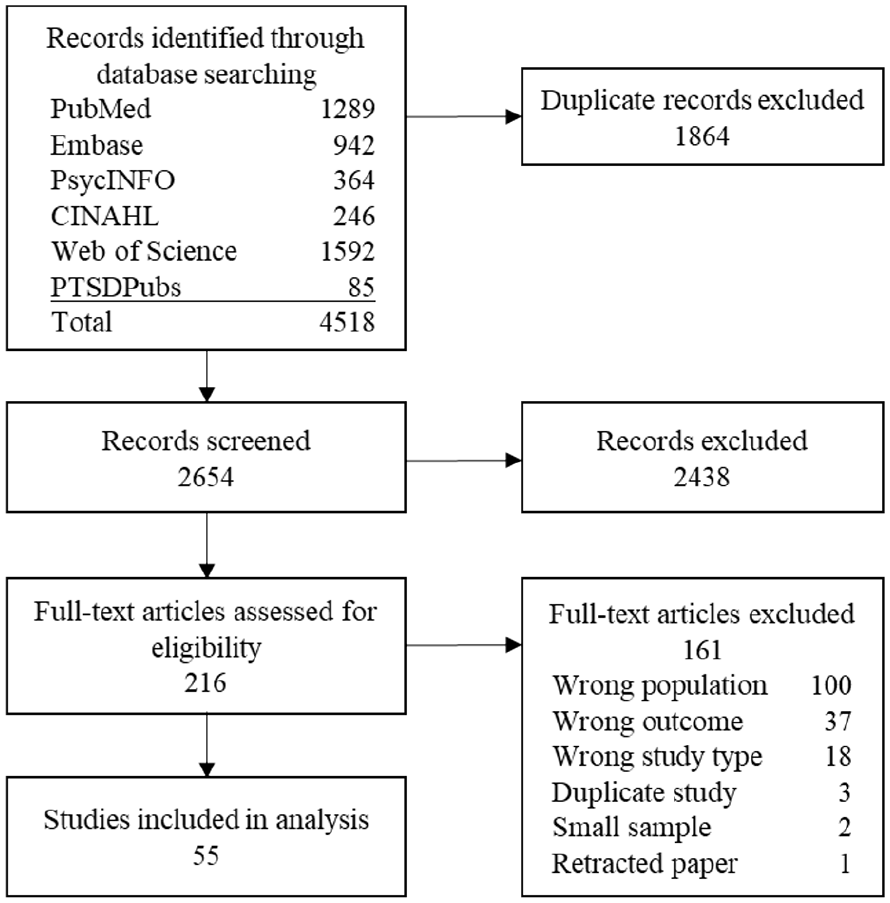
Flow chart of study selection.
Study Population
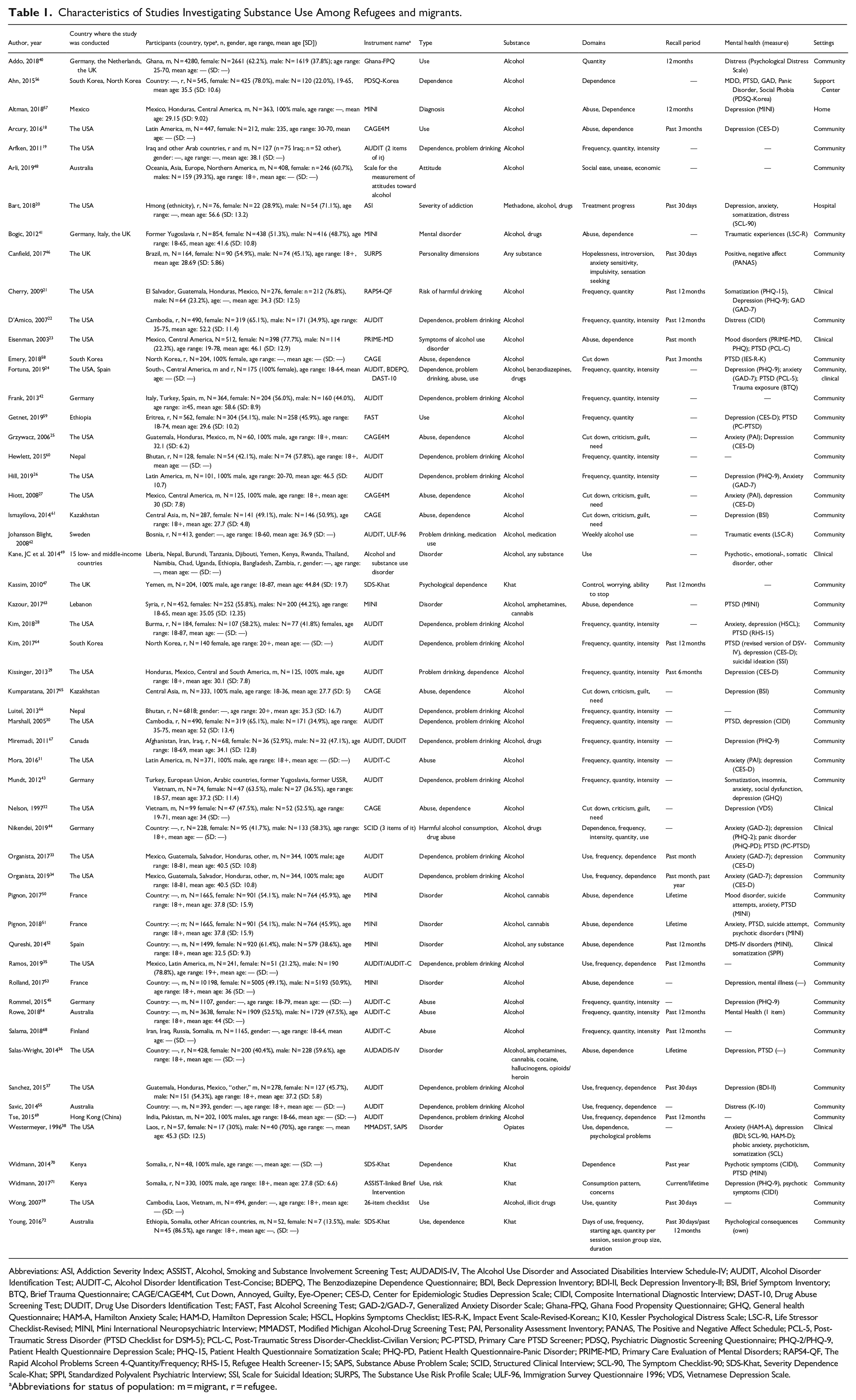
The articles reported on 41 787 individuals. Sixty-eight percent of those individuals were non-refugee migrants and 32% were refugees (Table 1), with 50.9% (n = 31) being female and 49.1% (n = 38) being male. The age range of the participants was 18 to 87 years. Most of the studies were conducted in the USA (n = 22, 40%),18-39 Germany (n = 6, 10.9%),40-45 and in the UK (n = 4, 7.3%).40,41,46,47 Twelve studies (21.8%) did not report the countries from which the refugees came.36,43-45,48-55
Characteristics of Studies Investigating Substance Use Among Refugees and migrants.
Abbreviations: ASI, Addiction Severity Index; ASSIST, Alcohol, Smoking and Substance Involvement Screening Test; AUDADIS-IV, The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV; AUDIT, Alcohol Disorder Identification Test; AUDIT-C, Alcohol Disorder Identification Test-Concise; BDEPQ, The Benzodiazepine Dependence Questionnaire; BDI, Beck Depression Inventory; BDI-II, Beck Depression Inventory-II; BSI, Brief Symptom Inventory; BTQ, Brief Trauma Questionnaire; CAGE/CAGE4M, Cut Down, Annoyed, Guilty, Eye-Opener; CES-D, Center for Epidemiologic Studies Depression Scale; CIDI, Composite International Diagnostic Interview; DAST-10, Drug Abuse Screening Test; DUDIT, Drug Use Disorders Identification Test; FAST, Fast Alcohol Screening Test; GAD-2/GAD-7, Generalized Anxiety Disorder Scale; Ghana-FPQ, Ghana Food Propensity Questionnaire; GHQ, General health Questionnaire; HAM-A, Hamilton Anxiety Scale; HAM-D, Hamilton Depression Scale; HSCL, Hopkins Symptoms Checklist; IES-R-K, Impact Event Scale-Revised-Korean;; K10, Kessler Psychological Distress Scale; LSC-R, Life Stressor Checklist-Revised; MINI, Mini International Neuropsychiatric Interview; MMADST, Modified Michigan Alcohol-Drug Screening Test; PAI, Personality Assessment Inventory; PANAS, The Positive and Negative Affect Schedule; PCL-5, Post-Traumatic Stress Disorder (PTSD Checklist for DSM-5); PCL-C, Post-Traumatic Stress Disorder-Checklist-Civilian Version; PC-PTSD, Primary Care PTSD Screener; PDSQ, Psychiatric Diagnostic Screening Questionnaire; PHQ-2/PHQ-9, Patient Health Questionnaire Depression Scale; PHQ-15, Patient Health Questionnaire Somatization Scale; PHQ-PD, Patient Health Questionnaire-Panic Disorder; PRIME-MD, Primary Care Evaluation of Mental Disorders; RAPS4-QF, The Rapid Alcohol Problems Screen 4-Quantity/Frequency; RHS-15, Refugee Health Screener-15; SAPS, Substance Abuse Problem Scale; SCID, Structured Clinical Interview; SCL-90, The Symptom Checklist-90; SDS-Khat, Severity Dependence Scale-Khat; SPPI, Standardized Polyvalent Psychiatric Interview; SSI, Scale for Suicidal Ideation; SURPS, The Substance Use Risk Profile Scale; ULF-96, Immigration Survey Questionnaire 1996; VDS, Vietnamese Depression Scale.
Abbreviations for status of population: m = migrant, r = refugee.
Description of Instruments
Among the 55 articles, we found 24 different standardized instruments (Table 2). The AUDIT was the most frequently applied instrument (n = 20, 36.4%),19,22,24,26,28-30,33-35,37,42,43,55-61 followed by62-73 the CAGE18,25,27,32,74-76 and the MINI41,50-53,77,78 (each n = 7, 12.7%). Eight instruments exclusively measure alcohol use, 5 focus on drugs and/or medication, and 11 instruments measure both alcohol and drug use. The mean number of items in the instruments was 16.3 (SD = 13.3).
Characteristics of Instruments Used in the Studies to Measure Substance Use Among Refugees and Migrants.
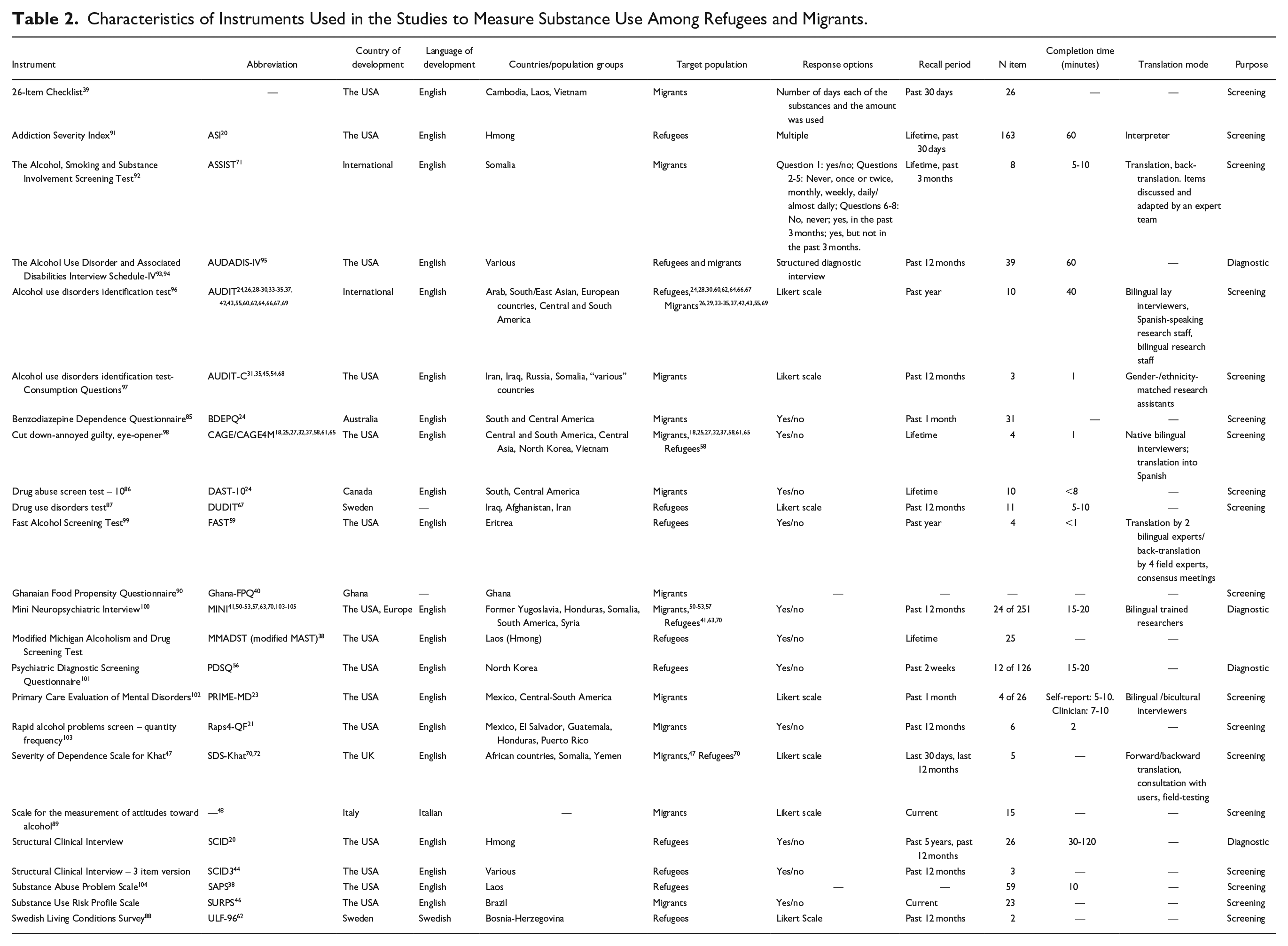
The instruments use a variety of scoring scales. These include Likert-type scales (e.g., Alcohol, Smoking and Substance Involvement Screening Test [ASSIST], AUDIT, Drug Use Disorders Identification Test [DUDIT]), binary scales (e.g., CAGE, Severity Dependence Scale [SDS]), and composite scales (e.g., Addiction Severity Index [ASI], MINI). Instruments containing domains for frequency and quantity of substance use apply frequency counts.
The instruments applied in the included studies were predominantly developed in English (n = 18, 75%) (Table 2). Moreover, the majority was developed in the USA, except the AUDIT (several countries), the BDEPQ 79 (Australia), the DAST-10 80 (Canada), the DUDIT 81 (Sweden), the ULF-96 82 (Sweden), the Scale of measurement toward alcohol 83 (Italy), the SDS-Khat 47 (UK) and the Ghana-FPQ 84 (Ghana). All instruments are available in English. Thirteen instruments (54.2%) are available in more than 2 languages. Completion time was reported for 14 instruments (58.3%) and ranged from 1 to 120 minutes (Table 2).
Description of Studies
The studies investigated substance use among persons coming from 24 specific countries around the world, mostly in Asia and South and Central America (Table 1). One study reported on the ethnicity of participants. 20 Twelve studies (21.8%) did not indicate where participants came from.36,43-45,47,48-55 Studies used translated versions of the instruments, mainly into Spanish (n = 18,32.7%)18,21,24,29,35,36,42,52,78 and French (n = 5, 9.1%).44,50-53 Furthermore, measures were translated into 28 other languages.17,20,22,28,30,32,38,39,41,42,44,46,47,50-53,56-59,61,74-76,85-91 Seven studies (12.7%) applied instruments in more than one language.39,41,42,44,85-87
Most studies investigated a variety of substances (n = 36, 65.5%)18,19,21-23,25-35,37,40,42,43,45,48,53-56,58,59,61,75,76,78,87,88,91 other exclusively alcohol use (n = 36, 65.5%),38,46,47,85,89,90 drug use (n = 13, 23.6%),20,24,39,41,44,49-52,57,60,77 or alcohol and drug use. Forty-five studies (81.8%) evaluated substance use together with other mental health conditions. Twenty-nine investigated depression,18,20,21,24-34,36-38,43-45,53,58,60,75,76,78,88,90,91 15 studies anxiety,20,21,24-28,31,33,34,38,44,50,51 and 14 Post-Traumatic Stress Disorder.23,24,28,30,36,44,50,51,58,74,77,88,89,91
Instruments were interviewer-administered in most studies (n = 41, 74.5%),18-20,22,23,25-36,38,41,43-45,47,50-53,55,56,59,60,74-78,85,87-91 self-reported (n = 8, 14.5%)40,42,46,48,54,57,58,61 or used audio computer-assisted self-interviewing (n = 5, 9.1%).21,24,37,39 Other instruments were administered heterogeneously.18,25,27,32,40,74-76 Four studies (7.3%) used instruments as a diagnostic test for SUDs.20,78,88,92
Item Content
The 469 items of 24 instruments were coded and assigned to 46 domains (Table 3).
Domains of Instruments Included in the Review.
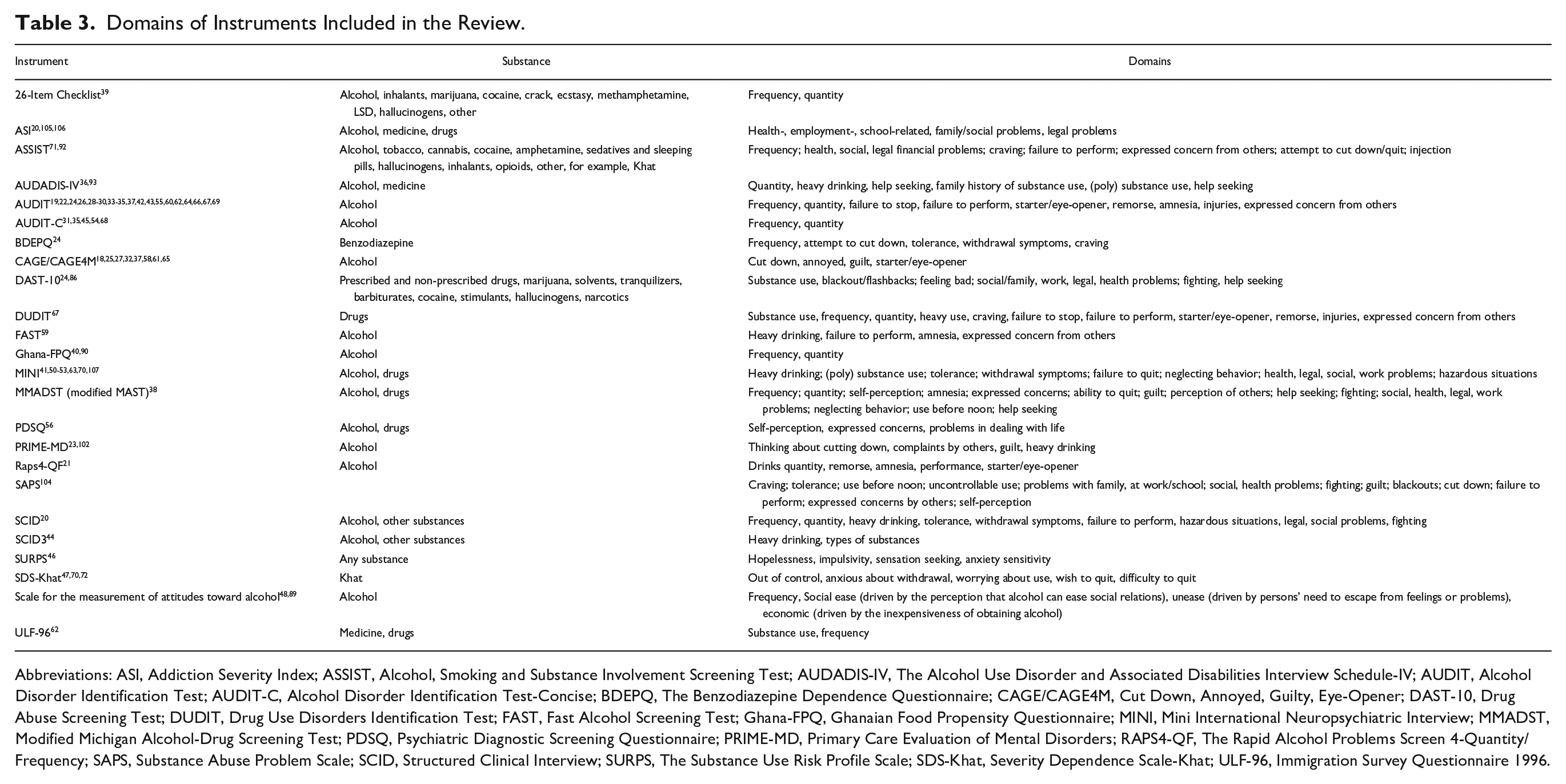
Abbreviations: ASI, Addiction Severity Index; ASSIST, Alcohol, Smoking and Substance Involvement Screening Test; AUDADIS-IV, The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV; AUDIT, Alcohol Disorder Identification Test; AUDIT-C, Alcohol Disorder Identification Test-Concise; BDEPQ, The Benzodiazepine Dependence Questionnaire; CAGE/CAGE4M, Cut Down, Annoyed, Guilty, Eye-Opener; DAST-10, Drug Abuse Screening Test; DUDIT, Drug Use Disorders Identification Test; FAST, Fast Alcohol Screening Test; Ghana-FPQ, Ghanaian Food Propensity Questionnaire; MINI, Mini International Neuropsychiatric Interview; MMADST, Modified Michigan Alcohol-Drug Screening Test; PDSQ, Psychiatric Diagnostic Screening Questionnaire; PRIME-MD, Primary Care Evaluation of Mental Disorders; RAPS4-QF, The Rapid Alcohol Problems Screen 4-Quantity/Frequency; SAPS, Substance Abuse Problem Scale; SCID, Structured Clinical Interview; SURPS, The Substance Use Risk Profile Scale; SDS-Khat, Severity Dependence Scale-Khat; ULF-96, Immigration Survey Questionnaire 1996.
Figure 2 shows a map of the 46 domains derived in the content analysis of the instruments’ items sorted by themes. Six themes were identified: Patterns of use, risk of dependence, social factors and resources, psychological factors, performance issues, and health issues. Domains related to patterns of substance, especially frequency, quantity, and heavy intensity, were most frequently assessed across instruments. Sixteen instruments (66.7%) assessed behavior related to risk of dependence, with attempts or failure to quit substance use and concerns about substance use expressed by other persons being included most often. A variety of health issues (e.g., general health problems or specific symptoms of substance use) were investigated in 11 instruments (45.8%). Domains related to the social environment (e.g., problems with other persons or getting into fights) were included in 9 instruments (37.5%). Among the least frequently assessed domains were those related to psychological factors (e.g., feelings of guilt, remorse, or worry because of substance use and other mental health symptoms. The list of articles from which the specific domains are derived is shown in Figure 2.
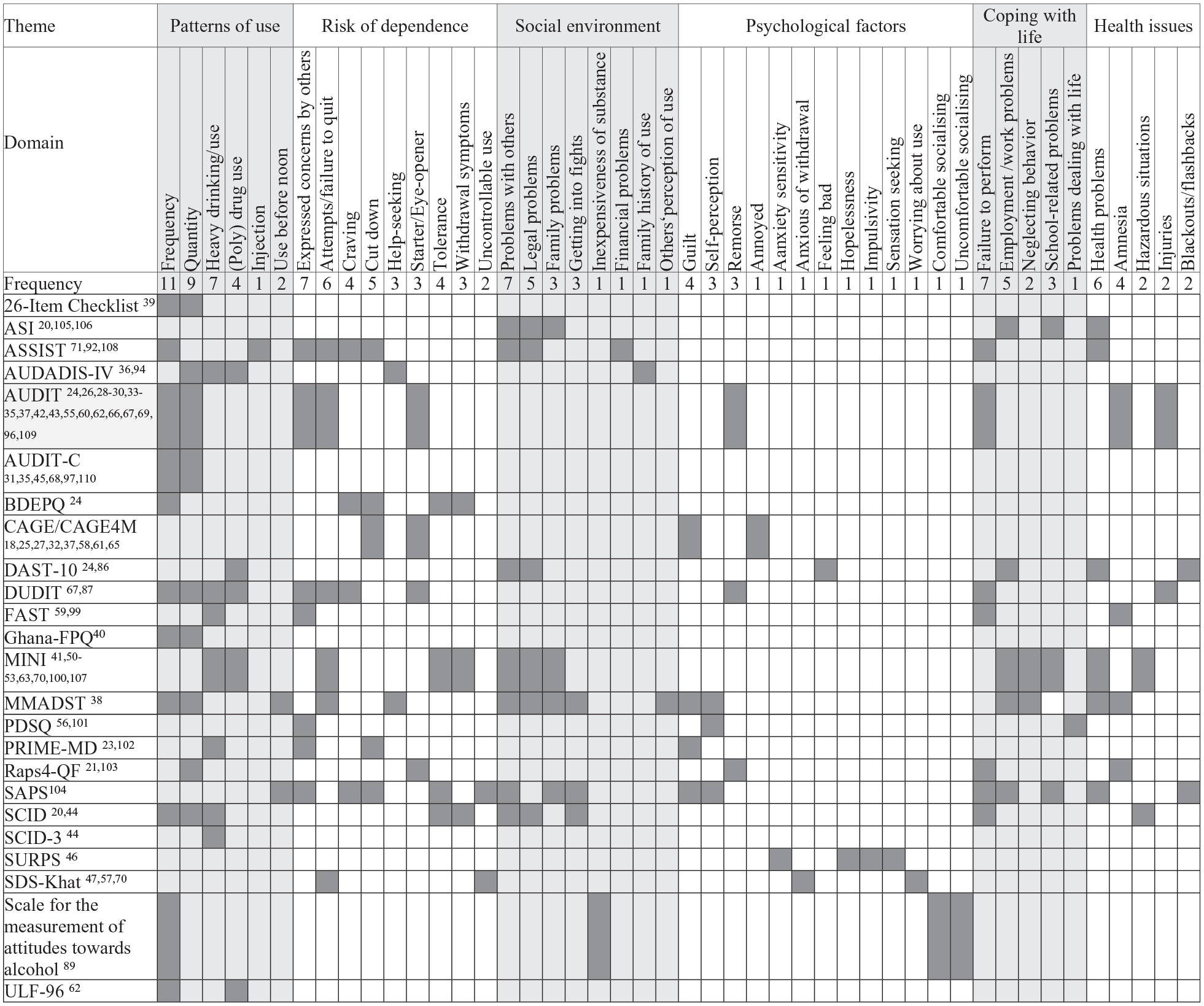
Heat map of item content in substance use instruments.
Psychometric Properties
The psychometric properties of the instruments were assessed based on Terwee’s criteria. 16 Most of the instruments performed well in internal consistency and structural validity. Indeterminate results for content validity were mainly due to insufficient information. In the absence of multiple-group confirmatory factor analysis, most results for cross-cultural validity were also indeterminate. Additionally, Pearson correlations between the instruments and these recognized gold standards were less than 0.7, indicating negative results. As a result, criterion validity showed poor overall measurement performance.
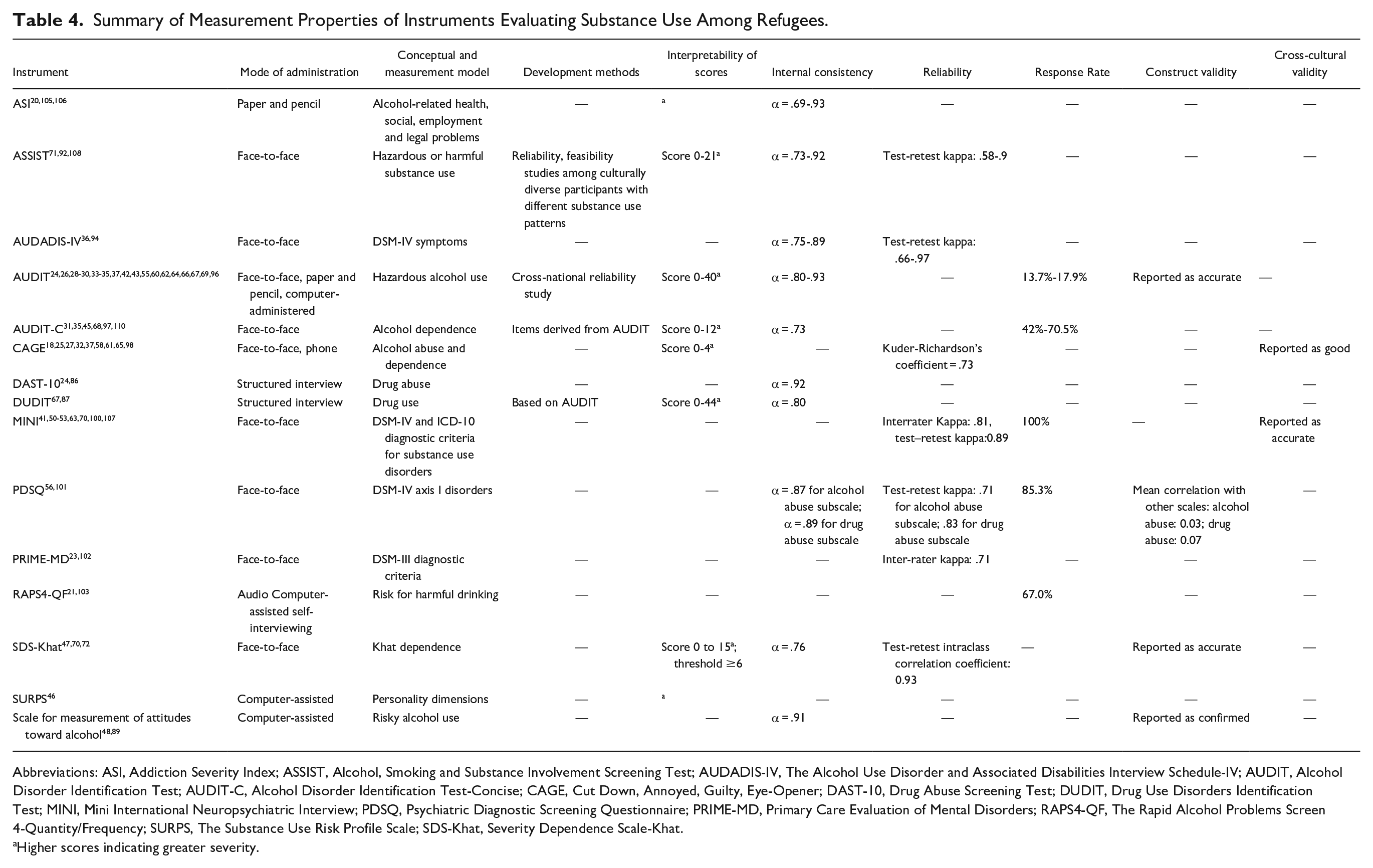
Table 4 displays the measurement properties of the substance use instruments. Some instruments have been extensively tested for their psychometric properties, such as the ASI93-98 and the AUDADIS,92,99-102 which were found to have good to excellent reliability and validity. Fourteen studies provided the response rate, which varied between 13.7% 42 and 90.2% 90 (Table 4).
Summary of Measurement Properties of Instruments Evaluating Substance Use Among Refugees.
Abbreviations: ASI, Addiction Severity Index; ASSIST, Alcohol, Smoking and Substance Involvement Screening Test; AUDADIS-IV, The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV; AUDIT, Alcohol Disorder Identification Test; AUDIT-C, Alcohol Disorder Identification Test-Concise; CAGE, Cut Down, Annoyed, Guilty, Eye-Opener; DAST-10, Drug Abuse Screening Test; DUDIT, Drug Use Disorders Identification Test; MINI, Mini International Neuropsychiatric Interview; PDSQ, Psychiatric Diagnostic Screening Questionnaire; PRIME-MD, Primary Care Evaluation of Mental Disorders; RAPS4-QF, The Rapid Alcohol Problems Screen 4-Quantity/Frequency; SURPS, The Substance Use Risk Profile Scale; SDS-Khat, Severity Dependence Scale-Khat.
Higher scores indicating greater severity.
The conceptual and measurement models were described for all instruments. Development methodologies vary considerably between them. For three of the most frequently used instruments (AUDIT, MINI, and ASSIST), items were generated with input from the target population, and the instruments were piloted. For AUDIT-C and DUDIT, items were generated with target population input, or they were piloted. For the remaining instruments, no information on development methodology was available in the selected sources.
Data on the psychometric properties of substance use instruments for refugees and migrants were scarce and incomplete. Psychometric properties were tested for 13 instruments. As responsiveness and cultural validity were not assessed for any of the instruments, they were not included in Table 4. Reliability was above the minimum acceptable value for internal consistency for 10 instruments (all Cronbach’s α ≥ .70). No information on reliability was reported for the other instruments. Content validity was not tested for any of the instruments. Construct validity was assessed for 4 instruments (AUDIT, Psychiatric Diagnostic Screening Questionnaire, SDS-Khat, and Scale for measurement of attitudes toward alcohol), although the evidence varies.
Best Evidence Synthesis
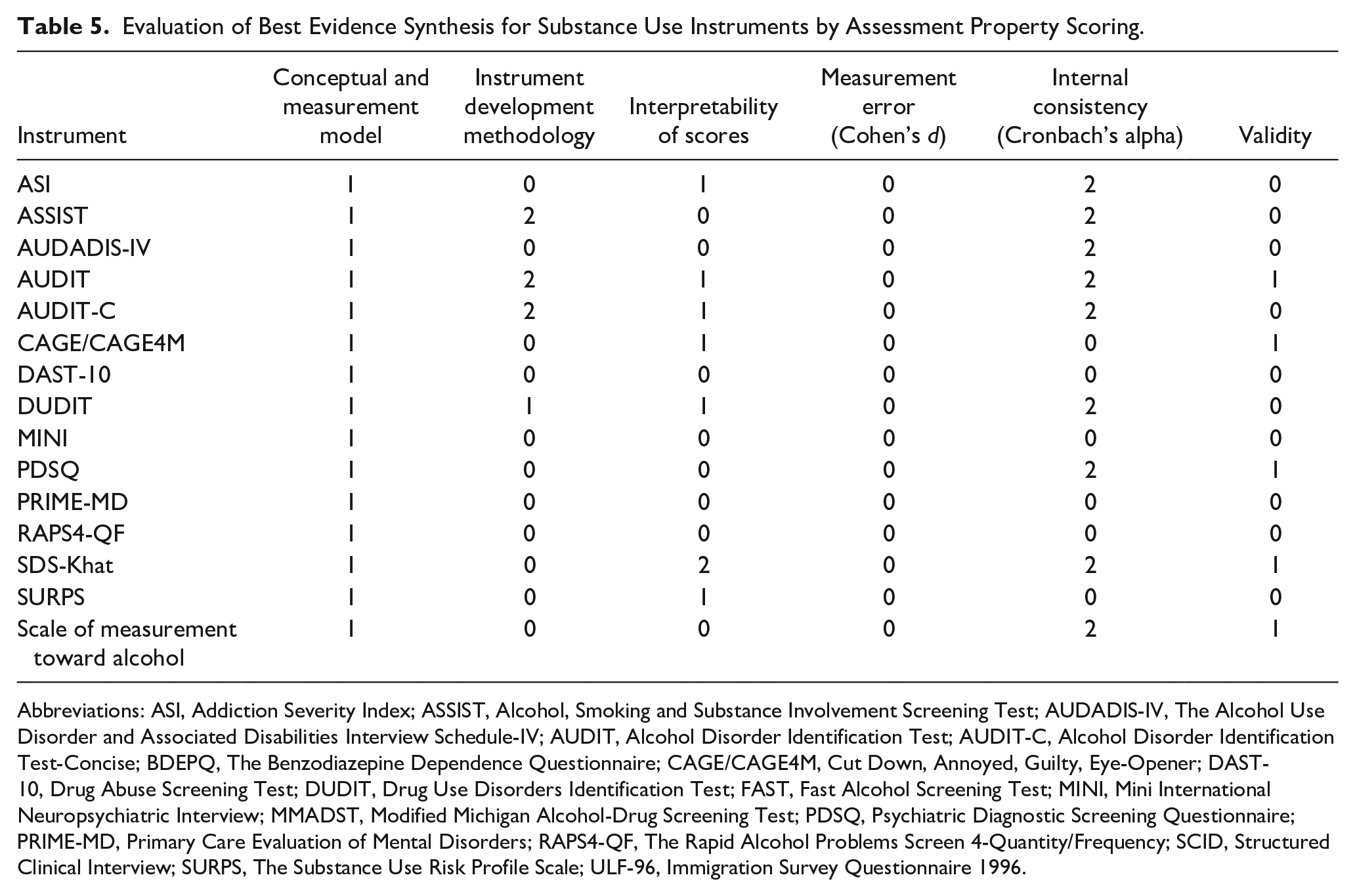
A best evidence synthesis was performed according to the method summarized in Supplemental Table 2, by integrating the studies’ methodological qualities and measurement property assessments of instruments. As none of the included studies reported on responsiveness and cross-cultural validity, these properties were not included in the best evidence synthesis. The performance of each instrument’s measurement properties is shown in Table 5. In general, the instruments performed best in the categories of internal consistency and development methodology, where 9 and 3 instruments achieved (“2”) respectively. None of the studies analyzed measurement error.
Evaluation of Best Evidence Synthesis for Substance Use Instruments by Assessment Property Scoring.
Abbreviations: ASI, Addiction Severity Index; ASSIST, Alcohol, Smoking and Substance Involvement Screening Test; AUDADIS-IV, The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV; AUDIT, Alcohol Disorder Identification Test; AUDIT-C, Alcohol Disorder Identification Test-Concise; BDEPQ, The Benzodiazepine Dependence Questionnaire; CAGE/CAGE4M, Cut Down, Annoyed, Guilty, Eye-Opener; DAST-10, Drug Abuse Screening Test; DUDIT, Drug Use Disorders Identification Test; FAST, Fast Alcohol Screening Test; MINI, Mini International Neuropsychiatric Interview; MMADST, Modified Michigan Alcohol-Drug Screening Test; PDSQ, Psychiatric Diagnostic Screening Questionnaire; PRIME-MD, Primary Care Evaluation of Mental Disorders; RAPS4-QF, The Rapid Alcohol Problems Screen 4-Quantity/Frequency; SCID, Structured Clinical Interview; SURPS, The Substance Use Risk Profile Scale; ULF-96, Immigration Survey Questionnaire 1996.
Overall, 4 instruments (DAST-10, MINI, PRIME-MD, and RAPS4-QF) performed poorer than the other instruments included in this review. Six instruments had at least 2 strong positive (“2”) or 3 moderate positive (“1”) ratings for measurement properties and were thus identified as the best rated (AUDIT/AUDIT-C, DUDIT, SDS-Khat, CAGE, ASSIST).
Discussion
Twenty-four different instruments measuring substance use in refugee populations were used in 55 articles included in this review. The item content analysis of the instruments identified 46 domains. The most frequently included domains were related to patterns of use and risk of dependence. Domains related to mental health were investigated less often. Mental health conditions, however, are frequent both in individuals using substances,103,104 and in refugee populations.105,106 In addition to mental health conditions, behavior and social roles may be affected by using substances. 107 Domains aiming at describing psychological risk assessments were the least frequently included domains. None of the included instruments contained culture- or refugee-specific domains.
A variety of scoring scales were applied in the reviewed substance use instruments, such as Likert Scales and binary responses. Comparing results between different instruments may be challenging because of the differences in scoring systems. Instruments also use different cutoff points to define problematic substance use, leading to inconsistent interpretations of risk level or problem severity. Instruments assessing different domains may further complicate comparisons, because scores in one domain may not have the same meaning as scores in another domain. The purpose of the instruments—whether for screening or diagnosis—also affects the understanding of the results, creating ambiguity in comparisons between findings.
Assessment of psychometric properties showed that some properties were not as extensively reported as others in the included studies. In particular, evidence of validity, reliability, and responsiveness was scarce. Cross-cultural validity was not reported for any of the instruments. None of the instruments had been tested for all measurement properties, but 6 instruments (AUDIT/AUDIT-C,24,29,31,33,34,42,45,55,57,59,61,87 DUDIT,60,81 SDS-Khat,47,85,89 CAGE,18,25,37,74,76 ASSIST90,108) had better performance in both methodological quality and measurement properties.
The review suggests that most instruments have been developed in English-speaking countries. Our findings are therefore in line with meta-reviews suggesting that instruments assessing mental health conditions have been developed mostly for white English-speaking populations.109-113 In place of a mere translation of instruments into languages other than those in which they were developed, we propose the utilization of more sophisticated statistical techniques for the exploration of cross-cultural performance, such as differential item functioning analysis. 114 Additionally, the sensitivity and response behavior in non-English-speaking populations were not reported. The response behavior may be similar or different. In order to gain a deeper understanding of the response behavior, it would be beneficial to conduct further studies that investigate this phenomenon in different population groups.
Despite a comprehensive and systematic literature search and consideration of a wide range of domains, including the content and psychometric properties of substance use instruments, our review has some limitations to consider. We did not investigate gray literature, which may have led to the omission of relevant studies. One shortcoming in the assessment of item content and psychometric properties might be that information was derived only from included studies that specifically investigated substance use among migrant and refugee populations, from first publications and manuals. Evidence reported in other studies outside this context was not included in the assessment and the resulting best evidence synthesis. We were not able to assess the psychometric properties of the instruments for specific substances measured and for specific groups to whom the instruments were applied. As the majority of the studies included in this review were cross-sectional, we were unable to investigate whether and how psychometric properties might change over time, for example, due to acculturation processes. Another limitation is that it was not possible to extend the search period or perform an updated search due to the limited time available to conduct this study in the context of a joint research project. With the ongoing changes related to migration worldwide, future research will benefit from conducting an updated literature review starting from 2019. Moreover, to avoid potential cultural bias and consider aspects from an emic perspective, it will be advantageous in the future to conduct reviews in heterogeneous research groups. Despite these potential shortcomings of our review, our study has several strengths, such as the structured and transparent approach to searching and evaluating instruments based on a systematic search and evaluation of studies using substance use instruments.
While research consistently shows that substance use varies among refugee and migrant populations, the use of generic instruments may have shortcomings in enhancing our comprehension of the extent of substance use and the severity of its impact. The advantage of refugee- and migrant-specific instruments is that they provide more relevant and sensitive results than generic instruments, which are applicable across populations. 115 Specific instruments may be more suitable to monitor the course of treatment and estimate its effectiveness. 116 Yet, no final recommendations can be made for instruments to be used in refugee populations, as the instruments should be validated with the population groups. Moreover, it might be necessary to conduct research on “idioms of distress” and “idioms of substance use” employing interdisciplinary research methods. Idioms of distress are specific ways of communicating emotional suffering and refer to the culturally mediated ways of experiencing distress and emotions.107,117,118
Conclusion
To our knowledge, this is the first systematic review of instruments used to measure substance use among migrants and refugees. The results highlight the advantages and limitations of existing instruments. Considering the limitations, it might be necessary to conduct further research into the cultural idioms of distress associated with substance use and to consider incorporating these aspects into specific instruments.
Supplemental Material
sj-docx-1-saj-10.1177_29767342251348146 – Supplemental material for Measuring Substance Use in Refugees: A Systematic Review of Assessment Instruments
Supplemental material, sj-docx-1-saj-10.1177_29767342251348146 for Measuring Substance Use in Refugees: A Systematic Review of Assessment Instruments by Jutta Lindert, Kim-Julian Behr, Sarah Arndt, Marija Jakubauskiene, Paul A. Bain, Sascha Milin, Lisa Marie Schuh and Ingo Schäfer in Substance Use & Addiction Journal
Footnotes
Acknowledgements
We thank Martha Nathan for contributing to the study.
Author Contributions
All authors have been actively involved in this study and contributed substantially. In particular, J.L. has designed the study, supervised data searches and analysis, and written the first draft of the manuscript. K.B. and S.M. have collaborated in screening and data extraction. J.L. and K.B. conceptualised the data analysis. K.B. has analysed the data and contributed to the preparation (writing) of the manuscript. M.J. has collaborated in screening and data extraction. P.A.B. and J.L. have conceptualised the search. P.A.B. has done the systematic search. All authors have contributed to the final manuscript.
Data Availability Statement
All data generated or analysed during this study are included in this article. Electronic database searches and assessment criteria are provided in the Supplemental Material.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the German Federal Ministry of Education and Research (grant no. 01EF1805A-E). The funding sources were not involved in any stage of the study design, collection/analysis/interpretation of data, writing the report, or in the decision to submit the article for publication.
Compliance,Ethical Standards,and Ethical Approval
An ethics statement is not applicable because this study is based exclusively on published literature.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.