
Abstract
Introduction:
During the postpartum period, new parental responsibilities may compound changing social, community, and health care environments to increase risk of health and drug-related problems. This study examines both county-level and individual-level factors associated with hospitalization among individuals with opioid use disorder (OUD) throughout the first-year postpartum.
Methods:
A cohort of individuals with OUD at delivery were identified in Pennsylvania hospital discharge data (n = 1966). Multilevel logistic regression models examined county-level (median household income, rurality, jail rate, OUD treatment facilities, hospital beds) and individual-level (demographics, insurance, tobacco use, other substance use disorders, mental health conditions) factors associated with inpatient hospitalizations (all-cause, OUD-related, mental health-related) in the early (0-42 days) and late (43-365 days) postpartum periods.
Results:
In total, 280 individuals (14%) with OUD had at least 1 hospitalization in the first-year postpartum. After adjustment, higher county densities of OUD treatment facilities were associated with lower odds of all 3 types of hospitalizations in early postpartum, including 80% to 86% reduced odds of OUD-related hospitalizations for those in counties with the 3 highest quartiles of treatment facility densities compared with the lowest quartile. These associations did not remain significant in late postpartum. All maternal age groups, compared with those aged 25 to 29, had increased odds of a mental health-related hospitalization in early postpartum, and the youngest age group (17-24 years) had increased odds in late postpartum. Experiencing any hospitalization from 0 to 42 days postpartum was positively associated with all 3 types of hospitalizations in late postpartum.
Discussion:
County health care and drug treatment systems are associated with hospitalizations among individuals with OUD throughout the first-year postpartum. Addressing policy, sociocultural, and structural barriers to accessing these services should be a priority for improving postpartum health and reducing drug-related harms in this period.
Keywords
Highlights
Individual-level and county-level factors may impact postpartum health and drug use.
Hospitalizations in early and late postpartum among those with opioid use disorder (OUD) were examined.
Higher OUD treatment densities were associated with lower early postpartum hospitalizations.
Individual factors, such as maternal age or mental health conditions, were associated with postpartum hospitalizations.
Addressing postpartum social and structural barriers to health care and treatment is critical.
Introduction
Opioid-related mortality is a leading cause of death in the first-year postpartum.1-5 During this period, new parental responsibilities may compound changing social, interpersonal, health care, and community environments to increase risk of overdose and related health problems.6-9 The contexts of these environments may increase vulnerability to adverse drug-related outcomes among persons with opioid use disorder (OUD) during this vulnerable life stage. Contrastingly, communities with better access to health services, drug treatment facilities, and social resources may mitigate these outcomes. As the drug crisis continues to impact communities across the United States, understanding the social and structural contexts that impact vulnerable pregnant and postpartum populations remains essential. 10
The association of community environments to opioid use and overdose have been well documented in the general US population.11-15 These contextual factors have most commonly been examined at the county level, where overdose and mortality data are widely available and at which state resources are often allocated. A systematic review of county-level factors found that economic disadvantage, incarceration, opioid prescribing rates, and family distress were the most common factors positively associated with opioid mortality in the general population. 16 Other potentially important county-level correlates of opioid use and mortality include rurality and access to health care services and drug treatment.14,17 While rural counties in the United States have had the greatest increases in prescription opioid supply, the largest burden of opioid overdose and mortality remains in urban counties.18-20 Access to health care and drug treatment also varies greatly by geographic region,21,22 and hospital bed size in a county, reflecting overall health system capacity, has been inversely associated with opioid mortality. 13
Among the general population of pregnant persons, community-level and county-level factors have been linked to severe maternal morbidity, maternal mental health, and preterm birth,23-28 of which many of these outcomes disproportionately impact individuals with OUD.29-31 Limited research has examined county-level contextual factors associated with health or opioid-related problems among high-risk groups of pregnant and postpartum persons with OUD.32,33 Polysubstance use patterns, for instance, among pregnant persons with OUD may differ in rural and urban counties. 34 Yet, little information exists about how county environments increase or protect against adverse health-related and drug-related outcomes in the postpartum period. For instance, geographic availability of and access to medication for OUD (MOUD) and other drug treatment are essential for preventing drug overdose in the postpartum period.35,36
This study aimed to examine the relationship between county-level factors and hospitalizations during the first-year postpartum among a cohort of persons with OUD. Using Pennsylvania statewide hospital discharge data, we simultaneously examined the associations between both residential county-level factors and individual-level factors, such as demographics and co-occurring substance use disorders (SUDs) and mental health conditions, with 3 types of postpartum hospitalizations: all-cause, OUD-related, and mental health-related. Our goal was to identify specific factors associated with OUD-related and other types of hospitalizations to inform community and structural interventions among this postpartum population.
Methods
We used inpatient discharge records from the Pennsylvania Health Care Cost Containment Council (PHC4), a state-run agency that collects hospital discharge data from all non-federally run hospitals and ambulatory centers in the state. A cohort of all females in the calendar year 2018 who had a hospital delivery record with an OUD diagnosis code (ICD-10 codes used are presented in Supplemental Table 1) was identified. Delivery served as the index hospitalization, and all subsequent inpatient hospitalizations across the state for the individual in the first-year postpartum (2018-2019) were identified and included. Study protocols were deemed exempt by the Institutional Review Board at the University of Pittsburgh.
In total, 2086 individuals with OUD in Pennsylvania had a delivery hospitalization in 2018. Analyses excluded 31 non-Pennsylvania residents, 26 individuals with invalid identification numbers who could not be tracked for postpartum hospitalizations, and 45 individuals missing race/ethnicity data (see the CONSORT diagram in Supplemental Figure 1). The remaining sample of 1984 individuals resided in 65 of 67 Pennsylvania counties. Two counties (Cameron and Forest), both considered rural, had no residents in the sample with delivery records with OUD in 2018. Of the remaining 65 counties, 7 (McKean, Montour, Potter, Snyder, Sullivan, Union, and Warren) had <4 individuals in our sample, resulting in statistical power limitations. Thus, individuals residing in these counties (n = 13) were removed from the analysis. One additional county (Juniata) was removed due to missing county-level data, excluding 5 individuals. This resulted in a total analytical sample of 1966 individuals at delivery residing in 57 counties. Individuals excluded from the final sample were more likely to have private health insurance at delivery than those included in the sample (22.5% vs 12.7%, P = .007), but did not significantly differ in any other patient-level characteristic, including age, race/ethnicity, tobacco use or other SUD, or mental health condition.
Measures
Hospitalization records consisted of a primary and up to 17 secondary diagnosis codes, 5 procedure codes, basic patient demographics, and residential county and ZIP code. Delivery hospitalizations were linked to all postpartum hospitalizations up to 365 days following delivery. Postpartum records additionally included the number of days between the delivery index hospitalization and each new postpartum hospitalization.
Postpartum Hospitalization Outcomes
All new hospitalizations within 1 year of delivery were examined. Transfers to other acute care hospitals or units within the same hospital were not considered a separate hospitalization. If a patient was transferred or discharged to a specialty hospital or unit distinct from the index hospitalization (eg, transferred to psychiatric hospital following delivery), the second admission was considered a separate hospitalization (n = 6). Outcomes included 3 types of hospitalizations: all-cause, OUD-specific, and mental health-related hospitalizations. All-cause hospitalizations included all postpartum inpatient admissions, for any reason, including OUD-related and mental health-related hospitalizations. Hospitalizations were designated as OUD related or mental health related if any ICD-10-CM codes for these conditions were present in the primary or any secondary diagnosis codes (Supplemental Table 1). OUD hospitalizations included those with a diagnosis code for OUD or an unintentional opioid overdose/poisoning. Mental health-related hospitalizations included those with a diagnosis code for depression, anxiety, bipolar disorder, self-harm or suicidal ideation, and schizophrenia or delusional disorders.
All postpartum hospitalizations were classified into 2 time periods: early postpartum (0-42 days post-delivery) and late postpartum (43-365 days post-delivery). Six weeks (or 42 days) indicates the end of the subacute postpartum period, 37 corresponding to the resolution of biological changes related to pregnancy and the recommended postpartum care visit occurring historically between 4 and 6 weeks. Given these biological, health care, and other social and interpersonal factors that may differ throughout the first-year postpartum, all outcomes are examined separately in each time period.
County-Level Contextual Factors
Each hospital record contained the patient’s residential county, and individuals were assigned to their residential county at delivery hospitalization. While we could determine whether an individual moved counties from the time of delivery to a postpartum hospitalization, we could not assess whether individuals moved counties among those who were not hospitalized during this period. Thus, counties were considered time-invariant and the residential county at delivery hospitalization was considered an individual’s county for the entire 1-year period.
County-level data were obtained for the year 2018, in which all deliveries in the sample occurred, or the most recent year data were available. County annual household median income was obtained from the 2018 American Community Survey 5-year estimates 38 and rescaled to per $10 000 USD. Counties were classified using the National Center for Health Statistics Urban-Rural Classification Scheme for 2013, 39 the most updated available, which classifies counties into 6 categories. We collapsed these categories to form 3 urban-rural county classifications: (1) central/fringe metro; (2) medium/small metro; and (3) micropolitan/noncore. The 2018 rate of incarceration in jails per 100 000 county residents, representing the average number of residents in local jails in the county at a given time, was obtained from the Vera Institute’s Pennsylvania Incarceration Trends. 40 This rate was rescaled to per 10 000 residents.
Reflecting health care system capacity in a county, the number of hospital beds in non-federally run acute care hospitals in 2018 was obtained from the Pennsylvania Department of Health 41 and rescaled to a rate of beds per 10 000 residents. OUD treatment facilities were obtained from the 2018 National Directory of Drug and Alcohol Abuse Treatment Facilities. 42 Facilities that did not treat OUD were excluded. These data include facilities identified as substance use treatment facilities or programs and may not include individual providers that prescribe buprenorphine who are not based at one of these facilities. OUD treatment facilities per 100 000 county residents was calculated and then categorized into quartiles by county, corresponding to <2.4, 2.5 to 3.3, 3.4 to 4.3, and 4.4 or more treatment facilities per 100 000 county residents. Mental health professional shortage areas in 2018 were obtained at the county-level from the Pennsylvania Department of Health. 43 These shortage areas are determined by the Health Resources and Services Administration based on the population-to-mental health provider ratio.
While other Census-derived county-level variables, such as education, unemployment, and owner-occupied housing, were originally examined, they were removed from final analyses due to multicollinearity with county median household income (data not shown).
Individual-Level Factors
Patient demographics, including age (17-24, 25-29, 30-34, 35+), race/ethnicity (non-Hispanic [NH] Black, Hispanic/Latino, NH White), and primary insurance (public vs private), were included from the delivery record. Those with public insurance included 96% who had Medicaid and 4% who had Medicare. Co-occurring SUDs and mental health conditions were identified on delivery records and dichotomous variables for tobacco use, other SUDs (including alcohol, cannabis, cocaine, sedatives, and/or stimulants), and mental health disorders (including depression, anxiety, bipolar disorder, schizophrenia, and/or delusional disorders) were created. Delivery type (Cesarean vs vaginal) and pregnancy-related conditions, including anemia, pre-existing or gestational diabetes, hypertension, and pre-eclampsia, were obtained from delivery records (Supplemental Table 1).
Analysis
In Stata version 16 (College Station, TX, USA), the relationship between postpartum hospitalizations and both county-level and individual-level factors was examined using multilevel logistic regression models, allowing hospitalizations to vary by county. Six total models were fit, examining each of the 3 outcomes (all-cause, OUD-related, and mental health-related hospitalizations) separately in the early and late postpartum periods. All models included county-level contextual characteristics and individual-level factors. In the models examining hospitalizations in late postpartum (43-365 days post-delivery), a dichotomous independent variable for having any hospitalization in early postpartum (0-42 days post-delivery) was additionally included.
We conducted 2 additional sensitivity analyses. First, a sensitivity analysis examined pregnancy-related variables. Models for each of the 3 outcomes, as described above, were fit with and without the pregnancy-related variables (delivery type, anemia, preexisting or gestational diabetes, hypertension, and preeclampsia). Model fit was examined using the log-likelihood and likelihood-ratio test. Second, a similar sensitivity analysis was conducted to assess mental health providers availability and the relationship with mental health-related hospitalizations. Models of mental health-related hospitalizations in both early and late postpartum were fit with and without a county-level variable of mental health shortage areas and model-fit was assessed.
Results
Among the 1966 individuals with OUD at delivery (Table 1), the majority were between ages 25 and 34 (69.3%) and had public health insurance at delivery (87.3%). A minority were identified as NH Black (8.6%) or Hispanic/Latino (2.5%). Co-occurring conditions were commonly documented at delivery, with 62.9% having tobacco use, 18.8% another SUD, and 36.8% a mental health disorder. Among the 57 counties included, there was an average of 34.5 (standard deviation = 46.3) individuals in the sample at delivery residing in each county. Approximately half of the sample resided in 13 central/fringe metro counties (n = 974; 49.5% ), a third in 23 medium/small metro counties (n = 675; 34.3%), and a sixth in 21 micropolitan/noncore counties (n = 317, 16.1%). OUD treatment facilities varied greatly by county, with an average of 8 facilities per county (median = 5, range = 0-79).
Individual-level (n = 1966) and County-level (n = 57) Factors Among Persons With OUD at Delivery Hospitalization.
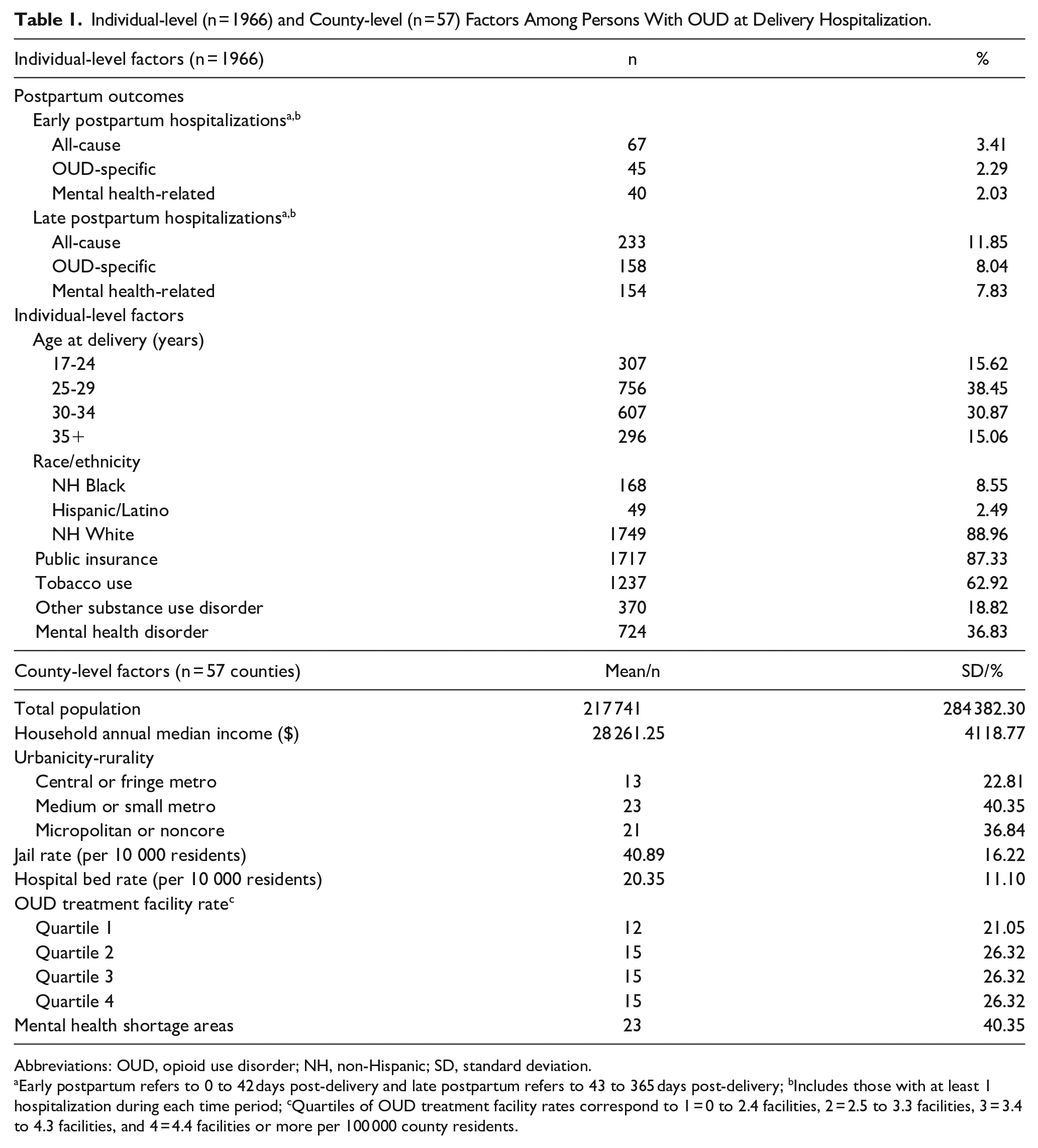
Abbreviations: OUD, opioid use disorder; NH, non-Hispanic; SD, standard deviation.
Early postpartum refers to 0 to 42 days post-delivery and late postpartum refers to 43 to 365 days post-delivery; bIncludes those with at least 1 hospitalization during each time period; cQuartiles of OUD treatment facility rates correspond to 1 = 0 to 2.4 facilities, 2 = 2.5 to 3.3 facilities, 3 = 3.4 to 4.3 facilities, and 4 = 4.4 facilities or more per 100 000 county residents.
In total, 280 individuals with OUD (14.2%) had at least 1 inpatient hospitalization within 1 year of delivery (Table 1), with an average of 1.7 hospitalizations (median = 1) among those hospitalized at least once. Sixty-seven (3.4%) and 233 (11.9%) individuals were hospitalized at least once for any reason in the early (0-42 days) and late (43-365 days) postpartum periods, respectively. Of those who had at least 1 hospitalization in late postpartum, 20 (8.6%) had previously been hospitalized in the early postpartum period. In total, 190 individuals (9.7%) had at least 1 OUD-related hospitalization within the first-year postpartum, with 42 (22.1%) having OUD as the primary diagnosis code on at least 1 hospitalization. Similarly, 179 individuals (9.1%) had at least 1 mental health-related hospitalization, with 66 (36.9%) having a mental health condition as the primary diagnosis code on at least 1 hospitalization. Of those who experienced a mental health-related hospitalization, individuals had anxiety (67.6%), depression (57.5%), and bipolar disorder (30.7%) most commonly documented at discharge.
In multivariable models of all-cause hospitalizations (Table 2), individuals living in counties in the second (adjusted odds ratio [AOR] = 0.36, 95% confidence interval [CI] = 0.14-0.90), third (AOR = 0.30, 95% CI = 0.12-0.74), or highest (AOR = 0.48, 95% CI = 0.19-1.19) quartile of OUD treatment facility densities, compared with those in the lowest quartile, had decreased odds of a hospitalization in early postpartum, although it was not statistically significant in the highest quartile versus the first. This association was not significant in any quartiles in late postpartum. Those with another SUD (other than OUD or tobacco) at delivery had higher odds of a hospitalization in early postpartum (AOR = 1.80, 95% CI = 1.04-3.12), but also did not significantly differ in odds in late postpartum. Having any hospitalization in early postpartum was associated with 3.2 times the odds of having a hospitalization in late postpartum (95% CI = 1.84-5.66). We did not detect an association between any other county-level or individual-level factors with all-cause hospitalizations in either period.
Individual-level and County-level Factors Associated With All-Cause, OUD-Related, and Mental Health-Related Hospitalizations From 0 to 42 Days and 43 to 365 Days Postpartum Among Persons With OUD (n = 1966).
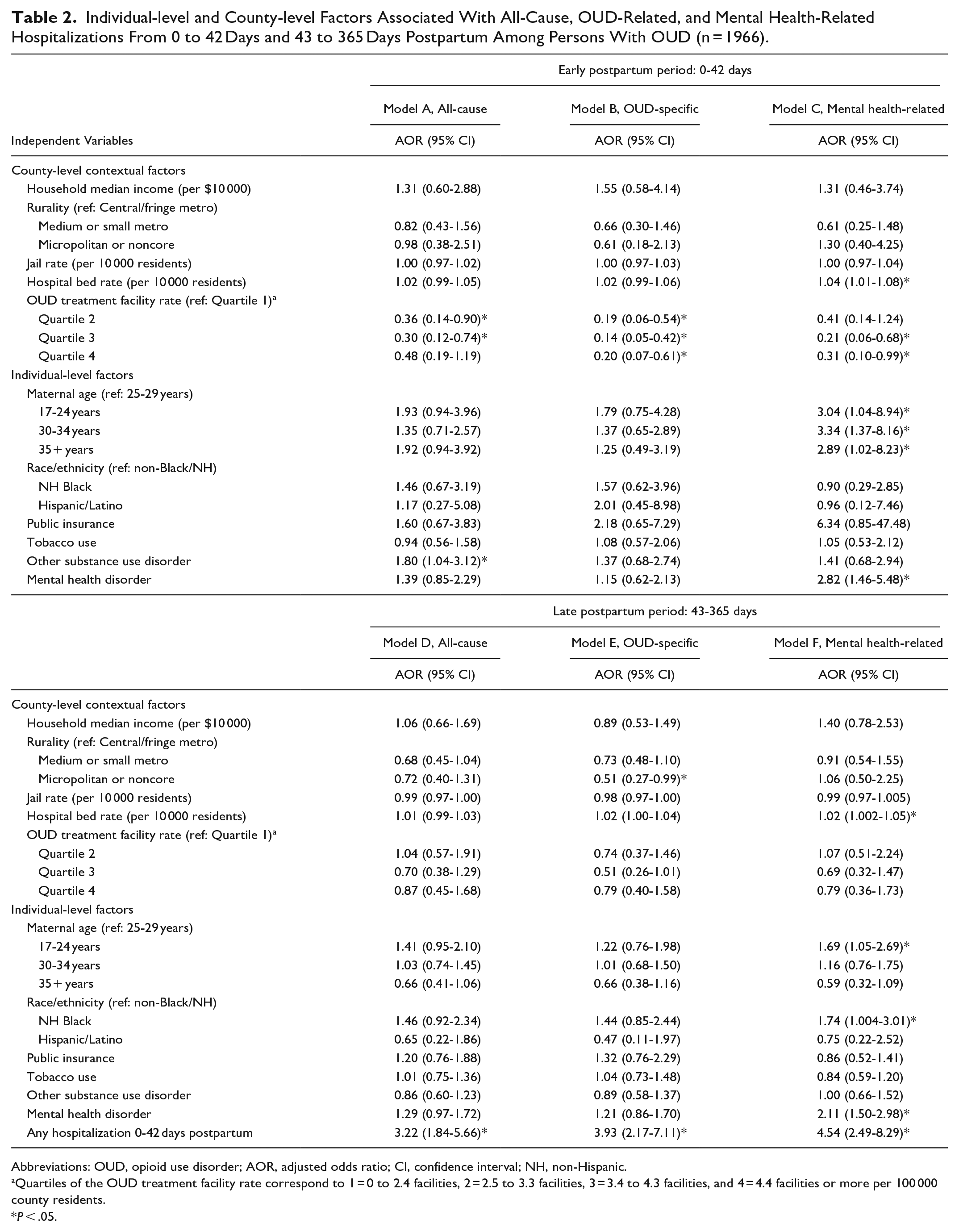
Abbreviations: OUD, opioid use disorder; AOR, adjusted odds ratio; CI, confidence interval; NH, non-Hispanic.
Quartiles of the OUD treatment facility rate correspond to 1 = 0 to 2.4 facilities, 2 = 2.5 to 3.3 facilities, 3 = 3.4 to 4.3 facilities, and 4 = 4.4 facilities or more per 100 000 county residents.
P < .05.
In models examining OUD-related hospitalizations, living in a county with a higher rate of OUD treatment facilities was strongly associated with lower adjusted odds of OUD-related hospitalizations in early postpartum. Compared with those living in counties in the lowest quartile of OUD treatment facilities rates, those in counties in all other quartiles had between 80% and 86% lower odds of experiencing an OUD-related hospitalization in early postpartum. Similar to all-cause hospitalizations, this association did not remain from 43 to 365 days postpartum. In late postpartum, those in micropolitan/noncore counties (most rural) had approximately half the odds of an OUD-related hospitalization than those in central/fringe metro counties (most urban) (AOR = 0.51, 95% CI = 0.27-0.99). Having any hospitalization from 0 to 42 days postpartum was associated with increased odds of having an OUD-related hospitalization from 43 to 365 days postpartum (AOR = 3.93, 95% CI = 2.17-7.11).
Mental health-related hospitalizations were associated with county-level and individual-level factors in both time periods. After adjustment, the rate of hospital beds per 10 000 county residents was associated with slightly increased odds of experiencing a mental health-related hospitalization in both early (AOR = 1.04, 95% CI = 1.01-1.08) and late (AOR = 1.02, 95% CI = 1.002-1.05) postpartum. In early postpartum, compared with those in counties with the lowest quartile of OUD treatment facilities, those in all other quartiles also had between 59% and 79% decreased odds of a mental health-related hospitalization, although it was not statically significant in the second quartile versus the first. Like other types of hospitalizations, this association did not remain in the late postpartum period. All age groups, compared to those aged 25 to 29, had ~3 times the odds of a mental health-related hospitalizations in early postpartum. In late postpartum, those aged 17 to 24 compared with 25 to 29 (AOR = 1.69, 95% CI = 1.05-2.69) and who identified as NH Black versus non-NH Black/NH (AOR = 1.74, 95% CI = 1.004-3.01) had increased odds of a mental health-related hospitalization. As expected, having a mental health disorder documented at delivery was associated with 2.8 and 2.1 times the odds of mental health-related hospitalizations in early and late postpartum, respectively. Having any hospitalization from 0 to 42 days postpartum was strongly associated with increased odds of a mental health-related hospitalization in the later period (AOR = 4.54, 95% 2.49-8.29).
Lastly, delivery type and pregnancy-related conditions were not associated with any postpartum hospitalizations in analyses. A sensitivity analysis of pregnancy-related variables found no substantial differences in model results or fit when removing these variables from multivariable models (data not shown). Thus, the more parsimonious models without these variables were presented (Table 2). Similarly, the sensitivity analysis of county-level mental health professional shortage areas in relation to mental health-related hospitalizations found no differences in the model results or fit. Mental health shortage areas were not independently associated with mental health-related hospitalizations in either the early or late postpartum period (data not shown) and was therefore not included in final models.
Discussion
This study examined county-level and individual-level factors associated with hospitalization in the first-year postpartum among individuals with OUD. We found that ~14% of the sample experienced at least 1 postpartum hospitalization, comparable to other published rates of postpartum hospitalizations among those with OUD 44 and substantially higher than the general postpartum population.45-47 Overall, our findings emphasize the importance of county health service availability, especially drug treatment. We found reductions in the odds of all types of hospitalizations among individuals living in counties with greater OUD treatment facility densities in the early postpartum period. This positive finding contributes to previous evidence that increased drug treatment and MOUD access can help prevent overdoses and opioid-related problems.14,35,36 Moreover, the reduced rates of all-cause and mental health-related hospitalizations associated with treatment facility availability highlight the potential role of drug treatment in the overall health of this population. Increasing access to drug treatment should be a major component of any community opioid crisis strategy and overdose prevention plans for vulnerable populations, especially during critical windows such as the early postpartum period.
While the reduction in OUD-related hospitalizations associated with treatment availability in early postpartum is promising, this association did not remain for any type of hospitalization in the late postpartum period (43-365 days post-delivery). This is concerning, as previous research has suggested that the highest overdose rates occur in late postpartum.36,48,49 It is possible that individual buprenorphine providers, which are not included in our treatment facilities variable, are particularly important in this period and account for the lack of association between county OUD treatment facilities and late postpartum hospitalizations. Though, this is unlikely given that research suggests MOUD utilization, particularly buprenorphine, drops considerably postpartum.6,50-52 Rather, the lack of association between hospitalizations and treatment availability may indicate the importance of accessibility, rather than just geographic availability, of opioid treatment in the late postpartum period. One barrier to drug treatment is the discontinuity postpartum of health insurance and Medicaid, the primary insurer of persons with OUD and more than 85% of individuals in our total sample at delivery. During the period of this study, Medicaid eligibility after 60 days postpartum decreased in most states, including Pennsylvania, leading some to lose access to health services and drug treatment. 53 Our study could not assess continuous Medicaid enrollment and eligibility status, and we were thus unable to evaluate the loss of coverage postpartum. Nevertheless, given recent Medicaid expansions to increase postpartum coverage to a full-year post-delivery, research will need to reevaluate this relationship in communities. Other mechanisms, such as other social and structural barriers to treatment, may play a substantial role in limiting treatment access and utilization and should be further considered in future research. For instance, qualitative research has identified a number of barriers to treatment among pregnant and parenting populations, including child custody concerns, mental health conditions, intimate partner violence, stigma, childcare, and limited treatment openings.54-58 County treatment availability is likely not enough to overcome this multitude of barriers, making treatment inaccessible even when availability in a community is adequate. Interventions should aim to address these interpersonal and structural barriers and assess the effect of reducing these barriers in preventing health-related and opioid-related problems postpartum.
Mental health-related hospitalizations were positively associated with the hospital bed size per 10 000 residents throughout the first-year postpartum. This finding may speak to the lack of appropriate mental health providers in communities even in regions with overall health system capacity, leading individuals who need mental health care to seek it in locations where it is readily available such as hospitals. 59 While mental health professional shortage areas were not independently associated with mental health-related hospitalizations in our sensitivity analyses, hospital bed size rates remained positively associated in both postpartum periods, even when controlling for these shortage areas. This indicates the independent effect of county hospital bed capacity and may suggest that at least some mental health care is being received, even if only through inpatient hospitalizations. Generally, more severe cases or episodes result in an inpatient mental health admission, and outpatient mental health care, including in primary care, and prevention programs should be available and accessible in all communities. 60
Other than health services and drug treatment access, few other county-level contextual factors were associated with hospitalizations in the first-year postpartum. This contrasts with research among the general population, which has found associations between county-level opioid-related outcomes and income, incarceration, and urbanicity. 16 In pregnancy and postpartum, it is possible that other individual-level factors and health care services play a more prominent role in hospitalizations than outside of the perinatal period, 33 potentially limiting the association between these county-level factors. Moreover, other studies often examine drug-use outcomes among the general population, while our study specially examines a high-risk group with an already-diagnosed OUD, who may have differing exposures, risk and protective factors, and determinants that contribute to these outcomes than those found in other studies. It is also possible there is a mismatch between the county and the most important spatial resolution for these factors related to hospitalizations in the postpartum period. For example, household median income may have the strongest effect at a more resolved spatial unit, such as neighborhoods or census tracts, rather than at the county level. Further research is needed to investigate these contextual factors among a variety of high-risk groups and at differing spatial resolutions to ensure interventions are appropriately targeted to and implemented in communities in which they will be most effective.
Mental health-related hospitalizations also varied by individual-level demographics, including age and race. All age groups, compared with 25-year-olds to 29-year-olds, had increased odds of a mental health-related hospitalization in early postpartum, and the youngest group (17-year-olds to 24-year-olds) had increased odds in late postpartum. These results among our sample with OUD reflect trends among the general postpartum population in which younger women and adolescents have the highest risk of mental health concerns throughout the first-year postpartum,61,62 which has been linked to lower social support and socioeconomic resources among younger women.61,63 Additionally, NH Black individuals with OUD in our sample had increased odds of mental health-related hospitalizations from 43 to 365 days postpartum compared with non-NH Black/NH individuals. This finding is consistent with documented postpartum and non-perinatal mental health disparities among Black women in the United States,64-66 and future research should aim to better disentangle and address the mechanisms underlying these disparities. Lastly, for all types of hospitalizations, a strong predictor of hospitalizations from 43 to 365 days postpartum was having any hospitalization in the first 6 weeks postpartum. Improved care and interventions targeting those with OUD experiencing hospitalizations in this earlier postpartum period could help reduce later hospitalizations. Better transitions to non-pregnancy care may provide important prevention opportunities and help to maintain those with OUD in long-term health care.
Limitations
While this study is strengthened by a large population-based sample of pregnant persons with OUD, we only investigated postpartum inpatient hospitalizations, thus our results do not extend to emergency department visits or other health or overdose events that do not result in hospital contact. Hospital discharge data are susceptible to misclassification and reporting bias and likely underestimate SUDs and mental health conditions.67,68 We used both primary and secondary diagnosis codes to classify OUD-specific and mental health-related hospitalizations. While this provides a broad overview of all related hospitalizations, we recognize that a hospitalization with a primary diagnosis for OUD or a mental health condition may be very different from a hospitalization for another concern (eg, pregnancy-related condition, injury) complicated by these secondary diagnoses. Further research is needed to assess differences in these hospitalizations with primary versus secondary codes. Additionally, these data have a limited number of individual-level covariates and other important factors were unable to be examined, such as MOUD utilization, infant health status, child custody and child-protective service involvement, socioeconomic status, and involvement in other social and criminal justice systems.
We limited our contextual factors to the county level in order to maintain a multilevel data structure with sufficient power to assess differences between county and individual levels. Our data did not support analyses at smaller spatial units, such as neighborhoods or municipalities, where different contextual factors may be associated with risk for postpartum hospitalization. Moreover, due to a low number of individuals in the sample in some counties and limited statistical power, 10 counties in the state (n = 18 individuals) were excluded from the analysis. Almost all the excluded counties were rural, likely resulting in a slight overrepresentation of suburban and urban county residents. As described previously, individuals were also linked to county data based on their residence at delivery, and we could not account for a change in county residence by the time of a postpartum hospitalization. Even though we were able to assess county change for those who were hospitalized postpartum, we had no way to assess the mobility of those who were not hospitalized during this period (this similarly applies to other time-varying individual-level variables, such as insurance type). Thus, only individual-level and county-level exposures at the time of delivery hospitalization were examined. Similarly, we did not assess whether the county of residence was the same or differed from the county in which both the delivery and postpartum hospitalizations occurred.
Conclusions
Community contexts are important compounding factors of other vulnerabilities in the postpartum period. In addition to individual-level characteristics, county-level contextual factors, especially health care system and drug treatment landscapes, are important contributors to hospitalizations among postpartum individuals with OUD. Policies and structural barriers to services and care must be addressed to increase not only the availability of, but also accessibility to, these services across the first-year postpartum. While drug treatment may prevent worsening problems, structural improvements in health system access and delivery in communities are needed to improve the long-term health of this maternal population.
Supplemental Material
sj-docx-1-saj-10.1177_29767342251341171 – Supplemental material for Multilevel Factors Associated With Hospitalizations in the First-Year Postpartum Among Persons With Opioid Use Disorder
Supplemental material, sj-docx-1-saj-10.1177_29767342251341171 for Multilevel Factors Associated With Hospitalizations in the First-Year Postpartum Among Persons With Opioid Use Disorder by Jessica Frankeberger, Robert W. S. Coulter, Marian Jarlenski, Elizabeth E. Krans and Christina Mair in Substance Use & Addiction Journal
Footnotes
Author Contributions
JF and CM originated the study and obtained funding. RWSC, MJ, and EEK provided suggestions on study design and the analysis. JF conducted the data analysis and drafted the initial manuscript. All authors participated in interpreting the results, contributed to the writing of the manuscript, provided critical feedback to the manuscript, and approved the final manuscript draft for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institutes of Health (NIH), National Institute on Drug Abuse (NIDA) grants F31DA052142 and T32DA023356, National Institute on Alcohol Abuse and Alcoholism (NIAAA) grant K01AA027564, and the University of Pittsburgh’s Clinical and Translational Science Institute through NIH grant UL1TR001857. The NIH had no role in the study design, analysis, interpretation of data, the writing of the report, or in the decision to submit the paper for publication.
Compliance,Ethical Standards,and Ethical Approval
This study was reviewed and deemed exempt by the Institutional Review Board at the University of Pittsburgh. This research was conducted in accordance with the Declaration of Helsinki.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.