
Abstract
Background:
Substance use disorders (SUD) are a significant public health challenge, necessitating that clinicians are trained in SUD treatment and harm reduction (HR) strategies. Despite this, no studies have assessed the extent of SUD and HR training across all medical schools. This study assesses the current state of SUD and HR curriculum among medical students in the United States and Canada.
Methods:
From May to July 2023, we conducted an anonymous online survey via email invitation to student affairs’ offices of all 220 accredited US and Canadian medical schools. The survey assessed the curricula students were exposed to related to SUD treatment, HR, and stigmatizing attitudes.
Results:
A sample of 568 students from 52 medical schools (23.6% of all US and Canadian medical schools) completed the survey. Participants reported that in their medical school they were taught about: recognition of an opioid overdose (80.0%), identifying and treating opioid withdrawal (68.2%), principles and practices of HR (60.6%), administering naloxone (56.6%), the importance of syringe service programs (51.8%), prescribing methadone and/or buprenorphine (29.5%), and counseling patients on safe injection practices (11.4%). In addition, participants reported that they were taught: how to identify drug-seeking behavior (36.4%), that people who use heroin are “drug abusers” (24.4%), to withhold opioid pain medication from patients who are known or suspected to use drugs (15.9%), and that medication for opioid use disorder is another form of addiction (12.6%).
Discussion:
We found large curricular gaps related to the administration of medications for opioid use disorder and treating opioid overdose and withdrawal, as well as a significant prevalence of stigmatizing attitudes. Renewed efforts are needed to implement comprehensive and destigmatizing SUD curricula. The study is limited by response bias and is expected to overestimate the extent of HR related curriculum, indicating the true gap is likely higher than reported.
Keywords
Highlights
This study surveyed a sample of 568 students from 52 medical schools in the United States and Canada to assess the current landscape of substance use disorder and harm reduction education.
Significant gaps exist in undergraduate medical education regarding substance use disorder treatment.
Only 29.5% of students reported training on prescribing medications for opioid use disorder and only 56.6% received training on administering naloxone.
Introduction
Substance use disorders (SUDs) are a significant public health challenge in the United States and Canada, with 40.3 million Americans diagnosed with one or more SUDs in 2020, and 21.6% of Canadians meeting diagnostic criteria for lifetime SUD.1,2 Additionally, overdose deaths remain at crisis levels, with more than 107 000 reported in the United States in 2023. 3 In Canada, there were a total of 47 162 opioid overdose deaths between January 2016 and March 2024. 4 Healthcare is a crucial engagement point for people who use drugs (PWUD) to receive care, including SUD treatment. Therefore, it is important for clinicians to be adequately trained in treating people with SUDs. Nevertheless, little is known about the prevalence of SUD-related education in medical school curricula.
Harm reduction (HR) is a clinical and social practice, and a social justice movement aimed at reducing negative health outcomes associated with substance use. It plays a vital role in combating the overdose crisis. 5 HR interventions include providing access to sterile syringes, overdose education and naloxone distribution, drug checking, and more. Educating first responders, patients at risk, and their family members about overdose prevention and recognition, and distributing naloxone decreases the rate of opioid overdose deaths. 6 HR spaces are also often effective in linking PWUD to other healthcare services, including medications for opioid use disorder (MOUD).
Additionally, HR training of medical students has been linked to a decrease in stigma toward PWUD. 7 Stigma among healthcare providers negatively impacts the delivery of care and contributes to poorer health outcomes, and some clinicians may perceive their patients as deceptive in seeking medical attention, leading to withholding necessary medications and interventions.8,9 Despite its critical role in SUD-related healthcare, the degree to which HR is incorporated into medical school curricula has not been fully characterized. 10
This study aims to assess the prevalence of SUD and HR-related education among undergraduate medical students in the United States and Canada. By describing the gaps in medical education—where physicians’ foundational learning occurs—this study also seeks to identify gaps where SUD and HR curricula can be standardized across medical schools. This is the first study to comprehensively survey US and Canadian medical students about SUD and HR treatment in their curricula.
Methods
Study Design
We distributed an anonymous online survey questionnaire to medical students across the United States and Canada between May and July 2023. We sent an initial email invitation to student affairs offices of 220 Liaison Committee on Medical Education and American Osteopathic Association accredited US medical schools, and Committee on Accreditation of Canadian Medical Schools accredited Canadian medical schools. We sent follow-up emails to schools with incomplete or no response after a 2-week interval. Due to sparse initial responses, we made additional efforts to encourage participation, including messaging through addiction medicine listservs and increased outreach efforts through various student HR and addiction medicine interest groups. In these instances, we requested that students send the survey to their entire medical school or class, rather than just complete it themselves or send it to students in these interest groups, to reach the widest possible sample of medical student participants.
Survey Development
The survey contained sociodemographic questions and a section evaluating undergraduate medical education (UME) curriculum on substance use and HR. Sociodemographics collected included age, gender identity, sexual identity, race, ethnicity, name of medical school, year in medical school, preclinical/clinical phase of curriculum, and career specialty interest. The survey featured 7 questions assessing the curriculum related to SUD treatment and HR. The questions were developed by our research team and have not previously been utilized, to our knowledge. These questions had “Yes,” “No,” and “Unsure/Don’t Know” options and included the following statements: in my medical school training, I was taught. . .how to identify and treat opioid withdrawal, the importance of syringe service programs, how to counsel patients on safe drug injection practices, how to recognize an opioid overdose, how to administer Narcan (naloxone), how to prescribe methadone and/or buprenorphine (MOUD), and about the principles and practices of HR. Additionally, there were 4 questions assessing stigmatizing attitudes taught in UME curriculum. These questions also had “Yes,” “No,” and “Unsure/Don’t Know” as answer options and included the following statements: in my medical school training, I was taught. . .to withhold opioid pain medication from patients who are known or suspected to use drugs, that medication for opioid use disorder is another form of addiction, that people who use heroin are “drug abusers,” and how to identify drug-seeking behavior in a patient requesting pain medication. The survey was reviewed and preliminarily tested with a group of twelve medical, graduate, and undergraduate students. Feedback was collected from these participants and subsequently incorporated. The survey took approximately 10 minutes to complete.
Data Analysis
Survey answers were entered online and were collected using Qualtrics (Qualtrics, Provo, UT, USA) hosted by the University of California, Los Angeles (UCLA). Data were analyzed using R Version 4.2.2. This study was certified as exempt from Institutional Review Board (IRB) reviewed by the UCLA IRB given the collection of only anonymized data through an online platform.
Results
Participant Demographics
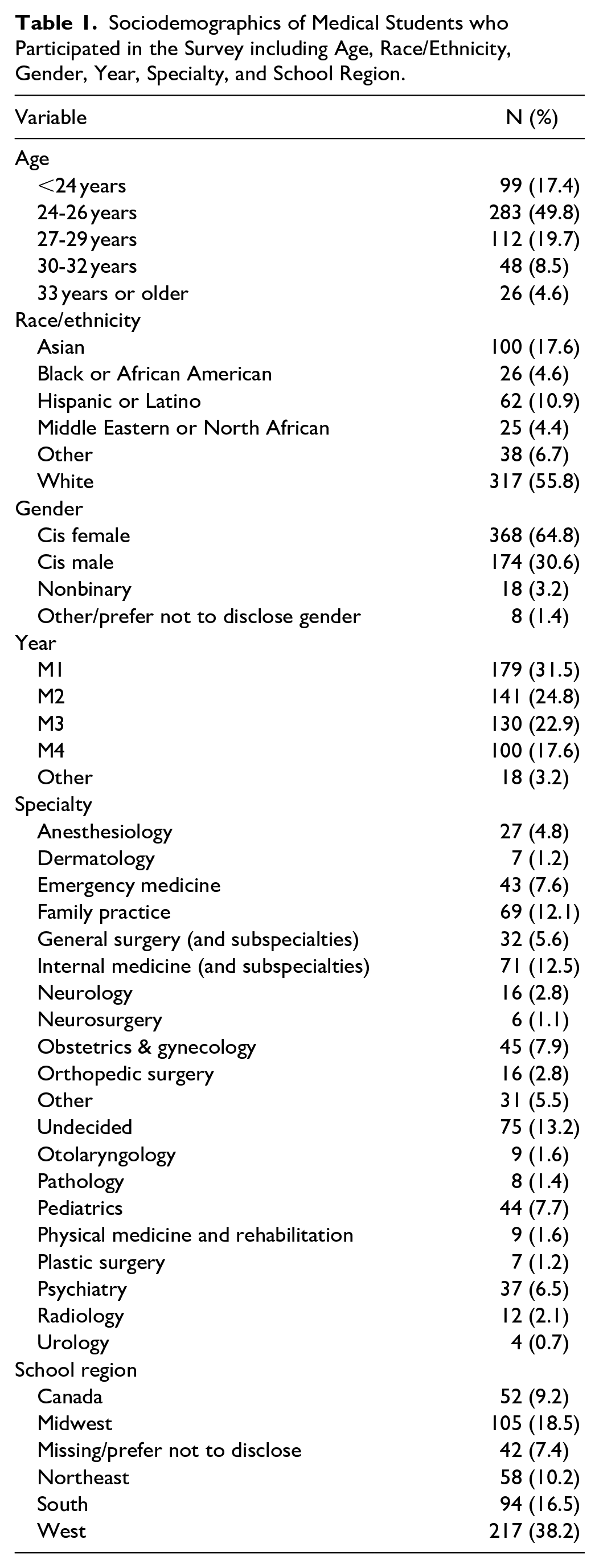
A total of 568 students from 52 medical schools (23.6% of US and Canadian medical schools) responded to the survey; participant demographics are displayed in Table 1. A majority of the respondents were aged 24 to 26 (49.8%), followed by age 27 to 29 (19.7%), and <24 (17.4%). Most respondents were non-Hispanic white (55.8%), followed by Asian (17.6%), and Hispanic or Latino (10.9%). Students in their M1 year made up 31.5% of respondents, followed by M2 (24.8%), M3 (22.9%), and M4 (17.6%). The most prevalent specialty interest was Internal Medicine and subspecialties (12.5%) followed by Family Practice (12.1%) and Obstetrics and Gynecology (7.9%).
Sociodemographics of Medical Students who Participated in the Survey including Age, Race/Ethnicity, Gender, Year, Specialty, and School Region.
SUD and HR Curriculum
In their medical school training, 80.0% of participants reported being taught how to recognize an opioid overdose, 56.6% reported receiving training on administering Narcan, 11.4% reported training on how to counsel patients on safe drug injection practices, 29.5% reported being taught how to prescribe methadone and/or buprenorphine, 68.2% reported training on identifying and treating opioid withdrawal, 51.8% reported learning the importance of syringe service programs (SSPs), and 60.6% reported learning about the principles and practices of HR (Figure 1).
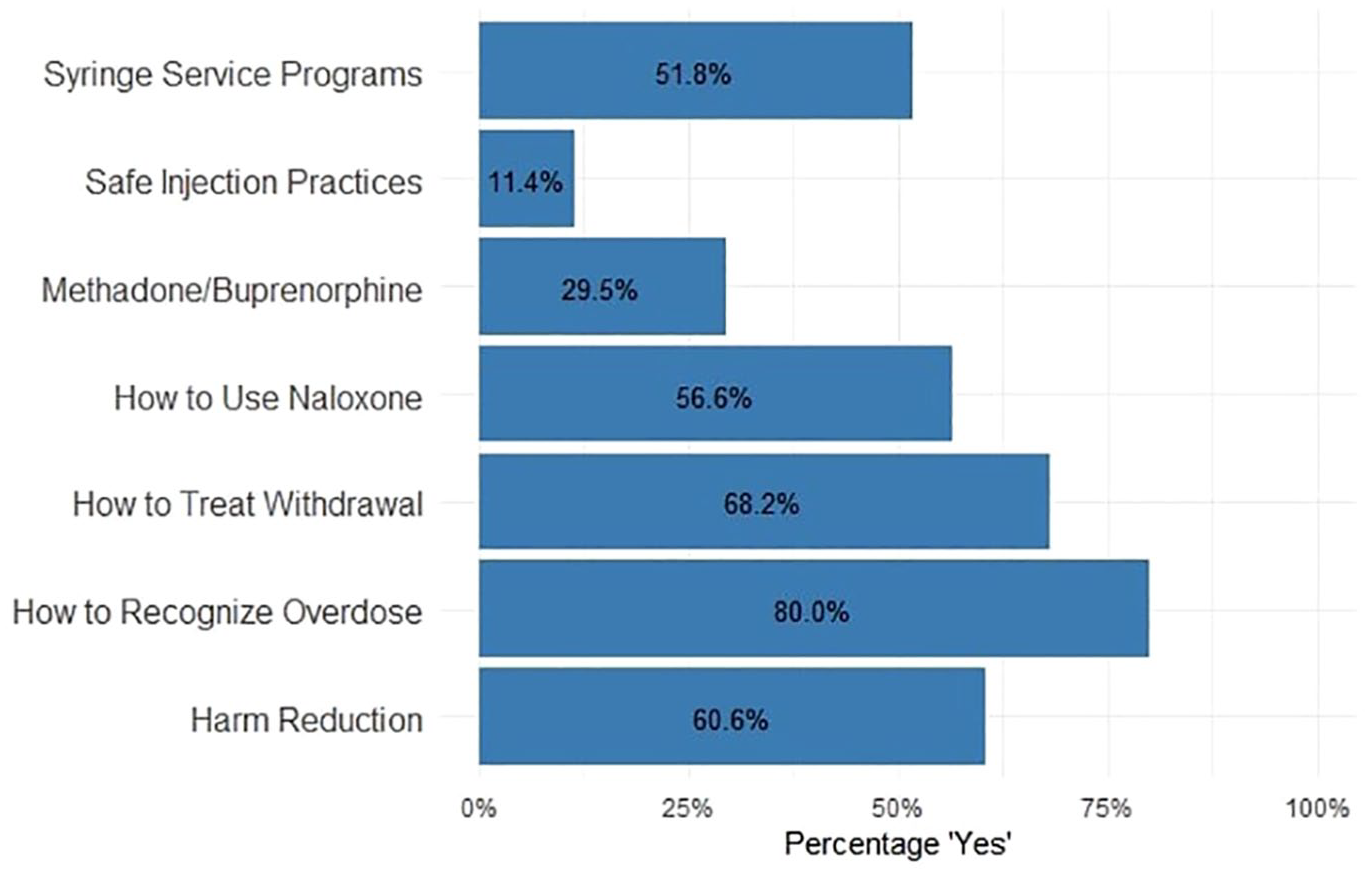
Substance use and harm reduction curriculum.
Stigma Within Curriculum
In their medical school training, 36.4% of participants reported being taught how to identify drug-seeking behavior in a patient requesting pain medication, 15.9% reported that they were taught to withhold opioid pain medication from patients who are known or suspected to use drugs, 12.6% reported being taught that medication for opioid use disorder is another form of addiction, and 24.4% reported they were taught that people who use heroin are “drug abusers” (Figure 2).
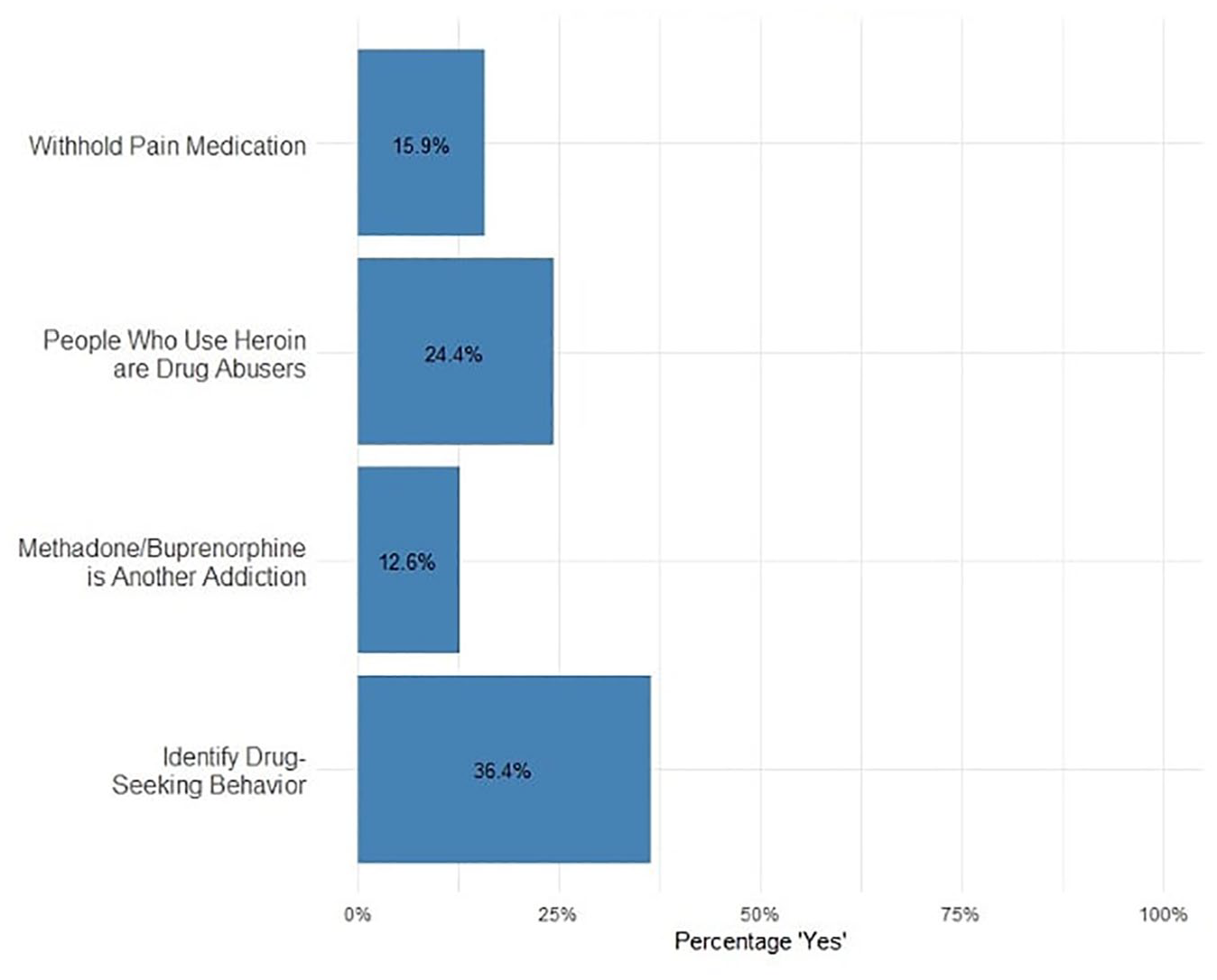
Stigmatizing attitudes in curriculum.
Discussion
This study utilized an anonymous online survey questionnaire to assess the current landscape of curricular content related to SUD treatment and HR education in UME. To the authors’ knowledge, this is the first comprehensive study of its kind, and the findings highlight significant gaps in training related to SUD treatment and HR, as well as the persistence of stigmatizing attitudes toward PWUD being taught to medical students. The results underscore the need for a more comprehensive and destigmatizing approach to substance use education in UME.
MOUD is the first-line treatment for opioid use disorder (OUD) and has been proven to decrease mortality risk, reduce recurrence of use, and improve treatment retention.11-15 Despite these benefits, only 29.5% of medical students reported being taught how to prescribe MOUD. Although no studies have specifically evaluated the prevalence of MOUD education in UME, a 2019 scoping review by Muzyk et al identified 43 articles on SUD educational initiatives, with only 2% addressing OUD treatment. 16 This finding aligns with the small percentage of students who reported receiving MOUD education. Even with the well-established advantages of MOUD, a majority of individuals with OUD remain untreated, revealing a gap that could be addressed by incorporating MOUD training into UME. 17 An updated, standardized SUD curriculum across all medical schools is necessary to address this gap.
Physicians play a pivotal role in the overdose crisis both through direct life-saving interventions and by educating patients and the community about overdose prevention and response. Eighty percent of participants report being taught how to recognize an opioid overdose, and only 56.6% reported receiving training on administering naloxone. While reports of naloxone training in medical schools, primarily through student-led initiatives, have increased in recent years, there is no consensus or widespread mandate for naloxone training in UME.18-21 Naloxone trainings for medical students are proven to improve medical student’s knowledge of overdose prevention and response, providing a promising avenue for future physicians to participate in overdose prevention efforts with their patients. 18 A mandatory and standardized overdose prevention and naloxone administration training across all medical schools would address the current gaps and improve future patient knowledge and safety.
Stigma in healthcare toward PWUD is a well-described and significant barrier to quality care, negatively affecting health outcomes and leading PWUD to avoid seeking medical care due to the fear and experiences of mistreatment. 8 One example of this stigma is the use of stigmatizing language, such as referring to people as “drug abusers” instead of using person-first language. Twenty-four percent of participants reported being taught that people who use heroin are “drug abusers.” Physicians and the National Institute on Drug Abuse have called for improvements in the language surrounding addiction, but the prevalence of stigma within UME curricula has not been previously described.22,23 Evidence shows that HR training in medical education can reduce stigmatizing attitudes toward people who inject drugs, suggesting that incorporating such training may be a valuable strategy to address stigma in UME and ultimately improve health outcomes for PWUD. 7
Despite the value of HR education, only 60.6% of participants reported learning about the principles and practices of HR and 51.8% of students reported learning about the importance of SSPs. Beyond its value for improving stigmatizing attitudes toward PWUD, HR strategies reduce the adverse health effects associated with substance use and are vital in addressing the ongoing overdose crisis.5,7 By incorporating HR education into UME curricula, future physicians can be better equipped to support PWUD with compassionate, evidence-based care that prioritizes their health and dignity.
Limitations
Several limitations should be considered when interpreting the findings of this study. Not all medical schools were successfully reached and participation was voluntary, and therefore the results may not be representative of the entire medical student population in the United States and Canada. Participation in this survey was voluntary, which may have led to a higher response rate from medical students with interest in these topics, possibly increasing the percentage of students that reported learning about SUD and HR curriculum. Additionally, the survey was subsequently shared through addiction medicine and HR interest groups, further compounding the selection bias. This is likely to lead to a sample that is more educated on addiction treatment and HR than the national average, making our findings overly optimistic. The true gaps are likely higher than reported here. Finally, the survey assessing curriculum content was developed specifically for this research and has not been validated in prior studies. There is no standard definition for what constitutes sufficient education regarding the curriculum topics assessed. As a result, participants may have interpreted these questions differently, leading to varying thresholds in their responses.
Conclusions
This novel study utilized an anonymous online questionnaire to assess the current state of HR education and stigma within UME in the United States and Canada. The findings reveal significant gaps in the curriculum related to SUD and HR education and the persistence of stigmatizing attitudes toward PWUD. These gaps in education, which have likely persisted for a long time, have contributed to patients with SUD not receiving compassionate care from physicians. This highlights the urgent need for a more comprehensive and destigmatizing approach to SUD education in UME. We hypothesize that incorporating HR principles and compassion-based SUD education into medical school training will better prepare future physicians to engage in evidence-based practices, advocate for policy changes, and effectively address the needs of their patients, generating meaningful progress.
Footnotes
Author Contributions
All authors conceived the survey and implementation tools. All authors managed and contributed to the operation of the training and the survey. TA, JF, and AN took the lead in writing this manuscript. All authors provided critical feedback and contributed to the writing of the manuscript and all authors approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CLS was supported by grant funding from the National Institute on Drug Abuse (grant K01DA050771). DGM was supported by grant funding from the National Institute on Drug Abuse (grant K08DA048163).
Compliance,Ethical Standards,and Ethical Approval
Certified IRB Exempt by the UCLA Web IRB (IRB #23-000387).