
Abstract
Communication is essential in efforts to reduce drug-related harm. Nursing professionals play a key role in harm reduction practices; therefore, this qualitative study aims to describe their perceptions of communication in drug-related harm reduction and how to develop such communication. Nine (n = 9) semi-structured interviews were conducted with nursing professionals with experience in addiction treatment, analysed through inductive content analysis. The study adhered to the Consolidated Criteria for Reporting Qualitative Research (i.e. COREQ). The current communication was described as multi-channel, invisible, undervaluing and unprofessional communication. The development themes were communication about services, accessible, early-stage, supportive, open, responsible and narrative communication. The need for visible and ethical communication emerged. Strengthening service-related communication and healthcare professionalism is essential to support help-seeking. Open and responsible communication could normalise discourse, and early integration into everyday environments could enhance prevention. The findings highlight the value of low-threshold services and the engagement of people who use drugs and lived experience experts in developing communication.
Introduction
Access to high-quality substance use disorder treatment remains a global challenge, undermined by low investment in effective services as well as stigma and discrimination. The use of psychoactive substances has significant health impacts, including widespread physical and mental morbidity and a high risk of overdose and suicide. 1 People who use drugs (PWUDs) face multiple challenges that increase their vulnerability, such as social exclusion. 2 Stigma impacts many aspects of PWUDs’ health, including access to and use of support services. 3
Health communication plays a vital role in supporting vulnerable populations, helping to reveal the underlying factors behind health inequalities and promoting behavioural and social changes to support better health. 4 Communication is also an essential part of drug-related harm reduction efforts.5,6 Harm reduction is an evidence-based approach that can reduce infectious diseases and overdoses, while improving the quality of life and access to services for PWUDs. It encompasses practices and policies aimed at minimising the physical, social and legal harms associated with drug use and drug policy. These include, among other things, needle and syringe exchange programmes and providing information on safer use. 7
Nursing professionals, defined as nurses with formal education and professional registration, play a key role in harm reduction activities and frontline engagement with PWUDs. 8 Therefore, viewing communication related to harm reduction through their lens offers valuable insights for developing communication practices.
Background
Communication plays a key role in promoting health and health equality. 4 It can be seen not only as one-way message transmission, but also more broadly as building connections and dialogue. 9 In the context of health, communication encompasses various channels, including verbal, written and visual forms, through which information is exchanged (e.g., patient–professional interactions, social media, organisational communications, news, and policy briefs). 10 The present study examines communication in a broad sense, from individual-level interactions, such as communication between a patient or client and a professional, to community- and societal-level communication, such as communication in the media.
Communication in harm reduction can be examined more closely through its core principles.11,12 In healthcare encounters, these principles emphasise a respectful, empathetic and patient-centred approach that highlights realistic goals and values small steps forward. Patients remain responsible for their choices but receive support despite setbacks. Applying these principles may strengthen the patient–professional relationship and support improved treatment outcomes. 11 Harm Reduction Theory (HRT) provides a valuable basis for communication strategies by acknowledging risky behaviour as part of human experience, and promoting realistic, non-judgmental and empowering support. It highlights incremental progress and the role of environmental factors in facilitating change. This perspective may encourage open dialogue and enhance understanding of the underlying factors behind harmful behaviour. 12
Communication in drug-related harm reduction aims, among other things, to increase awareness of the harms and risks of drugs and ways to reduce them. Characteristics, habits and reactions to health risks vary among PWUDs, highlighting the importance of targeting communication to different groups. 5 Important audiences include those with problematic and occasional drug use, experimenters and young people, but communication should also be directed at professionals, decision-makers and the public. This is especially important because reducing negative attitudes towards PWUDs in society and the service system is essential for reducing harm. 6
Reducing stigma is a key communication topic in drug-related harm reduction. 13 For example, previous studies highlight narrative and empathetic communication as effective stigma-reduction strategies. 14 However, some efforts aimed at reducing stigma, such as mass media interventions, have been observed to have shortcomings, including an inadequate definition of stigma, negative portrayals of PWUDs and their low involvement in the interventions. 15 In some cases, campaigns have inadvertently reinforced negative stereotypes and increased the stigma experienced by PWUDs. 16 In the healthcare context, the negative effects of stigmatising language have been shown to extend to patient care.17,18 Communication-focused interventions targeting healthcare professionals have, however, successfully improved interactions with PWUDs and supported progress in reducing substance use. 19
Overdose prevention is another key communication focus. 13 Previous research has examined PWUDs reactions to risk communication,20,21 and how PWUDs perceive and utilise online educational information on overdose prevention. 22 Messages that fill knowledge gaps and are perceived as personally meaningful, 20 messages that are compassionate and build trust, 21 as well as plain language and action-focused messages 22 are some recommended approaches. mHealth applications have shown promising results in communicating with patients at risk of overdose 23 and are considered an acceptable method for delivering harm reduction information. 24 Similarly, communication through peer networks of PWUDs has been found effective. 25 Furthermore, anonymous online environments are viewed positively by PWUDs because they enable non-judgmental access to information, which is especially valued by those who are employed or have families. 26
Finnish drug policy can be described as a dual-track model in which crime prevention activities, health services and limited harm reduction services are parallel. The policy is under pressure to reform; for example, by decriminalising drug use. 27 In 2023, the number of drug poisoning deaths was the highest in Finland's history. 28 To prevent drug-related deaths, measures such as improving access to services, enhancing the flow of information between authorities, service providers and PWUDs, engaging PWUDs in dialogue, and implementing targeted campaigns are considered important. 6
To conclude, communication plays a crucial role in promoting the harm reduction approach and reaching individuals in need of support. The literature emphasises the need for further development and enhancement of communication, including greater consideration of target groups and attention to language use. Communication in harm reduction encompasses a broad phenomenon occurring at many levels and contexts, and the present study examines it comprehensively, from frontline practice to the policy level. It is not limited to specific communicators, audiences, channels, topics or contexts because the aim is to address the overall scope of communication. The emphasis is on communication aimed at minimising the harms associated with drug use, in line with harm reduction, 7 rather than on communication primarily aimed at preventing drug use.
The present study approaches the topic from the perspectives of nursing professionals a viewpoint that has received limited attention. Nurses working on the front line of harm reduction efforts 8 have a central role in understanding the phenomenon under study. The present study aims to describe nursing professionals’ perceptions of communication in drug-related harm reduction and how to develop such communication.
Methods
The study employed a qualitative descriptive interview design. Semi-structured interviews were used to gain in-depth information about the professionals’ lived experiences and personal understanding of the phenomenon under study. 29 The study addressed the following research tasks: (i) to describe nursing professionals’ perceptions of communication in drug-related harm reduction and (ii) to describe nursing professionals’ perceptions of developing communication in drug-related harm reduction. The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was used to review the research report. 30
Setting
Participants were recruited from one Finnish wellbeing services county. In Finland, social and healthcare services are organised by 21 wellbeing services counties and the City of Helsinki. The basis of the system is public social and healthcare supported by government funds. 31
Recruitment
Purposive sampling was employed as the professionals were considered key informants due to their relevant experience and understanding of harm reduction. 32 The inclusion criteria included social or healthcare professionals working in the wellbeing services county with experience in the addiction treatment field. From November 2024 to February 2025, participants (n = 9) were recruited via nurse leaders from all addiction treatment units in the wellbeing services county, with assistance from contact persons. Nurse leaders were well informed about the study's purpose and procedures. They received an email request to forward the interview invitation to professionals they deemed suitable for the study. The email included a cover letter outlining the study's purpose, the procedure, and the researcher's role and affiliation. Interested participants, who were not previously known to the researcher, then contacted the researcher by email. The study was also presented to nurse leaders at two online meetings held in October 2024 and January 2025, and promoted through the organisation's internal communication channels.
Data collection
The data was collected between December 2024 and April 2025 through semi-structured online interviews using Teams (Microsoft Corp.). All interviews were conducted once, recorded, and lasted 50–60 min (average time 55 min). In total, nine (n = 9) nursing professionals were interviewed, of whom seven (n = 7) were interviewed individually and two (n = 2) as a pair. The first researcher (SN) conducted all interviews, and only the interviewer and interviewees were present. One person who initially registered was ultimately unable to schedule an interview and was therefore excluded from the study.
All interviews were transcribed into a Word document (Microsoft) totalling 160 pages (Open Sans, 11-point font, single spacing). Field notes were taken to support observations; however, only the transcribed interview data were analysed. The main themes of the interviews were professionals’ perceptions of current communication in drug-related harm reduction and their views on how to develop that communication. Questions were asked to clarify themes related to different elements of communication, based on the communication process elements identified in previous literature4,9 and the core principles of harm reduction, 11 and are presented in detail in Table 1.
Interview themes.

Data analysis
Research on communication in drug-related harm reduction is limited, so inductive content analysis was used to extract relevant information.33,34 The first step involved carefully reading the transcribed interviews to gain a deep understanding of the content and identifying expressions, typically sentences or short phrases, related to the research tasks, with a focus on manifest content. The original expressions were carefully simplified into meaning units, which were then manually coded and organised using tabulation. Codes with similar content were initially grouped into subthemes (n = 33 and n = 35, respectively), which were then combined into themes (n = 14 and n = 15) and finally into main themes (n = 4 and n = 7) designed to address the research tasks and capture professionals’ perceptions. The analysis was conducted by the first researcher (SN) in Finnish and subsequently translated into English following discussion with the research team.
Ethical considerations
Permission for the research was granted by the wellbeing services county where the study was conducted. The ethical regulations governing Finnish research do not require ethical approval for studies that do not involve patients, cause no harm and do not involve intervention in physical integrity. 35 As the present study meets these criteria, no ethical approval was required or sought. The study was conducted following the ethical principles of the Helsinki Declaration. 36 Although the study participants were not PWUDs, special attention was paid to PWUDs’ rights, including respectful language at all stages of the study.
The participants were provided with information about the research and its voluntary nature. At the start of each interview, verbal consent to participate was obtained. Indirect personal data describing participants’ professional backgrounds were stored separately from the interview data and were not linked to individual interviews. Recordings were destroyed once all interview data had been accurately transcribed. Any other potentially identifying information, such as names and locations, was also removed. Participants’ personal data are protected in accordance with the General Data Protection Regulation. 37
Results
Nine (n = 9) nursing professionals participated in this study, seven (n = 7) of whom were women. Participants were aged between 35 and 63 years (mean age 49 years). Their professional backgrounds included registered nurses (n = 6), mental health nurses (n = 2) and a public health nurse (n = 1). Three (n = 3) held a Master's degree in social and healthcare, four (n = 4) had a Bachelor's degree or an equivalent previous college qualification and two (n = 2) had completed upper secondary education in social and healthcare. Their length of work experience in their current profession ranged from 3 to 36 years (mean 17.5 years) and, in their current position, from 1.2 to 17 years (mean 5.5 years).
Nursing professionals’ perceptions of communication in drug-related harm reduction
Four main themes described nursing professionals’ perceptions of communication in drug-related harm reduction: (i) multi-channel communication; (ii) invisible communication; (iii) undervaluing communication; and (iv) unprofessional communication (Table 2).
Nursing professionals’ perceptions of communication in drug-related harm reduction.

Abbreviation: PWUDs = people who use drugs.
According to professionals, multi-channel communication reflected communication in harm reduction as it was carried out by several actors (Figure 1), levels and contexts (Figure 2). The role of third-sector organisations as communicators was central. Communication between professional networks was seen as effective. The police were seen as successful communicators to young people and on dangerous drugs. PWUDs were recognised as active information sharers in peer networks and with professionals. Nursing professionals described themselves as communicators in their practice. This role emphasised respectful interaction with patients, as well as advocating for them within the healthcare system and in dialogue with other healthcare practitioners. Communication was also carried out by social media influencers and lived experience experts in online environments, and the media as communicators about dangerous drugs and describing the real lives of PWUDs.

Actors in communication in drug-related harm reduction, as described by nursing professionals.
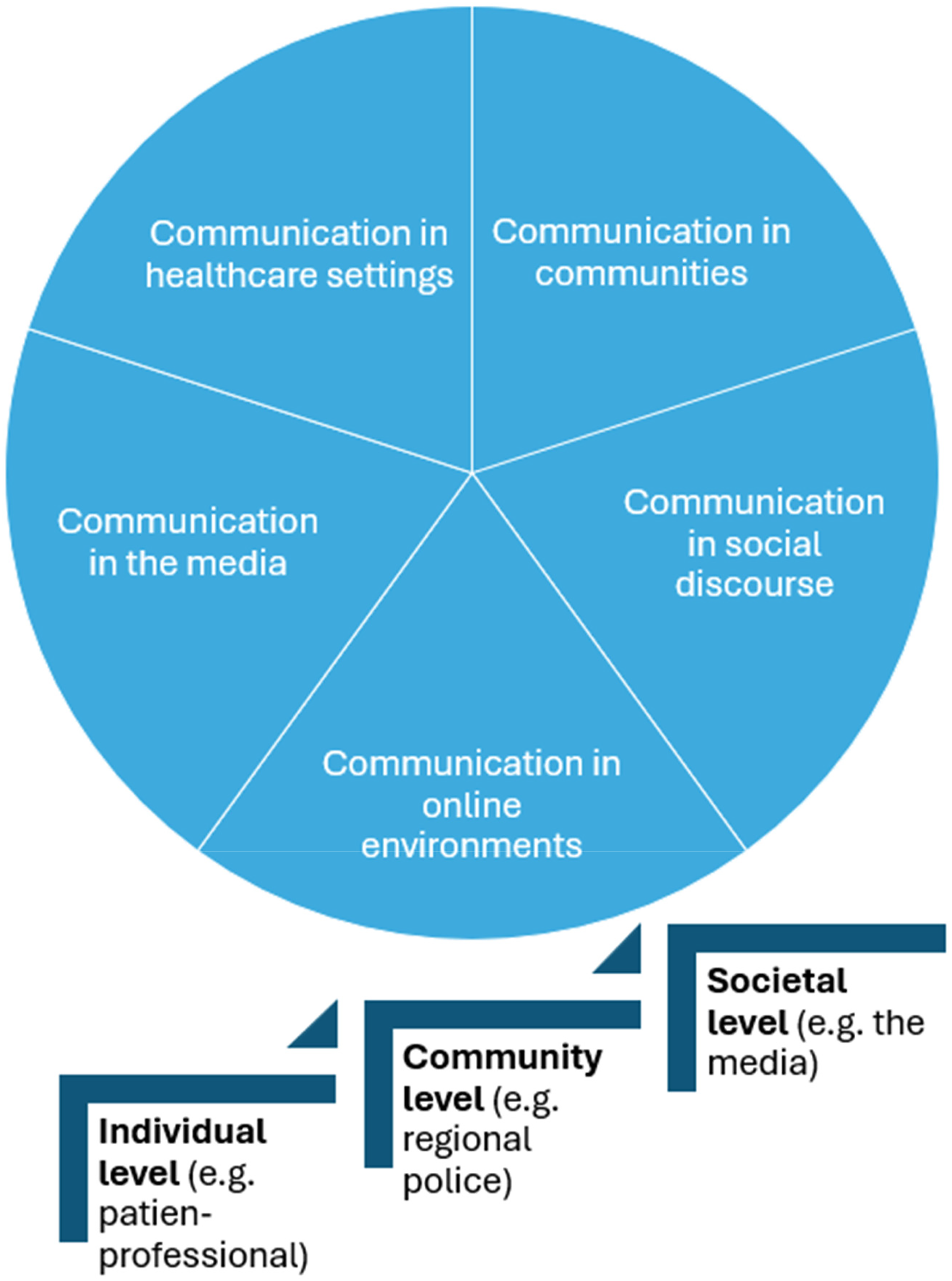
Levels and contexts of communication in drug-related harm reduction, as described by nursing professionals.
Although communication was carried out by many actors, professionals described it as invisible. Invisible communication was characterised by a lack of information about services and treatment options. Professionals described the wellbeing services county's communication as both invisible and faceless. They believed that communication was not reaching those in more disadvantaged positions, especially as information was seen to be increasingly available in digital form: That people would even know that it [drug addiction] is something that is treated here in primary healthcare, but no. People don’t get any information about it. (P3) There is such a stigmatising discussion in society … such a judgmental discussion still exists. These drug consumption rooms have been in the discussion … which conveys that they are considered hopeless cases, second-class citizens. (P4) One of the biggest problems, when thinking about this kind of communication, is probably the attitude of the nursing staff towards these issues. Many people don’t understand what the idea behind [opioid maintenance treatment] is. It's a shame, as this will certainly be reflected in the patient when they sense that they are not a particularly valued patient group. (P1)
Nursing professionals’ perceptions of developing communication in drug-related harm reduction
Seven main themes described nursing professionals’ perceptions of developing communication in drug-related harm reduction: (i) communication about services; (ii) accessible communication; (iii) early-stage communication; (iv) supportive communication; (v) open communication; (vi) responsible communication; and (vii) narrative communication (Table 3).
Nursing professionals’ perceptions of developing communication in drug-related harm reduction.

Abbreviation: PWUDs = people who use drugs.
Regarding the development of communication, professionals emphasised the need for communication about services, including information about treatment options and opportunities to access help. In this context, they highlighted the importance of inviting communication that encourages service use, suggesting that providers should be personally visible to humanise the services. Communication should convey both the ease of accessing services and the genuine willingness of providers to help: It would be absolutely brilliant for the wellbeing services county in January and August to inform people in a direct way, saying, did you know how easy it is to access substance use treatment services? or that [service providers] would somehow show up on their faces there. (P6) They know these [drug-related] things very well … maybe more about some life management issues, they just need these kinds of help with all these housing and social issues, and where to get that help. (P1) First of all, communication to those young people, really young people. It must start in primary school, soon, it seems like it could even be in nursery settings, they are starting to be so young, the first … experimenters. And educating parents. It is hugely important to communicate with them too. (P8) Those other colleagues who didn’t mainly treat people who use drugs … so the conversation between us. I have experienced that as one of the hardest jobs, that I had to defend to my own colleagues why I treat these people in my work. So, informing them about that matter and communicating about it is … the key thing. (P6) By meeting them on the same level as a human, without you putting more stigma on it. Otherwise they will disappear into hiding, and there will be much more harm, instead of somehow getting them into treatment. Education … to improve understanding of the challenges faced by people living with addiction … and how to approach them. (P4) There should be such equality that if we communicate on those social media channels. We have a huge range of different peer groups … and services for our neuropsychiatric clients. Then why don’t we also communicate on the same level about low-threshold services for PWUDs? (P6) I would say about the tone of the communication … that it is factual, open, and neutral, that it is just that neutrality. That you often read in newspaper headlines about the recreational use of drugs and then that a party drug and a drug for the better circles … the elite. So stupid. Those kinds of positive terms should be removed. (P5) They are really great [lived experience experts]. We have now started to use them more … or when we have noticed that it would be good with this young person … that we should act now before we go too deep. (P5)
Discussion
The present study has described nursing professionals’ perceptions of communication in drug-related harm reduction and how to develop such communication. The results illuminated the multifaceted nature of communication in harm reduction and provided valuable insights into the effectiveness and appropriateness of communication by drawing on interviews with nurses working directly with clients in addiction care. Communication was described at the individual, community and societal levels and in different contexts, especially in healthcare settings, as well as in communities, social discourse, online environments and the media. The results highlighted young people and families, vulnerable groups, and healthcare professionals as key target audiences for communication. Third-sector organisations were recognised as key communicators, while health authorities were urged to take a stronger role in communication. The participants’ observations reinforce earlier findings on the need to develop communication, emphasising the need for visible and ethical communication in the service system and at the societal level.
Findings such as the undervaluation conveyed through communication, and the need for encounters with PWUD to be responsible, equal and respectful, highlight the importance of strengthening ethical principles in communication. The vulnerable position of PWUDs, together with nurses’ own ethical value base – grounded in encounter patients with dignity and respect 38 – might be reflected in the findings. Professionals acknowledged communication shortcomings in their work environments but emphasised the need to promote these ethical principles in communication across society as well.
Professionals criticised the general lack of communication and emphasised the responsibility of health authorities in communication, especially regarding services. Previous research indicates that communication about treatment options is limited compared with preventive topics, 13 and, as the present study highlights, respondents perceive that communication about treatment options is insufficient. As the use of harm reduction services is hindered by widespread stigma-related factors, 3 it is justified to promote visible communication that encourages help-seeking. In Finland, the responsibility for organising social and health services was transferred to the wellbeing services counties in 2023, which may have contributed to the described communication shortcomings, such as impersonality. However, the results revealed criticism of the unequal position of communication in harm reduction compared to other patient groups, highlighting the need for critical evaluation. This unequal status continues to limit its visibility and hinder open discussion. Aligning communication more equally could help normalise discourse and demonstrate respect for individuals facing drug-related challenges. Greater emphasis should be placed on communication within early family settings as well as in occupational healthcare, where drug-related discussions ought to be more fully integrated. However, due to the sensitivity of the topic, the need for anonymous communication platforms, such as the Dark Web, 26 is important to consider.
Criticism was also directed at healthcare, where the need for communication reflecting professional competence was identified. Prior studies indicate that stigmatising language in healthcare is negatively associated with the implementation of care.17,18 Greater attention to language by healthcare providers could therefore contribute to more effective care. Respondents assessed the lack of awareness of addiction as a disease as partly explaining the shortcomings in communication but considered that awareness could be enhanced through education and leadership. Ensuring professional competence and establishing a respectful culture for patient care at the managerial level, are key areas for future development. Professionals’ perspectives suggest alignment with the principles of HRT, 12 which emphasise a supportive, non-judgmental and realistic approach, and which could offer a useful foundation for guiding interaction. The present study revealed nursing professionals’ strong understanding of the practical aspects of communication, offering valuable insights into how healthcare teams’ dialogue practices, attitudes and choice of language and tone influence the way messages are conveyed to PWUDs.
Societal concern over the rise in drug-related deaths among youth in Finland 6 is also reflected in the results of the present study, which emphasised communication at an early stage and creating messages appropriate for the developmental level of adolescents. The results showed that the police communicate successfully with young people, providing an important foundation for developing communication, as prior research has identified fear of punishment as a key barrier to seeking help in overdose situations. 39 Building trust in authorities is one goal in harm reduction efforts. 6 Professionals recommend involving lived experience experts in youth-targeted communication, particularly to enhance the perception of risk, which has previously been found to be relatively low among this age group.20,21 Moreover, the present study emphasises the importance of responsible messaging, particularly when addressing young people; for example, avoiding terms that may depict drug use positively.
Professionals identified certain harmful aspects of communication and emphasised the need for responsibility. The negative effects of some communication campaigns recognised in prior research, such as reinforcing stigma, 16 also that highlight the need for evidence-based, carefully designed strategies and a thorough understanding of target groups to facilitate culturally sensitive and meaningful communication. Previous research supports both the use of a narrative approach 14 and the involvement of target groups 20 in communication development – both of which are also recommended by this study. Previously, the participation of PWUDs in communication processes has been limited.13,15 Granting them and lived experience experts a greater role in the communication process could yield beneficial outcomes, and strengthening collaborative dialogue with authorities would also be a worthwhile subject for further research.
It is worth emphasising the need for a face-to-face communication for vulnerable groups, as highlighted in the results. Although respondents identified challenges in digital communication with these groups, eHealth is seen as an acceptable means of communication, such as for overdose prevention, 23 and the provision of sterile injection equipment. 24 Furthermore, previous research has shown that active communication within PWUD peer networks, which also emerged in the present study, can be an effective way of conveying harm reduction information. 25 These findings could be worth examining in more detail in collaboration with PWUDs. Overall, the multiple communicators identified in the present study can be viewed as a strength in terms of the diversity of existing communication structures. In addition, the effective communication between professionals and stakeholders, as highlighted in the findings, provides a solid foundation for development efforts.
Methodological considerations
Trustworthiness of the study was ensured by critically assessing credibility, dependability, and transferability throughout the research process. 33 The findings are based on the personal perceptions of nine nurses from one Finnish wellbeing services county. They were experienced professionals, which strengthens the credibility of the results. 40 All interviews followed the same guide to enhance dependability, including two preliminary interviews (n = 2). 34 The interviews generated rich data and enabled a multifaceted description of the topic. A key strength of the study lies in its comprehensive examination of communication. The interviews approached communication from multiple perspectives. However, narrowing the focus to a specific communicative phenomenon might have yielded more detailed insights. The sample size was considered sufficient due to data saturation, 41 but, given the broad scope of the topic, a larger number of participants might have offered additional or alternative perspectives.
The study details participant selection, characteristics, data collection, analysis and research context sufficiently to allow assessment of transferability to similar settings. 33 To protect participants’ anonymity, detailed descriptions of their personal and professional contexts – such as work units or geographical locations – were not included. This limits the transferability, as drug use-related characteristics may vary between regions.
The research team comprised three female nursing science researchers: a Master's student (BHSc), a doctoral researcher (MHSc) and a Professor (PhD). The first researcher (BHSc) conducted the analysis through repeated data reviews and collaborative reflection with team members, all experienced in qualitative analysis. Verbatim transcripts were carefully condensed to preserve participants’ authentic perceptions and ensure all relevant data were included. As the transcripts were linguistically comprehensible, they were not returned for participant verification. Instead of returning the results for participant feedback, which could have strengthened the credibility, the validity of the interpretations and the minimisation of biases were ensured through team discussions. 33 The first researcher had no prior experience in addiction treatment, supporting an objective stance throughout the interviews and analysis. 34
The first researcher created a table visualising the study's themes, as reviewed by the other two researchers. Table 4 outlines the analysis process with illustrative examples, supporting credibility and dependability. 33 Authentic quotations were included to demonstrate the connection between data and findings. 34
Example of data analysis.

Conclusions
To reduce drug-related harm, it is important to increase the visibility and ethics of communication across various contexts, such as healthcare systems and society more broadly. Strengthening the role of health authorities as communicators – especially regarding services – and promoting equality in communication compared to other patient groups is essential. Open and responsible communication that highlights facts and uses both factual and humane language could help normalise discussions around drug use. Early integration of such communication into everyday environments – particularly family settings – may also support the prevention of related problems. Within healthcare, raising awareness of addiction disorders and developing communication and encounter skills is crucial to appropriately reach and support those in need. The findings advocate the central role of low-threshold services and the importance of involving PWUDs and lived experience experts in developing communication for harm reduction.
Implications
The findings highlight the essential role of visible and ethical communication in raising awareness of effective treatments and support services for substance use disorders, building trust in healthcare and encouraging help-seeking. They encourage healthcare organisations to strengthen professionalism and foster a respectful culture which could help individuals access support, and enhance positive, well-functioning healthcare teams. Future efforts are also encouraged to promote open, responsible and early communication to prevent harm. The results further affirm the value of face-to-face encounters and shared dialogue in reducing drug-related harm.
Supplemental Material
sj-docx-1-njn-10.1177_20571585261427865 - Supplemental material for Nursing professionals’ perceptions of communication to reduce drug-related harm: A descriptive qualitative study in Finland
Supplemental material, sj-docx-1-njn-10.1177_20571585261427865 for Nursing professionals’ perceptions of communication to reduce drug-related harm: A descriptive qualitative study in Finland by Satu Nurkkala, Tarja Kvist and Petra Kämäräinen in Nordic Journal of Nursing Research
Supplemental Material
sj-docx-2-njn-10.1177_20571585261427865 - Supplemental material for Nursing professionals’ perceptions of communication to reduce drug-related harm: A descriptive qualitative study in Finland
Supplemental material, sj-docx-2-njn-10.1177_20571585261427865 for Nursing professionals’ perceptions of communication to reduce drug-related harm: A descriptive qualitative study in Finland by Satu Nurkkala, Tarja Kvist and Petra Kämäräinen in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We thank the contact persons of the Wellbeing Services County and all the participants for their contributions to the research.
Ethical statement
The study was conducted following the ethical principles of the Helsinki Declaration. The ethical regulations governing Finnish research do not require ethical approval for studies that do not involve patients, cause no harm and do not involve intervention in physical integrity (Finnish National Board on Research Integrity TENK, 2019). As the present study meets these criteria, no ethical approval was required or sought. Study participants, nurses, not patients, were provided with information about the research and its voluntary nature. At the beginning of the interview, they were asked to give verbal consent to participate in the study.
Author contributions
All authors have contributed significantly to the work and have approved the final manuscript. S.N. (MHS): Conceptualisation and design, methodology, data collection, data analysis, writing (original draft and revision, tables). T.K. (PhD, professor): Conceptualisation and design, methodology, validation, writing (original draft and revision), supervision. P.K. (MHS, doctoral researcher): Conceptualisation and design, methodology, validation, writing (original draft and revision), supervision.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.