
Abstract
Background:
Over 3 million Americans have an opioid use disorder (OUD), and only a fraction receive treatment. Public opinion is crucial in enacting evidence-based policies. Few studies have examined the public’s perception of blame for the ongoing opioid overdose epidemic directed at distinct groups. We assessed US adults’ perceived blameworthiness for the epidemic and examined factors that may influence the perceived blameworthiness.
Methods:
We conducted a national survey in 2022 using the AmeriSpeak® panel to assess US adults’ perception of blame toward individuals with an OUD and external contributors. Of the 3335 eligible panel members invited to participate, 1233 (37%) completed the survey. We developed a measure of knowledge and understanding of OUD, with a higher value indicating a greater understanding of the nature of OUD and recovery—including knowledge and beliefs on evidence-based treatment and relapse. We analyzed the relationships between sources of blame, knowledge, and understanding of OUD, and individual-level correlates.
Results:
Higher score of knowledge and understanding of OUD was associated with lower odds of blaming individuals with OUD (odds ratio [OR] = 0.73, 95% confidence interval [CI] = [0.51, 1.05]) and greater odds of blaming external contributors: healthcare providers (OR = 1.49, 95% CI = [1.05, 2.12]), pharmaceutical companies (OR = 2.17, 95% CI = [1.50, 3.15]), and health insurance companies (OR = 1.42, 95% CI = [0.97, 2.09]). Those who are female, non-Hispanic White, Democrat, have higher education, or have friends or family who misused opioids tended to score higher in knowledge and understanding of OUD.
Conclusions:
Perceived blameworthiness for the opioid overdose epidemic is related to knowledge and understanding of OUD. Public health campaigns with a bipartisan agenda to increase evidence-informed knowledge about OUD targeting people of color and with lower education may help reduce the blame toward people with an OUD, which in turn may increase support for evidence-informed policies.
Highlights
US adults’ perception of blame for the opioid overdose epidemic is related to knowledge and understanding of opioid use disorder (OUD) regarding the nature of OUD, evidence-based treatment, and recovery.
Americans with a greater understanding and knowledge of OUD may support policies designed to help individuals with an OUD because they are less likely to blame people who have (or had) an OUD or misuse (or misused) opioids.
Understanding and knowledge of OUD differ by race/ethnicity, political affiliation, education, and having a personal connection with individuals who misuse (or misused) opioids.
Introduction
The United States is in an ongoing battle against the opioid overdose epidemic. The opioid overdose death rate increased by 381% from 2010 to 2021, 1 and provisional data suggest that nearly 83 000 opioid-involved overdose deaths likely occurred in the United States, 2022. 2
The epidemic is driven by opioid use disorder (OUD). OUD is characterized by clinically significant impairment or distress because of opioid use. Specifically, OUD may present as health problems, disability, or failure to meet work, school, or home responsibilities. 3 Over 3 million people in the United States are estimated to meet the OUD criteria. 4 While evidence supports Food and Drug Administration (FDA)-approved medications 5 and policies for supporting individuals with OUD, 6 only 7.1% to 13.4% of US adults with OUD received treatment in 2015 to 2019.7,8
Public opinion is crucial in enacting public policies.9,10 Increased public support for evidence-based strategies (eg, increasing access to naloxone, medication for addiction treatment, and emergency care for overdose with limited immunity from criminal consequences) is vital to curtail the opioid crisis. Attribution theory11,12 suggests that people interpret others’ behaviors in relation to their perceptions of what causes those behaviors. Studies reported that public support for solutions to stigmatized health conditions, including OUD, may be influenced by the public’s perceptions of who is responsible or “to blame” for the condition.13-15 For example, when individuals experiencing a stigmatized condition such as mental illness and substance use disorder are perceived as personally responsible for their condition, the public is more likely to support punitive policies against these individuals. 16 Whereas, when situational factors beyond the individual’s control are perceived to be to blame, the public prefers policies designed to compensate or help individuals with a stigmatized condition.14,17
Several groups are often blamed for the opioid crisis. First, pharmaceutical companies downplayed the risk of addiction and misled physicians and the healthcare industry about the benefits of opioids.18-21 Relatedly, physicians who overprescribed opioids and health insurance companies that failed to encourage safer and effective alternatives22,23 are often viewed as culpable for the epidemic. 24 On an individual level, individuals who have (or had) an OUD or misuse (or misused) opioids are often viewed as personally responsible for their predicament. 25 People who use opioids are often blamed for lacking self-control, and their addiction is perceived as the product of willful misconduct. 26 Finally, friends or family members are reported as one of the common sources to obtain illicit opioids and sometimes accused for providing the drugs.23,27,28
Knowledge and understanding of OUD and effective treatment may influence perceptions of who is to blame for the epidemic and further policy preferences. Substance use disorders are considered medical conditions rather than behavioral choices in neurobiological research. 29 Regarding OUD as a medical condition is associated with lower levels of stigma, not endorsing OUD as a crime, and agreeing with policies to help people access OUD treatment. 30 However, to our knowledge, no studies have examined if increased knowledge and understanding of OUD deters opioid overdose epidemic blame away from individuals as opposed to external contributors.
Other factors may influence the perception of blame for the epidemic. OUD stigma varies based on partisan media consumption 31 and political affiliation; self-identified Republicans report higher OUD stigma than Democrats 32 and are more likely to endorse punitive efforts like mandatory sentences and prosecuting illicit drug use.32-34 Young people hold less stigma toward OUD, though racial difference remains mixed.30,32 Furthermore, personal opioid misuse may help one relate to the challenges of OUD and is thus associated with holding less stigma toward the condition. 20
The public’s perceptions of who is “to blame” for the opioid crisis can influence policy preferences.13-15,17 This study assessed US adults’ perceived blameworthiness for the epidemic and what factors are associated with the blameworthiness toward distinct groups. This study also explored the potential role of OUD knowledge that may influence the perceived blameworthiness.15,17
Methods
Participants
We conducted a survey using a representative sample of US adults ages 18 and older drawn from NORC’s AmeriSpeak® Panel. AmeriSpeak is a probability-based noninstitutionalized panel of over 45 000 panel members designed to be representative of the US household population. The sample was selected using strata based on age, race, ethnicity, education, and gender. Details about the sampling frame can be found in Supplemental Appendix A.
Procedures
The survey was offered in English and Spanish, online and by phone, from April 21 to May 3, 2022, and took average 20 minutes to complete. As part of AmeriSpeak’s monthly Omnibus survey, randomly selected eligible panel members were invited to participate. Voluntary and informed consent was obtained from all respondents. AmeriSpeak’s Omnibus survey is used to understand the public opinion, attitudes, and behavior of the US population. Respondents who did not respond to the initial outreach were contacted by phone and email several times. Participants were offered the cash equivalent of $5 to $7. Of the 3335 eligible panel members invited to participate, 1233 (37%) completed the survey. The study was approved by the NORC Institutional Review Board. Weighting adjustment was made based on age, gender, census division, race, ethnicity, education, housing tenure, and household phone status to address oversampling of certain subgroups and nonresponses (see Supplemental Appendix A about the weighting procedure).
Measures
Sources of Blame for the Opioid Overdose Epidemic
We assessed what entities participants blamed “for the opioid epidemic” on a 5-point Likert scale adapted from previous blame research from “not at all to blame” to “completely to blame.” 35 The 5 blame sources included: (a) people who have/had an OUD or misuse/misused opioids; (b) healthcare providers who prescribed opioids; (c) friends/family members who introduced their friends/family to opioids; (d) pharmaceutical companies that produced opioids; and (e) health insurance companies. For analyses, responses were dichotomized into a “not to blame” (encompassing “not at all to blame,” “might be to blame,” and “a little bit to blame”) and “to blame” (“moderately to blame” and “completely to blame”) and used as our primary outcomes.
Knowledge and Understanding of OUD
We developed a set of 29 items of knowledge and beliefs related to OUD based on National Institute on Drug Abuse (NIDA)’s fact sheets on general misperceptions of opioids 36 and feedback from an advisory workgroup and substance use researchers. This measure has shown good reliability in prior research.30,37 Respondents reported their agreement to each item on a 5-point Likert scale from “strongly disagree” to “strongly agree.” We conducted the principal component analysis to select coherent items that represent a substantial variation and are closely related to knowledge of OUD; 8 principal components had eigenvalues >1, and we selected the items with factor loadings >0.3 from the first component. This resulted in 13 items, and we further deselected 2 items that did not represent the knowledge or understanding of OUD but rather opinions about what their friends and doctors should do. The resulting 11 items represented regarding OUD as a medical condition, knowledge and attitude about the condition, available treatments, and recovery process. Full-item wording can be found in Supplemental Appendix B.
We calculated the average of the 11 items per person to represent knowledge and understanding of OUD, with a higher value indicating a greater understanding of the nature of OUD and recovery, including knowledge and beliefs on evidence-based treatment and relapse (α = .73); the score was used as our secondary outcome.
Experience of Opioid Misuse
Personal opioid misuse was assessed by asking if they had ever taken an “opioid medication (e.g., fentanyl, oxycodone, hydrocodone, methadone, buprenorphine, etc) in a way other than as directed by a medical provider or non-prescribed/illegal opioids.” Participants were also asked if they have “any family members or close friends ever had OUD or misused opioids, used in a way other than prescribed/intended or developed a problem with them.” Personal experience and indirect experience via family/friends opioid misuse were assessed with “Yes, within the last year,” “Yes, more than a year ago,” or “No” response options.
Personal Characteristics
The AmeriSpeak panel’s sociodemographic characteristics are updated annually. In this study, we included gender (male, female), age (18-29, 30-44, 45-59, 60 or older), race/ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, non-Hispanic other or multiracial, Hispanic), education (less than high school, high school graduate or equivalent, vocational degree, Bachelor’s degree, postgraduate degree), census regions, household income (<$30 000; $30 000-$59 999; $60 000-$99 999; $100 000 or higher), and employment (full-/part-time employed, unemployed, not in labor force). We measured political affiliation by asking “do you consider yourself a Democrat, a Republican, an Independent, or none of these?” on this survey.
Analytic Plan
We calculated descriptive statistics of survey respondents’ characteristics. We analyzed bivariate associations using Rao-Scott chi-square tests between each source of blame and independent variables. We used multivariate logistic regressions for each of the 5 dichotomized sources of blame on independent variables: knowledge and understanding of OUD, age, gender, census region, political affiliation, race/ethnicity, income, education, and employment status. To assess whether our findings were sensitive to the way we dichotomized the level of blame, we conducted a sensitivity analysis using proportional odds models for each outcome without dichotomizing them. We report weighted odds ratios (OR) and 95% confidence intervals (CI) to reflect uncertainty around the OR. We also examined what factors are associated with individual’s knowledge and understanding of OUD by using multivariate linear regression. We report weighted regression coefficients and 95% CIs. All analyses were conducted in SAS/STAT, Version 9.4 of the SAS System, SAS Institute Inc.
Results
Two-thirds of survey participants (66.9%, 95% CI = [63.2, 70.6]) blame (indicated by responding moderately or completely to blame) friends or family who introduced their friends or family to opioids for the epidemic. The next most common sources of blame were pharmaceutical companies that produced opioids (55.1%, 95% CI = [51.2, 59.0]), followed by healthcare providers (50.9%, 95% CI = [47.0, 54.8]); individuals who have/had an OUD (41.8%, 95% CI = [37.9, 45.6]); and health insurance companies (33.8%, 95% CI = [30.1, 37.6]).
Table 1 shows summary statistics on the survey participants’ characteristics. Close to a quarter of adults are estimated to have ever misused opioids, and about a third has friends/family members who have ever misused opioids. The average score of knowledge and understanding of OUD was 3.7 in the 1 to 5 range.
Characteristics of Adult Survey Participants in the United States, 2022 (n = 1233). a
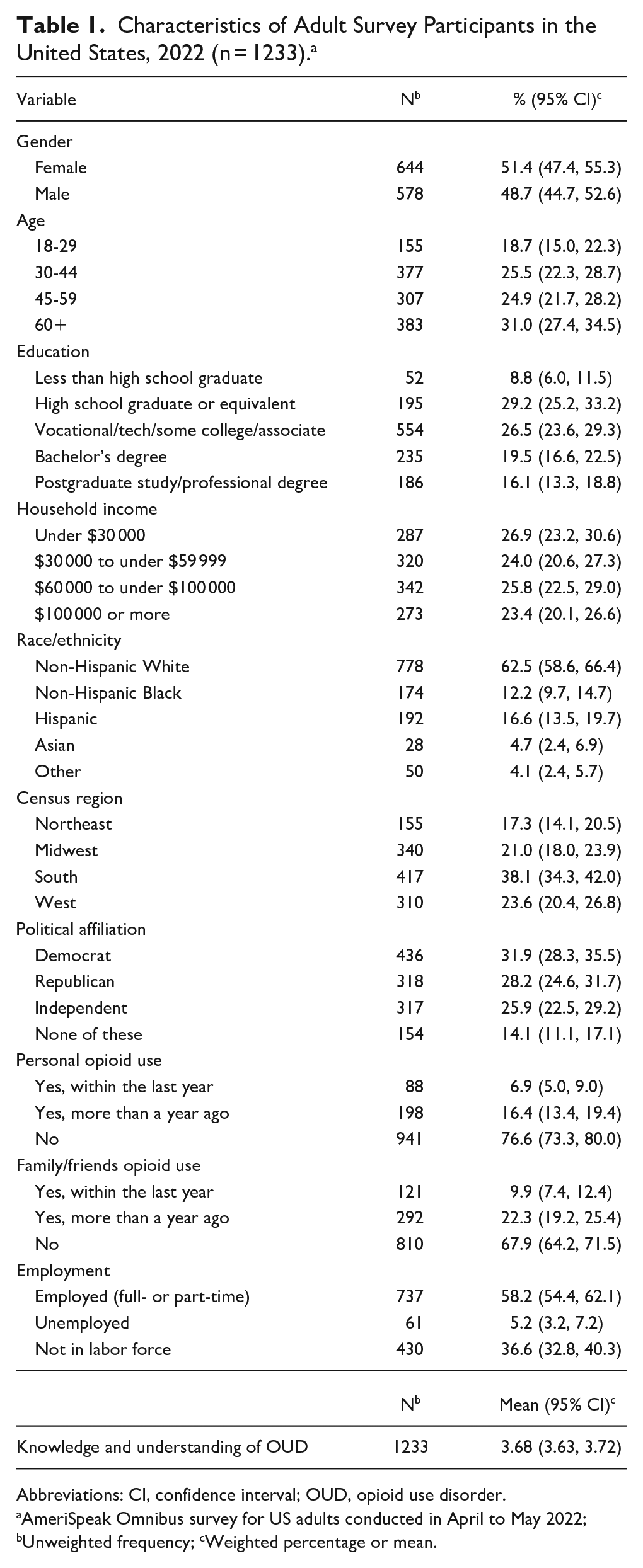
Abbreviations: CI, confidence interval; OUD, opioid use disorder.
AmeriSpeak Omnibus survey for US adults conducted in April to May 2022; bUnweighted frequency; cWeighted percentage or mean.
Figure 1 presents the average score of knowledge and understanding of OUD by the level of blame directed at each source. The average score generally decreases as the level of blame directed at people who have/had an OUD increases; whereas, it increases with increasing levels of blame directed at healthcare providers. The respondents saying external contributors are “completely to blame” have the highest average scores of knowledge and understanding of OUD.
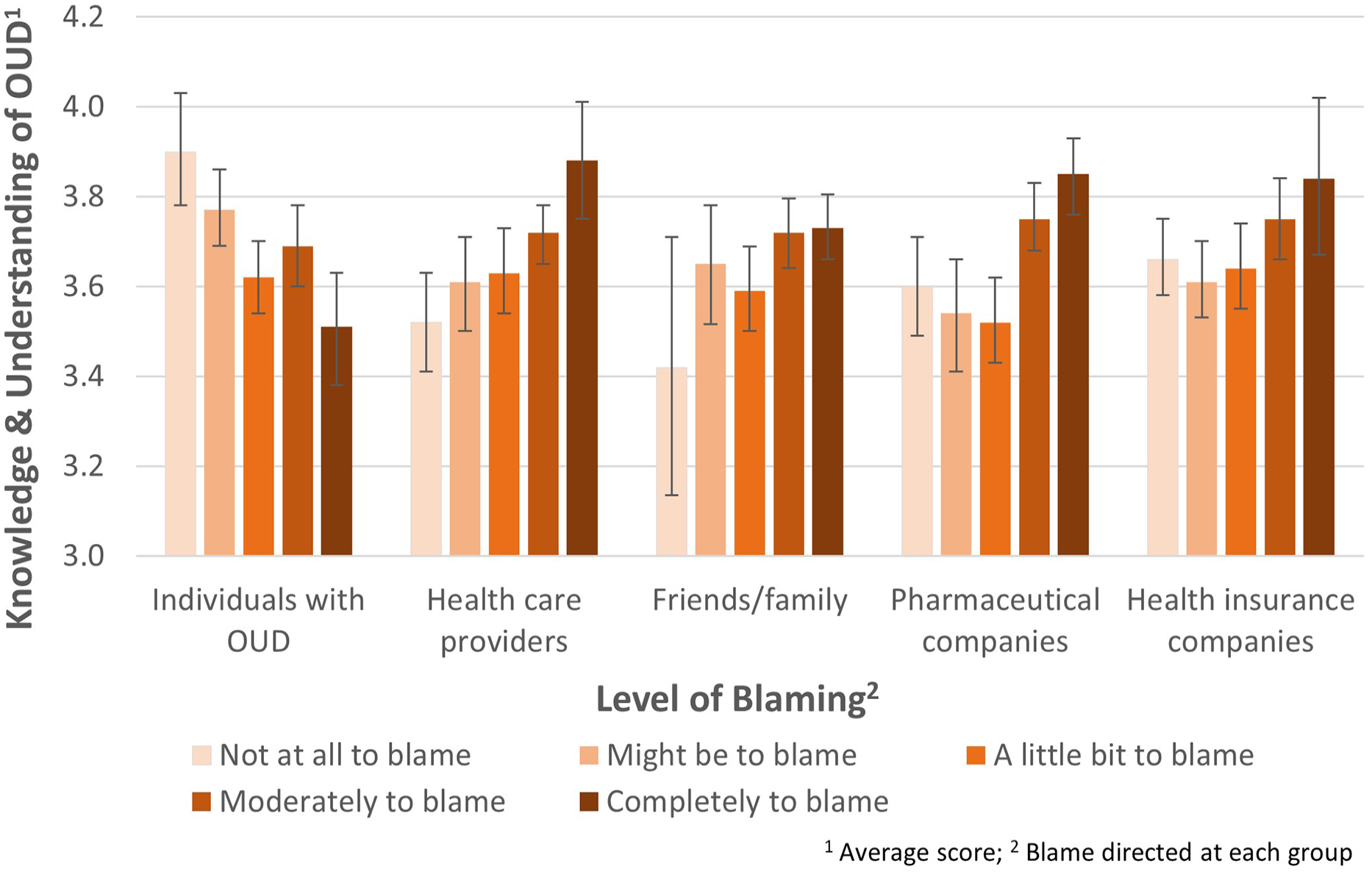
Knowledge and understanding of OUD and blameworthiness directed at various sources in 2022. The y-axis shows the average score of knowledge and understanding of OUD. The x-axis shows the level of blame directed at each source; a darker color reflects more blaming. The error bars indicate 95% confidence intervals of the average scores.
Sources to blame also varied by political affiliation. One-third of self-identified Democrats (33.7%, 95% CI = [27.5, 40.0]) blamed individuals who have/had OUD, while 53.6% (95% CI = [46.2, 61.1]) of Republican participants blamed them. The largest difference between Democrat and Republican affiliations was for blame directed at pharmaceutical companies (66.4%, 95% CI = [59.9, 72.8] of Democrats vs 38.8%, 95% CI = [31.7, 45.8] of Republicans).
Table 2 shows multivariate logistic regression results. One more point in the average score of knowledge and understanding of OUD was associated with (1) 27% lower odds of blaming individuals who have/had an OUD, (2) 49% greater odds of blaming healthcare providers, (3) 117% greater odds of blaming pharmaceutical companies, and (4) 42% greater odds of blaming health insurance companies, controlling for covariates. Compared to self-identified Democrats, Republicans had 131% greater odds of blaming individuals who have/had an OUD, 36% lower odds of blaming healthcare providers, 69% lower odds of blaming pharmaceutical companies, and 64% lower odds of blaming health insurance companies.
Perceived Blameworthiness Toward 5 Different Entities and Respondent Characteristics. a
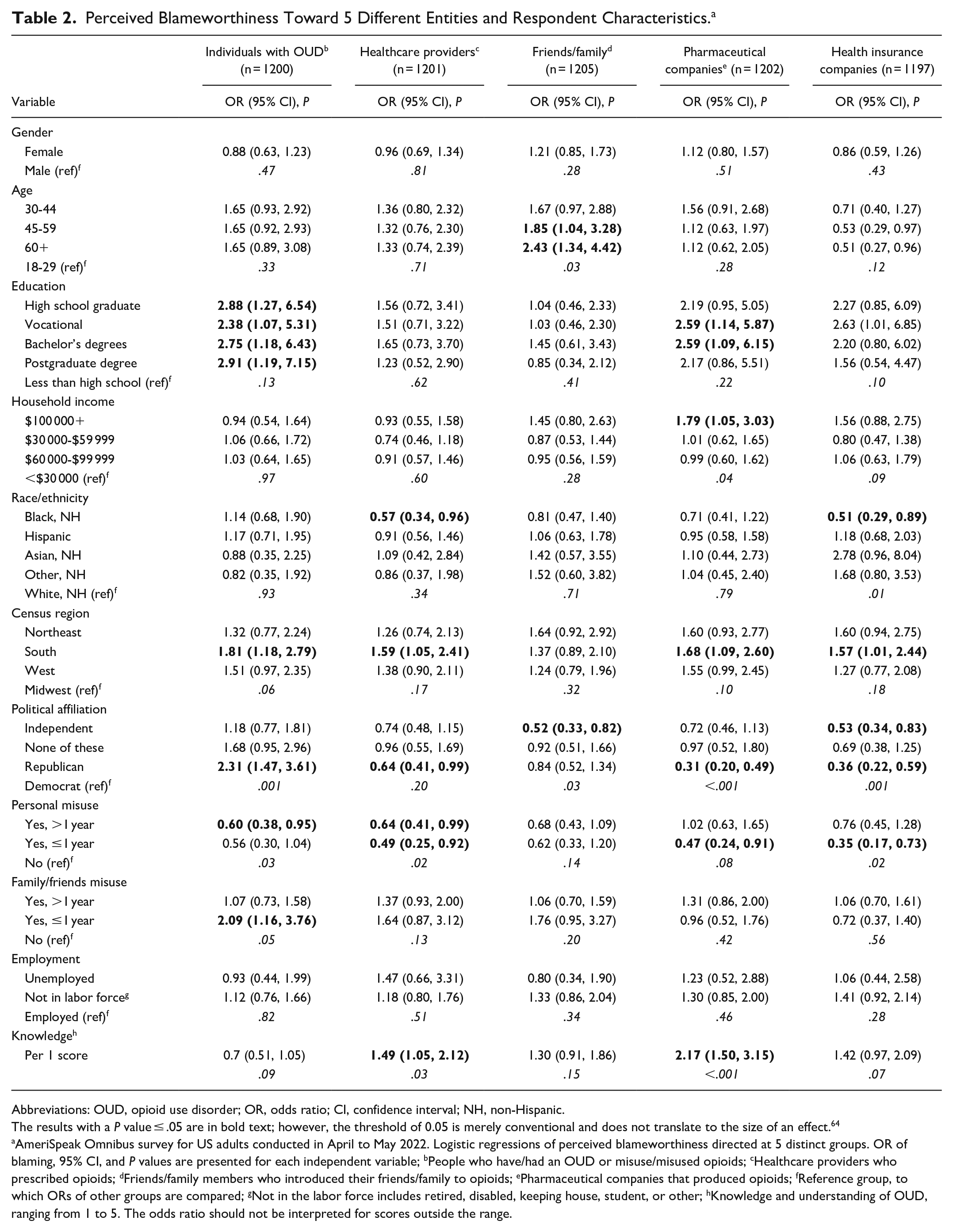
Abbreviations: OUD, opioid use disorder; OR, odds ratio; CI, confidence interval; NH, non-Hispanic.
The results with a P value ≤ .05 are in bold text; however, the threshold of 0.05 is merely conventional and does not translate to the size of an effect. 64
AmeriSpeak Omnibus survey for US adults conducted in April to May 2022. Logistic regressions of perceived blameworthiness directed at 5 distinct groups. OR of blaming, 95% CI, and P values are presented for each independent variable; bPeople who have/had an OUD or misuse/misused opioids; cHealthcare providers who prescribed opioids; dFriends/family members who introduced their friends/family to opioids; ePharmaceutical companies that produced opioids; fReference group, to which ORs of other groups are compared; gNot in the labor force includes retired, disabled, keeping house, student, or other; hKnowledge and understanding of OUD, ranging from 1 to 5. The odds ratio should not be interpreted for scores outside the range.
Respondents who have ever misused opioids were less likely to blame individuals with OUD than those who have not; in fact, they were less likely to blame any sources considered in this study, especially if the personal misuse occurred within the last year. In contrast, individuals with friends/family members who have misused opioids in the past year were significantly more likely—the odds were twice greater—to blame individuals who have/had an OUD than those without friends/family member experience in the previous year. Respondents with income over $100 000 were more likely to blame pharmaceutical companies than those making less than $30 000.
The sensitivity analysis using proportional odds models without dichotomizing the sources of blame measures produced comparable results as in Table 2. The cumulative odds of blaming individuals who have/had an OUD below any fixed level decreased with greater score of knowledge and understanding of OUD; for example, the odds of blaming individuals with an OUD a little bit or less is 44% lower for one score increase, than the odds of blaming them moderately or completely (OR = 0.56, 95% CI = [0.41, 0.76]). On the contrary, the cumulative odds of blaming external contributors increased with greater score. The results can be found in Supplemental Appendix C.
We further examined what is associated with knowledge and understanding of OUD among US adults using a multivariate linear regression (Table 3). Age, income, census region, and employment were removed from the final model because of their large P values; however, we included the personal opioid misuse, despite its large P value, to compare its result with indirect experience of opioid misuse by friends/family. Having friends/family members who have misused opioids more than a year ago was associated with higher scores, though personal opioid misuse appeared to be not associated with the outcome. Women scored slightly higher, on average, than men. Self-identified Democrats had greater scores than Republicans, Independents, and nonaffiliated participants. Having higher education was also associated with greater scores. Compared to non-Hispanic White, all other race/ethnic groups tended to have lower scores.
Knowledge and Understanding of OUD and Respondent Characteristics. a
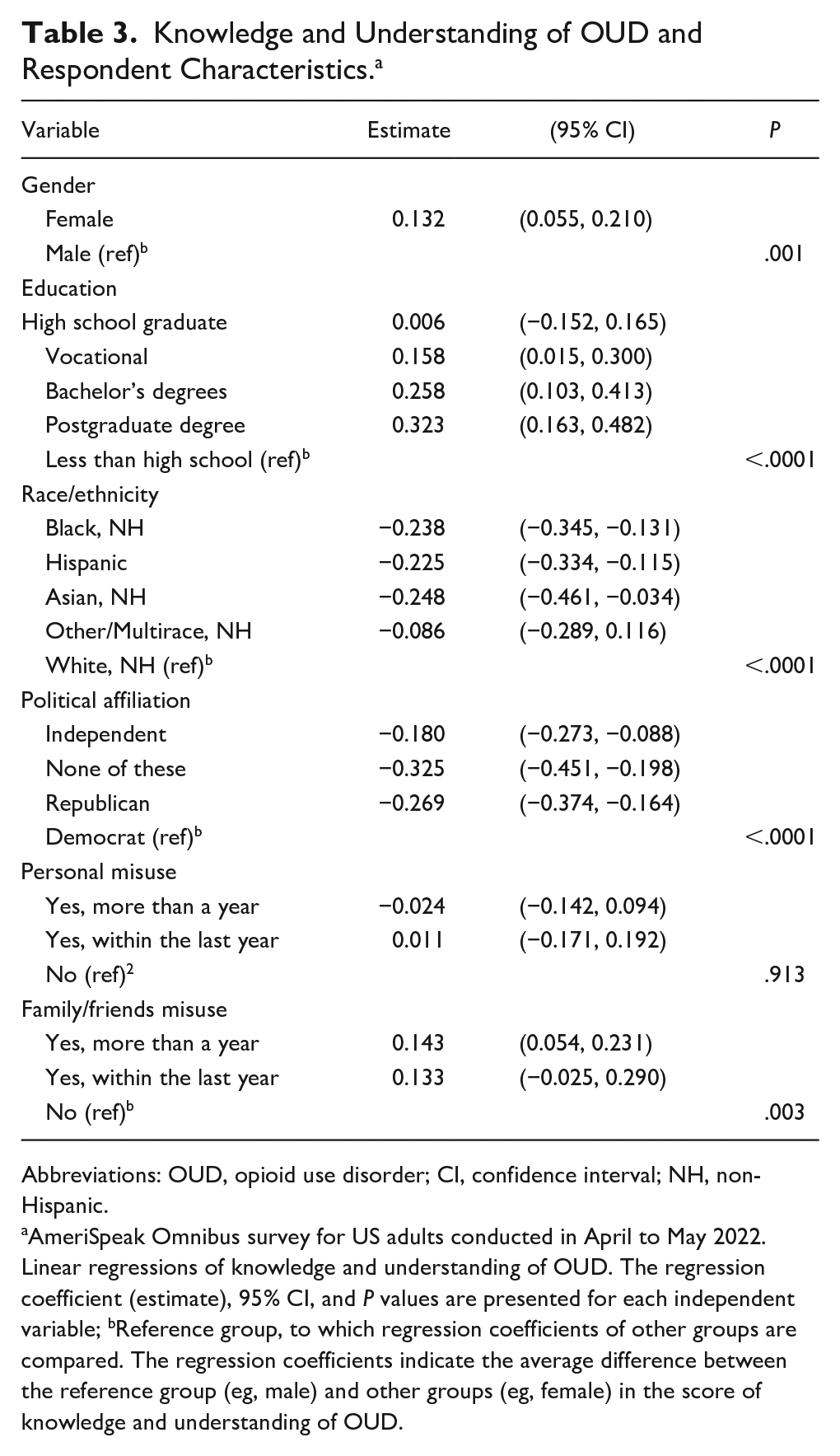
Abbreviations: OUD, opioid use disorder; CI, confidence interval; NH, non-Hispanic.
AmeriSpeak Omnibus survey for US adults conducted in April to May 2022. Linear regressions of knowledge and understanding of OUD. The regression coefficient (estimate), 95% CI, and P values are presented for each independent variable; bReference group, to which regression coefficients of other groups are compared. The regression coefficients indicate the average difference between the reference group (eg, male) and other groups (eg, female) in the score of knowledge and understanding of OUD.
Discussion
This study assessed US adults’ perceived blameworthiness for the opioid overdose epidemic and potential factors associated with the blameworthiness. Greater knowledge and understanding of OUD, defined as an understanding of the nature of OUD and recovery—including knowledge and beliefs on evidence-based treatment and relapse, was associated with a lower likelihood of blaming individuals who have/had an OUD and more likelihood of blaming external contributors: pharmaceutical companies, healthcare providers, and health insurance companies. Our findings indicate that knowledge and understanding of OUD are associated with individuals’ perceived blameworthiness, suggesting that building a better understanding of the disorder among adults may help increase preference for policies that support individuals with OUD, as opposed to criminalizing them.15,17
Extant literature supports our findings in that greater understanding of health conditions can directly relate to the levels of stigma toward those conditions. For example, greater education to improve mental health literacy and increased knowledge about HIV are associated with reduced stigma and positive attitudes toward these conditions.38-42 However, few studies have addressed pathways between knowledge, stigma, and perceptions of blame toward health conditions like OUD. This study indicates that OUD knowledge is associated with blame for entities involved. More studies, including longitudinal studies, are needed to better parse the relationships between knowledge, stigma, and assignments of blame.
Attribution theory helps explain the observed associations between the perceived blameworthiness and the measure of knowledge and understanding of OUD. A few instrument items used to assess knowledge and understanding of OUD in this study are directly relevant to internal attribution,11,12 including the items describing people with an OUD “lack self-control” and “can choose to quit using opioids at any time” (Supplemental Appendix B). Internal attribution assigns blame to personal characteristics, while external attribution assigns blame to situations or factors outside a person’s control.11,12 Attribution studies suggest that different types of attribution influence stigma toward certain health conditions and policy preferences.43,44 For example, people with substance use disorder are often viewed as having more control over their condition, and this perception of internal attribution can lead to anger and hostility from the public,45,46 and often lead the public to believe that those who experience substance use disorders deserve the negative consequences and social isolation.25,47,48 On the contrary, external attributions put greater responsibility to, for example, food industry for obesity and the smartphone industry for smartphone addiction,49,50 leading to favorable opinions toward policies punishing the industry and supporting individuals with the condition. The perceived blameworthiness of individuals with disorders may shape motivations to support or punish them through public policies.30,46
Public health advocates’ strategies may guide how to reduce the perception of internal attribution and increase external attribution. It is well documented that the tobacco industry used a personal responsibility argument to shift responsibility away from the tobacco companies and onto their customers who suffered smoking-related diseases in the context of litigation and to gain public support for a perceived right to smoke.51,52 This tactic has been adopted by food, beverage, and alcohol industries to sway public opinion and policymakers’ actions by stressing consumers’ responsible product use. 53 Tobacco control and public health advocates emphasized the failure of corporate responsibility (such as manipulative marketing) to create support for regulation and taxation to protect vulnerable consumers.54,55 Similarly, framing the discussion of OUD with a focus on the addictive nature of opioids and the actions of the policymakers that can change the environment will help deter opioid overdose epidemic blame away from individuals and further increase support for evidence-informed policies. 56
Another important finding of this study is that perceived blameworthiness was associated with personal opioid misuse. Adults who have ever misused opioids, compared to those who have not, were less likely to blame individuals with OUD and other sources examined in this study. This suggests that people with personal misuse experience tend to blame less or not blame, probably because they often have less stigmatizing attitudes toward the condition.13,30,57 Conversely, we also observed that having friends/family members who ever had OUD or have misused opioids was associated with blaming individuals with OUD. This finding is consistent with other studies; those whose close friends/family members misused opioids are more likely to gravitate toward internal attribution. 58 Based on our study, about 1 in 10 adult Americans—approximately 26 million—had friends/family members who have misused opioids within the last year in 2022. We need to account for these Americans who indirectly experienced opioid misuse and OUD through friends or family when designing policy interventions and communication strategy. These family members and friends likely observed the struggles that opioids posed for their family members or friends as individuals and that part was most salient for them.59,60
Our results also show that greater educational attainment, non-Hispanic White race/ethnicity, Democratic political affiliation, and personal connection to individuals with OUD were associated with a higher score of knowledge and understanding of OUD. A public health campaign with a bipartisan agenda to increase evidence-based knowledge about OUD targeting people of color and those with lower education may help reduce blame toward people with OUD and increase support for policies that help individuals in need. 30 While research on perceptions of communities of color toward OUD remains limited, research suggests that the Black community may view OUD through a lens reminiscent of the crack cocaine epidemic era, fearing the stigma of criminalization and social judgment.61-63 The nuanced perspectives and cultural experiences within these communities should be studied further and accounted for when designing the educational campaigns.
Our study has limitations. First, the survey was conducted in April to May 2022 and may not represent more recent US adults’ perceptions of blame for the opioid overdose epidemic. Since the data collection, US adults’ perceptions of blame may have been influenced by recent increased bipartisan support for evidence-based policies and media about the role of major opioid manufacturers in creating and perpetuating the epidemic. In late summer 2023, a naloxone formulation became available over-the-counter, and an increasing number of restaurants and bars stock them to prevent opioid overdoses and deaths; these recent changes may have increased awareness of OUD and available treatment. Also, our analyses utilizing the dichotomized level of blame may have not fully reflected the nuanced levels of blame reported; however, our sensitivity analysis resulted in a similar conclusion (Supplemental Appendix C). Third, we measured knowledge and understanding of OUD using 11 items selected from 29 items. Although we used principal component analysis to select coherent items, there is a chance that we missed important items that reflect different dimensions of OUD knowledge. Fourth, we examined perceived blameworthiness toward the 5 groups, but other entities are also blamed for the opioid crisis, including prescription drug distributors, the Joint Commission, and hospital administrators.24,65 Finally, our cross-sectional survey design presents observed associations and does not allow causal inference that knowledge and understanding of OUD may influence perceptions of blame for the epidemic. Longitudinal research is needed to examine the role of knowledge and understanding of OUD in pathways to perceived blameworthiness.
Effective policy interventions to combat the opioid crisis are contingent on a unified societal commitment. However, such support can be hindered by divergent beliefs concerning the origins, nature of the problem, and responsibility for the crisis. Our analysis of public perceptions of blame informs the development of targeted educational campaigns and interventions to improve knowledge and understanding of OUD.
Conclusion
This study examined US adults’ perceived blameworthiness for the opioid overdose epidemic and its association with knowledge and understanding of OUD. Greater knowledge and understanding of OUD were associated with a lower likelihood of blaming individuals who have/had an OUD and greater likelihood of blaming external contributors. This study also found that certain demographic characteristics and a personal connection with people suffering from OUD were associated with the level of knowledge and understanding of OUD. These findings suggest the need for public health campaigns to increase the knowledge and understanding of OUD.
Supplemental Material
sj-docx-1-saj-10.1177_29767342241262556 – Supplemental material for Pointing Fingers: Who US Adults Blame for the Opioid Overdose Epidemic
Supplemental material, sj-docx-1-saj-10.1177_29767342241262556 for Pointing Fingers: Who US Adults Blame for the Opioid Overdose Epidemic by Yoonsang Kim, Alex Kresovich, Kai MacLean, Phoebe Lamuda, Marie Ngobo-Ekamby, Cedasia McQueen, John Schneider, Harold A. Pollack and Bruce G. Taylor in Substance Use & Addiction Journal
Footnotes
Author Contributions
YK led the conceptualization of the research question, data analysis, results interpretation, and manuscript writing. BGT and PL primarily contributed to conceptualizing the research question, interpreting results, and revising the manuscript. AK and KM contributed to the literature review and manuscript writing. MNE and CM were responsible for the literature review and data analysis. JS and HAP reviewed and revised the entire manuscript. All authors have reviewed, edited, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute on Drug Abuse (NIDA) through the Justice Community Opioid Innovation Network (JCOIN), Methodology and Advanced Analytics Resource Center (MAARC) under award number 1U2CDA050098 (PIs: John Schneider and Harold A. Pollack) and subaward to NORC at the University of Chicago (AWD100228). The contents of this publication are the authors’ responsibility and do not necessarily represent the views of NIDA.
Compliance,Ethical Standards,and Ethical Approval
The study was reviewed and approved by the Institutional Review Board, NORC at the University of Chicago.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.