
Abstract
Background and Objectives:
Youth substance use is associated with significant psychological, neurological, and medical complications. Risk factors for substance use among children and adolescents in the general population include peer and/or parental substance use, certain psychiatric illnesses (eg, Attention-Deficit/Hyperactivity Disorder, depression), and history of maltreatment. Co-occurring substance use and psychiatric illness have been associated with increased suicidality, but few prior studies have characterized substance use among child/adolescent inpatients. As such, it remains unclear how substance use contributing to acute psychiatric presentations has changed since the start of the COVID-19 pandemic.
Methods:
This is a retrospective cohort study of 816 unique child/adolescent psychiatry inpatients with urine drug screening (UDS) results from a diverse urban setting. Charts of patients hospitalized between June 1, 2018 and November 30, 2021 were reviewed for sociodemographic characteristics, indication for admission, psychiatric history, hospital course, treatment plan, and discharge diagnosis. Differences in sociodemographic and clinical characteristics, such as age, race, and diagnoses, between patients with and without positive UDS were explored throughout various periods of the COVID-19 pandemic. Descriptive and comparative statistics were performed, as well as a logistic regression model to identify the predictors of positive UDS.
Results:
Of the study sample, 18% had a positive UDS. Older age, diagnosis of impulsive or behavioral disorder, and a history of violence were found to be predictors of positive UDS. Asian/South Asian or Hispanic/LatinX race and history of a developmental or intellectual disability were found to be negative predictors. The frequency of positive UDS in this population did not change based on COVID-19.
Discussion and Conclusions:
Multiple factors may predispose children and adolescents to substance use. Though no impact of COVID-19 was found in this sample, longer-term studies are needed.
Scientific Significance:
This study identifies independent predictors of active substance use in the child and adolescent psychiatric inpatient population.
Keywords
Highlights
There are multiple sociodemographic factors which may predispose children and adolescents to substance use, including older age, White race, and history of violence or child protective services involvement.
Psychiatric contributors to substance use may include a history of impulsive or behavioral disorder, as well as history of suicide attempts.
This study found no impact of the COVID-19 pandemic on substance use in child and adolescent psychiatric inpatients.
Introduction
The majority of substance use begins during adolescence, often between 15 and 17 years of age, though at times as early as age 10. 1 This time period involves neurodevelopmental and psychosocial changes that increase the risk of engaging in substance use. 2 Exposure to substances during adolescent neurodevelopment affects key brain areas impacting attention, learning, and memory, and increases the risk for developing psychiatric disorders.3,4 Structural effects include smaller volumes in the prefrontal cortex and amygdala in adolescent marijuana consumers, accelerated decrease in gray matter in frontal regions in adolescent alcohol consumers, and impaired hippocampal cell genesis in cocaine exposure.5 -7 Substance use in adolescence has been associated with significantly increased risk of developing substance use disorders (SUDs) in adulthood, with research showing that age at first substance use inversely correlates with lifetime incidence of developing a SUD.8,9 In the United States, alcohol has been the most misused substance in the child and adolescent (CA) population, followed by marijuana, with studies finding 36% of youth reporting lifetime use and 22% reporting current use.1,10
Psychiatric disorders, particularly attention-deficit/hyperactivity disorder (ADHD) and depression, have been associated with an increased risk of substance use.9,11 -13 Co-occurrence of substance use and mental health problems has been attributed to common underlying vulnerabilities (eg, poor executive functioning, family dysfunction), “self-medication” of psychiatric symptoms, and adverse impacts of substance use on the developing brain. 14 Other factors that might increase the risk of substance use in the CA population have been identified, including male gender, child maltreatment (physical, sexual, emotional abuse), behavioral disinhibition, aggression, poor self-regulation, and antisocial behaviors.9,12 Maladaptive parenting practices, parental substance use, and peer substance use also likely contribute. 15 Youth with co-occurring substance use and mental health problems are at an increased likelihood for emergency department visits and subsequent hospitalization and use a greater amount of acute care resources. 16 However, few studies have characterized co-occurring substance use among adolescent psychiatric inpatients, highlighting the importance of further research.17,18
Coronavirus disease 2019 (COVID-19), the disease caused by the SARS-CoV-2 virus, has amplified the risk factors for substance use, including increasing stress, family system changes and dysfunction, and social isolation.19 -21 An early study found that adolescent substance use among the general population increased at the start of the pandemic, while subsequent studies found that adolescent substance use was largely unchanged.22,23 One independent systematic review found that youth substance use largely decreased during the pandemic, with alcohol and cannabis remaining the most common substances. 24 A study examining clinical CA patients presenting for emergency psychiatric evaluation found that substance use increased during the initial months of the pandemic, though longitudinal data were not available. 25 Overall, limited data exist thus far on the impact of the pandemic on substance use among youth with acute psychiatric needs.
Given limited data on youth with acute psychiatric needs, the investigators sought to examine substance use in CA patients that were psychiatrically hospitalized. We aimed to determine if the COVID-19 pandemic led to an increased prevalence of positive urine drug screening (UDS) among the CA psychiatric population. The study also aimed to determine if certain sociodemographic or clinical factors increased the likelihood of having a positive UDS. Specific substances tested on routine UDS were examined, including cannabis, opiates, benzodiazepines, and stimulants. We sought to evaluate if any of these factors might independently predict substance use in this population, and, in addition, to examine outcomes, such as length of stay or need for emergency medications for agitation, in patients with positive UDS as compared to those without positive UDS. The study also aimed to compare previously reported substance use with current UDS results.
Methods
This retrospective study was approved by the Institutional Review Board at Icahn School of Medicine at Mount Sinai (STUDY-21-01676). The charts of all patients admitted to the CA inpatient psychiatry unit at a private psychiatric hospital in New York City between June 1, 2018 and November 30, 2021 were reviewed. For patients admitted multiple times during this period, only the chart of the first admission during the study period was reviewed. The patient population is a representative cross-section of New York City and the surrounding region. Variables of interest were extracted by the study team, including sociodemographic information, such as age, gender identity, and racial identity, as well as the history of involvement of a social services department such as child protective services or the administration for children’s services.
Clinical information, such as psychiatric diagnoses, history of substance use, UDS results, and length of hospitalization were also collected. Psychiatric diagnoses were grouped according to the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) classification, and included Mood Disorders (depressive disorders and bipolar spectrum disorders), Anxiety Disorders (generalized anxiety disorder, panic disorder, etc.), Psychotic Disorders (schizophrenia-spectrum illnesses), Impulsive or Behavioral Disorders (intermittent explosive disorder [IED], oppositional defiant disorder [ODD], conduct disorder), ADHD, and Developmental Disorder/Intellectual Disabilities (autism, cerebral palsy, severe learning disabilities, etc.). 26 Prior history of substance use was defined as either being self-reported problematic use or having a documented SUD. Substance use/misuse are defined separately from a SUD, with a disorder generally considered to occur when the use/misuse of a substance causes clinically significant impairment, such as health problems, injury, or failure to meet responsibilities at school or at home. For the purpose of this study, a diagnosis of a SUD was not determined based on UDS results, given that the degree of impairment was not defined.
This study specifically examined patients with positive UDS results upon admission or taken shortly thereafter, as this was thought to be the best indicator of active substance use. Patients with positive UDS results due to prescribed medications (eg, stimulants, benzodiazepines) or medications that were administered in the emergency department were not considered as positive. Substances that are tested for on routine UDS include: amphetamines, cocaine, opiates, phencyclidine (PCP), methadone, methadone metabolites, benzodiazepines, barbiturates, cannabinoids, fentanyl, tramadol, oxycodone, buprenorphine, and 6-acetylmorphine. UDS results were grouped by class of substance (cannabis, opioids, benzodiazepines, or stimulants), in addition to an “Other” group, which included PCP and barbiturates. As patients hospitalized in our unit are sometimes referred from outside facilities, the exact substances tested on each UDS may have varied slightly; however, the aforementioned substance groupings were consistently tested for.
To examine the effects of the COVID-19 pandemic, the investigators divided the above timeframe into 3 main periods based on pandemic data from New York City. June 1, 2018 through March 16, 2020 was classified as “pre-quarantine,” as this was the date when local schools were closed due to the pandemic. March 17, 2020 through March 22, 2021 was classified as “quarantine,” as March 22 was the date when public high schools were reopened. Everything after March 22, 2021 until November 30, 2021 was classified as “post-quarantine.” Policies regarding UDS prior/upon admission to the inpatient unit did not change throughout COVID-19.
Data were extracted by the study team (SL, PShanker, TB, DM, PStaudenmaier, AL). Interrater reliability on the coding of the aforementioned variables in a subset of charts was high, over 95%. The coding team met regularly during data extraction and any chart for which there was disagreement or confusion was reviewed by the entire study team for consensus. Statistical calculations to examine the collected variables were conducted with IBM SPSS software Version 29.0. 27 These included descriptive statistics to characterize the sample (frequency, mean, standard deviation); chi-square test for comparisons of categorical variables (such as gender, race, diagnoses); and independent t-tests and analysis of covariance for group comparisons on continuous variables (such as age, length of stay, and number of prior hospitalizations). Effect sizes were calculated for statistically significant results using Cohen’s d statistic for variables compared with t-tests (d), Omega squared statistic for variables compared with analysis of variance (Ω 2 ), and Cramer’s V statistic for variables compared with chi-squared tests (φc). A logistic regression model was developed to identify independent clinical and sociodemographic predictors of positive UDS results in the study population. Backward elimination was used in the regression model to control for confounding variables.
Results
Sample Characteristics
Of the 1101 charts that were reviewed, 816 had documented UDS results: 147 (18.0%) were positive and 669 were negative. Throughout the study period, the percentage of admissions of patients with positive UDS results remained relatively constant (Figure 1). The timeline of the COVID-19 pandemic was not found to correlate to positive results (Table 1).
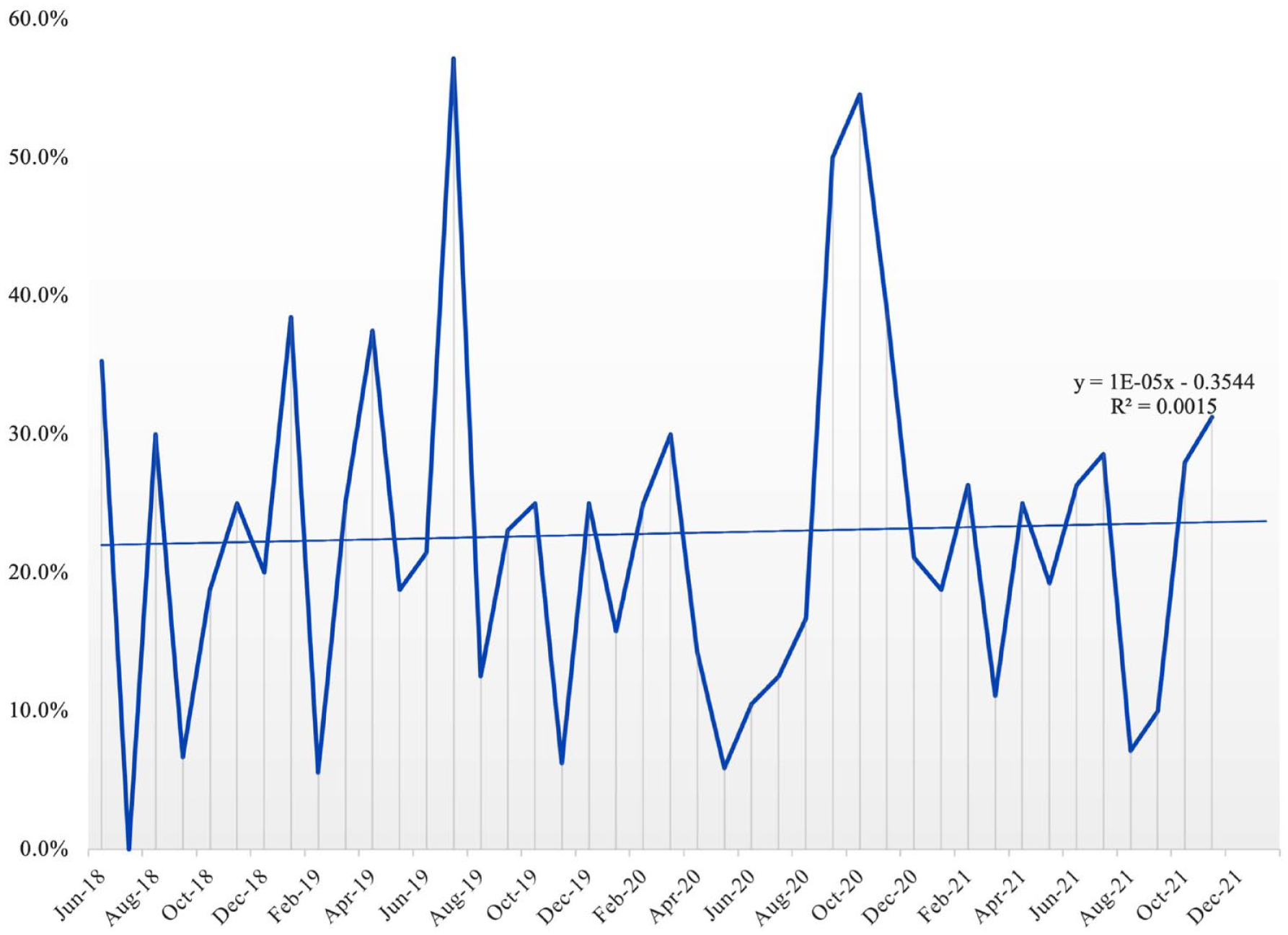
Figure depicting the percentage of admissions with positive UDS over the study time period, showing an overall constant rate of slightly greater than 20%.
Sociodemographic and Psychiatric Factors of Study Sample.
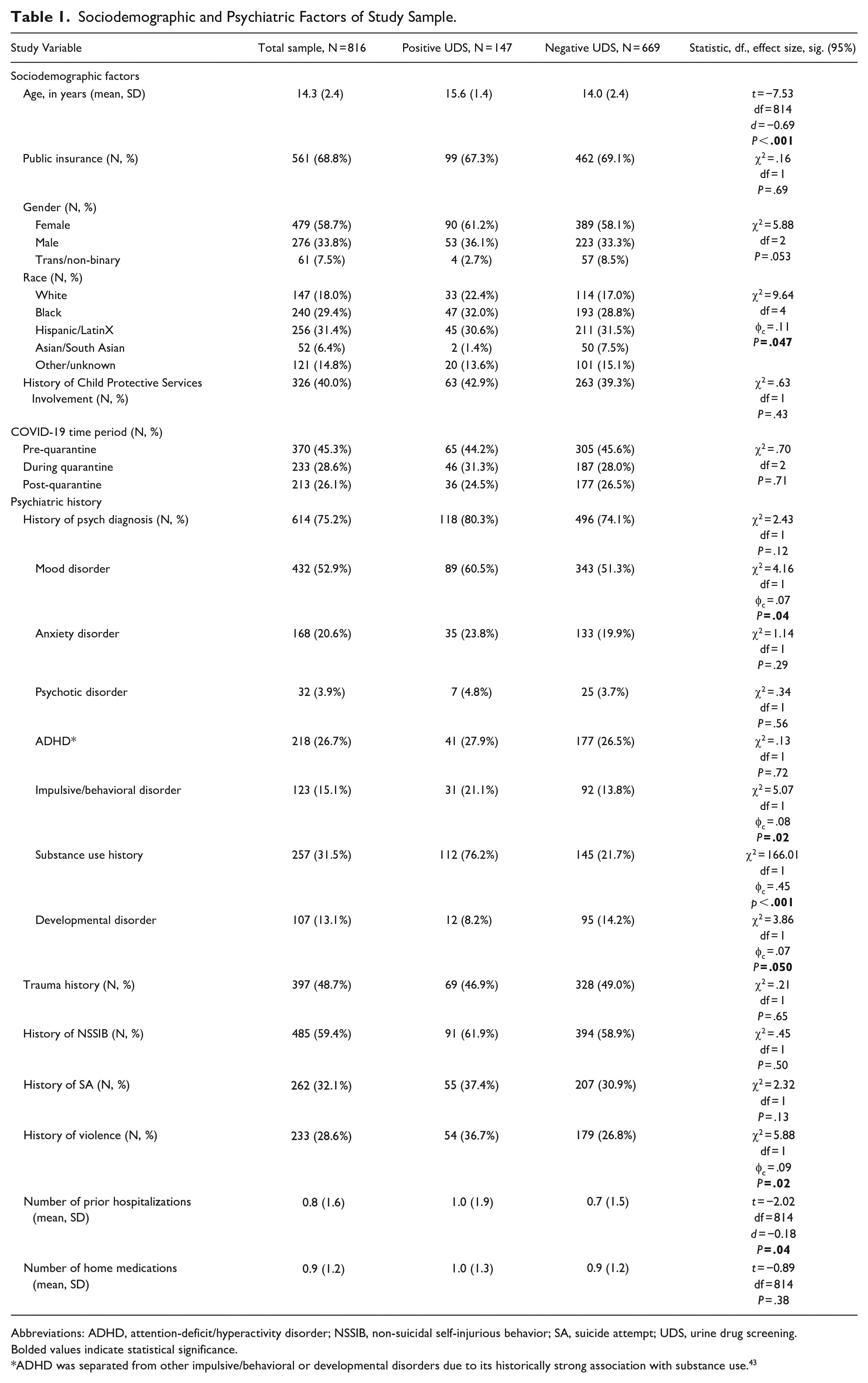
Abbreviations: ADHD, attention-deficit/hyperactivity disorder; NSSIB, non-suicidal self-injurious behavior; SA, suicide attempt; UDS, urine drug screening.
Bolded values indicate statistical significance.
ADHD was separated from other impulsive/behavioral or developmental disorders due to its historically strong association with substance use. 43
The overall sample was about 14 years old, predominately female, non-White, and with public health insurance (Table 1). Three quarters of the sample had a history of psychiatric diagnosis, most commonly a mood disorder (over 50%). Slightly under one-third of the sample had a reported history of substance use. About half of the sample disclosed a history of sexual, physical, or emotional trauma. Suicidal behavior was high in this sample, with over half of the sample having a history of non-suicidal self-injurious behavior (NSSIB), and about a third having a history of a suicide attempt (SA) prior to admission. The most common reason for admission in this sample was for suicidal ideation, followed by SA (Table 2). Patients were hospitalized on average for about 10 days, and around 17% required emergency use of medications for agitation while hospitalized (Table 2).
Admission and Discharge Information From Study Sample.
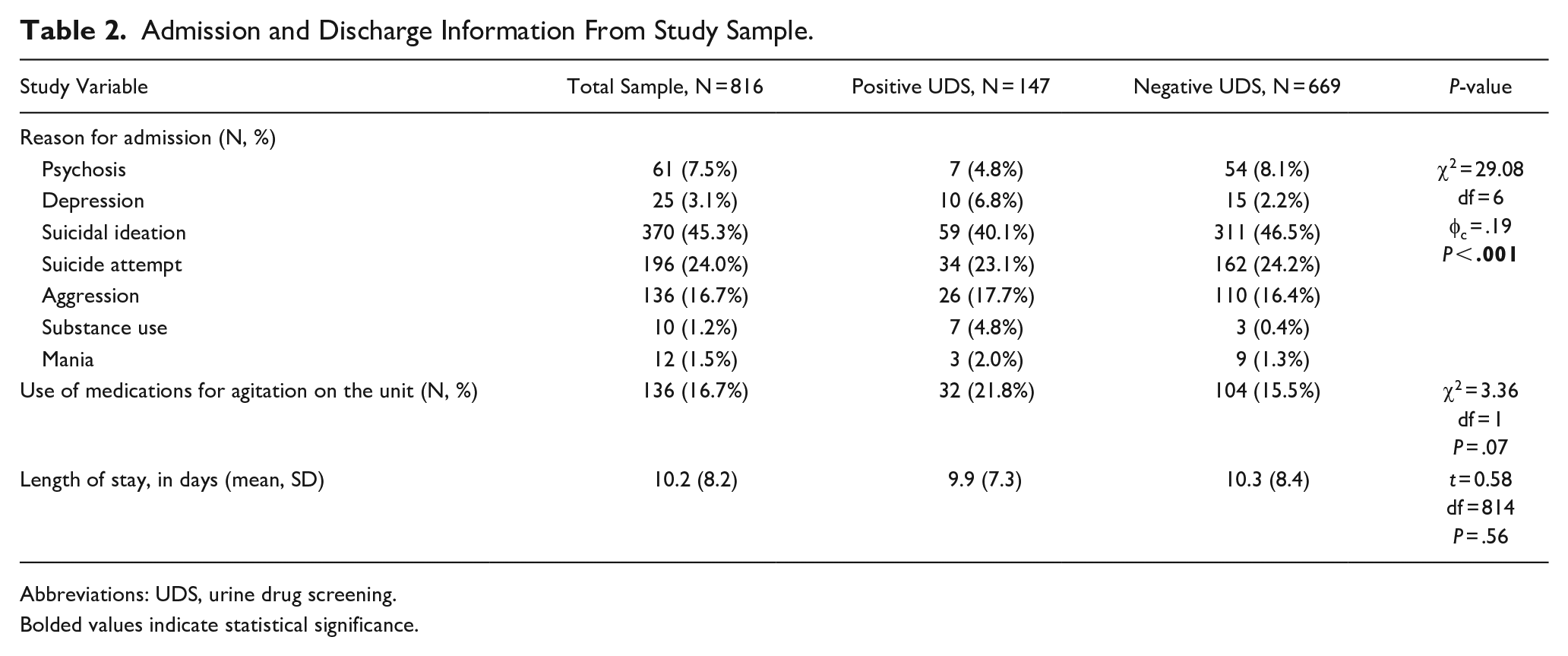
Abbreviations: UDS, urine drug screening.
Bolded values indicate statistical significance.
Sociodemographic Differences Between Groups
Patients with positive UDS were on average older by about a year and a half (Table 1). Significant racial differences were found, with Asian/South Asian participants being less likely to have a positive UDS (Table 1). Of all White patients, 22% had a positive UDS, the highest of all racial groups in this analysis (compared to 20% of Black patients, 18% of Hispanic/LatinX patients, and 4% of Asian/South Asian patients). Patients who identified as transgender or non-binary appeared less likely to have positive results than cisgendered patients, though this did not reach statistical significance (P = .053; Table 1).
Clinical Differences Between Groups
Patients with positive UDS were no more likely than those without to have a history of a psychiatric diagnosis prior to admission (Table 1). However, they were more likely to have a previously diagnosed mood or impulsive/behavioral disorder, and less likely to have a history of developmental disorder. Patients with positive results were more likely to have a history of violence as well as a greater number of prior psychiatric hospitalizations (Table 1). There were no significant differences between groups in prior SAs or history of NSSIB. About 3 quarters of patients with a positive UDS had prior substance use history, as compared to about 1 quarter of patients with a negative UDS (Table 1). Patients with positive results were more likely to be admitted for depression, or, unsurprisingly, for a substance-related reason. There were no significant differences in terms of length of stay or use of as-needed medications for agitation on the unit (Table 1).
A logistic regression model was created to identify predictors of having a true positive UDS report (Table 3). The previously discussed variables that were statistically significant (age, race, violence history, number of prior hospitalizations, and specific diagnoses) using comparative statistics were entered into the model. Two of the 7 variables were found not to be significant and removed by backward elimination. The model for the remaining predictors was significant (−2Log Likelihood = 614.31, χ2 = 128.37, df = 10, P < .001). Positive predictors in this model of positive UDS included older age (odds ratio [OR] = 1.69, 95% CI [1.49, 1.93], P < .001), history of impulsive or behavioral disorder (OR = 2.18, 95% CI [1.22, 3.91], P = .01), and history of violence (OR = 2.32, 95% CI [1.42, 3.79], P < .001). Negative predictors included being Hispanic/LatinX (OR = 0.52, 95% CI [0.30, 0.91], P = .02), being Asian/South Asian (OR = 0.08, 95% CI [0.02, 0.37], P < .01), having “Other” race (OR = 0.45, 95% CI [0.23, 0.89], P = .02), and history of a developmental or intellectual disability (OR = 0.32, 95% CI [0.16, 0.66], P < .01; Table 3).
Logistic Regression Predicting Positive UDS.
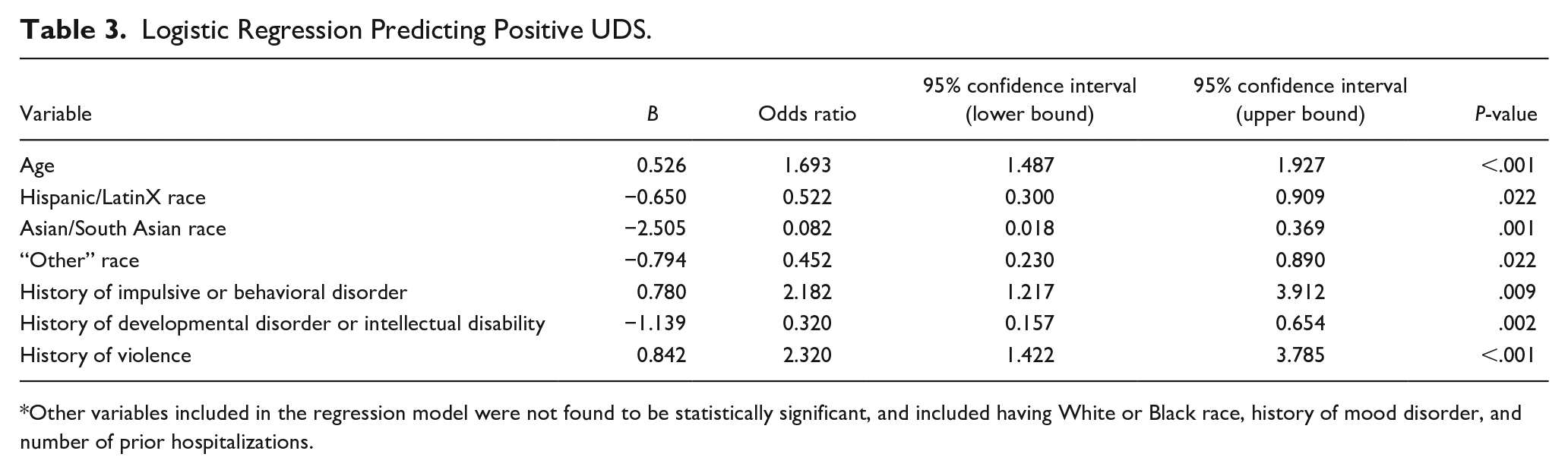
Other variables included in the regression model were not found to be statistically significant, and included having White or Black race, history of mood disorder, and number of prior hospitalizations.
Specific Substances
Of patients with positive UDS, 84.4% tested positive for cannabis, 3.4% for opioids, 12.2% for benzodiazepines, 7.5% for stimulants, and 7.5% for “other” substances. Males were more likely than females or transgender/non-binary people to test positive for cannabis (94.3% vs 80.0% and 50.0%, respectively, χ2 = 8.87, df = 2, φc = .25, P = .01). Trans/non-binary people were more likely to test positive for “other” substances than males or females (50% vs 1.9% and 8.9%, respectively, χ2 = 13.0, df = 2, φc = .30, P < .01). No other differences were found in terms of individual classes of substances. Due to the logistic regression findings, these were separated by racial group; however, there were no significant findings, with the predominant substance among all races being cannabis (>80% of all cases; Figure 2).
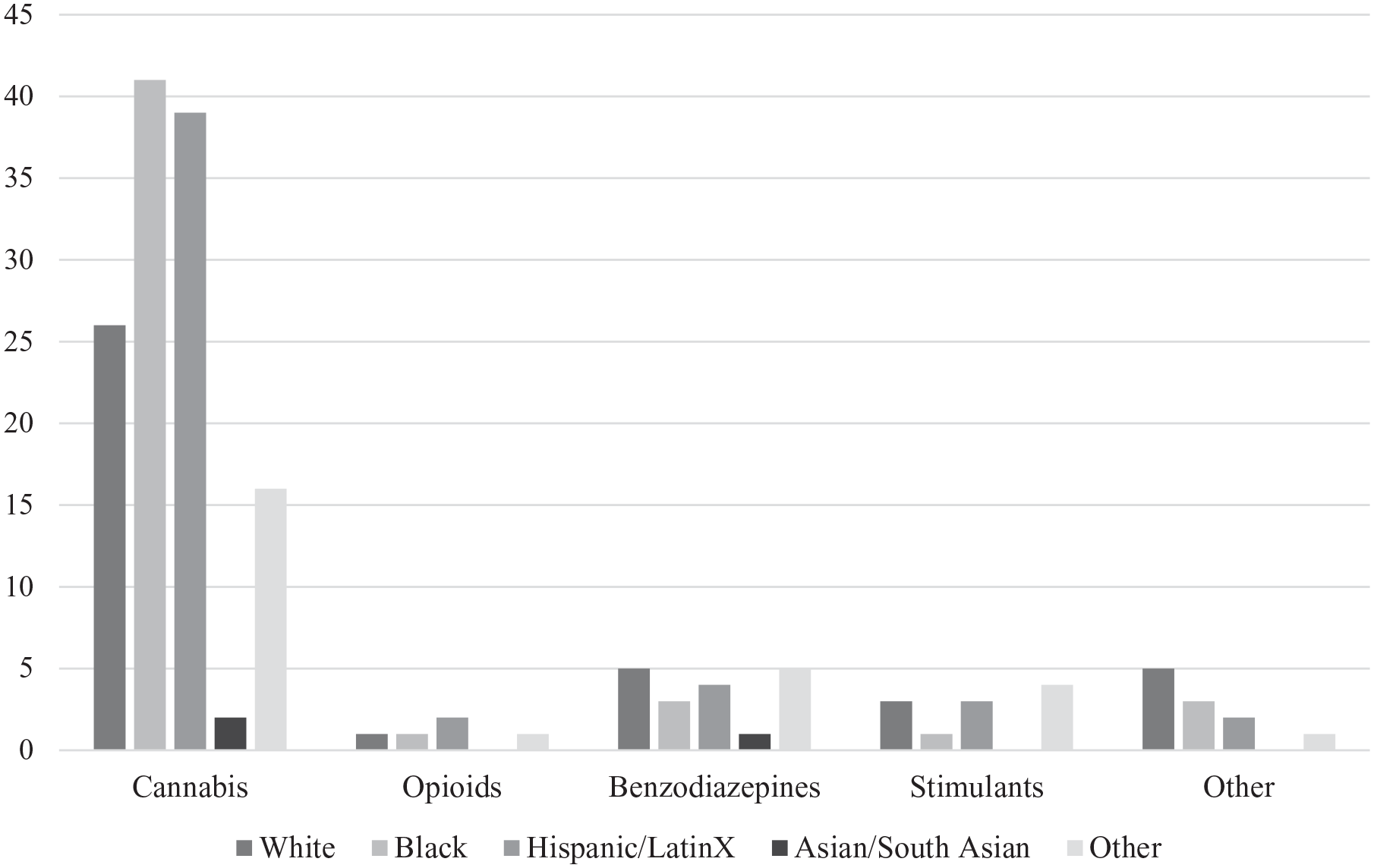
Figure depicting the number of admitted patients with positive UDS for each class of substance, separated by patients’ racial/ethnic identities.
Discussion
Impact of the COVID-19 Pandemic
As shown in Figure 1, there was a relatively constant proportion of admissions with positive UDS over the study period. Of the included patients, 18% had a positive UDS result, and 31.5% had prior substance use based on self-report and/or chart review. This is consistent with prior reports, which have shown that overall rates of substance use in the CA population have remained relatively stable; however, unlike other reports, we did not observe an increase in the frequency of UDS which were positive for cannabis. 28 In contrast to the findings of Dumas and in accordance with subsequent reports, no significant change occurred throughout various phases of the COVID-19.22,24
Sociodemographic Findings
Participants with positive UDS were on average older than those without by approximately 2 years. This is consistent with prior reports that older adolescents use substances at a higher rate. 29 One study found that for every year between the ages of 13 and 21 years that an adolescent does not use substances, the lifetime likelihood of developing a SUD decreases 4% to 5%. 30 Adolescents demonstrate increases in risk-taking and novelty-seeking behaviors as they progress through development, likely related with hormonal changes and alterations in reward circuitry. 31 Based on our regression model, every year increase in age significantly increased the odds of having a positive UDS (OR = 1.69, 95% CI [1.49, 1.93], P < .001; Table 3).
Race was found to correlate with UDS results, with Asian/South Asian patients making up a smaller percentage of those with a positive UDS. This finding carried over into the regression analysis, which found having either Asian/South Asian or Hispanic/LatinX race decreased the odds of having positive UDS. This is somewhat consistent with prior findings, which have historically shown that Asian patients have lower lifetime and recent substance use than other races. 32 Prior studies examining Hispanic/LatinX, White, and Black patients have been inconsistent, with some indicating that Hispanic/LatinX patients use substances at an increased rate compared to White or Black patients, which was not the case in our study.32,33 Our study may be unique in that our patient population is derived from the urban New York City setting, which affords us rich cultural diversity for analysis. Though differences in frequency of positive UDS differed between groups, there were no differences in terms of which substances resulted as positive.
Psychiatric and Clinical Findings
We found that patients with positive UDS were more likely to have a history of mood disorder. Literature has consistently demonstrated that depression and substance use are intertwined. Up to 35% of adolescents with a depressive disorder develop a co-occurring SUD, and prior reports have shown that the severity of depressive symptoms positively correlates with substance use.34,35 Also included in the category of mood disorders for this study are bipolar spectrum disorders, which can elevate the risk of substance use, particularly during manic episodes, so this is consistent with prior literature. 36 Additionally, it is suggested that adolescent-onset (age 13 and above) bipolar disorder is associated with a higher risk of substance use compared to child-onset bipolar disorder, potentially due to a desire for mood-altering effect. 36
In this study, we did not find any significant association between positive UDS and anxiety disorders. The relationship between anxiety disorders and substance use may vary by specific disorder, and findings have been overall inconclusive. 37 Some studies have found that generalized anxiety disorder and panic disorder are associated with substance use, with the relationship being stronger in boys than in girls, and somewhat variable based on race/ethnicity. 38
In this population, individuals with an impulsive or behavioral disorder, such as IED or ODD, were more likely to have a positive UDS. The regression analysis suggested that having a history of this type of disorder may increase the odds of a positive result by twofold. Prior studies have found that patients with ODD have a high risk (almost 50%) of developing SUD. 39 Potentially, a low sensitivity to punishment and a hyposensitivity to reward may predispose these patients to “sensation-seeking behavior,” in addition to impairments in executive functions limiting control over emotional behavior. 40 Similar findings exist related to IED which found that lifetime SUDs were significantly more common in patients with IED, and that IED preceded a SUD in over 80% of cases where substance use occurred, suggesting that IED itself is a risk factor for substance use. 41
Our study found no relationship between UDS results and ADHD, which is somewhat unexpected given that ADHD has historically been strongly associated with substance use. Studies suggest that not only is substance use more prevalent in patients with ADHD, but these patients also tend to have a younger first use of substances with a faster progression. 42 Because of this known association, ADHD was separated from other impulsive/behavioral or developmental disorders. We found in our sample that patients with a history of ADHD were on average significantly younger than those without (13.4 years vs 14.6 years of age, respectively), which may explain a lack of significant findings.
In our sample, there were fewer positive UDS results among patients with a developmental disorder or intellectual disability, with the regression model showing a significant decrease in likelihood. This is inconsistent with recent literature in the adult population, which has found that people with mild-to-borderline intellectual disabilities are at a higher risk of developing a SUD. 43 Our findings may differ from prior literature given that we combined those with intellectual disabilities with patients that had severe learning disabilities, cerebral palsy, or those that meet criteria for level 3 autism spectrum disorder in the DSM-5. 26 Additionally, in our sample, patients with a history of developmental/intellectual disability were on average younger than those without, so this finding may be partially due to age.
Our data did not find that patients with a history of trauma were more likely to use substances. This finding was surprising, as prior literature has demonstrated that children who experience trauma or maltreatment are at an elevated risk for developing problematic substance use, in addition to potential earlier onset of use. 12 Trauma has also been shown to increase the risk for tobacco, alcohol, and other illicit substance use, and adolescent girls with a history of sexual abuse are approximately 5 times more likely to have problematic use of multiple substances.12,32 However, information related to trauma history may not have been accurately captured on admission.
Patients with a positive UDS had a higher incidence of a history of violence in this sample, with the regression model showing that a history of violence more than doubled the odds of having a positive result. This is consistent with prior studies, where history of violence increased the risk of substance use by 2-3×. 44
About a third of included patients had documented prior substance use, consistent with prior studies. 10 Patients who had positive UDS results were significantly more likely to have either reported problematic substance use to providers, or to have a SUD documented in their chart. This suggests that the majority of patients who presented and had a positive UDS had previously experimented with substances. Of the patients who had a positive UDS, 35 (23.8%) did not report/denied any history of substance use, likely reflective of some hesitance to disclose their use to providers.
In this sample, there were no differences between groups in terms of length of admission or in the use of emergency medications for agitation. This was somewhat surprising, given the above results that history of violence and substance use may be closely connected. Potentially, abstaining from substance use on the unit and/or receiving psychiatric care mitigated the risk for aggression. Many providers may be wary of admitting adolescents with co-occurring SUDs due to the fear of disruptive or agitated behavior while admitted, however, these results suggest similar outcomes with no greater concerns for safety on the inpatient units.
Limitations
This study was not without limitations. Our analyses completely relied upon the review of electronic medical records, which may have had conflicting or inaccurate data. When extracting data from the charts, the investigators primarily relied on admission and discharge notes, which may have prevented the discovery of a substance-related issue at another point during the admission. There were 1101 charts that were reviewed for this study, however only 816 had information about UDS results. This may introduce bias, as patients who were unwilling to provide urine samples may be more likely to have substance-related issues, which would not have been analyzed in this study. However, as one of the only few child/adolescent psychiatric inpatient units with a large catchment area, many patients’ UDS may have been obtained from referring emergency departments and not imported into their hospitalization records. Additionally, patients who had no UDS data were younger, with 33.2% of patients with no UDS being under the age of 12 years compared to 16.9% of patients with UDS data being under the age of 12 years. This may reflect clinician bias that there is less need to obtain a UDS from younger patients.
As previously discussed, alcohol and nicotine are 2 frequently misused substances in the youth population, however these substances are not measured in routine UDS and therefore data related to these substances were not available for analysis. Additionally, while the study sample was overall large, the number of patients with a positive UDS was smaller, and several of the subgroups analyzed were particularly small, such as patients of Asian/South Asian descent. This study involved a significant number of statistical tests, which increases the risk of type I error. Strengths of the study include an overall large and diverse sample size, allowing generalizability to other clinical populations, as well as the collection of detailed sociodemographic and clinical information.
Conclusion
Multiple sociodemographic and psychiatric factors may predispose CA patients to substance use, which can have long-term negative, medical, and psychiatric effects. This study, despite some limitations, is unique in that it compares UDS results to previously reported substance use as well as examines the impact of COVID-19 on substance use among youths in the inpatient psychiatric setting. While our analyses found no impact of the COVID-19 pandemic on UDS results among inpatients, further and more long-term studies are needed. It is crucial to identify and address substance use in the CA population, to prevent future SUDs, improve mental health and psychiatric stability, and to minimize negative structural effects on the brain from substance use.
Footnotes
Author Contributions
S.L. and P.Sh were involved in planning the work. T.R was involved in supervising the work. S.L., D.M., T.B., P.Sh, P.St., and A.L. collected the data. S.L. performed the statistical analyses and designed the figures and tables. S.L. wrote the initial draft of the manuscript. All authors subsequently revised the manuscript, discussed the results, and agreed on the content prior to submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance,Ethical Standards,and Ethical Approval
This study was approved by the Institutional Review Board at Icahn School of Medicine at Mount Sinai (STUDY-21-01676).