
Abstract
Background:
Injection drug use (IDU) is a risk factor for hepatitis C virus (HCV) acquisition and occurs disproportionately among women who exchange sex (WES). However, little is known about HCV epidemiology in this population. We estimated HCV seroprevalence, identified correlates of HCV seropositivity, and characterized social networks by HCV serostatus and IDU history among WES in the Seattle, Washington, area.
Methods:
This was a secondary analysis of data from the 2016 National HIV Behavioral Surveillance survey in the Seattle, Washington area, a cross-sectional survey that used respondent-driven sampling (RDS) to enroll WES for money or drugs (N = 291). All participants were offered rapid HCV-antibody testing. We estimated HCV seropositivity and used log regression methods to estimate crude and adjusted prevalence ratios (PRs) for correlates of HCV seropositivity among WES. Using RDS recruitment chain data, we computed homophily indices to estimate the extent to which participants were likely to recruit another participant with the same HCV serostatus and IDU history.
Results:
In the study sample of WES in the Seattle, Washington area, 79% reported lifetime IDU and 60% were HCV seropositive. HCV seropositivity was strongly associated with ever injecting drugs (PRadj: 7.7 [3.3, 18.0]). The RDS homophily scores for HCV seropositivity (0.07) and ever injecting drugs (0.02) suggested that participants did not tend to recruit others with the same characteristics beyond what would be expected by chance.
Conclusion:
Among this sample of WES in Seattle, Washington area, HCV seroprevalence was high and strongly associated with a history of IDU. The high burden of HCV among WES suggests this marginalized group would benefit from additional harm reduction services and targeted HCV treatment campaigns to reduce forward transmission. We saw little evidence of preferential recruitment among WES who were HCV seropositive or reported a history of IDU, suggesting the potential futility of peer-based referrals for HCV treatment.
Introduction
Injection drug use (IDU) is common among women who exchange sex (WES) globally.1 –4 Research in Russia found that 22% of WES report lifetime IDU, 3 while more recent research in Iran 4 and Kenya 1 found that over 47% and 70% prevalence of lifetime use, respectively. Studies from international settings have also documented that sex exchange is associated with hepatitis C virus (HCV) acquisition,5 –7 likely driven by high rates of co-occurring IDU. However, sexual exposure facilitated by the presence of sexually transmitted infections and multiple sexual partners, as well as non-injection drug-related risks, also contributes to HCV risk.5 –7 Among people who inject drugs (PWID), women are more likely than men to engage in risky injection behaviors such as sharing injection equipment and having drugs prepared by another person,8,9 and are less likely to be treated for HCV. 10 Such findings, taken with multiple recent HIV outbreaks among PWID in the United States,11 –15 highlight the vulnerability of WES who inject drugs to bloodborne pathogens, including HCV. While there is recent work on the epidemiology of HCV among LGBTQ+ populations in the United States (eg, those that share an increased risk of bloodborne pathogens),16,17 we know of no such work focusing on WES. Most research on the epidemiology of HCV among WES has been conducted among populations outside of the United States.
Direct-acting antivirals (DAAs) have revolutionized the HCV landscape, allowing for shorter, safer, and more effective treatment than interferon therapy.18 –20 DAAs not only provide an opportunity to durably cure HCV but also prevent transmission among WES and other groups at risk through a treatment as prevention approach.21,22 To ensure that HCV treatment and prevention strategies are successful among WES in the United States, additional work is needed to better understand the interplay between IDU, sex exchange, and HCV risk, as well as strategies for linkage to care in this population.5,6,23 Previous studies among PWID have found peer referral to be an effective means of linking PWID with HCV care,24,25 but most of this research has been conducted outside of the United States, and to our knowledge, none has focused on WES.
To address these knowledge gaps, we used data from a cross-sectional survey of WES in the Seattle, Washington area to (1) estimate the prevalence of HCV seropositivity, (2) identify correlates of HCV seropositivity, and (3) characterize social networks among WES by analyzing participant recruitment trees and measuring whether and to what extent individuals were likely to recruit others with the same HCV serostatus or IDU history.
Methods
Study Sample
The present study used cross-sectional data from the 2016 National HIV Behavioral Surveillance (NHBS) survey in the Seattle area conducted by Public Health—Seattle & King County (PHSKC). The survey was conducted during the NHBS-HET cycle, which focuses on low-income people at higher risk for HIV through heterosexual sex. In 2016, 5 NHBS sites (including Seattle) were selected to participate in a demonstration project that focused on WES. The survey eligibility criteria were similar to the parent NHBS-HET survey but differed in 2 ways: low-income status was not an eligibility criterion and only cisgender women were eligible. Specifically, potential participants were eligible if they (1) had a valid survey coupon, (2) had not already participated in the 2016 NHBS survey, (3) lived in King County, Washington or Snohomish County, Washington, (4) were 18 to 60 years old at the time of their study visit, (5) reported having vaginal or anal sex with a person of the opposite sex in the past 12 months, (6) were cisgender women, and (7) were able to complete the NHBS survey in English or Spanish. Women who did not report exchanging sex for money or drugs were eligible for the survey. However, we only included the subset of women who reported exchanging sex in this analysis.
Between June and December 2016, staff interviewed participants at a field site located close to downtown Seattle, Washington and at a homeless service center in North Seattle. Project leadership suspended the latter site after a short time due to limited recruitment success. PHSKC staff recruited participants using respondent-driven sampling (RDS), 26 a recruitment method designed to study small, marginalized populations. In accordance with RDS methods, 26 project staff selected initial “seed” participants. Eligible participants received $50 for completing the survey and having a rapid HIV test, plus $10 for each additional participant they referred (adjusted to $20 midway through the recruitment process). To focus recruitment on WES, respondents who completed the survey and reported exchanging sex for money or drugs could recruit up to 5 other individuals. Participants were linked to their recruiter by a unique identifier associated with the recruitment coupon. Participants who did not report exchanging sex in the last 12 months could complete the survey and receive testing but could not recruit other participants.
Data Collection
After obtaining informed consent, PHSKC staff conducted face-to-face structured surveys with participants using portable computers. Project coordinators trained staff to administer surveys in a standardized manner, and question logic was applied automatically by the survey computer interface. Staff members administered both Core and Local surveys. The Core survey was common to all NHBS sites and consisted of demographic, behavioral, and health questions. The Local survey was administered after completion of the Core survey and addressed partner violence, sexual practices, condom use, intentions to get pregnant, and interactions with local service agencies. Core and Local survey questions used for the present study are detailed in the “Measures” subsection. Staff offered OraQuick® (OraSure Technologies, Inc., Bethlehem, PA, USA) rapid HIV and HCV testing upon completing surveys and uploaded test results to a secure data transfer portal. Interview staff collected dried blood spot specimens from participants with positive rapid HIV tests for confirmatory Western Blot testing at a partner laboratory. At the time of testing, participants received pre- and post-test counseling, with referrals as needed. Including the interview and optional testing, visits lasted 60 to 90 minutes.
Measures
Reported sex exchange in the last 12 months was determined in the Core NHBS survey with the question, “in the past 12 months, did [a casual sex partner] give you money or drugs to have sex with him?” Participants who did not report ≥1 casual sex exchange partner in the Core survey were asked in the Local survey, “in the past 12 months, did one or more men give you money or drugs to have vaginal, oral or anal sex with them?” Participants who answered “yes” to either question were included in the present analysis.
The primary outcome of interest was HCV seropositivity, measured by rapid HCV-antibody test result. Study staff also collected survey data on history of HCV infection (i.e., “Has a doctor, nurse or other healthcare provider ever told you that you had hepatitis C?”) and treatment (i.e., “Have you ever taken medicine to treat your hepatitis C infection?”).
The NHBS Core and Local surveys included measures of several exposures of interest. We organized these into demographic, behavioral, health, and experiential characteristics (Supplemental Table S1). Unless otherwise noted, we treated exposure variables in analyses as they were collected by PHSKC staff (ie, analyses used data exactly as they were originally coded) and were specific to the 12-month period preceding a study visit.
Analysis
Our analytic sample included women who reported exchanging sex for money or drugs in the last 12 months, determined by the data collected in the Local NHBS survey. We conducted statistical analyses in the RStudio environment. 27 Using the EpiR package, 28 we estimated HCV seroprevalence among WES. We used bivariate log binomial regression models to estimate prevalence ratios (PRs) for HCV seropositivity comparing individuals by demographic, behavioral, health, and experiential characteristics previously described. These variables were selected from the available dataset because they aligned with Social Determinants of Health defined by the US Department of Health and Human Services 29 and/or were found to be potentially associated with HCV following a literature review.1 –6 We included correlates found to be significantly associated with HCV seropositivity in bivariate analyses (α ≤ .05) in a multivariate model to estimate adjusted PRs (PRadj), but omitted those that were either only available for participants who injected drugs or had >5% missingness. We planned to use log binomial regression for the multivariate model. However, this model did not converge, so we opted for Poisson regression, a method to estimate PRs that is appropriate in this case. 30 Using RDS Analysis Tool 31 we analyzed participant recruitment trees by calculating homophily indices. 32 Using RDS Analyst, 33 we visualized these recruitment trees.
RDS analytic methods can include an adjustment for the recruitment method, 34 an approach that is useful when attempting to generalize to the population of interest. However, based on the high frequency of reported histories of IDU in the sample, we determined that it was unlikely that the sample was representative of all WES in the Seattle area. Therefore, we analyzed the data as a convenience sample, as has been done previously. 10
Results
In total, 383 participants completed the 2016 NHBS Seattle, Washington area survey, 298 of whom were cisgender women and reported exchanging sex for money or drugs in the past 12 months. Of these 298 WES, 7 were excluded because they did not complete HCV serologic testing. This yielded an analytic sample of 291 WES. RDS referral began with 21 seeds, 8 of which resulted in at least 1 referral and were considered productive. Excluding the seed participants, among the productive seeds, the median number of participants in a referral chain was 9 (Interquartile range [IQR]: 7, 40). There were 16 waves of referral.
Most participants were White (65%), at least 40 years old (65%), and born in the United States (96%, Tables 1 and 2). Street-based sex exchange was the most common means of meeting clients (61%), followed by public places (51%), through a drug dealer or drug house (50%), and through family or friends (50%). Ten (3%) participants were living with HIV; 7 self-reported positive HIV status, and 3 had a new HIV diagnosis through NHBS. Challenging socioeconomic circumstances were common; half (50%) of participants were unstably housed or experiencing homelessness, 67% attained a high school degree/general education degree (GED) at most, and 79% reported an annual income of under $20 000.
Demographic Characteristics With Log Binomial Regression Prevalence Ratio Estimates for Hepatitis C Seropositivity Among Cisgender Women Who Exchange Sex, Seattle, Washington Area (National HIV Behavioral Surveillance, HET4, 2016) N = 291.
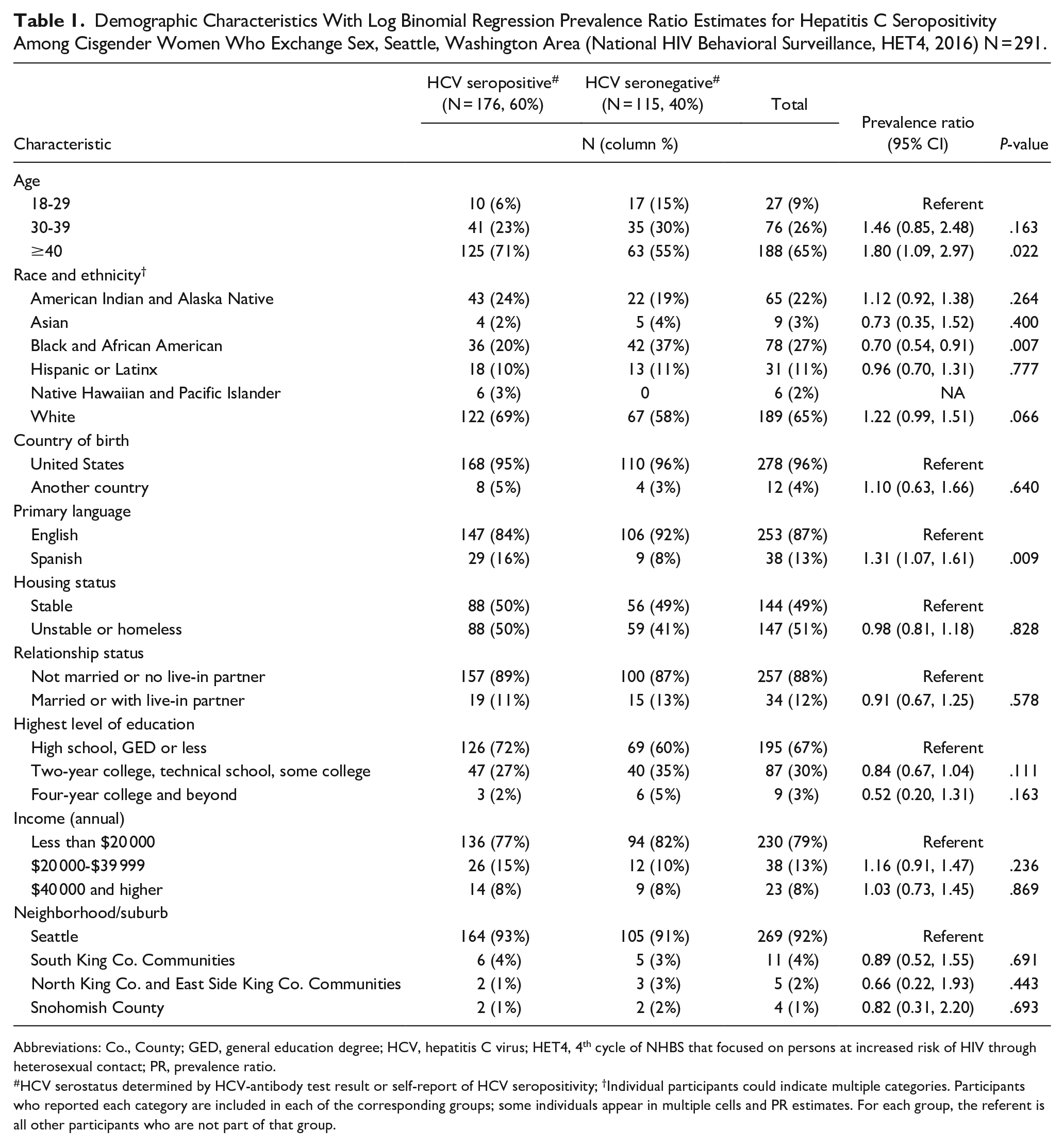
Abbreviations: Co., County; GED, general education degree; HCV, hepatitis C virus; HET4, 4th cycle of NHBS that focused on persons at increased risk of HIV through heterosexual contact; PR, prevalence ratio.
HCV serostatus determined by HCV-antibody test result or self-report of HCV seropositivity; †Individual participants could indicate multiple categories. Participants who reported each category are included in each of the corresponding groups; some individuals appear in multiple cells and PR estimates. For each group, the referent is all other participants who are not part of that group.
Substance Use, Sex Exchange, and Health Characteristics With Log Binomial Regression Prevalence Ratio Estimates for Hepatitis C Seropositivity Among Cisgender Women Who Exchange Sex, Seattle, Washington Area (National HIV Behavioral Surveillance, HET4, 2016) N = 291.
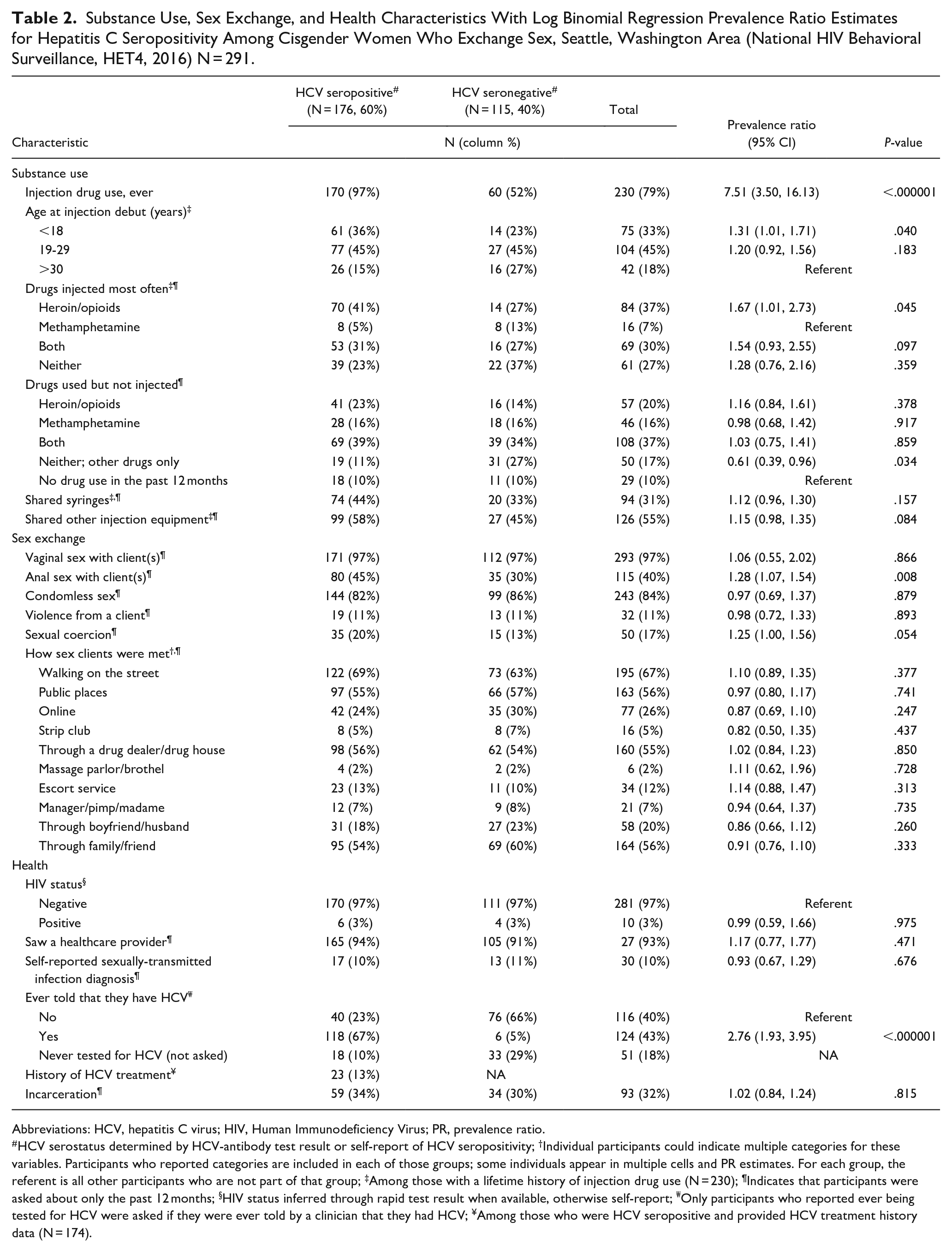
Abbreviations: HCV, hepatitis C virus; HIV, Human Immunodeficiency Virus; PR, prevalence ratio.
HCV serostatus determined by HCV-antibody test result or self-report of HCV seropositivity; †Individual participants could indicate multiple categories for these variables. Participants who reported categories are included in each of those groups; some individuals appear in multiple cells and PR estimates. For each group, the referent is all other participants who are not part of that group; ‡Among those with a lifetime history of injection drug use (N = 230); ¶Indicates that participants were asked about only the past 12 months; §HIV status inferred through rapid test result when available, otherwise self-report; ₩Only participants who reported ever being tested for HCV were asked if they were ever told by a clinician that they had HCV; ¥Among those who were HCV seropositive and provided HCV treatment history data (N = 174).
Most participants (79%) reported ever injecting drugs. Overall, 65% report injecting drugs in the past 12 months, among whom 57% reported that heroin/opioids were the primary drug they used. Of those who injected drugs, 60% reported sharing injection equipment of any kind in the past 12 months. A total of 32% of participants had been incarcerated in the past 12 months, 11% reported physical violence from a client, and 17% reported sexual coercion by any partner in the past 12 months. Healthcare use was high with 93% of participants reporting any healthcare provider visit in the past 12 months, including routine care, emergency department, or urgent care.
We estimated an overall HCV seroprevalence of 60% (95% CI: 55, 66) among WES in the Seattle, Washington area. HCV seroprevalence was 74% (95% CI: 68, 79) among those who reported ever injecting drugs and 10% (95% CI: 4, 20) among those who had never injected drugs. Among HCV-positive participants, only 13% reported prior HCV treatment.
In bivariate analyses, participants who were HCV seropositive were more likely than those who were HCV seronegative to report ever injecting drugs (PR: 7.51 [95% CI: 3.33, 16.96], Tables 1 and 2), to be at least 40 years old (PR: 1.80 [1.09, 2.97]), to speak primarily Spanish (PR: 1.31 [1.07, 1.61]), to report having anal sex with client(s) in the last 12 months (PR: 1.28 [1.07, 1.54]), to report meeting a client through an escort service in the last 12 months (PR: 1.25 [1.00, 1.55]), and to have ever been told by a clinician that they had HCV (PR: 2.76 [1.93, 3.95]). Those who were HCV seropositive were less likely to be Black or African American (PR: 0.70 [0.52, 0.91]).
Among participants who reported a history of IDU (N = 230), those who were HCV seropositive were more likely to start injecting before the age of 19 (PR: 1.31 [1.01, 1.71]). Using participants who indicated that methamphetamine was the most frequently injected drug as the referent, heroin as the most frequently injected drug was associated with higher HCV seroprevalence (PR: 1.67 [1.01, 2.73]). In the multivariate model, the only correlate that remained strongly associated with HCV seropositivity was history of IDU (PRadj: 7.66 [3.26, 18.01], Table 3).
Multivariate Poisson Regression Prevalence Ratio Estimates for Hepatitis C Seropositivity Among Cisgender Women Who Exchange Sex, Seattle, Washingtion Area (National HIV Behavioral Surveillance, HET4, 2016) N = 289. †
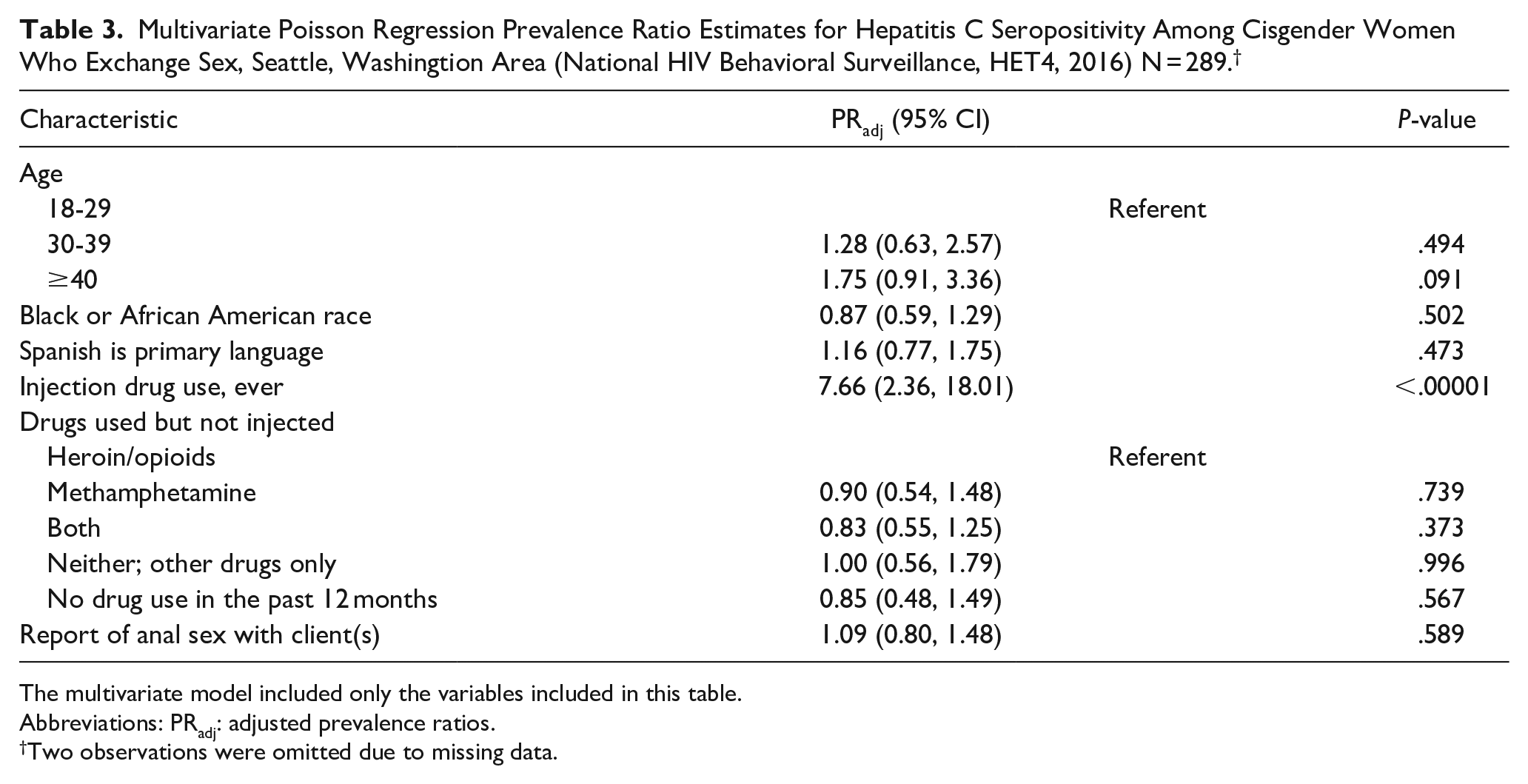
The multivariate model included only the variables included in this table.
Abbreviations: PRadj: adjusted prevalence ratios.
Two observations were omitted due to missing data.
We present recruitment trees of participants, color coded by their HCV status (Figure 1) and IDU history (Figure 2). The RDS homophily scores revealed that (1) participants who were HCV seropositive recruited other HCV-seropositive participants preferentially 7% of the time, (2) HCV-seronegative participants recruited other HCV-seronegative participants preferentially 24% of the time, (3) participants with a history of IDU recruited others with a history of IDU preferentially 3% of the time, and (4) participants with no reported history of IDU recruited others with no history of IDU, preferentially 26% of the time. Affiliation matrices and associated homophily indices are presented in Tables 4 and 5.
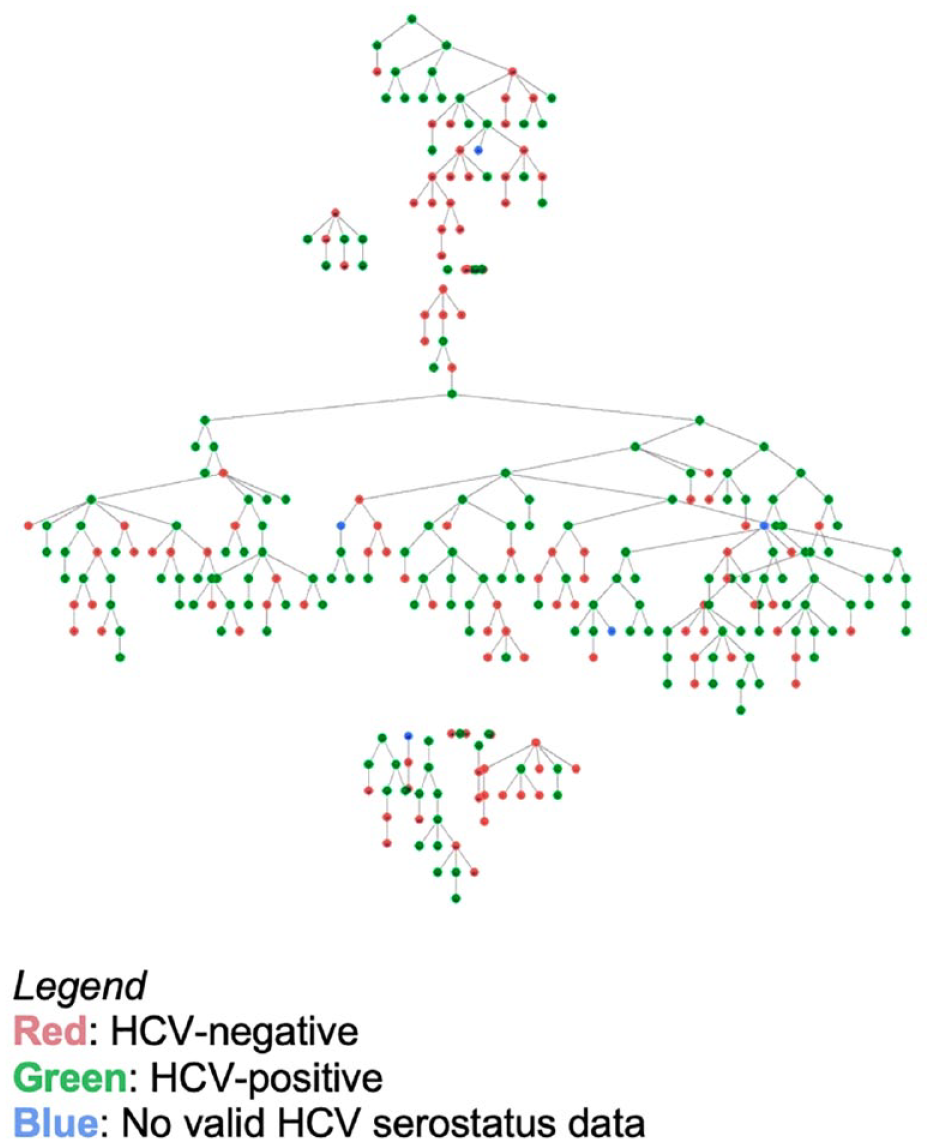
Recruitment tree of HCV status among women who exchange sex in Seattle, Washington (NHBS HET4, 2016).
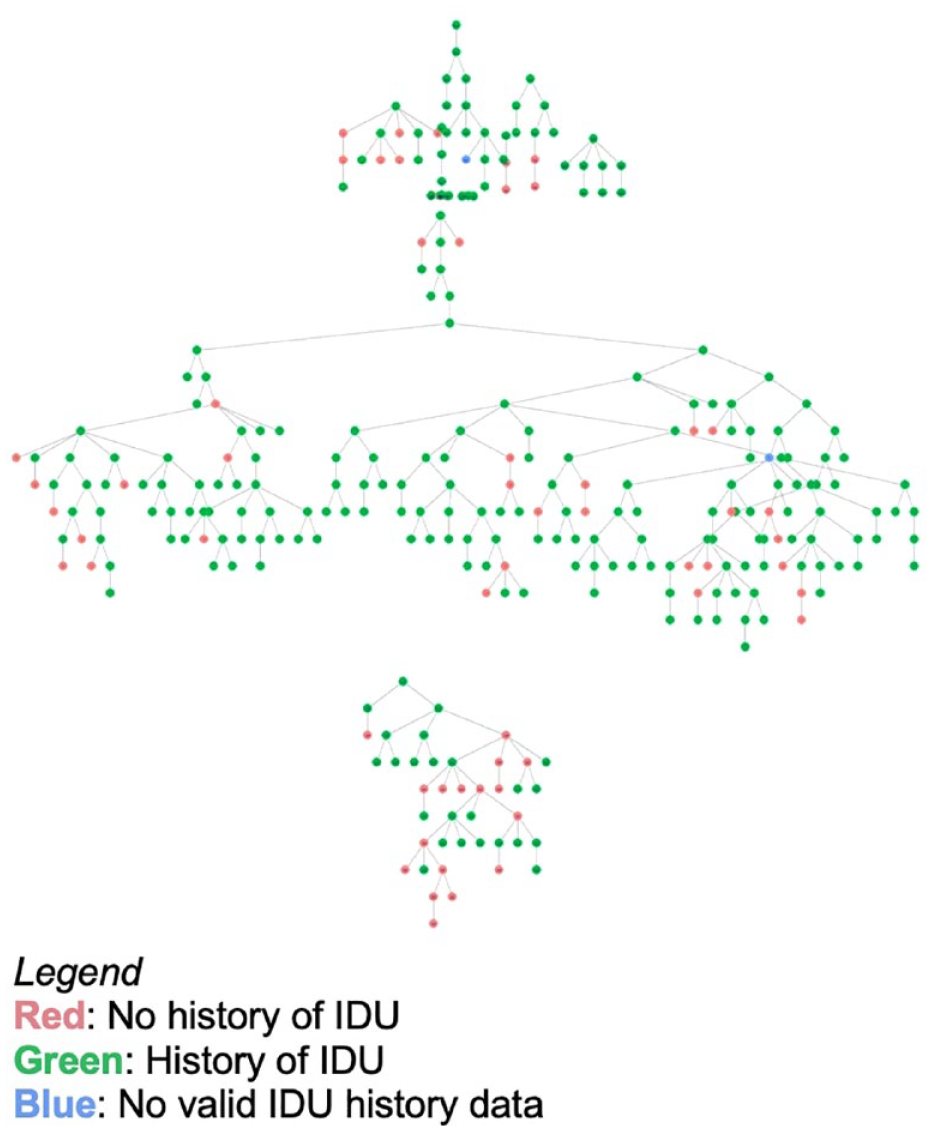
Recruitment tree of IDU history among women who exchange sex in Seattle, Washington (NHBS HET4, 2016).
Affiliation Matrix and Associated Homophily Scores for HCV Status Among Cisgender Women Who Exchange Sex, Seattle, Washington Area (National HIV Behavioral Surveillance, HET4, 2016).
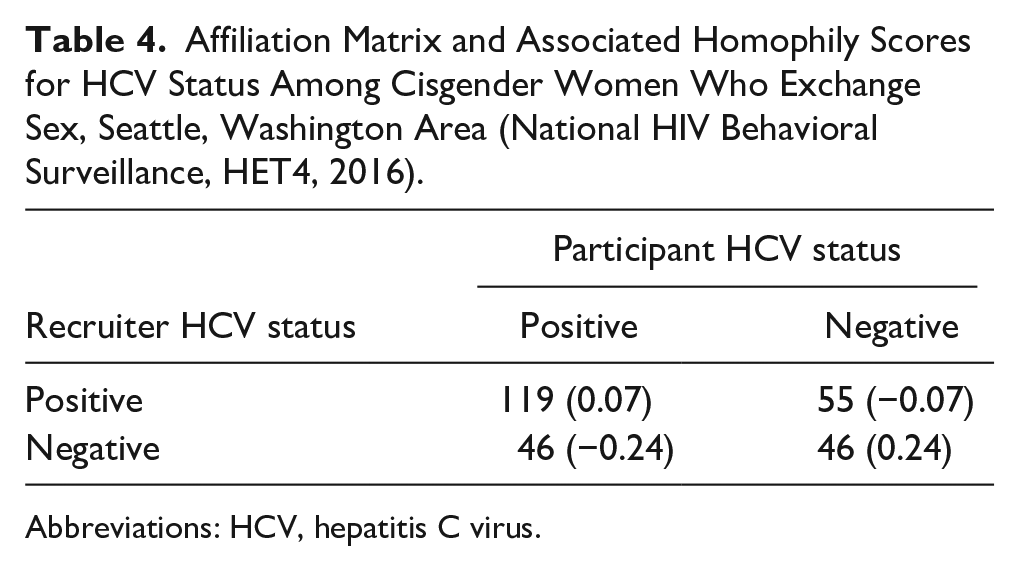
Abbreviations: HCV, hepatitis C virus.
Affiliation Matrix and Associated Homophily Scores for IDU History Among Cisgender Women Who Exchange Sex, Seattle, Washington Area (National HIV Behavioral Surveillance, HET4, 2016).
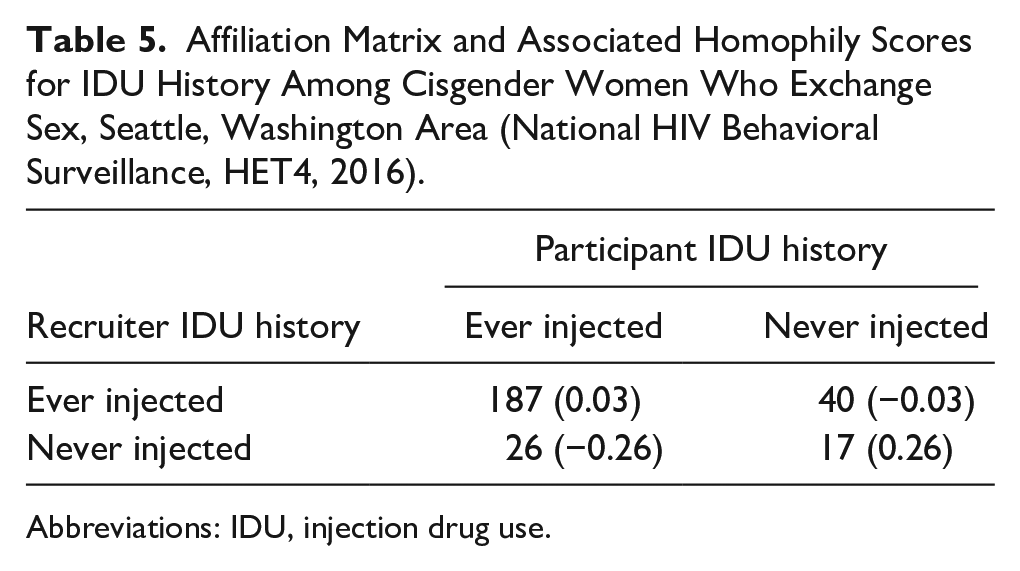
Abbreviations: IDU, injection drug use.
Discussion
The majority (nearly 80%) of individuals in our survey of WES in the Seattle, Washington area—most of whom engaged in street-based sex exchange—reported ever injecting drugs, explaining the high HCV seroprevalence (60%) in this sample. Notably, approximately half were unstably housed or experiencing homelessness, and few reported ever receiving HCV treatment. The sociodemographic makeup of this sample also bears similarities to that of individuals who were part of an HIV outbreak in Seattle, Washington, 35 which PHSKC identified 2 years after these data were collected. While this survey sample is likely not a representative sample of all WES in the Seattle, Washington area, our findings highlight that there is a subgroup of WES who have substantial healthcare needs. It is important that injection-related risk factors are not overlooked in this population where prevention and screening efforts are often focused on sexual risk factors alone.
The finding that younger age at initiation of injection was associated with HCV seroprevalence is not surprising, as those who began injecting at an earlier age have likely spent more time injecting and therefore had greater opportunity to acquire HCV. We also found that those whose most frequently injected drug was heroin were more likely to be HCV seropositive than those whose most frequently injected drug was methamphetamine. This finding—that HCV seropositivity is associated with the use of specific substances among PWID—is consistent with recent work from other areas in the United States,36,37 suggesting that HCV transmission among WES may be linked to drug use networks. Future work should be explore this phenomenon among WES.
The high prevalence of lifetime IDU in our sample of WES highlights the need for targeted HCV services and interventions for this population. WES—as well as other women who have HCV—are likely to encounter barriers and stigma when accessing health care.38,39 One strategy for reaching stigmatized communities is through peer referral. For example, a team from the University of British Columbia found that peer referrals to drug treatment were effective for WES. 40 Based on this and other work among populations with a high HCV burden,24,25 we hypothesized that HCV treatment interventions involving peer referral of networks may be beneficial to WES. Given the RDS recruitment strategy employed in this survey, we were able to evaluate if participants who have HCV were more or less likely to recruit (eg, be networked with) other women with HCV who exchange sex. Unfortunately, we did not see compelling evidence of this. Results of the homophily index calculations suggest that WES who are HCV seropositive and those who had a history of IDU were only marginally more likely to recruit others who shared these qualities. It is possible that this is because we did not specifically ask respondents to recruit other WES known to have HCV. These findings suggest that WES may build social links on their shared experience of engagement in sex exchange or other relationships, rather than along the lines of drug use behaviors or health experience.
With a treatment course as short as 8 weeks, DAAs present an opportunity to cure HCV durably and expeditiously. Although our findings suggest that peer referral to treatment may be ineffective, several potential alternative models exist. An incentivized walk-in care model, such as that of the Max Clinic at PHSKC 41 has proven effective in improving HIV viral suppression levels among patients with complex needs. 42 Similar to the sample of WES in our study, housing instability and IDU are common among Max Clinic patients. An expanded HCV care model for WES may also mirror the SHE Clinic, a partnership between Harborview Medical Center and Aurora Commons, an established, community-based agency serving homeless people in North Seattle. 43 SHE Clinic provides comprehensive healthcare services to women, including HCV treatment, and may present a scalable model for other locales. An additional potential model of care includes pharmacy-based or pharmacist-driven HCV treatment provision, which has been shown to be feasible and acceptable for PWID.44,45
This study has several important limitations. First, we did not have access to HCV RNA laboratory results, so we were limited to estimating associations between ever having had HCV as opposed to having a chronic or current infection, which likely has more public health significance. Second, we cannot be sure that our sample is representative of WES in the Seattle, Washington area. Third, these data were collected in 2016. Considering the displacement experienced by many people because of the COVID-19 pandemic, it is conceivable that the profile of this small and potentially transient population has shifted since that time. Fourth, while concerns regarding the statistical reliability of RDS recruitment and analysis methods are well documented,46 –48 we elected to analyze our data as a convenience sample to avoid potentially inducing bias with RDS weighted analysis. Lastly, self-reported data—particularly that concerned with sexual and drug use behaviors—always carry a risk of misclassification. Additionally, as we used cross-sectional data, we were limited in our ability to make risk inferences and could only identify associations between participants’ characteristics and HCV serostatus.
We acknowledge that seroprevalence does not reflect the true burden of active disease. Based on prior work,49,50 we estimate that up to 75% of those who are HCV seropositive may have an active, chronic infection. We used data collected in 2016, and since that time, HCV incidence among PWID has increased nationally. 51 Concurrently, HCV treatment for PWID has been increasing locally in the era of DAAs. 52 Notably, Washington State has enacted policies which have removed Medicaid restrictions to HCV treatment for persons who are actively using drugs 53 and it encourages providers to offer HCV testing and treatment to people who use drugs. 54 HCV treatment scale-up has taken place locally since these data were collected, thus it is possible that many study participants who had a chronic HCV infection have since been treated. Yet, prior research suggests that policy changes in WA has not rapidly translated into increased numbers of treated patients, pointing to implementation gaps. 55 Furthermore, WES who inject drugs experience intersectional stigma and it is conceivable that members of such a marginalized population do not access the consistent healthcare needed for HCV treatment success. Indeed, work from members of this authorship group that used 2018 NHBS data found that women who inject drugs were less likely than men to be treated for HCV. 10
As the opioid epidemic and concurrent stimulant use epidemic persist, populations of WES may continue to carry high burdens of HCV due to frequent IDU, and further study is warranted to mitigate these potential public health crises for this highly marginalized group. In the context of widely available DAA treatment, public health agencies and medical providers are equipped to intervene in the spread of HCV among WES, and future studies should explore the best way to approach and address this public health problem.
Supplemental Material
sj-docx-1-saj-10.1177_29767342231208936 – Supplemental material for High Seroprevalence of Hepatitis C Virus Among Cisgender Women Who Exchange Sex in the Seattle, Washington Area
Supplemental material, sj-docx-1-saj-10.1177_29767342231208936 for High Seroprevalence of Hepatitis C Virus Among Cisgender Women Who Exchange Sex in the Seattle, Washington Area by Michael P. Barry, Maria A. Corcorran, Judith I. Tsui, Courtney Moreno, Susan E. Buskin, Brandon L. Guthrie and Sara N. Glick in Substance Abuse
Footnotes
Acknowledgements
The authors wish to thank the NHBS interview staff at Public Health—Seattle & King County. Without their work, the present study would not have been possible.
Author Contributions
MPB and SNG conceived of the study. MPB, CM, and SNG conducted statistical analyses. All authors provided subject matter expertise and contributed to the development of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by cooperative agreement with the Centers for Disease Control and Prevention (6 NU62PS005094-01).
Compliance,Ethical Standards,and Ethical Approval
The Washington State Institutional Review Board approved all data collection activities. The University of Washington Human Subjects Division approved the present analysis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.