
Abstract
Background:
Children with developmental disabilities often face challenges in executive function, impacting emotional regulation, problem-solving, and social skill development. Due to their disabilities, these children become more isolated and have fewer opportunities for social engagement, which is crucial for successful interactions at home, in school, and in the community. Parents seek accessible social opportunities for their children but often report a lack of such services, which highlights the need for these interventions.
Materials and Methods:
To address this need, a 10-week interprofessional Interactive Vaulting (IV) occupational therapy program incorporating horses was implemented by an occupational therapist and IV instructor to facilitate targeted social skills in children with developmental disabilities. This quasi-experimental one-group pretest-posttest design applied the Cognitive Orientation to daily Occupational Performance model to structure interventions. Sessions were 60 minutes in length and included stationary barrel practice, horse grooming, team-building games and activities, and vaulting maneuvers on the horse. Fifteen children aged 5–13 years completed the program.
Results:
Statistical analysis yielded significant improvements in six areas of executive function as indicated by the Behavioral Rating Inventory-2 rated by the interacting vaulting instructor and in two areas rated by parents. Participants also showed significant improvements in group functioning, including activity participation, social interaction, and group membership, as measured by the Social Profile.
Conclusion:
These findings support further development and research of social skill groups developed through interprofessional collaborations that utilize horses as a tool and partner in practice.
Background
Developmental disabilities affect approximately one in six children, according to the Centers for Disease Control and Prevention. 1 These disabilities encompass a broad range of cognitive, neurological, neurobehavioral, and motor-based diagnoses such as intellectual disability, attention deficit hyperactivity disorder (ADHD), autism, cerebral palsy, and Down syndrome. They are best understood as a spectrum of disorders that vary in prevalence, onset, and severity and typically emerge at birth, during infancy, and childhood. Children with disabilities often exhibit delays in key areas of growth, including motor acquisition, central processing, such as problem-solving and reasoning, language development, and social and emotional functioning.1,2 When delays persist into adolescence and adulthood, it can have long-ranging impacts on the ability to learn and grow with typical peers.3,4
A common challenge for these children is the development of social skills, which affects their ability to interact with peers at school and in the community. These children have lower levels of participation in social and leisure activities, poorer psychosocial health, and increased feelings of loneliness and social isolation compared to their typical counterparts.5–7
Children with disabilities exhibit a wide range of deficits in social skills, often struggling with interpersonal communication and appropriate face-to-face interactions with others. These children struggle to appropriately modulate their volume or tone of voice during a conversation and hold eye contact. 3 Furthermore, nonverbal communication, including the ability to decode facial expressions or decipher body language, can be especially challenging for these children.3,8 They may also have difficulty understanding other people’s perspectives and taking turns during a conversation. 8 Unfortunately, lingering social skill deficits have contributed to unemployment or underemployment, a lack of friendships and romantic relationships, and low rates of independent living. Ultimately, this all leads to a diminished quality of life.9,10
Executive Functioning
A major factor in a child’s social development is their level of executive function.11,12 Previous studies have identified a positive correlation between a child’s social skills and underlying executive function, which encompasses higher-order cognitive processes like inhibition, organization, shifting, working memory, self-control, and planning.13,14 Executive functions may impact a child’s ability to recall someone’s name, organize or plan a social interaction, and execute these plans. They may also have difficulty shifting their responses smoothly in conversation according to what a peer has said and monitor their own behavior. 8 Research has found that children and adolescents with autism spectrum disorder exhibited global executive functioning difficulties compared to the population average, especially in the areas of shifting and cognitive flexibility. Furthermore, children with intellectual disabilities experienced executive function difficulties when compared to their typically developing peers in executive-loaded working memory, inhibition, planning, switching, and fluency. 15 Additionally, children diagnosed with attention deficit-hyperactivity disorder have delayed executive functions, including decreased attention, decreased working memory, and diminished ability to control actions and impulses. 16 These challenges make it exceptionally difficult for children to develop social skills during typical family and peer interactions.
Parent Interest in Alternative Approaches
Interest in and use of complementary and alternative approaches has grown as parents have identified gaps in both the structure and availability of services to help their children.17–19 They also reported that physicians lack knowledge and are not interested in learning about complementary interventions. 20 The social issues these children experience create a plethora of challenges, including depression and loneliness, which negatively impact family cohesion and quality of life. 21 The more isolated children with disabilities become, the fewer opportunities they are afforded to develop social skills to successfully engage with their peers and fully participate in life. Therefore, innovative and collaborative interprofessional approaches must be developed to address the social skill barriers children with disabilities face; programs using animals such as horses may be especially appealing and appropriate for children with developmental disabilities.
Use of Horses
Horses have unique attributes that make them a wonderful learning partner. They have a high emotional acuity to read and respond to human emotions,22,23 produce a calming effect, and alter their communication to assist humans in problem-solving.22,24,25 Furthermore, it has been found that the natural farm environment contributes to the learning process.24,25 These findings reinforce the use of horses in interventions that foster the development of social, emotional, and behavioral skills. Integration of equines into therapeutic environments and activities has grown in popularity and has shown promise in developing social skills, specifically engaging with peers, and decreasing maladaptive behaviors.26–28 Evidence reveals that equine-assisted services produce an improvement in executive function and social skills in children with autism. Specifically, gains have been found in therapeutic riding to improve social cognition, communication, and language. 26 Executive functioning, social functioning, and problem-solving skills have improved when using structured equine-assisted activities on the ground and on the horse with goal-oriented interactions in mind.29–31 Additionally, ground activities with a sensory focus, therapeutic riding activities, and socialization activities resulted in significant improvement in social communication, attention, and sensory tolerance. 30
A little-studied and less well-known equine service is Interactive Vaulting (IV). IV is a program that involves a group of up to six children, one horse, and one instructor. The ratio of participants to horse fosters an inviting environment for social interaction and encourages development of cognitive, emotional, and behavioral skills needed to interact with peers, instructors, and the horse. Furthermore, group socialization opportunities foster teamwork, teach respect for the horse and teammates, and allow reciprocal exchanges between children to explore ideas other than their own, take turns, and develop agreed-upon solutions to challenges. One of the goals of IV is to perform gymnastic movements while on the horse or on a barrel.32,33 Movements are practiced on a stationary barrel first, then on the dynamic surface of the horse’s back while controlled by a horse handler who guides in gaits in a controlled circle.33,34 At first, movements are typically performed at the walk, but depending on the skill of the rider, these movements can be executed in other gaits such as the trot or canter. Gymnastic maneuvers begin with the development of foundational skills such as sitting without support on the horse, and advancing to more complex moves such as kneeling or standing on the horse. 33 IV, because of the social skill practice it affords, could be strategically used by health care professions, such as occupational therapy, to help children develop executive functioning and social skills.
Occupational Therapy and Horses
Current literature supports the use of horses in occupational therapy service delivery. One study found clinically significant improvements in social skills, goal attainment, and motivation following occupational therapy in a 10-week program that integrated horses as a tool. 35 The sessions consisted of greeting the horses, ground activities, mounted activities, and social and life skill activities. Children demonstrated improved behavior and decreased irritability and hyperactivity through the duration of the program through therapist and parent report.35,36 Furthermore, an equine-assisted occupational therapy program utilizing the Cognitive Orientation to Daily Occupational Performance model (CO-OP) provided individual sessions to children with ADHD once per week over a course of a 12-week period. Sessions consisted of riding activities and riding-related ground activities such as grooming and tacking, resulting in improved executive function and life satisfaction with children diagnosed with ADHD. 37
Development of a Tailored Social Skills Group
Despite the compelling need for children with disabilities to develop social skills, there remains a lack of accessible social opportunities 21 and tailored social skill programs. 38 To address this gap, a 10-week interprofessional program called Partners in IV and Occupational Therapy (PIVOT) was developed with two specific research aims. The first was to determine the influence of the program on executive function in the children with disabilities participating. The second was to determine the program’s impact on children’s ability to participate, socially interact, and cooperate in a group that incorporated horses. To date, research on a collaborative occupational therapy IV program has not been conducted, thus warranting investigation.
Materials and Methods
This study utilized a quasi-experimental one-group pretest-posttest design to explore the impact of an interprofessional occupational therapy group using horses on children with disabilities’ executive function and social participation.
Partners in interactive vaulting and occupational therapy (PIVOT)
An occupational therapist and certified IV instructor developed the PIVOT program at a therapeutic riding facility in the southeastern United States. The occupational therapist had 30 years of clinical experience, while the PATH-certified therapeutic riding instructor had 20 years of experience and had an IV certification. Both professionals played pivotal roles in the development of the group. The PATH International Certified Vaulting Instructor managed the horse during vaulting activities and contributed valuable expertise during unmounted sessions. This included teaching participants about horse behavior, how horses express emotions, their responses to humans, and strategies for integrating the horse into both mounted and unmounted activities with the children.
The occupational therapist took the lead in designing and implementing the social skills group. They collaborated with parents and children to establish individualized social skill goals and tailored the group experience to each child’s unique needs, ensuring the program was both engaging and effective. Group sessions were developed with the overarching goals of developing and improving participants’ ability to work as a team, understand and use verbal and nonverbal communication to interact with others, and develop problem-solving skills. The PIVOT program consisted of 10- to 60-minute sessions with one horse and up to six children. Graduate occupational therapy students assisted in the data collection and implementation of the groups as part of the requirements for their degrees.
Program framework
The PIVOT program was developed using the CO-OP approach, which “is a goal-based, task-oriented approach that draws on cognitive strategy used to effect change in occupational performance.” 39 The CO-OP model utilizes metacognitive approaches that facilitate self-discovery of strategies that promote generalization and transfer of acquired skills to improve occupational performance in a variety of activities that are meaningful to the individual. 39 CO-OP is also a highly individualized intervention model; each child works collaboratively with caregivers and the therapist to choose individual goals to be focused on during the program and beyond. 40 This collaboration is a critical component of the success of the CO-OP model, as extensive literature supports the importance of child-chosen goals contributing to intrinsic motivation and autonomy necessary for persistence in goal attainment efforts.39,40 Furthermore, the role of parent involvement is noted to be crucial in the generalization and transfer of skills acquired during therapy sessions into daily life activities that support increased engagement in meaningful occupations in novel contexts. 40
Goal-setting process
The goal-setting process begins prior to the first PIVOT session. All parents were sent an email introducing the program, describing the CO-OP approach, and including a list of potential social skills for goal development (look at the speaker, accept help from a peer, etc.). It was recommended that parents have a conversation with their child to discuss and identify goals that would be of focus for the 10-week session. During the first two sessions, group facilitators helped the child narrow the focus of their efforts on two social skill goals for each participant. Goal sheets were then developed for each participant that included the goal, the plan for achieving the goal, and evidence to determine if their efforts were successful. Parents were provided with a copy of these goals to post in a prominent place at home but were advised not to review them with their child. By the third session, goals were displayed on a wall to be referenced throughout sessions. Program activities were structured using the Goal-Plan-Do-Check problem-solving strategy. 39
Session description
Mounted activities on the barrel and/or horse
Each PIVOT session included 30 minutes of mounted games and 30 minutes of unmounted games and activities tailored to the needs and abilities of the group. At the beginning of each session, each child was required to “check-in” and review their social skills goals with a group facilitator and “plan” how they were going to address their social skill goals. They then engaged in group activities, which is reflective of the “do” part of the CO-OP model. Mounted activities involved practicing vaulting movements one at a time on a stationary barrel and then attempting them on the horse. Once children mastered gymnastic moves safely, teamwork activities were added to mounted activities using both the barrel and the horse. For instance, in Simon Says, the child on the horse instructed participants on the ground to complete movements following the game’s rules. For children engaged on the ground, it required sustained attention, listening skills, and impulse control as they waited for their turn to lead. To further challenge children, they were instructed to determine as a group their order for mounted activities. This encouraged children to negotiate with peers of who should go first and reflect on how their choices may affect others. Additionally, unmounted activities further challenged teamwork, requiring them to listen, take turns, and regulate their emotions during challenging interactions.
Unmounted activities
Unmounted activities included team-building activities that focused on developing verbal and nonverbal communication, identification, and managing emotions within themselves and others. One activity titled Fragile: Handle Friends with Care aimed to increase awareness of others’ feelings and understand actions that can hurt them. Children were paired in teams of two and given a hard-boiled egg and materials to wrap their egg in to protect it. The objective was to use the materials they were provided to keep the egg from cracking when dropped from a mounting block. After all the eggs were dropped, the children unwrapped them. A large team discussion followed, using the analogy that cracks in eggs are like our feelings—fragile and easily hurt. To add more challenge, scenarios were provided for the entire group to determine what emotion a person could be experiencing and how to prevent it and/or comfort someone with hurt feelings. At the end of the session, each child completed a “checkout” and reviewed their goals with a group facilitator. The child’s performance was reviewed, with the child commenting on whether they achieved their goals and the strategies used. The facilitator also provided feedback, highlighting specific examples of when the child exhibited behaviors that supported progress toward their social skills goals and those that did not. The session incorporated social-emotional learning centered around the horse partner. One activity invited participants to pick a card from a basket, each featuring a negative word or phrase often unfairly said about the horse. Descriptors like “fat,” “dumb,” and “ugly” were listed on the cards. Each child shared their chosen card, and facilitators used facial expressions, tone, and body language to act out the hurtful words—not directed at the horse, but with the horse present. This led to a discussion about how the horse might feel hearing such words, sparking lively conversations about the inaccuracy of the terms. The children naturally came to the horse’s defense, demonstrating their emotional empathy—not just for themselves, but for their equine teammate.
Following this dialogue, each child was encouraged to write a positive word on a new card and share their chosen word with the horse. Discussions emphasized the value of using truthful and supportive language to nurture growth and foster a sense of belonging for all.
Participants
After obtaining approvals from the Institutional Review Board and the Institutional Animal Care and Use Committee, children with disabilities who were eligible to participate in the PIVOT program were identified using convenience sampling. To be included in the study, participants needed to be ambulatory, capable of following simple directions, able to adhere to safety rules, and open-access of medical contraindications for unmounted and mounted horse work. Fifteen children, 10 males and 5 females, completed the study. The mean age of children in the group was 8.6 years (SD 2.6 years), ranging in age from 5 to 13 years of age (Table 1). Five children were in each group.
Participant Description
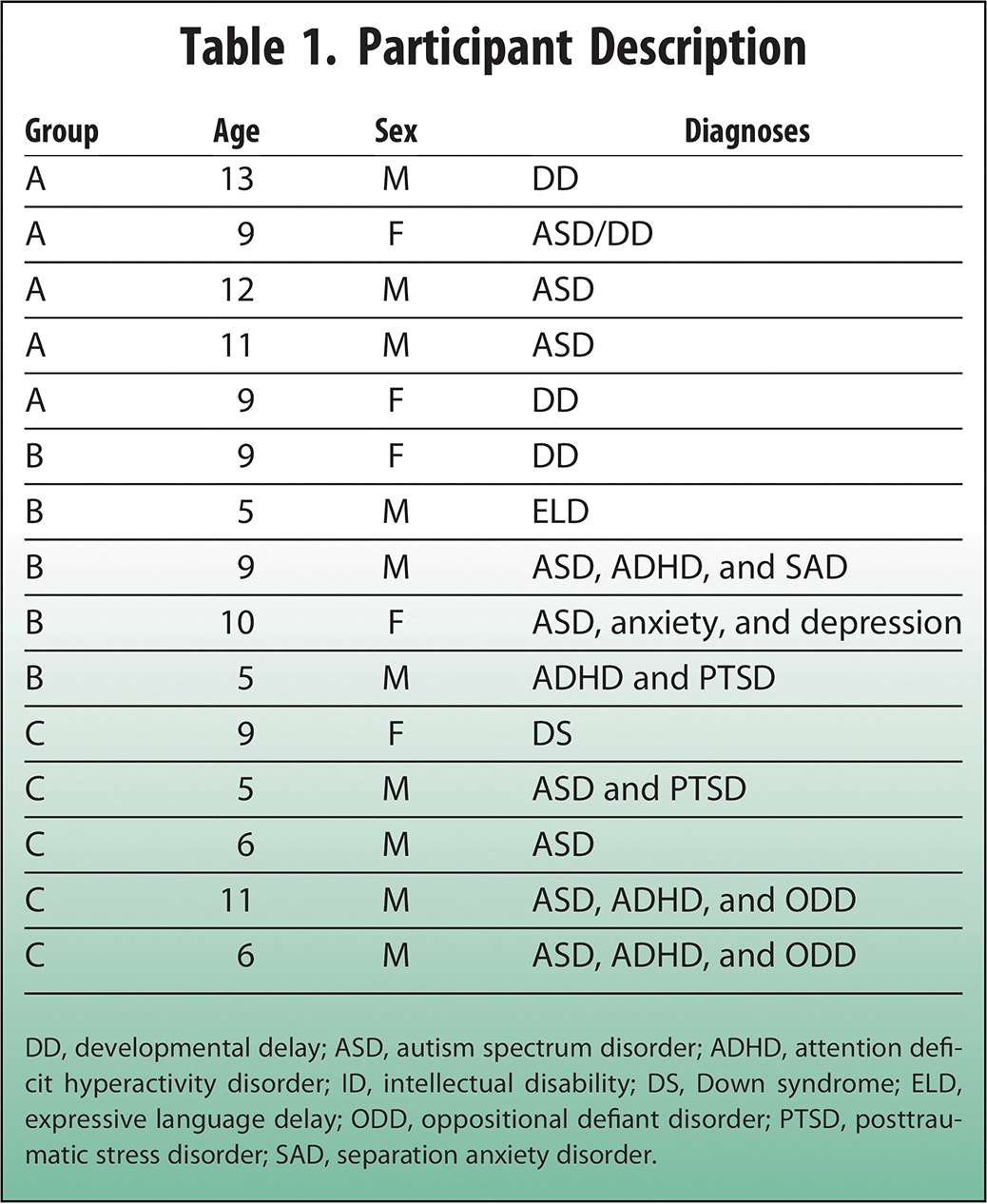
DD, developmental delay; ASD, autism spectrum disorder; ADHD, attention deficit hyperactivity disorder; ID, intellectual disability; DS, Down syndrome; ELD, expressive language delay; ODD, oppositional defiant disorder; PTSD, posttraumatic stress disorder; SAD, separation anxiety disorder.
Instruments
Two objective measures were utilized to evaluate executive function and behavioral interactions of participants at the beginning of the first session and at the end of the last session. The Behavioral Rating Inventory of Executive Function, Second Edition (BRIEF-2) assesses executive function in children and youth ages 5–18 years. 41 This assessment measures three domains of executive functioning, the Behavioral Regulation Index, Emotional Regulation Index, and Cognitive Regulation Index. It also provides an overall Global Executive Composite Score (Table 2).
Description of BRIEF-2 Clinical Scales 41
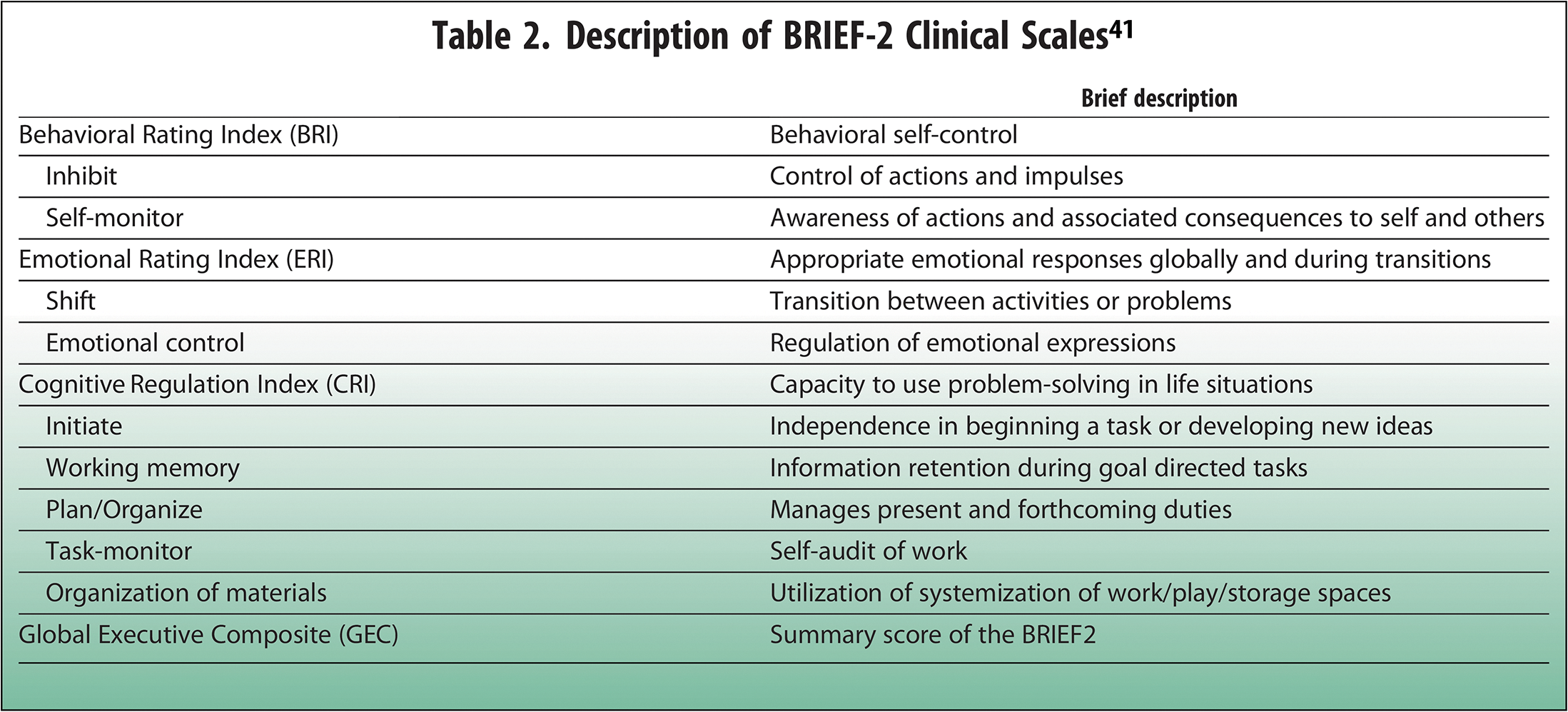
This assessment has 63 items, rated by the parent or caregiver living with the child using the parent form and by the IV instructor using relevant sections of the teacher form. The frequency of various behaviors uses a scale of never, sometimes, or often. T-scores are used to interpret indexes and scales, with scores between 60 and 64 mildly elevated, 65 and 69 potentially clinically elevated, and scores at or above 70 clinically significant. Validity and reliability of the BRIEF-2 have been well established.41,42 Increases in t-scores in or into the clinically significant range is indicative of concern and potential worsening of behaviors.
The Social Profile is an observational instrument that assesses behavioral interactions of individuals in groups in three areas: activity participation, social interaction, and group membership. The assessment demonstrated good validity and reliability43,44 and has two versions. The children’s version assesses ages 18 months to 11 years, while the adult/adolescent version assesses individuals 12 and older. Social Profile scoring is based upon an incremental group continuum, reflecting individual behaviors consistent with group level. These levels range from the lowest level of interaction (parallel group), to associative, then advancing to the basic cooperative in the children’s version and parallel group, associative and basic cooperative, supportive cooperative, and mature in the adult/adolescent version. The children’s version was used in this study. Scoring is completed using a Likert scale of 0 (never) to 5 (always), and a higher score at lower levels of the continuum indicates more rudimentary skills. 43 This assessment was designed to show change over time. For example, it is hoped that with intervention the child would demonstrate behaviors at higher group levels. As the child progresses in their ability to participate in groups, mean scores on lower levels of group function (parallel) would decrease, and mean levels of higher levels of group performance would increase, demonstrating increased ability to participate in group situations with peers. The Social Profile was completed the first week by observation and scored by two people, the PI and a graduate student, to ensure accuracy and interrater reliability.
Data analysis
All data obtained through the BRIEF-2 and the Social Profile were de-identified and analyzed using the Wilcoxon signed ranks exact test due to the lack of normal distribution of scores. This test explored differences in executive function (provided by the BRIEF-2) resulting from the PIVOT program from the IV instructor and parent perspectives. Results from the Social Profile explored social participation and group skill performance resulting from the PIVOT program. Effect sizes were calculated to determine the magnitude, or clinical effect, of the PIVOT program on the children involved in the study, with 0.2–0.49 indicating a mild effect, 0.5–0.79 indicating a moderate effect, and 0.8–1.0 indicating a large effect. 45
Results
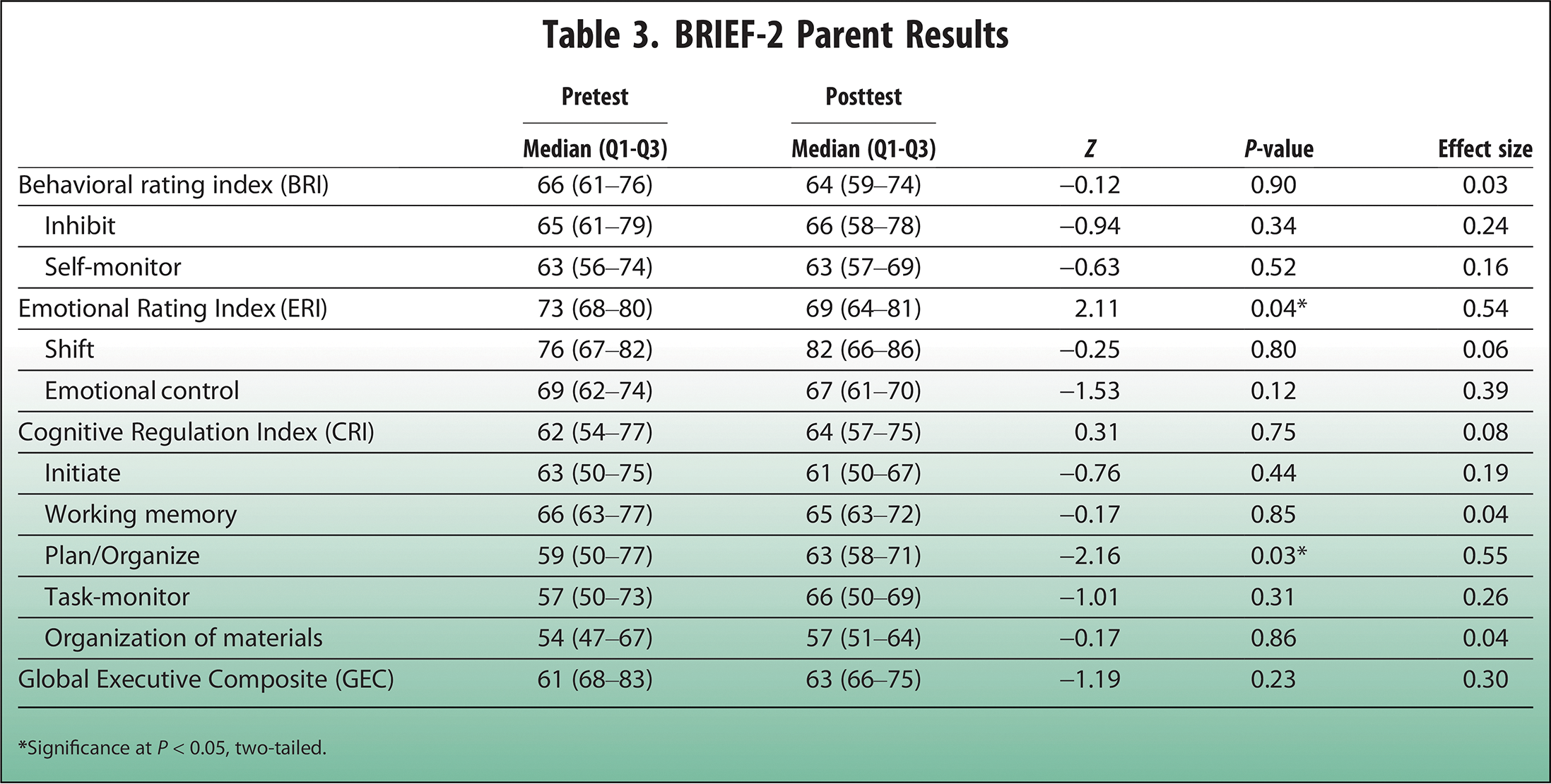
Results obtained from the BRIEF-2 parent report indicated significant differences on the Plan and Organize scales. Median scores increased, which is indicative of a worsening of scores on this scale from pre- to posttest. One potential reason for this increase is that posttest data were collected over an extended break, which could account for the increase in score. A change in routine and potential lack of structure during a break could contribute to this finding. In contrast, significant positive findings were found on the Emotional Rating Index, where the median score dropped from pretest to posttest (Table 3). These results gleaned moderate effect sizes, while all others had small effect sizes.
BRIEF-2 Parent Results
In contrast, the IV instructor rating scales reflected statistically significant differences from pre- to post-program on 6 of the 9 executive function scales and indexes. Behavioral scales that reached significance included Inhibit and Self-Monitoring, which was also reflected on the Behavioral Rating Index. The Emotional Control scale results were remarkable, while the Shift scale did not reach significance. Overall, the Emotional Rating Index was significant. The Cognitive scale that reached significance was Working Memory; however, Initiate—and Plan/Organize—were not significant. Interestingly, both parents and the IV instructor reported significant changes related to emotion, but only parents reported negative changes on the Plan/Organize scale. Overall, the clinical relevance of the results was marked, as medium to large effect sizes were found on 6 of the 9 indexes and scales on the BRIEF-2, strongly supporting the practical therapeutic impact of the program (Table 4).
BRIEF-2 Instructor Results
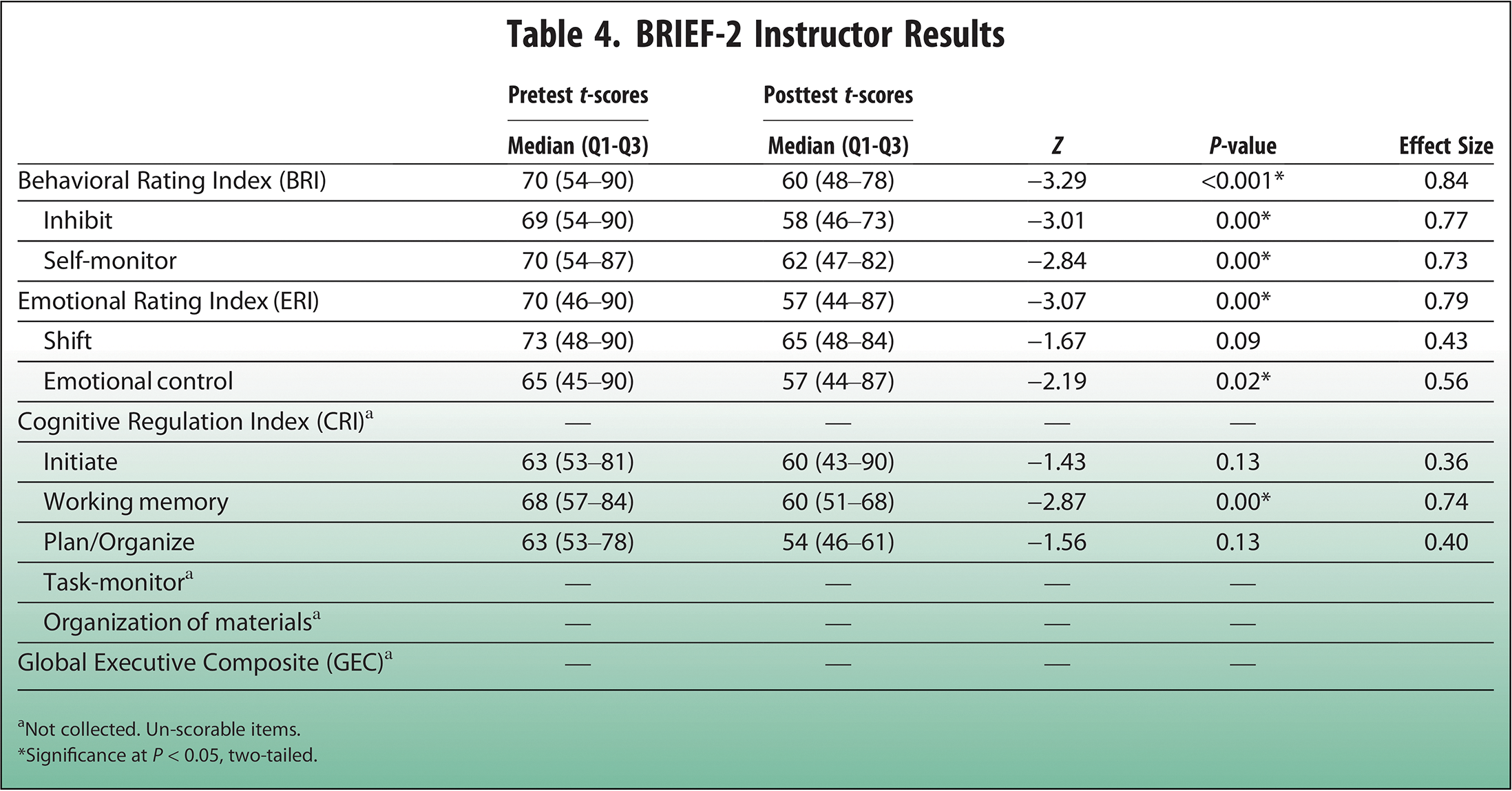
Not collected. Un-scorable items.
*Significance at P < 0.05, two-tailed.
Statistically significant positive changes in social interaction in the children were evidenced by decreased median parallel group scores, with corresponding increases in skills noted by increased median Associative and Basic Cooperative scores. Children demonstrated improvements in skills that included giving and seeking assistance from others and experimenting with group member roles such as leading, listening to ideas, and following the will of the group.
Children also demonstrated significant changes in their ability to socially interact. Median Parallel Social Interaction group scores decreased, while median Associative and Basic Cooperative scores increased. These gains reflect improvements in skills such as seeking and helping others and exploring group roles, including leading, listening to ideas, and following group decisions.
Significant progress was also observed in Group Membership and Roles, which assess a sense of belonging within the group. While Parallel median scores remained unchanged, substantial increases were noted in Associative and Basic Cooperative levels. At the Parallel level, children required consistent guidance from the group leader to engage. However, as they advanced, they displayed greater cooperation and emerging competitive behaviors while adhering to socially acceptable actions. The findings further yielded moderate to large effect sizes on eight of nine areas on the Social Profile (Table 5), which supports the clinical relevance of the PIVOT program.
Results of Social Profile in OT Intervention Group
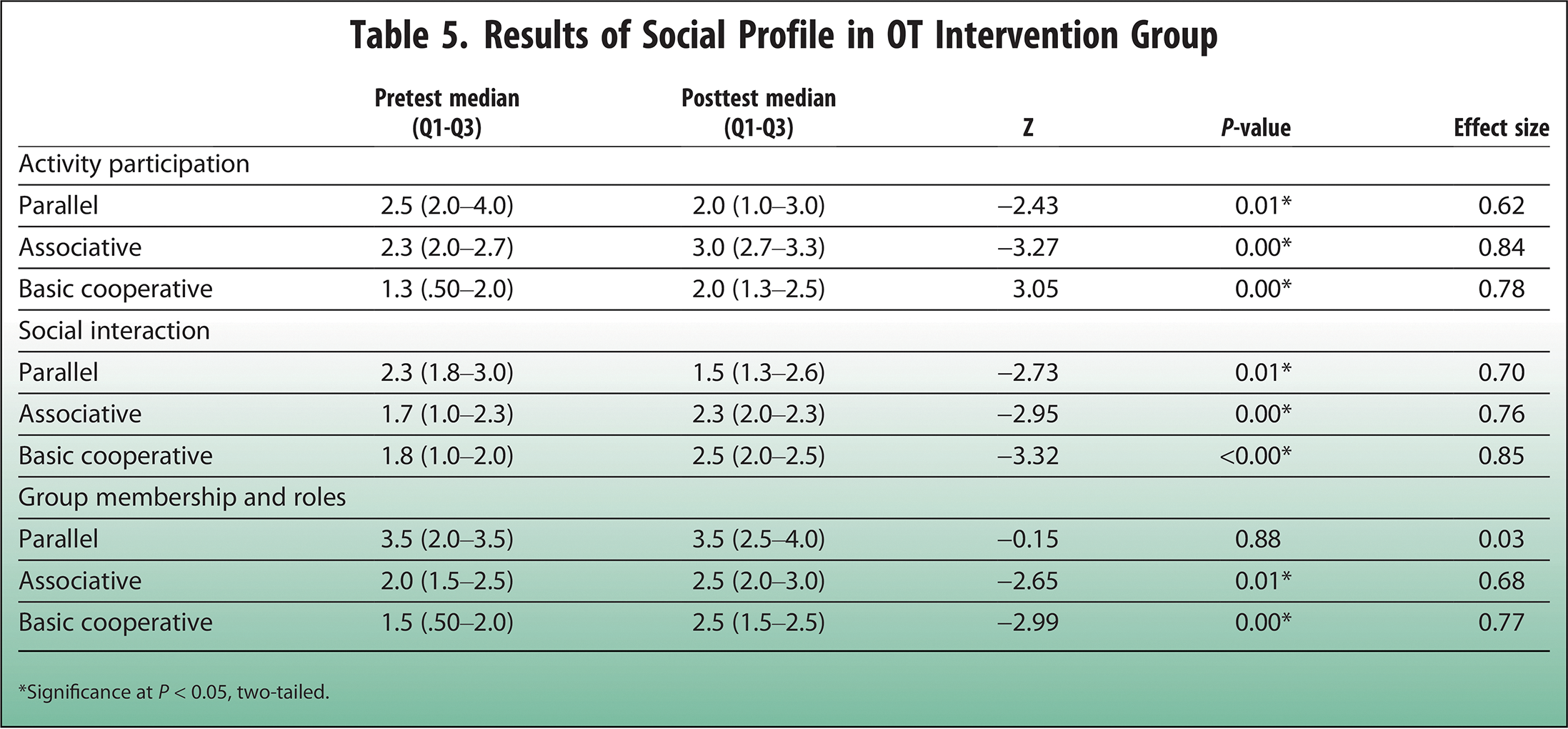
*Significance at P < 0.05, two-tailed.
Discussion
The results of this study support the use of the PIVOT program, as participating children demonstrated meaningful behavioral, social, and emotional growth. Parents’ assessments of their child’s executive function on the BRIEF-2 revealed significance on one scale and index. Notably, median scores increased on the Plan/Organize scale, potentially influenced by reduced daily structure. Encouragingly, there was a decrease in ERI median scores with a moderate effect size, further endorsing the clinical utility of the program. Behavioral changes observed included improved emotional control during challenging activities, reduced impulsivity, and an increased ability to wait for game and activity instructions. Children also showed flexibility in accepting alternative ways to complete tasks. Mixed results on the BRIEF-2 are understandable, considering parents’ broader context in evaluating their child’s progress.
Results on the BRIEF-2, as reported by the IV instructor, achieved significance in most areas of executive function assessed. These results could be explained by the week-by-week interaction with the children and observing incremental changes over the course of the 10-week program. The children exhibited behavioral gains as evidenced by their increased sustained attention, the ability to initiate tasks and accept challenges, and remembering directions in a busy group environment.
Differences in perception of performance between the IV instructor and parents could be attributed to the reductionistic view of the instructor, who only saw children in pre-planned group activities. Differences in perception of EF may exist due to the lack of generalization of skills when with family, at school, or out in the community. Although skills may not yet be used in day-to-day life, moderate to high effect sizes were noted, lending evidence for the clinical effectiveness of the PIVOT program. These findings provide critical information and suggest that the next step to enhance the program would be to encourage parents to use the social skill strategies used in the program in everyday contexts.
Results gathered from the Social Profile were significant and had medium to large effect sizes in eight of nine in the areas of Activity Participation, Social Interaction, and Group Membership and Roles. Again, support for the PIVOT program in clinical practice was found. Gains were noted in the children’s ability to engage and enjoy sharing activities with peers and complete activities with less adult support and encouragement. In addition, children were observed appropriately by asking and giving help when requested from a peer, accepting challenges such as being the leader of an activity, and offering ideas to solve a problem.
One of the key outcomes of this research is the development of the PIVOT program, as it had marked differences from traditional social skill programs. The innovative use of the horse, the farm milieu, and the interprofessional nature of the group provided a unique learning laboratory for the children. The PI, an occupational therapist, collaborated with the IV instructor to develop each group session. Central to PIVOT was the intentional designation of the horse as a teammate, which encouraged children to improve verbal and nonverbal communication not only with each other but also with the horse during both mounted and unmounted activities. The IV instructor guided children in communicating with the horse, developing horsemanship skills such as grooming and tacking, and performing vaulting maneuvers. Successfully completing these activities required building a relationship with the horse—a motivational process that could potentially foster bonds with other animals. Research highlights the benefits of animal companionship, including reduced isolation and loneliness in children with neurodevelopmental disabilities,7,46 as well as providing social support. 47
Since social skill development was the program’s primary objective, these findings support further investigation of the CO-OP model to structure social skill interventions. Researchers have continually emphasized the importance of using a replicable framework for rigorous study, and the CO-OP model espouses those features.48,49 The Goal-Plan-Do-Check problem-solving strategy provided a consistent problem-solving and feedback routine, which was an important routine for the children, but also standardized the structure of the group interventions. Furthermore, normalizing the pursuit of social skill goals across the group made a potentially sensitive topic open to conversation. In addition, the tenet of guided facilitation, specific to the CO-OP approach, encouraged children to navigate the social interaction autonomously, where adults offered suggestions and potential solutions to social issues when asked, versus dictating to the child on how to manage the social interaction. This allowed children the time and space for experimentation to find socially acceptable solutions when involved in group activities.
Conclusions
Results of this study identified significant differences in executive function and social participation in children with disabilities who participated in the PIVOT program. Furthermore, moderate to large effect sizes were also revealed, which supports its use in clinical practice. PIVOT included a unique mixture of ingredients, such as an interdisciplinary approach, a structured and replicable framework, and incorporation of the horses as a teammate in the learning process. Further investigation is needed to examine its efficacy with specific diagnoses (i.e., autism) and expand the program to include opportunities for children to generalize the skills learned in the program into their everyday life.
Limitations and Future Directions
The limitations of this study are evident but offer valuable insights for future research. First, the small sample size and lack of a homogeneous diagnostic group presented challenges. Future studies should aim to increase sample size and consider grouping participants by diagnosis to evaluate diagnosis-specific benefits.
Moreover, there is a notable scarcity of research on the feasibility and efficacy of interdisciplinary approaches, particularly those involving complementary methods with horses. Collaborating with other professionals could create more opportunities for children to develop and generalize social skills.
This study also lacked a comparison group. Future research could compare ground-based horsemanship interventions to mounted approaches to determine which yields better outcomes. Lastly, the limited generalization of skills, as reported by parents, reduces the broader impact of the findings. Including a parent education component in future programs could support the integration of program goals and skills into real-world contexts.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was partially supported by the North Carolina Horse Council.▪