
Abstract
Introduction:
Attention deficit hyperactivity disorder among adults has been associated with deficits in executive functioning and poor quality of life. The purpose of this study is to examine feasibility of the Cognitive Functional Remote Group intervention among adults with attention deficit hyperactivity disorder.
Method:
Mixed-method feasibility study. Five adults with attention deficit hyperactivity disorder received 16 weekly sessions of Cognitive Functional Remote Group.
Results:
The target population was easily recruited and showed interest in the treatment. All participants completed the intervention and were moderately-very highly satisfied with different aspects of the intervention. Additionally, pre–post measures demonstrated high rates of clinically significant improvements in the quality of life measure and less so in executive functioning. Three central themes emerged from qualitative analyses of participants experiences relating to (a) Identity development through group process; (b) Occupation-based learning of self-awareness and cognitive functional strategies and (c) Feedback on group setting and content and relating to advantages and disadvantages of remote (Zoom) format.
Conclusion:
This study supported Cognitive Functional Remote Group feasibility among adults with attention deficit hyperactivity disorder. Quantitative findings point to the responsiveness of quality-of-life measures. Qualitative findings suggest gains in identity development, awareness and acquisition of cognitive functional strategies through occupation-based learning in a telerehabilitation group therapy format. Further controlled studies are warranted.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental chronic disorder characterized by patterns of inattention and/or hyperactivity/impulsivity with significant impairment in occupational functioning (American Psychiatric Association, 2013). The prevalence of ADHD in adults ranges between 1.4 and 3.6%, with far-fetching implications (Kooij et al., 2019). The findings in the literature show that ADHD in adulthood critically affects daily functioning in various aspects of life, such as work, study, relationships, financial responsibility, health management and leisure, as well as the quality of life (QoL) (Brod et al.,2015; Goffer et al., 2019; Kooij et al., 2019; Nimmo-Smith et al., 2020). For example, college students with ADHD typically attain lower grades than their peers and experience difficulties in their varied occupational roles that negatively impact their QoL (Barkley, 2015; Goffer et al., 2019). Moreover, many studies show that there are detrimental psychological effects such as poor self-esteem and self-efficacy and higher psychiatric comorbidity, especially with depression and anxiety (Kooij et al., 2019), which further impede daily functioning and QoL (Brod et al., 2015).
Deficits in executive function (EF) are considered to be one of the central mechanisms underlying the functional difficulties and impaired QoL in ADHD (Barkley, 2015; Brown, 2009; Stern et al., 2017). Executive dysfunction is attributed to core neurological deficits of the prefrontal networks, in charge of self-regulation and enabling goal-directed behavior (Barkley, 2015). EF models in ADHD identify characteristic deficits in self-regulation, such as inhibition, working memory and shifting that are required for intentional control of cognition, emotion and behavior (Silverstein et al., 2020). Considering the dominant role of EF on goal-directed behavior and the evidence supporting its negative impact on daily functioning and QoL, it has been identified as a central target for intervention (Stern et al., 2017).
The “gold standard” recommended treatment today for adults with ADHD is a combination of pharmacological and nonpharmacological treatments, which focus on reducing symptoms, improving daily functioning and QoL (Kooij et al., 2019; National Institute for Health and Care Excellence, 2018). Pharmacological treatments are effective first-line treatments for ADHD (Kooij et al., 2019). However, up to half of patients discontinue pharmacological treatment within the first 3 years of treatment due to side effects and treatment ineffectiveness (Kooij et al., 2019). Among the nonpharmacological treatments, cognitive behavioral therapy (CBT) is the most frequently studied (Fullen et al., 2020; Nimmo-Smith et al., 2020). CBT concentrates on cognitive restructuring and changing maladaptive behavioral strategies together with the enhancement of self-esteem (Fullen et al., 2020). Another intervention mentioned in the literature is dialectical behavior therapy (DBT), which is based on cognitive behavioral techniques for emotional regulation and employs the use of mindfulness and acceptance principles (Fullen et al., 2020). Mindfulness is defined as intentionally paying attention to present-moment experiences and is based on the core principles of acceptance and self-compassion (Fullen et al., 2020). Studies show that CBT, DBT and mindfulness treatment are all effective for improving ADHD symptoms (Fullen et al., 2020; Nimmo-Smith et al., 2020). CBT Studies also improve psychological measures (Fullen et al., 2020; Nimmo-Smith et al., 2020). In addition, there are controversial interventions with limited evidence, such as neurofeedback, psychoeducation, dietary supplementation and homeopathy (Nimmo-Smith et al., 2020).
Occupational therapy, may have a unique contribution to the nonpharmacological treatment of adults with ADHD, considering its expertise in understanding EF within the context of daily life (Agarwal et al., 2012). The Cognitive Functional (Cog-Fun) model is an occupation-centered intervention that aims to promote participation in life roles and QoL among individuals with ADHD and executive dysfunction (Maeir et al., 2018). The Cog-Fun focuses on the development of metacognitive skills, including adaptive self-awareness to ADHD implications, online awareness (i.e. self-awareness within the context of a specific task) and cognitive functional strategies within the context of individualized occupational goal attainment (Levanon-Erez et al., 2019). The main change mechanisms of the Cog-Fun include: (a) metacognitive learning, (b) environmental supports, (c) occupation-centered intervention and (d) positive engagement (Maeir et al., 2018). The effectiveness of Cog-Fun was examined among children, adolescents and adults with ADHD and has shown statistically significant improvements in EF, awareness, participation and QoL (Kastner et al., 2022; Levanon-Erez et al., 2019).
The supply of occupational therapy services is still limited compared to the growing demand in the general population for these services (Hung and Fong, 2019). Both group intervention and telerehabilitation services can contribute to bridging this gap between supply and demand. Group intervention is defined as the treatment of several clients in one space, which presents the individual’s point of view while referring to the content and to the group processes as levers for change (Mahon et al., 2017). In recent years, group interventions for adults with ADHD have also been developed. Studies conducted among adults with ADHD reported that CBT, DBT and mindfulness that were administered in a group setting had positive implications on ADHD symptoms. In addition, several studies have even shown an advantage of group versus individual treatment in this population (Fullen et al., 2020).
Telerehabilitation refers to the use of information and communication technologies to provide remote rehabilitation services to people in their preferred settings (Hung and Fong, 2019). Telerehabilitation can improve accessibility and cost-effectiveness since it allows services to be delivered to people in their homes without the therapist being physically present (Caprì et al., 2020). Furthermore, specifically in adults with ADHD, telerehabilitation might be beneficial considering problems in treatment persistence, time management and effort recruitment (Sehlin et al., 2018). However, there may also be disadvantages, such as challenges using technologies, issues involving privacy and attitudes of clients and clinicians (Beit Yosef et al., 2019). In recent years, several studies examined Occupational therapy (OT) cognitive telerehabilitation in adults with acquired cognitive impairments, such as among adults with chronic brain injury (Beit Yosef et al., 2019) and adults with cancer (Maeir et al., 2020), yet have not been examined in adults with ADHD. So far, studies on the Cog-Fun Adult intervention model have been conducted in a face-to-face individual therapy setting. In order to explore the potential benefits of group remote occupational therapy for adults with ADHD, we developed the Cog-Fun Remote Group (Cog-Fun RG) intervention.
The purpose of this study is to examine the feasibility of the Cog-Fun RG. Specifically, we aimed to examine: (a) recruitment, retention, adherence and acceptability; and (b) responsiveness of potential outcome measures in preparation for a controlled study. It was hypothesized that Cog-Fun RG would be found to be a feasible intervention for adults with ADHD.
Methods
Study design
Feasibility study using mixed quantitative and qualitative methods.
Intervention: Cog-Fun RG
The Cog-Fun RG comprises 16 weekly 90-minute sessions (see Table 1) based on the Cog-Fun Adult model (Kastner et al., 2022; Maeir et al., 2018). The original Cog-Fun Adult manual was adapted to a remote group format and validated with a focus group of six experts in Cog-Fun and group therapy. The major adaptations to the original protocol involved addressing the therapeutic group process, changing the session structure, emphasis on collaborative learning and integrating individual occupational goals (termed “mini goals”) into the group setting.
Content goals and group process according to the sessions.
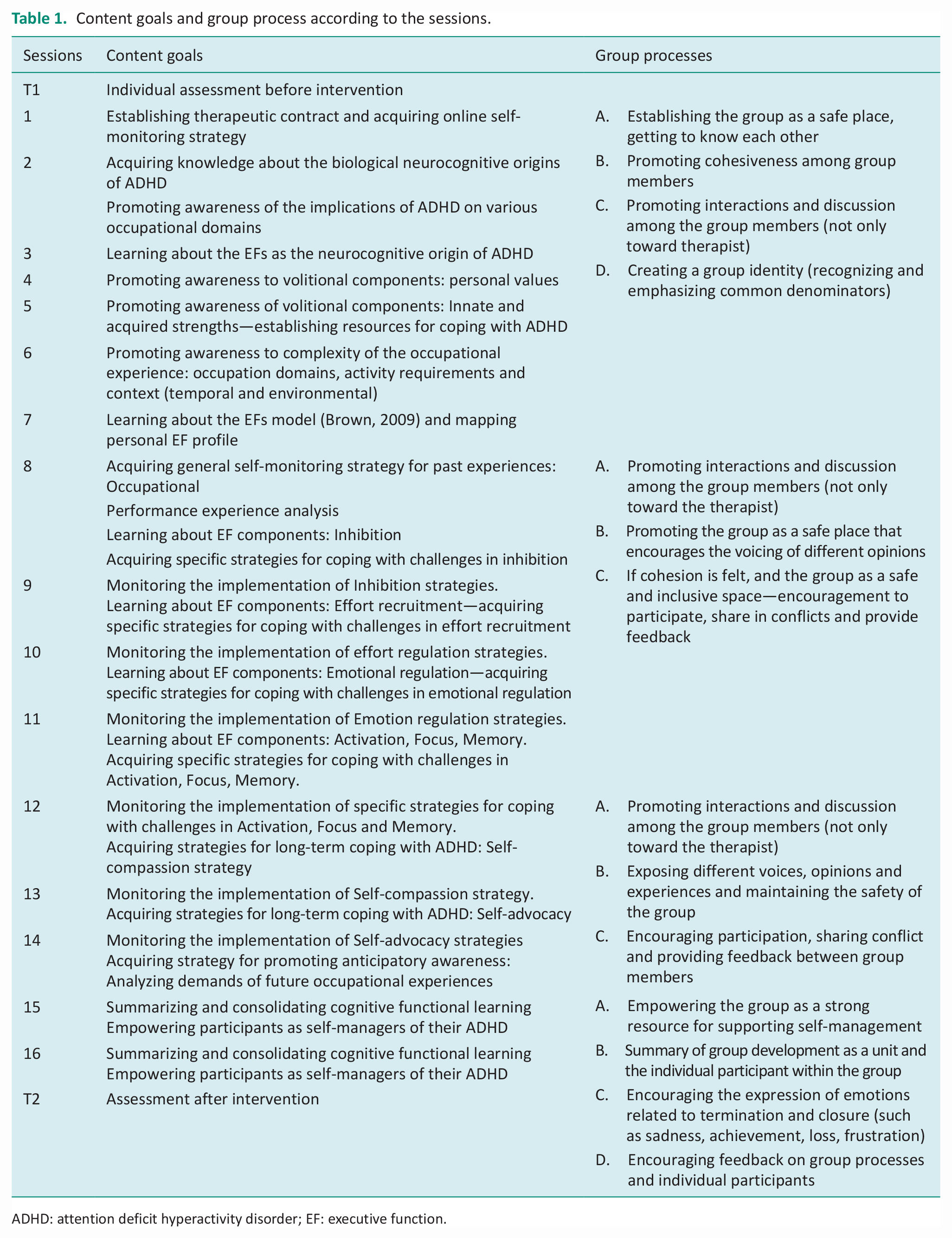
ADHD: attention deficit hyperactivity disorder; EF: executive function.
Cog-Fun RG emphasizes promoting awareness and acquiring EF strategies in an occupational context via the therapeutic group processes. The structure of each session was based on Cole’s (2012) OT Group framework including the components of Introduction, Collaborative Learning, Generalization, Application and Summary. In addition, each session has specific Cog-Fun content goals (i.e. understanding ADHD as a disorder of EF and its impact on daily life activities; cognitive functional strategies), as well as general group process goals, such as cohesion, interpersonal learning and universality. Group process goals were defined according to Yalom and Leszcz (2005) therapeutic factors (TFs) that transpire due to interpersonal interaction in the group. The content and group process goals according to the sessions are presented in Table 1. Following is a brief description of the components of each session.
The Introduction component of each session includes presenting the session topic, online self-monitoring and reviewing the “mini-goal” (determined at the end of each session). The online self-monitoring involved each participant attending to physical aspects in themselves (e.g. level of alertness, thirst, hunger) and in their immediate context (e.g. what do you see and hear). This initial online self-monitoring activity, was designed to promote a joined sense of presence among participants as well as to develop online awareness, which is a basic tenet of Cog-Fun. The second component, Collaborative Learning, comprises a learning activity addressing content such as Browns model for EF in ADHD (Brown, 2009), volition, occupation domains, activity requirements and context and so on. The learning activity was adapted to the neurocognitive profile of adults with ADHD, that is, adjusted to difficulties focusing and sustaining attention and limited working memory. Therefore, Collaborative Learning includes very short audio-visual presentations, personalizing the content to participants’ occupational experiences (inside and outside of the group) and shared processing. The next component, Generalization, comprises a brief review and summary of main themes while highlighting shared and unique experiences of the group members. The Application component includes an individual written assignment followed by group sharing. Participants are requested to complete a short structured summary addressing two questions: (1) What did I learn about myself during the session (from the activity/others)?; (2) What did I learn about others in the group? In the group discussion participants share one meaningful insight from the assignment. Finally, each participant sets a “mini-goal” for practice during the week, such as reflecting on specific executive deficits (e.g. impulsivity) in their daily occupations at the end of the day, trying out a cognitive functional strategy at work or in the group, or planning a social activity. The last component, Summary, includes a review of the main themes that were discussed during the session.
Participants
Five adults with ADHD were recruited, three females and two males. The inclusion criteria were: (a) valid diagnosis of ADHD from a certified medical expert; (b) score >64 (clinical cutoff) on one or more scales of the Behavior Rating Inventory of Executive Function–Self-Report (BRIEF-A; Roth and Gioia (2005)), which indicates a significant difficulty in EF; (c) over the age of 18 and (d) fluent Hebrew speaker. The exclusion criteria were: diagnosis of severe neurological and/or psychiatric disorders based on self-report. The participants were recruited using convenience sampling through advertising on social networks. Considering the fact that the study was conducted on Zoom, there were technical constraints in relation to the number of participants. In order to support meaningful interpersonal processes via Zoom on the computer screen, the number of participants was limited to five persons.
Measures
Demographic questionnaire
A questionnaire was constructed for the study that includes personal details such as gender, age, education, marital status, residence, diagnosis of ADHD and health status.
Feasibility measures
Recruitment, retention and adherence
Information regarding the number of eligible participants, recruitment procedure and retention was documented in therapist logs. Good adherence was considered as participation in 80% of the sessions and completion of all questionnaires pre and postintervention.
Potential effectiveness
Behavior Rating Inventory of Executive Function for Adult’s
The BRIEF-A (Roth and Gioia, 2005) is a self-report questionnaire for adults that evaluates EF in everyday situations. The questionnaire is composed of 75 items rated on a three-level scale (1 = never, 2 = occasional, 3 = often). The items are classified into nine scales that represent EF domains and into two indices. The first is the Behavioral Regulation Index (BRI) which consists of inhibition, shifting, emotional regulation and behavioral monitoring. The second is the Metacognitive Index (MI) which consists of working memory, initiation, planning/organization, task monitoring and organization of materials. These two indices create a summary score, the Global Executive Composite. T scores are calculated for each scale and index. A higher score indicates more difficulty with EF; a score of 65 or above indicates clinical impairment. A significant improvement in the indices is defined as an improvement of five points or more at reassessment. The BRIEF-A questionnaire was standardized on a sample of 1136 healthy adults aged 18–90, and there are norms according to age (Roth and Gioia, 2005). The BRIEF-A has moderate to high internal consistency (αs = 0.73–0.98), high test–retest stability (rs = 0.82–0.94) and moderate interrater agreement between self- and informant reports (rs = 0.44–0.68). The measure has been translated into Hebrew and has been shown to significantly differentiate between adults with and without ADHD in Israel (Stern and Maeir, 2014).
The Adult ADHD Quality-of-Life scale
The Adult ADHD Quality-of-Life scale (AAQoL; Brod et al., 2005) assesses QoL in adults with ADHD and is widely used in research and clinical settings. This self-report questionnaire consists of 29 items which are rated on a scale from 1 (never) to 5 (often), yielding a total and four scale scores (Productivity, Life outlook, Relationships and Psychosocial health) ranging from 0 to 100; higher scores indicating better QoL. A clinically significant improvement on the AAQoL is considered an eight-point change (Brod et al., 2015). The scale has good internal consistency (α = 0.93) and test–retest reliability (intraclass correlation coefficient α = 0.86) and discriminates between groups with and without ADHD (Brod et al., 2005). The AAQoL has been translate to Hebrew and found to have sound psychometric properties in the Israeli adult ADHD population (Goffer et al., 2019; Stern and Maeir, 2014).
Acceptability
Semi-structured interview
An interview constructed for the study evaluates satisfaction from the intervention and the experienced impact on participants daily functioning. The interview includes 12 satisfaction questions rated on a five-point scale (from 1 = “very small extent” to 5 = “very large extent”) regarding the group in general, structure, content, group process and changes in daily functioning. In addition, the interview includes seven open-ended questions about positive and negative aspects of the intervention, suggestions for improvement, expectations and impact on daily functioning. The interview was conducted by the first author (SGS) at the end of the intervention; the duration of the interview was about an hour.
Procedure
This study was approved by the The Hebrew University Institutional Review Board (reg. no. 10032020). Participants were informed of guaranteed confidentiality and their right to discontinue their participation at any time. All participants signed informed consent. The study was advertised on social media, interested candidates received a brief explanation of the study and questionnaires were sent via email. After confirming suitability to the study, candidates were invited to a meeting with one of the researchers to explain study procedures, confirm access and familiarity with Zoom remote platform and to sign informed consent. The intervention program included 16 weekly group sessions of 90 minutes each, conducted in the afternoon on Zoom video-conferencing. The intervention was conducted by the two researchers, who are occupational therapists qualified to treat according to the Cog-Fun protocol. At the end of the intervention, participants completed reassessment of the BRIEF-A and AAQoL as well as a semi-structured interview to assess satisfaction with the intervention.
Statistical analyses
Descriptive statistics depicting median and interquartile range were calculated on AAQoL and BRIEF outcomes before and after intervention to explore potential effectiveness. In addition, rates of clinically meaningful improvements were provided for each measure. Qualitative content analysis of the semi-structured interviews was used to examine acceptability. Data analysis followed the process suggested by Braun and Clark (2006). First, the interviews were transcribed. Next, the two researchers, separately, familiarized themselves with the data by reading it several times. Next, they generated initial codes and themes. Then, they discussed the possible themes. After agreeing on the themes, the researchers, separately identified the relevant codes for each theme. Finally, specific examples for each theme were selected to be presented in the results.
Results
Study population
Sociodemographic and clinical characteristics of the participants are presented in Table 2. The final sample consisted of five participants aged 24–29. One participant reported having been diagnosed with comorbid anxiety disorder. Three participants reported irregular medication use, and two participants reported no use of medication. All of the participants completed the intervention to the end.
Socio-demographic and clinical characteristics of the participants (N = 5).
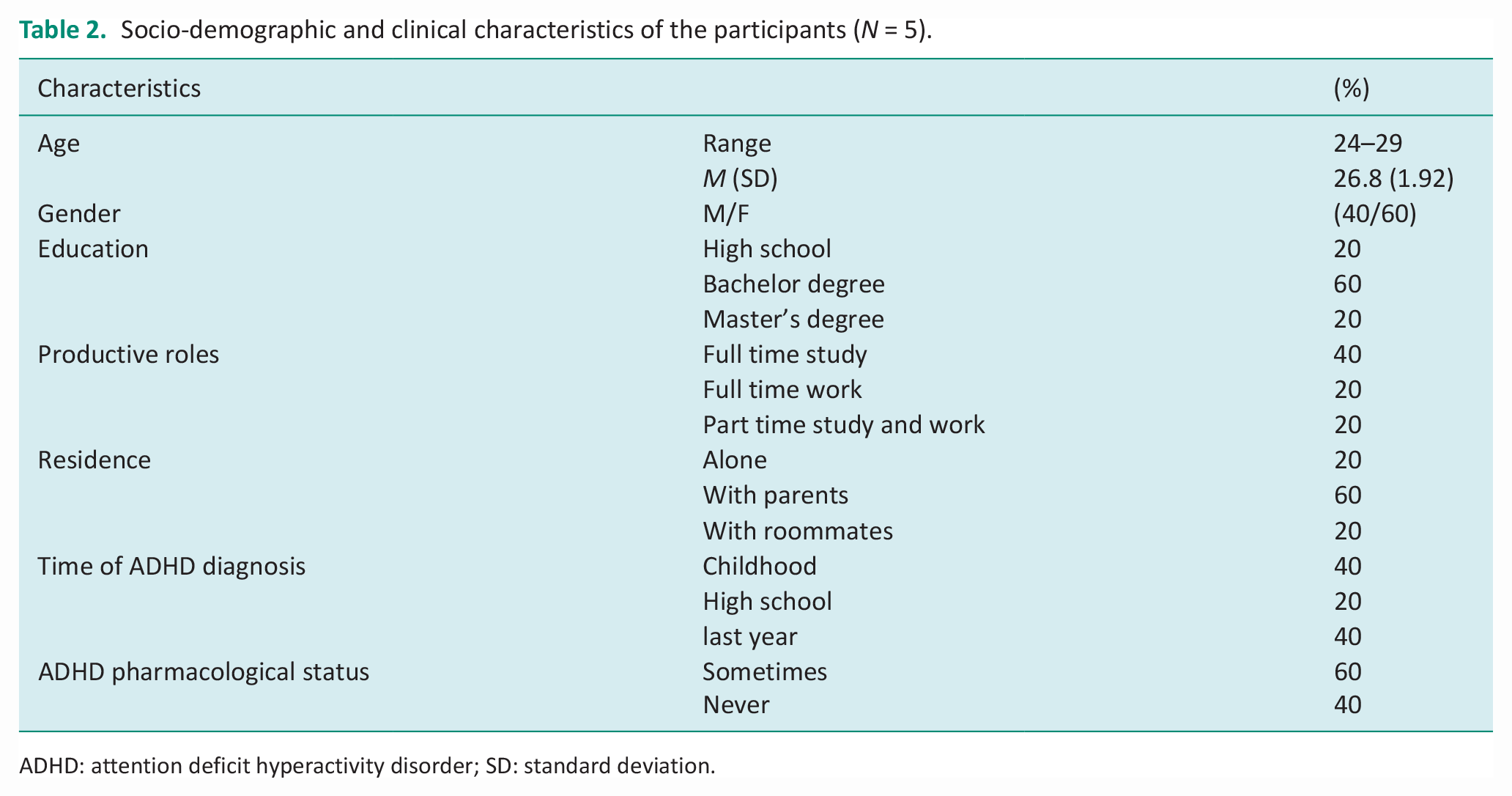
ADHD: attention deficit hyperactivity disorder; SD: standard deviation.
Recruitment, retention and adherence
Study recruitment took place in November 2020. A convenience sampling method was used and participants were recruited via social media ads. Fifteen potential participants with a valid diagnosis of ADHD were identified within a few days after the advertisement. The first five were invited to participate in the study, completed the baseline assessment and started the intervention in December 2020. All the participants completed at least 80% from the 16 weekly sessions, and all completed postintervention assessments.
Responsiveness of outcome measures
Descriptive statistics are presented in Table 3. There were a range of pre–post differences in the outcome measures. Besides the median and Interquartile Range (IQR) scores, the table delineates the frequency of participants that showed clinically meaningful improvements. Regarding the AAQoL, the highest improvement was found for AAQoL productivity scale (100%) and the lowest for Psychological Outlook and Relationships (40%). Regarding the BRIEF, the rates of clinically significant improvement were lower than that found for the AAQoL. Median change scores of the BRIEF scales were highest for Plan Organize and Task monitor scales and lowest for Inhibit.
Change in AAQoL and BRIEF-A from baseline to postintervention.
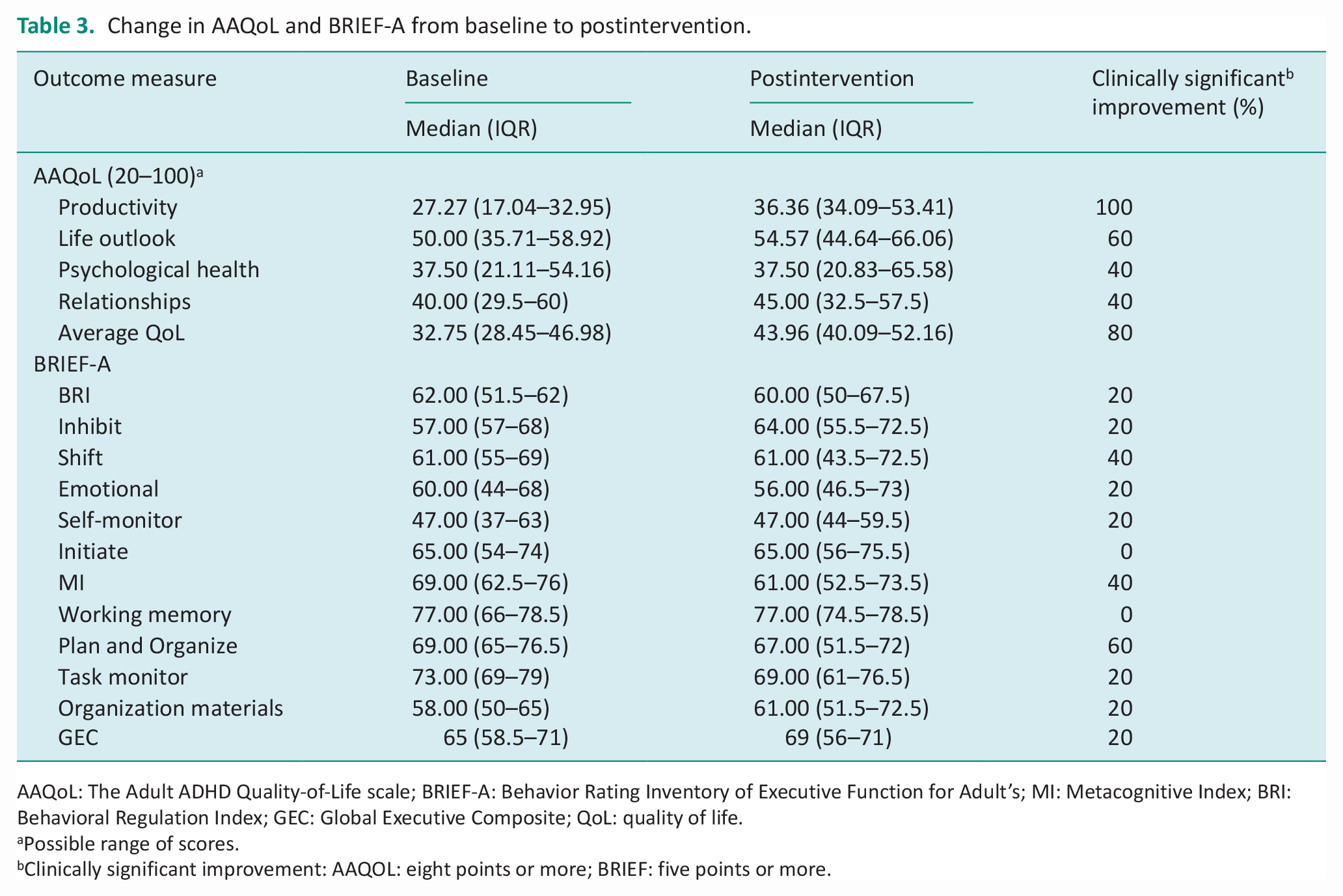
AAQoL: The Adult ADHD Quality-of-Life scale; BRIEF-A: Behavior Rating Inventory of Executive Function for Adult’s; MI: Metacognitive Index; BRI: Behavioral Regulation Index; GEC: Global Executive Composite; QoL: quality of life.
Possible range of scores.
Clinically significant improvement: AAQOL: eight points or more; BRIEF: five points or more.
Acceptability
Descriptive analysis of satisfaction from the intervention in general revealed varied results, ranging from moderate (40%) to very high satisfaction (60%), yet all participants expressed their desire to continue the treatment if possible. Additionally, all participants expressed high to very high satisfaction with the group support and that the group was a safe and enabling space for them. Finally, most participants (80%) expressed high satisfaction with the process of learning from their peers.
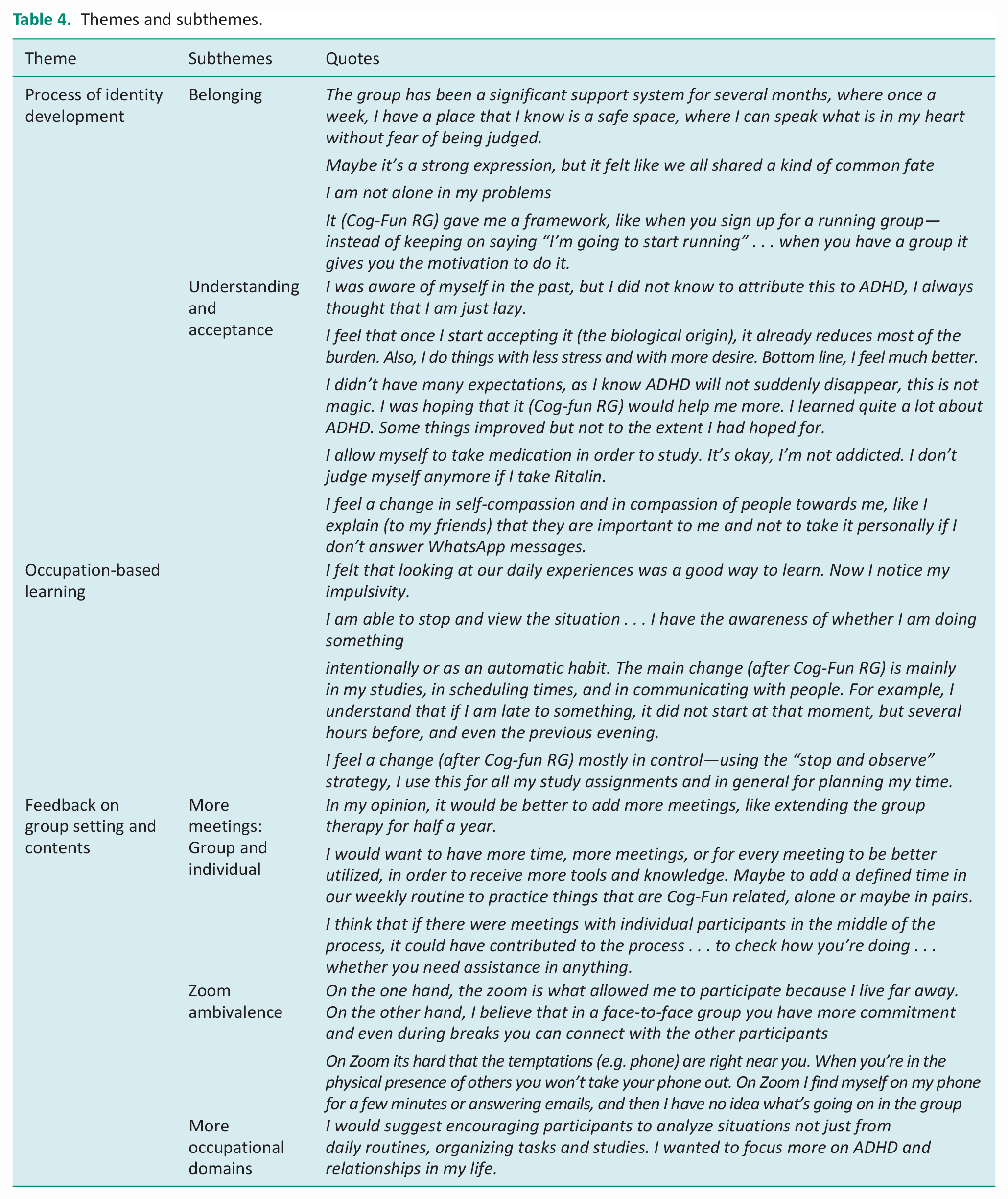
Qualitative thematic analysis of the responses to the open-ended questions revealed three main themes: (a) process of identity development, (b) occupation-based learning and (c) feedback on group setting and content. The themes, subthemes and sample quotes are presented in Table 4.
(a) Process of identity development. Several interrelated components were identified that contributed to a positive process of identity development. Firstly, participants sense of belonging to the group. This sense of belonging was fostered by experiencing the group as a safe place, where their difficulties were not judged and were similar to those of the other participants. Second, the accepting setting of the group set the stage for their own understanding and self-acceptance. An important enabling factor was the novel understanding that their challenges stemmed from their biological profile and were not related to character flaws. This biological attribution of ADHD supported coherence and justification in using medications. Finally, as they gained self-understanding and acceptance, they were more able to explain themselves and self-advocate in their social circles.
(b) Occupation-based learning. The participants described the benefits of learning from specific occupational experiences (as opposed to general, theoretical discussions about occupations). This reflective practice, monitoring specific situations in the group (referring to occupational performance experience analyses, see Table 1, unit 2), contributed to developing awareness of what actually occurs in their daily life. The monitoring strategy practiced in the group setting seemed to be transferred outside the group, as depicted by reports of acquiring a general self-monitoring strategy (stop and observe). Implementing this strategy provided a greater sense of control in various occupations, as opposed to automatic behavior without awareness.
(c) Feedback on group setting and content. The participants gave feedback on the setting and the content of the group. There was an overall experience that they wanted more therapeutic time, as in more group or individual sessions and more structured practice time in between sessions. This request for additional time relates to the feedback on content whereby participants expressed a need for more knowledge and tools and addressing more occupational domains (such as social participation). Regarding the remote setting, participants listed both advantages and disadvantages of the Zoom format. On the one hand, this format enabled participation from distant areas, was less demanding on time resources and was suitable for distancing requirements during the COVID-19 pandemic. On the other hand, the home and the computer setting present many tempting distractions and pose barriers to persistent engagement in the therapy session.
Themes and subthemes.
Discussion
The purpose of this study was to examine the feasibility of Cog-Fun RG in terms of: (a) recruitment, retention, adherence and acceptability; and (b) responsiveness of potential outcome measures in preparation for a controlled study. Feasibility was supported, and clinically significant gains were found in the QoL measure and, to a lesser degree, in the EF measure. Qualitative findings pointed to three main themes: (a) process of identity development, (b) occupation-based learning and (c) feedback on group setting and content. These encouraging results provide a foundation for further development and study of the Cog-Fun RG intervention for adults with ADHD. Following is a detailed discussion of the study outcomes.
Responsiveness
The results of the AAQoL questionnaire showed high rates of clinically significant improvements in the productivity scale and the total score. Baseline scores revealed low self-reported QoL in line with the literature, which shows that adults with ADHD report lower QoL than typical adults (Agarwal et al., 2012; Stern et al., 2017). Considering the centrality of QoL as a significant outcome in healthcare (Kim, 2020), the clinically significant improvements in AAQoL are noteworthy. The scale with the lowest rate of improvement was the “Relationship” scale. This trend was also found in a recent Cog-Fun A pilot study (Kastner et al., 2022) and may be explained by the greater focus on productivity and self-care than on the social domain. Furthermore, the qualitative findings confirmed that participants experienced the intervention as too highly focused on “daily routines, tasks and studies” and expressed a need to increase the focus on their social participation.
The changes in EF were examined according to the two main indices of the BRIEF self-report questionnaire. Overall, the BRI median scores were lower (less EF impairment) than the MI scores at baseline, and demonstrated lower rates of clinical improvement after the intervention. These findings may be related to previous studies showing that adults with ADHD self-report more severe impairments in metacognitive EF, such as working memory, planning and organizing comprising the MI, compared to reporting less impairments in the emotional and behavioral regulation aspects of EF as represented by the BRI (Stern and Maeir, 2014). In the qualitative findings, participants reported that due to the intervention, they were more aware of EF impairments such as impulsivity and emotional dysregulation (“Now I notice my impulsivity”). Accordingly, there may have been a baseline “bias” toward more self-report of impairments in the MI scales. Furthermore, the apparent increase in awareness of behavioral dysregulation supports the finding whereby the “inhibition” scale showed the highest increase in self-reported impairment, whereas the “planning and organization” scale showed the highest decrease in self-reported impairment (i.e. improved EF function). There is a possibility that the intervention may positively reduce EF impairment, especially in the metacognitive aspects of EF as measured by MI. In addition, the intervention may promote awareness of behavioral regulation EF impairment. According to metacognitive principles, awareness is a prerequisite for strategy acquisition supporting everyday functioning (Toglia, 2018). Thus, it may be suggested that an additional measure of awareness be incorporated in the research protocol. Moreover, perhaps the intervention should be extended to leverage the improved awareness of behavioral regulation aspects of EF in daily life as an impetus for functional improvement. Compared to other nonpharmacological intervention for adults with ADHD that measured effectiveness on ADHD symptoms and psychological outcomes (Fullen et al., 2020; Nimmo-Smith et al., 2020), the outcomes of this study were designed to reflect the cognitive functional outcomes expected from an OT Cog-Fun intervention.
Acceptability
Satisfaction from the intervention was moderate to very high according to quantitative measures. However, the qualitative analyses enable a deeper understanding of the participants individual experiences. The findings suggest that the intervention may have played a role in “recovery” oriented processes of developing an occupational identity of a person living with ADHD, who is able to reflect on their occupational experiences and intentionally use strategies to support their participation. This resonates with the Model of Human Occupation and a recent study on occupational identity among adults with ADHD, stressing the need for interventions that promote this aspect of occupational adaptation (Paley Altit et al., 2019).
All participants described the group as a safe place and a powerful resource for learning and growth. The subtheme of belonging that was described by the participants expresses the significance of the relationships that connect the participants to each other and to the group itself. According to Yalom, group cohesiveness in a group intervention is the equivalent of the therapeutic relationship in an individual intervention (Yalom and Leszcz, 2005). Additional TFs are interpersonal learning and universality. Accordingly, the qualitative findings revealed that a positive facet of the group was the opportunity for learning from each other, as well as feeling that “we have a common fate and I am not alone in my problems,” representing universality, which also helps to reduce the stigma of ADHD. The sense of belonging that was fostered in the group may have contributed to self-acceptance and self-advocacy toward others, as depicted in the subthemes. Developing an understanding of the biological underpinning of ADHD and being able to attribute difficulties to a biological source emerged as a powerful mechanism in self-acceptance. (“I am not messed up” “before the Cog-Fun RG I always thought that I am just lazy”) This finding of negative misattribution of challenges (prior to intervention) is supported in the literature, as it negatively impacts the occupational identity of individuals with ADHD and contributes to social and self-stigma (Maeir et al., 2018). Self-understanding and acceptance are necessary prerequisites for advocating for oneself in society and also for engaging in a learning process. This learning process was reflected in the second theme of occupation-based learning. Here participants reported that linking learning to occupations supported online awareness and acquisition of cognitive functional strategies which contributed to their daily functioning.
These findings are in line with the multi-context treatment approach (Toglia, 2018) as well as research showing that the use of strategies had a positive impact on functioning in employment, education and parenting of adults with ADHD (Kysow et al., 2017). The participants also mentioned that learning from their own occupational experiences as well as those of their peers, was beneficial to them. These findings are similar to a previous study of Teen Cog-Fun for adolescents with ADHD, whereby the discovery of strategies through reflecting on specific occupational experiences was more beneficial than “suggestions” made by parents or by therapists (Levanon-Erez et al., 2019).
Importantly, these recovery aspects addressed above need to be considered from a realistic perspective, taking the chronicity and persistence of challenges into account. Along with understanding and self-acceptance, participants described the disappointment of discovering that they are still coping with challenges daily and that ADHD will not go away. This theme resonates with the conceptualization of the recovery journey in chronic mental health conditions, as a dynamic, nonlinear process with “ups and downs” (Doroud et al., 2021).
Feedback on group setting and content was the final theme that emerged from the qualitative analyses and included aspects relating mainly to “a need for more,” for example, more time, more individual attention, more structured practice, more tools and more occupational domains. This feedback may be considered in future protocol modifications; however, these suggestions should also be considered in terms of their potential negative impact by increasing effortfulness and dropout. In addition, adding individual therapy sessions may be helpful for monitoring each participants process, yet may also impede the group process. Thus, further research is required in order to examine the effectiveness of the intervention prior to recommending protocol changes. Regarding the remote Zoom format, feedback showed that the use of a virtual environment for the intervention was both a promoting and limiting factor. The participants described that there were more distracting stimuli due to the use of Zoom, which led at times to a lack of focus during sessions. On the other hand, the use of Zoom enabled participants to participate from different geographical areas, as well as during times of social interaction restrictions as imposed by the COVID-19 pandemic (Daigle and Rudnick, 2020). In addition, considering the difficulties in time management, which are characteristic of adults with ADHD, the remote intervention may have reduced the burden of managing limited time resources. Furthermore, regarding the group interpersonal processes, the use of the Zoom platform did not appear to be a barrier in the group process as well as the specific Cog-Fun RG content. Future controlled studies may compare the advantages and disadvantages of Cog-Fun RG versus face-to-face
Study limitations
This study has several limitations. Firstly, the sample was small and the age range of the participants was small. Secondly, we did not conduct a follow-up assessment. In preparation for a future controlled trial, the study would have benefited from a more diverse and larger sample, and from adding a long-term assessment. Finally, this study provides preliminary evidence regarding the feasibility of Cog-Fun RG intervention within a research setting and cannot speak to the extent to which findings would generalize to the clinical, community-based practice settings.
Conclusion
This study supported the feasibility of Cog-Fun RG among adults with ADHD in terms of recruitment, adherence and acceptability. Quantitative findings point to the responsiveness of the AAQoL to the intervention. Qualitative findings suggest gains in identity development, awareness and acquisition of cognitive functional strategies through occupation-based learning in a telerehabilitation group therapy format. Further controlled studies are warranted.
Implications for occupational therapy practice: Key findings
Group telerehabilitation is feasible for adults with ADHD. Remote delivery enables participation yet also may involve challenges in coping with distractions.
Participation in Cog-Fun RG may enable positive identity development, awareness and acquisition of cognitive functional strategies and clinically significant improvements in QoL.
Cog-Fun RG requires further research to examine its effects on these outcomes.
What this study adds
Group telerehabilitation is feasible for adults with ADHD and may benefit in terms of awareness, identity, strategies and QoL. However, further controlled studies of Cog-Fun RG in community settings are required.
Footnotes
Acknowledgements
Adi Maoz, Efrat Ben-naeh, Jennifer Budman, Ifat Velder-Shukrun, Dana Zeides-Taubin, Mayan Cohen, Stav Levy, Orit Fisher, Nirit Levanon-Erez and Ruthi Traub, for their feedback on the protocol development.
Research ethics
This study was approved by the Hebrew University Institutional Review Board (reg. no. 10032020), the year 2020. All participants signed informed consent.
Patient and public involvement data
During the development, progress, and reporting of the submitted research, Patient and Public Involvement in the research was included in the conduct of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Supported by the Yuval Lester memorial fund.
Contributorship
Equal contributorship.