
Abstract
Background:
Hypertension (HTN) is a leading lifestyle disease and a major cause of morbidity and mortality worldwide, especially in sub-Saharan Africa. Clinical practice guidelines (CPGs) serve as useful tools for clinical decision-making by leading clinicians to measure appropriateness and ultimately measure the quality of care and reduce clinical inertia.
Objectives:
This study aimed to assess prescribers’ awareness, adherence to CPGs, barriers to it, and its associated factors among prescribers working at public hospitals in Northwest Ethiopia.
Design:
A multicenter explanatory sequential mixed-methods study was conducted between October 01, 2023 and January 30, 2024.
Methods:
STATA version 17.0 was used for analysis, following entry of data into EpiData (version 4.6.0.0). Adherence of prescribers to HTN CPGs was determined using the scoring system results of the JNC 7 adherence scale. Associations between variables were assessed by the Chi-square (χ2) test. An adjusted odds ratio (AOR) with 95% CI with a p-value <0.05 was considered statistically significant in multivariable logistic regression analysis.
Results:
In the present study, out of 403 prescribers approached, 370 completed the interview, resulting in a response rate of 91.8%. Most of the prescribers (90.5%) were aware of HTN CPGs. More than one-third (41.1%) of the prescribers were low adherent to the HTN CPGs. Prescribers with 1–5 years (AOR = 3.22, 95% CI = 1.27–8.15) and 6–10 years (AOR = 4.59, 95% CI = 1.62–11.05) of experience; the availability of resource in the hospital (AOR = 1.78, 95% CI = 1.11–2.87), and qualification, with general practitioners (AOR = 2.98, 95% CI = 1.46–6.10) and nurses (BSc and above) (AOR = 7.29, 95% CI = 3.55–10.91) were significantly associated with high adherence to CPGs. The qualitative part of the study identified barriers to HTN CPGs, including limited resources, patient influence, and complexity of the guidelines. Participants recommended improving access, updating and simplifying CPGs, and enhancing institutional support.
Conclusion:
More than one-third of the prescribers were low adherent to CPGs. Continuous training and education in terms of using evidence-based therapeutic guidelines is crucial in patient care and reduces clinical inertia. To promote excellence in clinical practice, concerted efforts are needed to promote application of evidence-based HTN treatment guidelines.
Plain language summary
High blood pressure (hypertension) is a major public health issue, especially in Sub-Saharan Africa. Following clinical practice guidelines is important to improve patient care. This study assessed at how prescribers in public comprehensive specialized hospitals in Northwest Ethiopia are following clinical practice guidelines during management of high blood pressure. Out of 370 prescribers, most knew about the clinical guidelines, but over half were not fully following them. Factors like work experience, qualification, and resources availability were associated with adherence to clinical practice guidelines. Interviews with some prescribers also revealed challenges like lack of access to medicines, patient pressure, and complex guidelines. They suggested better access, regular training, and simpler clinical guidelines to help improve patient care. Overall, more support is needed to help prescribers use clinical practice guidelines consistently in treating high blood pressure.
Introduction
Hypertension (HTN) is a global public health problem. 1 In sub-Saharan Africa (SSA), it is currently considered to be one of the main causes of morbidity and mortality. 1 Despite this, public health responses to the epidemic are mainly inadequate. Numerous governments in the region are behind schedule in putting high blood pressure control and awareness programs into place for the entire population, including high-risk groups.2–4 The number of hypertensive patients worldwide is estimated to be over one billion, and by 2025, it is predicted to reach 1.56 billion, marking a roughly 60% increase from 2000.5,6 Every year, HTN and its complications cause about 9.4 million deaths. 7 HTN has also been attributed in recent years to approximately 50% of deaths from heart disease and stroke cases.8,9 In SSA, cardiovascular diseases, including HTN, are the main causes of death.10–12
Evidence-based medicine is the cornerstone of safe medical practice. Evidence-based practice reduces unnecessary costs, enhances patient outcomes, and establishes a benchmark for enhancing patient treatment outcomes in the future. 13 Clinical practice guidelines (CPGs) are evidence-based statements endorsed by a systematic review and an assessment of the merits and demerits of alternative care options with recommendations to optimize patient care. 14 CPGs aim to improve patient care by promoting beneficial interventions and discouraging ineffective or harmful ones. 15 Even though there is varying adherence to CPGs, existing evidence demonstrates that following therapeutic guidelines improves treatment outcomes. 16
Worldwide, numerous CPGs have been issued for HTN treatment to be used as reference criteria for prescribers. 17 The most recently published CPGs for HTN treatment are the Joint National Committee (JNC 8). 18 Despite the development and issuance of CPGs, many prescribers still treat hypertensive patients according to their preferences and clinical experience.19,20 Adherence to CPGs and standards is required to make sure point-of-care testing is safe, clinically acceptable, and affordable. 21 Reporting and Learning from Best Practice guidelines is a “landmark initiative” in the WHO World Alliance for Patient Safety 2021–2030 to reduce the global burden of avoidable medication-related harm. 22 The central role of CPGs is to help prescribers make better decisions. Non-adherence to CPGs is believed to contribute significantly to poor delivery of clinical care and, hence, poor treatment outcomes. 23
The Government of Ethiopia (GOE) is working to fortify the healthcare system to adjust it to the Sustainable Development Goals and is confronting an increase in non-communicable diseases, including hypertension. The GOE is implementing a plan to transform the Ethiopian Food and Drug Authority (EFDA) to make its operations more efficient with the aim of ensuring 100% availability of vital and essential medicines at all levels of the healthcare conveyance system without stock deficiencies. 24 The GOE developed guidelines on clinical and programmatic management of major non-communicable diseases, including HTN, on June 10, 2016, and standard treatment guidelines (2021), which are readily available in all hospitals in Ethiopia.25,26 Ethiopia had not established clinical governance, which is defined as the system through which healthcare organizations are responsible for improving health service quality through adherence to CPG, 27 despite the above-mentioned activities done to improve the healthcare system.
Extensive efforts are required to build, clearly define, and raise prescribers’ awareness about clinical governance in developing countries.10,28,29 In Ethiopia, this is the first documented study that measures awareness and adherence of prescribers to HTN guidelines in line with the local and international guidelines. This study is of great importance in providing baseline data on non-adherence to the CPGs, the causes, and possible solutions to address this challenge (non-adherence to CPGs) in health care and policymakers in developing appropriate evidence-based strategies and implementing appropriate health programs for the public. Improving CPG adherence has the potential to optimize the treatment of HTN, reduce the burden of HTN-related complications, and ultimately improve patient outcomes. Therefore, this study aimed to assess prescribers’ awareness, adherence to CPGs, barriers to it, and associated factors among prescribers working at comprehensive specialized hospitals in Northwest Ethiopia.
Methods
Study period, design, and settings
Between October 01, 2023 and January 30, 2024, a multicenter explanatory sequential mixed-methods study was conducted to evaluate the prescribers’ awareness, adherence to clinical practice guidelines for the management of HTN, suggestions of prescribers for future use, barriers to it, and associated factors in Northwest Ethiopia. In the northwestern Amhara region, there are five public comprehensive specialized hospitals (CSHs), which include Debre Markos, Tibebe Ghion, Felege Hiwot, Debre Tabor, and the University of Gondar. The University of Gondar CSH is located 750 km northwest of Addis Ababa, and the hospital serves more than 7 million people in the Amhara region. Debre Tabor CSH, which is located at a distance of 667 km from the capital city, Addis Ababa, and 104 km from Bahirdar City, provides services for more than 3 million people in the area. Felege Hiwot and Tibebe Ghion CSHs are located in Bahir Dar City, the capital of the region, which is 565 km from Addis Ababa, and the hospital serves about 5 million people. Debre Markos CSH is located 300 km from Addis Ababa and provides service for an estimated population of 5 million.
The quantitative component used a hospital-based interviewed based questionnaire to assess prescribers’ awareness, adherence to CPGs, and its associated factors among prescribers working at CSHs in Northwest Ethiopia. The qualitative component adopted an interpretive phenomenological approach to explore underlying barriers that hindered prescribers from adhering to CPGs from the perspectives of healthcare providers and their recommendations.
Source population and study population
The population source was all prescribers working at CSHs in Northwest Ethiopia. The study population comprised all prescribers who were available at work in the respective CSHs during the data collection period.
Eligibility criteria
For quantitative component of the study, all prescribers available at work during the data collection period, and prescribers who have been working at the CSHs for at least 6 months to ensure familiarity with the prescribing practices were included in this study.
Prescribers who were on leave or otherwise unavailable during the data collection period, and prescribers who refused to consent to participate in the study were excluded from the study.
For the qualitative component of the study, healthcare providers at CSHs in Northwest Ethiopia who were selected as key informants were included and healthcare providers who were unwilling to participate as volunteers or who did not possess sufficient detailed information.
Sample size and sampling technique
The sample size was determined by using a single population proportion formula with the assumption of a 95% confidence level, 5% margin of error, and P = 50.0%, the estimated proportion of prescribers’ adherence to local and international CPGs is not known in Ethiopia to the best of a literature search of the authors. Therefore, n = [(Z1 − α/2) 2 * p * (1 − p)]/d2, n = [(1.96)2(0.5) (1−0.5)]/(0.05)2 = 384; by using a contingency of 5%, that is, 384*5% = 19; the calculated sample size was 384 + 19 = 403. Where d = margin of error, p = proportion of sample population, Za/2 = the value under a standard normal table using a 95% confidence interval, and n = the total sample size. However, since the total population in our study was <10,000 (2600), we recalculated the sample size using the correction formula: Nf = n/(1 + n/N), where Nf was the actual sample size using the correction formula, n was the minimum sample size (403), and N was the actual population size (2600). By substituting these values into the formula, we found that Nf was equal to 349. Additionally, considering a 5% contingency for non-response rate, the minimum sample size required for this study was 366. Finally, we decided to approach the minimum sample size determined using a single population proportion formula (403), intentionally to increase the power of the study. However, during data collection, 33 prescribers declined to participate, resulting in a final sample size of 370, which is not below the target sample size determined using the correction formula (366). Despite the high non-response rate, this sample size, which is above the target, provides sufficient data to support meaningful analysis and conclusions. Prescribers were involved in this study using the convenience sampling technique. The sample size for the qualitative part was not computed. The data were collected until the information for the study was saturated.
Key informants were selected purposively to ensure the inclusion of healthcare providers. This targeted approach allowed for a deeper exploration of the insights related to barriers that hindered prescribers from adhering to CPGs.
Operational definitions
Clinical practice guidelines: CPGs are a document that has paramount importance in guiding clinical decisions, ease of diagnosis, and treatment optimization in healthcare. In this particular study, CPGs are related to therapeutic guidelines for the management of HTN. 30
Prescriber: The person who is licensed or authorized to write/prescribe medications to humans and or animals, in this study, prescribers mean physicians (general practitioners and specialists) and nurses (BSc and above). 31
The adherence assessment was conducted using a reviewed and modified JNC 7 adherence tool, which consisted of 18 criteria related to hypertension CPG recommendations. Each criterion was weighted and coded as either 1 or 2, depending on the relative importance of the item being assessed. A total possible score of 29 was obtainable from the 18 items. Adherence levels were classified using percentage thresholds: low adherence: <60% (corresponding to a total score of 0–17), 32 and high adherence: ⩾60% (corresponding to a score of 18–29). 32
Hypertension: According to guidelines from the American College of Cardiology (ACC) and the American Heart Association (AHA), normal blood pressure: <120/80 mmHg, elevated: systolic between 120 and 129 mmHg and diastolic <80 mmHg, hypertension (Stage 1): systolic 130–139 mmHg or diastolic 80–89 mmHg, hypertension (Stage 2): systolic ⩾140 mmHg or diastolic ⩾90 mmHg, and hypertensive crisis: systolic ⩾180 mmHg and/or diastolic ⩾120 mmHg. 33
Data collection tool preparation and procedures
A self-administered questionnaire was used to collect the data from study participants. Following a review of the existing literature, a questionnaire was prepared.5,11,18,20,23,34,35 Initially, the questionnaire was prepared in English and reviewed by experts in this area for its consistency. An expert with bilingualism was also appointed for translation into Amharic, the local language, and it was translated back into English to check consistency. To ensure the questionnaire’s quality, it was face-validated for its content by medical practitioners and two clinical pharmacists with expertise in the field. Then, a pretest was conducted on 5% of the prescribers (20 prescribers) at a hospital not included in the main study. After having a full day of training about the questionnaire and ethical issues, data collectors (clinical pharmacists) collected both the pretest and the main research article data. Study participants were informed of the study’s objectives before participating. Cronbach’s Alpha reliability test was done to measure the reliability of the study participants’ answers to the questionnaire, which yielded 0.74, an acceptable range.
We determine the adherence of prescribers using a modified JNC 7 adherence tool, 32 and by having modifications after review by a panel of experts in the field, including internists and senior clinical pharmacists. Following a consensus review by a panel of experts, the original hypertension clinical practice guideline framework, based on the JNC 7 recommendations, was adapted to align with the local healthcare context and the specific objectives of the study. In the Ethiopian context, the JNC 7 adherence tool was adapted, and the adaptation process aligned with the principles outlined by the ISPOR Task Force for Translation and Cultural Adaptation, though with certain tailored modifications suited to the study’s specific needs and resource constraints. English is the primary language of medical education and practice in Ethiopia, particularly among prescribers. Therefore, the tool maintained its original English language format. The tool underwent cultural adaptation to ensure it reflected Ethiopian clinical realities, such as the availability of medications, follow-up practices, and diagnostic protocols in local healthcare settings. A panel of local clinical experts (internists and clinical pharmacists) reviewed the tool for clinical relevance and feasibility. A panel of local experts (physicians and clinical pharmacists) reviewed the tool to assess content relevance, clarity of wording, and feasibility in the Ethiopian setting. Feedback from a panel of local experts informed minor adjustments, ensuring the instrument was contextually appropriate.
Overall, a total score of 29 was obtained based on the 18 criteria. Classification of adherence was made as low adherence for those scoring a value of <60% (total score ranged from 0 to 17) and high adherence with a scoring value of ⩾60% (score from 18 to 29). The reviewed and modified JNC 7 adherence measuring tool included 18 criteria, which were coded either 1 or 2 based on the level of importance of the outcome being measured in the tool, which is found within the questionnaire, which is uploaded as Supplemental Material.
Qualitative component
Data were collected through in-depth interviews using a semi-structured interview guide. An interview guide was developed by the investigator, focusing on health care professionals’ experiences on barriers that hindered prescribers from adhering to CPGs. The interview guide was translated into Amharic to facilitate better communication with the participants. The interviews lasted approximately 45 to 60 min. Interviews were conducted from January 11 to 30, 2024, and were audio recorded after obtaining verbal consent from participants. The interviews were held in private and convenient locations to encourage open dialogue by a researcher with a Master of Clinical Pharmacy and training in qualitative data collection, including in-depth interviewing techniques. The interviewer has prior experience conducting interviews with healthcare providers and patients. He has no history of any personal relationship with participants. Notes were also taken to complement the recordings. Data collection was continued until thematic saturation was reached, meaning no new themes or insights emerged from additional interviews. The interviewer stopped when three interviews in a row did not give any new codes or topics, and when everything already had seemed solid and complete. Through this procedure, the interviewer was able to decide that data collection could end because more interviews were unlikely to yield new insights. All the participants were volunteers throughout the interview time. This study was conducted and reported based on the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist of 32 items. 36
Management of data quality, entry, and statistical analysis
The collected data were entered into STATA version 17.0 and were analyzed after being checked for completeness and consistency. Q-Q plot and histogram tests were used to test the normality of continuous variables. Descriptive statistics were used, and data were presented as frequencies and percentages (%; n) for categorical data, or the median for continuous variables. Multicollinearity among predictor variables was checked by using the variance inflation factor, and collinearity was not found. Associations between variables were assessed by the Chi-square (χ2) test. In the bivariate analysis section, all independent variables with a p-value <0.25 were chosen to be part of the final multivariable logistic regression analysis model. An adjusted odds ratio (AOR) with 95% CI with a p-value <0.05 was considered statistically significant.
Qualitative component: Audio recordings from the interviews were transcribed verbatim, which was checked by returning to the participants, translated and analyzed thematically. By using Open Code software (version 4.03), translates are read line by line. Initial codes were generated by labeling the most commonly shared statements by the participants related to factors associated with prescribers’ adherence to CPGs through two coders. Key themes and subthemes were generated, reflecting patient-, provider-, and system-level barriers.
Trustworthiness: To ensure the trustworthiness of the study, prolonged engagement with participants was undertaken. We also checked our first results with some of them to see if they agreed. Plus, we kept track of all our choices during the study. The team was also aware of its own biases and tried to keep them in check.
Results
Sociodemographic characteristics of the prescribers
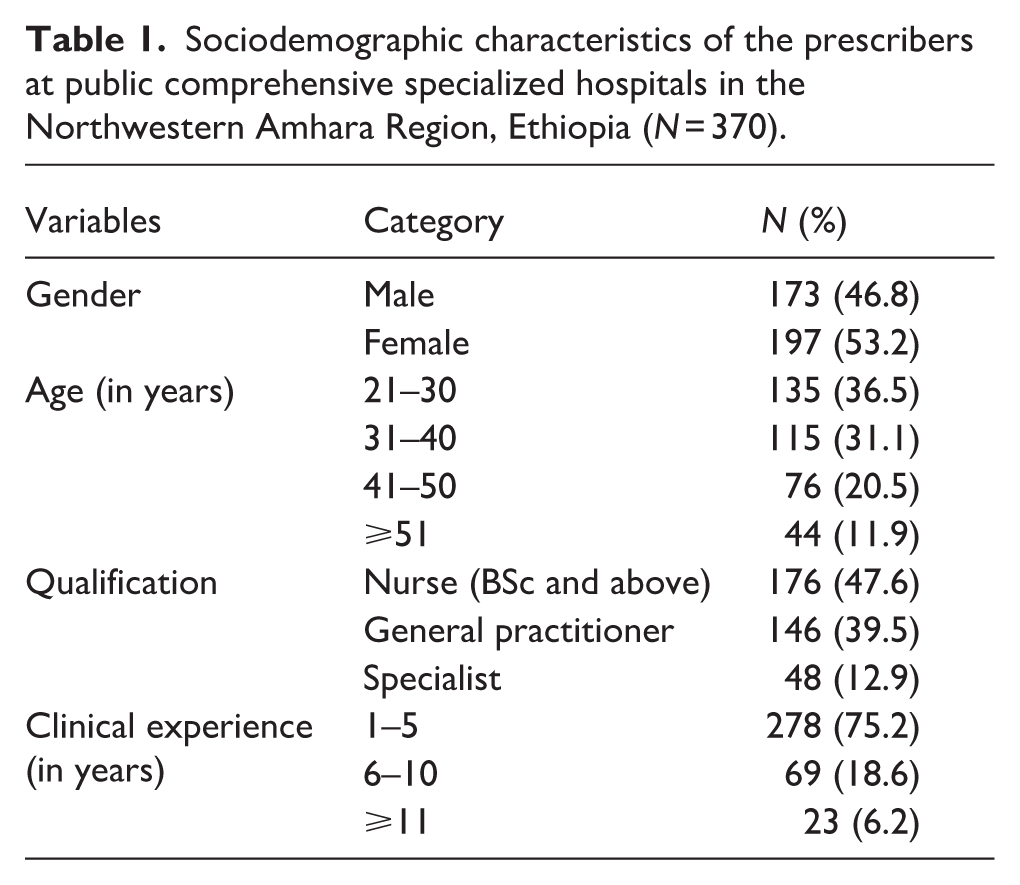
In the present study, out of 403 prescribers approached, 370 completed the interview, resulting in a response rate of 91.8%. More than half of prescribers were females (53.2%), the median (IQR) age of prescribers was 35 (16), and nearly one-third of them (36.5%) were under the age category of 21–30 years. The majority of the prescribers (47.6%) were nurses (BSc and above), followed by general practitioners (39.5%). Regarding clinical experiences, the majority of prescribers (75.2%) were below 6 years of working experience (Table 1).
Sociodemographic characteristics of the prescribers at public comprehensive specialized hospitals in the Northwestern Amhara Region, Ethiopia (N = 370).
Prescribers’ awareness and adherence to HTN CPGs
The majority of the prescribers, 90.5% (335/370), were aware of HTN CPGs, and about 80.9% (271/335) used CPGs for managing HTN. Of those prescribers using the CPGs, 59.9% (127/271) reported following updated HTN CPGs, and more than half of prescribers reported that 56.8% (210/370) were aware of the Ethiopian HTN CPGs (Table 2). The majority of prescribers, 68.4% (253/370), revealed that they refer to CPGs daily, followed by every week, 14.6% (54/370) (Figure 1). Adherence of prescribers to HTN CPGs was determined by using the Scoring system results of the JNC 7 adherence scale, and over one-third of prescribers (41.1%), were low adherent to the HTN CPGs (Figure 2).
Prescribers’ awareness and adherence to CPGs for the management of hypertension at public comprehensive specialized hospitals in the Northwestern Amhara Region, Ethiopia (N = 370).

HTN: hypertension; CPG: clinical practice guideline.

Prescribers’ frequency of clinical practice guidelines use for management of hypertension at public comprehensive specialized hospitals in the Northwestern Amhara Region, Ethiopia (N = 370).

Prescribers’ adherence to clinical practice guidelines for management of hypertension at public comprehensive specialized hospitals in the Northwestern Amhara Region, Ethiopia (N = 370).
The association of variables with adherence to HTN clinical guidelines
In the present study, the association of variables with the prescriber’s adherence to HTN clinical guidelines; duration of clinical experience (χ2 = 11.269, p = 0.004), the availability of resources used for the provision of clinical service in the hospital (χ2 = 4.962, p = 0.026), and qualifications of prescribers (χ2 = 9.297, p = 0.010) were among variables associated with prescribers adherence to CPGs (Table 3).
The association of variables with the adherence to HTN clinical guidelines at public comprehensive specialized hospitals in the Northwestern Amhara Region, Ethiopia (N = 370).

HTN: hypertension; CPG: clinical practice guideline.
CPGs followed by prescribers
The most commonly followed CPGs by prescribers were the Joint National Committee (JNC) HTN clinical practice guideline (39.62%) and the National Institute for Health and Clinical Excellence (NICE) clinical practice guideline (23.58%), and the Ethiopian NCD, 2016/STG, 2021 (16.98%) (Figure 3).

Commonly followed clinical practice guidelines by prescribers for the management of hypertension at public comprehensive specialized hospitals in the Northwestern Amhara Region, Ethiopia (N = 370).
Factors associated with prescribers’ adherence to CPGs
Multivariable logistic regression analysis showed associations between the duration of clinical experience and adherence to CPGs among prescribers at Public CSHs in the Northwestern Amhara Region, Ethiopia. Prescribers with 1–5 years (AOR = 3.22, 95% CI = 1.27–8.15) and 6–10 years (AOR = 4.59, 95% CI = 1.62–11.05) of experience; the availability of resource in the hospital (AOR = 1.78, 95% CI = 1.11–2.87), and prescriber qualification was significantly associated with adherence to CPGs, with general practitioners (AOR = 2.98, 95% CI = 1.46–6.10) and nurses (BSc and above) (AOR = 7.29, 95% CI = 3.55–10.91) showing higher odds of adherence compared to the reference group (Table 4).
Bivariate and multivariable logistic regression analysis of factors associated with prescribers’ adherence to hypertension clinical practice guidelines at public comprehensive specialized hospitals in the Northwestern Amhara Region, Ethiopia (N = 370).

HTN: hypertension; CPG: clinical practice guideline; AOR: adjusted odds ratio.
1.00 = a reference.
p-Value < 0.05 is considered significant.
Qualitative results
Barriers that hindered prescribers from adhering to CPGs
This study aimed to explore the barriers that hindered prescribers from adhering to CPGs and to identify potential solutions to overcome these challenges, by interviewing nine health care providers selected as key informants (Table 5). Barriers related to patients, guidelines, and the healthcare system were the primary influencing factors that were hindered prescribers from adhering to CPGs.
Sociodemographic characteristics of the participants interviewed working at public comprehensive specialized hospitals in the Northwestern Amhara Region, Ethiopia (N = 9).

Thematic areas
Identifying the barriers that hindered prescribers from adhering to CPGs were categorized with 5 themes and 14 sub-themes (Table 6).
Themes and subthemes developed from the data on barriers that hindered prescribers from adhering to CPGs.

CPG: clinical practice guideline.
Theme 1: System-related factors
Prescribers emphasized that resource and access limitations including unavailability of both CPGs and essential medicines were a major challenge to evidence-based practice. Many reported that clinical guidelines were either difficult to obtain or not readily accessible in their work settings. Similarly, shortages of essential medicines limited the ability of prescribers to implement guideline-recommended treatments, forcing them to rely on suboptimal alternatives.
Subtheme 1: Resource and access limitations
Prescribers consistently pointed out that limited resources undermine their ability to adhere to CPGs. Two key issues emerged: the lack of readily available guidelines in hospital wards and the inconsistent supply of essential medicines. Without easy access to CPGs, providers are forced to rely on memory or personal judgment, which increases variability in patient care. Similarly, when recommended medications are unavailable in hospital pharmacies, clinicians are compelled to substitute with less optimal alternatives, making it difficult to follow evidence-based recommendations.
Lack of access to CPGs
Most of the time, we don’t have the guidelines in the ward. Even if they exist, they are not easily accessible when we need them. (Participant 2, internist)
Lack of access to essential medicines
Even if the guideline recommends a certain drug, if it is not available in the hospital pharmacy, we are forced to use what is on hand, not what is recommended. (Participant 5, BSc nurse)
Subtheme 2: Workload and time constraints
Finally, lack of time due to heavy workloads and competing responsibilities was highlighted as an important barrier. Prescribers explained that limited consultation time restricted their ability to thoroughly consult and apply guidelines in daily clinical decision-making.
Lack of time
Prescribers frequently highlighted time pressure as a major barrier to guideline adherence. Heavy patient loads and limited consultation time make it difficult for clinicians to refer to guidelines during practice. Even when they are willing to follow CPGs, the fast-paced nature of service delivery forces them to rely on experience and quick decision-making instead.
We see too many patients in a day. There is no time to check the guideline for every case, even when we want to. (Participant 8, cardiologist)
Theme 2: Patient-related barriers
Another barrier identified was the influence of patients’ preferences and demands on prescribing practices. Prescribers often faced pressure from patients who requested specific medications or resisted certain treatments, which occasionally led to deviation from guideline recommendations.
Subtheme 1: Patients’ preferences
Prescribers noted that patients’ expectations and demands can influence clinical decisions, sometimes leading to deviations from guideline-recommended care. Many patients arrive with preconceived ideas about specific drugs, often based on advice from peers or information from non-medical sources. In such situations, clinicians may feel pressured to satisfy patients’ demands, even when the requested medication is not aligned with the CPG, to maintain trust and avoid conflict.
Patients’ pressure on prescribers
Sometimes patients come insisting on a drug they heard about, and if we don’t prescribe it, they feel dissatisfied. This pressure often makes us compromise the guideline. (Participant 5, internist)
Theme 3: Barriers related to characteristics of the guidelines
Prescribers noted that features of the guidelines contributed to non-adherence. Some described the guidelines as being too lengthy or overloaded with information, making them difficult to navigate during routine practice. Others felt that the guidelines were not user-friendly or adaptable to local contexts, and a few reported disagreements with certain recommendations, which reduced their willingness to consistently apply them.
Subtheme 1: CPGs overload
Prescribers expressed that the sheer volume of information contained in hypertension guidelines makes them impractical for day-to-day clinical use. In a fast-paced clinical environment, it becomes difficult to read through lengthy documents, which discourages consistent use of the guidelines: The guidelines are too bulky. In a busy clinic, it’s almost impossible to go through all the details. (Participant 7, MSc nurse)
Subtheme 2: CPGs are not user-friendly
Clinicians emphasized that the complex structure and technical wording of the guidelines make them less accessible. They explained that if guidelines were simplified such as being summarized into algorithms, flowcharts, or pocket guides they would be easier to apply in routine practice: The way the guideline is written is complex. If it were summarized and simplified, it would be easier to apply. (Participant 4, internist)
Subtheme 3: Lack of agreement with CPGs
Some prescribers reported that certain recommendations do not align with the local clinical context, resource availability, or patient population needs. This mismatch creates skepticism and leads to selective adherence, where providers may disregard recommendations, they feel are unrealistic or impractical.
Some recommendations do not fit with the reality we face here. So, we don’t always follow them. (Participant 1, BSc nurse)
Theme 4: Recommendations to improve adherence to CPGs
In addition to identifying barriers, prescribers suggested several strategies to enhance adherence to hypertension management guidelines. These recommendations targeted resource availability, capacity-building, guideline design, and institutional support.
Subtheme 1: Ensuring continuous availability of essential medicines
Prescribers emphasized that the unavailability of recommended antihypertensive drugs often forced them to deviate from guidelines. They pointed out that consistent access to essential medicines would make it easier to provide evidence-based care without compromising treatment decisions.
If the recommended drugs are always available in the hospital, it will be easier for us to follow the guidelines without compromise. (Participant 6, internist)
Subtheme 2: Regular training on CPG use
Healthcare providers noted that many clinicians lacked regular refresher sessions on hypertension guidelines. They explained that continuous professional training would strengthen their knowledge and confidence, ultimately supporting greater reliance on CPGs in clinical practice.
Many of us need refresher training on how to use the updated guidelines. Training builds our confidence to rely on them. (Participant 3, internist)
Subtheme 3: Updating of CPGs
Prescribers highlighted those parts of the current hypertension guidelines were outdated, leading to discrepancies with evolving treatment practices. They recommended that guidelines should be revised at regular intervals to remain relevant and aligned with new evidence.
Some parts of the guideline are outdated. If they are revised regularly, they will better fit the current practice. (Participant 9, general practitioner)
Subtheme 4: Improving access and availability of guidelines
Easy access to CPGs was seen as a critical enabler of adherence. Providers stressed that having printed or digital copies readily available in every ward would reduce the tendency to rely on memory or personal judgment.
Every ward should have copies of the guidelines, either printed or digital. Easy access makes a big difference. (Participant 4, general practitioner)
Subtheme 5: Simplifying and making guidelines user-friendly
Clinicians explained that lengthy and complex documents discouraged frequent use of CPGs during busy clinical hours. They suggested that simplified versions, such as flowcharts, algorithms, or pocket guides, would make the guidelines more practical for daily use.
If the guideline could be summarized in a simpler format, maybe as flowcharts or pocket guides, we would use it more often. (Participant 9, general practitioner)
Subtheme 6: Strengthening clinical governance and audit mechanisms
Participants underlined the importance of regular monitoring and evaluation to ensure compliance with guidelines. They believed that structured audits and feedback mechanisms would improve accountability and encourage more consistent application of CPGs.
There should be regular monitoring and audits to make sure we are following the guidelines. This will encourage accountability. (Participant 7, MSc nurse)
Subtheme 7: Increasing the role of clinical pharmacists
Several prescribers recommended expanding the involvement of clinical pharmacists in hypertension care. They emphasized that pharmacists’ expertise in medication management would help ensure treatments are consistent with the guideline and improve multidisciplinary collaboration.
Having clinical pharmacists working with us would help ensure that treatments are consistent with the guideline. (Participant 2, internist)
Discussion
The objective of this mixed-methods study was to assess prescribers’ adherence to hypertension HTN CPGs in Northwest Ethiopia and to determine the barriers influencing their adherence and highlight the need for interventions. It is essential to properly manage HTN by following evidence-based CPGs to prevent complications. 37 Prescriber adherence to CPGs for HTN treatment is frequently below optimal levels, leading to reduced treatment outcomes, especially in resource-limited settings, 12 and the study on uncontrolled HTN and associated factors in Northwest Ethiopia highlighted the need for interventions to improve CPG adherence and enhance the quality of HTN care in northwestern Ethiopia. 38
The findings of the present multi-center cross-sectional study provide important understandings into prescribers’ adherence to current CPGs for the treatment of HTN. In the quantitative phase, the study found that the majority of prescribers, 90.5% (95% CI: 87.1–93.1), were aware of HTN CPGs, and a significant proportion (80.9%) reported using these guidelines to manage hypertension. This high level of awareness and utilization of HTN CPGs among the study participants is encouraging and suggests that prescribers recognize the importance of evidence-based practices in managing HTN. However, only about 60% of those using the CPGs reported following the updated CPGs. This study finding was consistent with the study conducted so far,23,35,39 and somewhat in contrast with previous literature,11,40 which might be due to the study setting, sample size, or the healthcare system management of the countries. This finding indicates that while awareness and use of HTN CPGs are relatively high, there is a need to ensure prescribers are kept up-to-date with the current HTN treatment recommendations.
In our study findings, more than half, 56.8% (95% CI: 51.5–61.9) of the prescribers were aware of the Ethiopian HTN CPGs, NCD, 2016/STG, 2021.25,26 The use of locally adapted CPGs is vital to ensure recommendations are bespoke to the context of the healthcare system. 30 The finding suggests a need for the dissemination of Ethiopian HTN guidelines and the implementation of these evidence-based therapeutic recommendations. 41 Over one-third, 41.1% (95% CI: 38.4–51.8), of the prescribers revealed low adherence.
This low adherence is concerning, as it suggests many prescribers are not fully implementing evidence-based HTN treatment. Factors contributing to low adherence should be further explored, such as access to CPGs, access to essential medicines, lack of time, or other barriers. The present study result is consistent with the study conducted in South Africa, where about 48.1% of doctors were low adherent to CPGs, 20 and 46.5% in Iowa, an upper Midwestern region of the United States. 42 One reason for low adherence to CPGs might be that many prescribers still manage HTN according to their preference and clinical experience.19,20 Adherence of prescribers to HTN CPGs variation might be due to study design, health care system, continuous professional development campaign (education and training), and clinical governance. Encouragingly, the majority of prescribers (68.4%) reported referring to CPGs daily, indicating a general openness to using these resources to guide clinical decision-making. However, the fact that over 30% of prescribers use the guidelines less frequently suggests the need for interventions to promote regular CPG utilization.
The qualitative study findings provided deeper insight into these results, the study revealed barriers hindering prescribers’ adherence to CPGs for hypertension management through interviews with nine healthcare providers in Northwest Ethiopia. Key barriers identified were categorized into system-related factors (including limited access to guidelines and essential medicines, as well as heavy workloads), patient-related factors (notably patient preferences and demands), and issues inherent to the guidelines themselves (such as being lengthy, complex, and not contextually adaptable). Participants also highlighted a lack of agreement with certain CPG recommendations. To improve adherence, prescribers recommended ensuring consistent availability of essential medicines, providing regular training, updating and simplifying guidelines, enhancing access, strengthening clinical governance mechanisms, and involving clinical pharmacists in care delivery. Most of our study findings align with previous studies conducted so far. Lack of access to CPGs was the common barrier to CPG adherence for the majority of prescribers in the study conducted in Sudan. 23 Physicians’ wish to know more about the CPGs before applying them was the main barrier, according to the study conducted in Bahrain. 34 Lack of leadership and structural support in addition to prescribers’ lack of awareness of CPGs at the study in Saudi Arabia; overload of CPGs, and the perception that CPGs were not matching the needs of patients in Norway; lack of training and access in China; lack of time and unavailability of guidelines in Sweden; lack of time, followed by lack of resources in Estonia were the main barriers for prescribers from adhering to CPGs.43–48
In the present study, the multivariable logistic regression analysis revealed that prescribers’ duration of clinical experience was significantly associated with adherence to HTN CPGs. Prescribers with clinical experience of 1–5 years and 6–10 years were more likely to adhere to the guidelines compared to those with more than 10 years of experience. This finding suggests that prescribers with relatively shorter clinical experience are inclined to consult and follow evidence-based CPGs,5,11,21,45 which might be due to exposure to CPGs during their recent training or a greater sense of the importance of adhering to CPGs.
The availability of resources required for the provision of clinical services was also found to be significantly associated with prescribers’ adherence to the guidelines. This highlights the paramount importance of healthcare system resources in facilitating the use of evidence-based recommendations.16,34 Furthermore, the analysis identified prescribers’ qualifications as a significant factor associated with adherence to HTN CPGs. Both general practitioners and nurses were more likely to adhere to the guidelines compared to specialists. Due to their regular handling of common medical conditions and reliance on standardized protocols, general practitioners and nurses typically exhibit stronger adherence to treatment standards, whereas specialists, who frequently handle more difficult cases, may diverge from guidelines based on specialized judgment. Studies suggest that training may contribute to a better understanding and application of evidence-based CPGs in HTN treatment. 46 By addressing identified factors associated with CPG adherence, healthcare systems can work toward raising a culture of evidence-based clinical practice and improving the consistency and quality of HTN management.5,11,23,41
Convergence between the quantitative and qualitative strands strengthened the study’s conclusions. Quantitative findings showed that although most prescribers were aware of the hypertension CPGs, more than one-third demonstrated low adherence. A number of factors were associated with high adherence to CPGs, including having fewer years of work experience, the availability of resources in the hospital, and being a general practitioner or nurse with a BSc and above. Quantitative results were strongly supported by the qualitative study outcomes. Prescribers participated in the qualitative study revealed inadequate resources, the complexity of guidelines, and patient-related pressures as major barriers to adherence, directly aligning with the quantitative identification of resource availability and professional background as predictors of guideline adherence. The qualitative study findings recommendations moreover include, improving access to materials, simplifying and updating the CPGs, and strengthening institutional support, further reinforce the need to address the systemic and organizational factors reflected in the quantitative results. The findings of both quantitative and qualitative studies provide a consistent and complementary understanding of the determinants of CPG adherence to hypertension management. Both sets of findings emphasize the need for systemic, educational, and organizational interventions to improve adherence.
Finally, these findings align with the 2023 ESH and 2024 ACC/AHA guidelines, which emphasize accurate blood pressure measurement, early initiation of combination therapy, lifestyle changes and counseling, and structured follow-up. However, qualitative data of this study indicate challenges with implementing these recommendations due to constraints in staffing, equipment availability, and workflow organization. This shows a gap between clinical guideline expectations and real-world clinical practice in resource-limited settings like Ethiopia. A study in Turkish underscores a significant gap between emergency medicine residents’ practice and the recommendations of the 2023 ESH and 2024 ACC/AHA guidelines, which stress precise blood-pressure classification, careful evaluation of asymptomatic elevations, and use of ambulatory or home monitoring. 49 The qualitative findings further illuminate the reasons behind this variation, identifying barriers such as limited resources, patient influence, and the complexity of the guidelines. Residents highlighted the need for easier access to updated and simplified CPGs, as well as stronger institutional support, to facilitate adherence. This discrepancy between guideline recommendations and clinical practice, along with evidence linking improved blood-pressure control to reduced alexithymia and better emotional regulation, emphasizes the critical role of structured, guideline-based education and ongoing reinforcement during residency to bridge knowledge gaps and standardize hypertension care. 50
Therapeutic concordance fosters an empathetic, collaborative relationship between healthcare providers and patients, involving them in decision-making, which enhances blood pressure control and minimizes adverse drug reactions (ADRs) in patients with treatment-resistant hypertension (TRH).51,52 Improving hypertension management requires addressing barriers to concordance, including patient-related factors like knowledge gaps and cultural beliefs, as well as physician-related factors such as time constraints and communication issues, to strengthen the therapeutic alliance. 51 By improving therapeutic concordance, healthcare providers can better manage hypertension and empower patients to engage actively in their health.51,52
The integrated findings of this mixed-methods study reveal both encouraging levels of CPG awareness and persistent gaps in practical adherence, and to enhance evidence-based hypertension management, the study underscores the need for improved training, simplified guidelines, adequate resources, and strengthened clinical governance.
Strengths and limitations of the study
This study provides valuable insights into the adherence of prescribers to current CPGs for the treatment of HTN in Northwest Ethiopia. The strengths of the study are being multicenter, focusing on current CPG adherence, and data collection comprehensiveness and its mixed-methods study design, while the limitations include the study design, which limits the ability to establish causal relationships of variables, and prescribers may be inclined toward what is perceived to be acceptable that is, response bias, as self-reported adherence may not reflect actual clinical practice. The use of convenience sampling in the quantitative phase is a notable limitation; although, we prefer to use it to accommodate prescribers’ schedules, hospital duty rotations, and the need to minimize disruption of routine clinical services. To enhance external validity and reduce bias, future longitudinal research should consider probability sampling.
Conclusion and recommendations
More than one-third of the prescribers were low adherent to CPGs. The most common barrier for prescribers to adhere to CPGs was a lack of access to CPGs, followed by a lack of access to essential medicines and patients’ pressure on prescribers. The multivariable analysis in this study highlights the significance of prescribers’ clinical experience, resource availability, and qualifications as factors associated with adherence to HTN CPGs. To enhance adherence to HTN CPGs, it is essential to improve the availability of essential medications, diagnostic tools, and materials. Concerted efforts are needed to promote the adoption and consistent application of evidence-based HTN treatment guidelines among healthcare providers. This may involve targeted educational campaigns, integration of CPGs into electronic medical record systems, and continuous professional development activities. Addressing barriers to CPG adherence through a multifaceted approach could help ensure more consistent, evidence-based HTN treatment and improved patient care.
Supplemental Material
sj-docx-1-taj-10.1177_27558428261420524 – Supplemental material for Prescribers’ adherence to clinical practice guidelines for the management of hypertension at public hospitals in Northwest Ethiopia: An explanatory sequential mixed-methods study
Supplemental material, sj-docx-1-taj-10.1177_27558428261420524 for Prescribers’ adherence to clinical practice guidelines for the management of hypertension at public hospitals in Northwest Ethiopia: An explanatory sequential mixed-methods study by Tilaye Arega Moges, Samuel Berihun Dagnew, Woretaw Sisay Zewdu, Samuel Agegnew Wondm, Getachew Yitayew Tarekegn, Desalegn Addis Mussie, Teklie Mengie Ayele, Sisay Sitotaw Anberbr, Bayih Endalew Bitew, Abraham Nigussie Assefa, Addisu Assfaw Ayen and Fisseha Nigussie Dagnew in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
The authors would like to thank Debre Tabor University, the data collectors, and the respected hospitals and staff.
ORCID iDs
Ethical considerations
Ethical approval for this study was obtained from the ethical review committee of Debre Tabor University (with reference number CHS 333/2023), and this was provided approval for all participating hospitals. All the methods and procedures were conducted based on the Helsinki Declaration.
Consent to participate
Written informed consent was obtained from all the study participants by explaining the objective of the study.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data will be available upon reasonable request of the corresponding author.
Supplemental material
Supplemental material for this article is available online.