
Abstract
Pulmonary hypertension is a disease process affecting the pulmonary circulation and is defined by an increase in pulmonary artery pressure subsequently causing right ventricular failure. Vascular complications, including arteriovenous fistulae, are recognised, but are uncommon complications of spinal surgery. Arteriovenous fistulae increase venous return to the right heart and can induce a high-output cardiac state, mimicking pulmonary arterial hypertension and right heart failure. We present a 47-year-old man with a 1 year history of worsening dyspnoea, exertional pre-syncope and leg swelling presenting with severe right heart failure. The previous year, he had complex spinal surgery, which included discectomy, laminectomy and bilateral nerve reconstruction at L5-S1 level. Initial non-invasive investigations including echocardiography and chest imaging raised the possibility of right heart failure presumed secondary to pulmonary vascular disease. Clinical examination and right heart catheterisation were in keeping with a high cardiac output state, and invasive saturation monitoring was suggestive of a sub-diaphragmatic shunt. Subsequent imaging confirmed the presence of an iatrogenic ilio-iliac arteriovenous fistula. The patient underwent urgent endovascular repair, which resulted in resolution of his symptoms and haemodynamics. We describe the case and present a review of the relevant literature.
Keywords
Introduction
Pulmonary hypertension (PH) is a disease process affecting the pulmonary circulation and is defined by an increase in pulmonary artery pressure (mean pulmonary artery pressure > 25 mm Hg) during right heart catheterisation. Causes of PH include idiopathic pulmonary arterial hypertension (PAH), connective tissue disease, congenital heart disease (group 1), left-sided heart disease (group 2), hypoxic lung disease (group 3), chronic thromboembolic disease (group 4) and miscellaneous causes (group 5). A less recognised cause of PH is high blood flow through acquired systemic arteriovenous fistulae. Arteriovenous fistulae increase venous return to the right heart and can induce a high-output cardiac state, mimicking PAH and right heart failure. 1 Timely identification and treatment of an arteriovenous fistula can dramatically improve patients’ haemodynamics as well as symptoms. We describe a case and present a review of the relevant literature.
Case report
A 47-year-old man, non-smoker who was previously fit, presented with a 1 year history of worsening dyspnoea, pre-syncope and leg swelling. The previous year, he had complex spinal surgery, which included discectomy, laminectomy and bilateral nerve reconstruction at L5-S1 level. There was no relevant family history.
Following his surgery, he had multiple hospital admissions with right heart failure requiring intravenous diuresis. Echocardiography demonstrated preserved left ventricular (LV) function, but showed a severely dilated right ventricle (RV). The right atrium was severely dilated, while the left atrium appeared normal. There was severe tricuspid regurgitation and a rim of pericardial fluid. Cardiac magnetic resonance imaging (CMR) demonstrated a D-shaped LV consistent with RV pressure/volume overload and PH.
He was subsequently referred to a tertiary centre for further investigations. Examination revealed an elevated jugular venous pressure (JVP) with a loud second heart sound. There was a systolic murmur heard throughout the precordium, peripheral oedema and ascites. A bruit was heard over the abdomen. Blood investigations demonstrated haemoglobin of 11.7 g/dL, normal liver and thyroid function, and NTproBNP of 3600 pg/mL. Pulmonary function tests demonstrated normal spirometry with a diffusion capacity of 75%.
Chest X-ray revealed cardiomegaly with central pulmonary vascular congestion. CT pulmonary angiography and high-resolution CT demonstrated a dilated main pulmonary artery at 35 mm and normal lung parenchyma. The right-sided cardiac chambers were significantly dilated and the left-sided chambers were normal. There was reflux of contrast into the inferior vena cava (IVC) and a large volume of ascites. There was no evidence of pulmonary thromboembolism. The radiological findings were consistent with severe right heart failure likely secondary to PAH.
During right heart catheterisation, the mean pulmonary artery pressure was 30 mm Hg with a pulmonary capillary wedge pressure (PCWP) of 24 mm Hg. Cardiac output was 13.5 L/min with a pulmonary vascular resistance of 0.4 Wood Units. We proceeded to left heart catheterisation, which demonstrated normal coronary arteries with a LV end-diastolic pressure (LVEDP) of 24 mm Hg, consistent with the PCWP. The mixed venous saturation (mvO2) was 86.3%. The elevated cardiac output and mvO2 raised the possibility of left to right shunting, and we proceeded to invasive saturation monitoring results, which are summarised in Table 1.
Results of invasive saturation monitoring during right heart catheterisation.

There was a significant discrepancy between the superior vena cava (SVC) and the IVC saturations, suggesting the possibility of a sub-diaphragmatic shunt. CT of abdomen and pelvis in the arterial and portal venous phase was performed. On the arterial phase imaging, there was evidence of contrast in a grossly dilated venous system and what appeared to be a communication with the right common iliac artery. Appearances were highly suspicious of an ilio-iliac fistula (Figure 1).
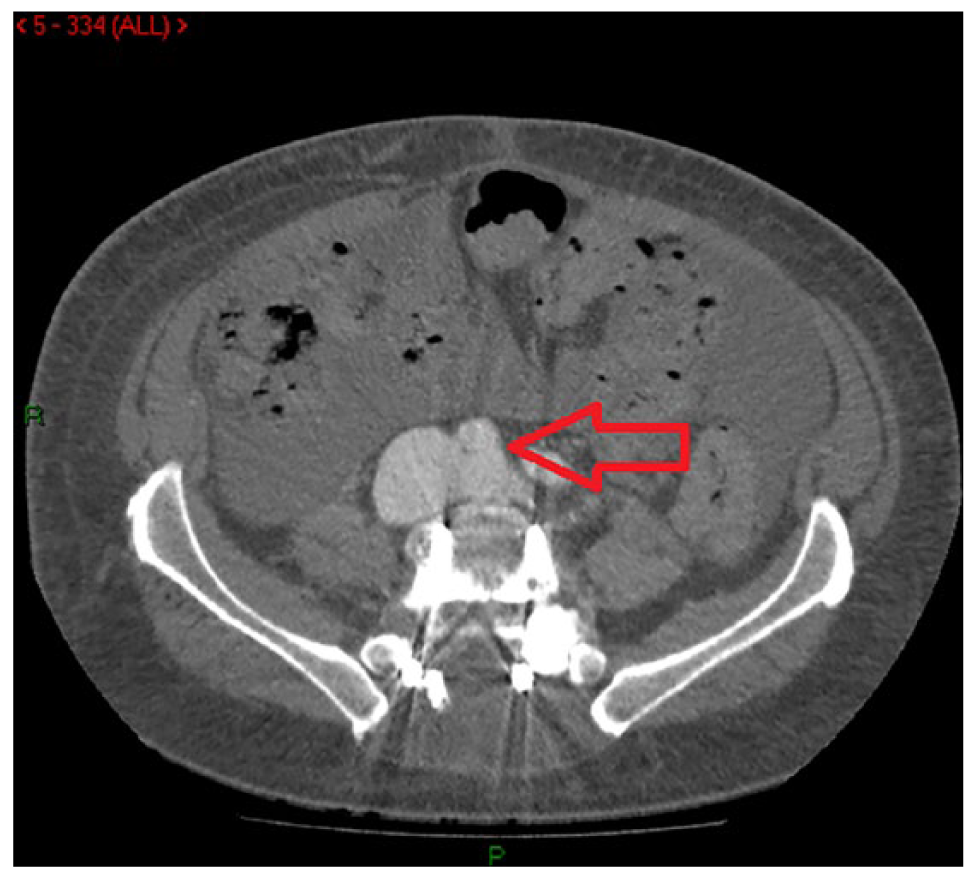
CT angiogram in the arterial phase. Both common iliac veins are demonstrated in this image – both have contrast present within them even though the imaging has been performed in the arterial phase, and the right common iliac vein in particular is grossly dilated. The right common iliac artery is indicated by the arrow – it is clear that there is no plane between the artery and the ‘arterialised’ venous system, consistent with the clinical suspicion of an iatrogenic arteriovenous fistula.
After multi-disciplinary team consideration, it was decided to manage the lesion endovascularly. The fistula involved the proximal common iliac artery. The key technical issue related to whether there was enough space to achieve a proximal seal if the right common iliac artery was to be managed in isolation. This was considered to be preferable to the alternative option of deploying a bifurcated stent graft in a young patient. Angiography demonstrated a large fistula with almost the entire contrast passing into the venous system (Figure 2). An Endurant™ stent graft limb was deployed percutaneously in the right common iliac artery, extending to the external iliac artery. Completion angiography demonstrated a significant improvement.

Pre-deployment angiography demonstrates a large volume of contrast in the inferior vena cava. In this image, the Amplatzer™ plug can be seen in the internal iliac artery origin and the Endurant™ stent limb can be seen in the common iliac/external iliac arteries ready to be released. In the post-deployment image, the Endurant™ stent graft limb is seen positioned well in the origin of the common iliac artery, extending into the external iliac artery – there is no contrast in the venous system demonstrated and the internal iliac artery has been adequately managed.
Following stenting, the patient regained his baseline functional level with almost immediate resolution of the peripheral oedema. At 10-week post-intervention, he did not have any cardiorespiratory symptoms. Echocardiography and CMR demonstrated normal functioning cardiac chambers with no tricuspid regurgitation.
Discussion
This report highlights a case of ilio-iliac fistula presenting as possible PAH with subsequent improvement in symptoms and haemodynamics following endovascular intervention. Initial investigations were focused on identifying a cardiac cause for the presentation. Thoracic and cardiac imaging was consistent with PH causing severe right heart failure. An extra-cardiac cause was initially suspected by the finding of an abdominal bruit and the subsequent right heart catheter findings of high cardiac output and invasive saturation monitoring. CT angiography confirmed the diagnosis.
Interestingly, in cases in the literature of patients presenting with a diagnosis of PH due to iatrogenic fistula secondary to lumbar surgery, the suspicion of an extra-cardiac shunt was only raised after right heart catheterisation. A 47-year old woman, with a history of lumbar surgery, was referred for evaluation of dyspnoea with progressive PH on echocardiography. 2 Right heart catheterisation confirmed PH and subsequent invasive saturation monitoring suggested an extra-cardiac shunt. CT of abdomen showed a fistula between her right common iliac artery and vein, and she underwent open surgical repair. In another case, a 36-year-old man had presented with progressive dyspnoea. 3 Imaging had resulted in a provisional diagnosis of PAH. On right heart catheterisation, high oxygen saturations in the IVC (92.3%) had prompted further imaging of the aorta, which demonstrated a fistula between right common iliac artery and right common iliac vein. In this case, it was likely related to a discectomy 16 years ago at L4-L5 level.
CT angiography is the non-invasive investigative modality of choice for diagnosing sub-diaphragmatic arteriovenous fistula. Digital subtraction angiography has similar sensitivity and specificity and allows immediate endovascular intervention. 4 A variety of interventional options have been described including laparoscopic suture, open surgical intervention and endovascular procedures. The advancement of endovascular techniques makes these the preferred treatment for iliac arteriovenous fistulae. The first such report documented an endovascular stent graft repair of a common iliac artery to IVC fistula. 5
Arteriovenous fistulae are rare iatrogenic complications of lumbar surgery and occur with an incidence of between 0.05% and 0.1%. 6 Arteriovenous fistulae have also been reported following appendicectomy, traumatic abdominal injury and can appear spontaneously. 7 Vascular injury and subsequent fistula formation during lumbar spinal surgery can occur due to the penetration of surgical instruments beyond the anterior longitudinal ligament. Iliac artery and veins are most frequently injured due to their relative immobility as well as their close proximity to L4-L5, where lumbar surgery is most performed. 8
Conclusion
In patients presenting with PH with a high cardiac output in the context of surgery and risk factors, it is important to consider iatrogenic fistula as a rare differential diagnosis. A detailed history combined with examination, with specific reference to the presence of bruits, may guide the clinician. With the advancement of endovascular technology, the majority of these cases will have minimally invasive therapeutic options that can resolve the cardiac and physiological dysfunctions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.