
Abstract
Thanks to the emergence of direct-acting antiviral agents, Hepatitis C (hepatitis C virus (HCV)) elimination is a real possibility. In 2016, the World Health Organization established a global strategy with the aim of achieving HCV elimination by 2030. However, the actual implementation of this strategy within healthcare systems worldwide has proven challenging, and the COVID-19 pandemic nearly completely halted HCV elimination programs. Seroprevalence studies in the general population attending health centers in Spain place us as a low-prevalence country, but recent reports have shown that the Emergency Department and hospital population show significantly higher prevalence rates, suggesting that studies in the general population may underestimate the true prevalence, especially in vulnerable people. Thus, HCV screening should be implemented through a combination of approaches: population-based programs, self-referral options, and opportunistic testing during any healthcare encounter. Here, we summarize the main updates to the measures adopted in the Strategy for the Elimination of Hepatitis C in Cantabria, a region in northern Spain, so that they can serve as inspiration for other regions. The update prespecifies primary operational and virological endpoints (coverage, linkage‑to‑care, time‑to‑treatment, and sustained virological response 12 (SVR12)), and secondary clinical outcomes, and it includes a pragmatic economic assessment (cost per diagnosis/SVR and budget impact).
Keywords
Introduction
In recent years, thanks to the emergence of direct-acting antiviral agents (DAAs), which achieve cure rates of over 95%,1–3 Hepatitis C (hepatitis C virus (HCV)) elimination is a real possibility. Therefore, in 2016, the World Health Organization (WHO) established a global strategy with the aim of achieving HCV elimination by 2030. 4 This strategy defines elimination as an 80% reduction in new HCV infections and a 65% reduction in HCV mortality. In the case of Spain in particular, the National Strategic Plan against Hepatitis C has set out different lines of action against HCV. 5 Recent studies are demonstrating a reduction in prevalence 6 and disease burden 7 primarily due to broad availability of treatment. As a result of its application in the Autonomous Community of Cantabria, a region in northern Spain, we designed a plan for the elimination of HCV whose main objective was its elimination in the period 2019–2021. 8 The Spanish autonomous community of Cantabria spans 5330 km2 and is home to 584,507 people. 9 Its demographic landscape is shaped by immigration, which accounts for an estimated 5% of the population, with the main nationalities being from Romania, Colombia, and Morocco. Regarding public health challenges related to substance abuse, it is estimated that 7% of the general population with an active HCV infection are identified as drug users.
The Strategy for the Elimination of Hepatitis C in Cantabria was successfully implemented in the region. 8 However, because of the COVID-19 pandemic and the advances in healthcare and technological knowledge in the natural history of HCV infection, it is necessary to update this strategy to adapt it to the new circumstances.
The COVID-19 pandemic that started in early 2020 has affected the comprehensive approach to HCV and led to a delay in all conventional diagnostic pathways, 10 as well as to a near-complete halt in HCV elimination programs.5,8 Therefore, to minimize the impact of the SARS-CoV-2 pandemic and remain on track for elimination targets, measures are needed to strengthen screening programs, re-establish the viral hepatitis care cascade, and enable treatment at early stages of liver disease.
It is also necessary to emphasize and further promote existing effective measures aimed at diagnostic simplification, such as the One-Step, 11 and Point-of-Care (POC) diagnostics, 12 together with microbiology laboratory alert systems, and micro-elimination strategies targeting at-risk populations or vulnerable groups (such as people living in prison, people living with human immunodeficiency virus (HIV), substance users, or people attending harm reductions facilities). 13
Data from 2020 seroprevalence studies, which analyzed the general population attending Spanish health centers, classify Spain as a low-prevalence country for active HCV infection. Specifically, the prevalence among those aged 20–80 was 0.17% in 2020, a decrease from 0.22% in 2018. 14 However, the rate of active infection is higher in men aged 50–59 years, reaching 0.86%. 15 These seroprevalence studies were conducted among individuals attending primary care centers in Spain, where participants were invited to undergo testing voluntarily. Thus, these estimates reflect a population of healthcare users who consented to serological testing, rather than a random sample of the entire general population.
Recently, opportunistic screening in the Emergency Department and hospital population has been found to show significantly higher prevalence rates (up to three times in some subgroups), suggesting that studies in the general population may underestimate the true prevalence, especially among the most vulnerable people who infrequently attend conventional healthcare facilities. 16 Furthermore, it highlights that there remain missed opportunities for care, 17 with some patients lost to follow-up after diagnosis. This underscores the importance of proactive strategies to re-engage individuals with HCV infection, including recall programs 18 that systematically identify laboratory-confirmed positive cases without treatment records in the electronic health system and link them back to care. 19
All these facts support the need to update HCV elimination strategies. A more proactive approach to HCV diagnosis is essential for its elimination. Diagnosis based on symptoms and/or risk of acquiring the infection has proven to be insufficient and of complex application in real clinical practice, including that individuals diagnosed in these situations usually present with an advanced liver disease.20,21 Therefore, HCV screening should be implemented through a combination of approaches: population-based programs, self-referral options, and opportunistic testing during any healthcare encounter. Here, we summarize the main updates of the measures adopted in the Strategy for the Elimination of Hepatitis C in Cantabria, so that they can serve as inspiration for other regions.
Rationale and changes since the 2019–2021 plan
Since the original Cantabria elimination plan (2019–2021), COVID‑19 disrupted diagnostic pathways and slowed elimination programs. Concurrently, evidence accumulated in our health system has shown higher HCV prevalence in emergency and perioperative populations, and the feasibility of simplified diagnosis. The updated strategy, therefore, (i) expands opportunistic screening beyond primary care to emergency and preoperative settings, (ii) consolidates reflex RNA/core‑antigen and comprehensive viral hepatitis diagnosis, (iii) streamlines assessment and treatment into a single visit with pharmacy dispensing, and (iv) implements retrospective database cross‑matching to recover patients lost to follow‑up.
In addition, hospital centers in the region fulfils the criteria to fit with the recently published “Ten steps to eliminate hepatitis C in hospitals.” 22
Objectives and endpoints
The primary objective of this protocolized update is to increase case finding and shorten time‑to‑cure across macro‑(population) and micro‑elimination settings in Cantabria by deploying simplified “one‑step” diagnostics, decentralized POC testing, and streamlined care pathways. Primary endpoints are as follows: (i) screening coverage and diagnostic yield (anti‑HCV and RNA positivity) across predefined settings; (ii) linkage‑to‑care among RNA‑positive individuals; (iii) time from index test to treatment initiation and proportion initiating therapy at the first visit; and (iv) sustained virological response 12 (SVR12). Secondary endpoints include the following: detection of advanced fibrosis/cirrhosis, incident hepatocellular carcinoma and liver decompensation, reinfections in ongoing‑risk groups, uptake of POC/dried‑blood‑spot testing, comprehensive viral hepatitis diagnosis (hepatitis B virus (HBV)/hepatitis D virus (HDV)/HIV reflex testing), recovery of patients lost to follow‑up, and setting‑specific micro‑elimination indicators. In parallel, we will conduct a pragmatic economic evaluation—focused on cost per confirmed diagnosis, cost per SVR, and annual budget impact from the regional health‑service perspective—leveraging laboratory, pharmacy, and electronic medical record data; indicators in Table 3 operationalize these endpoints for monitoring and evaluation.
Regional HCV elimination programs
Two research studies, the Cantabria Cohort 23 and the FOCUS program, have been instrumental in the development and implementation of the regional elimination programs. These research and innovation initiatives provided data, knowledge, training, and skills needed to efficiently develop and implement the regional plan.
The Cantabria Cohort stems from a research and action initiative to improve the regional health system and advance the health-related Sustainable Development Goals. 23 It is a population-based cohort including residents of Cantabria aged 40–69 years old. Among its main objectives are reducing HCV, HBV, and HIV in Cantabria and enhancing treatment through serological testing of all participants. It has already allowed HCV age screening in almost 40,000 participants, representing 16% of the target population. 24
On the other hand, the FOCUS program is an opportunistic screening program for HIV and HBV, and HCV in 42 primary care centers in Cantabria. Approximately 40,000 people will be screened by testing patients with no previous HIV and viral hepatitis test results who attend these centers. The processing and analysis of these samples will be performed at the Marqués de Valdecilla University Hospital. The program follows the ECDC Public Health Guidance on HIV, HBV, and HCV testing 25 and the National Decalogue for Hepatitis C elimination. 26 There is a similar FOCUS program with data available and published. The FOCUS-CRIVALVIR initiative illustrates the convenience of integrated opportunistic screening for HIV, HBV, and HCV within the Spanish healthcare system. The program has proven effective in uncovering hidden infections, enabling early linkage to care, and preventing new transmissions, while also being cost-saving compared to nonintervention.27,28 The initiative targeted the entire adult population (⩾18 years) attending primary care centers, specialized care, emergency services, and the local penitentiary, ultimately screening nearly 32,000 individuals between 2019 and 2022. Providing this context is particularly relevant in Spain, where HIV prevalence is estimated at 0.31% of the adult population. 27 Notably, HIV–HCV coinfection remains a significant clinical challenge, with approximately 20%–30% of people living with HIV historically affected by chronic HCV infection. 27
These initiatives have already generated baseline data, which informed the initial design of the regional plan, and they continue to provide updated information as they are progressively rolled out.
Opportunistic diagnosis in the primary care setting
According to our own data 29 and that of the Cantabrian Health Department, more than 85% of people between the ages of 40 and 70 visit their primary care doctor and/or nurse at least once a year. Data from the PREVHEP-ETHON study demonstrated that this age group carries the highest prevalence of active HCV infection, largely due to historical exposures prior to the introduction of systematic screening and blood safety measures. Moreover, economic modeling confirmed that initiating screening in this cohort identifies a substantial proportion of undiagnosed cases while remaining cost-saving for the healthcare system. 29
Therefore, an opportunistic case finding can be carried out in primary care consultations for people between the ages of 40 and 69.
A specific protocol for this healthcare process has been included within the electronic medical history of all patients whose age is between those indicated above. In addition, this protocol is activated annually for some risk factors for which there is a specific code (alcohol use disorder, drug addiction, hemophilia, some sexually transmitted diseases, etc.). Patients without risk factors who have a negative test result in the previous 5 years, or those with a previous diagnosis of hepatitis C (exceptions that are automatically configured in the electronic request system), will not need to be tested for HCV infection.
Opportunistic diagnosis in hospital settings
The target population for this program is individuals over 18 years of age who are seen in the hospital setting (such as emergency departments30,31), with the exception of individuals with a negative HCV test result in the previous 5 years or those with a previous diagnosis of hepatitis C (exceptions are automatically configured in the electronic request system).
Targeted HCV elimination programs
These programs are aimed at the active identification of cases in different high-prevalence or high-incidence groups with hepatitis C, including vulnerable adult populations (Table 1).
Target groups for micro-elimination programs and main institutions/departments responsible for their clinical management, who could contribute to the identification of HCV-infected individuals.

HCV: hepatitis C virus; HIV: human immunodeficiency virus.
Micro-elimination programs target adult populations (over 18 years of age).
Chemsex: Chemsex refers to the intentional use of certain psychoactive drugs before or during sex to enhance, prolong, or facilitate sexual experiences without any prevention measure—condomless—and with several partners at the same time.
There are very specific risk groups that will be captured directly from the hospital care consultations or in the aforementioned centers. The doctors responsible for each service involved in the care of these at-risk groups (infectious diseases unit, transplant units, psychiatry service, hematology service, social integration centers, and penitentiary centers) will be responsible for identifying the people at risk (see Table 1). Once identified, the digestive services will be responsible for checking their serological status and, in the event that this is not up to date, the patients will be summoned to the respective consultations for a conventional microbiological analysis following a reflex test diagnosis strategy.
We have previously developed some pioneering programs, such as JailFree-C 32 or Honest, 33 aimed at systematically screening and treating HCV infection in incarcerated individuals and those receiving non-custodial sentences. Both studies confirm that HCV micro-elimination is feasible in penitentiary-associated populations: in El Dueso prison (JailFree-C), universal screening and telemedicine-guided treatment achieved 96.9% SVR with no reinfections, while in individuals serving non-custodial sentences (HONEST project), navigator-assisted POC testing reached 92.8% screening, 2.9% active viremia, and 100% SVR among those completing follow-up.
Similarly, in the context of microelimination, it is instrumental to ease the diagnosis and to bring it closer to the target groups. Therefore, diagnostic techniques, such as dried blood spot tests or POC diagnostic methods, are employed. This decentralized diagnosis is then integrated into the usual circuits.
General intervention model: Diagnosis, treatment, and monitoring
We proposed updated diagnosis, treatment, and monitoring circuits within the health system, which applied both to the macro- and micro-elimination programs (Figure 1).

Care pathway integrating macro- and micro-elimination programs for early care and treatment of patients. Although the program is focused on HCV elimination, comprehensive diagnosis of viral hepatitis(*) has been integrated in the diagnostic pathway: any positive value, including HCV antibody will trigger automatically in the same sample the test for HIV, HBV, and HDV if it applies. Thus, reflex testing of HBV, HDV, and HIV is performed in all HCV-positive samples. Any HCV active infections, as HCV-PCR positive will trigger an alert to attend a consultation with the specialist.
The analytics will have the character of a reflex test, that is, those serological determinations that are positive or doubtful will be completed with a viral load determination with the same biological sample in the Microbiology Department. Therefore, viral load of the C virus by polymerase chain reaction and the genotype (if it is considered essential) will be performed without a new extraction being required. This same process will be carried out on subjects with an indeterminate result in the serology. Furthermore, reflex testing of HBV, HDV, and HIV will be automatically activated in the Microbiology Department in all cases testing positive for HCV. 34
All diagnoses of active infection by positive viral RNA detection are included in a weekly electronic alert, which is evaluated by the Hepatology Unit of the reference Digestive Service (Valdecilla University Hospital). In a single visit, the severity of the disease will be characterized by transient elastography to determine the degree of liver fibrosis and an abdominal ultrasound, as well as a comorbidities evaluation to carry out a personalized evaluation. Besides, a blood sample will be collected for potential phylogenetic analysis of the virus to subsequently determine possible reinfections. At the end of the consultation, they will be prescribed the corresponding treatment, which will be dispensed in the Pharmacy Service.
The follow-up of patients diagnosed with hepatitis C will be carried out in the digestive system consultations. Although the follow-up of treated patients will be individualized, the program provides for a homogeneous follow-up after the start of treatment, which includes a blood test 12 weeks after the end of treatment to determine the existence of SVR, that is, the absence of detectable viral load at that time. This will be the only follow-up visit for patients with non-advanced fibrosis who have SVR. In the absence of SVR, a subsequent visit will be scheduled, and rescue treatment will be offered. Follow-up for patients with advanced fibrosis and SVR will be carried out in the different Digestive System Services of the region, where esophageal variceal surveillance and hepatocellular carcinoma screening programs should be carried out according to standard clinical practice. All patients with SVR will be advised to have a new viral load determination annually in case of presenting risk behaviors to detect reinfections.
On the other hand, subjects with a negative result will be informed of the same by the healthcare professional who recruited them. Based on the risk group to which they belong or the risk practices they maintain, their doctor will explain the need for periodic annual follow-up.
This approach incorporates several improvements (Table 2) and simplifications of note:
Best clinical practices incorporated in the Strategy for the Elimination of Hepatitis C in Cantabria.

Decentralized diagnosis: the system increases the capacity to record POC tests performed at the sites/centers where these individuals are cared for, their supervision by the central microbiology laboratories, as well as the inclusion of the results in the patient’s medical record.
Simplified pre-treatment assessment and diagnosis: the information needed to start the treatment is just the presence of HCV viral load and/or core antigen and evaluation of the possible pharmacological interactions. It is also recommended to evaluate the presence of liver fibrosis but overall, the strongest recommendation is to perform the baseline assessment in a simplified manner (in a single visit if possible) or by ensuring reflex testing in the laboratory for all individuals with a positive anti-HCV test result. In this sense, reflex test diagnosis is key to prevent losses in referrals caused by delays and allows a greater number of patients to be evaluated for treatment while optimizing resources and time, thereby alleviating the strain on healthcare services.
Comprehensive diagnosis of viral hepatitis: the high degree of similarity in the epidemiology of these viral infections, given that they share risk groups and transmission routes, means that the risk of co-infection with HBV, HCV, HDV, and HIV, in their different combinations, is high. Given the high risk of contracting chronic viral infections and the low health care of the population at risk or vulnerable groups, the implementation of comprehensive diagnosis in community centers has proven to be viable, feasible, and effective, minimizing missed testing opportunities, optimizing their coverage, and showing positive results in terms of testing rates. Still, there is a need to perform a comprehensive diagnosis in the case of sexually transmitted infections such as syphilis and gonorrhea, which are not included in our strategy.
Streamlined appointment circuit: Automated alert systems linked to the patient’s electronic medical record help to identify and notify the specialist of the need to perform serology for any possible viral hepatitis, thus favoring early diagnosis. The incorporation of electronic alerts warning of the existence of an infection in the event of a positive case in the microbiology laboratory report and/or in the medical history increases the referral of patients to the specialist for their evaluation and management of the infection.
Simplified treatment: the treatment is dispensed in its entirety in a single visit, during which it will be explained to the patient. Given the simplicity of the treatment and the support of new technologies, physical monitoring of the treatment may not be necessary, except in cases associated with exceptional situations.
Avoid lost to follow-up: as recently recommended, a retrospective outreach program is being implemented to locate patients lost to follow-up. 35 This program involves cross-referencing HCV-antibody, RNA test databases, and EMR review from 2015 to the present. To ensure ongoing monitoring and address potential follow-up issues proactively, similar database cross-referencing will be conducted biannually.
Dissemination, communication, and training
Chronic viral hepatitis is a group of diseases that typically remain asymptomatic until advanced stages. Therefore, it is essential to educate and raise awareness among healthcare professionals, especially in primary care, about the importance of detecting undiagnosed cases in the general population, as well as identifying risk factors (see Table 1). In addition, decentralizing the screening and treatment process also needs training of non-healthcare personnel who offer tests to ensure patient acceptance of screening and subsequent treatment in hard-to-reach populations.
Moreover, educating at-risk and vulnerable populations about risk factors, the consequences of liver disease, and the benefits of treatment would improve prevention, case detection, and linkage to healthcare. For instance, it has been shown that education combined with tools such as electronic alerts can significantly increase detection rates.59,60 Similarly, civil society plays a fundamental role in eliminating viral hepatitis, being crucial to reaching difficult-to-access populations that largely distrust healthcare professionals. It is necessary to involve them to promote action plans (i.e., awareness campaigns like World Hepatitis Day, July 28th, or Yellow July—Julho Amarelo—in Brazil) on promoting prevention, diagnosis, and treatment, and to make them participants in public health interventions across different settings.
Thus, designing campaigns aimed at civil society would help raise awareness about the importance of viral hepatitis and reduce the stigma of the disease. The recommendations in this regard are aimed at the following:
- Increasing the training and awareness of all healthcare professionals, especially primary care professionals, about the importance of actively searching for individuals to achieve the goals of controlling and eliminating hepatitis B, C, and D.
- Intensifying the role of scientific societies through awareness and training campaigns aimed at healthcare professionals and patients.
- Broadening information to civil society in general about the importance of getting tested for viral hepatitis through awareness campaigns endorsed by scientific societies.
Program evaluation and endpoints
Regular evaluation of program outcomes is key to correct deficiencies. Therefore, a series of indicators has been defined (Table 3) to enable the implementation of correction measurements. This monitoring of the program’s functioning and results is under continuous evaluation and will be adapted to the recommendations that are published with the aim of being able to demonstrate the elimination of hepatitis C in our region. It is essential to prioritize developments in the health service information systems for the automation of extractions, and to improve the alert, citation, and collection of information on the management of viral hepatitis. In addition, it is a priority to develop a dashboard that allows the visualization of these indicators, as well as the objectives for the elimination of hepatitis C as recommended by the WHO, allowing health professionals to extract information in a repeated, simple, and cost-efficient way.
Key indicators for the evaluation of the elimination programs.
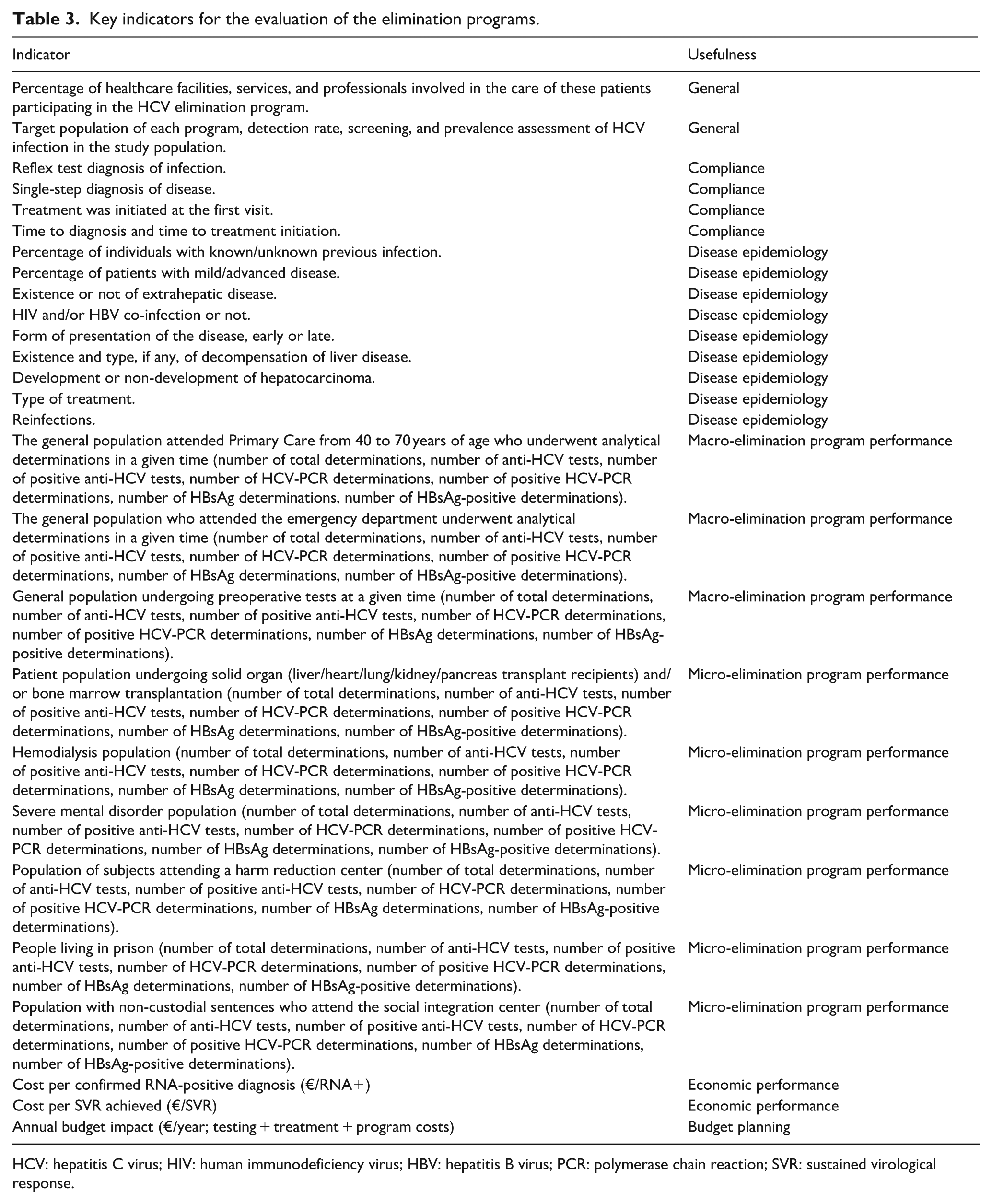
HCV: hepatitis C virus; HIV: human immunodeficiency virus; HBV: hepatitis B virus; PCR: polymerase chain reaction; SVR: sustained virological response.
Economic evaluation
In parallel with operational monitoring, we will conduct a pragmatic economic evaluation—focused on cost per confirmed diagnosis, cost per SVR, and annual budget impact from the regional health service perspective—leveraging routinely collected laboratory, pharmacy, and electronic medical record data. Results will be reported alongside program indicators and explored through sensitivity analyses (e.g., uptake of POC/Dried Blood Spots (DBS) testing, linkage to care rates, and drug acquisition costs).
Limitations
As a pragmatic, system-wide program, heterogeneity across settings and reliance on routinely collected data may affect precision; these will be addressed through standardized definitions and periodic data quality checks.
Concluding remarks
The updated strategy for the Elimination of HCV in Cantabria is a comprehensive plan to efficiently implement the best, scientifically proven practices in our Health System, with the ultimate goal of HCV eradication. Here, we aimed to highlight key elements that can inspire other regions for the development of their own elimination plans, not only in Spain but also worldwide, as we propose in Latin America. 61 Importantly, this strategy involves healthcare personnel, but also social workers, consultants, IT professionals, managers, and decision makers who are key to the success of the programs. Public education and collaboration are equally important to address the disease, whose symptoms go unnoticed until a complete cure becomes difficult. Therefore, the elimination of HCV requires significant efforts from a broad spectrum of stakeholders, long-term commitment to its goals, and strong conviction regarding its importance for the community as a whole.
Footnotes
Acknowledgements
We particularly acknowledge the contribution of the Task Force for the Elimination of Hepatitis C in Cantabria (listed in alphabetical order): Aitziber Illaro Uranga (Pharmacology Department, Marqués de Valdecilla University Hospital, Santander, Spain), Ana Batlle (Cantabria Health Service (SCS), Santander, Spain), Aroa Delgado Uria (Regional Primary Care Management, Cantabria Health Service (SCS), Santander, Spain), Ana Rodriguez (Microbiology Department, Marqués de Valdecilla University Hospital, Santander, Spain), Beatriz Josa Fernández (Regional Primary Care Management, Cantabria Health Service (SCS), Santander, Spain), Carmen Fariñas Álvarez (Infectious Diseases Department, Marqués de Valdecilla University Hospital, Santander, Spain), Fernando Andrés Mantecón (Regional Primary Care Management, Cantabria Health Service (SCS), Santander, Spain), Guillermo Pombo Alles (Spanish Society of Primary Care Physicians (SEMERGEN) of Cantabria, Spain), Inés De Benito Población (Microbiology Department, Sierrallana Hospital, Torrelavega, Spain), Isabel Priede Díaz (Spanish Society of General and Family Practitioners (SEMG) of Cantabria, Spain), Javier Cloux Blasco (Regional Primary Care Management, Cantabria Health Service (SCS), Santander, Spain), Luis Miguel Otero García (Regional Primary Care Management, Cantabria Health Service (SCS), Santander, Spain), María del Mar Navarro Córdoba (Cantabria Health Service (SCS), Santander, Spain), Marina Millan-Lorenzo (Gastroenterology and Hepatology Department, Sierrallana Hospital, Torrelavega, Spain), Marta Cobo Martín (Gastroenterology and Hepatology Department, Laredo Hospital, Laredo, Spain), Miguel García Ribes (Spanish Society of Family and Community Medicine (SEMFYC) of Cantabria, Spain), Montserrat San Martin Aparicio (Regional Primary Care Management, Cantabria Health Service (SCS), Santander, Spain), Pablo González Astorqui (Regional Primary Care Management, Cantabria Health Service (SCS), Santander, Spain), Purificación Mellado Encinas (Microbiology Department, Laredo Hospital, Laredo, Spain), Soledad Melgosa Moreno (Spanish Society of General and Family Practitioners (SEMG) of Cantabria, Spain), Susana Fernández Iglesias (Cantabria Health Service (SCS), Santander, Spain).
Disclaimer/publisher’s note
The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from the FOCUS program, developed by Gilead S.L.U., to implement effective blood-borne virus detection models that have enabled diagnosis and linkage to care for patients in need. The funding sources were not involved in the research design or preparation of the article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J. Crespo reports grant support and/or consultancy and lecture fees from AbbVie, Gilead Sciences, Bristol-Myers Squibb, Janssen, and MSD. J. Cabezas discloses grants, consultancy, and lectures from Gilead and AbbVie. The remaining authors declare no conflicts of interest. The funders had no role in the design of the program; in the writing of the manuscript; or in the decision to publish the results.
Data availability statement
Not applicable.