
Abstract
Background:
Pain is a subjective, multidimensional experience modulated by emotional states and mental processes. It may be a source of major alterations in quality of life, and it represents substantial costs for health care systems and society.
Objectives:
This research aims at exploring, in vulnerable persons living with chronic conditions, the relation between pain intensity and: (1) socio-demographic variables; (2) sedentary behaviour and physical exercise and (3) quality of life.
Design:
The EFFICHRONIC intervention is part of the Third EU Health Programme. It consisted of implementing the Chronic Disease Self-Management Programme in five European regions (in France, Italy, Spain, the Netherlands and the United Kingdom).
Methods:
Adjusting for a wide range of variables in multivariable regressions and using multiple imputation methods, we examined the associations between the intensity of pain and the other variables of interest in a large sample (1364 participants).
Results:
These analyses showed that women had more intense pain, as well as participants with a lower education level. The pain was, among all variables, the main predictor of sleep problems, fatigue, depression, self-perceived health and quality of life.
Conclusion:
Our results confirmed the importance of the social component in the complex aetiology of pain, and reinforced the idea that the recognition of the social determinants of health is essential. They are also in line with other studies showing the major impact of pain on an individual’s health and life. Decreasing social inequalities and vulnerability could clearly reduce the prevalence of pain.
Trial registration:
The study was registered at ISRCTN – The UK’s Clinical Study Registry (70517103).
Plain language summary
Pain is influenced by emotional states and mental processes such as attention, interpretation, memory, and anticipation. This study explores the relationship between pain intensity, socio-demographic factors, physical activity, and quality of life in vulnerable individuals living with chronic conditions. As part of the EFFICHRONIC intervention, a health education program implemented in five European regions, we analyzed data from 1,364 participants at baseline. Our findings show that women and individuals with lower education levels experience more intense pain. These results highlight the important role of social factors in the complex causes of pain. Reducing social inequalities and vulnerability could help lower the prevalence and impact of chronic pain.
Introduction
Background
Pain is a subjective, multidimensional experience inducing multiple repercussions on quality of life, sleep, mood, physical activity, self-perceived health, social relations, work and income.1–4 Indeed, pain imposes a significant emotional and physical burden on those affected, and leads to physical, psychological, social and economic vulnerabilities.5,6 Pain intensity depends on nociception 7 and central neuroplasticity, 8 but is also modulated by emotional states, socio-economic status and cognitive processes (such as attention, interpretation, memorization and anticipation).9,10
Pain is a very frequent reason for medical visits, 11 and constitutes an important workload for health systems. 12 For example, spinal pain is experienced by 80% of individuals at some point in their life in the United States, 13 and the prevalence in the elderly is estimated at 49%. 14 In France, 54% of adults had lived with pain in the past 2 years, 15 and 25% had experienced physical pain that was difficult to bear in the past year. 16 Patients who reported pain consulted healthcare professionals twice as often as the others. 17
In several chronic diseases, pain is one of the main symptoms affecting the daily life of patients. Chronic pain is defined as lasting more than 3 months. The general adult population in the European Union reported an average chronic pain prevalence of around 20%.18–20 The pathogenesis of chronic pain is complex and highly heterogeneous.21–23 Pain is closely linked to psychological and social distress, with reciprocal influences.24–27 It also depends on demographic and socio-economic factors: it is more frequent in the elderly, women and persons with a lower level of education or income.28–31
Chronic pain is a source of disability and major alterations in quality of life.20,32 It represents significant costs for health systems,33,34 including direct costs involved in the diagnosis and treatment (medical visits, analgesics), but also due to induced comorbidities (depression, addictions). 35 The annual additional medical cost is estimated at more than 1 billion euros in France. 17 In addition, chronic pain implies indirect costs in terms of work capacity: it represents a very significant proportion of the causes of sick leave, absenteeism, early retirement and permanent disability.35,36 Chronic pain induces a reduced likelihood of being employed full time, 36 and a decrease in productivity at work.37,38 Thus, in addition to its considerable impact on the quality of life of individuals, it reduces the competitiveness of the working population.
Vulnerable people, that is, individuals at a higher risk of adverse outcomes due to social, economic, demographic and environmental circumstances, 39 are more likely to be affected by chronic conditions. 40 As an example, the prevalence of chronic conditions reaches 60% among beneficiaries of the Medicaid programme in the United States (low-income people aged 18–64 years) against 50% in the general population (yet including people over 65 years). 41
Vulnerability can drive the incidence of chronic disease through its influence on modifiable risk factors,42–45 and reduced utilization of health care systems, due to barriers such as geographical isolation, scarcity of public transport or lack of social ties.46–48 People with low incomes find it less easy to adhere to a healthy lifestyle and have poorer general health.49,50 They generally tend to be most affected by the fragmentation of care services. 51 But vulnerability can also be the consequence of a chronic condition: illness aggravates social vulnerability and can push people into precariousness through job loss. 52
Although there is enough evidence to make it a high priority, as well as to conduct more research, chronic pain appears to have received few specific public health policy responses, especially in vulnerable populations. The research project EFFICHRONIC53,54 is a prospective and multicentric study, where socio-economically vulnerable participants with a chronic condition participate in the ‘Chronic Disease Self-Management Programme’ (CDSMP). 55
Objectives
In this article, we explore, in vulnerable persons (vulnerability being related to either older age, social isolation, economic deprivation or immigration), living with chronic conditions (according to the International Classification of Primary Care-2 56 ), the relation between pain intensity and: (1) socio-demographic variables (country, sex, age, education, income and social network); (2) sedentary behaviour and physical exercise; (3) quality of life (mental and physical), and its components (sleep problems, fatigue, psychological distress and general perceived health) and (4) work absenteeism.
Methods
Design
EFFICHRONIC53,54 is a European public health intervention implemented as part of the Third EU Health Programme, which addressed the chronic disease challenge. It aimed to improve the self-management of chronic diseases in vulnerable populations by deploying the CDSMP 55 across five European regions (Occitanie in France, province of Genoa in Italy, principality of Asturias in Spain, region of Rotterdam in the Netherlands and the region of London in the United Kingdom). The intervention focused on empowering patients through education and peer support, with the goal of enhancing health outcomes and reducing healthcare disparities. It was preceded by a baseline questionnaire, including socio-demographics (age, sex); education level (primary or lower, secondary, tertiary or higher); household composition (living alone or not) and various validated self-assessed scales (Table 1).
The instruments used in this study.
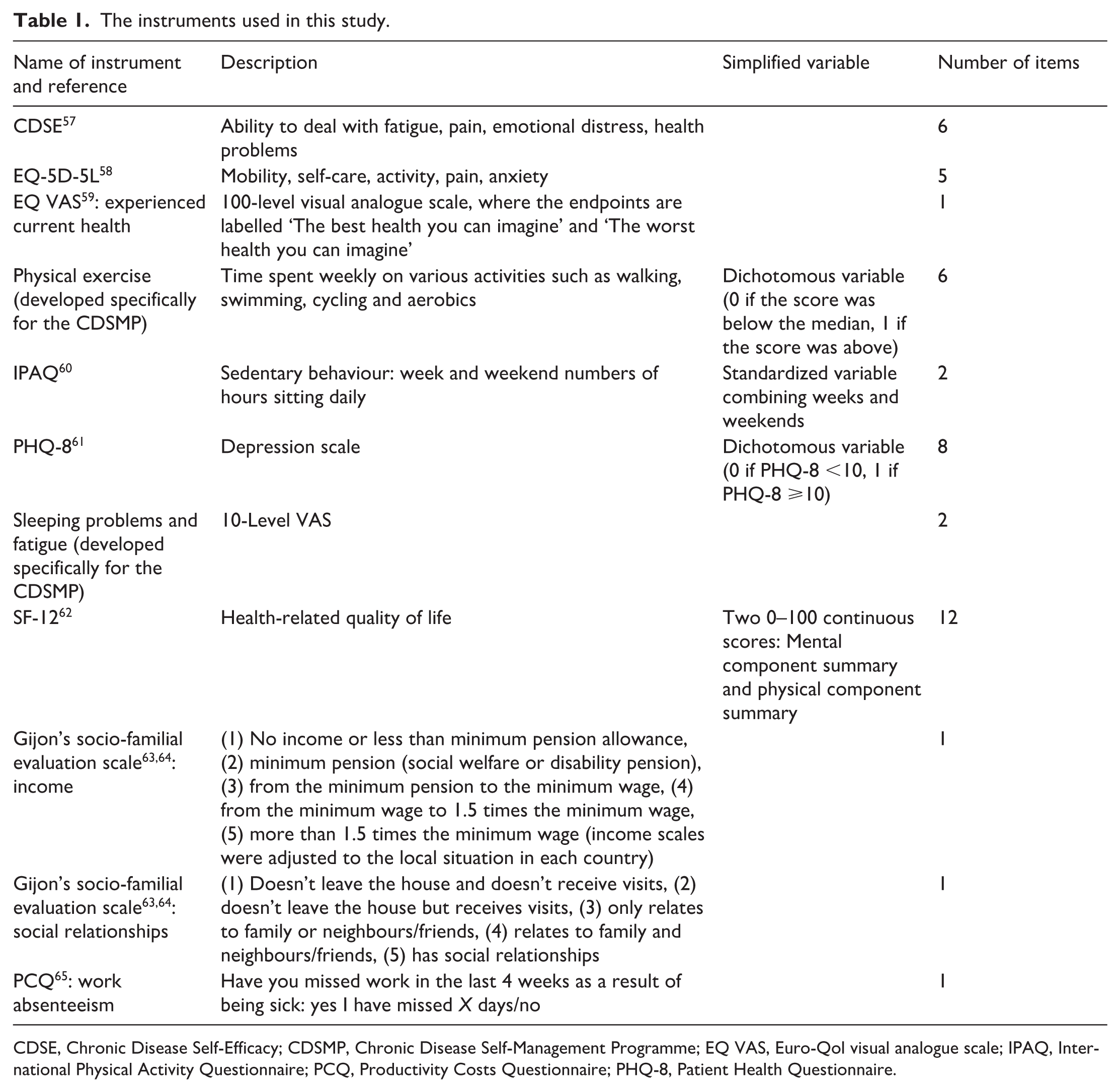
CDSE, Chronic Disease Self-Efficacy; CDSMP, Chronic Disease Self-Management Programme; EQ VAS, Euro-Qol visual analogue scale; IPAQ, International Physical Activity Questionnaire; PCQ, Productivity Costs Questionnaire; PHQ-8, Patient Health Questionnaire.
Sample
Participants have been recruited to receive the six sessions of the CDSMP intervention with the following inclusion criteria: being at least 18 years old, having at least one chronic condition (according to the International Classification of Primary Care-2 56 ) for at least 6 months and meeting at least one of the following vulnerability criteria: older people (over 65) living alone or in retirement homes, or experiencing social or family isolation; ethnic minorities; legal immigrants, refugees and asylum seekers (residing for at least 6 months), recipients of disability pensions or allowances and low-income individuals (below 60% of the median standard of living in 2015 66 ).
The development of EFFICHRONIC’s recruitment approach combined population-based and individual recruitment strategies. 67 First, vulnerability maps were developed to detect areas with higher vulnerability, based on specific deprivation indices, employing different methodologies. The maps are based on Population Census data in Spain (the MEDEA index 68 and an ad hoc rural index), France (the FDep index 69 ) and Italy (the Crevari and Caranci indices 70 ). In the United Kingdom, the National Index of Multiple Deprivation 71 produces an overall relative measure of deprivation and was consulted online. In the Netherlands, the most vulnerable areas at this study site were identified by stakeholders working in the community. Second, within those areas, potential participants were individually recruited following a variety of recruitment strategies. To reach the vulnerable population, alliances with local and regional authorities, health services, social care organizations and civil society were generated across the EFFICHRONIC sites. The recruitment process was adapted to the socio-economic context, the health system and cultural singularities of each country.
Outcomes
In the questionnaire at baseline, three questions were directly related to pain assessment:
Pain intensity in the EQ-5D-5L instrument (0: I have no pain or discomfort; 1: I have slight pain or discomfort; 2: I have moderate pain or discomfort; 3: I have severe pain or discomfort; 4: I have extreme pain or discomfort);
Interference of pain with work and daily activities in the SF-12 instrument (During the past 4 weeks, how much did pain interfere with your normal work or other regular daily activities? 0: Not at all, 1: A little bit, 2: Moderately, 3: Quite a bit, 4: Extremely);
Self-management of pain in the Chronic Disease Self-Efficacy (CDSE-6) instrument (How sure are you that you can keep any physical discomfort or pain of your condition from interfering with the things you want to do? Visual analogic 0–10 scale).
Pain intensity was the primary outcome, and the relation with other health-related and quality-of-life variables was assessed: sleeping problems, fatigue, depression, health, physical exercise, sedentary behaviour, mental quality of life and physical quality of life (Tables 1 and 2). 54
The variables used in this study.

CV, coefficient of variation; IQR, interquartile range.
Data analysis
All data have been handled confidentially, and scientific data were stored anonymously. Statistical analyses have been performed using R version 4.0.3. 72
Correlations between the three pain variables (pain intensity, interference of pain with work and daily activities and self-management of pain) were assessed using Pearson’s correlation.
Associations between the intensity of pain and other variables were evaluated using multinomial ordinal regression models (pain intensity being an ordered factor outcome). These multivariable models were built with only those variables that had a significant effect in univariable models (p < 0.05, after correction for multiple testing using the Benjamini-Hochberg procedure 73 ). We used proportional-hazards because the sample sizes were insufficient in some levels of factor variables to be able to fit a non-proportional-hazards model.
To further describe the relations between the variables, we used another multivariable regression, with only the variables that we expected to rather cause than consequences of pain (among the variables that were significant in the univariable models), namely country, sex, education level, income, social relations, physical exercise and sedentary behaviour.
For simplification purposes, we have then repeated these analyses using as an outcome a binary variable: ‘no pain’ versus ‘non-null pain’.
We also conducted other analyses, for each variable of interest, where pain was an explanatory variable instead of the outcome (adjusting for all other available variables, when significant in univariable models). For these models, we used either logistic regression models, multinomial ordinal regression models or general linear models, depending on the nature of the outcome.
Given the high rate of missing data for the probability of having missed work during the past 4 weeks, multiple imputation was performed using the R package ‘missRanger’,74,75 which combines random forest imputation with predictive mean matching. Each imputation was weighted by the degree of missing data for each participant, such that the contribution of data from participants with higher proportions of missingness was weighted down in the imputation. We set the maximum number of trees for the random forest to 200, but left all other random forest hyperparameters at their default. Parameter estimates for all five datasets were pooled to provide more accurate estimates.
Results
Study population
A total number of 2,951 vulnerable participants distributed over the 5 European countries have been engaged. After removing caregivers (who did not have a chronic disease) and participants who attended less than four sessions or who had missing or aberrant data for the variable pain intensity (Figure 1), data were analyzed for a total of 1,371 participants with at least one chronic condition (FR 185, IT 233, NL 220 SP 402, UK 331). The average proportion of missing values across all variables in the dataset was 4.1% (excluding the probability of having missed work during the past 4 weeks, for which the proportion of missing values was 52.5%; Table 2).

Flow chart of sample selection.
Correlation between the different pain scales
The 2 × 2 Pearson’s correlation tests between the three pain variables showed that they are all significantly correlated (pain intensity with interference: p < 10−15, correlation coefficient = 0.70; pain intensity with self-management: p < 10−15, correlation coefficient = −0.44; interference with self-management: p < 10−15, correlation coefficient = −0.48). Because of the tight link between these pain variables, the following analyses have been performed on only one of them: pain intensity. Pain intensity varied across countries (Figure 2(a)). The 2 × 2 correlations between quantitative variables are represented in Figure 2(b).

(a) Pain intensity across countries (kernel density estimate). (b) Correlations’ matrices (Pearson’s coefficients) between pain intensity and quantitative variables reflecting quality of life. The areas and colours of circles represent the absolute value of correlation coefficients.
Association between pain intensity and vulnerability factors
Average income was significantly lower in participants with highest pain intensity (pain level 3 or 4; N = 240; income = 3.27 ± 1.13) than in participants without pain (pain level 0; N = 294; income = 3.66 ± 1.31; Wilcoxon rank test W = 25,187, p < 0.0001). Participants with the highest pain intensity also had less social relationships than participants without pain (pain level 3 or 4: social relationships = 3.63 ± 1.00; pain level 0: social relationships = 4.32 ± 0.80; W = 18,251, p < 0.0001). Besides, participants with pain were on average older than those without pain (5-year-age category: 8.81 ± 2.89 vs 8.32 ± 3.16; W = 164839, p = 0.01), and women had on average a higher level of pain than men (1.50 ± 1.06 vs 1.29 ± 1.09; W = 181006, p = 0.0002).
Multivariable analysis with pain intensity as the outcome (multinomial ordinal regression)
Using a multinomial ordinal regression with pain intensity as the response variable, the multivariable regression (variables being previously selected using univariable models, if p < 0.05) showed that pain significantly depended on country (p < 0.0001), sedentary behaviour (p < 0.0001), fatigue (p < 0.003), sleep problems (p < 0.0001), physical quality of life (p < 0.0001), mental quality of life (p < 0.0001) and self-perceived health (p < 0.0001; Figure 3(a)). Imputing the missing data for all variables did not significantly change the results.

Multivariable multinomial ordinal regression model, with pain intensity as the outcome. More pain on the right of the dashed line, less pain on the left of the dashed line. (a) Model including all the variables that were significant in univariable models. (b) Model including a restricted number of variables.
A simplified model was also built that included only the variables country, sex, education level, income, social relations, physical exercise and sedentary behaviour. All these variables were significant (with p < 0.0001), except income (marginally) and sedentary behaviour (Figure 3(b)). The intensity of pain was higher in France and lower in Spain than in the three other countries. Women reported more pain than men. Participants with a high education level reported less intense pain. Those with a high level of social relationships reported less intense pain. Finally, participants had less pain if they performed more physical exercise (and tended to have less pain if they had less sedentary behaviour).
Multivariable analysis with a binary pain variable as the outcome (logistic regression)
We then compared the participants according to whether they reported some non-null level of pain (N = 1070) or not (N = 294). Among participants with pain, 69.0% were women (against 56.7% among those without pain), 20.0% had a low education level (against 23.3% among those without pain) and 22.0% had a very low or low income (against 18.8% among those without pain).
Using multivariable logistic regression, we found that participants experiencing pain significantly differed according to country (p < 0.0001), had more sleep problems (p = 0.03), as well as a lower physical quality of life (p < 0.0001), and a lower mental quality of life (p < 0.05; Figure S1).
Multivariable analyses with pain as an explanatory variable
The models where pain was considered as an explanatory variable showed that it was significantly associated with: sleep problems (p < 0.0001, Figure S2), fatigue (p < 0.0001, Figure S3), probability of depression (p < 0.0001, Figure S4), self-perceived health (p < 0.0001, Figure S5), physical quality of life (p < 0.0001, Figure S6) and mental quality of life (p < 0.0001, Figure S7).
Concerning the probability of having missed work during the past 4 weeks, our logistic regression analyses showed that the intensity of pain was not significantly associated with the risk of missing work, although marginally (p = 0.06; Figure S8). If the intensity of pain was considered as a continuous variable, the intensity of pain was positively associated with the risk of missing work, but this effect was not significant either (p = 0.07). Finally, running the model on imputed datasets did not reveal a significant association with pain either.
Discussion
This multicentric study allowed a thorough characterization of the factors associated with pain and its intensity in a large sample of persons with a chronic condition among vulnerable populations in five European countries (N = 1364).
In raw data, average income was lower in participants with a higher pain intensity, and they had fewer social relationships, as compared to participants without pain. Besides, participants with pain were on average older than those without pain. Finally, women had, on average, a higher level of pain than men. Multivariable analyses, adjusting for the whole set of variables that were significant in univariable models, showed that women had more intense pain, as well as participants with a lower education level. Although the participants had been included on the basis of vulnerability criteria, these results suggest an association of pain with low education level and low income, even within vulnerable populations, and confirm the impact of socio-economic status among the determinants of pain.
A strength of this study is the rather large sample size of 1364 participants from 5 countries. Moreover, the three questionnaire items on pain were significantly correlated between them, we can therefore consider that our measure of pain intensity is reliable. There is a rather abundant literature on the link between pain and vulnerability. Significant inverse associations have been found between more severe pain and lower educational achievement.23,76,77 Similarly, pain prevalence, intensity and functional interference were repeatedly found to be higher in people with a lower income.5,76,78,79 This was also observed when comparing people living in the most deprived areas with those living in the most affluent ones. 80 Low income and manual work seem to have cumulative effects on the odds of experiencing severe pain. 78 Sickness absence at work due to pain is also inversely related to socio-economic status. 77 The mechanisms underlying this association are not yet elucidated.
In the Austrian Health Interview Survey 28 (with more than 15,000 respondents), socio-economic status (based on education, income and profession) was inversely and gradually associated with the prevalence of severe pain, with the number of indicated painful body sites, with the intensity of pain and with the subjective level of feeling disabled through pain. Moreover, even at the same intensity of pain and the same number of painful body sites, people in the lowest socio-economic class were twice to three times more likely to feel disabled through pain than people in the highest socio-economic class. Similarly, other studies have shown that people in deprived socio-economic situations not only run a higher pain and chronic pain risk but also experience their pain as more severe/disabling than their more privileged counterparts.81,82 Depressive symptoms could be one of the mediators of the relationship between socio-economic status and pain, in terms of limiting the individual’s strategies to manage pain. 83 Higher levels of subjective socio-economic status significantly predicted lower odds of participants having been prescribed at least one analgesic drug in the previous 6 months, and this was true even after controlling for objective socio-economic status variables. 84
Vulnerable people with chronic conditions should be a priority of health policy and interventions. Over the last decades, literature on both chronic care 85 and integrated care 86 have gradually recognized the importance of social determinants in shaping people’s health. Both fields acknowledge that healthcare strategies and interventions should not only consider individual factors but also people’s environment (including socio-economic determinants). It is precisely the most vulnerable people with chronic conditions who most need social and community support as well as effective and integrated care. 87 Consequently, integrated healthcare strategies should prioritize them. However, individuals from vulnerable groups are usually hard to reach.42,46,88,89 They are often reluctant to attend the care system and do not seek support through the usual channels. 90 Areas with higher vulnerability are often left out of policy innovations and experiences due to their socio-economic complexity.
Vulnerability to ill health is shaped by systemic social dynamics that lead to increased exposure to risks, heightened susceptibility to their effects and limited capacity for coping or adaptation. Therefore, public health strategies must focus on addressing the underlying social and historical factors that perpetuate poor health outcomes in disadvantaged populations. To be effective, such interventions should be intersectoral, involving collaboration across different sectors, and participatory, engaging communities and stakeholders in the process. 91 However, the specific characteristics and mechanisms needed to achieve equitable outcomes in vulnerable populations remain insufficiently explored and are also very difficult to implement. Tailored approaches are essential to meet the unique preferences and needs of these groups. For instance, targeted training programmes have demonstrated success in improving pain management and enhancing the quality of life, even among vulnerable populations. One such study, utilizing the CDSMP, revealed a positive impact on pain outcomes, providing valuable insights into addressing chronic health conditions in disadvantaged groups. 92 This reimagined approach to health inequities emphasizes systemic change, tailored interventions and active collaboration, offering a pathway to more equitable health outcomes.
Another interesting finding of this study is that participants had less pain if they performed more physical exercise, and tended to have less pain if they had less sedentary behaviour (i.e. a smaller number of hours sitting per day). This distinction between sedentary behaviour and physical exercise has already been highlighted by studies of metabolic diseases: epidemiological data showed that high volumes of sedentary behaviour are detrimental to metabolic health, even in the presence of regular exercise, 93 suggesting that the health effects of sedentary behaviour are independent of those of exercise and that daily living physical activity is beneficial. However, in our context of cross-sectional analysis, reverse causality is indeed possible (patients experiencing pain were less inclined to engage in physical activity).
Finally, it is remarkable that pain was the main predictor of sleep problems, fatigue, depression, self-perceived health, physical and mental quality of life. This is in line with other studies showing the major impact of pain on an individual’s health and life.1,5 Pain is frequent in persons with a chronic condition, 94 but the causal relation is not necessarily unidirectional. Chronic pain can increase the risk for metabolic diseases and cardiovascular diseases, 1 through an impact on physical exercise and sedentary behaviour, and through the influence of pain on blood pressure. 95 Chronic pain can also induce depression and anxiety,24,25 either directly or through negative consequences on social and professional interactions, 36 and on sleep. 1 Anxiety can, in turn, be involved in immune diseases and cancers through an impact on inflammation. 96 Indeed, although our results are consistent with other published work, we cannot assert a causal link, all these phenomena being interconnected and interdependent.
In addition, it is important to recognize certain limitations of our study. The primary limitation lies in focusing on individuals with pre-existing chronic diseases rather than including any individual in a vulnerable situation. However, persons with any chronic condition have been included indiscriminately, as well as persons with diverse vulnerability criteria, and this is an originality of this research: the vast majority of other pain studies focus on a specific disease or a specific population, and are therefore difficult to generalize. Second, our results may not be generalizable outside the European context. Third, the absence of information on the type of chronic condition (articular, digestive, metabolic, etc.) is a weakness of this protocol, because these entities encompass a great diversity. Moreover, other useful information is missing, such as the height and body weight of participants, their ethnic/cultural background or the use of painkillers. Finally, the absence of a control group precludes a comparison between chronically ill patients with and without vulnerability criteria, which would have provided deeper insights into the specific impact of vulnerability on pain manifestations and their underlying determinants.
Overall, our results confirm the social component in the complex aetiology of pain. Decreasing social inequalities and vulnerability could clearly reduce the prevalence of pain,41,97 whereas managing pain would also reduce the risk of vulnerability. 36 Taken globally, these considerations clearly plaid in favour of integrated care, taking into account the patients’ individual characteristics and environment.
Supplemental Material
sj-docx-1-taj-10.1177_27558428251336656 – Supplemental material for Pain in vulnerable people with chronic conditions: a multicentric cross-sectional study
Supplemental material, sj-docx-1-taj-10.1177_27558428251336656 for Pain in vulnerable people with chronic conditions: a multicentric cross-sectional study by Charlotte Faurie, Demi Cheng, Claire Duflos, Liset Elstgeest, Rosanna Ferreira, Hein Raat, Verushka Valsecchi, Alberto Pilotto, Graham Baker, Marta M. Pisano and Yves-Marie Pers in Sage Open Chronic Disease
Footnotes
Acknowledgements
All the participants are warmly thanked for their investment. This is ISEM contribution 2025-065.
Ethics approval and consent to participate
The study follows the directives of the Helsinki Declaration and the corresponding ethical regulations are being respected at each study site. The protocol was approved by the French ethics committee (Comité de Protection des Personnes Sud-Ouest et Outre-Mer I, study number 9788), the Regional Ethics Committee of Liguria (study number 152-2018), the Medical Ethics Review Committee of the Erasmus University Medical Center, Rotterdam (Medical Ethics Review Committee-2017-1116) and by the Research ethics committee of the Principality of Asturias (study number 20/17). In the United Kingdom, the Health Research Authority was consulted, and it was concluded that approval from an ethics committee was not necessary. Participants provided written consent for publication before enrolment.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the European Union’s Health Programme (2014-2020; EFFICHRONIC 738127).
Competing interests
The authors declare that there is no conflict of interest.
Availability of data and materials
Not applicable.
Supplemental material
Supplemental material for this article is available online.