
Abstract
This critical review considers the status of 21st-century epidemiological theories of disease distribution, updating to 2024 prior analyses published up through 2014, and discusses the implications of these theories for research, practice, and pedagogy. Three key trends stand out: (a) the continued dominance of individualistic biomedical and lifestyle theories; (b) growth and elaboration of social epidemiological alternatives; and (c) the ongoing inattention to epidemiologic theories of disease distribution in the training of epidemiologists and public health professionals and in current efforts to improve the rigor of epidemiological research and causal inference. In a context of growing global political polarization, climate crisis, broader environmental and ecological crises, and stubbornly persistent health inequities within and between nations, producing actionable knowledge relevant to improving the people’s health and advancing health justice will require much greater engagement with social epidemiologic theories of disease distribution in research, pedagogy, and practice. At issue is critically engaging with the embodied truths manifested in the stories bodies tell in population patterns of health, disease, and well-being.
Keywords
Who and what explains the people’s health—that is, the embodied truths manifested in the stories bodies tell in population patterns of health, disease, and well-being
Moreover, as the phenomena of population health are dynamic and historically contingent, varying by time, place, and social group, so too are epidemiological theories of disease distribution. This variation exists for multiple reasons, which are relevant to any science, not epidemiology alone: there are changes in what needs to be explained, changes in technology, new discoveries, and changes in who does science1–3.
Hence, keeping abreast of changes in and contentions between diverse epidemiologic theories of disease distribution is as necessary as keeping up with methodological developments and discoveries in the field. In a context of global upheaval tied to climate crisis, broader environmental and ecological crises, COVID-19, mounting wealth inequities, and rising political polarization, this critical review accordingly provides a status update on the present state of contending epidemiologic theories of disease distribution, both dominant and alternative—and their implications for research, practice, and pedagogy.
Search Strategy
The search strategy for this critical review drew principally on literature searches I conducted between January and July 2023 to prepare the second edition of my book Epidemiology and The People’s Health: Theory and Context 1 ; it also is informed by the literature searches I conducted for prior critical reviews on the topic, published in 1994 4 , 2001 5 , and 2014 6 . For the book revision, I conducted a new literature search for each paragraph in the text to see if new literature addressed the points covered or if the cited authors had published new work on the topic; the databases included PubMed, Web of Science, Google Scholar, SCIELO, and the Harvard library HOLLIS systems (for books as well as articles). Second, I expanded the scope of the literature search (using the same databases) for new areas of work and conceptual frameworks that were either nascent or nonexistent at the time of preparing the first edition of the book (which I researched between 2008 and 2010, building on my scholarship in the area dating back to the late 1980s).
Selection Criteria
The literature cited in this critical review draws chiefly on the nearly 2,500 references included in the second edition of Epidemiology and The People’s Health: Theory and Practice 1 . The selected books and articles cited provide exemplars of the specified theories of disease distribution and their application.
Big Picture: Continuities and Some Notable Changes
Succintly stated, over the first quarter of the 21st century, the biomedical and lifestyle theories of disease distribution remain the dominant theories employed, as they were in the 20th century, and alternative social epidemiologic theories of disease distribution have expanded (see Textbox 1; 1, 6). Evidence supporting this statement based on data from the National Institute of Health (NIH) and PubMed is provided in Table 1.
Scientific prominence: active NIH funding (for July 2013* and for 2014–2022) and article citations in PubMed (for 2003–July 2013* and for August 2013–August 2022) for dominant theories (biomedical and lifestyle) and social epidemiologic alternatives.
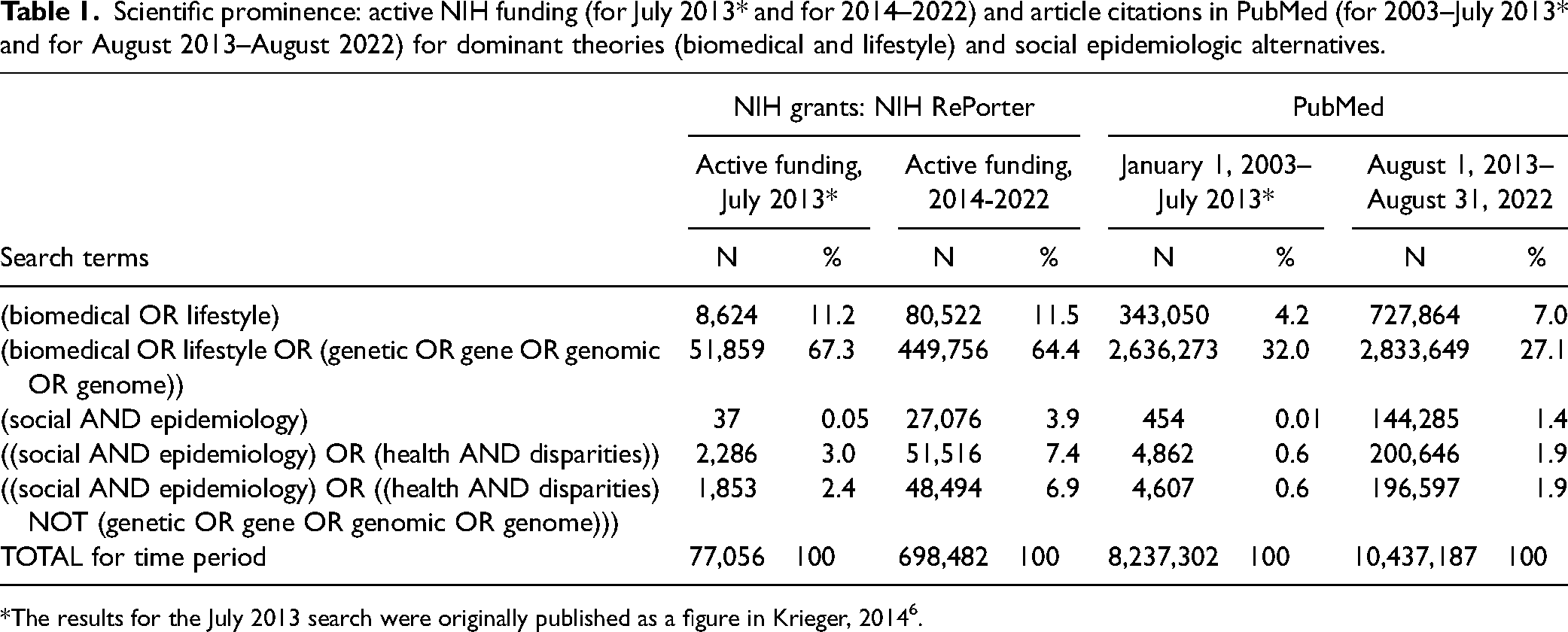
*The results for the July 2013 search were originally published as a figure in Krieger, 2014 6 .
Searching for terms employed in NIH grants and in PubMed or other databases can only offer a rough picture of funding and publication priorities; still, the crude picture is compelling. More nuance is provided by a study focused on racism and health that analyzed articles published in four of the world’s leading medical journals between 1990 and 2020 (The Lancet, JAMA, New England Journal of Medicine, British Medical Journal) 7 . Attesting to their gross neglect of work on this highly salient topic, among the 226,305 items published by these prestigious journals, only 1,213 (0.5%) included the term “racism,” of which over 90 percent were commentaries, viewpoints, or letters—not empirical research articles. Of these, the vast majority appeared in 2020, triggered by the onset of the COVID-19 pandemic and the brutal murder of George Floyd by police on May 25, 2020 7 .
New Developments in the Complementary Dominant Biomedical and Lifestyle Theories of Disease Distribution
New 21st-century developments in the dominant theories used in epidemiological research and applied in population health are well captured by their proponents’ designated terms: precision medicine, lifestyle medicine, and the developmental origins of health and disease framework 1 .
Initially termed personalized medicine and now increasingly called precision medicine8,9, this new field has a foundational basis in genomics and advances in big data science. Its premise is that precise knowledge of a person’s genome plus other molecular information spanning the full range of the “omics” will enable more precise diagnosis, clinical treatment, and prevention, at not only the individual but also the population level8,9. In 2015, the corresponding term precision public health was coined to refer to “1) applying emerging methods and technologies for measuring disease, pathogens, exposures, behaviors and susceptibility in populations; and 2) developing policies and targeted public health programs to improve health” 10 .
According to proponents of precision medicine, the chief obstacle to precise medical care, including preventive medicine, is inadequate information on individuals, commencing with their genomes8,9. Proponents of precision public health10,11 in turn consider key impediments to be “the immaturity of (a) data and (b) analytics” 10 . By contrast, more critical assessments of the promises and pitfalls of precision medicine and precision public health have pointed to problems of power and resources; a core component of the critique is that data, however important, by themselves have never been an antidote to entrenched inequities in exposures and resources shaping individuals’ health status and health care12,13.
The formal emergence of the field of lifestyle medicine has paralleled that of precision medicine. As clearly stated in the lead editorial in the 2007 inaugural issue of the American Journal of Lifestyle Medicine, its theoretical standpoint holds that the “epidemic of inactivity, obesity, poor nutritional habits, cigarette smoking, and other negative behaviors is driving most disease in the industrialized world” 14 , p. 7) and that “[w]hen it comes to the impact of lifestyle medicine on health, perhaps the cartoon character Pogo best summarized the problem when he stated, ‘We have met the enemy and he is us’” 14 , p. 9). The foci remains individual-level health behaviors, as elaborated variously in conceptual essays14,15, epidemiologic analyses, meta-analyses 16 , and even prescriptions for “planetary health” 17 . The societal and ecological context in which individuals make their “choices” is treated as a given, with individuals advised to make the healthiest choices possible14–17.
The impact of these dominant theories is likewise evident in the 21st-century developmental origins of health and disease (DOHaD) paradigm, which is primarily focused on the impact on adult disease risk of what was initially termed “fetal programming” 18 and then expanded to the “first 1,000 days of life” ( 19 , p. 1); the field’s first journal was founded in 2010 20 . Indicative of its approach, a 2019 DOHaD article by senior authors in the field included a section on “policy interventions” that declared, “measures such as reducing the rates of gestational diabetes and promoting breastfeeding can minimize the prevalence of evolutionary mismatch, while promoting prudent maternal nutrition from prior to conception and throughout pregnancy is likely to reduce the risk of developing erroneous PARs [predictive adaptive responses]” ( 21 , p.1), yet the authors provided no specifics as to what such policies would entail.
Hence, in a context of important 21st-century advances in work on myriad -omics and in data science, these dominant theories of disease distribution notably continue to focus predominantly on individual-level mechanisms of disease causation (spanning from the organism-level down to sub-molecular), defined principally in relation to genetics and behavioral “choices” 1 . The locus of action remains centered on medical interventions, dominated by private health care and life sciences industries1,12,13.
New Trends in Social Epidemiologic Sociopolitical Theories of Disease Distribution
Concomitantly, work on and use of alternative social epidemiologic theories of disease distribution has been on the rise, despite garnering only a miniscule fraction of the resources and attention commanded by adherents of the dominant theories of disease distribution1,2,6,22,23. Three notable new trends in the 21st century involving the sociopolitical group of social epidemiologic theories of disease distribution include: (a) the rise and subsequent depoliticization of social determinants of health (SDOH); (b) a renewed emphasis on the political economy of health, combined with new framings of political, commercial, and societal determinants of health; and (c) the rising visibility of Latin American social medicine-collective health, including in English-language literature 1 . Other sociopolitical theories of disease distribution continue to be employed in the 21st century, including health and human rights, fundamental cause, and population health1,2,6.
Also germane is the rising influence in epidemiology—and in public health more broadly—of two frameworks coming from outside of these fields: intersectionality24,25 and decolonization26,27. Introducing ideas relevant to analyzing population health, it is important to recognize that these frameworks were not intended to analyze explicitly how social conditions affect people’s biology and health status, including on what timescales, and involving what social and biological pathways. Instead, their critical contribution is to offer conceptual tools to analyze and challenge the intertwined adverse impacts of injustice in multiple domains (not health alone), as shaped by past and present power relations involving both societal systems (including colonialism, settler-colonialism, enslavement, capitalism, and imperialism) and the social groups forged by these systems (involving social relations of social class, racialized groups, gender, sexuality, nationality, Indigenous status, immigrant status, disability status, and more, singly and combined; 1,2,24–28). A growing number of social epidemiologic books, conceptual articles, and empirical studies invoke these frameworks when presenting their analysis of causal processes driving health inequities and interventions to advance health justice, including reproductive, environmental, and climate justice1,2,28–32 while also drawing on social epidemiologic theories of disease distribution to explicate the specific types of exposures, etiologic periods, and social and biological pathways at issue. The rising number of such publications suggests this trend of increasing influence will continue 1 .
Social Determinants of Health
In 2008 the World Health Organization (WHO) held its inaugural global conference on the social determinants of health, whose materials drew extensively on decades of social epidemiologic theorizing and empirical research1,33. A PubMed search readily revealed ( 1 , p. 121; 34 ) that the search term social determinants of health identified only one article for the years 1980–1989 and 18 articles for 1990–1999. For 2010–2019 the number jumped to 9,227, and for 2020–2022 the number equaled 11,035 articles ( 1 , p. 121; 34 ). Usage of the SDOH framework has been explicitly embraced by numerous influential global and national health agencies and, bridging public health practice and academia, is increasingly included in both policy documents and textbooks1,33,35–37. One characteristic feature in contrast to the DOHaD framework is to accord explicit attention to the societal context—and specific socially patterned exposures—that people are exposed to, and to do so across the life course1,5,22,23,35–37. not solely from conception to the “first 1,000 days of life” ( 19 , p.1). An explicit goal of the SDOH framework is to produce knowledge that can advance policy and action to improve the contexts in which people are born, live, work, play, ail, and die32,34–36.
Suggesting, however, that some recalibration of the SDOH framework may be underway, during the decade after its rise to prominence, the 2019 report by the Pan American Health Organization (PAHO) on Just Societies: Health Equity and Dignified Lives notably altered the WHO’s Commission on Social Determinants of Health (CSDH) 2008 model to lead with explicitly labeled “structural drivers” and included “more emphasis on colonialism, structural racism, and the importance of relationships to land” along with “the environment and climate change; human rights; and inequities according to gender, ethnicity, sexual orientation, life stage, and disability” ( 37 , p. 2249). Related, in 2023, the editors of the newly renamed International Journal of Social Determinants of Health and Health Services argued against what they termed “the unfortunate meaning, still common in reports and conferences, whereby SDOH becomes a list of individualized ‘risk factors’” ( 38 , p.118), while nevertheless noting that “SDOH remains a useful umbrella term to capture the political, economic, cultural, and ecological determinants of health” ( 38 , p.117).
Political and Commercial Determinants of Health
Also indicative of concerns about the rise of depoliticitized social epidemiologic frameworks, distanced from their roots in analyses of the political economy of health 1 , are new calls, since 2012, for work on both the political determinants of health38–46 (a topic first discussed explicitly in epidemiology literature in the 1980s; 1 ) and the corporate or commercial determinants of health38–40,47,48 (drawing on prior decades of work on the political economy of health; 1,6,22,23,38–40). Examples of new theorizing and empirical analysis in political epidemiology address the following: how democratic governance or its suppression or corruption is associated with population rates of health outcomes and health inequities40–44; the health impacts of sociopolitical stressors (e.g., campaign rhetoric and policies that target and dehumanize marginalized social groups) 45 ; and how political ideologies of politicians and their constituents (sometimes delimited by processes involving gerrymandering) affect population health profiles42,46. In part spurred by the near collapse of the U.S. banking industry in 2008 and the global recession thereby triggered1,40,43,49, and by broader work critiquing neoliberalism, market fundamentalism, and the concomitant privatization of public goods and erosion of democratic governance1,39,40,43,47–49, work on commercial determinants of health builds on decades of prior research exposing the adverse and inequitable health impacts of corporations and governments that prioritize shareholder value and private profits above all else1,39,40,43,47–49. Auguring further refinement of ideas and evidence is both the growing engagement of political scientists, in part spurred by the COVID-19 pandemic and by the growing impacts of political polarization on population health42–44, and the debates over whether work on the commercial determinants of health should focus on harmful commodities versus all commercial activities versus capitalism per se39,43,47,48, with some of this latter work distinguishing between different “varieties” of capitalism—that is, different types of welfare states 43 and other work referring to “capitalism” overall39,40,47,48. Attesting to the rising prominence of work in this area, in 2023 the WHO announced it will host its first global conference on the commercial determinants of health 50 .
Latin American Social Medicine-Collective Health and the Social Determination of Health
Also noteworthy is the growing influence of the varied theories of disease distribution termed Latin American Social Medicine and, in Brazil, collective health, which together emphasize what these theories term the social determination of the health-disease-care process and call for the practice of “critical epidemiology”1,51,52. In the 21st century, these theories have become increasingly visible in and beyond Latin America1,51,52 and have begun to engage more explicitly with Indigenous health and Indigenous frameworks, while also expanding their focus on environmental integrity1,51.
Reflecting in part different sociopolitical contexts, Latin American Social Medicine-Collective Health (LASM-CH) theoretical work has differed from most of the English-language social epidemiologic theories in several ways1,51,52. First, it has devoted more attention to the impact of capitalist development, imperialism, and politics on health1,51. Second, it has elevated critiques of biomedical positivism, structural functionalism, and their joint focus on static “risk factors” and “outcomes”1,51,52. Third, it has objected to the phrase “social determinants of health” because it is held to obscure who is doing the determining of (i.e., is causing and accountable for) the relevant exposures and, in effect, reducing these “social determinants” to “risk factors;” as an alternative, they focus on the social determination of what was initially termed the health–illness process, and then later the health–illness–care process1,51,52. Another difference stems from the histories of Latin American military dictatorships and oligarchies and the coercive power of the state, leading LASM-CH to emphasize the critical importance of collective action by non-state actors—that is, collectivities and social subjects, such as social classes and popular movements—to shape and improve population health and health equity via democratic empowerment of the people1,52. As societal conflicts over the meaning and exercise of economic and social democracy continue to grow in a context of increased strife tied to climate crisis and ecological degradation, the influence of LASM-CH will likely continue to rise1,51,52.
New Foci in Psychosocial Theories of Disease Distribution
During the 21st century, the focus of the social epidemiological psychosocial theories of disease distribution has remained on individuals’ brain-mediated psychological perceptions of—and their health-damaging or health-enhancing responses to—social conditions, social interactions, and social status1,5,22,23,36. What has become increasingly prominent, however, is use of the constructs of “allostasis” (first proposed by Sterling and Eyer in 1988 ( 53 , p.631; 54 ), and measurement of “allostatic load” (first proposed by McEwan and Stellar in 1993; 55,56).
The idea of allostasis refers to regulatory systems that achieve “stability through change,” using “feed-forward control from the brain to prevent errors” ( 54 , p.169; emphasis appears in the original), and stands in contrast to the dominant notion of homeostasis, primarily conceptualized as being error-correcting feedback ( 54 , p.169). As argued by Sterling in 2020, the model of allostasis thus “clarified why the brain should be in charge: it is simply more efficient to predict a need to satisfy it than to wait for an error and correct it” ( 54 , p. xi). Allostatic load in turn refers to “wear-and-tear from chronic over-activity or underactivity” of systems “that protect the body by responding to internal and external stress,” as measured by biomarkers pertaining to the functioning of “the autonomic nervous system, the hypothalamic-pituitary-adrenal (HPA) axis, and cardiovascular, metabolic, and immune systems” ( 56 , p.171). Elaborated since—especially with reference to early life exposures, cumulative disadvantage across the lifecourse, and psychoneurobiology1,22,23,36,54—the concepts of allostasis, allostatic state, and allostatic overload, along with their associated metaphors of imbalance, have increasingly informed 21st-century epidemiologic psychosocial ideas and research. For example, 76 percent of the 5,426 Web of Science entries indexed using these three terms have been published in the past decade (i.e., since 2013) 57 . Notably, alongside this increased focus on allostatic load as either outcome or mediator, the emphasis remains on psychological pathways and mechanisms, not on who and what socially structures the relevant patterns of exposures or precipitates the anticipatory activation of physiological responses to psychosocial stimuli1,6.
New Advances in the Ecosocial Theory of Disease Distribution
The ecosocial theory of disease distribution, which I first proposed in 1994 and have elaborated since (1,2,4–6,28; see Figure 1) currently stands as the most systematically articulated and widely-used social epidemiological theory of disease distribution in literature published in English that engages with societal (including structural), biological, and ecological phenomena, at multiple levels across the lifecourse and historical generation (1,2,58,59; see Textbox 2). New developments include conceptualizing health outcomes as emergent embodied phenotypes1,2,60 that, through their population distributions, reveal embodied truths that are actionable in both courts of law and in the court of public opinion—hence they are relevant to fostering change for health justice1,2,28. Core constructs and theses of the ecosocial theory of disease distribution are provided in Figure 1 and Textbox 2, respectively. Recent examples of the theory’s application both empirically and conceptually, published in the last five years (i.e., since 2019) are provided in Supplemental Textbox 1, with the theory increasingly used to guide work conducted in multiple continents on frameworks for understanding health inequities; cancer; reproductive health; mental health; impacts of racism on health outcomes, health behaviors, and health care; substance use; policing, carceral systems, and health; HIV care and outcomes; COVID-19; and climate change, political ecology, and health equity, articulated in relation to occupational and environmental health, environmental justice, and planetary health. Together, these growing applications and extensions of the ecosocial theory of disease distribution may well have the potential to take epidemiology to a new level—literally.
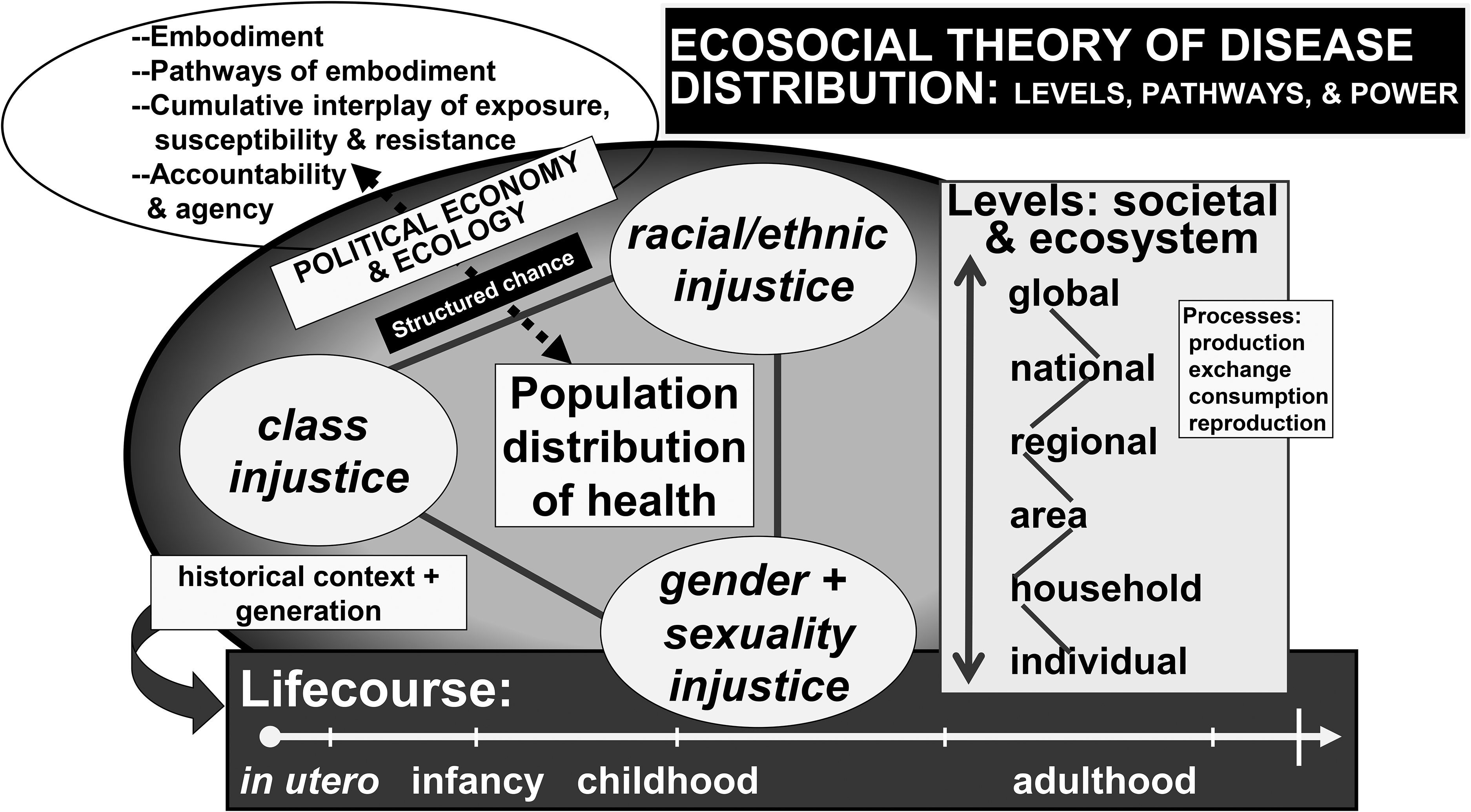
Core features of the ecosocial theory of disease distribution.
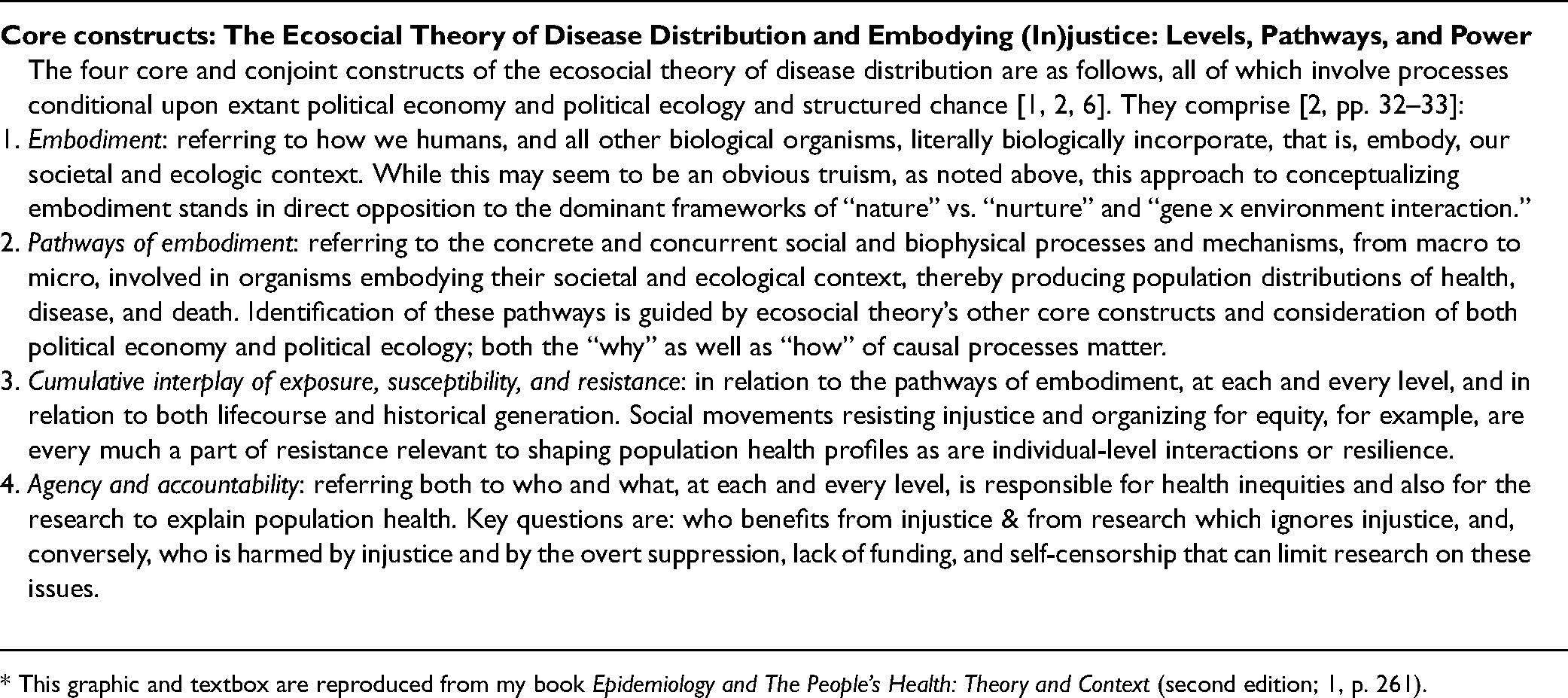
* This graphic and textbox are reproduced from my book Epidemiology and The People’s Health: Theory and Context (second edition; 1, p. 261).
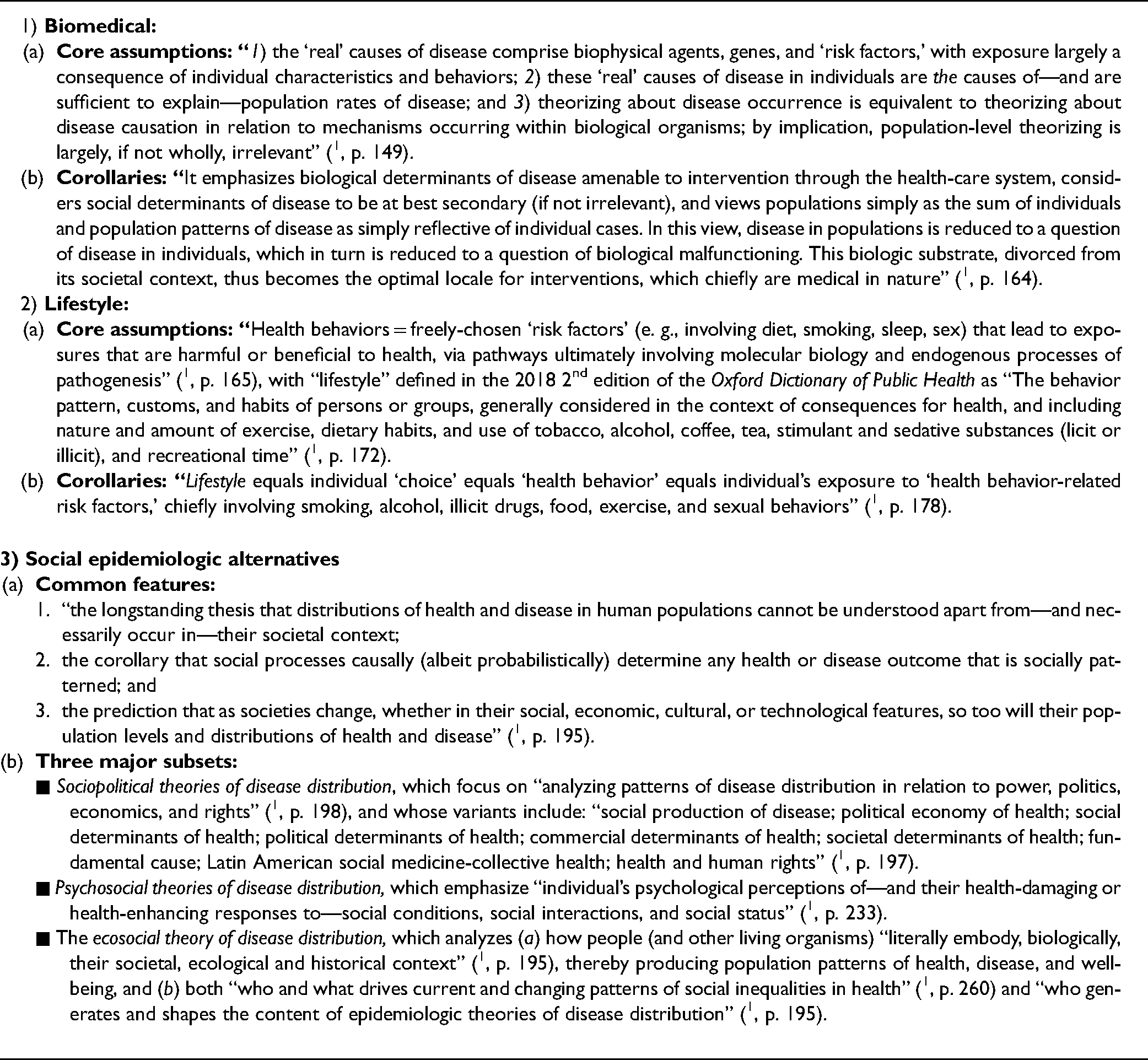
Core features of the dominant epidemiologic theories of disease distribution—biomedical and lifestyle—and the social epidemiological alternatives1,2,4–6.
Ecosocial theory of disease distribution: emergent embodied phenotypes, and embodied truths of health (in)justice: 11 theses*.
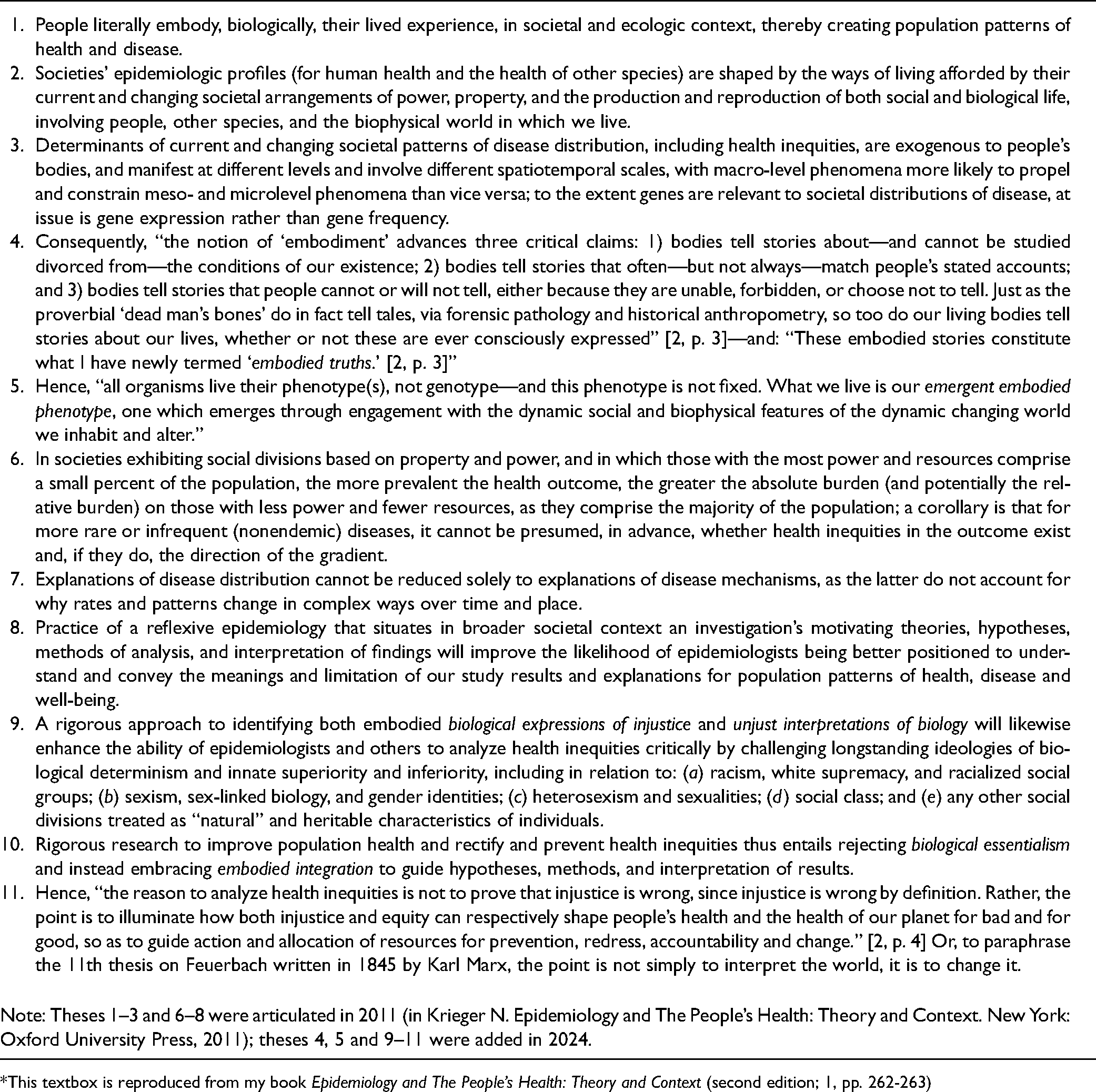
*This textbox is reproduced from my book Epidemiology and The People’s Health: Theory and Context (second edition; 1, pp. 262-263)
Problematic Paradox: A Continued Resounding Silence on the Importance of Epidemiologic Theories of Disease Distribution for Rigorous Research, Training, And Action
Yet, despite the growth and vitality of theorizing and empirical research premised on the social epidemiological alternative theories of disease distribution1,2,6,22,23,35–60 biomedical and lifestyle theories problematically remain the dominant influences on epidemiologic training and research (1,6; see Table 1).
Not only do contemporary epidemiologic training and textbooks still include very little critical discussion of epidemiological theories of disease distribution, their history, content, and application 1 , but similar omissions plague current recommendations for improving graduate education and training in epidemiology worldwide61–63. A global survey of applied epidemiologists based in 64 countries in 2019–2020 failed to ask any questions about the training these epidemiologists had received in epidemiological theories of disease distribution; by contrast, extensive questions were asked about the range of methods learned 63 . Revealingly, however, when summarizing the free text entry responses, the study authors noted the theme of more “training with a focus on cultural, political, and contextual understanding was needed” 63 . Similarly, within the United States, a 2015 review sponsored by the American College of Epidemiology noted that the training of epidemiologists insufficiently addressed what they termed the “‘upstream’ causes of disease” and the “broader societal factors that shape population health” ( 61 , p. 463). A follow-up report issued in 2017 remained silent on the need for training in epidemiologic theories of disease distribution 62 .
Additionally, 21st-century guidelines to improve the rigor of epidemiologic research continue to ignore the impact of epidemiological theories of disease distribution. Illustrating this problem are the original STROBE (“STrengthening the Reporting of Observational Studies in Epidemiology”) guidelines, first published in 2007, along with their updates and many extensions 64 . None of the STROBE guidelines include any mention of the relevance of epidemiologic theories of disease distribution for framing, critiquing, or improving study hypotheses, methods, or interpretation of findings. Thus, while the guidelines do call for hypotheses to be clearly stated, they are silent on recommending that researchers state the epidemiologic theories of disease distribution that inform the hypotheses being proposed, let alone how the findings are interpreted and contextualized.
The neglect of attention to epidemiologic theories of disease distribution is also evident in the 21st-century “causal revolution,” as designated by its proponents 65 , to improve methods for causal inference that is sweeping across epidemiology and other disciplines. From the outset, the singular focus has been on quantitative methods to analyze data, variously obtained from observational and experimental studies and mined for “machine learning” from “big data” sources, in order to identify causal effects 65 . However, even though early on epidemiologists vitally involved in this work recognized the crucial role of “background knowledge” 66 for understanding and correctly modeling the causal processes at play, there remains total silence about the role of epidemiological theories of disease distribution in shaping this “background knowledge,” let alone who and what structures this knowledge65–67.
Not surprisingly, such theoretical stances have spurred considerable controversy and debate led by epidemiologists explicitly trained in and employing social epidemiologic theories of disease distribution, who are appreciative of the methodological advances but leery of how they are being deployed68–71. These sharp exchanges have led to some backpedaling of initial claims that social epidemiologic research lies outside of the bounds of rigorous sciences that use causal inference methods72,73. It has likewise spurred new work explicitly informed by epidemiologic theories of disease distribution to improve use of causal inference methods in social epidemiology and to show the harms to causal inference posed by research that ignores the actual societal and ecological contexts in which people are born, live, ail, and die69–71,74.
Consequently, in a context of continued dominance of biomedical and lifestyle theories of disease distribution, the bulk of epidemiologists, both in the field and those being trained, are left to their own devices, free to populate myriad causal diagrams and webs with undertheorized assorted “variables,” as if hypotheses were independent of theoretical frameworks, and as if approaches to causal theorizing about determinants of population distributions and risk of disease are either self-evident, requiring no analysis, or else simply a matter of idiosyncratic inspiration (or ideological proclivities) 1 . If, however, transparency of assumptions is vital for valid scientific research, then explicit attention to epidemiologic theories of disease distributions is essential for the field—and as this article and the scholarship it cites make clear, the cost of ignoring these theories can be high, whether measured in wasted effort or, more profoundly, in people’s lives.
A Wake-Up Call
In closing, it is time—past time—for epidemiologists and others in public health to take stock and reject the status quo 1 . As climate crisis grows, as environmental and ecosystem degradation worsens, as health inequities stubbornly persist within and between nations, and as new evidence makes clear the myths of inevitable “epidemiologic transition” and ever-improving population health1,2,6,22,23,28–32,36–40,47,48,51,58,59 (take, for example, the recent trends of alarming declines in life expectancy in the United States, in a context of already much worse mortality and morbidity rates compared to many other wealthy industrialized nations; 75,76), it is clear that biomedical and lifestyle theories of disease distribution are not up to the task of confronting these challenges.
The continued dominance of these individualistic theories is inexcusable; the vital alternatives provided by diverse social epidemiologic theories of disease distribution offer more promise. But these social epidemiologic theories of disease distribution cannot be purely “social” or “social ecological” or be concerned solely with socially-defined “fundamental causes”1,2. Instead, they must engage, vitally, with the biophysical realities of life on this planet—as necessitated by the health impacts on humans and other species whose lives are causally interconnected, of mounting socially-structured ecological and environmental crises, both independent of and intertwined with climate crisis1,2,38,48,49,51,77,78. As emphasized by the ecosocial theory of disease distribution, taking on this challenge requires engaging with political ecology as much as it does with any notions of “social ecology”—and this joint reckoning with how we and other organisms embody our societal and ecological context, shaped by political economies spanning from global to local, is fundamental, causally, for understanding, analyzing, and working to change population patterns of health among humans and other species ( 1 , pp. 290–292).
Underscoring these points, since 2010, impelled both by climate change and, since the 2020 COVID-19 pandemic, conceptual and empirical research has been published in public health journals that explicitly draws on political ecology in conjunction with the ecosocial theory of disease distribution ( 1 , pp. 290–292). Conceptually, this work has sought to sharpen the critical political economy (and typically anti-capitalist) focus of research and interventions addressing links between climate change, ecological degradation, and the health of people and other species, alongside new work in social epidemiology renewing critical attention to the political, economic, and commercial determinants of health1,2,38,51,77–81. One focus of this work has been to develop explicit critiques of the lack of attention in the “One Health” and “planetary health” literature to political economy, health inequities, and Indigenous knowledge51,79–81. Other theoretical efforts have sought to clarify the overlaps and distinctions between “occupational and environmental health; political ecology of health; environmental justice; ecohealth; One Health; ecological public health; and planetary health” ( 80 , p. 420). Together, this conceptual and empirical research, drawing on political ecology and combined with further systematic articulation and application of the ecosocial theory of disease distribution, can strengthen the reach and rigor of the work epidemiologists do. Especially in this era of global climate change and fierce battles for climate and environmental justice, the stakes could not be higher for apt use of theory to get the questions and answers right regarding who and what is causing, and can change, the epidemiologic profiles of both people and other species.
By making conscious use of epidemiologic theory and having informed debates over the different epidemiologic theories of disease distribution at play, those of us who are epidemiologists or other public health professionals and advocates more broadly stand a better of chance of producing epidemiologic knowledge that reveals embodied truths that unmask accountability for the state of the people’s health and health inequities1,2. Such knowledge is essential for all engaged in the multisectoral, multigenerational work to prevent disease, improve population health and health equity, and advance health justice.
Supplemental Material
sj-docx-1-joh-10.1177_27551938241269188 - Supplemental material for Theorizing epidemiology, the stories bodies tell, and embodied truths: a status update on contending 21st c CE epidemiological theories of disease distribution
Supplemental material, sj-docx-1-joh-10.1177_27551938241269188 for Theorizing epidemiology, the stories bodies tell, and embodied truths: a status update on contending 21st c CE epidemiological theories of disease distribution by Nancy Krieger, PhD in International Journal of Social Determinants of Health and Health Services
Footnotes
Declaration of conflicting interests
The author declares there is no conflict of interest.
Declaration of funding
This work was supported in part by the author’s American Cancer Society Clinical Research Professor Award; the funder had no role in study design, data collection, data analysis, data interpretation, or writing of this article.
Correction (August 2024):
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.