
Abstract
Objective
COVID-19 disproportionately affects racial/ethnic minority groups in the United States. We evaluated characteristics associated with obtaining a COVID-19 test from the Veterans Health Administration (VHA) and receiving a positive test result for COVID-19.
Methods
We conducted a retrospective cohort analysis of 6 292 800 veterans in VHA care at 130 VHA medical facilities. We assessed the number of tests for SARS-CoV-2 administered by the VHA (n = 822 934) and the number of positive test results (n = 82 094) from February 8 through December 28, 2020. We evaluated associations of COVID-19 testing and test positivity with demographic characteristics of veterans, adjusting for facility characteristics, comorbidities, and county-level area-based socioeconomic measures using nested generalized linear models.
Results
In fully adjusted models, veterans who were female, Black/African American, Hispanic/Latino, urban, and low income and had a disability had an increased likelihood of obtaining a COVID-19 test, and veterans who were Asian had a decreased likelihood of obtaining a COVID-19 test. Compared with veterans who were White, veterans who were Black/African American (risk ratio [RR] = 1.23; 95% CI, 1.19-1.27) and Native Hawaiian/Other Pacific Islander (RR = 1.13; 95% CI, 1.05-1.21) had an increased likelihood of receiving a positive test result. Hispanic/Latino veterans had a 43% higher likelihood of receiving a positive test result than non-Hispanic/Latino veterans did.
Conclusions
Although veterans have access to subsidized health care at the VHA, the increased risk of receiving a positive test result for COVID-19 among Black and Hispanic/Latino veterans, despite receiving more tests than White and non-Hispanic/Latino veterans, suggests that other factors (eg, social inequities) are driving disparities in COVID-19 prevalence.
In the United States, the COVID-19 pandemic disproportionately affects racial/ethnic minority groups and people experiencing structural inequality. 1 -4 People of color have an increased risk of COVID-19 infection because they face adverse social determinants of health (SDH), such as living in areas with high-density housing and high poverty rates and relying on public transportation or working in nonrelocatable occupations that prevent social distancing. 3,5 -9
As the largest integrated health care system in the United States, the Veterans Health Administration (VHA) provides subsidized or free health care to veterans. 10,11 Although financial barriers to care are lowered at the VHA, veterans are not immune to the negative effects of the SDH they face outside the VHA. Equitable access to high-quality health care for all veterans is a cornerstone of the VHA’s health care mission. As such, identifying potential disparities in the VHA health care system is of paramount importance. A 2020 report found that Black and Hispanic veterans have an increased burden of COVID-19 that is not explained by underlying chronic conditions or where they receive care. 2,4 We examined potential disparities in COVID-19 testing and test positivity among veterans as part of an ongoing quality assessment to better understand this population and areas in which to focus data-informed improvement efforts.
Methods
Data Source and Study Population
We conducted a retrospective cohort analysis of veterans in active clinical care at the VHA using data from the VHA’s national electronic health record repository. We defined active clinical care as having 1 or more outpatient clinical encounters from January 1, 2018, through December 31, 2019. We excluded veterans if they died before January 1, 2020 (n = 381 561), were aged <18 (n = 53) or >115 (n = 6), or had missing data on date of birth (n = 1), demographic covariates of the VHA enrollment priority group (n = 18 938), or urban/rural status (n = 16 357). The final analytic cohort comprised 6 292 800 veterans.
Outcomes: COVID-19 Tests and Results
We examined 2 outcomes: (1) receiving a COVID-19 test in the VHA and (2) receiving a positive test result for COVID-19. We identified veterans tested for COVID-19 using a text-search algorithm of VHA laboratory records for SARS-CoV-2 polymerase chain reaction tests between February 8, 2020 (the first recorded test in the VHA), and December 28, 2020, as previously described. 2,4 We excluded tests with inconclusive results. Among veterans with multiple tests, we used their first negative test result if they never had a positive test result and their first positive test result otherwise. We did not include third-party tests (ie, tests ordered by public health departments).
Veteran Demographic Characteristics and Comorbidities
We retrieved data on age, sex, race, ethnicity, marital status, urban/rural status, priority group, and geographic region from the VHA’s electronic health record database. We defined race and ethnicity using the most common self-reported value and geographic region by VHA service districts. 11 We defined urban and rural areas using the US Census Bureau’s 2010 classification criteria. 12 We further defined highly rural areas as areas having a population density <7 people per square mile. 11 VHA priority group is an enrollment system that enrolls veterans into VHA care on the basis of service-connected disability rating, income, recent military service, and other factors. 11 We defined priority group in this analysis by 4 categories: high-disability veterans, low-/moderate-disability veterans, low-income veterans, and veterans with no service-related disability, as defined previously. 13
We used the Charlson Comorbidity Index without age as a proxy for patient comorbidities at baseline. 14,15 We defined each condition in the Charlson Comorbidity Index using relevant International Classification of Diseases, Tenth Revision codes 16 retrieved from health care encounters from January 1, 2018, through December 31, 2019, such that all comorbidities preceded COVID-19 testing.
VHA Facility Characteristics
VHA facility-level covariates included population demographic factors: sex (female/male), ethnicity (Hispanic/Latino, non-Hispanic/Latino), rural/urban (highly rural, rural, urban), race (White, Black/African American, Asian, American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander), age (18-24, 25-34, 35-44, 45-54, 55-64, 65-74, 75-84, ≥85), and marital status (divorced/separated/widowed, single, married). We defined VHA facility as the VHA medical center location (N = 130) where the patient was assigned a primary, mental health, specialty, or other care team. For patients with multiple care teams, we determined the facility in ranked order (primary, mental health, specialty, and other care), such that a veteran with a primary care team and a mental health team at different locations had the location of the primary care team.
Area-Based Socioeconomic Measures
We used 18 publicly available area-based socioeconomic measures as proxies of veterans’ county-level SDH. 17,18 SDH covariates focused on measures of poverty, education, health insurance, crowded housing, broadband internet access, income inequality, historic unemployment rates, and county composition of non–US-born and non-White residents (supplementary table available from authors upon request). We used the most recent data available; data spanned 2012 through 2018 and mapped veterans’ residences to counties using their most recent home zip code.
Statistical Analysis
We calculated risk ratios (RRs) for 2 associations: (1) obtaining a COVID-19 test from the VHA among all veterans in active care and (2) receiving a positive test result for COVID-19 among veterans who obtained a COVID-19 test from the VHA. For both associations, we used 4 nested generalized linear models with a Poisson distributional family and a log link function with 4 sets of covariates. Model 1 adjusted for demographic characteristics; model 2 adjusted for demographic characteristics and facility characteristics; model 3 adjusted for demographic characteristics, facility characteristics, and comorbidities; and model 4 adjusted for demographic characteristics, facility characteristics, comorbidities, and county-level SDH.
In model 4, for both testing and test positivity outcomes, we restricted the sample size to veterans residing in counties with no missing data on area-based socioeconomic measures. In models in which the outcome was receipt of a positive COVID-19 test result, we excluded 1 facility with <5 COVID-19 cases and combined the age categories of 18-24 and 25-34. All models had SEs clustered on VHA facility, and we calculated 95% CIs (α = .05) to determine the statistical significance of the RRs. We retrieved county-level characteristics from GitHub. 19 We conducted all statistical analyses using Stata version 16 (StataCorp LLC). The Stanford Institutional Review Board and the VHA determined this evaluation was nonresearch and did not require institutional review board review.
Results
Of 6 292 800 veterans, 822 934 (13.1%) were tested for COVID-19 at the VHA, of whom 82 094 (10.0%) received a positive test result during the study period. Veterans who were female, Black/African American, Hispanic/Latino, single or divorced/separated/widowed, urban, aged 45-74, low income, and high disability were overrepresented among veterans tested for COVID-19 (Table 1). Among veterans who received a positive test result for COVID-19, veterans who were male, Black/African American, Hispanic/Latino, and urban were overrepresented compared with the proportion of veterans who were tested for COVID-19. Although Black/African American veterans comprised 17.5% of the cohort, they comprised 23.2% of tested veterans and 25.8% of veterans who received a positive test result. White veterans comprised 72.0% of the cohort, 68.4% of veterans who were tested, and 64.9% of veterans who received a positive test result.
Demographic characteristics and social determinants of health among veterans in active care at the Veterans Health Administration (VHA), by COVID-19 test status and result, February 8–December 28, 2020
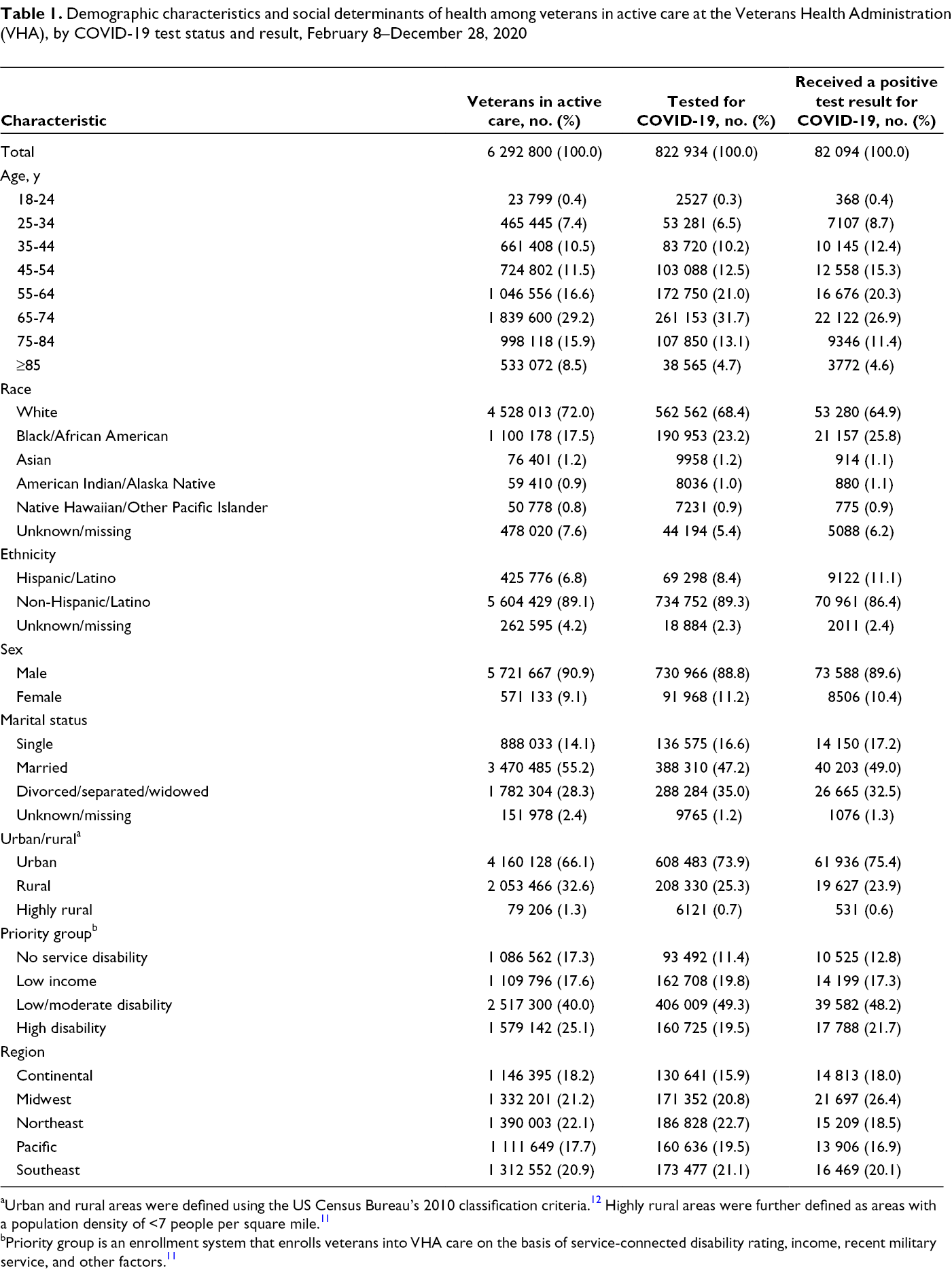
aUrban and rural areas were defined using the US Census Bureau’s 2010 classification criteria. 12 Highly rural areas were further defined as areas with a population density of <7 people per square mile. 11
bPriority group is an enrollment system that enrolls veterans into VHA care on the basis of service-connected disability rating, income, recent military service, and other factors. 11
Veterans tested for COVID-19 and veterans who received a positive test result tended to live in counties with a higher percentage of non-White and non–US-born residents than the total population of veterans in active care (Table 2). In addition, veterans who received a positive test result for COVID-19 more frequently resided in counties with a slightly higher percentage of people eligible for Medicaid and a higher percentage of people in crowded housing compared with veterans in active care. We found little to no differences among veterans in active care, veterans tested for COVID-19, and veterans who received a positive test result for COVID-19 by income inequality, poverty indices, unemployment rate, and in the percentage of households without a computer or without broadband internet access.
Veteran weighted median for area-based socioeconomic measures among veterans in active care at the Veterans Health Administration, by COVID-19 test status and result, February 8–December 28, 2020 a
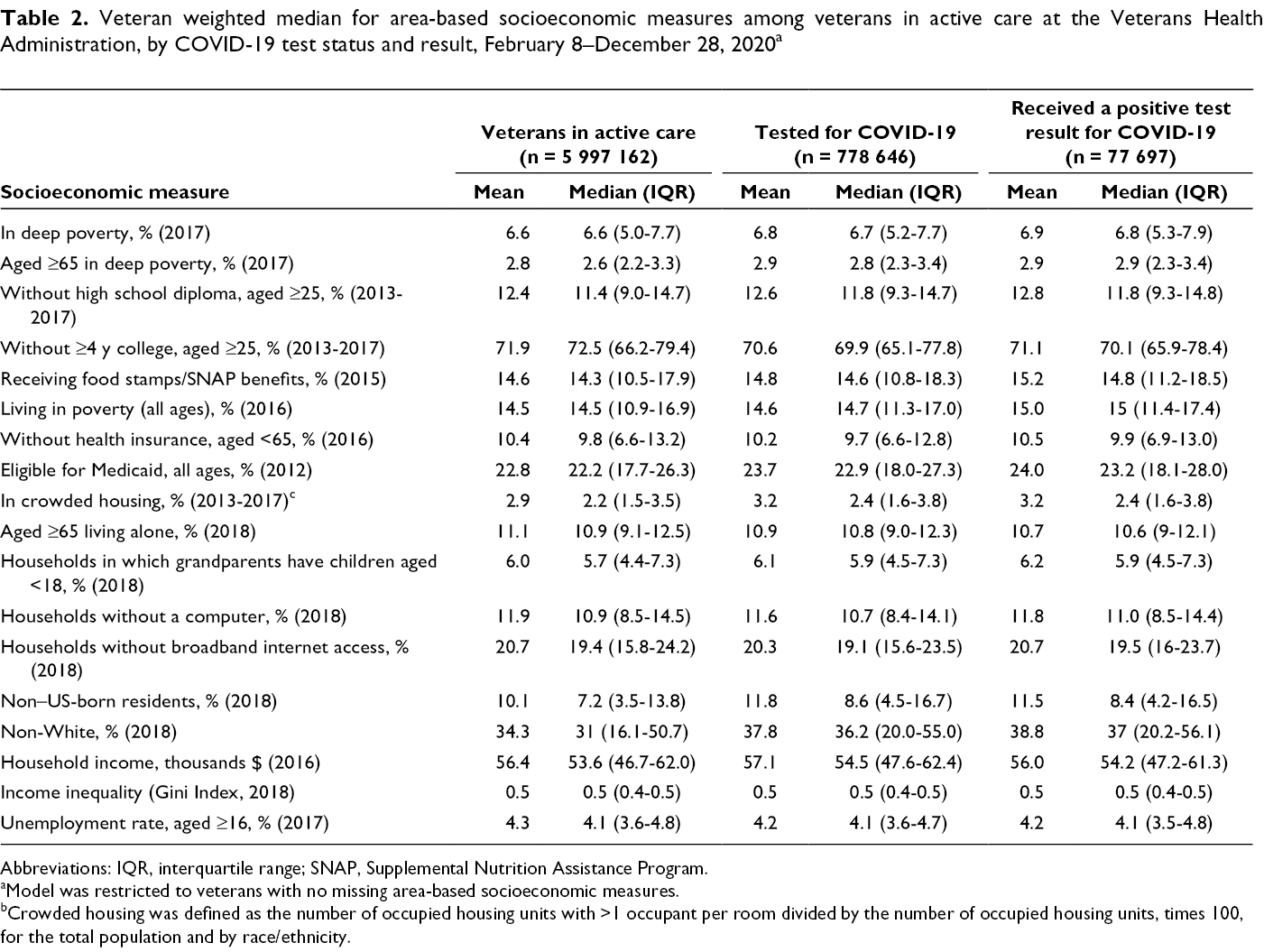
Abbreviations: IQR, interquartile range; SNAP, Supplemental Nutrition Assistance Program.
aModel was restricted to veterans with no missing area-based socioeconomic measures.
bCrowded housing was defined as the number of occupied housing units with >1 occupant per room divided by the number of occupied housing units, times 100, for the total population and by race/ethnicity.
In all models, veterans who were female (vs. male), Black/African American (vs. White), Hispanic/Latino (vs. non-Hispanic/Latino), with low/moderate service-related disability or high service-related disability (vs. no service-related disability), or low income (vs. not low income) were more likely to be tested for COVID-19 (Table 3). Veterans who lived in rural or highly rural (vs. urban) areas, were aged 18-44 (vs. 45-54), or were Asian (vs. White) were less likely to be tested for COVID-19. We found no differences in the likelihood of obtaining a COVID-19 test among American Indian/Alaska Native and Native Hawaiian/Other Pacific Islander veterans compared with White veterans. On average, in models adjusting for only demographic characteristics, the RRs were the strongest. Further adjusting for facility characteristics, comorbidities, and area-based socioeconomic measures attenuated the RRs across all demographic characteristics except sex. The relative risk of obtaining a COVID-19 test among females (vs. males) was 1.10 (95% CI, 1.08-1.12) adjusting for demographic characteristics but was 1.19 (95% CI, 1.17-1.21) in fully adjusted models.
Adjusted risk ratios for obtaining a COVID-19 test among veterans in active care at the Veterans Health Administration (VHA), February 8–December 28, 2020 a
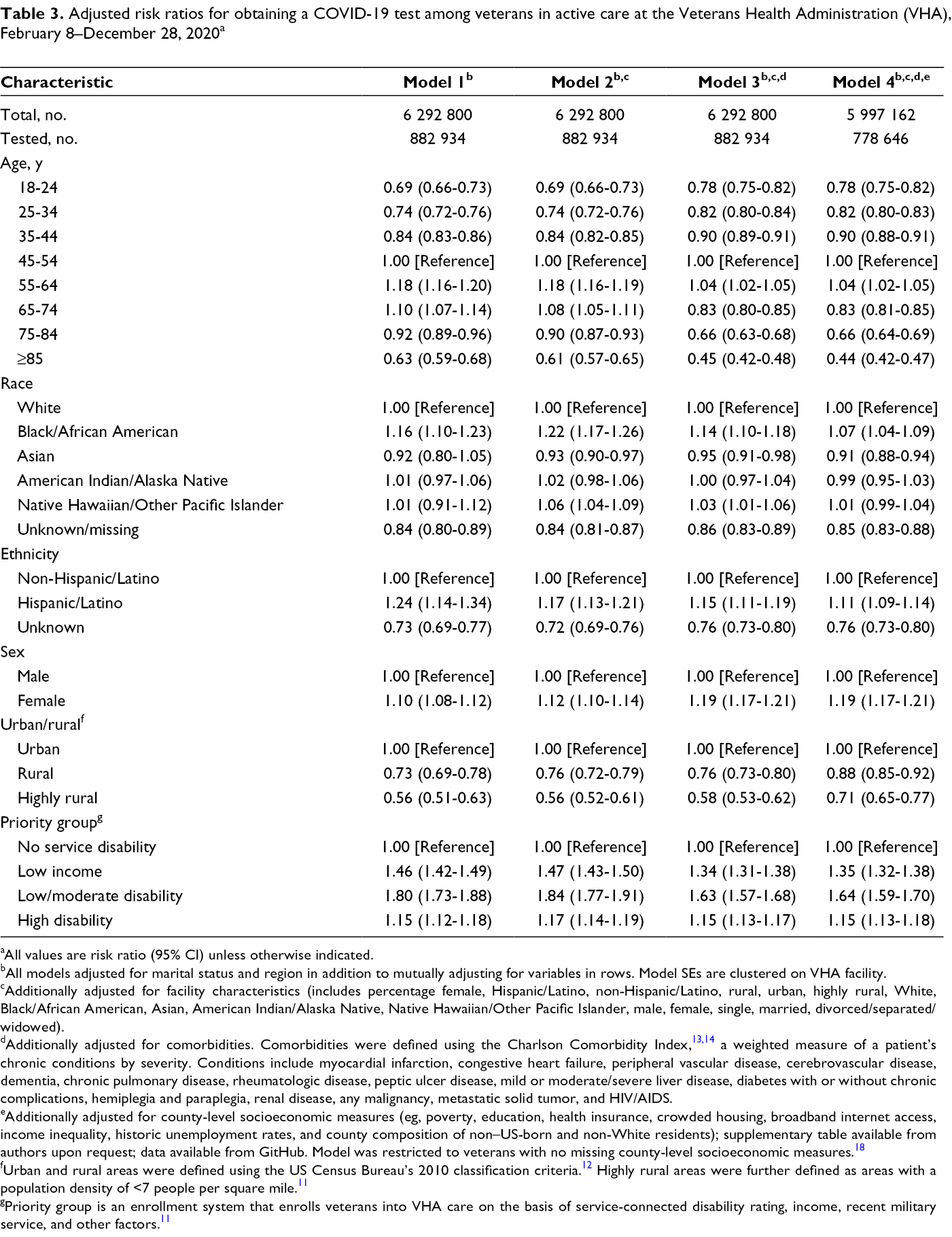
aAll values are risk ratio (95% CI) unless otherwise indicated.
bAll models adjusted for marital status and region in addition to mutually adjusting for variables in rows. Model SEs are clustered on VHA facility.
cAdditionally adjusted for facility characteristics (includes percentage female, Hispanic/Latino, non-Hispanic/Latino, rural, urban, highly rural, White, Black/African American, Asian, American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander, male, female, single, married, divorced/separated/widowed).
dAdditionally adjusted for comorbidities. Comorbidities were defined using the Charlson Comorbidity Index, 13,14 a weighted measure of a patient’s chronic conditions by severity. Conditions include myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, rheumatologic disease, peptic ulcer disease, mild or moderate/severe liver disease, diabetes with or without chronic complications, hemiplegia and paraplegia, renal disease, any malignancy, metastatic solid tumor, and HIV/AIDS.
eAdditionally adjusted for county-level socioeconomic measures (eg, poverty, education, health insurance, crowded housing, broadband internet access, income inequality, historic unemployment rates, and county composition of non–US-born and non-White residents); supplementary table available from authors upon request; data available from GitHub. Model was restricted to veterans with no missing county-level socioeconomic measures. 18
fUrban and rural areas were defined using the US Census Bureau’s 2010 classification criteria. 12 Highly rural areas were further defined as areas with a population density of <7 people per square mile. 11
gPriority group is an enrollment system that enrolls veterans into VHA care on the basis of service-connected disability rating, income, recent military service, and other factors. 11
In models for receiving a positive test result, adjusting for only demographic characteristics, veterans who were Black/African American, American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander, or missing race had higher RRs than White veterans, whereas Asian veterans did not (Table 4). In the final model, all non-White race categories had a higher risk of receiving a positive test result for COVID-19 compared with White veterans. We found strong associations among Black/African American veterans and Native Hawaiian/Other Pacific Islander veterans, with a 23% (95% CI, 1.19-1.27) and 13% (95% CI, 1.05-1.21) higher risk, respectively, of receiving a positive test result compared with White veterans. The risk of receiving a positive test result was more modest among Asian (RR = 1.06; 95% CI, 0.96-1.17) and American Indian/Alaska Native (RR = 1.05; 95% CI, 0.97-1.14) veterans as compared with White veterans. Hispanic/Latino veterans had a 43% higher risk of receiving a positive test result for COVID-19 than non-Hispanic/Latino veterans did (RR = 1.43; 95% CI, 1.36-1.50).
Adjusted risk ratios for receiving a positive COVID-19 test result among veterans in active care at the Veterans Health Administration (VHA) who obtained a COVID-19 test, February 8–December 28, 2020 a
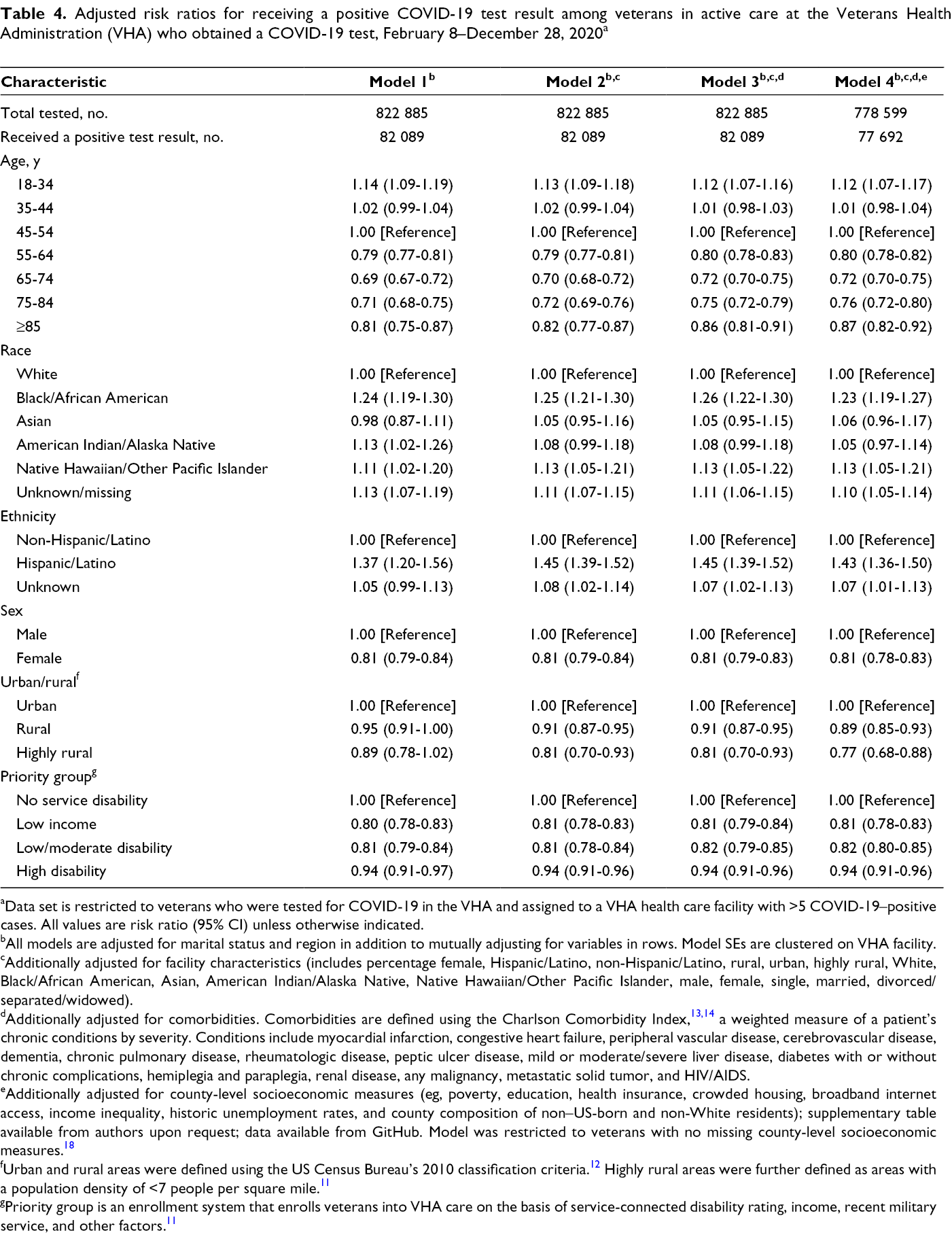
aData set is restricted to veterans who were tested for COVID-19 in the VHA and assigned to a VHA health care facility with >5 COVID-19–positive cases. All values are risk ratio (95% CI) unless otherwise indicated.
bAll models are adjusted for marital status and region in addition to mutually adjusting for variables in rows. Model SEs are clustered on VHA facility.
cAdditionally adjusted for facility characteristics (includes percentage female, Hispanic/Latino, non-Hispanic/Latino, rural, urban, highly rural, White, Black/African American, Asian, American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander, male, female, single, married, divorced/separated/widowed).
dAdditionally adjusted for comorbidities. Comorbidities are defined using the Charlson Comorbidity Index, 13,14 a weighted measure of a patient’s chronic conditions by severity. Conditions include myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, rheumatologic disease, peptic ulcer disease, mild or moderate/severe liver disease, diabetes with or without chronic complications, hemiplegia and paraplegia, renal disease, any malignancy, metastatic solid tumor, and HIV/AIDS.
eAdditionally adjusted for county-level socioeconomic measures (eg, poverty, education, health insurance, crowded housing, broadband internet access, income inequality, historic unemployment rates, and county composition of non–US-born and non-White residents); supplementary table available from authors upon request; data available from GitHub. Model was restricted to veterans with no missing county-level socioeconomic measures. 18
fUrban and rural areas were defined using the US Census Bureau’s 2010 classification criteria. 12 Highly rural areas were further defined as areas with a population density of <7 people per square mile. 11
gPriority group is an enrollment system that enrolls veterans into VHA care on the basis of service-connected disability rating, income, recent military service, and other factors. 11
Female (vs male) veterans and veterans with low, moderate, or high levels of service-related disability (vs no service-related disability) or low income (vs not low income) were more likely to receive a COVID-19 test but less likely to receive a positive test result once tested (Table 4).
Discussion
Compared with other health care systems, the VHA is testing a significantly higher proportion of traditionally disenfranchised groups that have an increased risk of COVID-19 infection. A study of patients’ Epic health records reported marginal testing differences by race and ethnicity, a 2.5 times increased likelihood of receiving a positive test result for COVID-19 among Hispanic patients compared with White patients, and a near doubling in the risk of receiving a positive test result for COVID-19 among Black and Asian patients compared with White patients. 20 In comparison, at the VHA, Black (vs White) and Hispanic/Latino (vs non-Hispanic/Latino) veterans were approximately 7% and 11% more likely, respectively, to obtain a test and 23% and 43% more likely, respectively, to receive a positive test result. Although the racial/ethnic disparities in receiving a positive test result for COVID-19 are significantly smaller in the VHA than in other health care systems, the higher risk of receiving a positive test result among racial/ethnic minority veterans compared with White veterans highlights important focus areas for health care equity.
Asian veterans were less likely to obtain a COVID-19 test than White veterans and had a weakly elevated risk of receiving a positive test result. Although Asian veterans use VHA services at similar rates as other veterans, Asian veterans on average report higher incomes than veterans of other racial/ethnic groups, which may affect their COVID-19 exposure risk. 21,22 Veterans with missing data on race were less likely than White veterans to obtain a COVID-19 test; however, this finding was expected because missing race is associated with low use of VHA health care services, as data on race are collected with each encounter at a VHA health facility.
Compared with White veterans, Native Hawaiian/Other Pacific Islander veterans did not have a higher likelihood of receiving a COVID-19 test but were more likely to receive a positive test result. We observed a similar but weaker association for American Indian/Alaska Native veterans, which may reflect the additional care that American Indian/Alaska Native veterans may receive through the Indian Health Service.
Female veterans were more likely than male veterans to be tested for COVID-19 yet were less likely to receive a positive test result once tested. This association is not clearly understood but may reflect a higher propensity or ability to seek care for COVID-19 symptoms, different symptom presentation, and/or a clinician’s increased likelihood of ordering a COVID-19 test for women than for men. 23 -26 Other key findings were among older veterans: veterans aged 55-64 were the most likely to receive a COVID-19 test, whereas veterans aged 75-84 and ≥85 were the least likely to be tested compared with any other age group. Veterans aged 55-64 may have fewer career- or childcare-related barriers to testing, whereas veterans aged ≥75 may be able to stay at home to reduce exposure to COVID-19 and the need for testing. 27
A key finding was a higher likelihood of testing among low-income veterans and veterans with a service-related disability. This is the opposite association found in non-VHA health care systems, because recent reports from California and New York report that more COVID-19 tests were administered in areas of higher socioeconomic status or with proportionally more White residents than in areas of lower socioeconomic status and with fewer White residents. 28,29 In this evaluation, the higher likelihood of testing yet lower risk of receiving a positive test result among low-income veterans and veterans with identified vulnerabilities may be the result of lowered financial barriers and several outreach programs at the VHA. As an example, the VHA rapidly expanded telemedicine during the pandemic, including a text-messaging protocol for home self-monitoring for COVID-19 infection, and clinicians contacted veterans at high risk for infection or illness. 30
Veterans who received a positive test result tended to live in counties with a higher percentage of people eligible for Medicaid, non-White residents, and non–US-born residents. These characteristics in part reflect an urban environment, because large metropolitan areas initially had a higher prevalence of COVID-19 than rural areas did. The higher prevalence of COVID-19 in metropolitan areas may also explain the substantially reduced likelihood of being tested and receiving a positive test result among rural and highly rural veterans as compared with urban veterans. Further investigation should account for individual socioeconomic characteristics, which may confound observed associations. 31
Our results are similar, but attenuated, to the results of Rentsch et al, 4 who examined a similar group of veterans with the same testing definitions for SARS-CoV-2 through July 22, 2020. Rentsch et al reported an adjusted odds ratio for a positive test result of 1.93 (95% CI, 1.85-2.01) among Black veterans as compared with White veterans and an adjusted odds ratio of 1.84 (95% CI, 1.74-1.94) among Hispanic veterans as compared with White veterans. 4 Although an odds ratio interpreted as a relative risk overstates the effect size, an odds ratio will approximate a relative risk when the outcome is rare (Rentsch et al reported a 6.4% test positivity rate). 32 Our analysis had nearly 6 months of additional follow-up; therefore, our attenuated results may reflect a reduction in racial/ethnic disparities as COVID-19 hotspots shifted from racially/ethnically diverse metropolitan centers to more rural and less diverse areas. Our work also accounted for some SDH and demonstrated that even after adjusting for SDH, demographic characteristics, facility characteristics, and chronic conditions, racial/ethnic disparities in testing and test positivity remain.
Strengths and Limitations
This evaluation had several strengths. First, we used a large nationwide electronic health record system that is powered to examine racial/ethnic minority veterans—populations commonly excluded or combined in analysis because of small numbers. Second, we used county-level SDH data based on place of residence rather than site of care. Third, self-reported data on race/ethnicity at the VHA also increased accuracy relative to state and national estimates, which have large proportions of missing data.
This evaluation also had several limitations. First, our study population was primarily male, although the large cohort included a substantial number of female veterans. As such, the generalizability of our results may be limited. Second, confounding by ability or preference to access VHA care (ie, previous health care use) may exist because previous engagement with the VHA predicts future engagement with the VHA. To account for potential bias between veterans enrolled at the VHA and veterans who actively use VHA health care, we restricted our evaluation to veterans with a recent history of VHA care (ie, care use in the previous 2 years) rather than all veterans enrolled in VHA health care. 33 However, the relationship between previous engagement with the VHA and testing is unclear; the VHA did not conduct systematic screening for each encounter but, rather, tested veterans on the basis of symptom presentation and exposure history. Test availability also varied by local caseload, facility supply, pre-operative screening procedures, and local policy. Future work should explore whether veterans’ likelihood of obtaining a COVID-19 test varied by type and frequency of care received at the VHA and by symptom presentation.
Third, for confirmed and consistent test accuracy, we evaluated only tests that were performed at the VHA. Therefore, results might not be representative of all veterans who received a positive test result for COVID-19, including veterans who were tested elsewhere. Further analysis may inform how veterans who come to the VHA for COVID-19 treatment but not for diagnosis differ from veterans who come to the VHA for both COVID-19 treatment and diagnosis. Fourth, we did not account for multiple testing; as such, our results reflect the risk of receiving a positive test result once tested rather than the risk of receiving a positive test result per test. Fifth, home address may be misclassified and may not capture data on where veterans spend most of their time, especially among homeless veterans whose addresses may reflect the VHA medical center domiciliary program. Most potential home address misclassifications would likely be attenuated because of the county-level aggregation. Sixth, although <10% of data on race/ethnicity were missing or unknown, accuracy is a concern with administratively collected data. 34,35 In the VHA, data on non-Black/non–African American minority groups and Hispanic/Latino veterans have poor concordance with racial/ethnic data from Medicare and the US Department of Defense; however, concordance was high (93%-99%) for White and Black/African American veterans. 34
Finally, SDH are a consequence of complex history and multilevel risk factors that drive health inequalities, especially during the COVID-19 pandemic, which we likely did not account for fully. 36,37 Additional research is needed to further examine the associations between SDH and COVID-19 testing and test positivity, with particular emphasis on differences by time, place, health care use, occupation, transportation, and financial resources. A better understanding of the mechanisms of these relationships would provide important insight that could inform future prevention efforts.
Conclusions
This large, nationwide evaluation of veterans identified increased risks of receiving a positive COVID-19 test result after obtaining a COVID-19 test among Black/African American, Native Hawaiian/Other Pacific Islander, and Hispanic/Latino veterans. Although Black/African American and Hispanic/Latino veterans were more likely than White and non-Hispanic/Latino veterans to obtain a COVID-19 test, the elevated risk of test positivity indicates that disparities remain. Disparities in positivity are lower at the VHA than disparities reported elsewhere, potentially because subsidized health care at the VHA lowers barriers to health care access among veterans. However, the remaining disparities suggest that veterans are not immune to the negative external effects of SDH and that social inequities drive disparities in COVID-19 prevalence. It is intended that this work will contribute to numerous other ongoing efforts designed to enhance the care of our veterans.
Footnotes
Acknowledgments
The authors thank Christopher Rentsch, Alison Liberty Greene, Zachary Veigulis, Lesley Park, and the VHA COVID-19 Shared Data Resource Team for their help in supporting this evaluation.
Authors’ Note
Jacqueline M. Ferguson and Hoda S. Abdel Magid contributed equally to this article. Mathew Kiang was affiliated with VA during the study but he is no longer affiliated with VA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Kiang reports grant no. K99DA051534 from the National Institute on Drug Abuse during the conduct of the study.