
Abstract
Oral conditions are major global public health issue. This study aimed to systematically analyze the incidence of and years lived with disability due to oral disorders by age, sex, and region in Eastern Sub-Saharan African (ESSA) region, from 1990 to 2023 using data, methods, and procedures of the Global Burden of Diseases (GBD) 2023 study. The Bayesian meta-regression tool for disease modeling (DisMod-MR 2.1) was used to quantify the incidence and years lived with disability. In 2023, there were an estimated 239.3 million (95% UI: 209.1, 270.6) new cases of oral disorders with an age standardized incidence rate (ASIR) of 45,553 per 100,000 persons (95% UI: 40360, 51457). In the ESSA, oral disorders accounted for 713,803 years lived with disability (YLD) in 2023. The age-standardized YLDs rate for both sexes associated with oral disorders was 265 in 1990 and 220 years per 100,000 population (95% UI: 124, 350) in 2023 corresponding to annualized rate of change of -17% (-25.2%, -8.5%). In the region, there were no statistically significant differences in the incidence and YLD rates by sex and country. The age-sex distribution of the incidence rate of oral disorders was higher among 5-9 years children of both sexes compared to the other age groups, where the rate decreased as age increased among both sexes. However, the age-sex distribution of the YLDs rate of oral disorders was higher among 95+ years of both sexes compared to the other age groups, where the rate increased as age increased among both sexes. There was slight decline in the trend of age-standardized incidence rate in the region. Except in Kenya, there was also a slight and statistically significant decline in the trends of the age-standardized YLDs rates from 1990 to 2023. In all countries, the leading cause of age-standardized incidence rate was caries of permanent teeth. From 1990 to 2023, despite the incidence and YLD rates of oral disorders have slightly decreased in the ESSA, it is considered still a public health challenge. Strengthening the oral health promotion policy and context specific public health interventions need to be considered to mitigate oral health disparities.
Plain language summary
The 1990-2023 Global Burdon of Disease (GBD) analysis of Eastern sub-Saharan Africa found 239.3 million new oral disorder cases in 2023, largely driven by permanent tooth decay, marking a significant public health challenge. While new cases were highest in children aged 5-9, the burden of disability (YLD) was highest in both sexes of 95+ years old population. This means that preventing incidence and YLD rate of oral problem is essential to reduce the burden on health services of the region.
Introduction
Oral disorders, including deciduous caries, permanent teeth caries, periodontal diseases, edentulism, and other oral disorders constitute a significant yet under prioritized aspect of the global non-communicable disease burden. 1
Oral diseases can cause pain, anxiety, disfiguring, and loss of working hours. They are ranked among the most prevalent health conditions affecting nearly half of the world’s population over their life course.2,3 In 2021, the direct and indirect costs associated with oral diseases were estimated to be $710 dollar globally. 4 People living in low-income countries are disproportionately affected because of inadequate oral hygiene practices, limited access to oral health services, malnutrition, and persistent poverty.2,5
In 2022, the World Health Organization has developed a global strategy to guide member states to promote oral health by reducing oral diseases and oral health inequalities. 6 However, there is scarcity of epidemiological information on the magnitude and burden of oral disorders to support targeted decision-making in resource-constrained settings. Lack of representative, comparable, and updated evidences might limit successful adoption and implementation of the global strategies. Up-to-date information on the global and regional burden of oral conditions is also crucial to monitor progress towards 2030 WHO global oral health target. 2
This study has aimed to estimate the incidence of and years lived with disability (YLDs) from oral disorders by sexes, age groups, and countries in Eastern Sub-Saharan African (ESSA) region from 1990 to 2023, using tools, procedures, methods, and input data of the Global Burden of Diseases (GBD) 2023 study. As a rationale, the study findings may be used for designing context-specific interventions, allocating resources, and monitoring progress.
Materials and methods
Study setting
This analysis was conducted in ESSA region, which included Comoros, Ethiopia, Burundi, Kenya, Madagascar, Eritrea, Malawi, Djibouti, Mozambique, Rwanda, Tanzania, Zambia, South Sudan, Somalia, and Uganda. The region has experienced rapid population growth, driven by high fertility rates and declining mortality rates. Healthcare access is limited, particularly in rural areas. 7
Data sources
This study used data from the GBD 2023 study, which was coordinated by the Institute for Health Metrics and Evaluation (IHME, University of Washington). The full list of the input data are available at: https://ghdx.healthdata.org/gbd-2023/sources.
Data analyses
For this study, the GBD 2023 study methods, procedures, and tools were used. The disease modeling with Bayesian meta-regression (DisMod-MR 2.1) was run to estimate incidence and YLDs. The YLD metric allows for standardized comparisons of non-fatal health burden between diseases. 8 The YLDs were measured by multiplying the prevalence of sequel from oral disorders by their corresponding disability weights.9,10 The spatiotemporal Gaussian process regression (ST-GPR) was applied to smooth variations in data and methods across locations and over time. Age-standardized rates were computed to adjust demographic variations. Trend changes in the incidence and YLDs from 1990 to 2023 were declared to be statistically significant if their 95% uncertainty intervals (UIs) did not include the zero value. In the GBD 2023 study, untreated dental caries referred to any tooth with unmistakable coronal cavity at dentin level, or root cavity in cementum that feels soft or leathery to probing; severe periodontitis referred to any pocket depth of 6mm or greater or attachment loss greater than 6mm; and edentulism referred to a complete loss of permanent teeth.11,12 The details of these GBD methods are found at: https://ghdx.healthdata.org/gbd-methods.
Ethics
This study was done as part of the GBD collaborators network by adhering to the GBD protocol, which is available at: https://www.healthdata.org/research-analysis/about-gbd/protocol.
Results
Incidence of oral disorders
Incidence of oral disorders by sex and location in the ESSA region, 1990 to 2023.

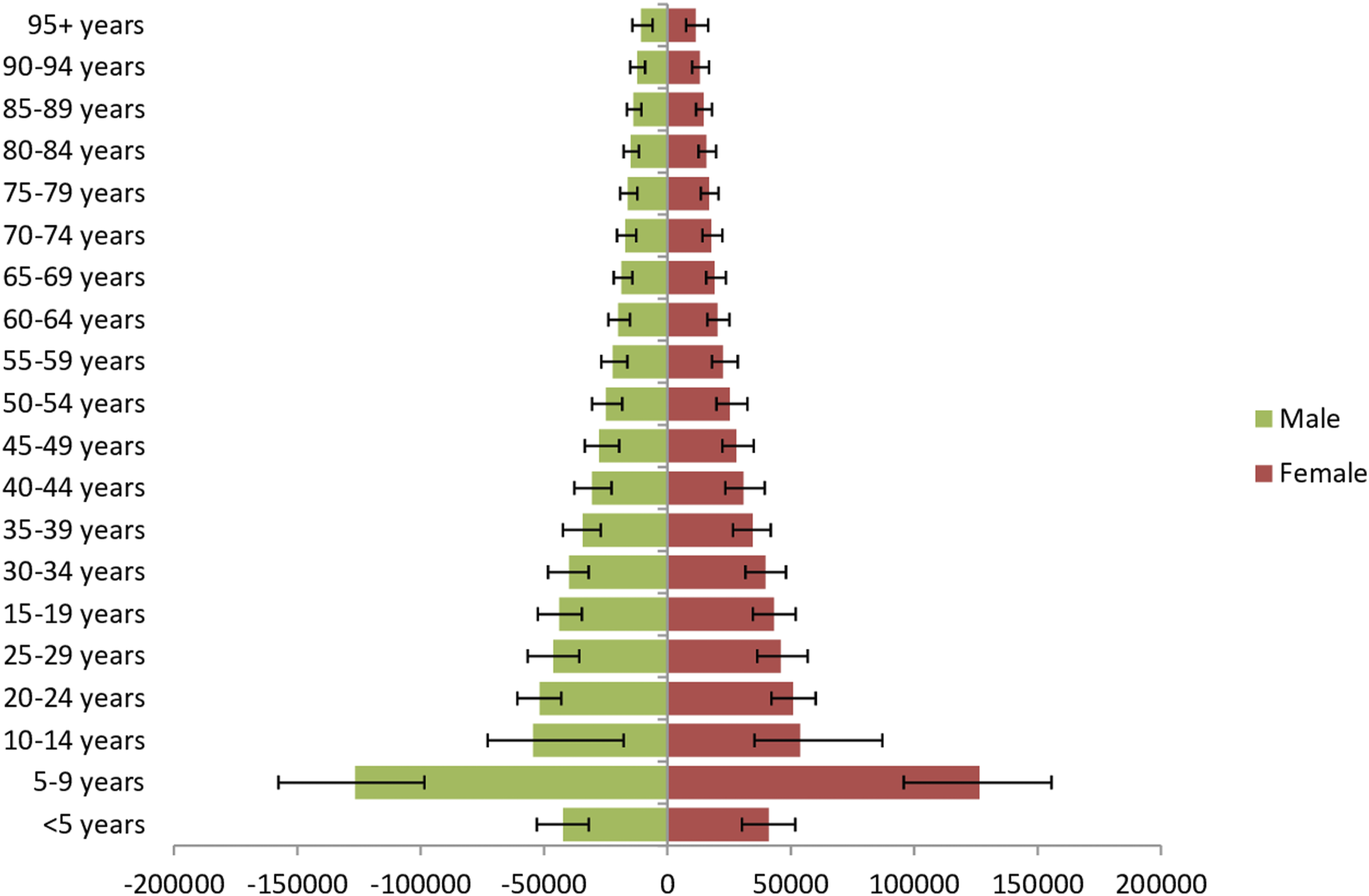
Incidence rates of oral disorders by age and sex in the ESSA region, 2023.

Age-standardized incidence rates of oral disorders in the ESSA region, 1990 to 2023.
Incidence of common types of oral disorders by sex in the ESSA region, 1990 to 2023.

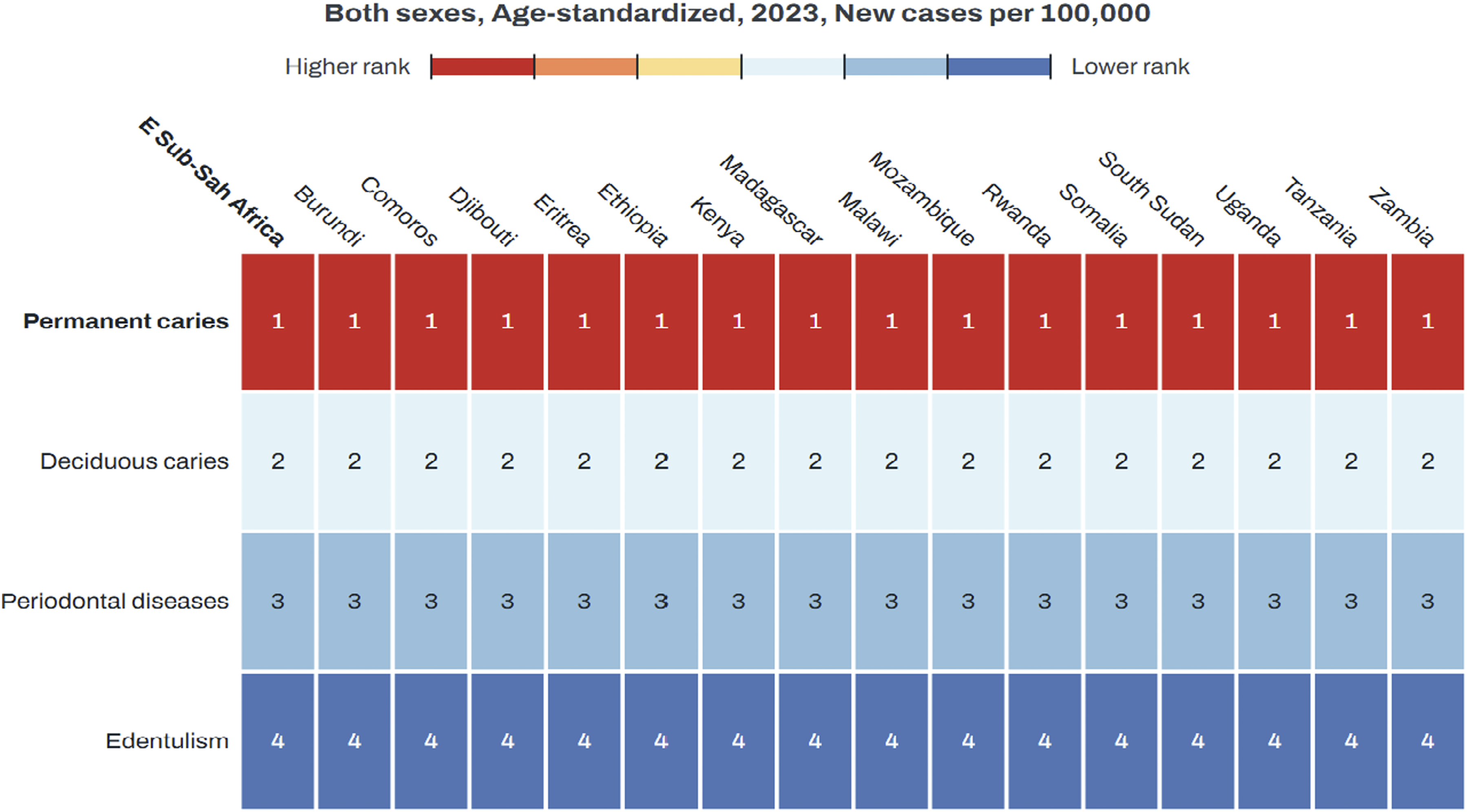
Age-standardized incidence rates from common types of oral disorders by countries in the ESSA region, 2023.
Years lived with disability from oral disorders
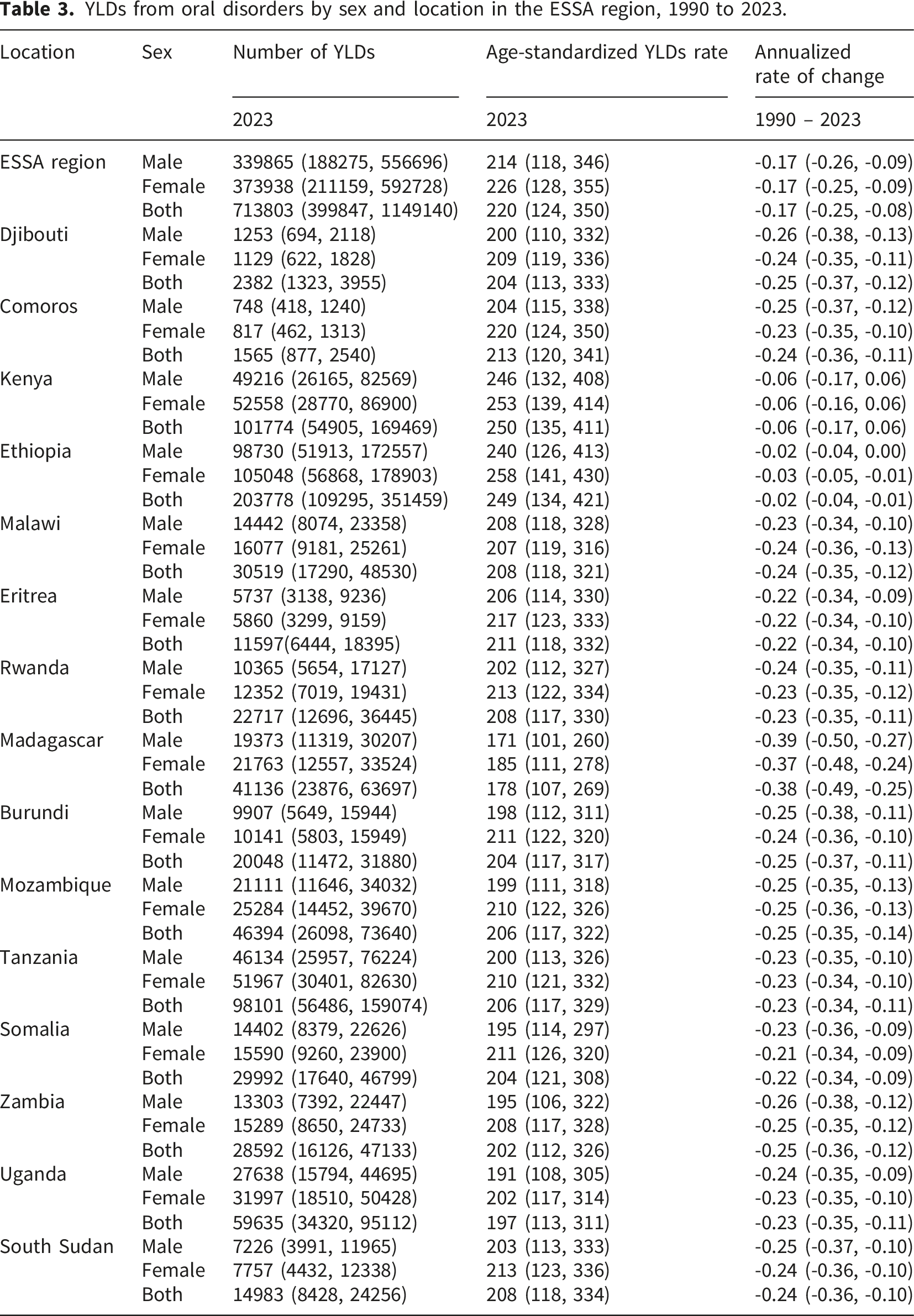
YLDs from oral disorders by sex and location in the ESSA region, 1990 to 2023.
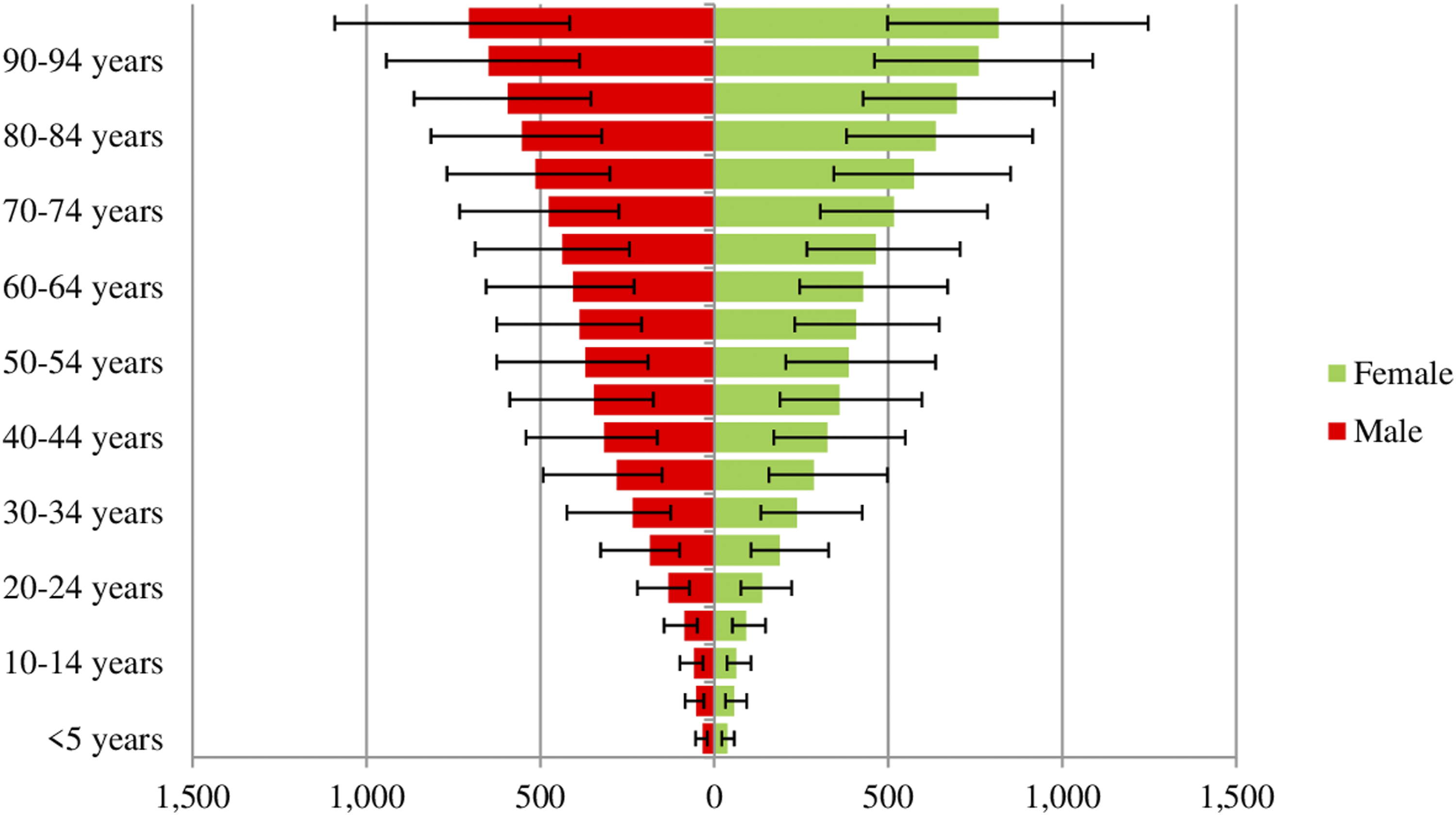
YLDs rate of oral disorders by age and sex in ESSA region, 2023.

Age-standardized YLDs rate from oral disorders in ESSA region, 1990 to 2023.
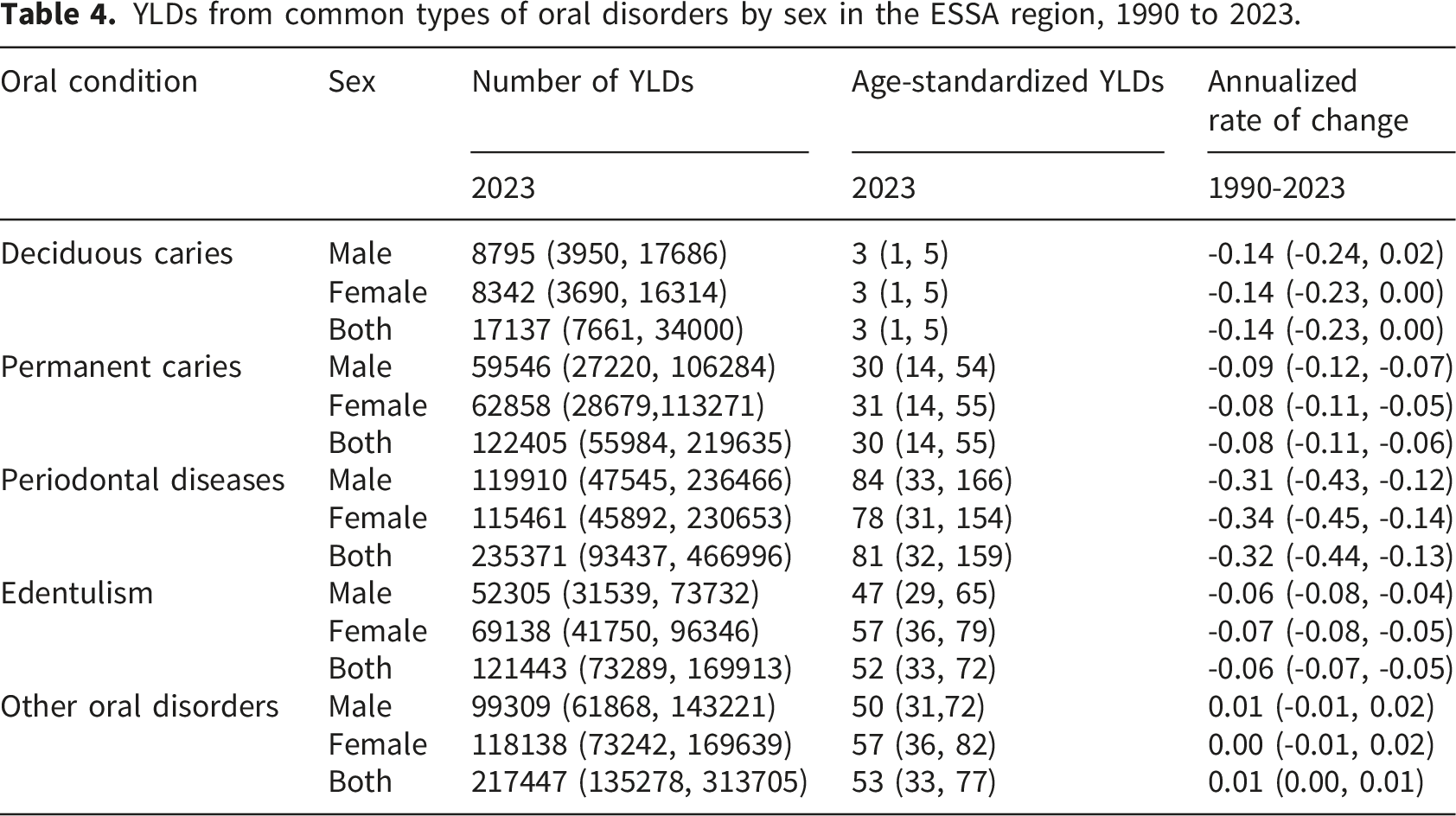
YLDs from common types of oral disorders by sex in the ESSA region, 1990 to 2023.

Age-standardized YLDs rate from common types of oral disorders by countries in ESSA region, 2023.
Discussion
This study determined the incidence of oral disorders and the YLDs in the ESSA region from 1990 to 2023. Despite the decrease in age-standardized rates of incidence and YLDs, oral disorders remained as significant public health issues in the region. Dental caries, periodontitis, edentulism, and other oral disorders contributed significantly to the incidence and YLDs. There was no gender difference in the age-standardized incidence and YLD rates for the burden of diseases caused by oral disorders in the ESSA in 2023. The age-sex distribution of the incidence rate of oral disorders was higher among 5-9 years children of both sexes compared to the other age groups, where the rate decreased as age increased among both sexes. However, the age-sex distribution of the YLDs rate of oral disorders was higher among 95+ years of both sexes and the rate increased as age increased among both sexes.
As oral disorders are chronic and progressive in nature, the age standardized incidence and YLDs in ESSA countries showed an increase with age across both sexes which indicates it can affect very young children but is a lifelong disease that runs through adolescence and adulthood. 13 In low and middle income countries (LMICs), there is high demand for treatment of oral conditions. YLD rate offer the potential to identify countries and systems in reducing the burden of oral condition. Consequently, integrating low cost interventions for dental care as part of the universal health coverage is needed.
Over the last two decades, integrating oral health into general health within national non-communicable disease (NCD) prevention programme has become a priority for WHO regions. 14 However, the recent GBD study on oral disorders estimated 239.3 million new cases in 2023, presenting a significant public health challenge that cannot be overlooked. In 2023, the age standardize incidence rate decreased slightly in the region. Conversely, in the 1990 to 2019 GBD study reported a slight increment. 15 Furthermore, studies indicate that the incidence of oral disorders has risen in LMICs.14–16 Despite oral health is still a major public health problem; with time and socio-cultural development overall improvement on the health status of the community including oral health could be the reason for the reduction of incidences. 17
In the ESSA region from 1990 to 2023, the age-standardized incidence rate of oral disorders showed a downward trend, with the exception of the Republic of Tanzania. This decrease could be due to the effective implementation of the historic 2021 World Health Assembly resolution, which promoted a shift in oral health policy and planning from a conventional restorative model toward a promotive and preventive model. 1 Furthermore, ESSA countries may have embedded oral health within the non-communicable disease (NCD) agenda, allowing essential health interventions to be initiated to achieve universal health coverage.
Across all countries, the leading cause of age-standardized incidence was caries of permanent teeth, followed by deciduous caries, periodontal diseases, and edentulism, a finding consistent with the 2021 Global Burden of Disease (GBD) study conducted in sub-Saharan Africa. 17 Within the region, there was variation in the age-standardized incidence among countries, with Ethiopia, South Sudan, and Kenya being the top Eastern sub-Saharan countries with the highest incidence of oral disorders, respectively. This variation could be due to differences in the speed of economic development, lifestyles, and eating habits, as well as the impact of conflict.18–22
The burden of oral disorders is high in Ethiopia due to a combination of factors including poor oral hygiene practices, limited access to dental care, and socioeconomic factors that contribute to poor nutrition and high sugar consumption. 18 In addition, in Ethiopia the lack of a comprehensive oral health policy and poor integration with general health policies could also contributed for the increased incidence rate. 19
There were no statistically significant differences in the incidence and YLD rates by sex and country.
In 2023, the number of top incident type of oral disorder was caries of permanent teeth with 129.2 million incident cases followed by caries of deciduous teeth with 106.5 million new cases reported. However, in the 2021 GBD study, we observed highest incidence of periodontitis in the sub-Sahara Africa. 20 The possible reasons could be due to early treatment of periodontal disease which could be traditionally performed through reinforced oral hygiene practices. It could be also due to the use of D. discoideum in combination with antimicrobial testing as a robust and sensitive model for screening oral antiseptics and underscore the potential of chlorhexidine-sodium DNA formulations as adjunctive oral care agents. 21
The current study shows that the YLDs of oral disorders showed a downward trend in 2023. In the ESSA, oral disorders accounted for 719,014.3 YLDs in 2023.The age-standardized YLDs rate for both sexes associated with oral disorders was 265 in 1990 and 220 years per 100,000 populations in 2023. The decline in YLDs in these countries showed that currently the prevention and promotion of oral health is improved. The decline could be also due to low sugar consumption. Studies also showed the sugar consumption in Eastern sub-Saharan Africa is generally lower than the global average. 22 In ESSA, YLD due to periodontal diseases is common, becoming an important public health concern, despite the highest reduction observed in this study. Hence, countries need to strengthen the implementation of health promotion policy. However, in 2021, in sub-Saharan Africa, Edentulism was the leading cause of oral disorders. 20
Ethiopia accounted for the highest of the entire ESSA region YLD in 2023, with age-standardized rate of 249 per 100,000 population and annualized rate of change of -2.3% (95% UI, -4.2%, -0.7%) down from 1990. The reason could be due to Ethiopia lacks a specific, comprehensive national oral disorder prevention policy. While the national health policy addresses the prevention and control of poverty-related diseases, including some oral health issues, there’s no dedicated oral health program within primary healthcare. 2 However, efforts are underway to integrate oral health into broader health initiatives and strengthen oral health program.
We did not observe increment in YLD in the Eastern sub-Saharan countries in 2023. This could be due to the implementation of the oral health promotion policy and indicates that the harm of oral disorders to human health has attracted attention by the respective ESSA countries. The highest reduction in Madagascar might be oral health policies and practices prioritize integrating oral health into general health initiatives and focusing on prevention, particularly for children like implementation of tax on sugar-sweetened beverages, and presence of oral health screening for early detection of oral diseases. 23 The country recognizes the importance of both modern and traditional medicine in oral healthcare, with initiatives supporting traditional practices alongside efforts to improve access to modern oral healthcare services.24,25
The age-sex distribution of the incidence rate of oral disorders was higher among 5-9 years children of both sexes compared to the other age groups, where the rate decreased as age increased among both sexes. However, the age-sex distribution of the YLDs rate of oral disorders was higher among 95+ years of both sexes and the rate increased as age increased among both sexes. The high age-standardized incidence rate of oral disorders in children especially in LMICs could be due to many factors like the less emphasis given to oral hygiene and poor dietary practices that predispose children to early dental disorders. In other study, however there was a significant disparity among males and females with specific oral disorder types. 26 And the high age-sex distribution of the YLDs rate of oral disorders among 95+ years of both sexes could be due to the effect of multiple chronic diseases over a lifetime that predispose them to different oral disorders. 27
A higher than the regional age-standardized rate of YLDs was observed in Kenya followed by Ethiopia. Though it was not statistically significance, the rate of YLDs was higher among females in each country across the ESSA region, except in Malawi [208 years per 100,000 population (95% UI: 118, 328)] among males and [207 years per 100,000 population (95% UI: 119, 316)] among females.
Study showed that in Sub-Saharan Africa women generally experience low quality of oral healthcare compared to men. Additionally, studies show higher prevalence of dental caries (tooth decay) in women than men in some African populations. 28
Preventing the incidence and YLD rate of oral disorders is essential to reducing the burden on the region’s health services. Consequently, policymakers should prioritize and strengthen the integration of oral health into promotive and preventive initiatives to achieve the universal health coverage agenda.
Countries in the ESSA also need to consider context specific interventions like reducing high sugar consumption, tobacco and alcohol use, and poor oral hygiene etc. that could prevent the different oral disorders. Countries need to increase political and financial commitment that could foster paradigm shift from treatment-oriented oral health care into more prevention and promotion approaches.
This study is not without limitations because the study is not comprehensive enough to include all oral disorders like mouth cancers and congenital malformations of the oral cavity.
Conclusion
From 1990 to 2023, despite the incidence and YLD rates of oral disorders have slightly decreased in the ESSA, it is considered still a public health challenge especially from the escalating burdens of caries of permanent teeth, and periodontal disease. Strengthening the oral health promotion policy and context specific public health interventions need to be considered to control the future burden, and mitigate oral health disparities.
Footnotes
Author contributions
ST conceived and designed the study. ST, YBT, AKB AA, and GW were involved in the analysis and interpretation of the findings. All authors have approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.