
Abstract
Background:
Previous studies from Brazil and West Africa have shown that patients with albinism can feel stigmatized and isolated, highlighting the importance of access to healthcare and support in improving their quality of life. Studies in the United States are lacking.
Objectives:
Our study aims to understand gaps in access to genetic testing, vision care, and community resources for patients with albinism.
Design:
A survey was distributed on the National Organization for Albinism and Hypopigmentation (NOAH) website and during in-person research sessions at the Medical College of Wisconsin or emailed to previous research participants.
Methods:
Multiple choice and open-ended questions were aimed at assessing access to resources, genetic testing, and vision health. The data were de-identified and analyzed.
Results:
A total of 47 responses were received between June 2022 and April 2023. Around 62% were based on self and 38% based on child; 66% of participants were women, 32% men, and 2% transgender. There was a wide distribution of age, location, household income, and education level. Almost 85% of participants had medical insurance, including 15% Medicare/Medicaid. Around 64% had genetic testing done, of those 40% had to travel an average of 459 miles (5–1700 miles, Mdn: 150 miles, M: 459 miles) to access it. About 34% felt their questions about albinism were not fully answered, for reasons such as questions not answered by their physician, using a 23&me kit, not seeing a genetic counselor, or genetic results that were inconclusive. Almost 83% felt they had good understanding of their visual health. Around 60% were aware of community resources related to improving quality of life related to visual health, but only 45% utilized them.
Conclusion:
While access to eye doctors is adequate in our surveyed population, access to genetic testing could be strengthened and awareness of community resources could be improved upon. This could be facilitated by eye doctors and primary care physicians.
Background
Inherited retinal diseases affect more than 2 million people worldwide and diagnosis can be difficult to establish based on exam and symptoms alone, which necessitates molecular genetic testing. 1 Since the development of the human genome project, genetic testing has become more widely utilized.2,3 New therapeutic approaches are emerging due to recent advancements in our understanding of the mechanisms leading to vision loss in inherited retinal diseases, elevating the importance of accurate genetic diagnoses for individual patients. 4
Albinism is a rare genetic disease that affects the pigmentation of skin, hair, and eyes with a prevalence of 1/18,000 in the United States.5,6 It is caused by a mutation in genes that are responsible for production or transport of melanin. 7 Symptoms include reduced vision, nystagmus, strabismus, and increased risk of skin cancer.7–10 While some forms of albinism are clearly visible when looking at an individual, others such as the X-linked ocular form caused by GPR143 mutations cause visual symptoms but present with normal or near-normal skin and hair color. 11 Ocular albinism requires genetic testing (though female carrier status can be detected using fundus autofluorescence) to diagnose and even in oculocutaneous albinism, the presence of hypomorphic alleles may complicate the diagnosis and require thorough genetic testing. 12
Objectives
The purpose of this study was to develop a survey to better understand gaps in access that individuals with albinism may face in relation to genetic testing, their visual health, and community resources. Several studies have looked at the relationship of public health and albinism in regions of West Africa and Brazil,7,13 but studies in the United States are lacking. The Brazilian study concluded that “irrespective of geographic location, patients with albinism can feel stigmatized and isolated. Initiatives to raise awareness of albinism are extremely important in all places worldwide” and “quality of life of patients can be markedly improved with access to health, support, and adequate guidance.” 7 Motivating our study, previous work has shown that when people understand their own medical problems and have access to resources, it improves their quality of life and lowers their disease severity. 14
Design
The study was approved by the Medical College of Wisconsin (MCW) Institutional Review Board (PRO 40631). We worked with the CTSI of Southeast Wisconsin Biomedical Informatics Core, which was used as a central location for data processing and management. REDCap (Research Electronic Data Capture) was used for data collection. 15 REDCap projects rely on a thorough, study-specific data dictionary defined in an iterative self-documenting process by all members of the research team with planning assistance from the CTSI Biomedical Informatics Key Function.
For individuals who had participated in research at the Eye Institute of MCW and had agreed to further correspondence, an informational letter/email was sent. The letter/email provided a summary of the project and a link to the REDCap survey. Survey information was also posted on the National Organization for Albinism and Hypopigmentation (NOAH) website. The posting provided a summary of the project and a link to the REDCap survey. If a potential participant was interested and clicked the link, they were taken to the first page of the survey, which included more detailed information about the project. After reviewing this information, they were prompted to click “Continue” to proceed with the survey only if they (1) were over 18 years old, (2) understood that participation was voluntary, and (3) understood that results would be used for research purposes. We do not know which method ultimately recruited each responder.
Methods
The first few questions of the accessibility survey (Supplemental Document 1) asked about the individual or any other family members having albinism and how this influenced their access to care. Because albinism is a genetically inherited condition, it is likely that having a family member with albinism caused the patient to be more informed about their own medical condition and influenced both their understanding of their health and their access to care.
The next set of questions were aimed at assessing whether the patient sees an eye care provider, the specific kind of eye care provider, how often they see them, and time elapsed between first visual symptoms and being seen in the clinic. These questions told us about both access to vision care and timeliness of care, as timeliness of care can often be representative of access or lack thereof. Timeliness is an aspect of access to health care according to the Agency for Healthcare Research and Quality and previous studies have shown that timeliness of care was reduced for adults with public insurance compared to adults with private insurance, and that uninsured adults were less likely than adults with private insurance to receive needed and timely care for an illness, injury, or condition. 16
The next few questions were about seeing a genetic counselor and about the participant’s ability to receive and access genetic testing. Based on the 2015 U.S. National Health Interview Survey, disparities in genetic testing access were greatest in the Hispanic population, non-citizens, uninsured individuals, and individuals with less education. 17 Because the Advanced Ocular Imaging Program (AOIP) at MCW and other research laboratories provide no-cost genetic testing that may be beneficial to patient’s understanding of their medical conditions and better treatment options, it is important to know if these individuals could easily have access to free genetic testing otherwise. If we find that many research study participants have easy access to genetic testing, it may be beneficial for both the patients and the generalizability of our study to increase our recruitment to be more inclusive of individuals who may otherwise not have access to free genetic testing. Previous research has shown that 25% of children who needed genetic services did not have access to them 18 and that children from high income families were twice as likely to receive genetic services. 19
The next few questions asked about self-reported understanding of medical diagnoses. This provided insight into health literacy of the patients and whether more needs to be done by medical providers to educate and advertise resources to improve health literacy. Previous studies have shown that low health literacy remains a significant public health challenge, which contributes to both health disparities and social determinants of health. 20 Populations that are at risk of low health literacy are also the ones that are most at risk for health disparities in chronic diseases. 21 Furthermore, this 2019 study concluded that health literacy is one of the few contributors to health disparities where individual-level intervention may produce a strong effect.
The next question asked about perceived quality of care to understand if patients perceived their care as validating and complete, as this directly relates to their satisfaction with medical care. 22
The next questions were about access and involvement in local organizations that may improve quality of life and provide resources for dealing with the patient’s visual conditions. If our study shows that a lot of individuals are not aware of such resources and are not involved with them, future efforts can be aimed at providing individuals with more information about how to get involved with local and nationwide resources (such as NOAH) and how these resources may help with improving vision-related quality of life. There are several organizations that provide resources, education, and classes on improving quality of life for patients with vision deficits, which could benefit patients immensely.
Standard demographics questions were chosen to better understand the population being surveyed and make our survey more generalizable. Understanding demographics that may relate to the aspects of visual care being studied will allow us to implement improvements that will be more likely to reach the populations that lack access and resources. Access to genetic testing could improve understanding of disease and create more treatment options. Perceived quality of care and frequent visits to eye doctors may influence quality of life and vision problem severity. Resources in the community are there to improve the lives of patients, but this only works if the patients know about them and can utilize them. Knowing more about these aspects of visual care for patients with albinism may allow for future improvements in health care and quality of life.
Data were collected from June 2022 until April 2023. The data were de-identified, exported as an excel sheet, and summarized with descriptive statistics. For the relationship between demographics with genetic testing and demographics with awareness of community resources, Fisher’s exact test was used to calculate the p value, which is the probability that the observed differences in groups are due to chance. A p value less than 0.05 was considered statistically significant. We have followed the EQUATOR STROBE guideline (Supplemental Document 2) for reports of observational studies. 23
Results
Demographics
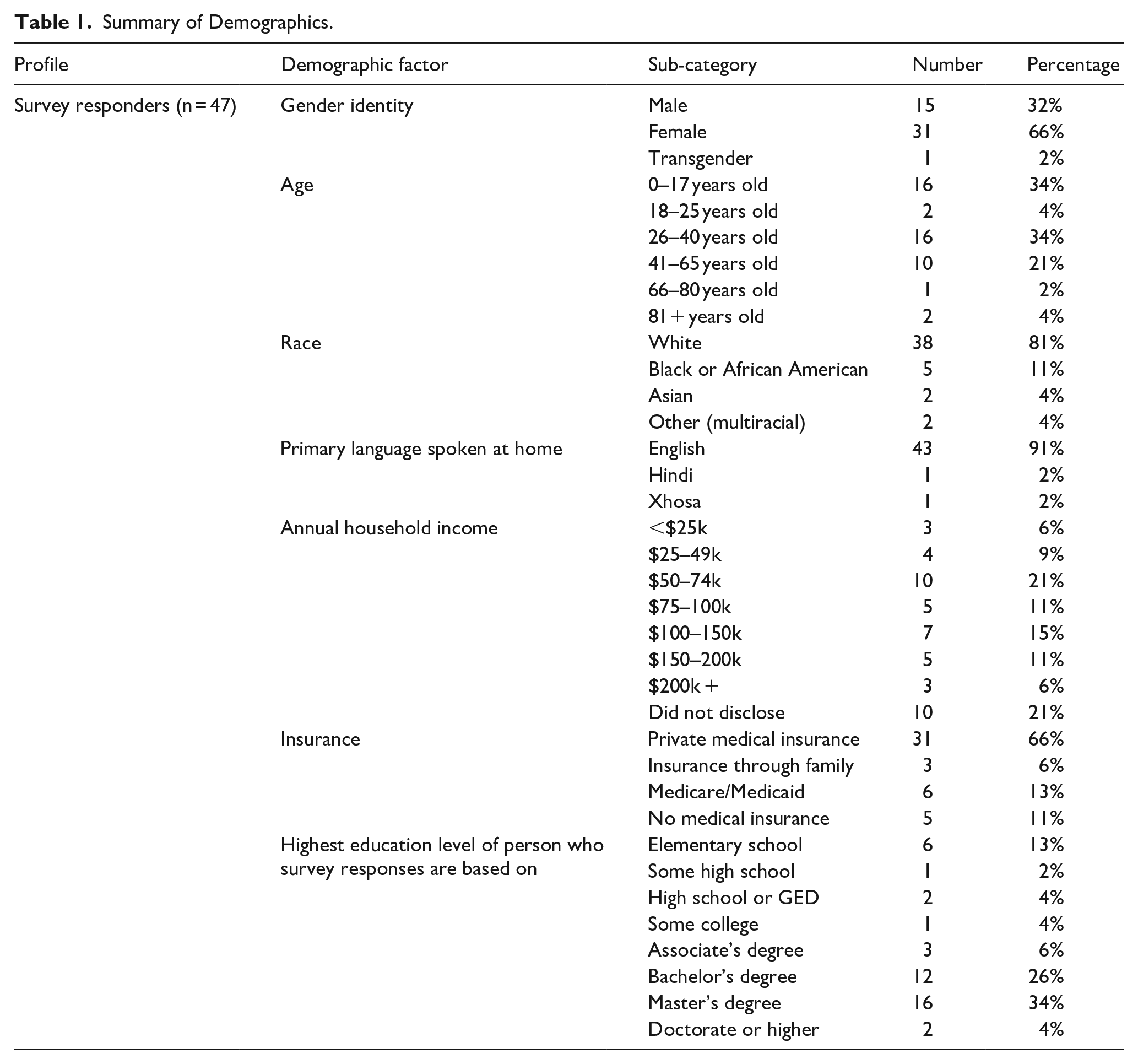
Of 47 unique responses, 62% were based on self and 38% based on child or minor. 66% of participants were women, 32% men, and 2% transgender. About 34% of participants were 0–17 years old (completed by adult on their behalf), 4% were 18–25 years old, 34% were 26–40 years old, 21% were 41–65 years old, 2% 66–80 years old, and 4% were 81+ years old. Participants were 81% White, 11% Black or African American, 4% Asian, and 4% Multiracial. The primary language in the home was 91% English, 2% Hindi, and 2% Xhosa. Annual household income varied greatly with 6% making less than $25k per year, 9% making $25–49k, 21% making $50–74k, 11% making $75–100k, 15% making $100–150k, 11% making $150–200k, 6% making $200k+. Almost 85% of participants had medical insurance, including 13% Medicare/Medicaid. About 11% of responders were uninsured. Of note, some individuals chose not to disclose certain answers, resulting in percentages that may not add up to 100%. These demographics are elaborated in Table 1.
Summary of Demographics.
Access to vision care
About 48% of survey responders felt that having a family member with albinism contributed to their own diagnosis and 41% felt that having a family member with albinism prompted them to see an eye care provider. All participants had seen an eye doctor at some point in their life, with 85% seeing an ophthalmologist and 49% seeing an optometrist. Almost 96% of participants first saw an eye doctor at ages 0–5 years old, 2% first saw an eye doctor at 6–10 years old, and 2% first saw an eye doctor at age 21+ years. As summarized in Figure 1, currently, 25% see an eye doctor every 6 months, 45% once per year, 28% once every 2 years, and 2% every 5 years. Almost 83% felt they had good understanding of their visual health, and 91% felt that their medical condition was fully worked up by their eye doctor.
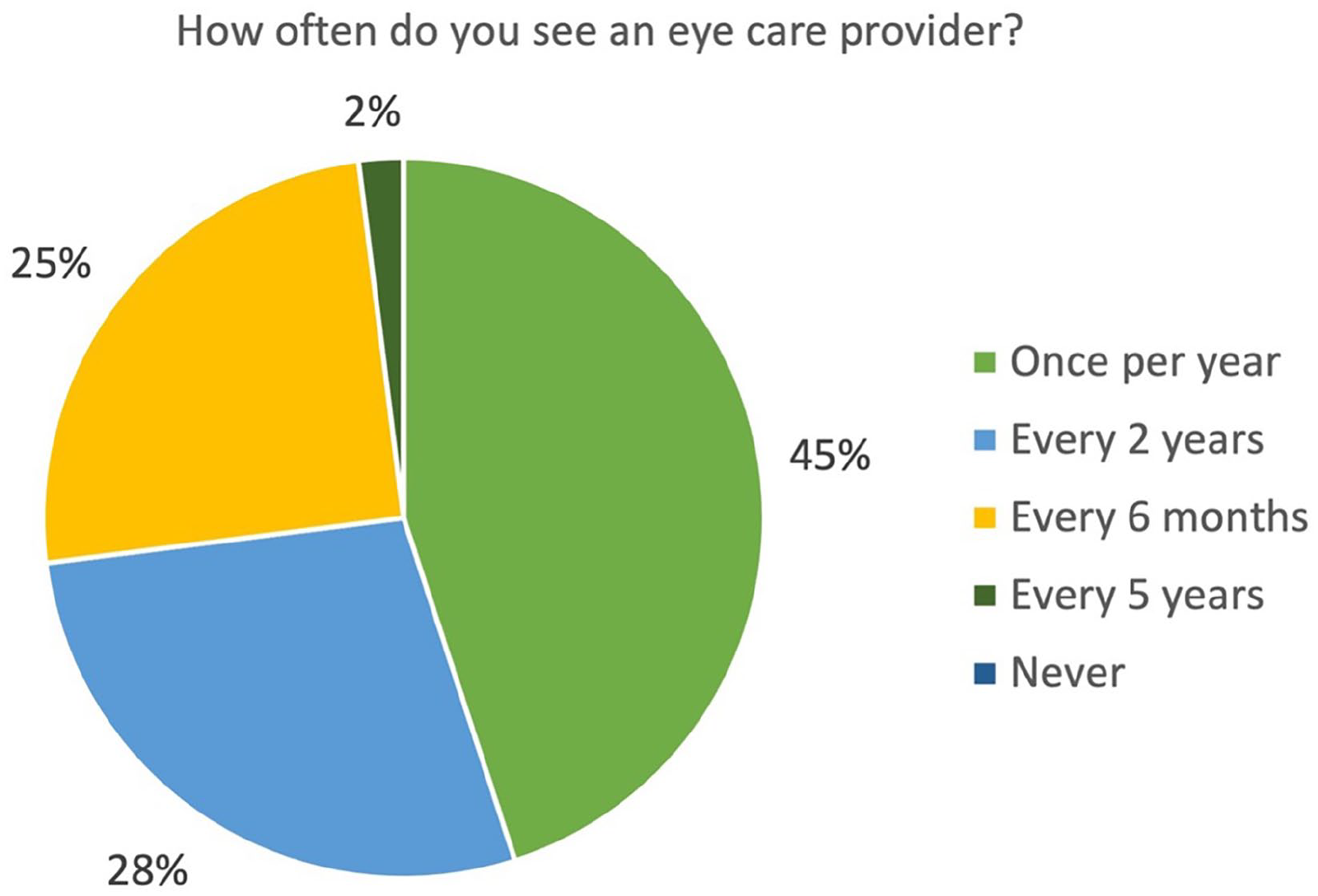
Seeing an Eye Care Provider.
Access to genetic testing
Around 62% had genetic testing done, of those 40% had to travel to access genetic testing (range: 5–1700 miles, Median: 150 miles, Mean: 459 miles). One individual indicated they got genetic testing done, but never received their results or followed up; they were counted as not having undergone genetic testing. Of the 38% who did not get genetic testing done, 28% cited lack of opportunity, 33% prohibitive cost, 6% geographic location, and 28% had no interest in getting tested. Obstacles to genetic testing are summarized in Figure 2. Some individuals chose multiple options and were counted for each category they selected. About 34% said that their genetic testing results were inconclusive. About 53% of participants had seen a genetic counselor to discuss albinism. They described their reasons for seeing a genetic counselor as 45% to better understand their medical condition, 15% family planning, and 4% as part of research. All individuals who answered that they were unaware of opportunities to get genetic testing had never seen a genetic counselor. Individuals described their reason for having genetic testing done as 33% ordered by a doctor as part of their medical workup, 17% ordered by a genetic counselor, 27% for personal understanding of their medical condition, 37% out of curiosity about their medical condition, and 10% for family planning reasons. The average year of having genetic testing done was 2014.8, with a range of 1990–2022, median of 2017.5 and mode of 2018. Almost 97% of the participants who completed genetic testing, received their results with 17% of results taking less than 1 month to receive, 48% taking 1–3 months, 7% taking 3–6 months, 10% taking 6 months to 1 year, and 17% taking more than 1 year. All individuals who answered that it took a year or more to receive their results, completed genetic testing as part of a research study. About 43% of participants said they decided to participate in a research study at least in part in order to receive genetic testing. About 28% of individuals who got genetic testing, did so through research study participation, with only one of those individuals being uninsured.

Obstacles to Genetic Testing.
Almost 90% felt like their genetic testing results did not affect their care. About 55% spoke to a genetic counselor once they received their result. About 65% said their results were conclusive. Of those that did not, they described having only one genetic mutation, having uncommon genetic mutations, or their results not showing a genetic mutation. About 34% felt their questions were not fully answered after receiving their genetic results, with some of the following reasons given: their physician did not spend enough time to explain what the results meant, kits like 23&me or ancestry did not explain what results meant, or their results were inconclusive/the corresponding genetic mutation was not found. Of the people who felt like their questions were not fully answered, 40% had received genetic testing results they described as inconclusive and 70% did not meet with a genetic counselor after receiving their results. Of the 10 individuals that stated they did not feel like their questions were fully answered, 9 of them either received inconclusive results, did not see a genetic counselor after receiving the results, or both. However, 80% of responders who received an inconclusive genetic testing result, did meet with a genetic counselor after their testing.
Access to community resources
About 60% of participants stated they were aware of community resources related to improving quality of life related to visual health. About 45% said they were part of a community organization that could help improve their quality of life related to their visual health. As summarized in Figure 3, for the 55% that were not involved in these community organizations, they cited the following reasons: 58% were not aware of the opportunity to join, 27% said their geographic location prevents them from joining, 23% had no interest in joining, 15% had no time to join, 11% felt it was too expensive, 8% felt their vision deficits prevent them from joining, 4% decided or someone told them there was no benefit to getting involved, and 4% said they were reluctant to join. Almost 94% of participants said that if they were to learn more about these resources, they would be interested in joining.
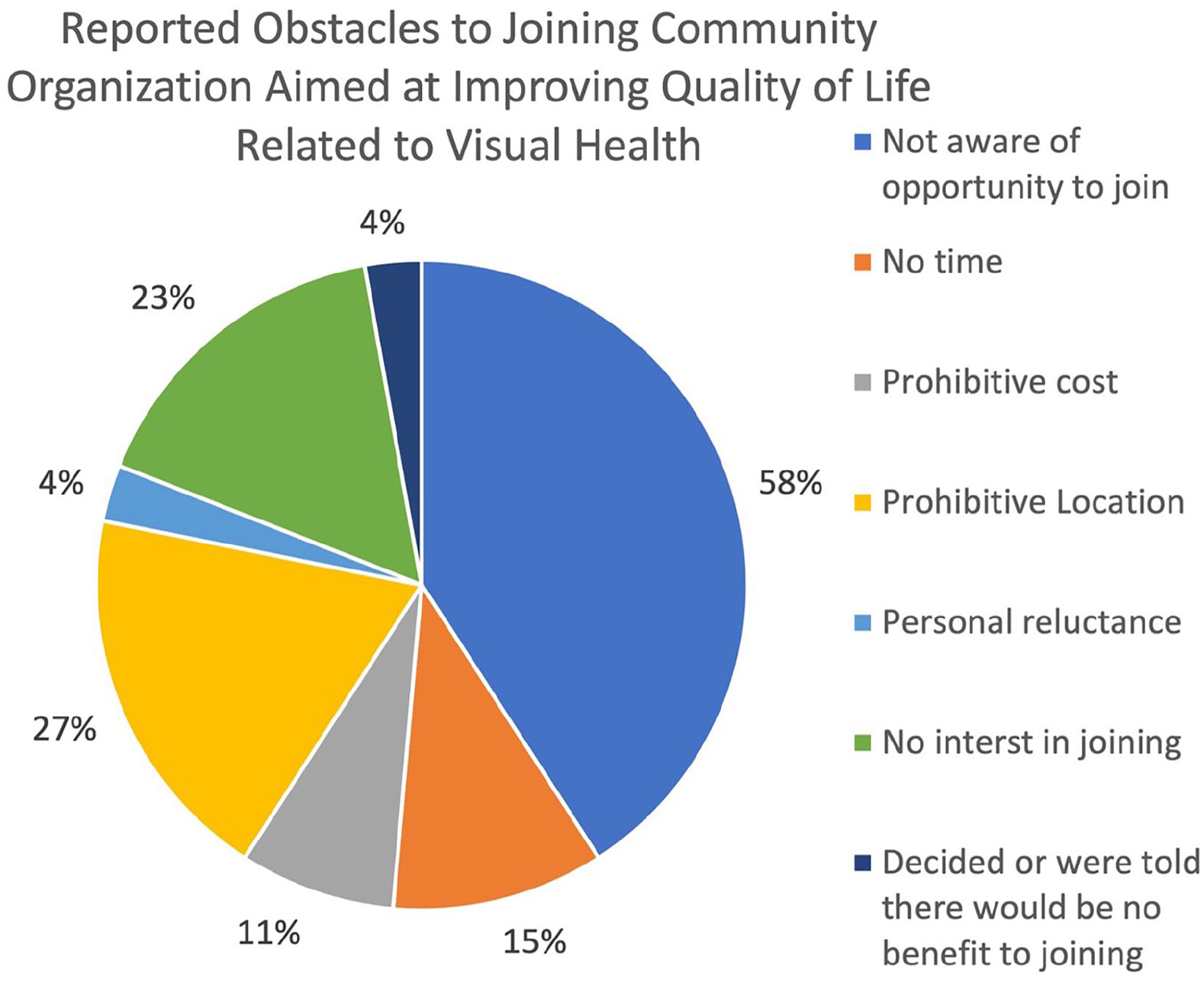
Obstacles to Joining Community Organizations that are Aimed at Improving Quality of Life Related to Visual Health.
Conclusion
Demographics
All survey participants were diagnosed with albinism or were filling out the survey on behalf of someone with albinism. About half had another family member who also had albinism. There was a wide distribution of ages, location, household income, marital status, and level of education, showing that despite the small size and time frame of this project, we were able to get a wide variety of individuals’ responses and that from these data we could extrapolate about the general US population with some limitations. However, the distribution of race was not as varied, with more than 80% of participants being white, even though albinism is more common in African American individuals in the United States. 24 A previous study in South Africa concluded that dark skinned individuals with albinism face stigma and othering due to myths and negative stereotypes. 25 There are no studies that have investigated this in the United States, but extrapolating the results of the study from South Africa, more research is needed to make conclusions about African Americans in the United States with albinism and their access, because the black experience with albinism seems to be inherently different from that of white individuals with albinism. Given the wide distribution of incomes in our cohort, it is difficult to draw conclusions regarding prevalence of poverty in the albino population. One 2024 study looked at cost-of-illness in inherited retinal diseases and concluded that non-health costs constituted 87%–98% of total costs for these individuals, specifically social support and services such as mobility training, occupational therapy, vision rehabilitation, assistive technology, and accessibility modifications could be contributing to diminished quality of life, poverty, and increased informal caregiving needs for individuals with IRDs. 26
Access to vision care
This population seems to have strong access to eye doctors, with most people seeing an eye doctor in the first 5 years of life and every few months to years currently. This population of patients also has a health insurance coverage of 85%, which is an improvement compared to the average US population, where only 50% of those aged 65 and older had at least one eye visit in any given year on Medicare, and only 7.3% of those aged 0–5 years, and 24.8% aged 6–17 years. 27 Most participants also responded that they have a good understanding of their care and feel that they were validated by their eye doctor, showing that this is not a major area of need in this population.
Access to genetic testing
There is room for improvement in access to genetic testing with 38% of responders not having undergone genetic testing. Of the individuals who did not get genetic testing done, 28% cited lack of opportunity and 33% high cost. Of the 5 individuals who cited not knowing where to get genetic testing, there was no discernable pattern among them with 40% being uninsured, and a variety of ages, highest degrees earned, and income ranges. Providing free or low-cost opportunities for more people to get genetic testing would be beneficial to this population. Location was a prohibitory reason for only one surveyed individual, who stated their geographic location prevents them from getting tested, showing this to be less of an obstacle. About 43% of our participants said that their decision to participate in research was at least in part to get genetic testing done, which shows that this is something patients are interested in and potentially otherwise do not have access to outside of a research study setting. Getting more advertising out to the general population about research studies that provide free genetic testing could be a good way to get more people access.
All individuals who answered that they were unaware of opportunities to get genetic testing had never seen a genetic counselor. This could indicate a strong reason to get a genetic counselor involved in the care of individuals with albinism, as this could help them be more aware of opportunities to get genetic testing, if that is something they are interested in. Primary care doctors, optometrists, and ophthalmologists who are seeing a patient with albinism should consider a referral to a genetic counselor for these individuals as part of their workup and diagnosis. Genetic testing is recommended by the American Academy of Ophthalmology and the European Reference Network for Rare Eye Diseases for all suspected or presumed IRDs with identified causative genes,28,29 but most clinical ophthalmologists are unfamiliar with genomic diagnostics. 1 In one 2021 study, providers felt that genetic testing was useful in IRD management but was infrequently utilized with only 1.5% of individuals with IRDs having genetic testing ordered by their ophthalmologist. 30 The current structure around IRDs and genetic testing does not adequately meet demand due to lack of IRD specialists and ocular genetic counselors, people with IRDs being geographically isolated, and limits in global use of genetic testing. 1 These problems will need more national and international policy changes and overhaul of education for medical providers and genetic counselors in order to be addressed, but talking about these deficiencies is a start.
About 34% said that their genetic testing results were inconclusive. Most of the time, this is because there are still genes that we do not know of, which cause albinism, and a lot of responders specified that their results were inconclusive because only one genetic mutation linked to albinism was found. The diagnostic yield of genetic testing for albinism according to other studies has a wide range. It was found to be 66% 31 and 91% 32 compared to 50.8% 33 and 78% 32 diagnostic yield for inherited retinal diseases overall. This means that in some individuals with albinism, genetic testing may not be diagnostic for their condition, potentially because they have a mutation that has not yet been linked to albinism. Foundation Fighting Blindness has a free program called “My Retina Tracker” that covers genetic testing for certain eligible inherited retinal disease diagnoses, but currently albinism is not eligible for the program.34–36 Based on the results of our study, a similar program to cover genetic testing in albinism would be beneficial to this group of individuals, both to cover their genetic testing and to help researchers identify more genetic mutations linked to albinism. Interestingly, 90% of responders felt like their genetic results did not affect their care—this could be due to the fact that even when genetic results are inconclusive, individuals can often have their diagnosis confirmed through detailed phenotypic assessments of their vision and skin.
There also seemed to be an association between individuals responding that they felt their questions were not fully answered and not seeing a genetic counselor after receiving their genetic results, this was true for 70% of the individuals who gave that response. Almost 90% of the responders who said they did not feel like their questions were answered either did not see a genetic counselor to discuss results or had inconclusive results, or both. This shows that it may be beneficial for anyone who gets genetic testing done to meet with a genetic counselor as it may result in more individuals feeling like their questions were answered and concerns were heard. There was also a smaller correlation (40%) with receiving an inconclusive genetic testing result and participants saying they did not feel like their questions were answered. There is no good solution for this, as more research is done and more genetic mutations are found to be associated with albinism, the number of inconclusive genetic testing results should decrease. In this case, speaking with a genetic counselor may also be helpful to get more information. Of our survey responders, 80% of individuals who received an inconclusive result did see a genetic counselor afterwards, so this may be less of an urgent area of focus.
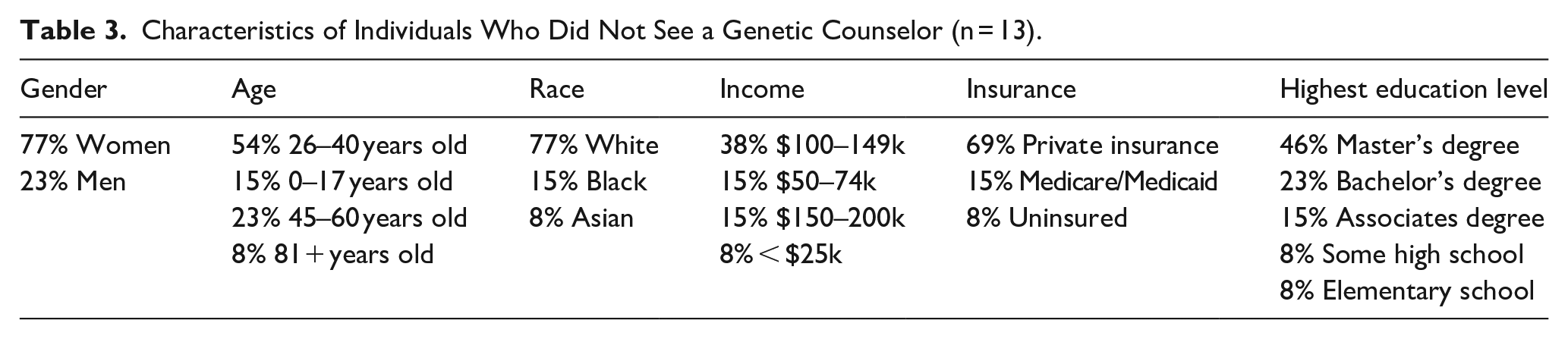
The average year of genetic testing was consistent with genetic testing becoming more frequent and accessible over time. All individuals who answered that it took 1+ years to get their results, completed genetic testing as part of a research study, showing that outside of this group, genetic testing results are received in a timely manner, so that should not be an obstacle to genetic testing. About 28% of individuals who got genetic testing did so as part of a research study and only one of those individuals was uninsured, showing that getting genetic testing for free through a research study may be a resource that individuals are not aware of. Based on Table 2, there did not seem to be a strong relationship between most demographics and getting genetic testing. However, a result that stood out was that 100% of individuals with income above 100–150k had genetic testing done, and the p value for the Fisher’s exact test evaluating income level and genetic testing reached significance at 0.0027, showing that this difference in income levels was unlikely to be due to chance. This result agrees with our finding that cost is one of the main prohibitive factors for getting genetic testing. Similarly, Fisher’s exact test for education level and likelihood of obtaining genetic testing was also statistically significant at 0.0139, which is likely due to certain education levels correlating with income. Based on Table 3, there did not seem to be any relationship between specific demographics and not seeing a genetic counselor to discuss genetic testing results.
Relationship Between Demographics and Genetic Testing.

Characteristics of Individuals Who Did Not See a Genetic Counselor (n = 13).
Access to community resources
About 58% of participants reported being unaware of community resources to improve their quality of life related to visual health, and 94% said that if they were to learn more about these resources they would want to get involved. This clearly indicates that there is room for improvement in advertising for community organizations that can help individuals with albinism improve their quality of life related to their vision care by hosting low vision clinics, educational sessions, and introducing them to other resources. This could be an area of focus for optometrists, ophthalmologists, family medicine doctors, dermatologists or other providers that work with patients with albinism routinely to tell more of their patients about nearby organizations that offer these services. As Table 4 shows, there was no clear relationship between certain demographics (such as having lower annual income or being uninsured) and being unaware of community resources. This was further supported by Fisher’s exact testing that did not reach significance for any of the demographic sub-categories analyzed. For this reason, providers seeing patients with albinism should discuss resources with all patients they see, regardless of insurance type, income, age, or other demographic factors.
Relationship Between Demographics and Awareness of Community Resources.

Limitations
Limitations of this study include a small number of participants and relatively short study period. The study was advertised on the NOAH website and to previous research participants at the MCW Eye Institute, but there is concern that individuals who are especially low income or who are not connected to the larger albinism community, do not know about (or do not have access to) the NOAH website and thus did not have the opportunity to participate in this study. It is possible that individuals who know about the NOAH website or have participated in research inherently have better access than those who do not and were not able to find the survey, thus our results may overestimate access to resources for the overall albinism community. By the nature of this study being an online survey, some individuals without access to computers or reliable Internet, including those who live in especially rural areas, may have been unintentionally excluded. Furthermore, the study is a voluntary survey, which lends itself to self-report bias.
Future efforts should be aimed at expanding genetic testing opportunities in the United States and worldwide, with European Reference Network for Rare Eye Diseases putting out a statement in 2021 calling for formal genomic testing pathways and arrangements to meet the demand for genetic testing and ensure access. 29 Greater access to genetic testing will benefit individuals, by giving them a better understanding of their disease, and society by furthering our understanding of the different albinism genotypes and phenotypes. There is need for expanding outreach and advertisement of local community resources to improve quality of life, because our study shows there is need for further knowledge about and utilization of these services.
Supplemental Material
sj-docx-1-map-10.1177_27550834251371501 – Supplemental material for Survey of genetic testing, community involvement, and vision care in Albinism
Supplemental material, sj-docx-1-map-10.1177_27550834251371501 for Survey of genetic testing, community involvement, and vision care in Albinism by Polina Prokhoda and Joseph Carroll in The Journal of Medicine Access
Footnotes
Acknowledgements
N/A
Ethical considerations
The study received ethical approval by the Medical College of Wisconsin (MCW) Institutional Review Board [PRO 40631] in June 2022 and followed the tenets of the Declaration of Helsinki.
Consent for publication
Respondents reviewed a statement on the first page of the survey regarding the risks and benefits of participating in the study and gave written consent by clicking the continue button if they agreed to participate on behalf of themselves or a minor.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported in part by the National Eye Institute of the National Institutes of Health under award number R01EY033580. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and material
N/A
Supplemental material
Supplemental material for this article is available online.
Trial registration number/date
PRO 40631/June 2022
Grant number
R01EY033580
Other journal-specific statements as applicable
N/A
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.