
Abstract
Background:
Achieving universal health coverage is one of the prominent targets of the United Nations’ sustainable development goals. Reducing out-of-pocket expenditure (OOPE) is essential because high OOPE can deter the use of healthcare services, which can lead to poor health outcomes and medical impoverishment.
Objectives:
The study sought to determine the effects of various factors such as Domestic General Government Health Expenditure, Gross Domestic Product, Government schemes and compulsory contributory healthcare financing schemes, and Voluntary health insurance schemes on OOPE per Capita in emerging economies.
Design:
Econometric methods using panel data
Data Sources and Methods:
The study analyzed the publicly available panel data from the World Health Organization using fixed, random, and dynamic models.
Results:
Domestic General Government Health Expenditure and Gross Domestic Product are associated with an increase in OOPE. Government schemes, compulsory contributory healthcare financing schemes, and voluntary health insurance programs are linked to a reduction in OOPE.
Conclusion:
In conclusion, this study, conducted through econometric methods on panel data, sheds light on the critical importance of reducing OOPE to achieve universal health coverage, aligning with the United Nations’ sustainable development goals. Countries shall implement a holistic approach focusing on preventive healthcare and health promotion, providing comprehensive health insurance, strengthening public health systems, and regulating medicine prices.
Plain language summary
This study examines how to make healthcare more affordable in developing countries. People often skip needed care due to high out-of-pocket costs (money paid directly for medical services). The researchers analyzed data across multiple countries to see what affects these costs. They found that while government spending on healthcare and a strong economy are good things, they can ironically lead to people paying more out of pocket for medical care. However, government healthcare programs, mandatory health insurance, and even voluntary insurance plans can all help bring these costs down. The study suggests that keeping these out-of-pocket costs low is key to achieving the United Nations’ goal of everyone having access to healthcare. Countries can achieve this by focusing on preventive care, ensuring everyone has health insurance, strengthening public health systems, and keeping the price of medicine under control.
Introduction
The United Nations’ sustainable development goals (UN SDGs) and their targets reflect a holistic approach to the overall development of all three elements of sustainability, such as environmental protection, economic efficiency, and social inclusion. Among its 17 goals, SDG 3 aims to ensure healthy lives and promote well-being for all ages. One of its prominent targets is to achieve universal health coverage (UHC), including financial risk protection, access to quality essential healthcare services, and access to “safe, effective, quality, and affordable essential medicines and vaccines for all.” 1 The concept of universality in UHC underscores the imperative that every individual should be afforded coverage, leaving no one behind. In addition, UHC requires that healthcare services are distributed based on an individual’s health needs, which means that those with greater needs, such as pregnant women, young children, and the chronically ill, should receive more services than others. Finally, the financial protection component of UHC stipulates that individuals’ contributions toward financing healthcare services should correspond to their capacity to pay. 2 UHC is an important strategy for achieving health equity. Health equity refers to equal access to healthcare for those in equal need 3 and access implies the timely use of services according to the need. 4 Amid a constantly evolving mix of players, initiatives, and objectives, the pursuit of health equity has remained a steadfast and cohesive objective of global health endeavors.
Achieving UHC necessitates a collaborative endeavor to reinforce the healthcare system, with health financing reforms constituting a pivotal component of this pursuit. The World Health Organization devised a health financing framework that emphasizes the integration of financing strategies into a national health policy, incorporating a service delivery plan. 5 The health financing transition refers to alterations in the level and makeup of health expenditure that coincide with economic progress. This transition encompasses two fundamental characteristics that are observable across countries and over time: (1) as economies develop, countries allocate more funds per capita to healthcare, and (2) out-of-pocket expenditure (OOPE) is less. Increasing health spending per capita will increase access as more resources are allocated. Reducing OOPE is important because high OOPE can deter the use of healthcare services, which can lead to poor health outcomes and medical impoverishment. 6 Various countries have put forward various trajectories to achieve UHC, which include social health insurance like payroll-tax financed schemes, providing public health services free of charge, and so on. 7 However, importing health financing reforms from one country to another without taking into account the distinctive circumstances of each country and its existing healthcare financing system is inadequate. The underlying causes of performance issues vary in each country, and it is these root causes that a health financing strategy must target with its proposed reforms. 5
OOPE and its determinants have received extensive attention in the literature. Previous macro-level investigations have identified various technological, institutional, socio-demographic, and health-financial factors (other than economic) as influential determinants of healthcare expenditures.8,9 Ke et al. 10 studied the trajectory of health expenditure in developing countries using panel data from 143 countries. A study conducted by Grigorakis et al. 11 investigated the influence of macroeconomic and public/private health insurance factors on OOPE across 26 EU and OECD countries from 1995 to 2013. Employing fixed/random effects and dynamic panel data methodology, the findings revealed a significant countervailing effect between public and private health insurance financing on OOP spending. A Tanzanian study found that non-communicable diseases impose a greater economic burden, leading to a higher risk of households experiencing catastrophic spending and impoverishment compared to communicable diseases. 12 Kitole et al.13,14 demonstrate the importance of equity in public social healthcare protection on household healthcare financing.
Despite existing studies, evidence from emerging economies is relatively scarce. Emerging economies, characterized by sustained market access, progress in reaching middle-income levels, and greater global economic relevance (Duttagupta and Pazarbasioglu 15 ), are home to about one-half of the global population. 16 In countries with emerging economies, the healthcare system faces various barriers like geographical inaccessibility, high cost of medical services, low availability of services including skilled manpower, lack of infrastructure, and technological barriers, which often lead to paper-based data collection and clinical information. 17 Apparently, various countries have made remarkable progress in implementing strategies for achieving UHC through many health financing strategies. For instance, India, one of the largest emerging economies, aimed in its National Health Policy to reduce the proportion of households facing catastrophic health expenditure from the current levels by 25% by 2025. 18 Subsequently, Pradhan Mantri Jan Arogya Yojana (PM-JAY), estimated as the world’s largest health insurance or assurance scheme fully financed by the government, provides a cover of Rs. 5 lakhs per family per year. The ongoing changes in healthcare systems across countries of emerging economies necessitate analyzing various aspects of OOPE. Such analysis can provide policy recommendations for improving healthcare access and achieving sustainability. Hence, this study aims to fill the gap by examining the effects of various financing schemes and gross domestic product (GDP) on the OOPE of emerging economies. The article is organized as follows: The next section explains the methodology, followed by results, discussion, and conclusion.
Method
Selection of countries
The countries with emerging economies were selected based on IMF listing. The countries were characterized as emerging economies based on their systemic presence, market access, and income. They were differentiated from advanced economies using five weighted variables: 0.40 × nominal GDP + 0.15 × population + 0.15 × GDP per capita + 0.15 × share of world trade + 0.15 × share of external world debt. The countries include Argentina, Brazil, Chile, China, Colombia, Egypt, Hungary, India, Indonesia, Iran, Malaysia, Mexico, the Philippines, Poland, Russia, Saudi Arabia, South Africa, Thailand, Turkey, and the United Arab Emirates These 20 emerging market countries account for 34% of the world’s nominal GDP in US dollars and 46% in purchasing-power-parity terms. 15
Selection of variables
Economic theory, particularly Keynesian principles, 19 suggests that individuals with higher income levels tend to have increased spending capacity on better quality food and healthcare services. Keynes highlighted the significance of income as a determinant of expenditure, introducing the concept of the marginal propensity to consume. Furthermore, total health expenditure encompasses both public and private components. Public health expenditure involves government and social insurance fund allocations, while private health expenditure includes OOPE and health insurance premiums. The impact of these expenditures on health status varies. An increase in out-of-pocket (OOP) health spending, a form of private health expenditure, can limit an individual’s spending on other goods and services, potentially leading to increased poverty and a cycle of deteriorating health. Conversely, an increase in public health expenditure may alleviate the burden of individual spending but could contribute to government budget deficits. However, it also contributes to societal health improvement, fostering human capital development and, in turn, promoting higher economic growth. 20 Low- and middle-income countries have experienced a significant shift toward demand-side financing mechanisms, giving prominence to Government-Sponsored Health Insurance (GSHI) schemes. Various GSHI initiatives have been implemented to improve healthcare service accessibility and shield individuals from financial crises associated with healthcare expenses. Two contrasting perspectives have emerged regarding private voluntary health insurance. Advocates assert that it has the potential to fill public financing gaps, while critics contend that private voluntary health insurance neglects social considerations, drives up healthcare costs, facilitates selective enrollment practices, and exacerbates inequities. 21
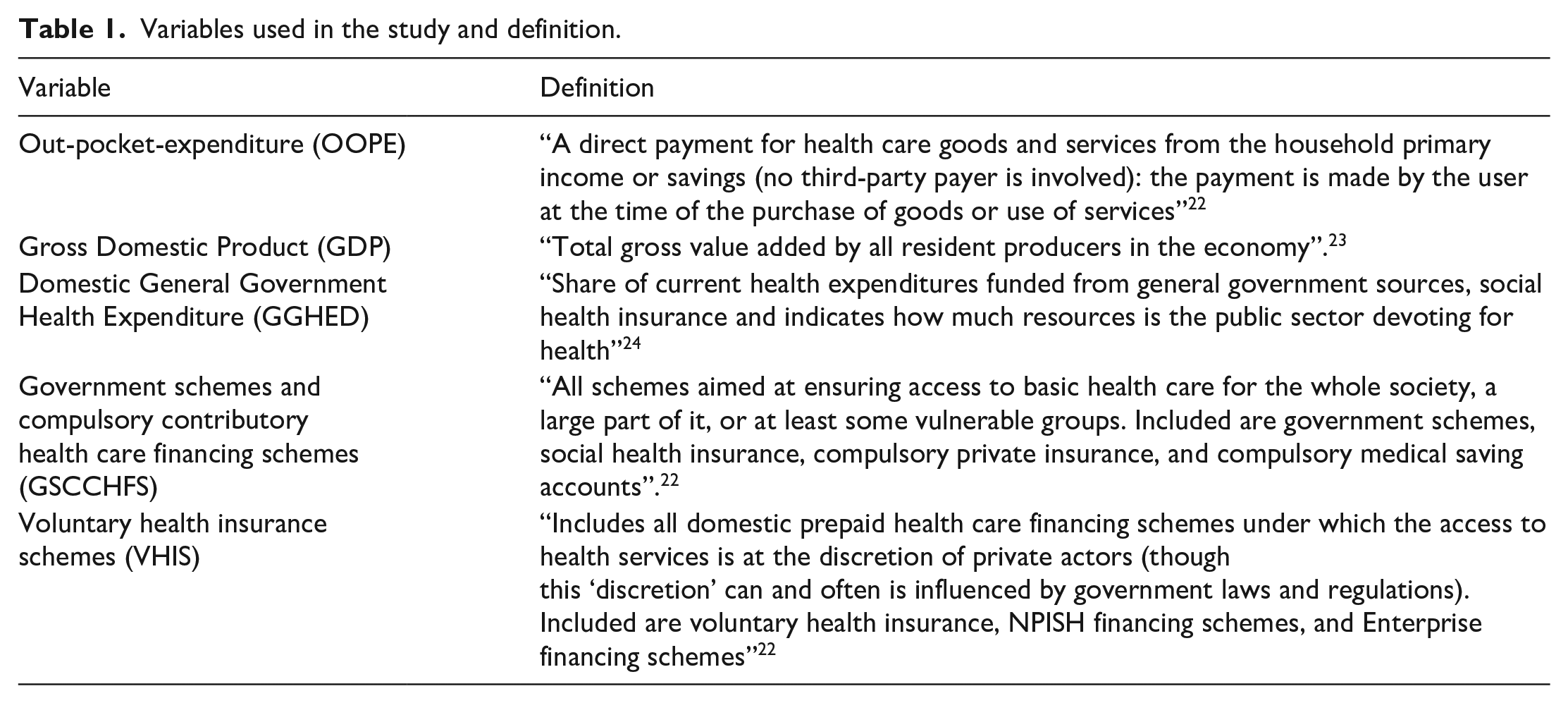
In the backdrop of the above, the current study explored the effect of Domestic General Government Health Expenditure (GGHED) per Capita, GDP per Capita, Government schemes and compulsory contributory healthcare financing schemes (GSCCHFS), and Voluntary health insurance schemes (VHIS) on OOPE. OOPE per capita was considered the dependent variable
The above indicators and sources are conceptualized in Table 1.
Variables used in the study and definition.
Data
Data from 2000 to 2020, retrieved from the WHO NHA database, 25 was used for the study. However, due to the incomplete data for the abovementioned variables, three countries (Saudi Arabia, Poland, and Turkey) could not be considered for the study.
Econometric model
Panel data, alternatively referred to as longitudinal or cross-sectional time-series data, entails tracking the performance of entities such as individuals, companies, countries, and states over a period. A panel data estimation is considered to be the best approach for studies covering multiple countries. Panel data estimation has various advantages over other methods like cross-sectional and time-series analysis: econometric models are more reliable, efficient, and improved as panel data analysis can provide a more accurate inference of the model with more degrees of freedom and sample variability; impact of omitted variables can be controlled; inter-individual differences are taken into account; and for countries with unbalanced panel data. Different data periods can be considered. 20 Hence, this study first analyzed static fixed effects panel data analysis followed by a dynamic model.
The static model allows for variable intercepts to represent country effects. The below equation is considered for the study following Rahman et al. 20


where
The individual impact of dependent variables on OOPE is estimated by using the following equation

Statistical estimations
Panel data estimations are generally of three types: Pooled OLS Method, Fixed effect (FE), and random effects (RE) method. In the pooled OLS method, all the observations are pooled together for running regression, indicating that there is no heterogeneity or individuality in cross-sectional units. The fixed effect method allows heterogeneity among the cross-sectional units by allowing them to have their own intercept value. This indicates that the intercept of individual or cross-section units may differ, but the intercept does not vary over time. Also, it is time-invariant and allows the cross-sectional effect to be correlated with regressors. On the other hand, in the random effect method, the “unobserved heterogeneity” behaves in a random fashion, and the cross-sectional effect is not allowed to correlate with the regressors, that is, Cov(X,α) is assumed to be zero. Hausman’s test was also conducted as a specification test to determine the best fit between FE and RE. In Hausman’s rest, the null hypothesis implies that RE is consistent. Apparently, many economic relationships are dynamic in nature, and panel data enables the researcher to have a better understanding of the dynamics of adjustment. Dynamic relationships are characterized by having a lag-dependent variable among the predictors. The “pmg” function can estimate linear panel models with heterogeneous coefficients using different Mean Groups estimators. When specifying the argument model = “mg,” the standard Mean Groups estimator, which averages individual time-series regressions, is used. If model = “dmg,” cross-sectional demeaning is performed to reduce the impact of common factors, similar to what is done in homogeneous panels when model = “within” and effect = “time.” Finally, if the model = “cmg,” the CCEMG estimator is used, which is consistent with the assumption of unobserved common factors and idiosyncratic factor loadings. This method incorporates cross-sectional averages of the dependent variable and predictors to account for common factors, along with individual intercepts and trends. 26 Hence, we estimated the dynamic model of panel data as well. All the models were estimated using Rstudio 2023.12.1
Results
The descriptive statistics of the variables are listed in Table 2. The OOPE trends in various income groups are presented in Figure 1. The plots show that OOPE is increasing among countries, but there has been no rapid increase in OOPE since 2010 in most countries. Plots where OOPE is plotted against GDP, GGHED, and VHIS are presented in Figures 2–4, respectively. The results for FE, RE, and DM are presented in Table 3. The Hausman test gave a p-value less than 0.05(χ2 = 49.285, df = 4, p value = 5.091e−10), and the null hypothesis of the fixed effect model being consistent cannot be rejected. The FE, RE, and MG models imply that OOPE increases with GDP. FE and RE indicate that GGHED has a significantly positive effect on OOPE. GSCCHFS and VHIS have a significant negative relationship with OOPE.
Descriptive statistics.


OOPE (2000–2020) in Emerging economies according to the income groups.

GDP vs OOPE Income group-wise.

GGHED vs OOPE Income GroupWise.
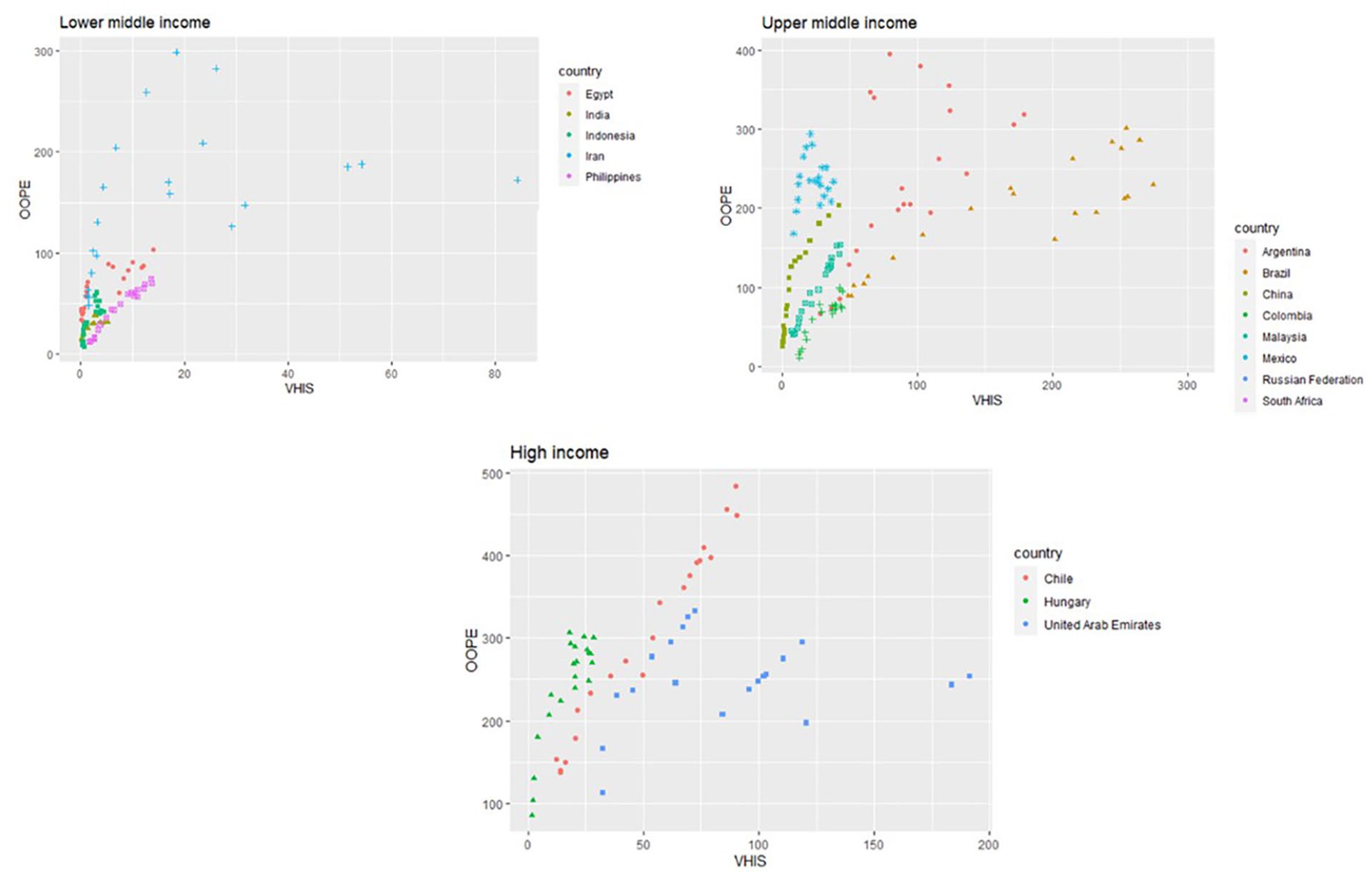
VHIS vs OOPE Income GroupWise.
Results of fixed, random, and dynamic panel data models.
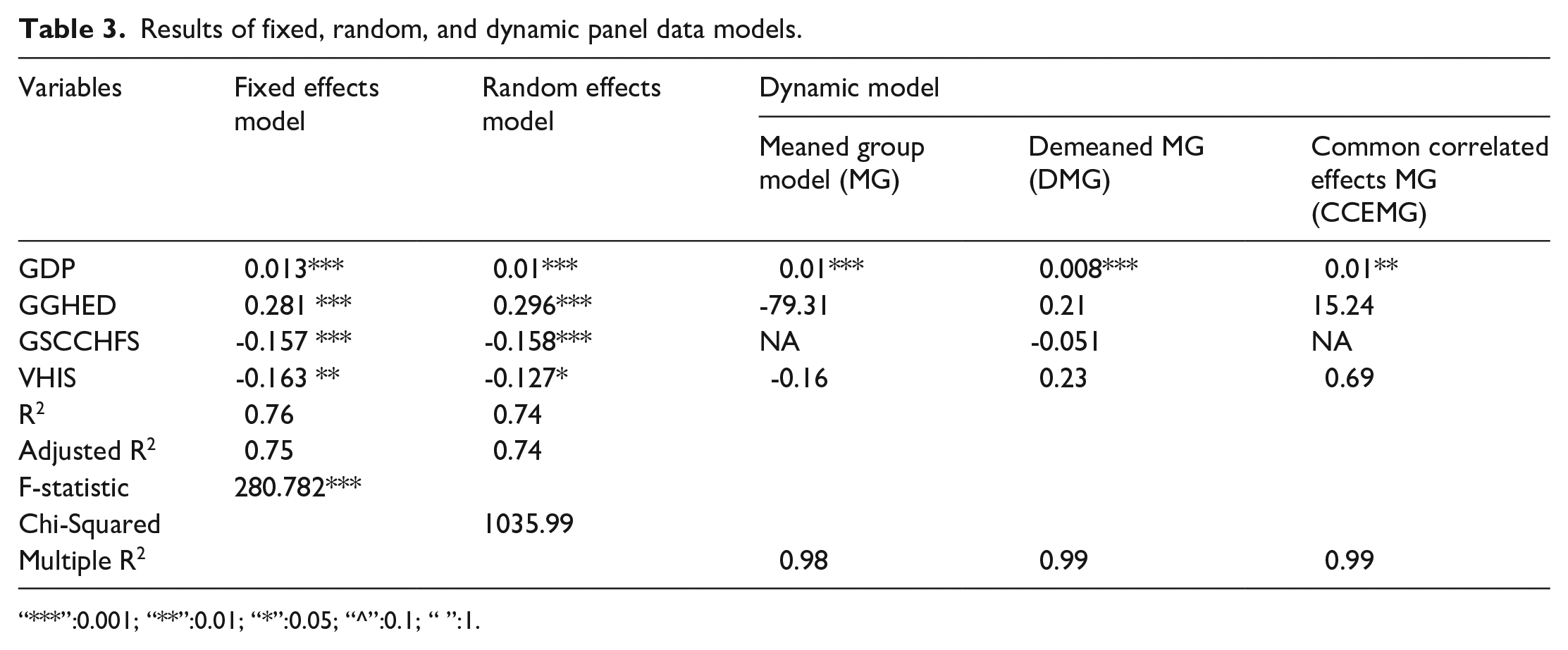
“***”:0.001; “**”:0.01; “*”:0.05; “^”:0.1; “ ”:1.
Discussion
While observing the OOPE across the years, many of the countries do not show a steep increase. This might be due to the implementation of efforts like the Millennium Development Goals 2000 (MDG). MDGs targeted to eradicate extreme poverty and hunger, achieve universal primary education, promote gender equality and women empowerment, improve maternal health, reduce child mortality, combat infectious diseases, and ensure environmental sustainability with global partnership and development by 2015 and beyond. MGDs paved the way for health promotion and infrastructure improvements across the globe. Following MDGs, SDGs also called on nations to implement financial protection for their citizens to reduce OOPE.
A positive and highly significant coefficient indicates that a higher GDP leads to higher OOPE. The positive correlation of GDP with OOPE is consistent with various other studies in the same context.10,27 This trend may be attributed to factors such as healthcare price inflation, greater adoption of costly medical technologies, and increased expenses linked to chronic diseases and aging populations. The positive correlation between GDP and OOPE suggests that as a country’s overall economic wealth expands, individuals tend to spend more OOP on healthcare. This observation raises several implications and potential explanations. Primarily, it may indicate that rising GDP correlates with heightened healthcare utilization or increased demand for healthcare services. This surge in demand could result in individuals spending more OOP, particularly if there are constraints in public healthcare coverage or if individuals opt for higher quality or specialized services not fully covered by public insurance schemes.10,27
The positive and highly significant GGHED coefficient suggests that greater government healthcare expenditure per capita is associated with higher OOPE. This could be due to increased utilization of publicly funded services or induced demand. Furthermore, the effect of GGHED can be explained by observing the components of the same: Social health insurance and compulsory health insurance. Social health insurance (SHI), which is legislated by the government, requires compulsory regular contributions from a specific group of people, primarily in formal employment and further extending to other groups. 28 Compulsory health insurance is the mandatory insurance that every citizen of a country must have. However, various studies have discussed schemes like SHI’s potential for achieving health equity. The results indicated that increasing OOPE may be due to the inability of the insurance to comprehensively cover the treatment expenses, which in turn transfers the burden to OOPE. Adding to this, improper policy designs and implementation, economic and political context, inadequacies, and inefficiencies in the system, including corruption and abrupt inflation of health services, could have contributed to the ineffectiveness of such domestic health expenditures, thus increasing the OOPE.
A negative and significant relationship of GSCCHFS indicates that greater government social health and family security expenditure per capita is associated with lower OOPE. This could be due to these programs providing alternative financing sources for healthcare. A negative and significant relationship of VHIS suggests that private health insurance coverage is associated with lower OOPE. This is expected as insurance covers a portion of healthcare expenses. Countries are advised to prioritize prepayment mechanisms and minimize their dependence on OOP payments for financing healthcare. Merely increasing government spending does not necessarily lead to a reduction in overall OOPE, particularly in countries with low government health spending. While increased spending may result in more available services, without addressing the overall structure of healthcare expenditure, it could also lead to increased OOP payments by individuals seeking these services. Thus, enhancing financial risk protection against OOP health expenditures in low-income countries necessitates a substantial increase in government spending and the establishment of a robust health financing system.
As fiscal space increases, governments tend to invest more in social sectors, including health. The fixed budget share, even without a higher priority for health, at least ensures an increase in absolute amount. In times of economic crises or negative economic growth, maintaining a fixed budget share for the health sector can lead to a reduction in the actual amount of funding allocated to the sector. Furthermore, different budget allocation methods, such as a fixed percentage or fixed absolute amount of funding, may affect health spending differently. 10
Policy implications
Amid the rising momentum of diseases, there is an immediate need to reduce OOPE to attain sustainability. The study proposes the following as a holistic policy approach for reducing OOPE.
Health promotion and preventive healthcare: policies must enable health promotion activities in various areas of life. Involving workplaces, residential areas, education institutions, etc., for health promotional activities and thereby educating people, which can facilitate preventive healthcare.
Comprehensive insurance coverage: the government expenditures will be reduced OOPE if it is designed and implemented properly. Health insurance must cover all minor and major ailments so that the public does not need to do any OOPE. Furthermore, there should be equitable access regardless of the insured amount or medium. The coverage must also focus on vulnerable populations and emerging diseases.
Strengthening public health systems: strong public health systems with state-of-the-art infrastructure can reduce the need for specialized care and, thereby, reduce OOPE.
Price regulations: in order to ensure affordability and prevent price gouging, governments can regulate the prices of essential medicines, medical devices, and healthcare services.
Addressing these challenges requires a comprehensive and adaptive approach involving collaboration between government bodies, healthcare providers, insurance entities, and the public, alongside careful consideration of the specific context and dynamics within each healthcare system. However, the implementation of policies encounters multifaceted challenges. Insufficient political commitment, financial constraints, and inadequate healthcare infrastructure pose hurdles to policy effectiveness. Resistance from stakeholders, legal complexities, and cultural factors further complicate the implementation process. Moreover, economic instability and external shocks, such as pandemics, can divert resources away from sustained policy efforts. In 2020, health systems exhibited shortcomings in either safeguarding individuals from the financial burdens of healthcare or sustaining access to essential services, signifying a lapse in fundamental functions. If the response to the COVID-19 pandemic in 2020 intensified a trend toward increased reliance on private healthcare, there is a necessity for policies that address cost coverage within this sector. In addition, initiatives encouraging patients to revert to the public sector are essential to uphold financial risk protection. 29 Alongside these challenges, equity issues emerge,13,14 as vulnerable populations may face barriers in accessing reduced OOPE benefits, exacerbating existing healthcare disparities. A strategic framework for reducing OOPE is presented in Figure 5.

A strategic framework for reducing OOPE.
Limitations and future directions for the study
The study could include data from 2000 to 2020 only, post which, there were various changes globally in healthcare spending due to COVID-19 and associated emergencies. The trend might differ in the current circumstances. Due to overburdened public hospitals, individuals often resort to private healthcare, which has been linked to a higher risk of incurring catastrophic health expenditures. This is concerning because the proportion of OOP spending directly impacts both financial security and access to necessary care. 30 Furthermore, the study acknowledges that many other variables, like health system characteristics, provider payment mechanisms, and so on, can affect OOPE. However, the modeling approach, including all such variables, was not feasible due to the unavailability of the data. The study urges future research to dig deep to understand various mechanisms to reduce OOPE.
Conclusion
The study sought to determine the effects of various factors like Domestic General Government Health Expenditure, Gross Domestic Product, Government schemes and compulsory contributory healthcare financing schemes, and Voluntary health insurance schemes on OOPE per capita in emerging economies. The study successfully analyzed the available panel data using fixed, random, and dynamic modes. It has been concluded that Domestic General Government Health Expenditure and Gross Domestic Product positively impact OOPE, similar to the previous studies. The government’s compulsory contributory healthcare financing schemes and voluntary health insurance have a negative effect on OOPE. The study’s results can guide the development of evidence-based policies to enhance the efficiency and equity of healthcare financing systems. For instance, if the econometric analysis identifies specific variables significantly impacting OOPE, policymakers can focus on implementing measures to address those variables, such as improving income levels, optimizing public health spending, or enhancing health insurance coverage.