
Abstract
Background:
Both constrained access to essential medicines and combatting marketing of substandard and falsified (SF) medicines are unmet health sector goals in Africa.
Objective:
To answer the question of how improved access can reduce the continuous surge of SF medicines in Africa.
Design:
We conducted a scoping review based on standard protocol.
Methods:
We searched articles published in the English language from PubMed/Medline, Cochrane Library, Embase, Scopus, Web of Science, and Google Scholar by using a systematic search query.
Results:
Seventy-one articles were included in this review. Access to quality essential medicines is still a major problem in developing countries in Africa and will continue as a threat for the next decade of health care. Ensuring access to quality medicines and preventing SF medicines in Africa need a systematic approach to address their underlying causes. Failure to ensure access to medicines is the major reason for the availability of SF medicines. Improving access to quality medicines can reduce SF medicine marketing and use. Manipulating the entire supply chain for efficiency, avoiding trade agreements that could reduce access, using compulsory licensing provisions, and pharmaceutical price control, providing incentives for drug development, and promoting rational use of medicines can improve access.
Conclusion:
Ensuring access to medicines and preventing SF medicine marketing cannot be achieved in the planned period in developing countries in Africa unless a comprehensive strategy is used. Improving access to quality medicines can reduce SF medicine marketing and use, that is, ensuring access through uninterrupted supply, improved efficiency, enhanced local production, preventing SF medicine entry, improved medication use system, and improved affordability. Therefore, it is essential to improve supply chain capability, address challenges of the supply chain, improve leadership and governance, establish country-specific anti-counterfeiting and anti-substandardization committees, and collaborate with all relevant stakeholders.
Plain Language Summary
Ensuring access to quality medicines and preventing SF medicines in Africa need ensuring access through uninterrupted supply, improved efficiency, enhanced local production, preventing SF medicine entry, improved medication use system, and improved affordability.
Keywords
Introduction
Health care services provided to patients should be safe, effective, patient-centered, timely, efficient, and equitable.1,2 Marketing of substandard and falsified (SF) medicines negatively affects patient safety, the national economy, public trust in the health care system, and the global health care system through increased emergence and transmission of resistant pathogens. 3 The use of SF medicines also increases the emergence of resistant microorganisms. Self-prescription and self-medication are contributing to SF marketing and use. 4 This along with static antibiotic pipeline (inadequate production of novel antibiotics) to tackle resistant microbes will increase global health threats from infectious diseases. 5 In addition to its adverse health effects, the marketing and use of SF medicines are associated with societal economic costs. 6
The crime against humanity through the marketing of SF medicines is one of the most complex safety problems in the health care delivery system of developing countries,7 –12 where access to quality medicines is limited or implementation of good pharmaceutical manufacturing practices is poor or absent. 3 The prevalence of SF medicines is high in developing countries. 7 Africa is a destination for about 42% of all SF medical products globally and 50% of Internet market drugs SF in Africa. 13 Another study also revealed the median prevalence of SF medicines among 25 low- and middle-income countries (LMICs) was 28.5% (11%–48.0%). 14 This means more than 4 out of 10 patients were taking medicines that would not meet their needs. Globalization of the pharmaceutical market and the use of technology including telemedicine and cyber medicine are contributing to the spread of SF medicines to developed countries. 15
Achieving universal health coverage, access to quality essential health care services, and equitable access to quality medicines; and supporting research and development of medicines for communicable and noncommunicable diseases that affect developing countries are two sustainable development goals (SDG) related to access to medicines. 16 Ensuring access to medicines (i.e. availability, affordability, accessibility, acceptability, and quality) and combating SF medicine marketing and use are unmet needs of SDG in developing countries.16,17 In addition, SF medicine marketing is a politically sensitive, complex process involving multiple players in the field.18 –21 Ensuring access to medicines and preventing SF medicine marketing are unachievable in the planned period, particularly in developing countries.7 –12 There is limited global collaboration toward SF medicine research with relatively better collaboration among the United States, the United Kingdom, and Germany. Dealing with these multi-sectoral problems in LMICs needs consideration of different strategies to deal with the root causes of the problems. Therefore, this scoping review was conducted based on standard protocol to answer the question of how improved access to essential medicines can reduce the continuous surge of marketing of SF medicines in Africa. 22
Methods
Data sources and search strategy
We searched articles published in the English language from the following databases: PubMed/Medline, Cochrane Library, Embase, Scopus, Web of Science, and Google Scholar by using a systematic search query provided under supplemental material from December 2000 to 31 December 2022. The following LMICs from Africa were included in the literature search. These countries include the Eastern Africa Community (EAC) region (Kenya, Tanzania, Uganda, and Ethiopia),23,24 Algeria, Angola, Ghana, 25 Kenya,26,27 Cameroon, and the Democratic Republic of Congo,28,29 Malawi, 30 Niger, 26 Nigeria,31 –33 Ethiopia,34 –36 Zambia,37,38 Uganda, 39 Tanzania, 25 and Zimbabwe. 40 The Southern African Development Community (SADC) (Angola, Botswana, Comoros, Democratic Republic of Congo, Eswatini, Lesotho, Madagascar, Malawi, Mauritius, Mozambique, Namibia, Seychelles, South Africa, United Republic Tanzania, Zambia, and Zimbabwe).41,42
Study types
Cross-sectional studies, observational studies, reviews, and case and control studies addressing access to medicines, marketing of SF medicine, prevention and control of SF medicine marketing and use, alignment of drug development drug policy research to public need, rational use of medicines, and global trade agreements related to access to medicines in Africa were included, whereas conference reports, case studies, books, and guidelines were excluded from the study.
Study selection
Selection and identification of potentially relevant articles were made based on the inclusion–exclusion criteria. Five hundred thirty-seven articles were retrieved by using the above search strategy, after removing duplications by using ENDNote Version 20, and 71 of them were found to be relevant for this review. The article selection process was drawn in the preferred reporting items for systematic review and meta-analysis (PRISMA) flow chart (Figure 1). 43 Two investigators independently reviewed each study’s abstract against pre-specified inclusion and exclusion criteria. Due to the variety of included studies (i.e. each study design has a different quality assessment tool) and the nature of the intended review (i.e. scoping review) in which data pooling is rarely involved, we did not evaluate the quality of included studies.
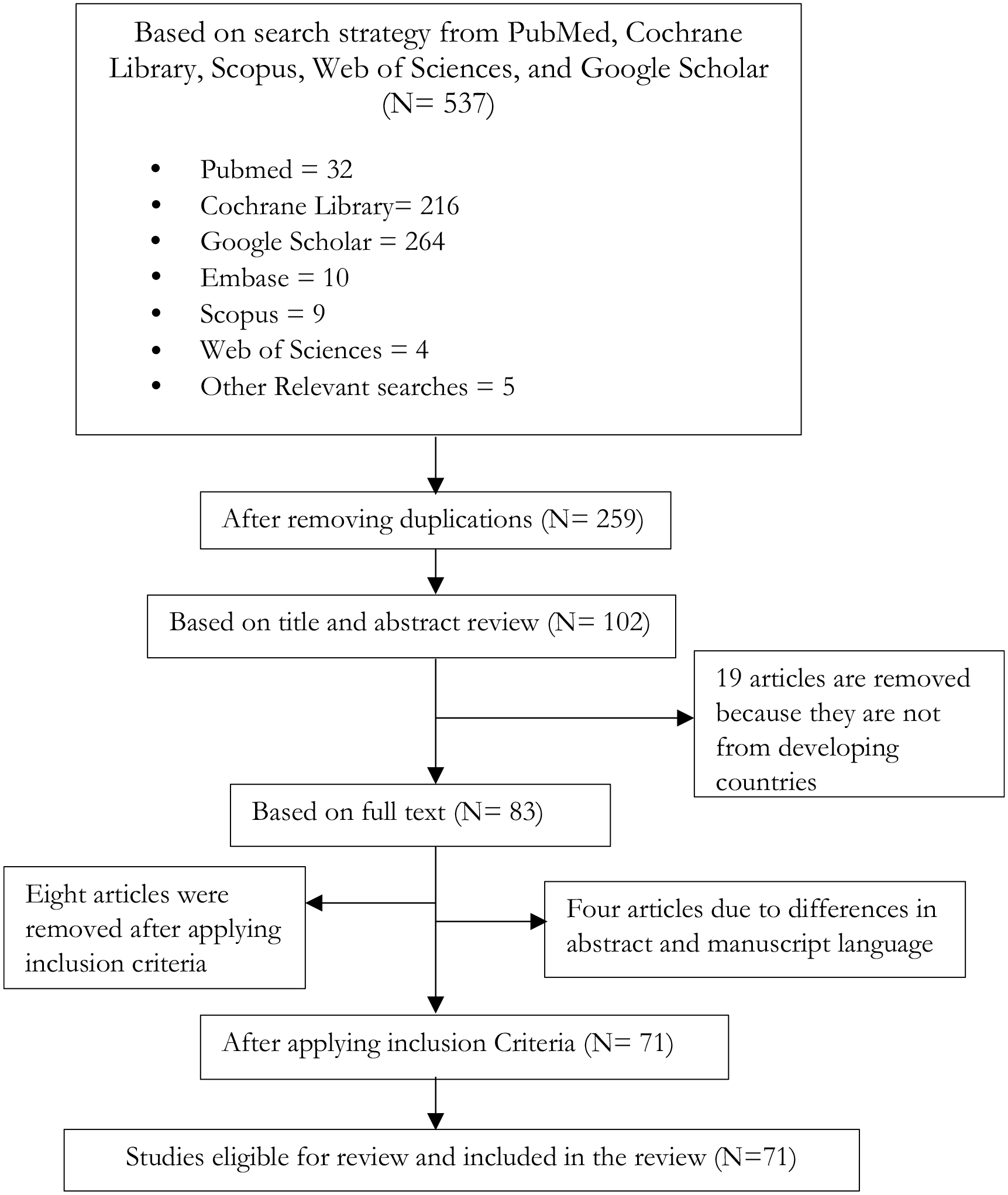
PRISMA Flowchart representing the result of the search and the number of articles excluded and eligible for review.
Data extraction
Two investigators reviewed the abstracts of all included studies. Access to medicines, marketing of SF medicines, prevention and control of SF medicine marketing and use, constrained access to essential medicines, alignment of drug development, and public need in Africa were addressed during abstraction. The third investigator checked these data for accuracy.
Data synthesis and analysis
We qualitatively described and synthesized data on constraints to access to quality essential medicines and the reasons for SF medicine marketing. In addition to this, we described strategies and opportunities for improving access to essential medicines in resource-constrained health systems.
Results
Description of included studies
Thirty-two articles were included in this scoping review. The included articles addressed the following six domains: prevention, detection, and response to SF medicine marketing and use13,33,41,44,45; regulatory framework and national capacity25,31,35,46,47; SF medicine marketing control challenges27,28,30,36,48; and health and economic burden of SF medicines.14,32,38,49,50 The role of collaboration and networking for combatting SF medicine marketing and use,26,39,51,52 strategies for combating SF medicines including improved access,16,41 poor alignment of research and development with the public need,16,53 –56 and policy framework and leadership commitment.25,35,40,41,47,56,57 A majority of studies emphasized the importance of addressing both access to medicine and SF medicine problems together.14,26,32,38,39,49 –52
Strategies to address SF medicine marketing and constrained access together can improve success rate and efficiency in resource utilization while fighting these unmet needs. In this scoping review, we discussed the following shared strategies: (1) prevention, detection, and response to SF medicines13,33,41,44,45; (2) supply chain and trade-related factors58 –65; (3) policy framework and regulatory capacity41,53,54,65–73,70 –73; (4) misalignment of new drug development research and the public need16,53 –56,74 –78; and (5) health system leadership commitment.40,56,79 –89 Finally, a systematic approach to address constrained access to medicines and counterfeiting was discussed.16,53,54,65,66,90
Prevention, detection, and response to SF medicines
The toll burden of SF medicines is in sub-Saharan Africa (SSA). For example, among 39 SSA countries, poor quality antimalarial drugs were attributed to 122,350 children below 5 years of age, and 74,188 children’s deaths were attributed to SF antimalarials in Nigeria per year. 91 Marketing and use of SF medicines are associated with economic (productivity loss, lost income, increased poverty, wasted resources, and increased out-of-pocket expense) and health (increased morbidity and mortality, progression of antimicrobial resistance, and loss of confidence in health care system) impacts. 41 Therefore, prevention, detection, and control of SF medicines are critical. Five articles addressed the prevention, detection, and response to counterfeit medicines.13,33,41,44,45 The extent of SF medicine marketing is highly variable among high-income, LMICs. For example, the prevalence of SF medicines is 20%–40% in LMICs and about 1% in high-income countries. 20 Africa alone is a destination for about 42% of global SF medicine marketing. 13 Developing countries are facing a dual problem (i.e. constrained access and SF medicines). Indeed, the first is the major cause of the latter. The core dares/challenges for access to medicines are inadequate financing, unaffordability, weak quality assurance, irrational use, and poor alignment of research and development with the public need16,27,28,30,36,48,53 –56 (Figure 2).
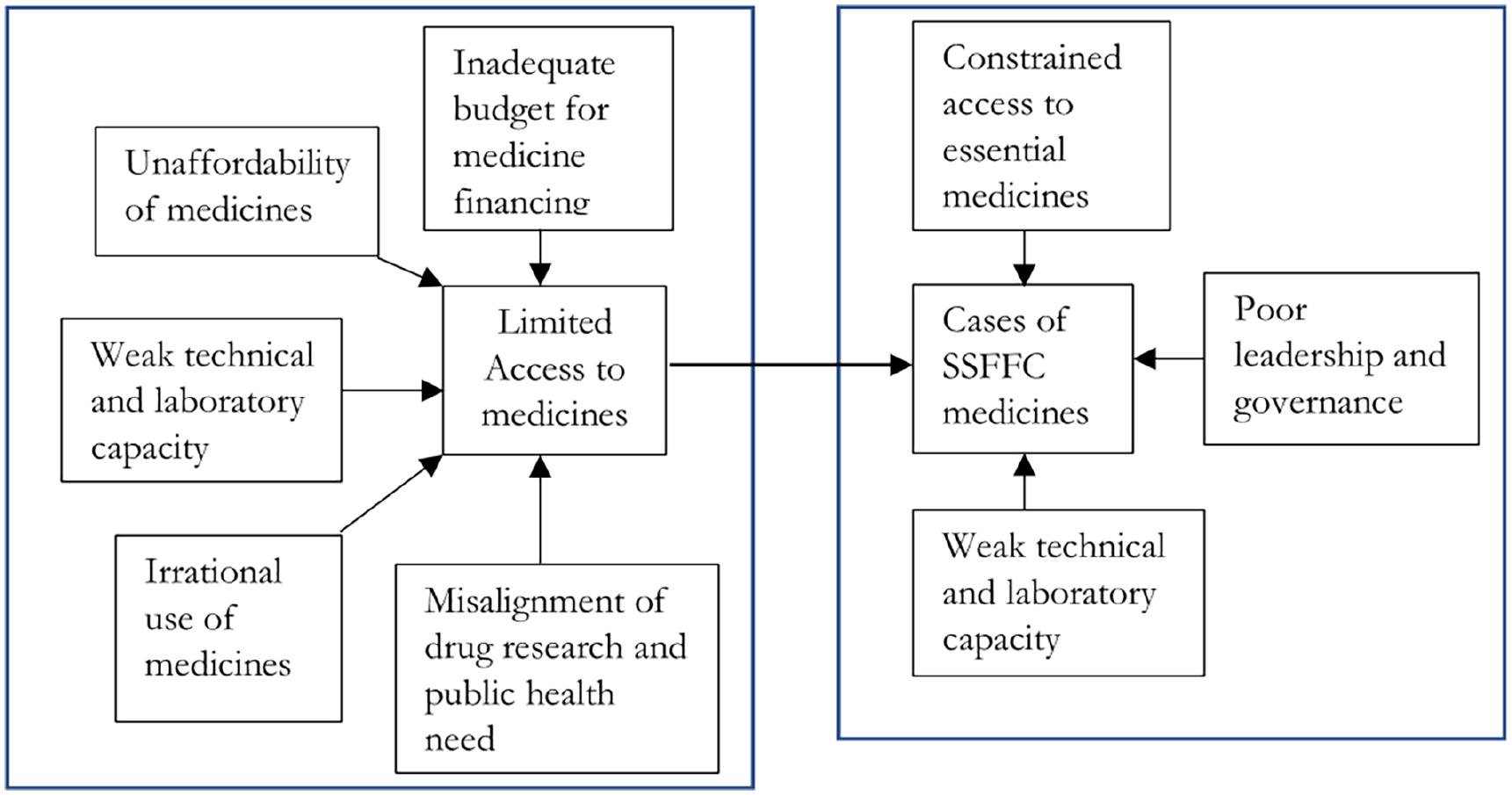
Relationship between cases of limited access to essential medicines and substandard and falsified (SF) medicines.
Supply chain and trade-related factors
Ensuring comprehensive pharmaceutical supply chain maturity and security at different levels is critical for improving access and reducing SF medicine marketing. Comprehensive supply chain capacity and maturity are defined in terms of the following core components: political commitment; strategic planning and management; human resource management; financial sustainability, policy and governance, evidence-based drug selection, forecasting and supply planning, good procurement, information management, quality control, and pharmacovigilance (PV); warehousing and storage; distribution; rational drug use; and waste management58,59 (Figure 3).

Conceptual framework for capability, maturity, and security of health supply chain at the national level, adapted from global supply chain network. Note: LMIS: logistic management information system; MIS: management information system; SOPs: standard operating procedures; KPIs: key performance indicators; &: and.
Patents of brand products are barriers to access to essential medicines for developing countries. 60 In response to this, the World Trade Organization’s Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) flexibilities is introduced. 61 The agreement affirms governments’ rights to grant compulsory licenses, the right not to enforce pharmaceutical product patents for some time, and contains an amendment to help countries that are incapable of manufacturing medicines to import them under a compulsory license.62,63 In addition to this, it is important to avoid or reduce TRIPS agreements that can reduce equitable access to quality medicines. 92 These include TRIPS-Plus intellectual property protections; investment pro-tection; procedural requirements for pharmaceutical pricing and reimbursement programs; provisions with implications for regulation of pharmaceutical marketing; regulatory requirements for assessment of safety, efficacy, and quality; and reduction/elimination of tariffs on medicines or their ingredients. 92 In addition to this rules applying to government procurement of pharmaceuticals; rules applying to state-owned enterprises and designated monopolies; procedural requirements for customs administration and trade facilitation; and rules applying to regulatory practices, cooperation, and coherence. 92
Lack of utilization of evidence-based health information is another factor affecting the establishment effective pharmaceutical supply chain. 64 This is because the entire supply chain process requires quality logistic management information system (LMIS) data. For example, the distribution system needs quality data to maintain a steady supply of pharmaceuticals and supplies to facilities where they are needed while ensuring that resources are used most effectively. A well-run distribution system should constantly supply medicines, keep medicines in good condition, minimize medicine losses caused by spoilage and expiry, rationalize pharmaceutical storage points, use available transports as efficiently as possible, reduce theft and fraud, provide information for forecasting medication needs, and incorporate quality assurance programs. 65
Another problem relies on the manufacturing process (i.e. raw material development to patient use). Every ingredient has its supply chain before it ever becomes a final dosage form, and at each stage, there are distribution, storage, and price markups. This indicates the possibility of counterfeiting and corruption in an entire supply chain.20,88,89
Regulatory capacity-related factors
The policy framework and leadership commitment include policy and legislation in fighting SF medicines, regulatory and industry response to SF medicines, and awareness creation and community response to SF medicine. 41 Another significant contributor to SF medicine marketing is weak technical and laboratory capacity.53,54,66,67 Critical points for quality assurance of pharmaceutical procurement include product selection, product certification, contract specifications, inspection of shipments, targeted laboratory testing, and post-marketing problem reporting system or PV. 65
Pharmaceutical policy-related factors
The objective of pharmaceutical policy is to ensure equitable access to quality medicines, promote rational use of medicines, enhance domestic production capacity, and ensure health security. Underreporting the incidence of SF medicines is a significant barrier to access to quality essential medicines in developing countries.68,69 Establishing functional PV contributes to ensuring access to safe, effective, affordable, quality-assured essential medicines.17,70 –73 The success of PV requires the involvement of many stakeholders, including consumers, health care professionals, drug and therapeutic committees, market authorization holders, public health programs, drug regulatory agencies, drug advisory committees, academia, and research institutions, and the World Health Organization (WHO) collaborating center for international drug monitoring (Figure 6).17,70 –73,93
Irrational use of medicines is another constraint to access to medicines. 56 Tackling the problem of irrational medicine use is important to improve health care delivery toward ensuring patient safety, allowing for optimal utilization of resources, and improving access to medicines. 94 This is because about 25%–70% of overall health expenditure in developing countries is on medicines, and the irrational use of medicines increases health care costs, treatment failure, and antimicrobial resistance. These factors together lead to the shifting of the limited health budget from financing medicines to health care.95 –97 Core interventions to promote rational use of medicines include multi-disciplinary national bodies to coordinate medicine use policies, using clinical guidelines, developing and using essential medicines lists, establishing drug and therapeutics committees in hospitals, problem-based pharmacotherapy training, and continuous in-service training medical professionals as a licensure requirement. Super-vision, audit and feedback, independent information on medicines, public education about medicines, avoiding perverse financial incentives, appropriate and enforced regulation, and sufficient government expenditure to ensure the availability of medicines and staff.65,96
Another hurdle to access to medicines in LMICs is the lack of production of some important medicines like medicines for neglected tropical diseases and drug-resistant tuberculosis, either due to insufficient local production or misaligned research and public need, 56 or inadequate health care financing is one of the reasons for constrained access to essential medicines in developing countries. In contrast to this inadequacy, approximately 20%–40% of all health care resources were wasted.98,99 Improving access to these medicines requires incentives for drug research and development, and improvement in health system efficiency.74,100
Misalignment of new drug development research and the public need
Other approaches to improve access to medicines include exploring research and development alignment with the public need-related factors.16,53 –56 Pharmaceutical innovation is different from innovation in other sectors, because of the greater need for patents, agency relationships, information asymmetry, selling of intermediate outcome (health care), and the third party pays. Therefore, it is important to provide appropriate incentives (financial and nonfinancial) or realign the existing ones to motivate investors to develop new essential drugs and control the cost of pharmaceutical markets. 74
Protecting patents (market exclusivity) of pharmaceuticals does not effectively stimulate drug research and innovation. Instead, it induced large amounts of research into drugs with little incremental therapeutic value (“me-too” drugs) and increased the price of potentially life-saving therapies. 75 The me-too drug is a pharmacologically active compound that is structurally related to a first-in-class compound, belonging to the same therapeutic class, and used for the same therapeutic purposes, but may differ in specificity, adverse reactions, or drug–drug interactions. 101
Due to the patent system, the pharmaceutical market monopoly led to misdirected innovation and marketing. High prices, high volumes of SF drugs, parallel imports, indirect price controls, and deadweight loss contribute to this misdirected innovation. The SF medicines adversely affect consumers’ health outcomes, harm the innovating drug company’s profitability by stealing their sales, and damage their reputation therapies. 75 It is important to realign financial incentives to foster therapeutic innovation and promote the rational use of medicines.75,102,103
Value-based pricing and public funding for clinical trials could help realign incentives toward genuine innovation while also keeping drug spending growth under check. Value-based pricing provides an incentive for discoveries and aligns research and development with social welfare. Public funding of clinical trials can reduce pharmaceutical costs, direct research efforts in a more socially productive, advanced innovation, and disincentivize “me-too” drugs.76,77 Savings could cover reward expenditures from reduced expenditures on patented drugs. 75
Another important tool for patient access to new medicines while managing uncertainty is managed entry agreements (MEAs). They are also referred to as risk-sharing agreements, special pricing arrangements, or patient access schemes. 78 Payers generally aim to provide patients with access to new medicines quickly after marketing authorization. At the same time, firms can maximize revenue by selling the highest possible volume of their products at the highest possible price as early as possible in the market exclusivity period. MEAs reduce the consequences of making a poor coverage decision in the face of uncertain effects of a new treatment on health outcomes and/or health care budgets. 78 These agreements can made as financial (confidential discount or rebate, patient-level treatment or expenditure cap, patient-level free initial treatment, population-level expenditure cap, and population-level price-volume agreement) and/or performance-based (patient-level coverage with evidence development, patient-level payment by results, patient-level conditional treatment continuation, population-level coverage with evidence development, and population-level payment by results). 78 These agreements could be an important tool to improve access to new innovative medicines in contextualized to specific country contexts. 104
Health system leadership and governance
Integrated leadership and management process is an important nonfinancial incentive for improving access to medicines by creating a positive work climate. 79 The health care service environment should be inspirational and accommodative for all workers, irrespective of their capacity and type. The leadership model that fits all these baskets of need is servant leadership. 80 This approach addresses the following dimensions: listening, empathy, healing, awareness, persuasion, conceptualization, foresight, stewardship, commitment to the growth of people, and building community. Servant leaders seek to develop a culture based on trust, justice, concern for others, a safe psychological environment, transparency, confidentiality, learning, constructive feedback, and service attitude. The leader builds a community in which employees are committed to putting the organization’s goal and the interest of customers first. 81 It is associated with improved psychological well-being, favorable job attitudes, improved job performance, and decreased workplace deviance 82 Another leadership style that can motivate health workers to perform beyond expected levels is transformational leadership. 56 Poor leadership in health care systems can adversely affect organizational work cultures and employee satisfaction and lead to burnout, staff turnover, dissatisfied workers, critical medical mistakes, and labor disputes. Internal employee satisfaction is a key for improving pharmaceutical supply chain performance.83,84,86 Employee satisfaction is a means for improving managerial efficiency in the organization. 85
The pharmaceutical sector is a wide and complex sector, including research and development, manufacturing, registration, pricing, licensing of professionals and establishments, selection of medicines, procurement, distribution, inspection, prescription, dispensing, PV, and medicines promotion. Each step is vulnerable to corruption and involves different professional experts, lawyers, and researchers. 88 Large amounts of money spent on the pharmaceutical sector (i.e. 20%–60% of the public health budget) are an attractive target for corruption. Corruption in the pharmaceutical supply chain reduces access to essential medicines, threatens public health, reduces the economy, and erodes public institutions’ image and credibility. 88
Robust governance of health system is necessary to ensure that resources devoted to the health sector ensure adequate access to health care and improved health.40,87 Efficient, effective, equitable, and responsive governance leads to positive health outcomes. At the same time, the nontransparent system can undermine the efficient and effective use of health care resources. 88 Increasing the level of transparency and accountability in the pharmaceutical system decreases vulnerability to corruption. Opportunities for corrupt practices can be minimized when standards and clear responsibilities are assigned; decisions and results are documented and made public to show whether standards and commitments have been met; and corrective actions, including sanctions, are enforced if necessary (Figure 4). 89

Impact of leadership, management, and governance on access to essential medicines and counterfeit drug marketing and distribution. Adapted from managers WHO lead and health finance and governance, expanding access and improving health.
Systematic approach to address constrained access to medicines and counterfeiting
Limited access to medicines and marketing and SF medicines are interrelated challenges of the health care system in developing countries. Both share a common underlying pathology and should be managed together. These factors include supply chain-related factors, drug regulatory capacity, pharmaceutical policy-related factors, misalignment of drug production and public need, and poor health system leadership and governance (Figure 5).16,53,54,65

Cases of underreporting of adverse drug reactions (ADRs) and strategies for improving PV and medication safety management systems adapted from available literature.
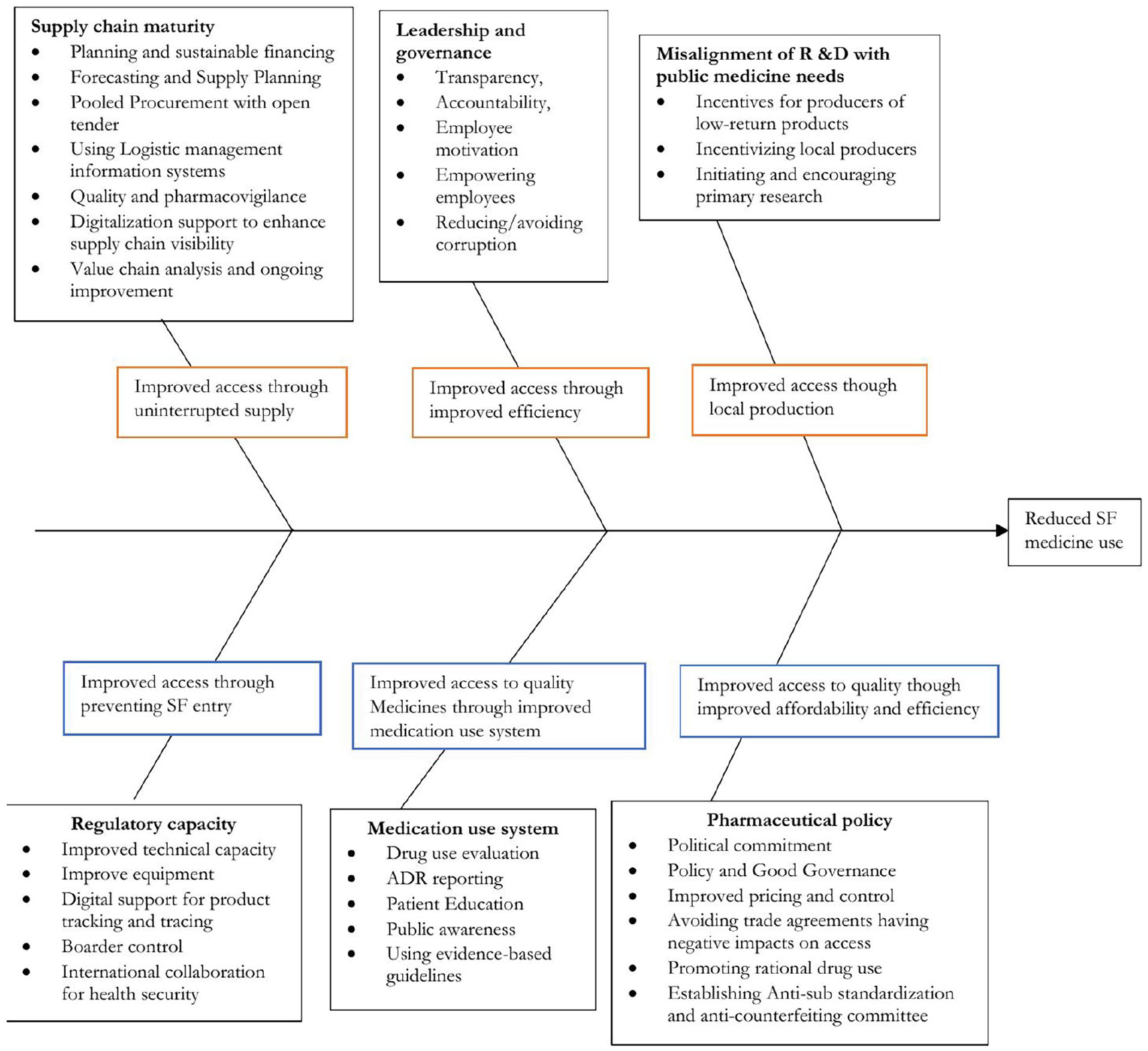
An Ishikawa diagram showing how the strategies implemented to improve access reduced SF medicine marketing and use, adapted from different literature.
Discussion
In this scoping review, we showed how improved access could reduce the continuous surge of marketing of SF medicines in Africa. Access to quality medicines is still a major problem in Africa and will continue as a threat for the next decade of health care.16,53,54,65,105 In addition to this, the burden of SF medicines is 20%–40% in developing countries. 20 Addressing constrained access requires involvement from the government, regulatory authorities, manufacturers, importers and exporters, health supply managers, health professionals, patients, and the public, and national and international trade agreements. 44 The most important causes of SF medicine marketing are constrained access to quality medicines, weak technical capacity of national regulatory bodies, poor supply chain management, weak pharmaceutical policy and implementation, misalignment of new drug development research, and the public need and poor governance.19,20,106 –111 Addressing these factors (themes) can improve access to medicines and reduce SF medicine marketing in Africa.
Theme 1: Supply chain and trade-related factors
The unaffordability of medicines is the reason for constrained access to medicines in developing countries.66,90 Removing taxes and duties on essential medicines, controlling markups, using pooled procurement often with more competitive methods, establishing efficient procurement period and frequency, enhancing local production and improving the health insurance system, and providing incentives for pharmaceutical manufacturers to invest in quality medicine production can improve affordability. Accessibility of health services can be addressed by increasing the operational hours of clinics providing free or subsidized care, decreasing waiting times by streamlining organizational processes and changes in regulations, and increasing the perceived quality of care.53,54
An inefficient procurement process contributes to constrained access to essential medicines. 16 Manipulating the procurement system for efficiency can help to ensure affordability and availability.65,112 Applying different procurement methods with due consideration of good procurement principles can help improve access to medicines. 25 The key principles of good procurement include reliable and sound financial management, procurement by generic name, explicit specification of standards, limitation of procurement to essential medicine list, supplier qualification, increasing procurement volume, and competitive procurement. And order quantities based on a reliable estimate of forecasted actual need, transparency and written procedures, separation of key functions, product quality assurance program, annual audit with published results, and regular reporting of procurement performance indicators. 65
In addition to this, procurement system review and looking at common bottlenecks are important to improve future planning. 113 Some of the identified bottlenecks include inaccurate plans, mismatched budget cycle, and funding cycle, delayed request submission, inadequate or missing specifications, specification changes made after purchasing procedures are initiated, mid-term budget cuts, withholding of programmed funds, slow contract planning by procurement unit, and problems with advertising. Similarly, bid deadline extension to accommodate amendment of bidding documents, slow approval process, protests by losing bidders and cancelation of a bid, shortage of raw materials, overbooked manufacturing schedule, shipping problems, slow processing of documents, no access to funds for port fees, irregularities in goods or documents, and pharmaceutical registration issues are reported bottlenecks. 65
Theme 2: Misalignment of new drug research and patient needs
The SF medicines adversely affect consumers’ health outcomes and harm the innovating drug company by stealing their market share, damaging their reputation, and reducing the incentives to innovate. 114 Therefore, the establishment of different incentives for brand producers like value-based pricing, open public funding for clinical trials,76,77 MEAs schemes, 78 and using compulsory licensing under TRIPS flexibilities 61 can help to improve access to essential medicines and reduce SF medicine marketing.
Improving quality to the highest level and reducing the price of brand products can facilitate the seizure of SF medicine marketing. Furthermore, the strategies that improve the brand-name company’s profit may benefit the counterfeiter inadvertently and even hurt consumer welfare. Therefore, it is important to carefully consider a trade-off among different objectives in implementing an anti-counterfeiting strategy. 115
Due to pharmaceutical market information asymmetry and agency problems, other approaches to increase access to medicines like avoiding trade agreement provisions that could reduce access to medicines, and making use of TRIPS flexibilities can improve access to medicines. 116 Similarly, supporting the production and introduction of generic medicines, applying strategies to delink the cost of medicines development and the final price of the medical product, and introducing country-specific pharmaceutical price control can contribute to improved access. 92
Theme 3: Prevention, detection, and response
Establishing functional PV is important to improve access to medicines. It requires creating public awareness about SF medicines to reduce the risk of the ultimate user, training health professionals and primary stakeholders of supply chain management, creating a motivational environment for reporting, digitalizing reporting systems, introducing PV in undergraduate health curricula, addressing policy gaps like poor oversight and weak penalties, 117 and improving the efficiency of the health care system by improving leadership and governance to reduce financial problems which is another challenge PV activities. 93 However, studies in Africa showed a low level of maturity in PV systems. For example, a comparative study done in East Africa (Ethiopia, Kenya, Rwanda, and Tanzania) showed that the national PV system did not have access to data on drug utilization and their respective maturity level was low and different. 118 Designing country-specific interventions to improve PV systems is important.
Theme 4: Pharmaceutical policy
Establishing formal anti-counterfeiting and anti-substandardization committees (AC-ASSC) at the national, regional, and facility levels, that focus on generating intelligence in anti-counterfeiting; formulating strategic policy direction for control; and influencing the behavior of stakeholders through (regulation, enabling, motivation, inspiration, coalition building, and communication) are important for reducing SF medicine marketing and use. In addition to this, influencing behavior through creating an enabling environment for the control and detection of SF medicines, and ensuring accountability of stakeholders regarding SF medicines can be done by AC-ASSC. 51
Theme 5: Regulatory capacity factors
Improving the technical and laboratory capacity of regulatory systems can cure some of the constrained access problems in Africa.53,54,66,67 Critical points for quality assurance of pharmaceutical procurement include product selection, product certification, contract specifications, inspection of shipments, targeted laboratory testing, and post-marketing problem reporting system or PV. 65 Pharmaceutical companies require functioning regulatory systems to avoid unnecessary delays in the marketing and distribution of their products. Countries with poor regulatory capacity delay market entry of quality products and create opportunities for SF medicine marketing. This affects quality producers, the health system, the government, and ultimately patients. 119 The regulatory system of many LMICs has a poor capacity to regulate medicine in their respective countries. 120 For example, a study conducted to evaluate national medicine regulatory agency capacity in Rwanda showed that 179 (71%) WHO indicators were fully implemented. 121 In addition to the regulatory system immaturity, the technical capacity of the regulatory workers is also low in LMICs like Africa. Therefore, it is important to train regulatory professionals to improve access to quality medicines. 122 In addition to this, regional harmonization of regulatory systems can improve access to medicines through improved collaboration across countries. 123
Theme 6: Health leadership and system governance
The pharmaceutical sector is a wide and complex sector, including different steps. Each step is vulnerable to corruption and involves different professional experts, lawyers, and researchers.88,124,125 Appropriate leadership and good governance can help to improve access to essential medicines by improving managerial efficiency through preventing corruption, and empowering and inspiring employees. 88 In addition to this, in an organization where there is a culture based on trust, justice, concern for others, transparency, confidentiality, learning, constructive feedback, and an attitude of service, there is little or no room for corruption.126,127 Finally, using technologies to enhance shipment visibility, transparency, accountability, and integrity in the system is important to reduce corruption in the sector. 128
Strengths and limitations
The strengths of this study rely on its comprehensive nature and inclusion diagrammatic presentation of how strategies implemented to improve access reduced SF medicine marketing and use. However, being the scoping review and inclusion of studies with different designs, it was possible to judge the quality of included studies. Therefore, the findings of this review should be extrapolated beyond the targeted countries with caution.
Conclusion
Access to quality essential medicines is still a major problem in LMICs in Africa and will continue as a threat for the next decade of health care. Failure to ensure access to medicines is the major reason for the availability of SF medicines in the legitimate supply chain. Manipulating the entire supply chain for efficiency, avoiding trade agreements that could reduce access to medicines, using compulsory licensing provisions, introducing generic medicines and pharmaceutical price control, providing incentives for drug development, and promoting rational use of medicines can improve access. Looking through the lens of improved access to quality medicines can reduce SF medicine marketing and use, that is, ensuring access through uninterrupted supply, improved efficiency, enhanced local production, preventing SF medicine entry, improved medication use system, and improved affordability.