
Abstract
Objectives:
The aim of the study was to verify the effectiveness of telemedicine in randomized controlled trials (RCTs) in terms of its influence on physical conditioning, quality of life, and health conditions in adults/elderly people affected by chronic diseases.
Design:
This was a systematic review and meta-analysis.
Methods:
The search covered RCTs published from 2011 to 2021 and was conducted using the PubMed, Embase, PEDro, Lilacs, and Cochrane Library databases, on volunteers of both sexes, that were rehabilitated, and/or monitored, and/or evaluated, specifically, via remote care. The extraction, quality of studies, and risk of bias were assessed using the RoB2 (risk of bias) tool, for analysis of the strength of evidence, the GRADE (Grading of Recommendations Assessment, Developing, and Evaluation) method was used, and for the preparation of meta-analysis was used at RevMan 5.4 (Review Manager) was used.
Results:
The database search identified 3949 potential articles for screening, 13 of which were eligible for the present systematic review, involving 1469 participants with chronic diseases (chronic obstructive pulmonary disease (COPD), asthma, heart failure, diabetes mellitus, and fibromyalgia). Through the meta-analysis, an advantage was identified for the remote intervention on physical conditioning (p = 0.001), with an estimated effect of 0.29 (0.11, 0.46) and on health conditions (p = 0.0004), –0.30 (–0.47, –0.14), while for quality of life, no significant difference was identified (p = 0.90), 0.01 (–0.13, 0.14).
Conclusion:
Telemedicine has clinical effectiveness for the outcome of physical conditioning and general health conditions in adults with chronic diseases when compared to usual care without face-to-face intervention.
Introduction
Non-communicable diseases (NCDs) comprised the greatest fraction of deaths, contributing to 73.4% of total deaths worldwide in 2017. With a growth of 22.7% from 2007 to 2017, with an additional estimate of 7.61 million deaths. Regarding lung diseases, chronic obstructive pulmonary disease (COPD) was responsible for 3.2 million deaths, and asthma was responsible for the other 495,000 deaths in this portion. 1
They are also the leading cause of morbidity among men and women, with an estimated 1.6 billion cases in 2017. These are identified by disability-adjusted life years (DALYs), which assume the sum of life years of potential lost due to premature mortality, and years of productive life lost due to disability. Respiratory diseases were responsible for 112 million DALYs, of which 81.6 million were due to COPD and 22.8 million were due to asthma. 2
These diseases are commonly treated face-to-face, with medication, guidance, and rehabilitation in hospitals and clinics. However, with technological advances, it has been possible to implement other forms of treatment, such as telemedicine, telehealth, and virtual rehabilitation. Such treatments, through the use of telecommunications, aim to reduce the side effects of diseases, in addition to improving cost-effectiveness, which has drastically impacted the health system.3,4
Telemedicine is defined as the use of information and telecommunications technologies to carry out healthcare from a distance, 5 that aims to provide medical care to patients without physical contact, through the use of electronic devices capable of connecting health professionals to patients and to each other, facilitating the enforcement of exams, diagnoses, and remote clinical follow-up. Telemedicine can also provide self-care and self-monitoring regimens for patients at home, which are ideal strategies to facilitate patient management in the absence of face-to-face consultations. 6
A systematic review reported that telerehabilitation assessments demonstrate positive results in controlling pain and edema, as well as improving range of motion, muscle strength, balance, gait, and functional assessment. 7 Research carried out in the field of musculoskeletal physiotherapy using telehealth tools has shown high levels of patient satisfaction regarding the form of remote intervention.8 –10 When comparing face-to-face interventions with the use of technology for remote assistance, the degree of satisfaction was significantly higher for the remote technique. 11 Although more studies are needed on the economic impact of using telehealth, research so far has shown a favorable cost-benefit ratio for this form of intervention compared to the traditional face-to-face model.12 –15
Although a review of the telehealth chronic disease management system has been conducted, addressing quality of life, depression, anxiety, and fatigue, 16 no studies have been found that specifically address physical conditioning and other health conditions.
Thus, this review aimed to verify the effectiveness of remote care in the assessment, and/or monitoring, and/or rehabilitation of adults/elderly people affected by chronic diseases, in terms of physical conditioning, quality of life, and general health conditions, through studies of randomized controlled trials (RCTs), for the order to provide information that can guide clinical practice, development of scientific projects (applications, electronic devices), deepening field research, in addition, to point out the best way of care between remote and face-to-face care, in mitigating the side effects caused by chronic diseases, thus presenting alternative care for adult/elderly patients, unable to access ambulatory care.
Methods
The preparation of this review followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The study is a systematic review with meta-analysis, performed in 2021, and a research protocol was registered on May 16, 2021, in the international database of systematic reviews, PROSPERO (CRD42021247886). Approval by a research ethics committee to conduct this meta-analysis was not required in Brazil. Research involving only public domain data that does not identify the research participants, such as a bibliographic review, does not necessitate approval by the CEP-CONEP System. The question guiding this review was as follows: Does telemedicine have superiority for the outcomes of physical conditioning, quality of life, and general health conditions of adults and/or elderly people with chronic diseases, when compared to usual care without face-to-face intervention, in RCTs. The hypotheses were: (1) Telemedicine is an effective alternative for the assessment, monitoring, and rehabilitation of patients suffering from chronic diseases. (2) Telemedicine is not an effective alternative for the assessment, monitoring, and rehabilitation of patients suffering from chronic diseases. To identify relevant studies, a search strategy was developed using the following keywords indexed in Medical Subject Headings (MeSH).
The databases searched were PubMed, Embase, PEDro, Lilacs, and the Cochrane Library. The search was performed, covering articles published from 2011 to 2021. The selected articles were manually organized according to the following search-term strategy: “chronic disease”/exp OR “diabetes mellitus”/exp OR “hypertension”/exp OR “chronic obstructive lung disease”/exp OR “malignant neoplasm”/exp OR “obesity”/exp OR “fibromyalgia”/exp AND “adult”/exp OR “aged”/exp AND “telehealth”/exp OR “telemedicine”/exp OR “telerehabilitation”/exp AND “traditional medicine”/exp OR “primary health care”/exp OR “self care”/exp OR “homebound patient”/exp OR “health education”/exp OR “medical information”/ exp AND “clinical outcome”/exp OR “treatment outcome”/exp.
After obtaining the relevant primary studies and eliminating duplicates, the articles were evaluated for their relevance, respecting the inclusion and exclusion criteria, as established by the population, intervention, comparison, and outcome (PICO) question.
The extraction and evaluation of data were performed by two authors who independently examined the records, selecting them for their quality and risk of bias through the Cochrane risk of bias (RoB2) tool, and in case of disagreement, a third author was asked to arbitrate.
Quality assessment and risk of bias
The potential risk of bias related to randomized trials was assessed using the RoB2.0. This tool assesses the risk of bias from five domains, including bias due to randomization/processing, bias due to deviations from intended interventions, bias due to lack of outcome data, bias in outcome measurement, and bias in the selection of reported outcomes. A domain was classified as low risk of bias when the evaluators found clarity in the results and that the involved researchers had methodically followed the objective of the study. A domain was assessed as high risk when the study contained considerable levels of bias, thus significantly decreasing confidence in the results. 17
Data extraction
Table 1 was constructed containing the authors’ names, follow-up time, study design, sample size, type of intervention, age group, and research results.
Characteristics of studies included.

Experimental group (Exp.): telemedicine (telehealth, telerehabilitation); control group (Cont.): traditional medicine without face-to-face intervention; N: number of participants; RCT: randomized controlled trial; M: mean; SD: standard deviation; p-value (< 0.05): statistical significance; COPD: chronic obstructive pulmonary disease; SGRQ: St George’s Respiratory Questionnaire; CAT: COPD Assessment Test; 6MWT: 6-minute walk test; ACQ: Asthma Control Questionnaire; CRDQ: Chronic Respiratory Disease Questionnaire; FIQR: Fibromyalgia Impact Questionnaire-Revised; mAQLQ: Mini-Asthma Quality-of-life Questionnaire; BDI: Beck Depression Inventory; HbA1c: glycated hemoglobin; KCCQ: Kansas City Cardiomyopathy Questionnaire.
Meta-analysis and data synthesis
Data synthesis was qualitative for the strength of evidence and quantitative through meta-analysis.
For the strength of evidence, the GRADE (Grading of Recommendations Assessment, Developing, and Evaluation) method was used, which classifies into four levels: high, moderate, low, or very low. Factors that lower the strength of evidence (study limitations, inconsistency of results, indirect evidence, imprecision, and publication bias), and (large magnitude of effect, dose–response gradient, and confounding variables that may have reduced the observed effect), are the factors that increase the strength of evidence. High confidence, when it is highly likely that the review finding is a reasonable representation of the phenomenon of interest. Moderate confidence, when the review finding is likely to be a reasonable representation of the phenomenon of interest. Low confidence, when it is possible that the review finding is a reasonable representation of the phenomenon of interest. Very low confidence when it is unclear whether the review finding is a reasonable representation of the phenomenon of interest. 31
As for the preparation of the meta-analysis, the tool used was RevMan 5.4 from the Cochrane Group. Understanding that the true effect of the treatment in the studies may be different between them, the type of model for analysis was the random effect, with continuous data type, in the inverse statistical method of variance, with the measure of effect being the difference of the standardized mean, with a 95% confidence interval. The results were synthesized to identify statistical heterogeneity, confidence interval, probability of significance, the weight of studies, and the trend of the effect between the analysis groups (intervention and control), as evidenced by the figure of the forest plot, for a better understanding of study trends and the meta-analysis conclusion. 32
Results
After searching the databases, 3949 articles were initially identified, of which 1065 were removed for being duplicates, 2613 were removed by filters used in the screening tools, and 144 were removed for other reasons (The articles were either not available in full or still in progress, and did not pertain to the subject of the study.). The remaining 127 articles underwent title analysis, and 54 were eliminated, leaving 73 articles to be subjected to a more careful analysis of content and potential risk of bias. Of these, three articles were eliminated for presenting a high risk of bias; 54 were eliminated for being protocols, by the non-randomized study design, by presenting a comparison outside the domain of this review, or because there was no complete data; two were eliminated because they only brought the data obtained between the groups; and one was eliminated for presenting patients ineligible for the inclusion criteria of this review. Ultimately, 13 articles were selected for inclusion in this research (Figure 1).

Flow diagram of selected studies.
According to a PubMed search of articles published between 2011 and 2021, research on telemedicine in adults with chronic diseases has been growing annually, with 103 articles published in 2011 and 179 in 2020, reaching a peak in 2019 with 259 publications.
Of the 13 trials included in this review, four are from the United States of America, two from Australia, and there was one publication each from Canada, Germany, Greece, Spain, Switzerland/Germany, Taiwan, and Turkey, nine of which are related to COPD, one with asthma, one with heart failure, one with diabetes mellitus (DM), and one with fibromyalgia. The included studies had a low or medium risk of bias according to the assessments of the authors of this review; this assessment was based on the Cochrane tool (RoB) (Figure 2).
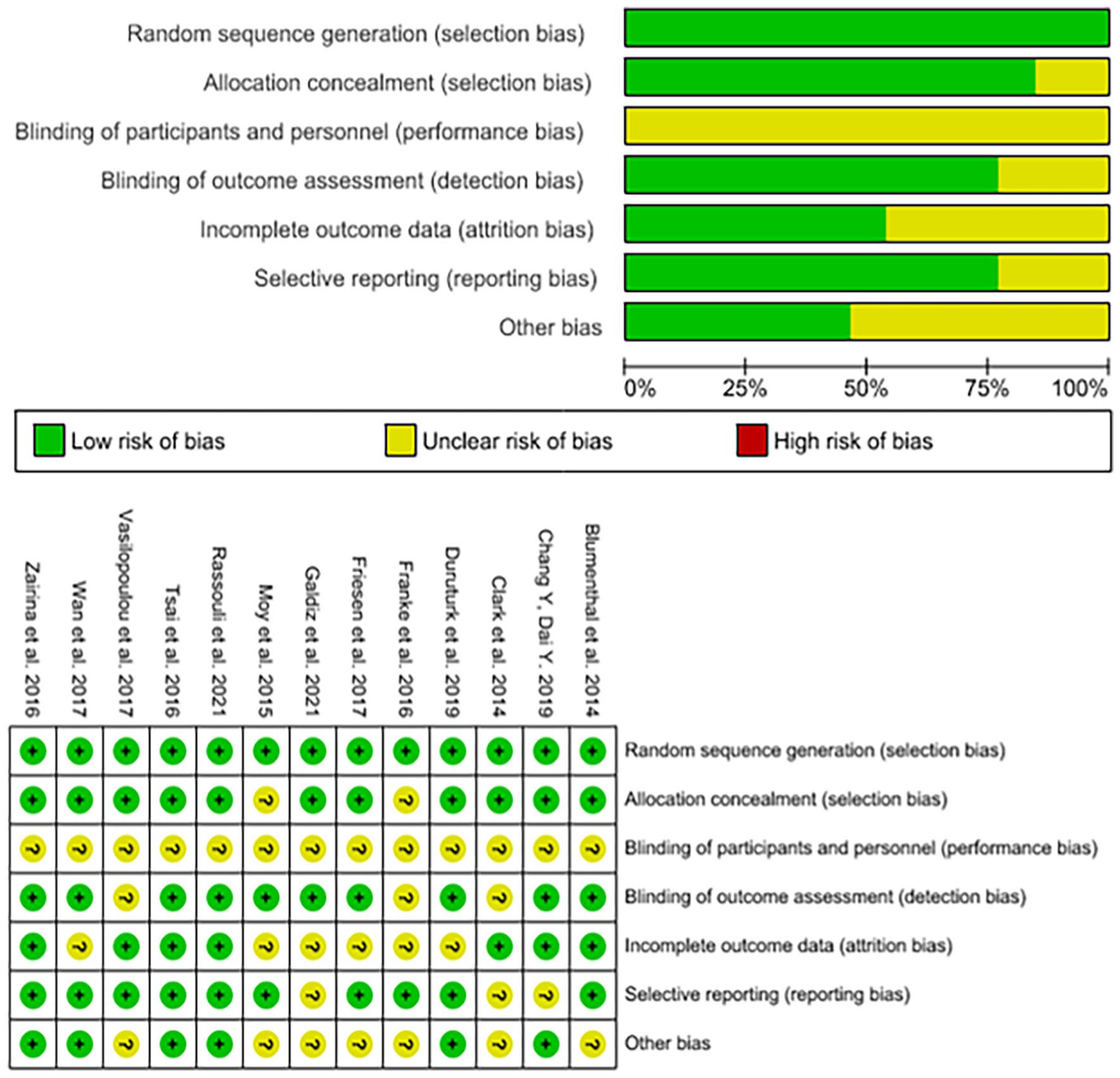
Risk of bias graph and summary, authors' judgments on each risk of bias item for included studies.
The data on physical conditioning, quality of life, and general health conditions are presented in Table 2 and Figure 3.
Summary of findings (grade evidence)—telemedicine compared to traditional medicine without face-to-face intervention.

CI: confidence interval; SD: standardized difference; SMD: standardized mean difference; 6MWT: 6-minute walk test; SGRQ: St George’s Respiratory Questionnaire
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect
Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect
Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
The quality of evidence was downgraded by one level due to the imprecision due to the small sample size.
Due to the nature of the intervention, it was impossible to blind the participants to the intervention.
The quality of evidence was downgraded by one level due to the indirectness regarding the difference in the population of the included studies.
The quality of evidence was downgraded by two levels due to the indirectness regarding the difference in population, and methods of intervention.
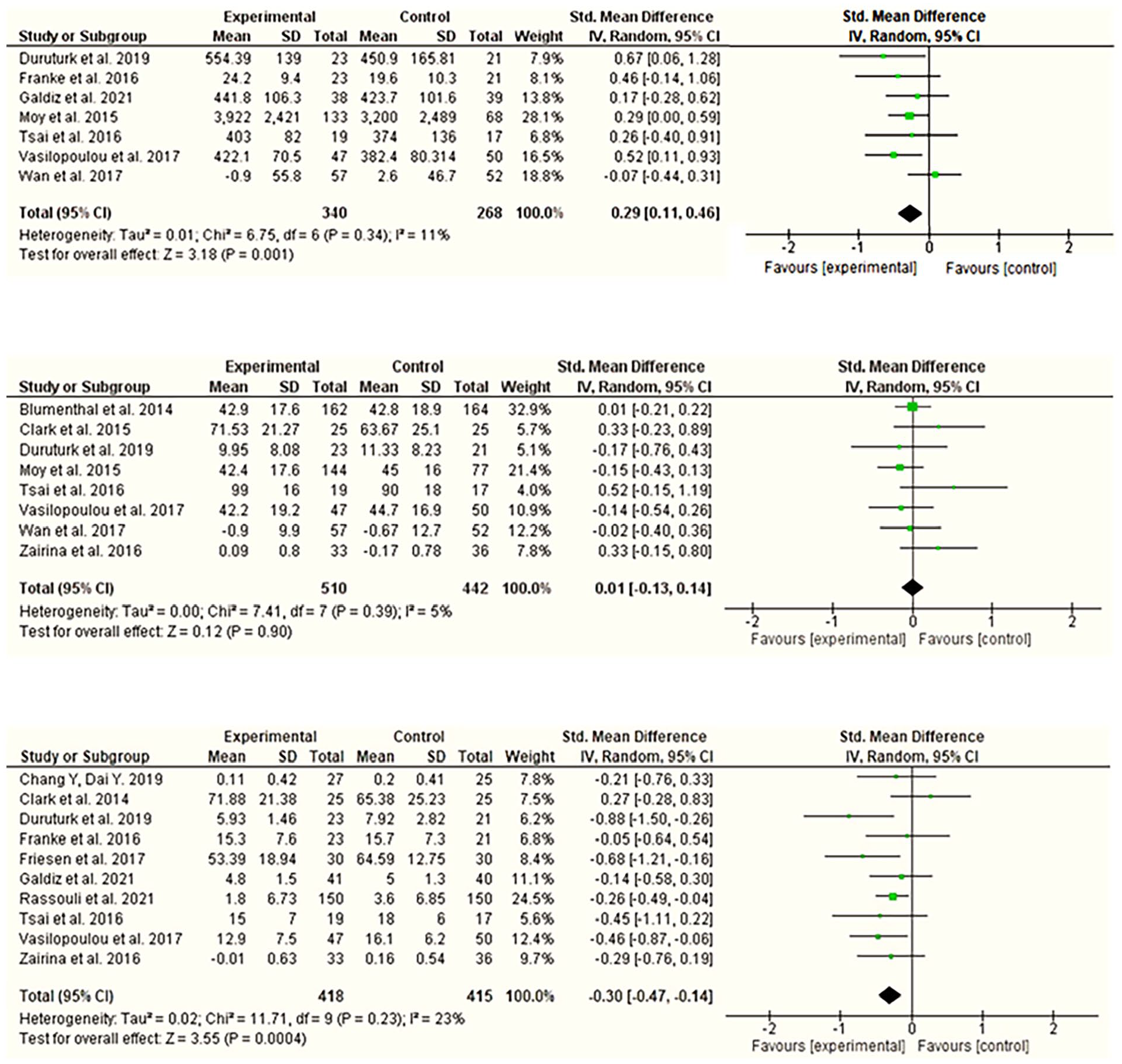
Forest plot comparison: Outcomes (physical conditioning, quality of life, and general conditions health), respectively.
Physical conditioning
A pedometer-based remote walking program can improve daily step counts in people with COPD after 4 months of intervention. 19
Telemonitoring is a simple method capable of improving physical training and physical activity at home in patients with COPD in the stable phase of the disease. 20
Home maintenance telerehabilitation was equally effective as outpatient rehabilitation and superior to usual care, showing an increase in daily activities. 23
Telerehabilitation can improve endurance exercise capacity in COPD patients compared to usual care. 22
The association of a pedometer with an instructional website improves daily step count and maintains walking for more than 3 months, mitigating declines in physical activity in the changing weather season. 21
Physical fitness significantly improved in patients with type 2 DM in the telerehabilitation group. 28
An important negative influence of exacerbations on physical function was identified during the study, and only patients in the telerehabilitation group without exacerbations appeared to increase their mean distance in the 6-min walk test compared to baseline in 12 months. 26
Quality of life
A pedometer-based remote walking program can improve quality of life domains over a 4-month intervention in people with COPD. 19
Telerehabilitation was as effective as outpatient hospital rehabilitation and superior to usual care in assessing the quality of life over 12 months. 23
The telerehabilitation group showed a significant trend toward improvement in the total quality of life score on the Chronic Respiratory Disease Questionnaire (CRDQ). 22
Although the statistical analysis of the survey did not demonstrate superiority between groups for quality of life, reports from participants in the Taking Healthy Steps study say otherwise. 21
Telerehabilitation through calisthenics exercises can be effective for the decline of depression and the improvement of the general state of health when compared to the control group. 28
A telehealth coping skills training program improves the psychological and somatic quality of life, as well as the functional capacity of volunteers with COPD. 18
Home intervention was effective for quality of life in volunteers with heart failure. 27
Self-management telehealth with an action plan and regular monitoring can improve the quality of life of asthmatic volunteers during pregnancy. 29
Health conditions
Although the intervention and control groups showed improvements in relation to baseline, no significant difference was identified in the COPD assessment test score. 20
Home maintenance telerehabilitation is effective for the maintenance of pulmonary rehabilitation, reducing the risk of acute exacerbation and the number of hospitalizations in volunteers with COPD. 23
Telerehabilitation, when compared to usual care, can improve self-efficacy and psychological status in COPD patients with high anxiety and depression scores in COPD patients. 22
Telerehabilitation is safe and effective as an alternative treatment model for the control of type 2 DM, which can improve glucose control and be an ally for the decline of depression, in addition to saving time, labor, and treatment costs. 28
Telerehabilitation has not shown general superiority over current clinical practice for volunteers with COPD. However, when longitudinal analyses were observed, during stable periods without disease exacerbations, benefits could be identified. 26
Telehealth was not successful in reducing mortality and the number of hospitalizations in patients with COPD. 18
Remote intervention improves health and functional status outcomes, self-care, self-efficacy, metamemory, and disease knowledge in volunteers with heart failure. 27
Self-management with an action plan, and regular monitoring by the medical team, improves the clinical status of volunteers with asthma during pregnancy, and reduces the number of unplanned hospitalizations. 29
A remote self-management education program can be a viable alternative for COPD patients to improve their knowledge about the disease, self-efficacy, level of activation, and ability to better deal with the impact of the symptoms of the disease, in addition to helping with the engagement of beneficial behaviors. 24
Telehealth reduced by 50% the symptoms of volunteers with COPD, in the COPD assessment test, an important indicator of disease progression. 25
A cognitive-behavioral pain course, offered remotely for adults with fibromyalgia, improves symptoms, such as depression, anxiety, and pain. 30
Discussion
This systematic review identified RCTs that used remote intervention for assessment, monitoring, or rehabilitation to study outcomes regarding physical conditioning, quality of life, and general health conditions in volunteers, adults, and the elderly with chronic diseases, as other reviews did not find significant evidence comparing telerehabilitation with face-to-face rehabilitation.
Telemedicine and its sub-areas (telehealth and telerehabilitation) were used according to various methods and with various electronic devices to adapt the quantity and duration of interventions, respecting the chronic conditions as well as the exacerbation of symptoms of each disease.
A remote program was used with 799 participants, 683 of whom had COPD, 36 of whom had asthma, 30 of whom had fibromyalgia, 25 of whom had heart failure, and 25 of whom had DM. The studies included presented a low or medium risk of bias, according to the assessments of the authors of this review.
The limited sample size, the short follow-up time, the number of interventions, and the lack of blinding of the team of investigators and participants regarding the interventions were the main limitations found in the studies. The lack of blinding for the intervention was justified by the nature of the study and certified by the blinding of the outcome assessors in more than 75% of the cases.
Although there is a difference between the studies regarding the number of volunteers, follow-up time, and number of interventions, a comparison among them was possible. In summary, the mean duration of the interventions was 24 weeks, with the study by Duruturk et al. having the shortest analysis time (6 weeks) and the study by Galdiz et al., the one with the longest time (48 weeks). In terms of the size of the sample undergoing intervention, the study by Tsai et al. had the lowest number (19 volunteers), and the study by Blumenthal et al., had the largest sample (162 volunteers), with an overall mean among all studies of 61 participants.
The technology used in remote care was simple, accessible, and with good applicability (smartphones, notebooks with cameras, and pulse oximeters). The data were sent by electronic devices, such as text messages, email, or the application platform. However, the main adversities found regarding the effectiveness of telemedicine are due to the participants' level of understanding of technology and their skill in handling electronic devices away from the team. Lack of accessibility, poor Internet quality, and a lack of electricity were other reported problems.
Of the 13 studies included, Galdiz et al., and Blumenthal et al., demonstrated that telemedicine was not generally superior to typical care, especially in terms of mortality and hospitalization outcomes. When the outcome was physical conditioning, Franke et al., Moy et al., Tsai et al., and Wan et al., concluded that the intervention was feasible and effective. Blumenthal et al., Clark et al., Franke et al., Galdiz et al., Moy et al., and Zairina et al., identified an improvement in the quality of life of the volunteers. In addition, in terms of the outcomes of health conditions (intensity and frequency of pain, exacerbation of symptoms, level of activation, self-efficacy, anxiety, and depression). Chang & Dai, Clark et al., Duruturk et al., Friesen et al., Galdiz et al., Rassouli et al., Tsai et al., Vasilopoulou et al., and Zairina et al., concluded that telemedicine indicated significant results.
In general, it was possible to identify in the qualitative analyses, that telemedicine shows superior effects, in terms of physical conditioning, quality of life, and general health conditions, when compared to those who did not receive any face-to-face rehabilitation, or were limited to educational guidelines only for self-care, but in the quantitative analysis, the results for quality of life showed no statistical difference between the groups.
The main limitation of this review is likely due to the careful selection process, which chose only RCTs, that used outcomes of telemedicine compared to outcomes of usual treatment without intervention in adult patients with some chronic disease, which may have contributed to a limited sample and heterogeneity regarding the studies included, due to a higher prevalence of studies related to chronic respiratory diseases. The strength of the evidence of the analysis was reduced mainly by indirect evidence (difference in population, comparison, or outcomes) and imprecision (large confidence interval, small sample, and event size).
Therefore, more experimental studies are needed, that carefully follow the entire analysis process, in a standardized form, with data loss limited to 10%, and a longer follow-up and sample period, in addition to investigating the effects of telemedicine on all the participants' physical and social conjunctures as well as the evaluation of effectiveness in other chronic diseases.
However, in most studies that used the 6-minute walk test to identify the effects of a remote intervention program based on physical exercises, a statistical significance in favor of the experimental group was evident, in addition to suggesting that the adoption of physical activity monitored by trained professionals can be beneficial to stable patients affected by chronic diseases.
Conclusion
The results of this systematic review identified the effectiveness of telemedicine for the outcomes of physical conditioning and general health conditions, indicating satisfactory clinical advantages for health professionals who apply remote intervention for the assessment, monitoring, and rehabilitation of adult/elderly patients with chronic diseases. In addition, telemedicine was shown to be a viable tool in the mitigation of inherent risks to patients with chronic diseases.
In the quality of life outcome, there was no statistical difference between the groups, suggesting nullity between telemedicine and the control group, in the quantitative analysis. However, the qualitative analysis brought a better perception of the volunteers, regarding the remote intervention, and its effectiveness.
However, the continuous study is needed to explore the different barriers of technology and telemedicine’s applicability to the health field, including quantitative and qualitative research that provides effectiveness and management data to facilitate understanding to include in the daily clinical practices of any patient with chronic disease, regardless of age and education level. It is recommended that future studies utilize a longer follow-up by the health team and a larger sample covering the entire population diversity (age, gender, race, education level, and clinical conditions).
Supplemental Material
sj-docx-1-map-10.1177_27550834231197316 – Supplemental material for Analysis of the effectiveness of remote intervention of patients affected by chronic diseases: A systematic review and meta-analysis
Supplemental material, sj-docx-1-map-10.1177_27550834231197316 for Analysis of the effectiveness of remote intervention of patients affected by chronic diseases: A systematic review and meta-analysis by Demetrius Ruben Borges de Rezende, Isadora Andrade Neto, Denise Hollanda Iunes and Leonardo César Carvalho in The Journal of Medicine Access
Footnotes
Acknowledgements
This study was supported by CAPES—Coordination for the Improvement of Higher Education Personnel—Brazil—Code 0001, UNIFAL—Federal University of Alfenas—Postgraduate Program in Applied Health Biosciences. Tutorial Education Program MEC-SESu.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.